
Abstract
Dentin matrix is a natural scaffold derived from complete or partial demineralization of human or animal dentin, capable of releasing growth factors and proteins essential for tissue regeneration and repair. Recent studies have identified the dentin matrix as an exceptional scaffold for the regeneration of dental and osseous tissues, attributed to its excellent biocompatibility, advantageous mechanical properties, and capacity for chemotactic induction. A substantial body of evidence supports its efficacy in promoting the formation of dentin bridges, facilitating the regeneration of the pulp-dentin complex, enhancing de novo bone formation, and mitigating alveolar bone resorption, thereby presenting innovative therapeutic approaches for the reconstruction of oral tissues. This review categorizes dentin matrices based on the degree of demineralization into partially demineralized dentin matrix and completely demineralized dentin matrix. Furthermore, the review consolidates current advancements and outlines future directions for the application of dentin matrix in pulp-dentin complex and alveolar bone regeneration. Despite the ongoing challenges related to the establishment of standardized preparation protocols, the continuous advancements in tissue engineering and regenerative medicine exhibit an advantageous potential for clinical application.
Impact Statement
Dentin matrix-based scaffolds represent an innovative strategy for regenerating the pulp-dentin complex and alveolar bone. This paradigm shift from prosthetic replacement to biological restoration can preserve compromised teeth and enhance bone regeneration, significantly improving clinical outcomes.
Introduction
Dental hard tissue loss or partial edentulism caused by multiple etiologies including dental plaque and nonplaque factors, significantly impacts patients’ quality of life. Conventionally, tooth defects are restored using composite resins, gutta-percha, and sealants, while partial or complete edentulism is managed with implants and fixed or removable prostheses. However, advances in tissue engineering 1 suggest that damaged dental tissues and alveolar bone may potentially be regenerated using bioactive materials. The regeneration requires multipotent stem cells with odontogenic/osteogenic differentiation capacity, scaffolds that support cellular proliferation and guide differentiation, and a biocompatible microenvironment to prevent immune rejection.
Extracellular matrix (ECM) 2 is an ideal scaffold for tissue regeneration, as it delivers molecular signals for lineage-specific differentiation and integrates mechanical cues with stem cells. The mechanical properties of tissues, including elastic modulus, tensile strength, and failure strain, are typically diminished following decellularization. 3 Consequently, while most ECM-based scaffolds exhibit excellent remodeling capabilities in soft tissues (e.g., skin, 4 liver, 5 blood vessels 6 ), their performance in hard tissue remodeling remains suboptimal.
For oral tissue regeneration, scaffolds must possess sufficient load-bearing capacity 7 to meet functional requirements. The demineralized dentin matrix, the demineralized primary component of teeth, can provide a cost-effective and load-bearing biomimetic alternative to synthetic materials, holding increasing potential in hard tissue remodeling. Moreover, its intrinsic bioactivity facilitates cell homing by promoting the recruitment, proliferation, and differentiation of progenitor cells. These attributes have attracted increasing interest in both clinical applications and tissue engineering research.
Recent experimental studies and clinical cases8–11 in oral and maxillofacial surgery have indicated the efficacy of autogenous dentin matrix grafts as viable alternatives to autologous bone grafts for reconstructing craniofacial bone defects. Conversely, the derivative materials and the fundamental mechanisms of dentin matrix in pulp–dentin complex and alveolar bone regeneration remain under investigation. This review systematically analyzes the classification of dentin matrices and their novel applications in pulp-dentin complex and alveolar bone regeneration, offering conceptual frameworks for future research directions.
Sources of Dentin Matrix
The human dentin matrix is predominantly sourced from orthodontically extracted teeth or third molars. Recent advancements have broadened the range of sources to include xenogeneic teeth, specifically caprine, 12 bovine,13,14 and porcine 15 origins, which have shown a comparable ability to facilitate the regeneration of dental hard tissues. Among these sources, porcine-derived dentin matrix 16 is noted for its mineral composition and bioactive molecular characteristics that closely resemble those of human dentin matrix.
Importantly, porcine-derived dentin matrix is characterized by elevated concentrations of immunomodulatory proteins, such as CD44, CD59, and CD58, which may provoke xenogeneic immune responses. Despite this, the osteo/odontogenic potential of porcine-derived dentin matrix remains significant, as evidenced by its continued ability to promote biomineralization in both dentin and cementum. 17
Classification and Preparation of Dentin Matrices
Dentin 18 is a complex mineralized tissue with the following weight-based composition: 70% inorganic content, 20% organic matrix, and 10% water. The mineral phase can be further categorized into two distinct compartments: interfibrillar minerals, which account for 70–75%, and intrafibrillar minerals, which constitute 25–30%. 19 Notably, although intrafibrillar mineralization represents a smaller fraction of the overall mineral content, it plays a critical role in enhancing the mechanical properties and structural integrity.
Collagen fibers’ size-exclusion characteristics, 20 which confine water and small solutes to interfibrillar spaces, 21 have prompted several research teams to explore targeted extrafibrillar demineralization. However, these efforts have limited efficacy.22,23
Currently, despite variations in dentin demineralization methods and subsequent treatment approaches across different studies, the demineralized dentin matrix is generally referred to as treated dentin matrix (TDM),2,24 demineralized dentin matrix (DDM),8,24,25 or auto-tooth bone (ATB).26,27 Notably, ATB 26 specifically denotes a subclass derived from autologous teeth, prepared via basic alcohol cleanser disinfection and short-duration demineralization with 10% EDTA. TDM, by contrast, generally refers to partially demineralized dentin with additional processing (e.g., sterilization). 28 Despite these subtle preparation differences, these terms (TDM, DDM, and ATB) are frequently used interchangeably in current research, lacking clear and standardized definitions and boundaries. To ensure clarity, this review collectively designates all demineralized dentin-based scaffolds as “DDM”.
This review proposes a classification framework predicated on the degree of demineralization: partially demineralized dentin matrix (pDDM) and completely demineralized dentin matrix (cDDM), with variations in protocols designed to suit clinical applications (Fig. 1, Table 1).
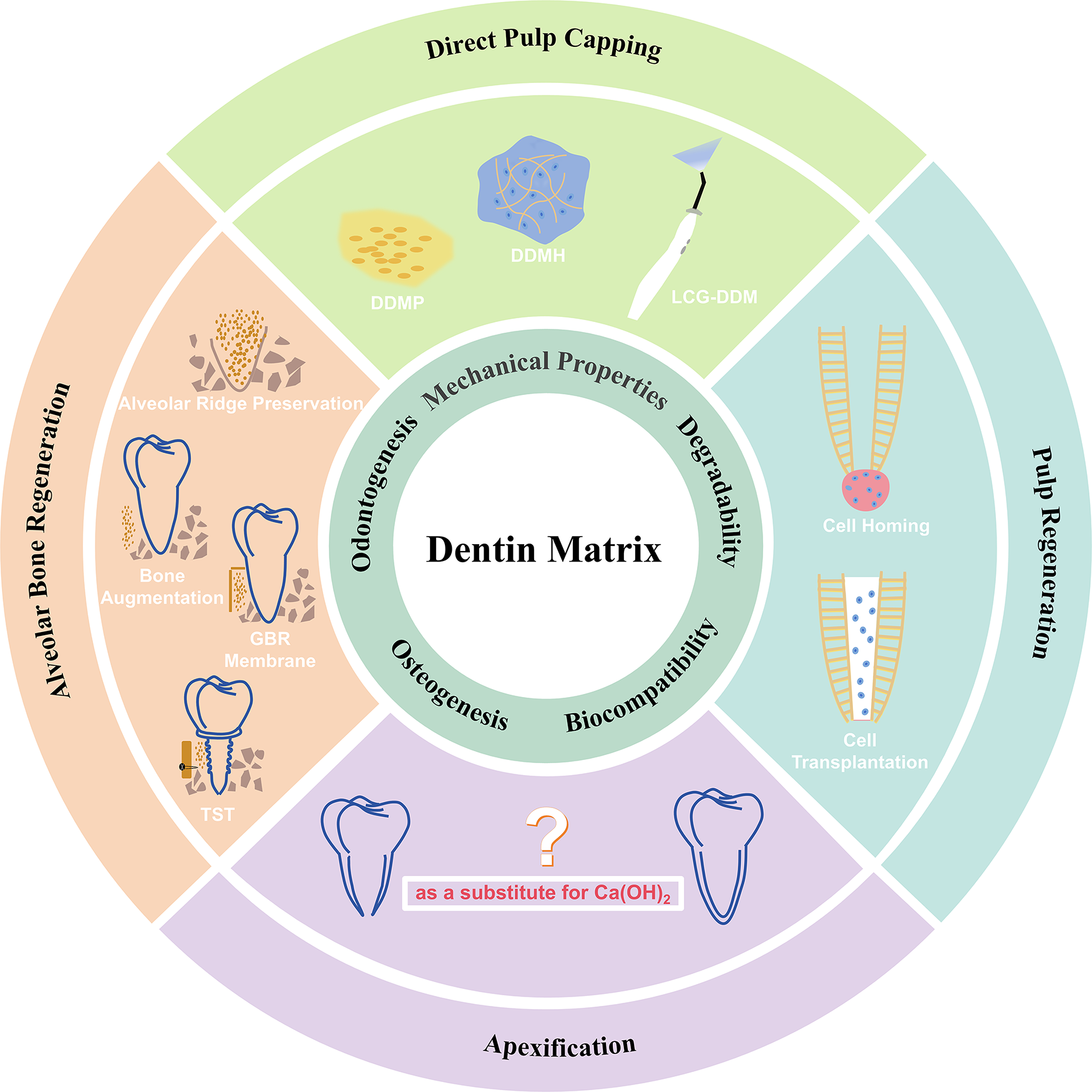
Applications of DDM. The key application directions of DDM in endodontics and alveolar bone regeneration. DDMP, demineralized dentin matrix paste. DDMH, demineralized dentin matrix hydrogel. LCG-DDM, gelatin-demineralized dentin matrix light-cured hydrogel. GBR, guided bone regeneration; TSH, tooth shell technique.
Different Demineralizing Agents and Times for DDM
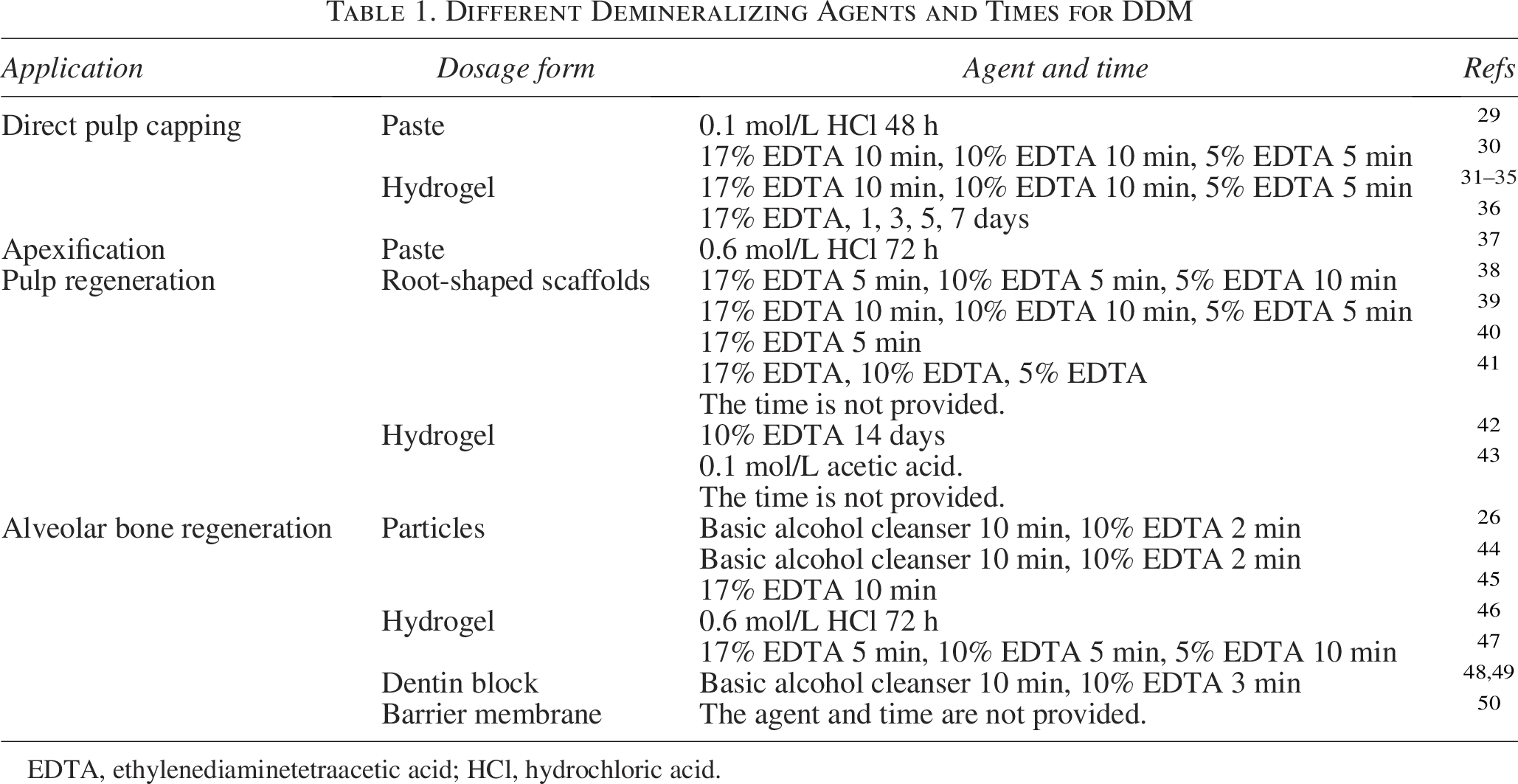
EDTA, ethylenediaminetetraacetic acid; HCl, hydrochloric acid.
The preparation of DDM initiates with extracted teeth undergoing sequential processing steps.26,29,38,51 The protocol involves crown removal using a high-speed handpiece, thorough curettage of periodontal tissues (including periodontal ligament, cementum, and superficial dentin), and complete elimination of pulp tissue and predentin with nickel-titanium files, followed by ultrasonic cleaning and demineralization. The resulting matrix is then engineered into various forms (Fig. 2).
Sources, preparation, and application forms of DDM. DDM is derived from human (autogenous, allogenic) or animal (xenogenic) teeth. The process begins with the removal of the crown, periodontal ligament (PDL), and cementum to obtain purified dentin. The dentin is then treated with demineralizing agent. Depending on the clinical application, the processed matrix can be fabricated into diverse forms, including root-shaped scaffolds, paste, hydrogel, particles, barrier membranes for guided bone regeneration (GBR) and dentin block for tooth shell technique.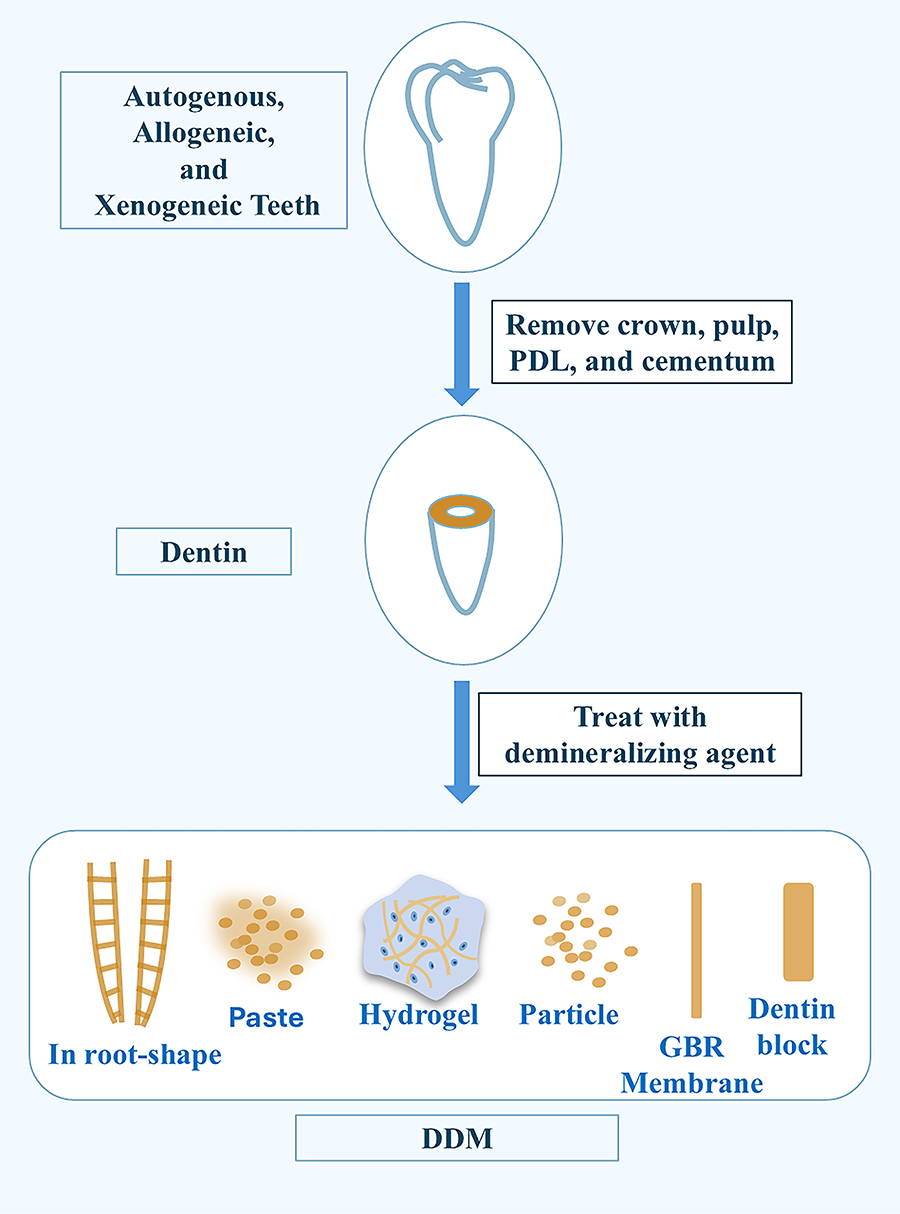
Two distinct processing methods yield different matrix types:
Partially demineralized dentin matrix (pDDM):26,38,51 Produced through graded EDTA or weak acid treatment (varying concentrations and durations) of either ground or intact dentin. Completely demineralized dentin matrix (cDDM):
29
Obtained via complete demineralization of dentin in hydrochloric acid solution.
Comparative evaluations 52 show fundamental differences between these matrices. pDDM exhibits preferable preservation of native growth factors and maintains the original architecture of dentinal tubules, creating an interconnected porous network that supports prolonged therapeutic release. In contrast, cDDM 29 shows more rapid degradation while surprisingly preserving bioactive components. These findings suggest that pDDM is more suitable for applications requiring sustained release, while cDDM may be better for situations necessitating rapid tissue turnover. Moving forward, efforts should prioritize the development of standardized metrics (e.g., demineralization extent, porosity) to enable more granular classification of DDM.
Properties of Dentin Matrix
Degradability and mechanical properties
cDDM exhibits rapid degradation kinetics, necessitating its combination with other materials to achieve optimal sealing efficacy. In contrast, pDDM indicates significantly slower degradation rates. Even when integrated into sodium alginate (SA) hydrogel53,54—a material recognized for its high degradability—to create pDDM hydrogel (pDDMH), 31 the degradation profile aligns with the natural formation rate of dental hard tissues. This phenomenon is likely attributable to dual mechanisms: 55 calcium ion-mediated crosslinking with SA polymers and the restricted chain mobility imposed by pDDM particles. Other formulations of pDDM, such as paste preparations, exhibit even more prolonged degradation, thereby providing sustained sealing capacity.
Importantly, pDDM maintains elastic modulus within the physiological range of natural hard tissues (34–40 kPa), 56 demonstrating compatibility with both dental and periodontal hard tissues, and thereby confirming its capacity to replicate the mechanical microenvironment of natural tooth hard tissues.
Immunogenicity and antigenicity
In various experiments, a range of sterilization techniques—such as freeze-drying, 29 autoclaving, 12 and chemical disinfection 57 —are routinely employed to inactivate potential microbial contaminants in DDM, thereby mitigating immunological risks while preserving its biological activity. However, the specific effects of these sterilization protocols on DDM’s immunological properties remain insufficiently investigated.
Both autogenous pDDM and cDDM 28 encompass a range of immunomodulatory molecules, notably transforming growth factor-β1 (TGF-β1), 58 which exerts anti-inflammatory effects through nuclear factor-kappa B (NF-κB) pathway suppression and IL-10 synergy, as well as osteopontin (OPN), which not only regulates mineralization but also recruits and activates immune cells (e.g., neutrophils) during inflammatory responses. Allogeneic pDDM and cDDM 12 have demonstrated efficacy in facilitating the regeneration of bone and dental tissues while minimizing significant inflammatory responses from the host. Xenogeneic pDDM and cDDM 15 can provoke mild to moderate inflammatory reactions. However, these responses tend to diminish over time, ultimately fostering a conducive microenvironment for enhanced tissue healing and regeneration.
These experimental findings directly confirm that DDM exhibits low immunogenicity. Furthermore, mechanistic studies have demonstrated that, beyond an initial inflammatory response, neither immune rejection nor foreign body reactions are observed with allogeneic or xenogeneic DDM.59,60 At the tissue level, DDM also displays nonimmunogenic or low antigenic properties, thereby providing further evidence that it can create a favorable microenvironment for tissue regeneration.
Odontogenic and osteogenic differentiation potential
pDDM and cDDM release multiple signaling factors, 61 including stromal cell-derived factor-1 (SDF-1), platelet-derived growth factor (PDGF), fibroblast growth factor (FGF), TGF, dentin matrix protein (DMP), dentin sialoprotein (DSP), and dentin sialophosphoprotein (DSPP). 62 These factors collectively regulate stem cell migration and differentiation, promoting the regeneration of both the pulp-dentin complex and bone tissue.63–65 These bioactive molecules facilitate tissue regeneration through two primary mechanisms (Fig. 3): (1) Activation of bioactive signaling pathways. For example, TGF-β1, DSPP, and DMP1 collectively regulate TGF-β/BMP 66 and Wnt/β-catenin pathways 24 to activate the differentiation of dental pulp stem cells (DPSCs) into functional odontoblasts. DSP promotes endothelial differentiation of DPSCs through DSPaa34-50-endoglin-AKT1 axis. 67 Moreover, FGF promotes the odontogenic and angiogenic differentiation of SCAP through the MEK/ERK, TAK1, and p38 signaling pathways. 68 (2) Direct regulation of mineralization, mediated by small integrin-binding ligand N-linked glycoproteins. For example, DMP1 is responsible for initiating and accelerating mineralization. DSP finely regulates the process of mineralization. OPN prevents excessive mineralization and ensures quality. 69
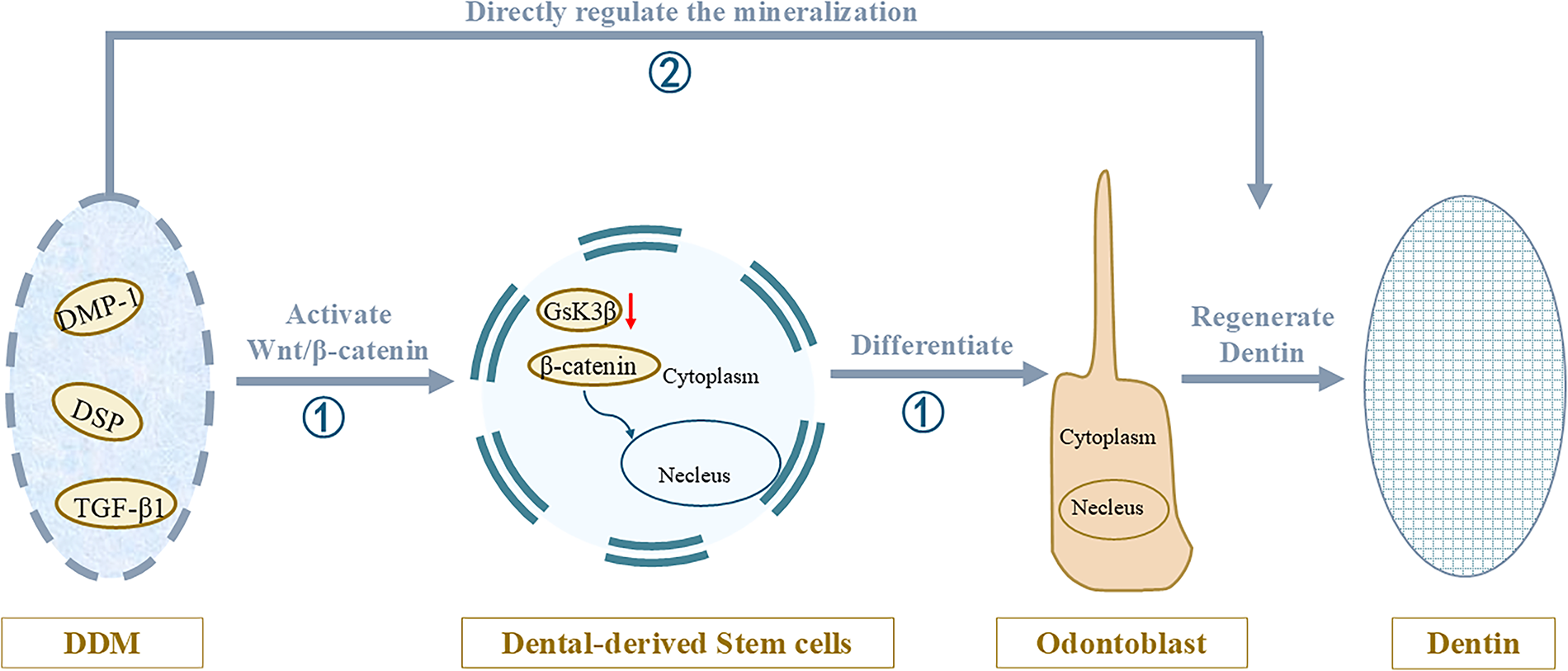
Two primary mechanisms of dentin regeneration.
Stability
As a bioactive scaffold, maintaining ECM viability presents a significant challenge. In 2014, Jiao et al. 70 revealed that cryopreserved pDDM in liquid nitrogen maintained mechanical integrity and dentin-derived protein release capacity for 6 months, confirming its clinical storage stability.
Clinical Applications
Direct pulp capping
Direct pulp capping (DPC) represents a conservative restorative procedure designed to preserve pulp vitality through dentin bridge formation following minor mechanical or traumatic pulp exposure.
Historically, calcium hydroxide [Ca(OH)2], 71 the most widely used capping material with a strongly alkaline pH (−12.5), frequently induced direct necrosis of adjacent pulp cells. The resulting reparative dentin bridge typically exhibits nonphysiological osteodentin lacking dentinal tubules. Discontinuities during dentin bridge formation often result in the development of tunnel defects. While mineral trioxide aggregate (MTA) 72 shows an improvement over pulp preservation outcomes, its clinical utility remains limited by cytotoxic aluminum ions and bismuth-induced tooth discoloration. Consequently, bioceramic materials 73 such as nRoot and iRoot BP Plus have gained prominence due to their enhanced biocompatibility and antimicrobial properties, demonstrating excellent clinical performance. However, these synthetic materials lack the bioactive signaling molecules required for DPSC homing and differentiation, potentially leading to excessive root canal calcification without achieving true dentin regeneration.
In 2011, Guo et al. 51 achieved complete regeneration of human dentin tissue with physiological tubule structure by implanting human dental follicle cells (DFCs) seeded on gradient-deminerized DDM scaffolds into murine subcutaneous models. This breakthrough prompted subsequent research to develop novel pulp capping agents based on this principle for vital pulp therapy in pulpotomy and reversible pulpitis cases.
Further clinical translation efforts in 2017 30 yielded DDM paste (DDMP), formulated by combining DDM powder with DDM extracts. When applied in DPC procedures on porcine pulp exposure models, DDMP induced the formation of thick, homogeneous dentin bridges without tunnel defects or significant vascular dilation, confirming preferable histocompatibility and regenerative potential.
However, DDMP presents two critical limitations: (1) a tendency to collapse into pulp tissue with consequent reduction of chamber height, and (2) suboptimal plasticity compromising handling properties. These findings drove the development of advanced formulations with improved physical characteristics.
In 2021, Holiel et al. 32 first developed DDM hydrogel (DDMH) using alginate hydrogel as the matrix phase. Their in vivo DPC experiments on orthodontically indicated teeth awaiting extraction demonstrated complete regeneration of the dentin-pulp complex. Histological analyses exhibited the presence of thicker, uniformly tubular dentin with a well-organized palisading layer of odontoblast-like cells. Subsequent research 31 in 2023 by the same group revealed that DDMH is biodegradable, exhibiting a degradation rate that aligns precisely with the rate of new dentin formation, thereby providing optimal space for postoperative repair of dentin defects. Further comparative studies by Sultan et al. 36 in 2025 showed that DDMH exhibits preferable antibacterial properties compared to MTA, significantly enhancing pulp preservation efficacy.
The swelling properties of hydrogels functionally address the poor moldability of DDMP. Meanwhile, with the growing application of photopolymerizable materials in tissue engineering, Sedek et al. 33 (2023) developed a novel gelatin-demineralized dentin matrix light-cured hydrogel (LCG-DDM) incorporating a photoinitiation system. Glycidyl methacrylate (GMA) serves as a key component, with higher GMA content resulting in enhanced hydrogel stability, slower degradation rates, and minimal weight loss, thereby partially overcoming the challenges associated with controlling DDMP degradation. Building upon this innovation, Cheng et al. 35 (2024) subsequently engineered gelatin modified by methacrylic anhydride (Gel-MA)/DDM scaffolds with optimized porosity, mechanical strength, and biological performance, enabling maximally efficient proliferation and differentiation of DPSCs. In subsequent in vivo studies using 64 canine teeth as experimental samples, Sedek et al. 34 verified that, compared with the positive control group (MTA), LCG-DDM could effectively promote the formation of a thicker (≥0.25 mm), more continuous, and more regularly arranged dentin bridge. This difference was statistically significant (p ≤ 0.05).
As evidenced by the aforementioned studies, pDDM-derived materials have presented better outcomes in pulp capping applications. In contrast, cDDM has been less extensively investigated for this purpose due to inherent limitations, including suboptimal mechanical properties and rapid dissolution kinetics.
Nevertheless, certain cDDM-based materials have achieved clinical success. Although cDDM lacks the dentinal tubule architecture necessary for the sustained release of therapeutic agents (e.g., drugs, proteins, or cells), it retains bioactive factors capable of promoting dentin regeneration. Notably, dental pulp mesenchymal stem cells exhibit enhanced adhesion and spreading on cDDM scaffolds prepared through a 6-hour demineralization process in 0.6 mol/L hydrochloric acid. 74 In 2023, Li et al. 29 developed pepsin-digested dentin matrix under acidic conditions and applied it and iRoot BP for pulp capping in rat maxillary first premolars. This combination resulted in significantly thicker dentin layers compared with the use of iRoot BP alone. However, the rapid degradation profile of the material presents a clinical dilemma: while it facilitates space for regenerative processes, it simultaneously increases the risk of microleakage. Therefore, when employing cDDM for pulp capping, it is essential to incorporate composite formulations with other biomaterials.
Apexification
Pulp necrosis in immature permanent teeth often leads to shortened roots, incomplete apical closure, and compromised dentin formation. These morphological defects may cause tooth discoloration, root resorption, pathological fractures, or eventual tooth loss.
Calcium hydroxide 75 continues to be the most widely used agent for apexification in immature permanent teeth, promoting continued root development. However, its limitations, including poor obturation quality, material resorption, and the necessity for frequent replacement, often lead to inadequate control of periapical inflammation, ultimately compromising optimal apical repair and barrier formation. These shortcomings have driven the development of novel apexification materials.
The 2003 study by Jiang et al. 37 was the first to investigate freeze-dried cDDM reconstituted with saline as an apexification material in immature permanent teeth. The study described preferable treatment success rates compared to calcium hydroxide after a 2-year follow-up.
While these findings suggested cDDM’s potential as an alternative inducer, critical parameters—including degradation kinetics, hydrophilicity/hydrophobicity, and retrievability—were not systematically investigated. Furthermore, the relatively short follow-up period precluded definitive conclusions regarding long-term complications. Most importantly, the absence of histological validation, which is considered the gold standard for healing assessment, limits definitive conclusions about cDDM’s capacity to replace calcium hydroxide.
Therefore, cDDM as a substitute for calcium hydroxide in apexification requires more rigorous investigation.
Pulp regeneration
Revascularization has been established as an alternative to traditional apexification procedures for immature teeth with pulp necrosis, largely attributed to its favorable therapeutic outcomes and more efficient treatment course in clinical practice. The protocol expects to induce apical tissue bleeding to form an intraradicular blood clot, which serves as a natural scaffold to support the proliferation and differentiation of stem cells, facilitating increased root length and thickness. However, this approach does not achieve true pulp regeneration.
Two principal strategies have emerged in pulp regeneration: cell transplantation and cell homing. Cell transplantation 76 involves the implantation of exogenous stem cells into the host to reconstruct damaged tissues. In contrast, the cell homing strategy77,78 relies on endogenous stem cell recruitment through precisely orchestrated chemotactic cues.
Cell homing
According to research, the signaling molecules that regulate the migration and differentiation of stem cells to promote the regeneration of the pulp-dentin complex 62 include SDF-1, PDGF, FGF, TGF, and vascular endothelial growth factor (VEGF), among others. These factors can be primarily released from the DDM.
In 2011, Zhang et al. 79 conducted an in vitro angiogenesis assay and discovered that a low concentration of dentin matrix components (0.01 mg/mL) was comparable to VEGF (2 ng/mL) in promoting angiogenesis. They suggested that this effect might be attributed to the synergistic action of multiple growth factors in the dentin matrix, rather than a single growth factor. This finding also provides new insights for future pulp regeneration research. In 2018, Widbiller et al. 80 introduced a collagen gel containing DPSCs at the root apex to simulate an in vivo condition and found that a fibrous scaffold containing dentin matrix proteins, when filled into the root canal, could further promote cell migration and the formation of pulp-like tissues.
While demonstrating significant therapeutic potential, cell homing presents limitations including suboptimal recruitment efficiency, considerable interpatient variability, and complex growth factor modulation. Future investigations should prioritize: (1) precise spatiotemporal control over the release of chemotactic factors from dentin matrices, and (2) development of dentin matrix-derived products with enhanced handling properties.
Meanwhile, animal studies employing cell transplantation strategies have shown at a histological level the remarkable capacity of DDM scaffolds to regenerate pulp-dentin tissues, paving the way for their initial application in clinical studies. 40
Cell transplantation
If chemotactic biological cues are the key factors for cell homing, then one of the critical materials for cell transplantation is the scaffold, 81 such as blood clots, autologous platelet concentrates, 82 including platelet-rich plasma, platelet-rich fibrin, and concentrated growth factors, as well as various types of biomaterials. In many revascularization cases, 83 the application of blood clots and autologous platelet concentrates has achieved satisfactory therapeutic effects. However, they lack some characteristics of ideal scaffolds, including good mechanical properties, controllable biodegradability, and growth factor release. Therefore, biomaterials have gradually emerged in the field of tissue engineering. As early as 2012, Yang et al. 38 embedded DFCs in a scaffold structure made of DDM in vitro and successfully observed dentin-pulp-like tissues on the DDM, including dentinal tubules, predentin, odontoblast-like structures, collagen fibers, and blood vessels. Immunohistochemical results showed that these tissues were positive for DSP, collagen type I (COL I) of pulp connective tissue, and neural markers (βIII-tubulin), indicating the formation of functional pulp tissues with nerves and blood vessels.
In 2015, Chen et al. 39 and in 2020, Meng et al. 84 constructed an anatomically shaped DDM scaffold incorporating different forms of DFCs, successfully verifying dentin-pulp complex regeneration. In 2021, Guo et al. 40 achieved functional tooth regeneration through DDM scaffolds constructed by demineralizing the roots of avulsed teeth, seeded with DPSC aggregates. In 2023, Huang et al. 41 fabricated a 3D-printed DDM/poly(ε-caprolactone) scaffold in root shape. After combining with DFCs and implanting into beagle dog mandibles, the construct demonstrated the regeneration capacity of dentin-like structures, functional vascular networks, and organized fibrous tissues. However, these experimental approaches utilizing DFCs or DPSCs transplantation primarily aim to achieve root regeneration. To enable more precise clinical application in pulp regeneration, researchers have shifted attention toward hydrogel-form dentin matrices tailored for the unique anatomical environment of root canal systems.
In 2024, Gould et al. 42 created a chitosan/SA hydrogel with an optimal pore size of approximately 96 µm loaded with bovine DDM. In 2025, Osman et al. 43 developed an injectable DDM-chitosan gel with different porosities. They found that the hydrogel presented excellent cell recruitment, odontogenic differentiation, biocompatibility, and controlled degradation in vitro, making it suitable for pulp–dentin complex regeneration. Nevertheless, both studies are confined to in vitro models and lack assessment of angiogenic potential.
Consequently, the clinical translation of dentin matrix-based strategies for pulp regeneration remains a significant challenge, primarily due to variations in dosage forms and material application protocols. Future investigations should therefore focus on two key aspects: determining the optimal porosity of DDM-based materials and assessing their ability to promote vascularization in vivo. Furthermore, while DDM naturally contains abundant growth factors, there are currently no experiments evaluating its signaling gradients, nor has the development of novel materials with sustained growth factor release capabilities been achieved. Thus, future efforts should also be dedicated to fabricating new DDM-based materials integrated with a sustained-release system.
Alveolar bone regeneration
With the advancement of implant technology, an increasing number of patients with partial or complete edentulism are opting for implant-supported restorations. However, this approach carries elevated risks of peri-implantitis. 85 Consequently, optimizing strategies to preserve compromised teeth and maintain peri-implant bone levels has emerged as a critical clinical priority for periodontitis patients.
Bone graft particulate materials
For teeth with uncertain prognosis or limited retention value after initial periodontal therapy, surgical interventions involving flap surgery and guided bone regeneration (GBR) represent viable clinical options. For teeth with grade III mobility and periapical bone resorption, if the bone defect is excessively large after extraction, alveolar ridge preservation surgery is required to provide appropriate sites for subsequent implant placement.
However, contemporary bone graft particulate materials 86 employed in GBR and alveolar ridge preservation procedures present persistent limitations, including the absence of osteoinductive potential, inherent immunogenic risks, and inadequate mechanical stability. 87
Earlier systematic evaluations by Li P 25 in 2018 and Li Y 86 in 2022 established DDM’s advantages over Bio-Oss, particularly regarding biodegradation kinetics and bone turnover markers. Substantial evidence61,88 shows that dentin matrix delivers advantageous osteoconductive and osteoinductive properties—whether used alone or with signaling molecules. These unique properties have established it as a clinically viable bone graft option.26,44,45,89
In 2022, Kanazirski and colleagues 26 treated a patient with severe peri-implant bone loss affecting approximately two-thirds of the root length at the mandibular left second premolar (tooth #35, FDI Numbering System) using DDM grafts. Further evidence emerged in 2024 when Garg’s research team 44 managed a mesial angular bone defect at the maxillary right first premolar (tooth #14, FDI Numbering System) through a comprehensive protocol involving flap surgery, thorough debridement, and DDM grafting. These two clinical cases, respectively, illustrate that DDM achieves promising results in treating bone defects induced by peri-implantitis and periodontitis. Follow-up examinations revealed newly formed bone with excellent radiographical density and vertical height maintenance.
In 2025, Zhang et al. 45 established an in vitro periodontal bone defect model in mice and performed bone augmentation surgery using DDM. Histological findings further confirmed that DDM can promote the formation of structurally intact and vascularized new bone tissue.
However, granular bone graft materials are prone to dispersion from the implantation site. To address this limitation, Bao et al. 46 combined DDM particles with fibrin glue in 2023, converting the granular bone graft material into a gel-like viscous bone substitute. This modified formulation not only adhered more securely to the surface of bone defects but also presented earlier, faster, and more complete bone healing promotion capabilities, as validated both in cellular experiments and animal models.
To better conform to the anatomical morphology of bone defect sites, Sultan et al. 47 incorporated DDM and hydroxyapatite nanoparticles into SA to develop a DDM-based hydrogel in 2023. In vitro cellular experiments showed that this hydrogel supports the survival and differentiation of bone marrow mesenchymal stem cells while facilitating bone formation.
These findings further confirm its capacity to deliver consistent regenerative outcomes. However, they have not verified whether DDM can promote the regeneration of functional periodontal ligament-cementum complex tissue while facilitating alveolar bone neoformation.
Tooth shell technique
The socket shield technique (SST), first proposed by Hürzeler et al. 90 in 2010, is a dental surgical approach that preserves a piece of root fragment during implant placement to facilitate osseointegration and maintain intact alveolar bone. However, this technique only applies to noninfected roots from endodontically treated or recently traumatized teeth. 91 Its application to periodontally compromised teeth is contraindicated because it poses risks of peri-implantitis and wound dehiscence, which can ultimately lead to implant failure.
Korsch and his team 48 developed the tooth shell technology (TST) using dentin blocks in 2021. TST is a technique used in immediate implant placement, where screw-retained dentin blocks are attached to buccal or lingual bone defects. The space between the implant and dentin blocks is then filled with DDM particles or other bone substitutes. This approach addresses the critical limitation of SST by rebuilding buccolingual bone defects caused by periodontitis or peri-implantitis.
Korsch et al. 49 compared tooth fragments with autogenous bone fragments and found that tooth fragments had better clinical success rates. They also found that even periodontally compromised teeth, after going through processes like demineralization, sterilization, and drying, can achieve comparable bone augmentation outcomes to healthy tooth fragments. 27 These results revealed that TST addresses the critical limitations of SST while enabling the reuse of periodontitis-affected teeth considered beyond repair.
Although this approach appears promising, it lacks histological results to confirm whether the dentin blocks undergo true ossification or simply remain as non-integrated dentin.
GBR membrane
Beyond bone grafting materials, the GBR membrane plays a pivotal role in preventing epithelial cell dominance during GBR. However, conventional GBR membranes 92 primarily function as passive physical barriers, lacking both mechanical stability and osteogenic properties, thereby restricting their efficacy when dealing with complex alveolar bone defects in periodontitis patients.
In 2021, Ku et al. 50 developed a biological barrier membrane (thickness: 300–800 μm) using dentin matrix, which possesses biomimetic properties similar to cortical bone. Histological evaluation at 3 months revealed complete replacement of the membrane by newly formed hard tissue. However, unlike the flexible, soft commercial collagen or polytetrafluoroethylene membranes commonly used in clinical practice, this membrane lacks tensile strength and exhibits inherent brittleness. These characteristics directly compromise its operational feasibility, barrier stability, and postoperative safety.
Future efforts should focus on material modification and optimization of fabrication processes, while clarifying the applicable scenarios for its use either alone or in combination with different bone substitute materials.
Summary and Outlook
Dentin matrix has become a unique biomaterial with broad clinical potential, characterized by its nonimmunogenicity, favorable mechanical properties, and abundance of bioactive factors.
As DPC agents, different dentin matrix formulas have proven to be highly biocompatible and capable of promoting dentin formation across multiple evaluation systems, including murine subcutaneous models, pulp exposure models, histological analyses, and clinical trials. However, the underlying molecular mechanisms remain incompletely understood. For apexification procedures, while one clinical trial reported advantageous outcomes, the lack of histological validation and supporting in vitro studies limits definitive conclusions. In pulp regeneration applications, dentin matrix has shown the capacity to promote pulp-like tissue formation through synergistic growth factor activity, although current evidence derives primarily from in vitro studies focused on root regeneration. Critical knowledge gaps persist regarding cellular recruitment efficiency and clinical translation protocols. In periodontal and peri-implant applications, case reports indicate successful preservation of compromised teeth when using dentin matrix as grafting materials or GBR membranes. Nevertheless, large-scale clinical studies with long-term follow-up are notably absent.
In summary, the dentin matrix represents a favorable class of scaffolds for dental tissue regeneration. Future research should systematically elucidate the impact of processing parameters—such as the choice of demineralizing agent, treatment duration, sterilization method, and nanomodification strategies—on the activity and stability of endogenous bioactive signaling molecules within the dentin matrix. Guided by these principles, the subsequent objective is to engineer a new generation of dentin matrix-based composite scaffolds that exhibit synchronized controlled release profiles and mechanical stability. Such advanced scaffolds are anticipated to meet the diverse requirements of a broad spectrum of clinical applications, ranging from pulp capping and apexification to the regeneration of the pulp–dentin complex and alveolar bone.
Authors’ Contributions
Conceptualization: K.Z. and S.L.; Writing—original draft: K.Z.; Writing—review and editing: Z.B., S.L., and Y.S.; Software: Z.B.; Visualization: Y.Z.; Methodology: Y.L.; Project administration: X.W.; Supervision: X.L. All authors have read and agreed to the published version of the review.
Footnotes
Acknowledgments
The authors would like to thank the Shanxi Province Key Laboratory of Oral Diseases Prevention and New Materials for the facilities provided.
Funding Information
This work is supported by Shanxi Provincial Youth Science Research Project (202403021222230).
Disclosure Statement
The authors declare no conflicts of interest.