
Abstract
Calcium hydroxylapatite (CaHA) has evolved from hard tissue applications to become a prospective bioactive filler for facial rejuvenation, offering both immediate volumization and long-term regenerative benefits. This review synthesizes literature up to 2025 to summarize the material properties, mechanisms of action, and clinical applications of CaHA-based fillers, evaluating their safety and efficacy. CaHA-based fillers provide structural support and stimulate collagen synthesis by activating fibroblasts, leading to sustained improvements in skin quality, volume restoration, and contour enhancement. Clinical evidence confirms the effectiveness of both pure CaHA and composite formulations combining CaHA with hyaluronic acid, which integrate rapid correction with prolonged regeneration. However, risks such as nodule formation, technical challenges, and the absence of reversal agents require consideration. CaHA-based fillers represent a significant advancement in minimally invasive facial rejuvenation by merging mechanical support with biological regeneration. Future research should focus on optimizing particle design, standardizing injection protocols, and developing multifunctional carriers to enhance safety and predictability.
Impact Statement
As a traditional material for bone and dental repair, calcium hydroxylapatite (CaHA) has surprisingly emerged as a bioactive soft-tissue filler for facial rejuvenation. This review clarifies why this inorganic material can stimulate collagen, restore volume, and improve skin quality, bridging its regenerative mechanisms with clinical practice. By summarizing current applications, efficacy evidence, and safety considerations, we aim to enhance professional understanding, promote wider adoption, and inspire further translational research in minimally invasive aesthetic medicine.
Introduction
The growing demand for a youthful appearance has driven the popularity of nonsurgical facial fillers. Facial aging involves volume loss, deterioration of skin texture, and alterations in contour, which are closely linked to fibroblast dysfunction, extracellular matrix (ECM) degradation, and collagen breakdown. 1 Available fillers each have distinct advantages and limitations. Hyaluronic acid (HA)-based fillers offer rapid results and good biocompatibility but are short-lived and lack intrinsic bioactivity. Poly-L-lactic acid (PLLA) and polycaprolactone fillers promote collagen regeneration but act more slowly and require advanced technique. Permanent fillers is used cautiously due to long-term risks.2,3 Therefore, developing fillers that provide both immediate volume and long-term regeneration while maintaining a favorable safety profile has become a key research focus.
In recent years, CaHA has emerged as a bioactive material with dual effects in soft tissue augmentation. Although numerous studies have demonstrated the clinical efficacy and safety of CaHA fillers, most existing reviews focus either on clinical outcomes or on general material characteristics, without clearly linking material properties to injection techniques and biological responses. As a result, the mechanisms underlying the unique clinical performance of CaHA remain insufficiently integrated.
The aim of this review is to provide a comprehensive overview of CaHA-based fillers by correlating their material properties with biological mechanisms, clinical techniques, and treatment outcomes. By integrating evidence from material science, experimental studies, and clinical practice, this review seeks to clarify the regenerative potential of CaHA, highlight practical considerations for its safe use, and identify current challenges and future research directions in facial rejuvenation.
Evolution of CaHA for Aesthetic Applications and Material Properties
CaHA, with the chemical formula Ca10(PO4)6(OH)2, is the primary inorganic component of human bone and teeth. It exhibits excellent biocompatibility, bioactivity, and degradability.4,5 Initially used in bone repair and dental engineering, CaHA has more recently been adapted for soft tissue augmentation. In aesthetic medicine, the term “CaHA” specifically refers to materials designed for soft tissue filling, distinguishing them from orthopedic applications.
Transition to soft tissue applications
In 2002, CaHA-based fillers received Food and Drug Administration (FDA) approval for vocal cord repair and urinary incontinence treatment.6–8 As evidence of their safety and efficacy in soft tissues accumulated, along with their recognized ability to stimulate collagen regeneration, 9 CaHA fillers were further developed. Since 2006, FDA-approved CaHA fillers have been indicated for correcting moderate-to-severe facial wrinkles and folds, as well as for treating HIV-associated facial lipoatrophy (FDA PMA P050052; P050037). 10
Material modifications for aesthetic use
Traditional orthopedic CaHA (hydroxyapatite, HAP) features larger particle sizes and high crystallinity due to sintering, resulting in a dense, low-degradability structure suitable for long-term bone support. 11 For soft tissue applications, however, materials must be biocompatible, injectable, and degradable. Key modifications include size control, morphology regulation, carrier optimization, and crystallinity adjustment. Particle size is precisely controlled to 20–45 μm, avoiding phagocytosis by macrophages or migration through capillary walls, while allowing injection through a 27G or smaller needle.12,13 Optimized synthesis produces smooth, regularly shaped microspheres that minimize mechanical irritation, reducing the risk of chronic inflammation and foreign body granulomas. 13 CaHA microspheres (approximately 30% by volume) are suspended in biocompatible, biodegradable gels such as sodium carboxymethylcellulose. This carrier provides immediate volume and facilitates smooth injection—extrusion through a 27G needle requires about 5 N of force, within a comfortable clinical range.14,15 The carrier degrades within 2–4 months, creating space for newly formed collagen.12,16 Different commercial formulations (e.g., Radiesse® and Rennova® Diamond Intense) exhibit variations in material properties to meet diverse clinical needs. 17 Unlike high-crystallinity HAP used in orthopedics, aesthetic CaHA features reduced crystallinity achieved via nonsintered synthesis. This balances degradability and structural stability, ensuring microspheres persist long enough (12–24 months) to drive neocollagenesis without inducing chronic inflammation.12,18
Rheological properties of CaHA-based injectable systems
As a key performance indicator following material modifications, the rheological properties of CaHA injectable systems—comprising CaHA microspheres suspended in a CMC gel—directly influence clinical handling and treatment outcomes. The main parameters are described below.
Viscosity (η*) reflects the filler’s resistance to shear flow and is crucial for achieving precise aesthetic correction. Measurements show that undiluted CaHA filler has a complex viscosity of 349,830 cPa (0.7 Hz), which is notably higher than that of most cross-linked HA fillers.15,19 This high viscosity ensures excellent stability at the injection site, with minimal diffusion into surrounding tissues, making CaHA ideal for precise contouring in areas such as the midface and chin. 20 When treating regions with thin or delicate skin, dilution with saline or lidocaine can adjust viscosity—for example, mixing with 0.3% lidocaine reduces it to 116,113 cPa, while a 1:2 dilution enhances spreadability.19–21 Such adaptability makes the filler suitable for neck rejuvenation and fine wrinkle correction, avoiding visible lumps or surface irregularities.20,22
Elastic modulus (G′) indicates the filler’s resistance to deformation and correlates with its ability to provide lift and maintain contour. Undiluted CaHA exhibits a G′ of 1407 Pa (0.7 Hz), substantially higher than that of HA fillers. 19 The high G′ of the CaHA-based filler provides superior lifting capacity, enabling effective correction of moderate-to-severe wrinkles and folds, as well as durable sculpting in deep tissue augmentation. 20 Adjusting dilution allows modulation of G′ to suit different clinical goals: Low-dilution formulations (e.g., 1:0.25, G′ = 113.2 Pa) are optimal for ligament lifting and bony contour enhancement, whereas higher dilutions (e.g., 1:3, G′ = 0.119 Pa) favor superficial skin quality improvement.23,24
Structural recoverability, where viscosity decreases under injection shear and recovers afterward, is a key feature that enhances clinical handling and functional adaptability. 19 The dissipation factor (tan δ) further distinguishes functional states: undiluted or low-dilution CaHA (tan δ < 1) behaves as an elastic material suitable for immediate volumization and contour correction.23,25 At dilutions of ≥1:0.5 (tan δ > 1), the system shifts toward viscous-fluid behavior, promoting biostimulatory activity for skin rejuvenation, scar improvement, and cellulite reduction.20,26 This tunable functionality allows CaHA fillers to address both immediate volume restoration and long-term skin-quality enhancement, broadening their aesthetic applications.
Mechanisms of Action
CaHA-based fillers operate through a combination of physical support and biological regeneration, encompassing three interrelated phases (Fig. 1).
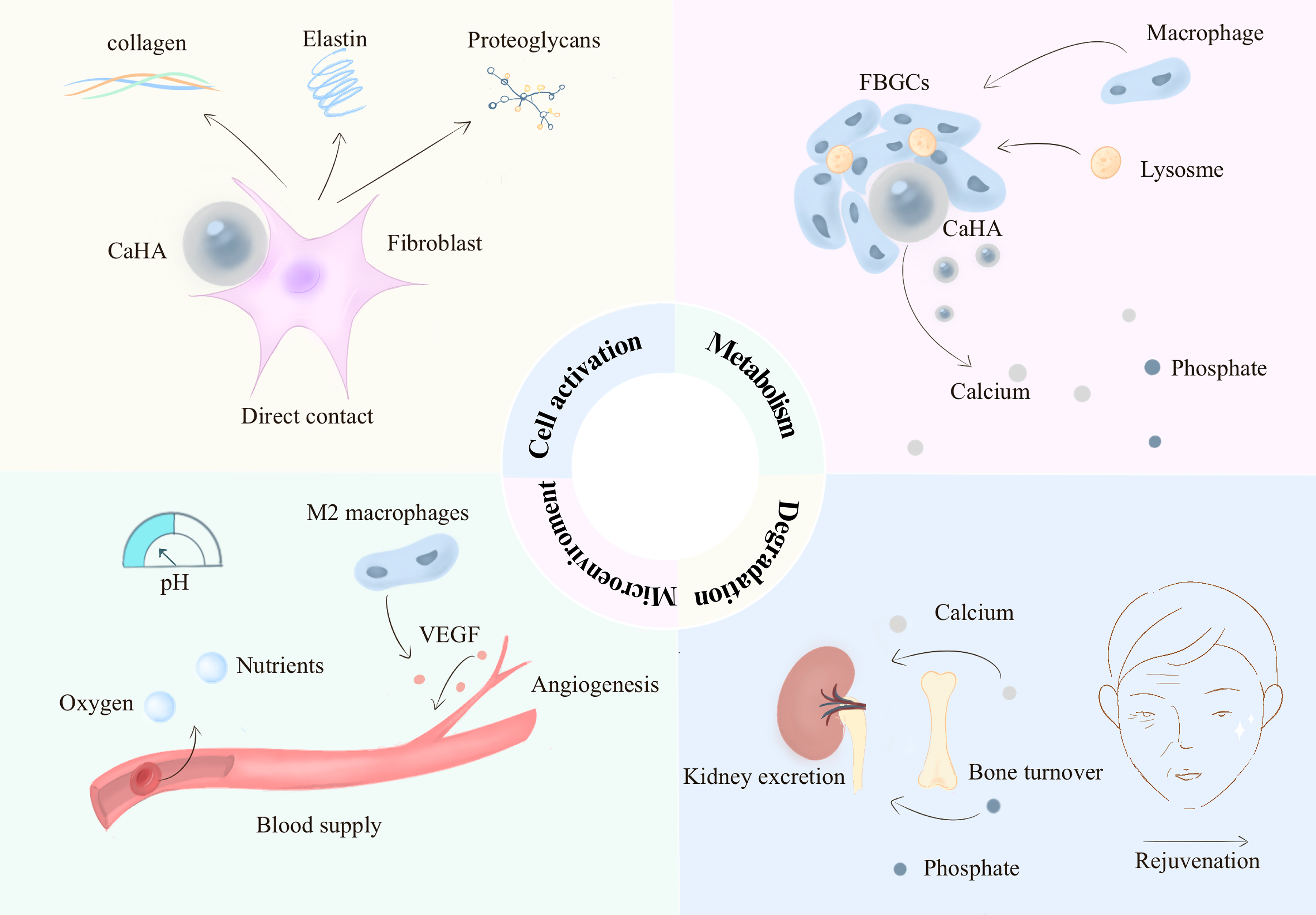
Biological mechanisms of action of calcium hydroxylapatite (CaHA)-based fillers in facial rejuvenation. The schematic illustrates four interconnected functional processes underlying the volumizing and regenerative effects of CaHA. Metabolism: Following implantation, CaHA microspheres interact with surrounding tissues and modulate extracellular matrix (ECM) turnover and biomechanical adaptation, contributing to metabolic remodeling of the local dermal environment and sustained tissue restructuring. Cell activation: Direct physical contact between CaHA microspheres and fibroblasts promotes cellular adhesion and proliferation, accompanied by activation of the transforming growth factor–β (TGF-β)/Smad signaling pathway, which upregulates expression of collagen type I and III, elastin, and proteoglycans. Microenvironment: CaHA influences the tissue microenvironment through reorganization of ECM architecture, maintenance of a favorable local pH environment, and polarization of macrophages toward the M2 phenotype, leading to secretion of vascular endothelial growth factor (VEGF) and platelet-derived growth factor (PDGF), enhancement of angiogenesis, and improved nutrient delivery to regenerating tissues. Degradation: Over approximately 12–24 months, CaHA microspheres undergo progressive phagocytosis and enzymatic degradation into calcium and phosphate ions, which subsequently enter normal physiological metabolic pathways or are eliminated, while neocollagenesis gradually replaces the microsphere scaffold to maintain long-term volumizing and rejuvenation effects.
Physical support
Building on the rheological properties described in Section 2.3, the CaHA microspheres and CMC carrier form a stable three-dimensional network upon injection, providing immediate volume restoration to correct tissue depressions.19,21 The structural integrity of this network is ensured by the system’s high G′ and controlled viscosity, which in turn guarantees excellent localized stability and prevents unwanted migration. This makes CaHA fillers particularly suitable for supraperiosteal placement, where they act as a “liquid implant” that resists gravitational descent of overlying soft tissue.27–29
Biological regeneration
After the carrier gel is absorbed, CaHA microspheres stimulate autologous tissue regeneration through sequential processes. Direct physical contact with CaHA promotes fibroblast adhesion and proliferation. 16 This interaction upregulates transforming growth factor-β1 (TGF-β1)/Smad3 signaling, downregulates Smad7, and enhances expression of COL1A1 and COL3A1 genes, leading to synthesis of type I and III collagen, elastin, and proteoglycans.20,30–33 During the first 3 months, microspheres serve as a physical template for fibrin mesh formation; from 4–8 months, gradual degradation aligns with collagen maturation to prevent volume loss.18,34 Furthermore, CaHA promotes reorganization and renewal of ECM components, optimizing collagen fiber alignment and maturation.34–36 Altered mechanical properties of the ECM can further positively influence fibroblast synthetic activity. 37 CaHA also helps maintain a favorable local pH and stimulates M2 macrophages to release vascular endothelial growth factor and platelet-derived growth factor, enhancing angiogenesis and nutrient supply.20,38,39
Degradation and metabolism
CaHA microspheres are degraded by macrophages and lysosomal enzymes over 12–24 months.13,20 The resulting calcium (Ca2+) and phosphate (PO4³−) ions enter normal metabolic pathways or are excreted by the kidneys. 40 Concurrently, newly formed collagen replaces the filler, sustaining rejuvenation effects for up to 24–36 months.12,16,20
Clinical Applications
Injection techniques
Indications and injection plans
Selection of an injection plan depends on the target anatomical layer, material form, and treatment objective. Deep injections are used for volume and structural support, while hyperdiluted injections target collagen stimulation for skin quality improvement. 41 Composite materials facilitate a combined approach. Specific strategies for different facial areas are detailed in Table 1.
Indications and Injections of Calcium Hydroxylapatite-Based Fillers in Facial Rejuvenation
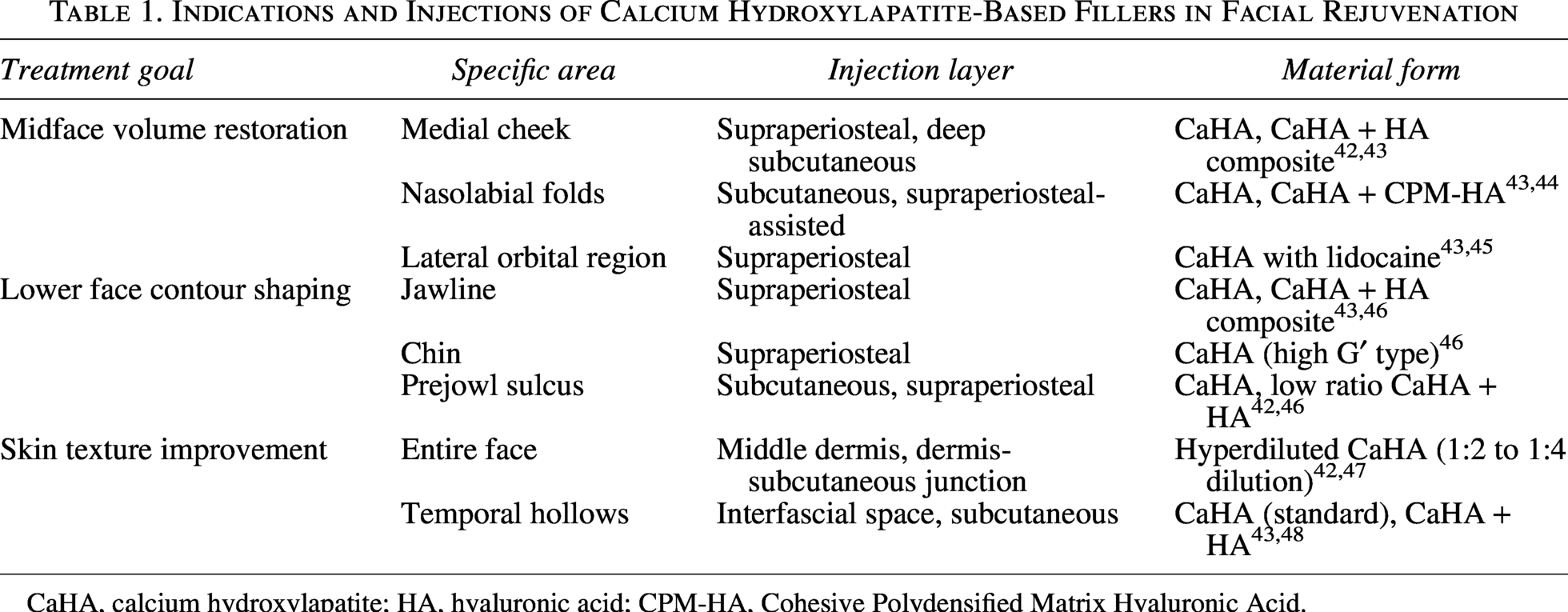
CaHA, calcium hydroxylapatite; HA, hyaluronic acid; CPM-HA, Cohesive Polydensified Matrix Hyaluronic Acid.
Key injection techniques
The appropriate injection technique is selected based on the target anatomical site and treatment goal. Retrograde injection is ideal for long-axis areas such as the jawline and cheeks, typically administering 0.1–0.3 mL per linear segment to ensure uniform distribution.42–44,46 Fan/Star-shaped injection is suited for broad areas such as the cheeks and temples, depositing 0.2–0.5 mL of product per sector with immediate physician massage to optimize spread. 42 Bolus injection is used for correcting localized depressions like the prejowl sulcus, with a small, precise bolus of 0.05–0.1 mL per point to prevent vascular compression and nodule formation.49,50 The Vectorial-Lift technique uses regionalized dilutions to target facial retaining ligaments for a lifting effect. 29 The six-point supraperiosteal injection, optimized for Asian facial anatomy, targets specific points on the eyebrow arch, lateral zygoma, and jawline, with injection of 0.25–0.3 mL per point significantly improving eyebrow lift and jawline definition. 51
Injection depth and safety considerations
Injection depth is critical for safety and outcomes. The high viscosity and particle characteristics of CaHA-based fillers necessitate precise placement within specific tissue planes. Placement in the supraperiosteal plane leverages bony support for product stability and avoids major vessels, reducing vascular injury risk. Deep subcutaneous placement, targeting fat pads, effectively restores volume while minimizing risks of superficial aggregation and visible nodules. 51 For skin texture improvement, hyperdiluted CaHA is injected at the dermis–subcutaneous junction. This requires strict volume control per injection point (typically 0.1–0.2 mL with a cannula), delivered via serial dot or short linear threading techniques. 42
Management of high-risk anatomical areas
Certain facial regions harbor critical neurovascular structures and require heightened caution. In the lateral orbital region, injections should be slow and strictly supraperiosteal, avoiding the zone within 1.5 cm of the lateral canthus where the zygomaticofacial neurovascular bundle is located.42,45,46,47 For the temporal region, the safest target is the interfascial space between the superficial and deep temporal fascia. Using a cannula (e.g., 25G or 23G) significantly reduces vascular penetration risk. A retrospective analysis of 113 patients using a cannula via the inferolateral orbital access point reported zero vascular complications.42,45,52
Dilution, anesthesia, and adverse reaction management
Proper procedural management is essential for patient comfort and safety. A common consensus recommends using 2% lidocaine as a diluent. A typical regimen is 1.5 mL of CaHA-based filler mixed with 0.5–1.5 mL of lidocaine. 42 A randomized, double-blind study confirmed the efficacy and safety of CaHA mixed with lidocaine. For higher dilution ratios, sterile saline can be added. 53 Immediate physician massage ensures even product distribution. Patients are instructed to massage treated areas twice daily for 3–7 days to reduce particle aggregation risk.42,54 Early nodules can often be managed with intranodular injection of lidocaine-saline followed by massage. Persistent nodules may require injection with 5-fluorouracil and triamcinolone over multiple sessions.42,48 McCarthy et al. 55 proposed a structured four-level algorithm for managing CaHA-related nodules, summarized in Table 2. Intraarterial injection can lead to severe outcomes. As CaHA-based fillers lack a specific reversal agent, management is supportive. CaHA is contraindicated in the glabella, and caution is required in the nasal dorsum and tip.42,56
Structured Management Levels for Calcium Hydroxylapatite-Related Nodules

5-FU, 5-Fluorouracil.
Clinical efficacy and evidence summary
The clinical efficacy of CaHA-based fillers has been evaluated using standardized outcome measures, including the Wrinkle Severity Rating Scale (WSRS) and the Global Aesthetic Improvement Scale (GAIS), together with objective assessments such as ultrasound imaging, elastography, and transepidermal water loss (TEWL).
Long-term efficacy and collagen stimulation effects of CaHA
Clinical data support the long-term efficacy and safety of CaHA-based fillers in volume restoration and collagen stimulation. In a comparative study by Durkina et al. involving 17 patients, the proportion rated as “significantly improved” was 100%, 89%, and 89% at 90, 180, and 360 days post-CaHA treatment, significantly higher than an HA control group (50%, 37.5%, and 37.5%). 50 A multicenter trial in 188 Chinese subjects using Aphranel® for nasolabial fold correction showed an 84.04% WSRS improvement rate at 24 weeks, with over half maintaining results at 12 months. 57 For jawline contouring, 62.9% of patients maintained ≥1-point improvement on the Merz Jawline Assessment Scale at 48 weeks, and 43.5% at 60 weeks without retreatment. 58 A retrospective analysis combining superficial enhanced fluid fat injection (SEFFI) with diluted CaHA (1:1) in 158 patients demonstrated progressive volume enhancement in temporal, malar, zygomatic, and jawline regions, with notable retention at 150 days and 80.3% of patients showing “Improved” or better skin quality on GAIS at 90 days. 59 An observational study by Wollina and Goldman 60 in 40 women receiving repeated CaHA injections every 12–14 months reported sustained high GAIS scores over 36 months, with only six subjects experiencing mild bruising or nodules, all resolving within 2–4 weeks, and no severe adverse events. Yutskovskaya et al. 54 observed marked increases in type I/III collagen 4–7 months postinjection. Ultrasound at 3 months after hyperdiluted CaHA treatment in the neck revealed a “coarse snowflake” collagen neogenesis pattern and an 11.1% increase in skin thickness. Combined treatment with fractional CO2 laser or radiofrequency enhanced collagen remodeling and skin tightening compared to CaHA alone.61,62
Synergistic advantages of CaHA + HA composite materials
Composite fillers balance immediate and long-term effects, improving skin texture and patient satisfaction. A retrospective study by Fakih-Gomez and Kadouc 63 in 41 patients using CaHA + CPM-HA composites in the cheeks and jawline showed significant improvements in the Merz Aesthetics Scale for the jawline® (Clinician-Rated Merz Aesthetics Scale for Jawline) at 3 months, maintained at 12 months, with durability surpassing CaHA alone. A prospective study of the hybrid filler HArmonyCa™, a composite injectable combining HA and CaHA, in 15 subjects confirmed immediate volume increase (1.7 cc per side at 48 h) and sustained retention at 180 days (2.1 cc per side, p < 0.0001) using two-dimensional and three-dimensional imaging and ultrasound assessment. 64 A systematic review of 13 studies by Meçani et al. 64 reported a mean satisfaction score of 8.6/10 in the composite group, higher than pure HA (7.2) or CaHA (7.8) groups, with adverse events occurring in only 3.5% of cases, mostly mild edema. Guida and Galadari64,65 documented a 23% increase in skin elasticity and 35% reduction in fine-line scores after treatment, with ultrasound confirming a 48% rise in collagen density. In the HArmonyCa study, elastography and corneometry at 180 days showed a 19.0% reduction in TEWL and a 13.8% increase in skin hydration. 66 A prospective trial (n = 15) reported TEWL reduction from 12.22 to 9.91 g/(m2·h) (p = 0.0039) and a 62% improvement in skin hydration at 24 weeks, indicating enhanced barrier function with the HA-CaHA combination. 67
Comparative advantages of CaHA with other fillers
CaHA-based fillers offer distinct benefits in inflammatory response, structural support, collagen induction, age adaptability, and biodegradability. CaHA does not significantly upregulate proinflammatory cytokines, reducing foreign body reaction risks and supporting natural skin recovery.34,68,69 CaHA-based fillers have high G′ and viscosity, performing better than HA fillers in areas requiring strong structural support, and the addition of lidocaine does not alter their rheological properties.12,21 Unlike PLLA-based fillers, which primarily stimulate type III collagen, CaHA promotes mature collagen formation and shows stronger collagen stimulation than HA-based products, enabling both immediate filling and long-term regeneration. 13 CaHA also offers faster visible results than PLLA, appealing to patients seeking short-term improvement.62,70 By adjusting the dilution ratio, CaHA-based fillers can meet the needs of different age groups. Preventive treatment in the 30–40 age group shows a 95% improvement rate; 80% of the 40–60 age group still shows improvement; for those over 60 years, higher concentrations can achieve 70% skin thickening and wrinkle improvement, activating fibroblasts to promote type I collagen synthesis and effectively reverse collagen degradation. 71 In postmenopausal women (n = 20), 84.9% were rated “Very Much/Much Improved” at 360 days despite hormonal collagen loss. 52 Unlike permanent fillers such as polymethyl methacrylate, CaHA-based fillers are fully biodegradable, with magnetic resonance imaging studies confirming no residual particles at 2.5 years, eliminating long-term foreign body risks.40,72,73
To clarify the clinical position of CaHA-based fillers, the major characteristics of commonly used filler materials are summarized in Table 3.
Comparison of Calcium Hydroxylapatite-Based Fillers with Other Commonly Used Filler Materials
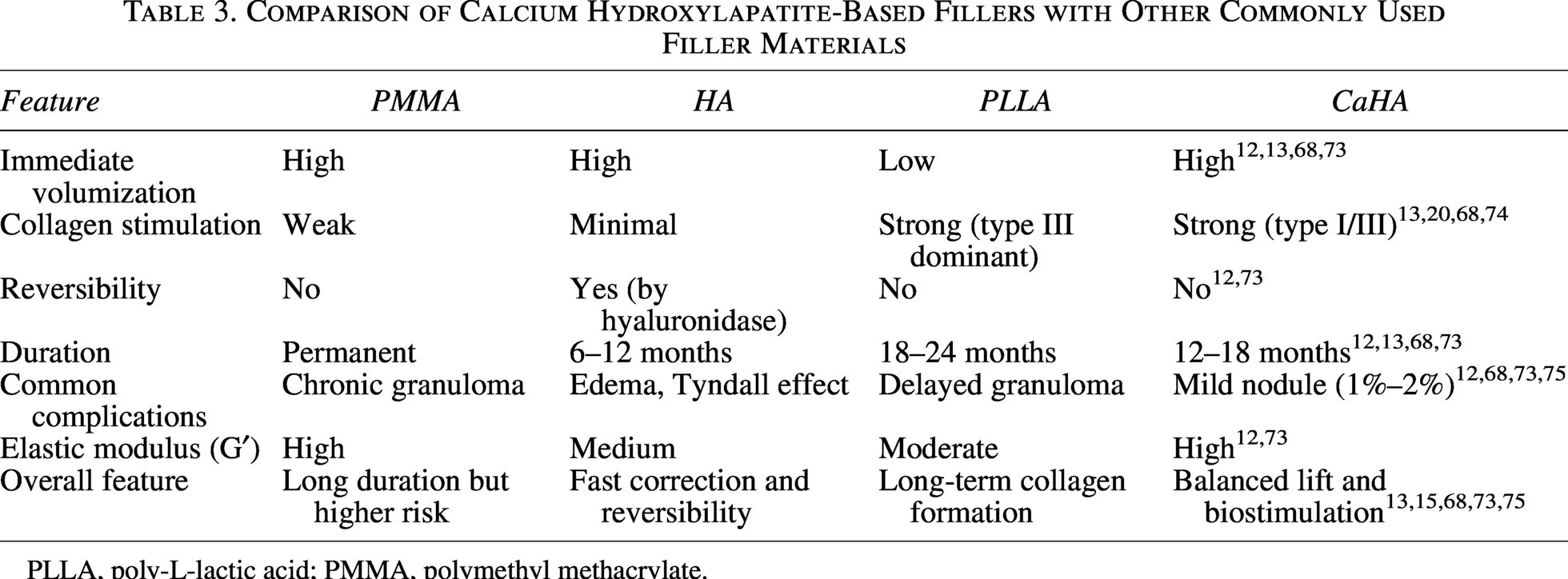
PLLA, poly-L-lactic acid; PMMA, polymethyl methacrylate.
Material and operational risks
Nodule or hard nodule formation
Nodule formation is often related to injection technique and material properties. Shallow injections or excessive volume at a single site can cause particle aggregation and palpable nodules. Nodule risk is higher in thin-skin areas (e.g., periorbital region): A multicenter study of 280 patients reported a 3.2% nodule rate in periorbital injections versus 1.1% in midfacial injections. 45 Irregularly shaped products with fragmented structures are especially prone to trigger local inflammation and nodule development. 75
Long-Term foreign body granulomas
Although uncommon, CaHA injections can occasionally cause chronic granulomatous reactions. Itamura et al. 49 first reported a case in which a 51-year-old woman developed a subcutaneous mass after repeated Radiesse® injections in the parotid region. Pathology confirmed a granuloma surrounded by multinucleated giant cells, indicating that if local inflammation interferes with phagocytic clearance, CaHA particles may persist and induce long-term foreign body responses.
Technical difficulty and risks of irreversibility
The high G′ of CaHA-based fillers requires placement in deep tissue to avoid visible nodules, contour irregularities, or vascular embolism. 76 Once intravascular injection occurs, CaHA cannot be quickly dissolved like HA with hyaluronidase; treatment is limited to vascular dilation, hyperbaric oxygen, and other supportive measures.74,77 This places higher demands on physicians’ anatomical knowledge and technical skill. Additionally, under standardized rheological and extrusion force testing conditions, CaHA-CMC demonstrates significantly higher extrusion forces through 27G needles compared with most HA fillers, which may increase operator fatigue during injection and potentially compromise uniform filler distribution when treating large areas.26,78
Discussion
CaHA-based fillers represent a paradigm shift from physical filling to biological regeneration, yet several key challenges must be addressed to advance the field. First, the balance between bioactivity and safety requires further refinement, necessitating studies to define parameters that promote robust collagen regeneration without provoking excessive tissue response or nodule formation.55,79 Second, the lack of standardized injection protocols and variations between commercial products hinder predictable outcomes; future work must establish universal guidelines for dilution, injection depth, and delivery, potentially aided by imaging tools like ultrasound for enhanced reproducibility.41,80 Third, the synergistic potential of combining CaHA with other modalities such as HA, energy-based devices, or novel hybrid formulations shows promise for enhanced collagen remodeling and skin tightening, though larger controlled trials are needed to confirm long-term safety and efficacy.80,81 Finally, a deeper understanding of the long-term tissue interactions and the management of rare complications, such as granulomas or fibrosis, is crucial, with emerging strategies like immune-modulating therapy offering new avenues for intervention.82,83 Overall, CaHA-based fillers are evolving into sophisticated bioactive platforms, and continued research into their mechanisms, standardized protocols, and strategic combinations will be pivotal for achieving more predictable, personalized, and effective outcomes in facial rejuvenation.
Ethics Statement
The authors have nothing to report.
Consent
The authors have nothing to report.
Authors’ Contributions
Y.H. and J.G. were involved in the conceptualization and planning of the article. Y.H., X.M., and J.G. revised and contributed to the individual sections of the article. All authors approved the final version of the article.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This study was funded by the