
Abstract
Three-dimensional (3D) printing technology, or additive manufacturing, has fundamentally transformed medical paradigms by shifting dentistry from traditional subtractive manufacturing to an era of personalized, biological regeneration. This review provides a comprehensive overview of the primary 3D printing classifications currently utilized, including stereolithography, fused deposition modeling, selective laser sintering, and material jetting, analyzing their specific technical principles and material capabilities. We systematically categorize their applications across diverse dental disciplines, ranging from endodontics, periodontal disease management, and prosthodontics to orthodontics, maxillofacial reconstruction, and temporomandibular joint regeneration. Beyond the fabrication of anatomical models and surgical guides, this article critically evaluates the efficacy of these technologies in constructing bioactive scaffolds and cell-laden hydrogels designed to induce osteogenesis and angiogenesis. Special emphasis is placed on the paradigm shift from passive mechanical restoration to active biological regeneration, highlighting the potential of bioprinting in restoring physiological vitality to native tissues. Despite current barriers regarding the trade-off between mechanical durability and biological activity, as well as vascularization challenges, the convergence of artificial intelligence and 4D printing promises to establish 3D printing as a foundational standard for the next generation of regenerative dental therapeutics.
Impact Statement
The integration of three-dimensional printing into dentistry marks a paradigm shift from inert prosthetic replacement to biological tissue regeneration. This review critically analyzes the current landscape of additive manufacturing, with a specific focus on its application in constructing bioactive scaffolds and tissue-engineered constructs for periodontal and maxillofacial regeneration. By systematizing the capabilities of technologies such as stereolithography, digital light processing, and bioprinting, this article provides tissue engineers and clinicians with a clear roadmap for selecting materials and methods. It highlights the translational potential of bioprinting in overcoming current limitations in oral tissue repair, serving as a vital reference for future research in personalized regenerative medicine.
Keywords
Introduction
Recent advances in digital dentistry have been driven by the rapid development of three-dimensional (3D) printing (additive manufacturing, AM), which enables the fabrication of patient-specific constructs with complex architectures. 1 (Fig. 1). While conventional restorative approaches effectively reinstate mechanical function, they fundamentally fail to regenerate the physiological vitality of native tissues. This limitation has prompted a paradigm shift from passive restoration toward biologically active regeneration.
Previous comprehensive reviews, such as those by Khorsandi et al. 2 and Jeong et al., 3 have extensively cataloged 3D printing materials and their broad clinical applications. However, most studies predominantly regard AM as a fabrication tool for structural replication, with limited emphasis on the underlying biological mechanisms that govern tissue regeneration. In particular, the interactions between printing-induced microarchitectures and cellular responses—such as mechanotransduction, immune modulation, and stem cell differentiation—remain insufficiently synthesized. As a result, the translational value of 3D-printed constructs in regenerative dentistry is often underexplored. In this context, we propose a conceptual shift by redefining 3D-printed constructs as active instructive microenvironments rather than passive physical scaffolds. By precisely controlling internal architecture, surface properties, and material composition, AM platforms can deliver biomechanical and biochemical cues that regulate cell behavior, modulate the immune microenvironment, and ultimately guide tissue regeneration. 4 This perspective integrates engineering design with biological function, bridging the gap between structural fabrication and regenerative outcomes.
Therefore, this review systematically classifies current 3D printing strategies in dentistry based on their underlying principles and biological effects. We focus on how printing parameters—such as pore geometry, surface energy, and build orientation—influence cellular responses and regenerative processes across dental pulp, periodontal tissue, and alveolar bone.5–11 Furthermore, we critically discuss key translational challenges, including mechanical–biological trade-offs, vascularization limitations, and clinical standardization, aiming to provide a mechanistic and clinically relevant framework for next-generation regenerative dentistry. 12 To ensure the transparency and reproducibility of this review, a systematic literature search following PRISMA guidelines and a quantitative bibliometric analysis (2015–2025) were performed. Detailed search strategies, inclusion criteria, and bibliometric visualizations are provided in the Supplementary Data.
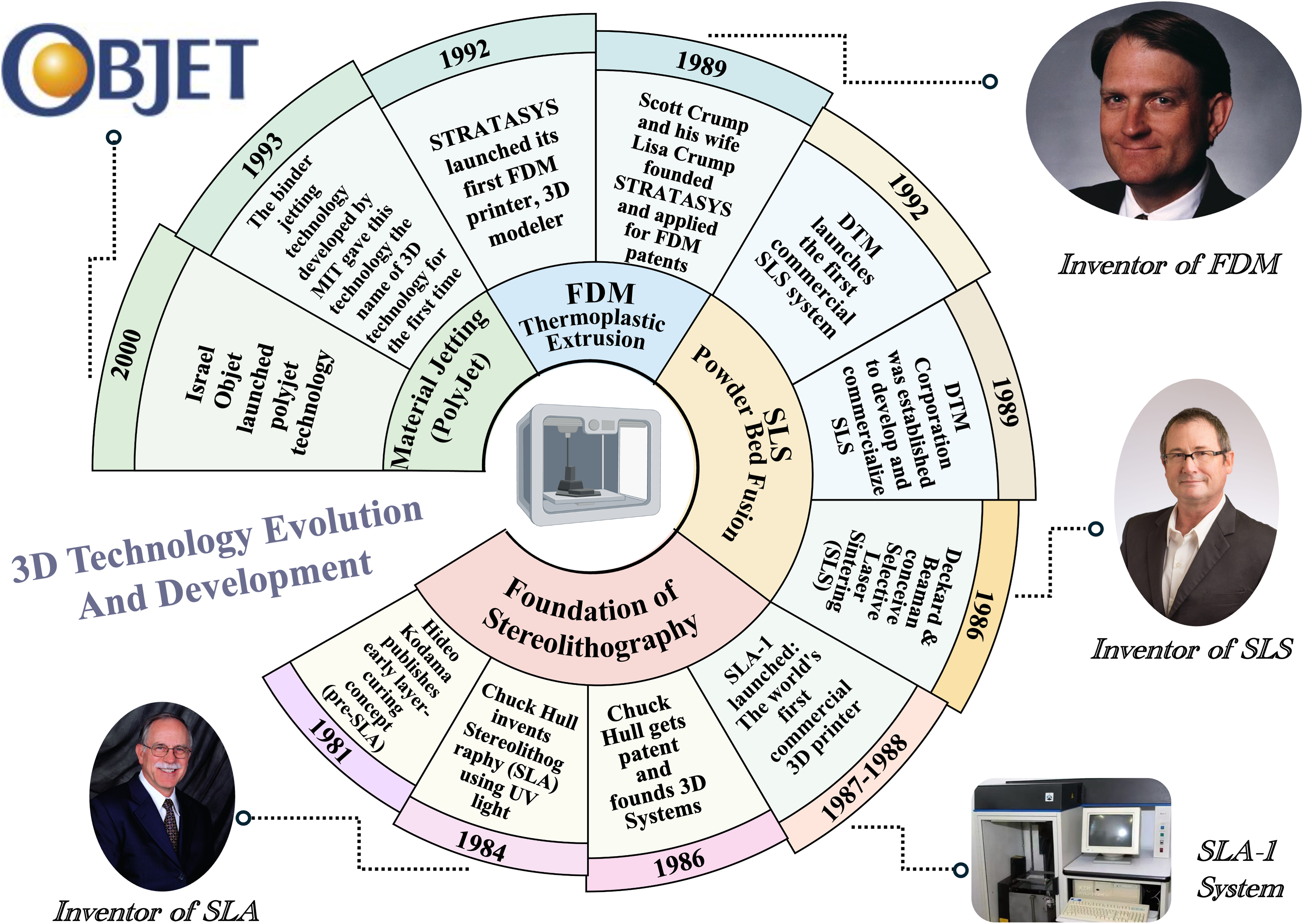
Timeline showing the historical development and key milestones of 3D printing technologies in dentistry.
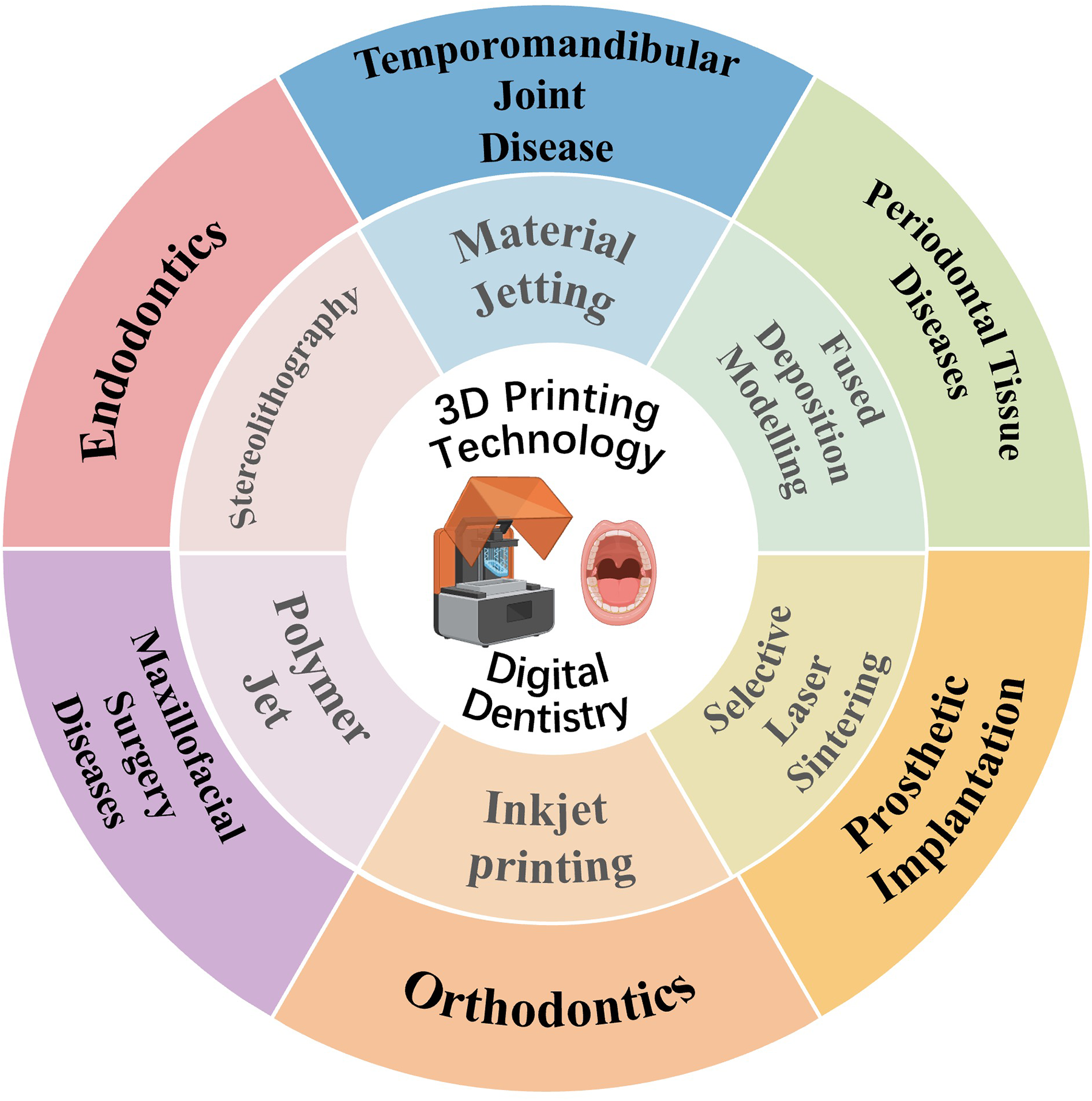
Clinical applications of three-dimensional (3D) printing technology in digital dentistry.
Classification of 3D Printing Technologies
Currently, the most prevalent AM techniques in dentistry are represented by stereolithography (SLA), fused deposition modeling (FDM), selective laser sintering (SLS), and material jetting (MJ). 13 While these technologies were initially developed for manufacturing traditional products, the current research frontier has shifted significantly. As elaborated in this section, distinct 3D printing principles impart fundamentally inherent physicochemical characteristics. They act as critical biophysical cues that profoundly modulate stem cell mechanotransduction, immune microenvironment remodeling, and directed tissue regeneration. Therefore, this section transcends basic technical classification to critically examine how these core 3D printing processes are strategically leveraged as biomimetic tools to guide complex oral tissue regeneration. This section will elaborate on these primary technologies (Table 1).
Comparison of 3D Printing Technologies in Dentistry
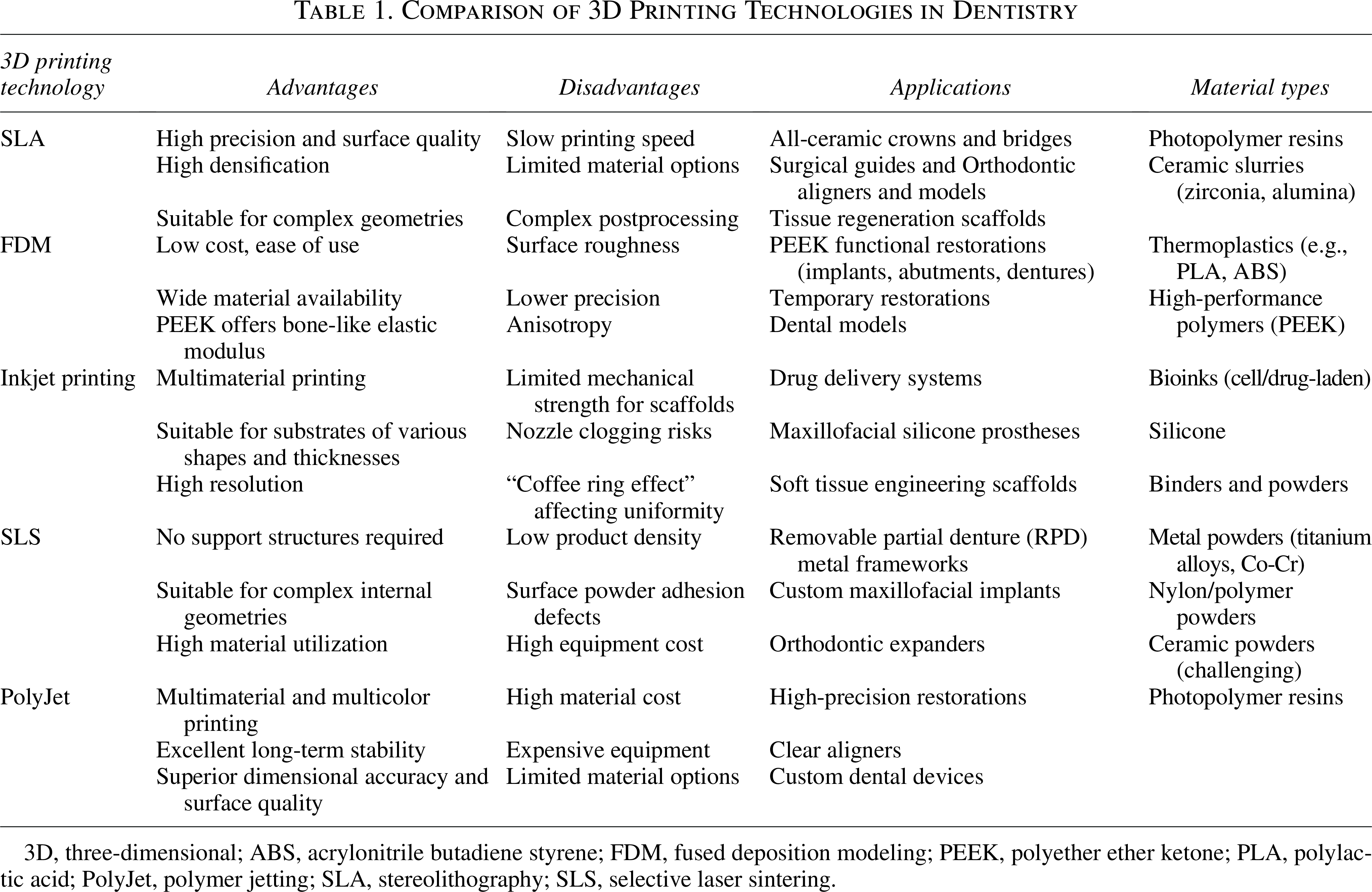
3D, three-dimensional; ABS, acrylonitrile butadiene styrene; FDM, fused deposition modeling; PEEK, polyether ether ketone; PLA, polylactic acid; PolyJet, polymer jetting; SLA, stereolithography; SLS, selective laser sintering.
Stereolithography
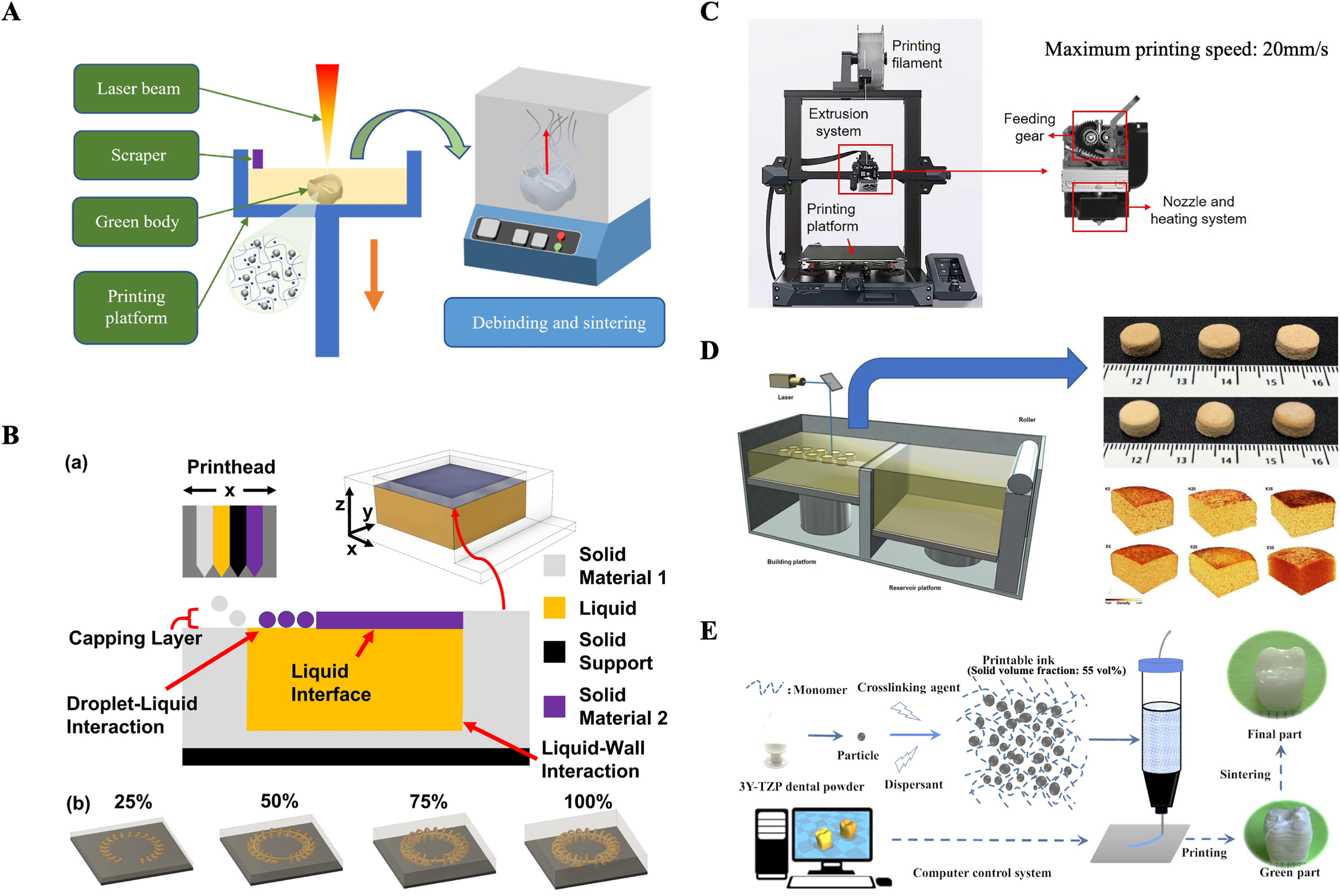
SLA is one of the earliest and most widely used 3D printing processes in dentistry. This technique uses an ultraviolet laser beam to scan and cure liquid photosensitive material point by point, thereby constructing a 3D solid object 13 (Fig. 3A). Recognized for its high precision and resolution, SLA demonstrates tremendous potential in all-ceramic AM. 14 Research indicates that SLA-fabricated ceramic components achieve high relative density and surface accuracy comparable with computer numerical control (CNC)-machined counterparts.15–18 Furthermore, SLA exhibits superior marginal fit compared with traditional subtractive manufacturing, enabling the accurate reproduction of minute anatomical structures.19,20 However, the “point-by-point scanning” mechanism limits production efficiency for large-scale objects. 21
The final precision of SLA prints is regulated by multiple factors, primarily print orientation and material properties. Print angle directly influences fabrication time and surface smoothness. 22 Research suggests that while specific orientations, such as 45°, may minimize root mean square error for intraoral implants, extreme angles like 0° or 90° introduce trade-offs between mechanical stress, delamination risks, and prolonged printing times. 23 However, studies indicate that moderate angle adjustments (e.g., 0°–20°) may have negligible effects on full-arch model fidelity, suggesting that optimal orientation is often case-dependent, 24 aligning with previous studies. However, due to variations in printing materials, printers, and other factors, current trends regarding the effect of printing angles remain inconsistent across different printing methods. Beyond geometric parameters, material characteristics play a critical role. Photopolymer resins typically undergo volumetric shrinkage during the liquid-to-solid transition, potentially causing uneven internal stress and warping. 25 In contrast, high-filler resins, such as those used for bioceramic scaffolds, exhibit lower shrinkage rates but possess higher viscosity. This imposes stricter requirements on the printer’s material deposition system to ensure structural integrity. 26
To address the speed limitations of traditional SLA, digital light processing (DLP) technology emerged as an optimization. While sharing the fundamental photopolymerization principle, DLP utilizes a microprojector (incorporating digital micromirror devices) to project light onto the entire resin surface simultaneously. 27 This “area exposure” capability significantly accelerates printing speeds compared with point-scanning SLA, making it particularly suitable for efficient chairside fabrication. 28 Although mechanical properties may vary slightly based on print orientation, DLP demonstrates accuracy sufficient for general clinical applications.19,29 Emerging iterations, such as digital press stereolithography (DPS), continue to evolve, though their stability requires further investigation compared with established methods. 30
Beyond conventional dental applications like surgical guides and orthodontic models,21,31–35 SLA and its derivative technologies hold significant value in tissue regeneration. Research indicates that SLA can be utilized to print novel microfluidic platforms for simulating biological phenomena.36,37 Moreover, SLA-printed bioceramic or polymer scaffolds can precisely mimic trabecular bone microarchitecture, offering new therapeutic strategies for personalized alveolar bone regeneration. 38 However, a critical biological bottleneck in translating these bio-inert models into in vivo tissue-engineered scaffolds is the inherent cytotoxicity of commercial photopolymer resins. From a material chemistry perspective, the photopolymerization process is often incomplete, leaving unreacted (meth)acrylate monomers and photoinitiators temporarily trapped within the cross-linked network. 39 Upon contact with physiological fluids, these unreacted substances readily leach out, accompanied by the release of micro/nano-sized polymer particles (MNPs) from the scaffold surface. 40 Crucially, from an osteoimmunology standpoint, these leached resin microparticles and toxic byproducts act as potent proinflammatory stimuli. Upon phagocytosis by macrophages, they trigger the polarization of naive macrophages toward the classical M1 (proinflammatory) phenotype, 41 while liquid monomer components severely disrupt the normal immunomodulatory functions of macrophages. 42 This prolonged inflammatory microenvironment effectively impedes subsequent stem cell recruitment and osteogenic differentiation.
To overcome this biological barrier, current research is shifting from passive adaptation to active material innovation, focusing on two main strategies: underlying chemical reconstruction and composite immunomodulation. The first strategy involves utilizing renewably sourced, circular photopolymer resins. By replacing traditional toxic (meth)acrylates with bio-based monomers, the leaching of proinflammatory byproducts is drastically reduced, fundamentally endowing the material with intrinsic biocompatibility and degradability. 40 The second core strategy is the fabrication of nanocomposite resins by doping them with inorganic particles such as hydroxyapatite (HA) or bioactive glass. These bioceramics not only compensate for volumetric shrinkage during the printing process but also actively remodel the immune microenvironment by inducing macrophage polarization toward the prohealing M2 phenotype, thereby establishing an ideal osteogenic niche for alveolar bone regeneration.43,44
Fused deposition modeling
FDM, or fused filament fabrication, constructs objects by extruding melted thermoplastic polymers (e.g., PLA, nylon) layer by layer (Fig. 3B). 45 While accessible, FDM is characterized by the “step effect” and inherent mechanical anisotropy, where Z-axis bonding is weaker than intralayer strength.46–48 This mechanical anisotropy implies that when subjected to complex external forces, parts are highly susceptible to delamination or fracture along the interlayer boundaries, posing a structural vulnerability. 48 Specifically, the build orientation (X, Y, and Z axes) fundamentally dictates the material’s mechanical properties. Parts printed horizontally within the X–Y plane benefit from continuous filament extrusion, thereby maximizing tensile and flexural strength. Conversely, parts oriented along the Z (vertical) axis rely solely on weaker interlayer thermal bonding, rendering them prone to delamination under stress. In clinical applications, this anisotropic behavior necessitates precise part orientation based on anticipated stress vectors. For instance, when fabricating fixed dentures, orienting the prosthesis parallel to the Z-axis makes it vulnerable to fracture under vertical masticatory forces. Therefore, horizontal (X–Y) or computationally optimized angular orientations (e.g., a 45° printing angle) are required to significantly improve the fracture resistance of the prosthesis. 49
However, in tissue engineering, this anisotropy can be strategically leveraged as a powerful biomimetic tool for complex tissue regeneration. The layer-by-layer extrusion process inevitably generates microgrooves and directional stiffness gradients. Stem cells, such as periodontal ligament stem cells (PDLSCs) and articular cartilage progenitor cells, actively sense these anisotropic physical cues through integrin-mediated focal adhesions. 50 This mechanotransduction process modulates cytoskeletal tension and triggers mechanosensitive signaling pathways, particularly the nuclear translocation of Yes-associated protein/transcriptional coactivator with PDZ-binding motif (YAP/TAZ), thereby driving “contact guidance.” 51 As a result, stem cells strictly align, elongate, and undergo lineage-specific differentiation along the designated printing trajectories. Therefore, contemporary regenerative medicine strategies no longer strive to eliminate FDM’s anisotropy; instead, they actively exploit its directional microarchitecture to reconstruct highly oriented physiological tissues, such as the periodontal ligament, skeletal muscle, and knee menisci.52,53
Although FDM generally exhibits lower precision compared with SLA54,55—with previous studies reporting a mean precision error of 74.4 μm for FDM-fabricated prostheses versus only 23.5 μm for SLA—industrial-grade printers can achieve high accuracy (e.g., 2 μm deviation), 15 and the printed parts often demonstrate superior flexural strength. 56 The quality of these constructs is strictly regulated by parameters such as layer thickness, print speed, and nozzle temperature, which must be optimized to minimize porosity and surface roughness while preventing defects like warping.57–60
A critical advantage of FDM in dentistry is its ability to process polyether ether ketone (PEEK). PEEK offers exceptional biocompatibility and an elastic modulus similar to human bone, allowing it to buffer occlusal stress—a property superior to rigid titanium or brittle resins. 61 Despite challenges regarding osseointegration and aesthetics,62,63 FDM facilitates the fabrication of PEEK-based functional implants, abutments, and dentures.63–66 Furthermore, FDM serves as a cost-effective method for producing drug delivery systems and porous scaffolds essential for tissue regeneration. 67
Selective laser sintering
SLS involves using a high-power laser to selectively sinter powdered materials (polymers, metals, ceramics) layer by layer (Fig. 3D). A key advantage of SLS is its ability to fabricate complex internal geometries without support structures, offering exceptional design freedom for personalized medical devices.68,69 In tissue engineering, this capability is pivotal for creating porous titanium implants that demonstrate excellent biocompatibility and elastic moduli close to those of the human mandible, thereby facilitating osseointegration.70,71 Furthermore, by adjusting laser scanning speeds, SLS allows for the fabrication of high-porosity drug delivery systems.
In clinical prosthodontics, SLS is widely used to manufacture removable partial denture frameworks and implant abutments. Studies indicate that these components exhibit lower stress levels and higher passive fit accuracy compared with traditional casting, significantly reducing manufacturing costs and errors.2,72–74 However, SLS faces limitations when processing ceramics; printed products often suffer from low density, surface powder adhesion, and cracks (linear shrinkage reaching 30–50%), necessitating complex postprocessing such as hot isostatic pressing.75–77 The quality of SLS prints is strictly governed by energy density parameters (laser power, scan speed, spacing), which must be optimized to ensure sufficient interlayer bonding and densification.78–80
Building upon the principles of SLS, selective laser melting (SLM) and direct metal laser sintering (DMLS) emerged as specialized extensions for metallic materials. Unlike SLS, which sinters particles, SLM fully melts metal powders into a liquid state, typically achieving higher density and precision comparable with traditional casting. 69 Similarly, DMLS operates without binders to produce high-strength functional parts. 81 Together, these technologies provide robust solutions for rigid structures such as surgical guides and orthodontic appliances.82,83
Material jetting
MJ constructs functional components by selectively depositing droplets of liquid materials (photopolymers, waxes, or bioinks) layer by layer through precision nozzles. 84 A primary advantage of this technology, particularly Inkjet Printing (Fig. 3C), is its voxel-level control and compatibility with heat-sensitive materials, making it ideal for pharmaceuticals and biological applications. 85 Despite technical challenges such as nozzle clogging, 86 MJ has demonstrated versatility in oral medicine: applications range from printing full-color silicone maxillofacial prostheses 87 and drug-loaded oral films 88 to fabricating ceramic bone tissue engineering scaffolds capable of inducing osteogenic differentiation. 89
PolyJet (PJ), a specialized form of MJ, ejects microdroplets of photopolymer resin cured instantly by ultraviolet light (Fig. 3E). 90 Its distinct advantage lies in multimaterial capabilities91,92 and exceptional dimensional accuracy with ultra-thin layers. 93 While PJ resins may exhibit different mechanical behaviors compared with traditional poly (methyl methacrylate) (PMMA), 94 the technology offers superior long-term dimensional stability critical for clinical workflows. 95
Although mechanical properties such as flexural strength are influenced by print orientation and layer thickness,96,97 the most significant potential of MJ in regenerative medicine lies in surface engineering. Research indicates that anisotropic surface structures generated by specific MJ printing strategies can actively guide human gingival fibroblasts (HGFs). This contact guidance promotes optimal cell adhesion, directed migration, and soft tissue-related gene expression, opening new avenues for manufacturing bio-guided dental prosthetics.94,98
Application of 3D Printing in Dentistry
3D printing in dentistry has evolved from fabricating bio-inert anatomical models to constructing personalized, bioactive scaffolds for tissue regeneration. By integrating digital imaging with AM, it enables precise anatomical matching while providing instructive microenvironments that support cell recruitment, vascularization, and tissue growth. Across disciplines, this technology is shifting treatment paradigms from passive restoration to functional regeneration. This section summarizes its key applications, with an emphasis on underlying biological mechanisms and regenerative outcomes (Fig. 1) (Table 2).
Categorization of Dental Applications and Each Printing Method
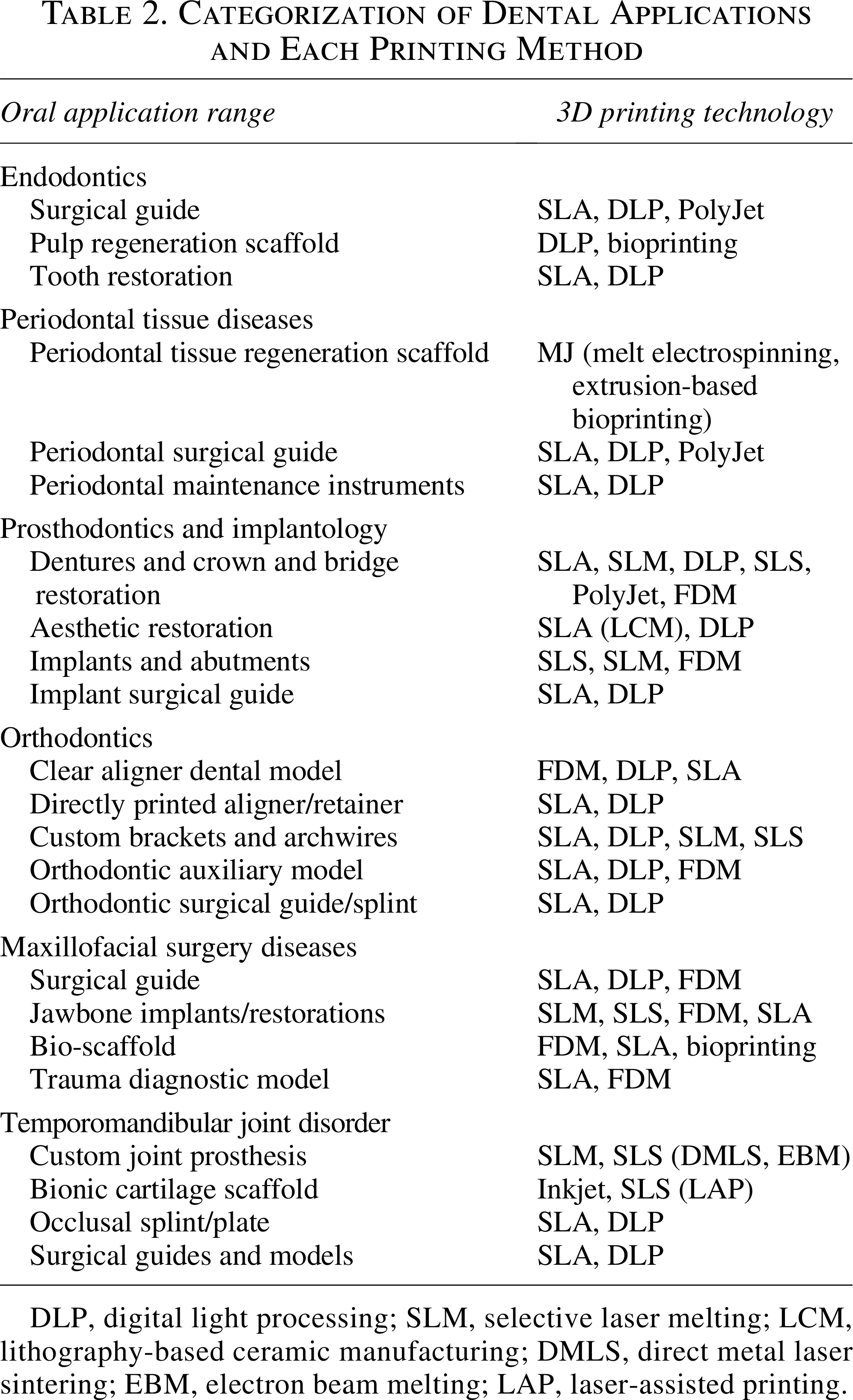
DLP, digital light processing; SLM, selective laser melting; LCM, lithography-based ceramic manufacturing; DMLS, direct metal laser sintering; EBM, electron beam melting; LAP, laser-assisted printing.
Bio-instructive mechanisms of 3D-printed architectures
3D-printed constructs regulate regenerative outcomes through a multiscale hierarchy of physical cues. At the macroscopic scale, printing-induced anisotropy (e.g., FDM toolpaths) provides “contact guidance,” triggering integrin-mediated focal adhesions and the nuclear translocation of YAP/TAZ. 99 This mechanotransduction cascade forces stem cells to align and elongate along designated trajectories. At the mesoscopic scale, pore geometry and size (typically >300 µm) dictate oxygen diffusion and interstitial fluid shear stress, which collectively modulate macrophage polarization toward a prohealing M2 phenotype and drive osteogenic differentiation.100,101 At the nanoscale, surface energy and topography (e.g., specific roughness ∼60 nm) govern the conformational unfolding of adsorbed serum proteins, such as fibronectin, exposing Arg-Gly-Asp (RGD) sequences to activate specific integrin pathways (e.g., Ras homolog family member A/Rho-associated protein kinase [Rho/ROCK], extracellular signal-regulated kinase [ERK]), thereby enhancing cell proliferation and matrix mineralization (Fig. 4).102,103
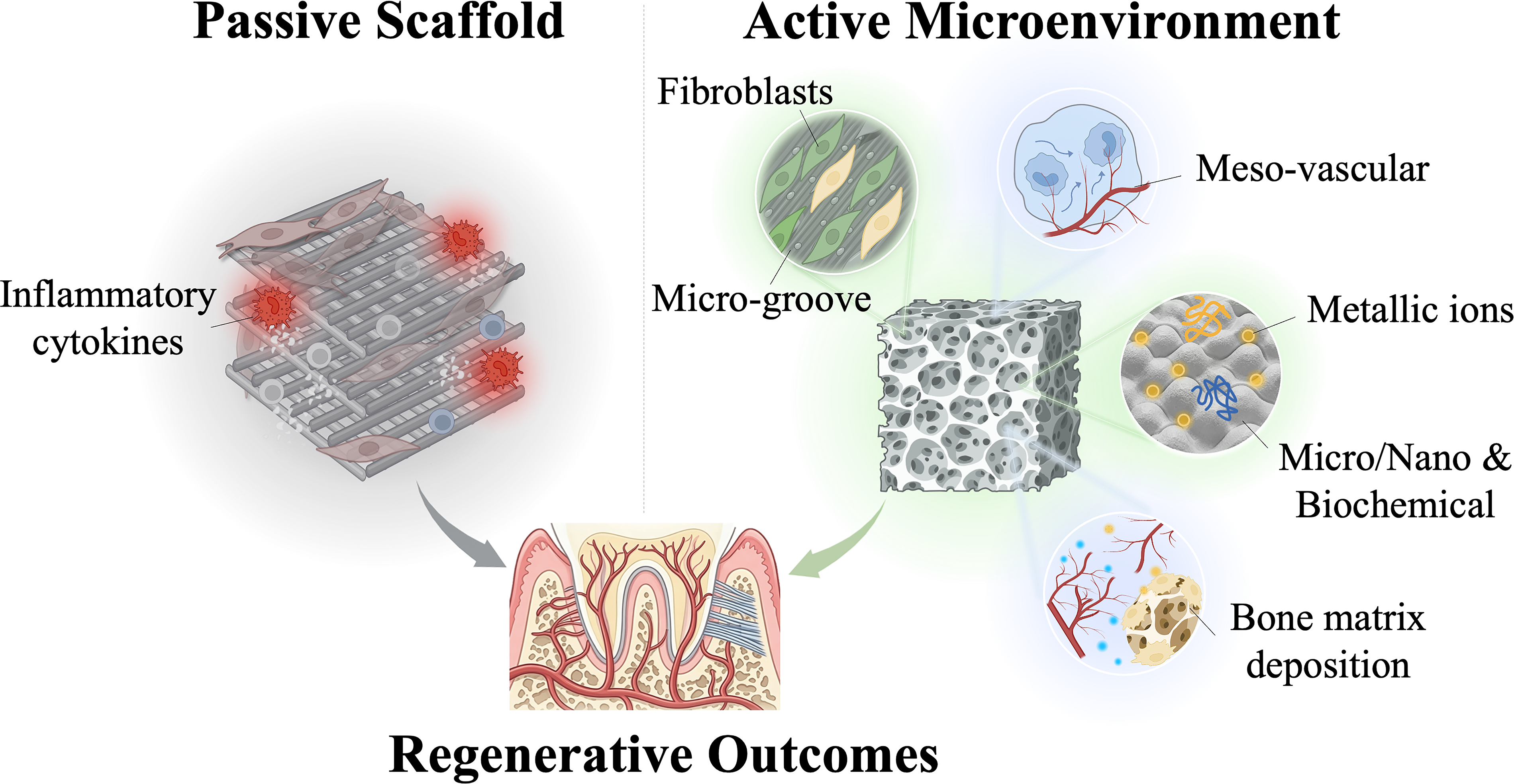
The paradigm shift of 3D-printed constructs from passive physical scaffolds to active instructive microenvironments.
Endodontics
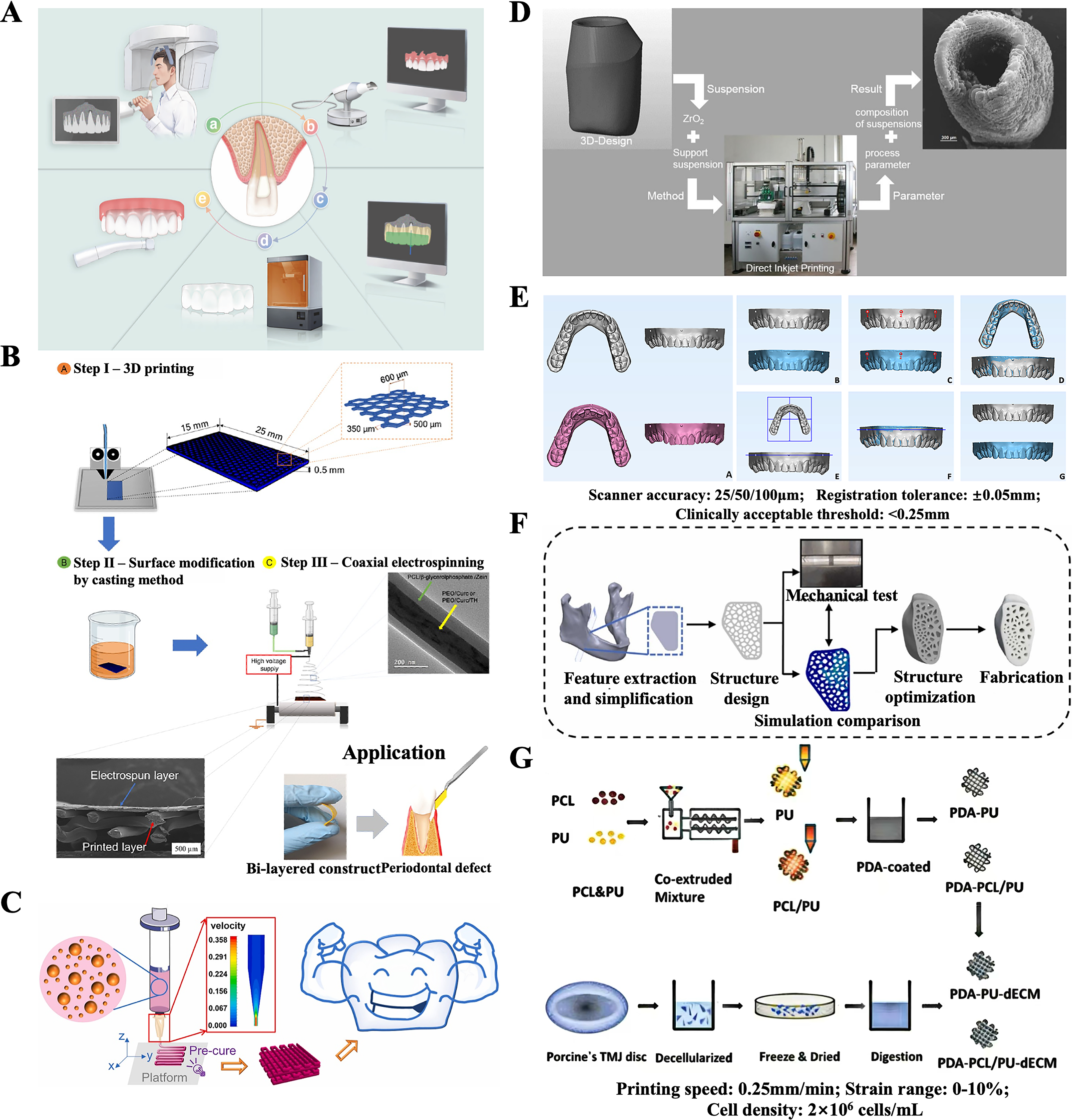
In endodontics, 3D printing is evolving from auxiliary surgical tools to biological regeneration strategies (Fig. 5A). Clinically, the technology is established in fabricating surgical guides for treating calcified root canals32,104 and pulp canal obliteration. 105 These guides visualize concealed structures and minimize iatrogenic damage during access preparation.3,32,104,106–109 Similarly, in apical surgery, printed guides assist in precise osteotomy and lesion enucleation, preserving cortical bone integrity.110,111 Further applications extend to restoring dental defects with monolithic resin cores, streamlining workflows compared with traditional post-and-core systems.112,113
To achieve true physiological vitality, contemporary endodontic research has shifted from inert guides toward 3D-bioprinted bioactive scaffolds to regenerate the pulp-dentin complex. By leveraging precisely controlled microarchitectures, such as polycaprolactone (PCL) bilayer scaffolds doped with bioactive glass, 114 these constructs provide biophysical cues that explicitly direct the odontogenic differentiation of human dental pulp stem cells (hDPSCs). 3 Crucially, smart scaffolds must address the most formidable hurdle: rapid revascularization within the narrow root canal. Utilizing DLP technology and gelatin methacryloyl (GelMA)-dextran emulsion bioinks, researchers have successfully constructed biomimetic hydrogels that regenerate vascularized, pulp-like tissue precisely matching complex root canal morphologies. 115 Moving forward, optimizing the degradation kinetics of these hydrogels to synchronize with nascent tissue formation, while overcoming their inherent mechanical limitations, remains a critical imperative.
Periodontal regeneration
The periodontium consists of soft (gingiva, PDL) and hard (cementum, bone) tissues, making regeneration challenging. 3D printing addresses this by fabricating multiphasic scaffolds with controllable porosity. While current clinical applications include surgical guides for crown lengthening 116 and splints, 117 the frontier lies in regenerative medicine (Fig. 5B).
Layer-by-layer manufacturing allows for the creation of bioresorbable barrier membranes for guided tissue regeneration. When integrated with melt-electrospinning, these membranes guide gingival fibroblast migration while preventing epithelial down-growth.118,119 Bioprinting further enables the precise placement of PDLSCs within collagen-based bioinks to reconstruct the physiological architecture of the periodontal complex. 120
However, reconstructing the highly ordered, obliquely inserted collagen fibers of the native PDL remains a formidable challenge. By leveraging FDM’s inherent deposition anisotropy, scaffolds with defined microgrooves can be fabricated to orchestrate the spatial parallel alignment of PDLSCs.121–124 This “contact guidance” specifically mimics the oriented architecture of the native PDL interface. Beyond orientation, mesoscopic pores (300–600 µm) establish fluidic channels for vascularization and induce M2 macrophage polarization.100,101 At the microscopic and molecular interfaces, surface topography and energy drive mechanosensing. Topographically, incorporating inorganic nanoparticles (e.g., bioactive glass) creates hierarchical roughness that transforms stem cells from a detached state into a highly adherent, elongated morphology via filopodia extensions.100,125,126 Surface modifications (e.g., graphene oxide [GO], hydroxyapatite [HA], or recombinant human collagen [RHC] grafting) elevate surface energy, driving the unfolding of serum proteins to upregulate osteogenic markers such as alkaline phosphatase (ALP).126–128 Beyond physical topography, functionally addressing the periodontitis-induced inflammatory microenvironment requires biochemical cues. For instance, dual-factor coatings comprising recombinant human enamel matrix proteins and Sialin-targeted oligopeptides (e.g., Sialintide) actively drive M2 macrophage polarization and guide cementum regeneration, effectively restoring periodontal homeostasis.129–131
Prosthodontics and implantology
In prosthodontics, 3D printing technologies (SLA, SLM, DLP) have streamlined the fabrication of temporary crowns, dentures, and frameworks, offering superior precision and material utilization compared with traditional methods (Fig. 5C).3,132–134 Digital workflows enable the production of fixed and removable prostheses with excellent marginal fit and aesthetic outcomes.135–143 Specifically, lithography-based ceramic manufacturing (LCM) has demonstrated efficacy in fabricating ultra-thin veneers,144,145 while digital smile designs facilitate gingival aesthetic management.146,147 However, the application of 3D-printed resins in permanent posterior restorations remains limited by mechanical complications. Studies indicate that current materials may struggle to withstand functional occlusal forces, necessitating future research into reinforced composites and finite element analysis (FEA) to optimize fracture resistance. 138
From a tissue engineering perspective, the most transformative application lies in implantology. 3D printing (particularly SLS and SLM) enables the fabrication of porous titanium implants with controlled pore size and interconnectivity (Fig. 5D). These structures mimic natural trabecular bone, facilitating mechanical interlocking and rapid osseointegration. 148 Beyond the implant body, 3D printing enhances the surgical environment. Custom surgical guides, including advanced designs with internal cooling channels, improve placement accuracy and prevent thermal osteonecrosis.149,150
For instance, SLA-manufactured guides for complex mandibular implant surgery enable precise spatial positioning and optimal bone coverage, preventing mucosal exposure and promoting robust osseointegration. 151 Furthermore, recent AM innovations integrate digitally routed internal cooling channels that dynamically deliver coolant directly to the bone-drilling interface, effectively mitigating the thermal osteonecrosis risks associated with traditional guides. 150 These dynamically deliver coolant directly to the bone-drilling interface, effectively mitigating overheating risks.
Crucially, concerning host–scaffold interactions, 3D-printed metallic implants exhibit distinct immunomodulatory profiles compared with conventional subtractive manufacturing. For instance, SLM-fabricated Ti and Co-Cr scaffolds significantly suppress proinflammatory interleukin-6 (IL-6) secretion. 152 Furthermore, their inherent high surface roughness and hydrophilicity of printed Ti-10Ta-2Nb-2Zr or nano-topographically modified Ta scaffolds significantly enhance functional protein adsorption (e.g., bovine serum albumin (BSA),103,153 while spontaneous passivation oxide layers (e.g., TiO2, Ta2O5) act as physical barriers against fibrinogen translocation. 154 This synergistic physicochemical profile ensures exceptional biocompatibility, corroborated by negligible hemolysis rates (0.629%) and normal wound-healing responses rather than chronic inflammation. 154 Beyond surface topographies, the immense specific surface area of 3D-printed pores drives a dynamic release of metal ions. Strategically harnessed, this “double-edged sword” actively orchestrates tissue regeneration: niobium ions upregulate ALP for osteogenesis, 154 while moderate cobalt (Co) release mimics localized hypoxia, activating hypoxia-inducible factor 1-alpha (HIF-1α) to promote robust angiogenesis. 152
Furthermore, the technology plays a critical role in soft tissue engineering around implants. For complex cases such as mandibular defects or full-arch immediate loading, printed guides ensure precise positioning while protecting the periosteum.151,155–158 Crucially, custom transmucosal profile formers can be printed to shape the peri-implant soft tissue, preserving the biological width and preventing collapse. 138 Future directions focus on integrating bioactive materials into these constructs to promote stable soft tissue attachment and long-term osseointegration.
Orthodontics
In the era of precision medicine, 3D printing has revolutionized orthodontics by enabling the fabrication of personalized appliances with high geometrical complexity. Currently, technologies like SLA, DLP, and FDM are routinely used to produce clear aligner models, brackets, and retainers (Fig. 5E).3,159 A major application is clear aligner therapy. While indirect fabrication (thermoforming over printed models) remains standard,160–162 the field is shifting toward direct 3D printing of aligners using shape-memory polymers. 3D-printed orthodontic aligners bypass the mold-making steps of traditional thermoforming sheets through direct printing technology, achieving efficient and dust-free production, shortening the cycle, and reducing costs, while also offering higher precision and resistance to deformation. 163 Comparative studies indicate that while traditional thermoformed materials maintain more stable tensile strength under oral simulation (37°C, 14 days), directly 3D-printed aligners exhibit significantly higher elongation at break (e.g., increased by 25.3%). This translates to superior adaptability, shape memory, and more suitable biomechanical responses within the oral environment. 164
Research indicates that directly printed attachments exhibit superior stress distribution compared with traditional composite bonding, reducing debonding rates. 165 Additionally, personalized brackets and elastic chains can now be digitally designed and printed, optimizing force transmission based on FEA.117,166,167 Beyond tooth movement, 3D printing enhances skeletal anchorage and surgery. Personalized guides for mini-implants (TADs) allow for safe placement in complex anatomical sites by visualizing bone volume via CBCT. 168 In orthognathic surgery, printed splints facilitate precise jaw repositioning, offering superior marginal fit and shorter fabrication cycles compared with manual methods.34,169 Although diagnostic models derived from IOS/CBCT data are widely used for growth analysis,170,171 future research must address the long-term biocompatibility and wear resistance of printed appliances to validate their clinical durability.172,173
Maxillofacial reconstruction
Maxillofacial defects resulting from trauma or tumors present complex challenges requiring the restoration of both intricate geometry and physiological function (Fig. 5F). 3D printing (SLA, SLM, FDM) has transformed this field from palliative reconstruction to functional regeneration. 174
Clinically, the technology is established in fabricating surgical guides for osteotomy, tumor resection, and jaw reconstruction. These patient-specific tools, derived from CT/CBCT data, significantly improve surgical precision and reduce operating time.175–179 Similarly, 3D-printed diagnostic models facilitate preoperative planning for complex trauma cases, enhancing the understanding of fracture patterns.180–182
In maxillofacial reconstruction, the multiscale architecture governs the repair of critical-sized defects. High porosity (60–95%) and nonorthogonal pore geometries generate the moderate shear stress necessary for bone marrow mesenchymal stem cell (BMSC) migration and microvascular self-assembly.102,183,184 Nanoscale topographies act as constraint anchors for cell membranes, activating Rho/ROCK signaling to enhance BMSC proliferation. 103
Translating these mechanobiological principles into functional constructs, recent studies highlight AM’s transformative role in complex mandibular reconstruction. 185 Advanced bioprinting (e.g., projection SLA) enables the fabrication of human mandibular models with perfusable vascular channels via co-printing osteogenic and endothelial bioinks. 186 For load-bearing segmental defects, composite implants—such as laser-sintered PEEK scaffolds embedded with 3D-printed β-TCP/stem-cell cores—have demonstrated robust stress-mediated osteogenesis and masticatory restoration in vivo.187–189 Ultimately, these advanced AM strategies circumvent the morbidities of autologous grafts and the biomechanical limitations of traditional metal plates, establishing a translatable paradigm for critical-sized defects.
These constructs serve not merely as mechanical fillers but as osteoconductive templates that degrade at a rate matching new bone formation.190,191 Future strategies focus on optimizing composite materials (e.g., HA/polymer blends) to balance mechanical strength with bioactivity,192,193 transitioning from permanent implants to fully resorbable regenerative therapies.
Temporomandibular joint regeneration
The TMJ is a complex articulation requiring the coordination of bone, cartilage, and ligaments. Conventional treatments for end-stage disorders often rely on off-the-shelf prostheses, which suffer from poor anatomical fit and limited longevity (Fig. 5G). 194 3D printing (SLM, EBM, bioprinting) offers a paradigm shift from mechanical replacement to biological regeneration.194–196 For joint reconstruction, 3D printing enables the fabrication of patient-specific prostheses with optimized porous microstructures. Research confirms that porous condylar implants reduce the elastic modulus mismatch and facilitate bone ingrowth for biological fixation.197–199 Unlike solid implants, these lattice structures allow for better stress distribution, though fatigue resistance remains a challenge that requires material optimization.
However, the ultimate goal of tissue engineering is cartilage and disc regeneration. 3D bioprinting can construct bionic scaffolds loaded with seed cells (e.g., chondrocytes, stem cells) to repair defective cartilage. These scaffolds can be designed with gradient micropore structures to mimic the natural osteochondral interface, promoting cell adhesion and matrix deposition. 194 While current hydrogels face limitations in mechanical strength and degradation rates, they offer a pathway to restore physiological function rather than just mechanical movement.
Clinically, the technology also supports conservative therapies. Printed occlusal splints and surgical guides, derived from multimodal imaging (CBCT/MRI), allow for precise functional analysis and intraoperative navigation.200,201 Future efforts must integrate bioactive cues into these constructs to achieve simultaneous vascularization and innervation for true joint regeneration.
Discussion
The integration of 3D printing into dentistry represents a fundamental paradigm shift from standardized, subtractive manufacturing to personalized, additive precision medicine. While the diverse applications reviewed—ranging from passive surgical guides to active bioactive scaffolds—demonstrate immense potential, the translation of these technologies from “bench to bedside” is currently hindered by a complex interplay of material science limitations, biological integration challenges, and the lack of clinical standardization.
The mechanical–biological trade-off
The primary challenge spanning all dental disciplines is the inherent trade-off between biological activity and mechanical durability. In restorative and orthodontic contexts, current resin-based materials often lack the long-term wear resistance, color stability, and bonding strength characteristic of traditional ceramics or natural enamel, leading to premature aging and fracture.138,165 Although 3D-printed metals such as titanium offer superior strength, they suffer from high stiffness that can cause stress shielding and potential imaging artifacts.71,202
To address this challenge, a quantitative comparison of the mechanical–biological trade-offs between FDM and SLA/DLP scaffolds is detailed in Table 3. Generally, while FDM-extruded thermoplastics provide robust initial mechanical support, ensuring biological viability demands high porosity, which exponentially compromises their modulus. Conversely, SLA-printed hydrogels offer excellent baseline cell survival and tunable stiffness but operate under strict dopant toxicity thresholds.
Quantitative Comparison of Mechanical–Biological Trade-Offs and Doping Strategies Between FDM and SLA/DLP Scaffolds

Numerous novel strategies are emerging to address these existing difficulties and bottlenecks in clinical dental 3D printing. Regarding material wear resistance and antibacterial properties, improvements can be achieved through nano-filler modification (e.g., titanium dioxide/zirconium oxide nanoparticle-reinforced resins) and the further development of gradient functional composites. 211 To enhance the surface activity and biocompatibility of 3D-printed materials, adjusting the laser scanning speed can alter the volumetric energy density, directly constructing multiscale surface topographies during the molding process. Furthermore, leveraging the “spheroidization effect” can form nanoscale particulate structures that increase cell adhesion sites. Additionally, by regulating SLM process parameters and incorporating bioactive ions (Ca, Si, etc.), cytotoxicity can be mitigated, and the surface properties of implant materials can be optimized. 212
The vascularization bottleneck
Beyond material constraints, the lack of functional vascularization remains the most significant limitation in regenerating large-volume tissues. Current 3D-printed scaffolds for complex defects in maxillofacial or periodontal reconstruction often fail to establish a microvascular network rapidly enough to support cell survival in the scaffold’s core. Without an adequate blood supply, the regenerative outcome is typically restricted to the scaffold periphery, leading to central necrosis.213,214 Similarly, achieving simultaneous innervation and vascularization for complex organs, such as the dental pulp and temporomandibular joint, remains experimentally immature. While current strategies employ porous structures to facilitate passive nutrient diffusion, 197 this approach is insufficient for larger constructs.
To address the issues of “sufficient mechanical support but insufficient biological guidance” and vascularization difficulties in 3D-printed bone scaffolds, a “Material-Active Factor-Vascularized Tissue Flap” three-in-one integration strategy can be considered. 215 To overcome the limitations of single-function bioinks and insufficient bone tissue vascularization, novel bioinks can be constructed by combining cell-laden decellularized liver extracellular matrix with methacrylated gelatin, synergistically promoting stem cell proliferation, osteogenic differentiation, and angiogenesis. 216 However, the sourcing, expansion, and quality control of patient-specific stem cells (e.g., hDPSCs, BMSCs) present significant logistical and ethical hurdles that currently impede widespread clinical translation.
Technical accuracy, standardization, and clinical translation
From a technical perspective, although 3D printing is synonymous with precision, errors accumulate throughout the digital workflow. In orthognathic and implant surgery, accuracy is often compromised by CBCT artifacts and, more critically, by the mobility of soft tissues, which cannot be rigidly captured by static imaging.155–157 In orthodontics, the “stair-step” effect characteristic of FDM printing can compromise the surface smoothness of aligners, affecting patient comfort. 162
In terms of clinical translation, when evaluating whether 3D-printed products meet clinical application standards, visible-light digital scanners/CBCT scans can be used to register and compare the scanning data with the original CAD design data.217,218 Establishing standardized processes will still require future multicenter, large-sample prospective studies focusing on core indicators such as prosthesis durability and surgical healing outcomes and establishing a long-term follow-up database. At the same time, standardized protocols for the entire process should be formulated, including 3D data generation and processing, operating procedures, quality assurance, sterilization, documentation, and storage. For example, 3D-printed products can be classified according to risk level, usage scope can be limited, a quality management system can be established, filings can be made to regulatory authorities, compliance declarations can be publicly released, production processes can be standardized, and clinical evaluations can be conducted, 219 while clarifying data acquisition accuracy, printing parameter thresholds, and quality control standards. A corresponding tiered training system should be implemented to lower technical barriers and promote the transition of 3D printing from experimental applications to routine clinical practice.
Economic and commercial considerations
Crucially, the clinical translation of dental 3D printing must account for economic feasibility. As AM achieves economies of scale, in-house production offers increasingly significant cost advantages over traditional outsourcing. For instance, transitioning to desktop 3D printing can reduce per-unit production costs by 80–98% across various restorative and orthodontic applications, with investment payback periods often achieved within weeks (Table 4).
Production Costs and Investment Payback Periods for Various 3D-Printed Dental Products
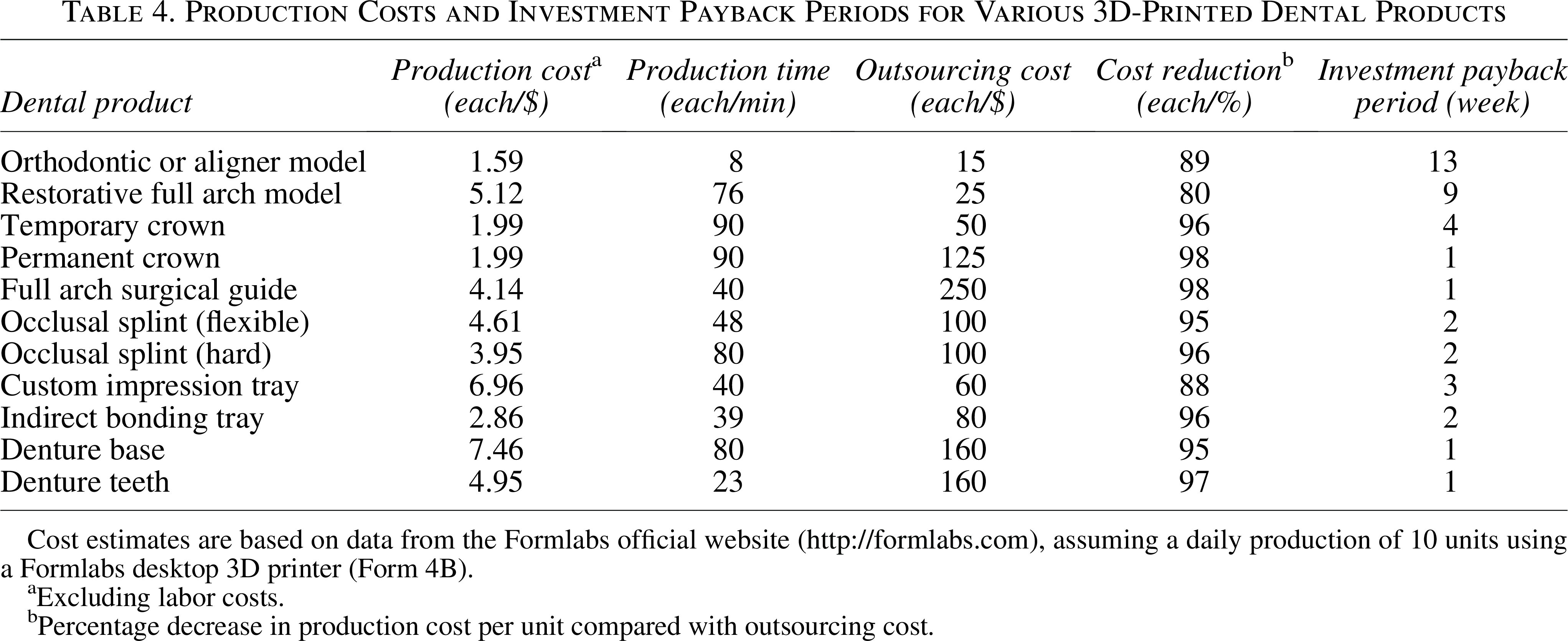
Cost estimates are based on data from the Formlabs official website (http://formlabs.com), assuming a daily production of 10 units using a Formlabs desktop 3D printer (Form 4B).
Excluding labor costs.
Percentage decrease in production cost per unit compared with outsourcing cost.
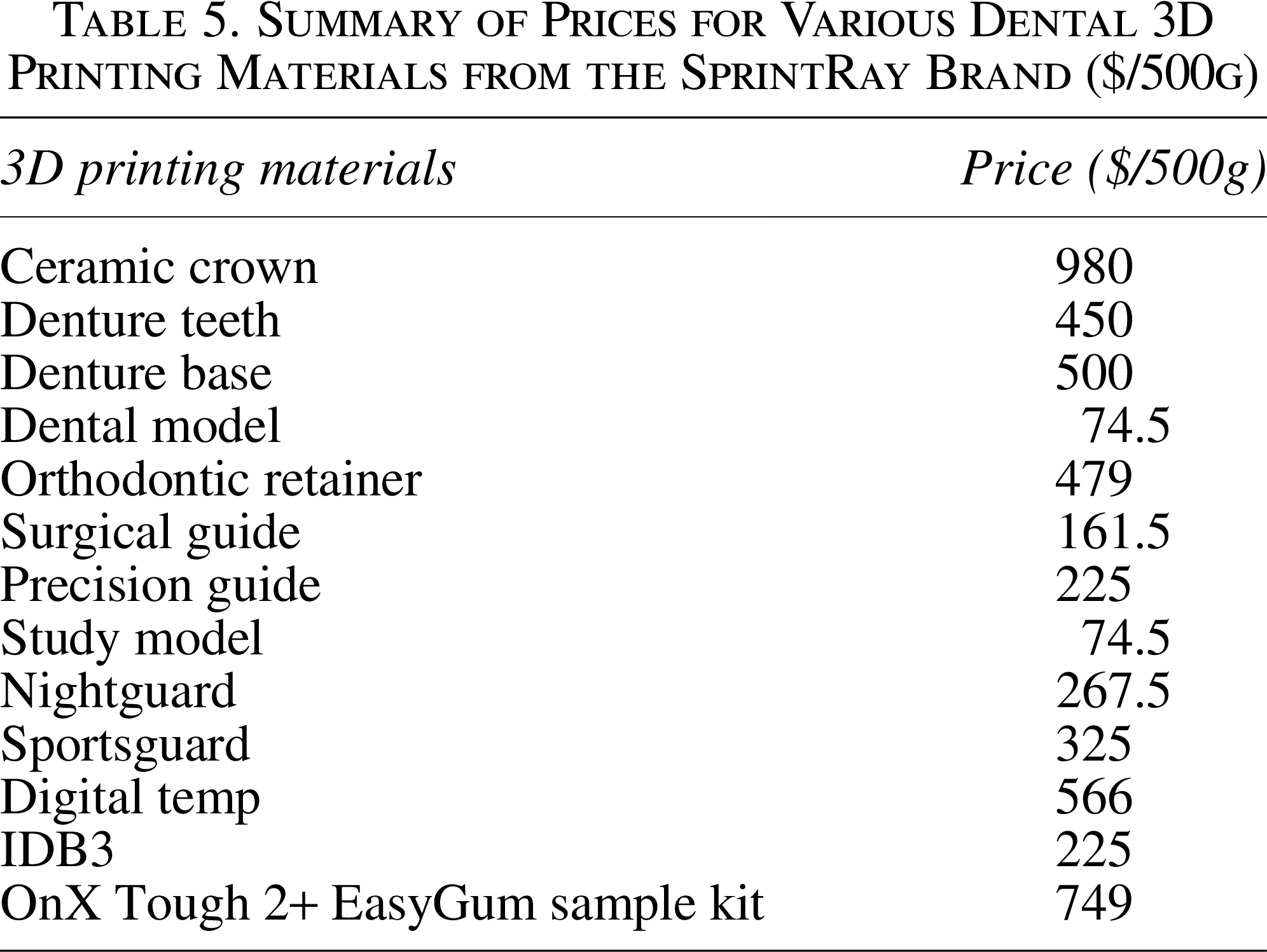
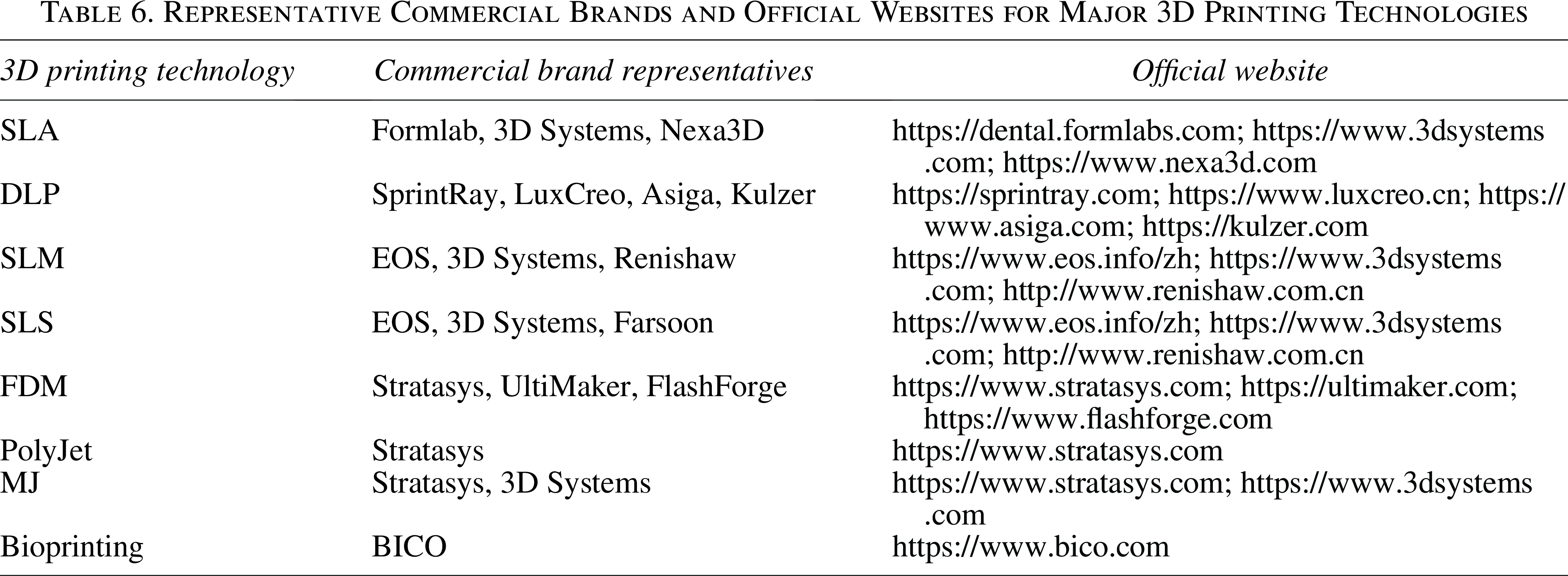
However, initial capital expenditures vary widely—from accessible desktop printers (∼$1,300) to industrial-grade systems (∼$70,000)—and consumable material costs strictly depend on the required biological or structural properties (Table 5). Ultimately, clinical decision-making requires practitioners to comprehensively balance equipment amortization, specific material pricing, and anticipated clinical volume (Table 6) to optimize return on investment.
Summary of Prices for Various Dental 3D Printing Materials from the SprintRay Brand ($/500g)
Representative Commercial Brands and Official Websites for Major 3D Printing Technologies
Future directions
To overcome these multifaceted limitations, the future of dental 3D printing lies in technological convergence. The integration of artificial intelligence (AI) is crucial; AI algorithms can automate image segmentation, compensate for soft tissue deformation, and optimize printing parameters to ensure reproducibility. 220 Furthermore, AI-driven design can customize the porous architecture of scaffolds based on FEA to match patient-specific biomechanics. Concurrently, the evolution from 3D to 4D printing—utilizing smart materials that change shape or properties over time—offers revolutionary possibilities.213,221 4D constructs could dynamically adapt to the oral environment, such as self-folding scaffolds for minimally invasive insertion or shape-memory aligners. Ultimately, material innovation must shift toward biomimetic composites incorporating growth factors and acellular matrices to actively modulate the immune response and guide regeneration.114,120,191
Conclusion
In conclusion, 3D printing has driven a definitive paradigm shift in dentistry, evolving from bio-inert subtractive restorations to the additive fabrication of bioactive, patient-specific regenerative constructs. While technologies like SLA, DLP, FDM, and powder bed fusion have achieved unprecedented control over biomimetic microarchitectures and immune modulation across dental disciplines, clinical translation remains hindered. The primary bottlenecks are the mechanical–biological trade-offs of current materials, the lack of functional vascularization in large-volume scaffolds, and the absence of standardized clinical protocols. Overcoming these barriers demands a multidisciplinary convergence. By integrating AI-driven design, multimaterial bioprinting, and 4D smart materials alongside rigorous economic balancing, 3D printing will transcend its specialized niche to become the foundational manufacturing standard of next-generation regenerative dentistry.
Authors’ Contributions
Z.L.: Conceptualization, writing—original draft, visualization, writing—review and editing. Q.D.: Conceptualization, writing—original draft, visualization. T.L.: Writing—original draft, visualization. L.G.: Writing—original draft, visualization, funding acquisition. J.W.: Supervision, project administration. W.R.: Conceptualization, supervision, funding acquisition, writing—review and editing. All the authors have read and agreed to the published version of the article.
Footnotes
Acknowledgments
The authors appreciate the technical support provided by the Core Facility of Guangzhou Medical University.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by Guangzhou Science and Technology Program [grant number:2024A03J0064]; Guangzhou Medical University 2024 Research Capacity Enhancement Program Major Clinical Research Projects [grant number: GMUCR202402023];Guangzhou Municipal Health Science and Technology General Guidance Project [grant number:20251A010081]; Zaiheng Digital Intelligence Life Science (Guangzhou) Co., Ltd. (Grant No. GYHX-202601).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.