
Abstract
Background:
Circumpolar nations are experiencing unprecedented environmental and public health policy challenges due to global climate change, exploitation of nonrenewable natural resources, the endangerment of myriad wildlife species, and growing sovereignty disputes. In a call to action, the Arctic states’ health ministers recently signed a declaration identifying shared priorities for mutual international cooperation. Among agreed-upon collaborations, an enhancement of intercultural understanding and promotion of culturally appropriate healthcare delivery systems is to be of high priority going forward.
Purpose and Aim:
In far north Canada, health policies perpetuated for generations upon indigenous communities have, traditionally, often had adverse consequences for the medically underserved inhabitants of these communities. This discussion addresses the cultural disconnect between the colonial era and current indigenous, decolonialist health and healing design strategies.
Method and Result:
In response, two architectural design case studies are presented that synthesize ecological site planning precepts with salutogenic architectural design attributes—a behavioral health and substance abuse residential treatment center and three elderhousing prototypes for construction in Canada’s Northwest Territories.
Conclusion:
This conceptual synthesis is practicable, transferable, and adaptable to varied, extreme climatic conditions, as reflective of best practices in the delivery of healthcare facilities that express a synthesis of ecohumanist and salutogenic values and methodologies. The discussion concludes with a call for empathic, evidence-based collaboration and research that further examines the blending together of prefabricated off-site construction with on-site construction approaches.
Keywords
Circumpolar nations are experiencing unprecedented international attention and mutual public health policy challenges due to global climate change, unabated exploitation of nonrenewable natural resources, endangerment of myriad wildlife species, and growing sovereignty disputes. In a call to action, the Arctic states’ health ministers in 2016 signed a declaration identifying shared priorities for mutual international cooperation. Among the agreed-upon areas of collaboration, enhancing intercultural understanding and promotion of culturally appropriate healthcare delivery systems would henceforth be of high priority aims (Chatwood et al., 2017). Indigenous communities in Canada’s far north region have historically been medically underserved, with healthcare facilities whose physical attributes typically perpetuate colonialist sensibilities. Subsequently, such health policies were rejected by the communities for whom they were intended, with north–south cultural disconnects, in the extreme, having persisted for generations. As a result, indigenous behavioral and social factors, health status, vernacular building traditions, and especially the long-standing healing role of the natural landscape warrant critical reappraisal in the current context (Martin, 2014).
The Arctic Human Health Expert Group, within the Arctic Council, established in 2009, functions as an international, policy-based forum for issues of concern in circumpolar regions. The aim is to promote the exchange and dissemination of knowledge for improving community health. In Canada, the structure of healthcare delivery in the far north has historically been structured along multiple north–south cultural and technological transference axes. Less attention has been accorded to circumpolar, that is, north–north, architectural and health-related perspectives. For purposes of this discussion, “far north” Canada is defined as the Yukon, Northwest Territories (NWT), and Nunavut. This predominance of north–south axiality often resulted in fragmented, culturally disconnected health policy outcomes—including with respect to healthcare facilities. Nunavut is typically served by regional centers in Ontario, the NWT served from Alberta, and Yukon served from British Columbia. Inuit people in Iqaluit, Nunavut, likely have far more to gain if their service providers look for collaborations in Nuuk, Greenland, rather than in Ottawa, the Canadian capital, for instance (Young & Chatwood, 2011). Given these historical, jurisdictional, and political complexities, it is worthwhile to examine this region more closely to glean lessons to be learned for the reappraisal of health policy, identifying direct care provider best practices, and for implementation by their commissioned architects and landscape architects.
Even defining what constitutes “circumpolar” can be controversial. One inclusive definition is based on the membership of the Arctic Council, whose membership consists of the United States, Canada, Denmark (with its self-governing territories of Greenland and the Faroe Islands), Iceland, Norway, Sweden, Finland, and Russia. As of 2019, far north Canada had a population of 107,000 with a population density of only .03 people/km2 (Statistics Canada, 2019). There are few cities (none with a population greater than 25,000) and many widely scattered small settlements with poorly developed physical services infrastructure (Government of Canada, 2009).
Currently, a growing number of indigenous and nonindigenous social workers and psychologists are actively “decolonizing” their practices, that is, basing their diagnoses and treatments on First Nations’ healing traditions. However, incorporating traditional healing practices in an appropriate setting requires thoughtful immersion in the inner profundities of culture, place-specificity, and local traditions. Relationships with elders and access to traditional healing practices are critical in this process (St-Denis & Walsh, 2017). Similarly, a growing number of indigenous and nonindigenous architects and landscape architects are currently working toward the decolonialization of their professional practices through immersion in culturally appropriate planning, design, and construction building methods in the far north. However, comparatively little progress has been made in the healthcare milieu, as evidenced from recent interviews with First Nations architects (Collinge, 2018). The result of south-to-north disconnection has been that large centralized nursing homes have been the norm based on the assumption it is far more cost-effective to have a large number of beds, that is, 100 beds, centralized at a single site. By contrast, the profession of social work, in particular, has recently made notable strides with regard to cultural attunement (Tamburro, 2013). Culturally attuned behavioral and social counselors have attained a measure of success in applying an autoethnographic or at minimum ethnographic perspective, whereby the customs and mores of individual peoples and cultures are systematically studied as part of a broader human-scaled perspective; the success of such strategies has, by extension, been incorporated as a core tenet of the recent Truth and Reconciliation Commission of Canada, in its published reports (Truth and Reconciliation Commission of Canada, 2015a, 2015b, 2015c).
A close affinity between human settlements and their landscape contexts remains an essential part of life in the circumpolar far north. This interdependency may be characterized as a contemporary expression of “ecohumanism”—environments that simultaneously support and foster behavioral, sociocultural, and ecological sustainability. Such indigenous places and buildings are therapeutic, and by extension ecohumanistic, because they are supportive including those that are health-related, that is, sweat lodges, healing lodges, insofar as they foster physical, psycho-emotive, and spiritual well-being with the landscape (Verderber, 2010; Wilson, 2003). Ecohumanist design strategies support their inhabitants’ short- and long-term functional performance requirements, their aspirations, and are ecologically sustainable, responsive, and adaptable without compromising either ecological or sociobehavioral attributes (Jiang & Verderber, 2016; Peters & Verderber, 2017). When present, these attributes resonate, endure, are deeply rooted in our evolutionary past (Kaplan & Kaplan, 1982) and often possess psychologically restorative properties (Kaplan, 1995).
Ecohumanist design premises are closely aligned with salutogenic design premises. Anton Antonovsky, a medical sociologist, defined the concept of salutogenesis (and by extension here, salutogenic design) as the confluence of multiple positive factors supportive of human health and well-being, in sharp contrast to then-prevailing, negativity-based definitions of sickness and disease associated with pathogenesis (Antonovsky, 1979). Salutogenesis is derived from the Latin salus, meaning “health,” and the Greek genesis, meaning “origin.” Antonovsky asserted humans need and require physically and cognitively supportive, meaningful environments as a means to cope with highly stressful everyday conditions, conditions that can threaten to destroy an individual’s sense of meaningful place attachment. The theory is premised on cognitive coherence, manageability, and “life meaning.” By extension, this perspective translates in healthcare environments into places for diagnosis and treatment that are functional and preferred on an everyday basis and in deeper, sociobehavioral and cultural terms. Such places naturally possess the amenity to resonate in the meanings and values they express.
The following discussion examines the planning, design, and construction of supportive, therapeutic healthcare facilities in far north regions with salutogenesis interpreted through the lens of an ecohumanism (Peters & Verderber, 2017). This is examined from a multifaceted perspective—therapeutic, behavioral, sociocultural, and physical health status determinants—and simultaneously from the perspective of ecological sustainability. Collectively, these determinants are viewed as constituting a more holistic definition of salutogenesis than has been typical in the literature, to date. Beyond, this perspective in architecture for health is complementary to the sizeable scientific literature on evidence-based design for health (Ulrich et al., 2008).
A holistic definition of salutogenic architecture—accounting for human and ecological well-being—posits that individuals are reluctant to relocate from familiar, ecologically stable buildings and places. These places are perceived as meaningful, enduring, and fundamental to one’s well-being. Unsupportive buildings and places, by contrast, challenge one’s mental health status and physical competencies. Comprehensibility—the ability to perceive, make sense of our surroundings—is the primary vehicle through which a psychologically disturbed or frail elderly person is able to effectively interpret, comprehend, why one is being relocated. A new healthcare setting—large or small in scale and scope—is ideally planned, designed, structured, and equipped with appropriate experiential as well as environmental supports to enable a relocated individual to function safely and effectively in both the short and long term, without posing opportunities for self-harm or harm to others in that care setting (Verderber, 2018).
Regional Context
Canada’s NWT served as the geographic setting for this investigation. The total population of the NWT was 44,469 (2011 census), including a population of 40.8% seniors aged 65 and older. Only 42.3% of these individuals have a regular physician (vs. 85.1% in Canada, overall), and repeat hospital stays for mental health treatment were 14.1% (2011). Residents in the NWT experience lower health status compared to the whole of Canada’s population per 100,000 residents, including life expectancy at birth (77.4% vs. 81.1%), avoidable deaths (310 vs. 204), avoidable deaths from preventable causes (210 vs. 133), hospitalized heart attack incidents (338 vs. 244), hospitalized incidents of stroke (175 vs. 145), self-injury hospitalizations (195 vs. 66), and hospitalizations attributable to alcohol and controlled substance abuse (1,315 vs. 239). In addition, the rates of heavy alcohol consumption (32.7% vs. 17.9%), obesity (33.7% vs. 20.2%), tobacco smoking (33.3% vs. 18.1%), and physical inactivity during leisure time (57.5% vs. 53.7%) are all greater than Canada’s overall population (Northwest Territories Health and Social Services System, 2018).
Persons residing in geographically remote communities experience significant unmet medical needs and continue to be subject to archaic governmental policies held over from the era of European-based colonization of Canada’s far north region. With respect to aged persons who reside in the NWT, 57% of the population do not have access to a family physician, more than triple the national average in Canada (15%). Chatwood et al. (2017) compared and contrasted the values identified in published governmental reports in Canada, versus grassroots, indigenous health-related values identified by the consensual process in far north communities. The former values, as identified in official reports, focus on human dignity, liberty, justice and fairness, respect, and nondiscrimination, whereas other values, as identified in the latter reports, focus on the significance of humanity, community voice and empowerment, mutual respect, cultural responsiveness, teaching and learning, nourishment, kinship, and holism (Chatwood et al., 2017). Against this backdrop, two case studies are presented below, based on recent graduate-level design studio projects at a Canadian university. This work was produced in 2018 and 2019 under the direction of the first author. 1
Case Study 1 (CS1): A Behavioral Health Rehabilitation Center Prototype
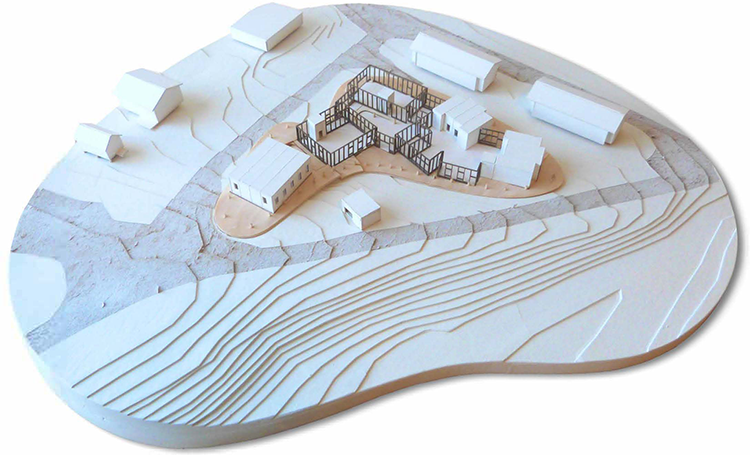
CS1, a prototype 22-bed residential behavioral health and rehabilitation center, was researched and designed by Erik Skouris. The site chosen is approximately 1 hr east of Yellowknife, in the NWT, in a remote landscape (Figure 1). The primary programmatic goal was to support indigenous teachings and rituals of knowledge transference through the Dene First Nations’ long-established cultural traditions—as applied to diagnosis and treatment of behavioral health and substance abuse–related disorders. The professional staff work on rotating, 2-week 24/7 shifts at the center, that is, psychiatric and social work counselors, physicians, and related support personnel; these specialists engage in ceremonial healing and wellness best practices drawn from long-established healing traditions. Treatment programs are centered on psychiatric, alcohol, and related controlled substance abuse, as the incidence of these disorders is of ongoing high concern in NWT First Nations and Inuit communities. As mentioned, rates of diagnosed depression in the far north are significantly higher than in other parts of Canada and especially in First Nations communities, which typically experience clinical depression rates at twice the national average. Moreover, the loss of life through suicide is an ongoing tragic aspect of everyday life in NWT communities, with rates significantly higher than the overall Canadian population (Young et al., 2016).
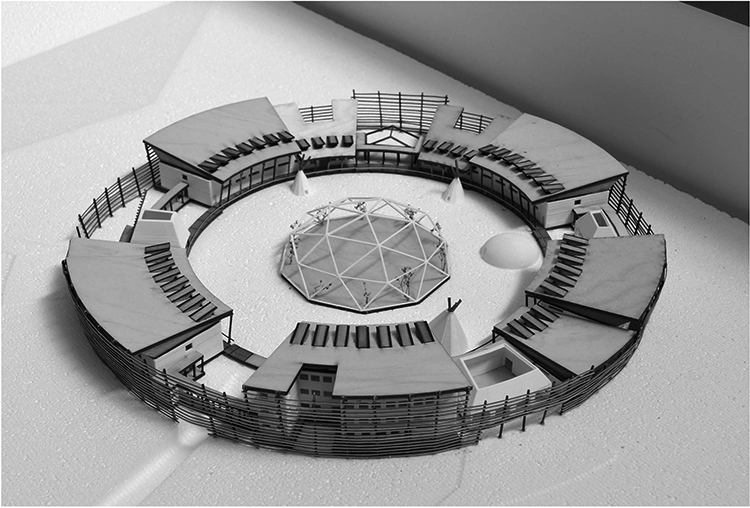
Behavioral health residential treatment center.
CS1 Salutogenic Design Concepts
(1) Participatory design process—A holistic design process centered on indigenous leadership, self-determination, and participation at all phases of project planning, including construction; (2) environmentalism—Sustainable and resilient environmental control systems, that is, heat, water management, and waste storage and disposal systems eliminating reliance on trucked-in potable water and diesel fuel; (3) self-determination—State-of-the-art job training and work placement programs for youth to attract them to careers in sustainable architecture and construction methods in far north regions; and (4) radiality—The medicine wheel and its fundamental geometric symbol—the circle—function as inspiration for spatial comprehension of physical space and its activation in consort with an individual’s deep-rooted connection to the land. The circle is a knowledge holder—Weekootowin, giving direction, by KöaàtöÃiada, to recuperation and improving one’s personal health status. Healing/treatment protocols typically consist of learning by experiencing, with one’s peers, in close affinity with the land. Hence, the plan of the center is radial, thus reinforcing safe enclosure and establishing an inward focus, further reinforced by a central courtyard with a large healing lodge at the center (Figures 2 and 3).
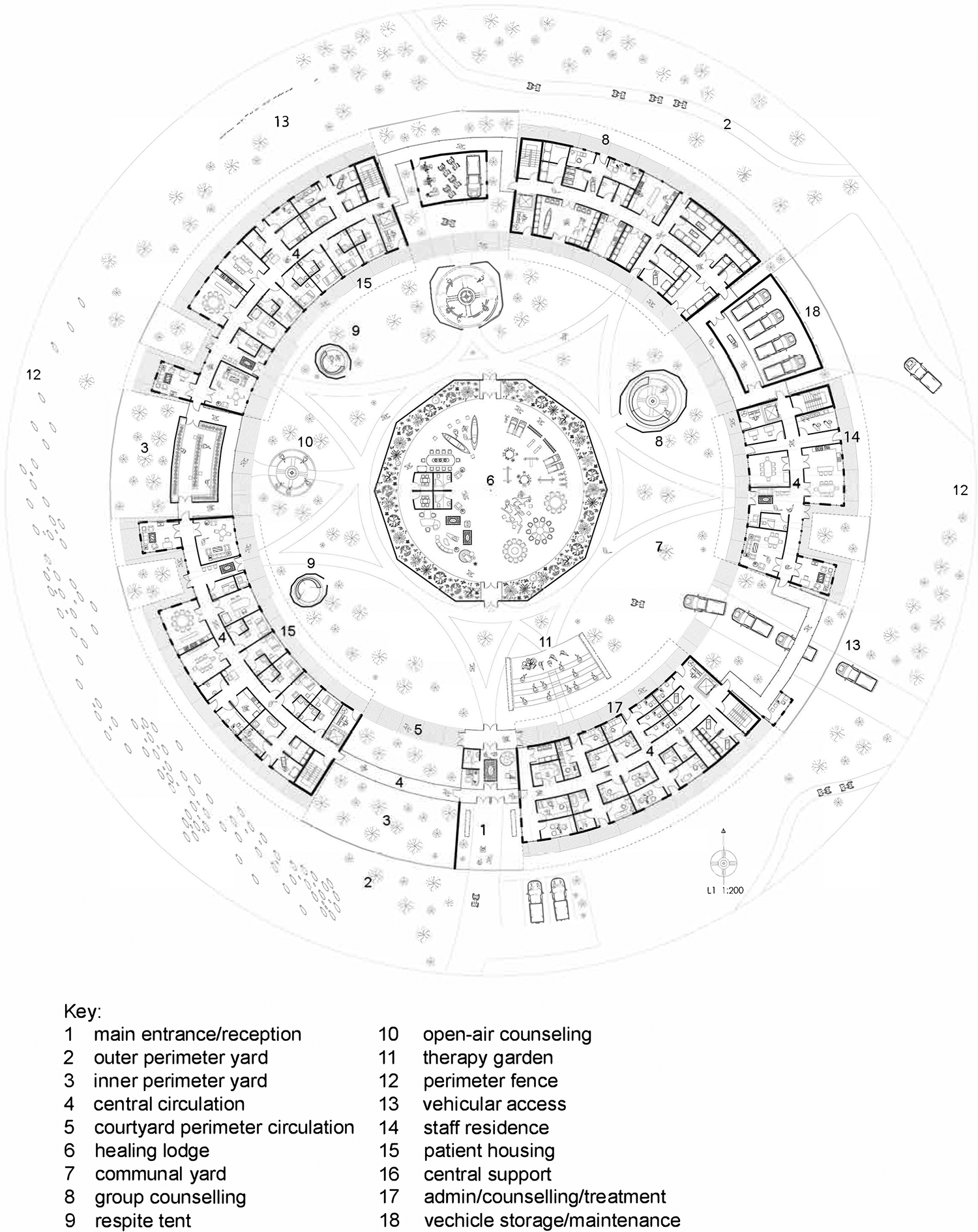
Behavioral health residential treatment center, main level plan.
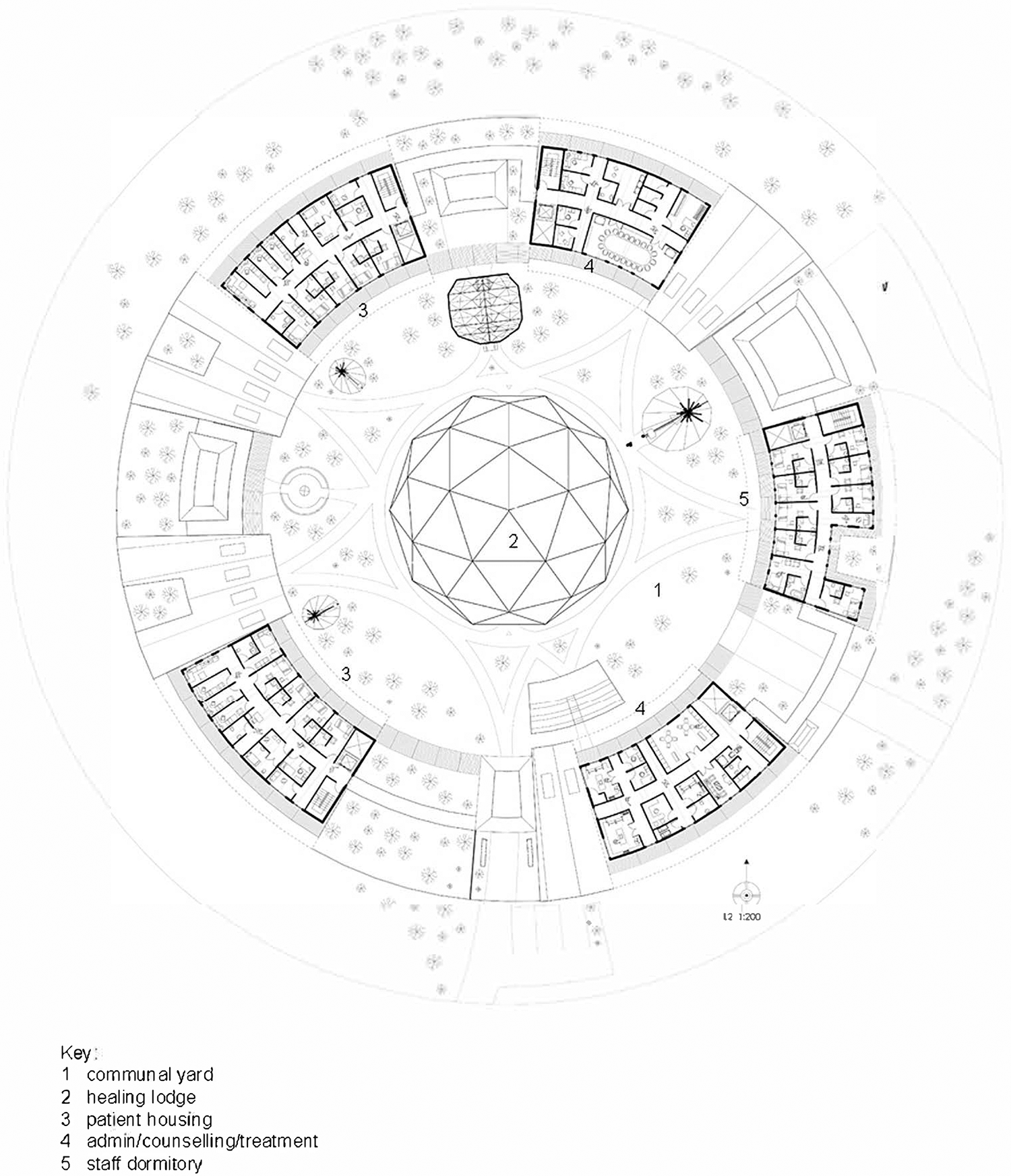
Behavioral health residential treatment center, upper level plan.
The courtyard houses traditional amenities, that is, teepee respite tent, open seating area with firepit, and a rock garden to encourage informal use by individuals and in the context of group therapy sessions. These amenities complement the architecture: Modular, with on-site conventional construction occurs in an A/B A/B pattern with intervening outdoor zones. The courtyard affords individual respite and/or group counseling sessions, as weather permits. Interior corridor circulation is circular, wrapping the courtyard, shifting from inner (courtyard) side to building’s midsection (double-loaded) conditions at intervals.
The healing lodge in the center of the courtyard recalls aboriginal sweat lodges. The sweat lodge, as a prime precursor of continued relevance, is incorporated as a salutogenic feature in a reprise of long-standing First Nations’ healing traditions. It has been found that treatment regimens centered on sweat lodge traditions continue to be effective in suicide prevention and in group therapy contexts (Duran & Duran, 1995). Sweat lodge ceremonies are holistic experiences focused on the restoration of psycho-emotive, physical, cognitive, and spiritual well-being (Smith, 2005). Sweat lodge participants have been found to attain a higher level of self-esteem (Wilson, 2003). The spiritual dimension functions as the baseline, the most fundamental aspect of this healing practice (Schiff & Moore, 2010).
Case Study 2 (CS2): Community-Based Elderhousing Prototypes
CS2 was researched and designed by Jake Pauls Wolf. The design goal was to create prototypes for the aged in the Beaufort Delta in the NWT, incorporating a hybrid of off-site prefabrication with on-site conventional construction. Three host communities were selected, places where residents’ and caregivers’ self-empowerment is achievable by means of decolonialist design strategies. Beforehand, fieldwork site visits were made to Yellowknife, Inuvik, and Tuktoyaktuk to obtain firsthand feedback vis-à-vis focus groups. This strategy was an alternative to government-sponsored long-term care facilities. These communities continue to be subjugated in this regard, with elders forced to relocate to large hospital-like facilities often remote from one’s town or village, distant from familial and social support networks. Currently, public health policy in the NWT dictates that all elders in need of long-term residential care be relocated to a central facility in Inuvik. The majority of these elders are Canadian residential school survivors (Truth and Reconciliation Commission, 2015c).
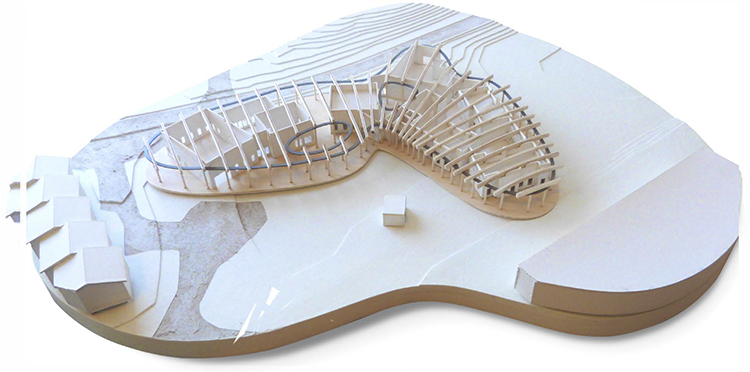
By contrast, residentially scaled, culturally grounded elderhousing is more appropriate. For one, it allows the individual to remain close to home. Inuvik would of necessity remain the baseline long-term care facility, regionally, supplemented by these proposed elderhousing centers. Based on the fieldwork, three prototypes were developed: a three-bed residence designed for each of the four communities, Ulukhaktok, Sachs Harbour, Paulatuk, and Tsiigehtchic (Figures 4 and 5); a six-bed prototype developed for communities where the population over age 70 is between 40 and 50 persons, including Tuktoyaktuk and Aklavik (Figures 6 and 7); and a comparable 12-bed prototype for communities where the elder population over age 70 ranges from 80 to 110 persons, that is, Fort McPherson and Inuvik (Figures 8 and 9).
Elderhousing prototype three-bed residence, model.
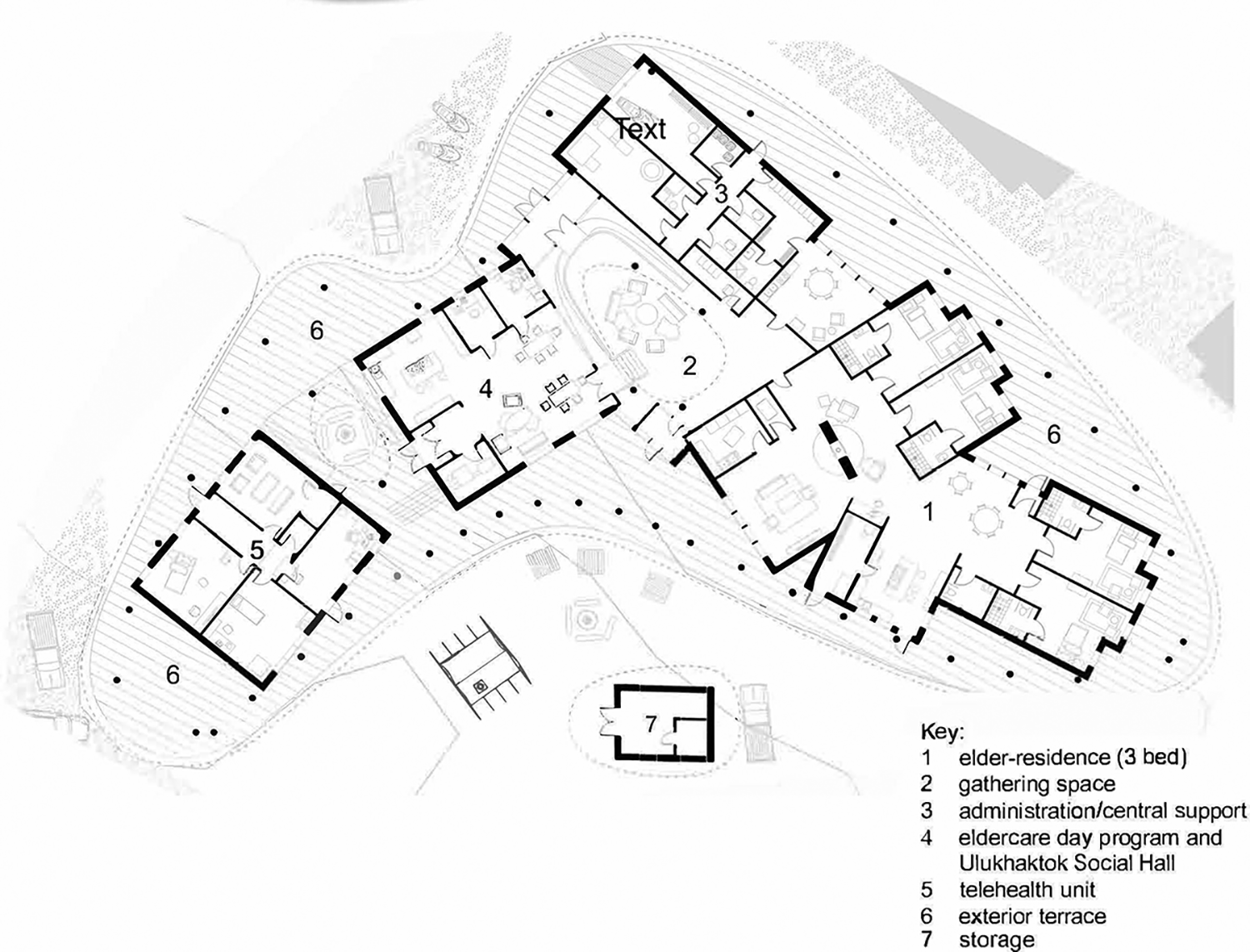
Elderhousing prototype three-bed residence, plan.
Elderhousing prototype six-bed residence, plan.
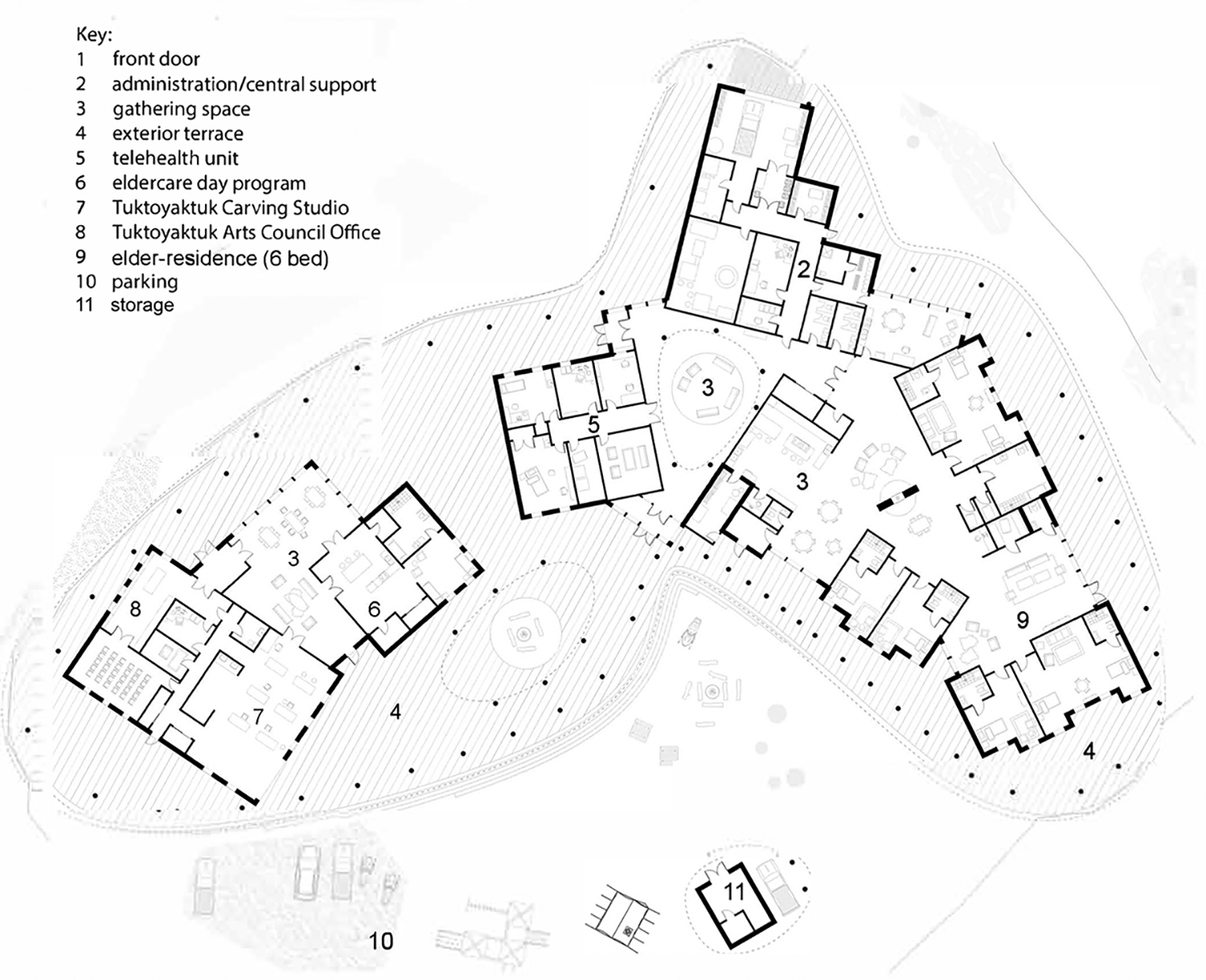
Elderhousing prototype six-bed residence, plan.
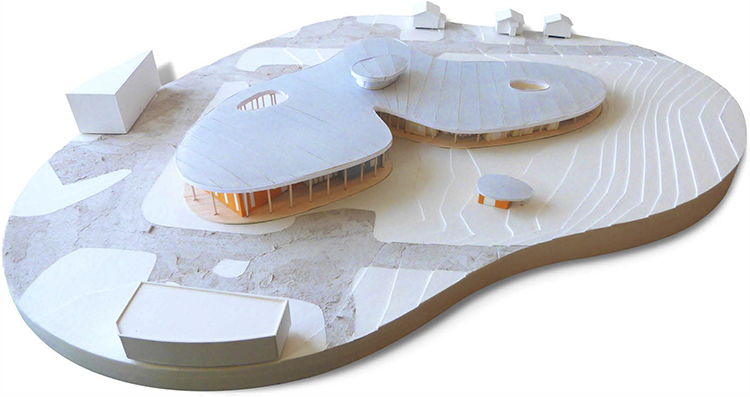
Elderhousing prototype 12-bed residence, model.
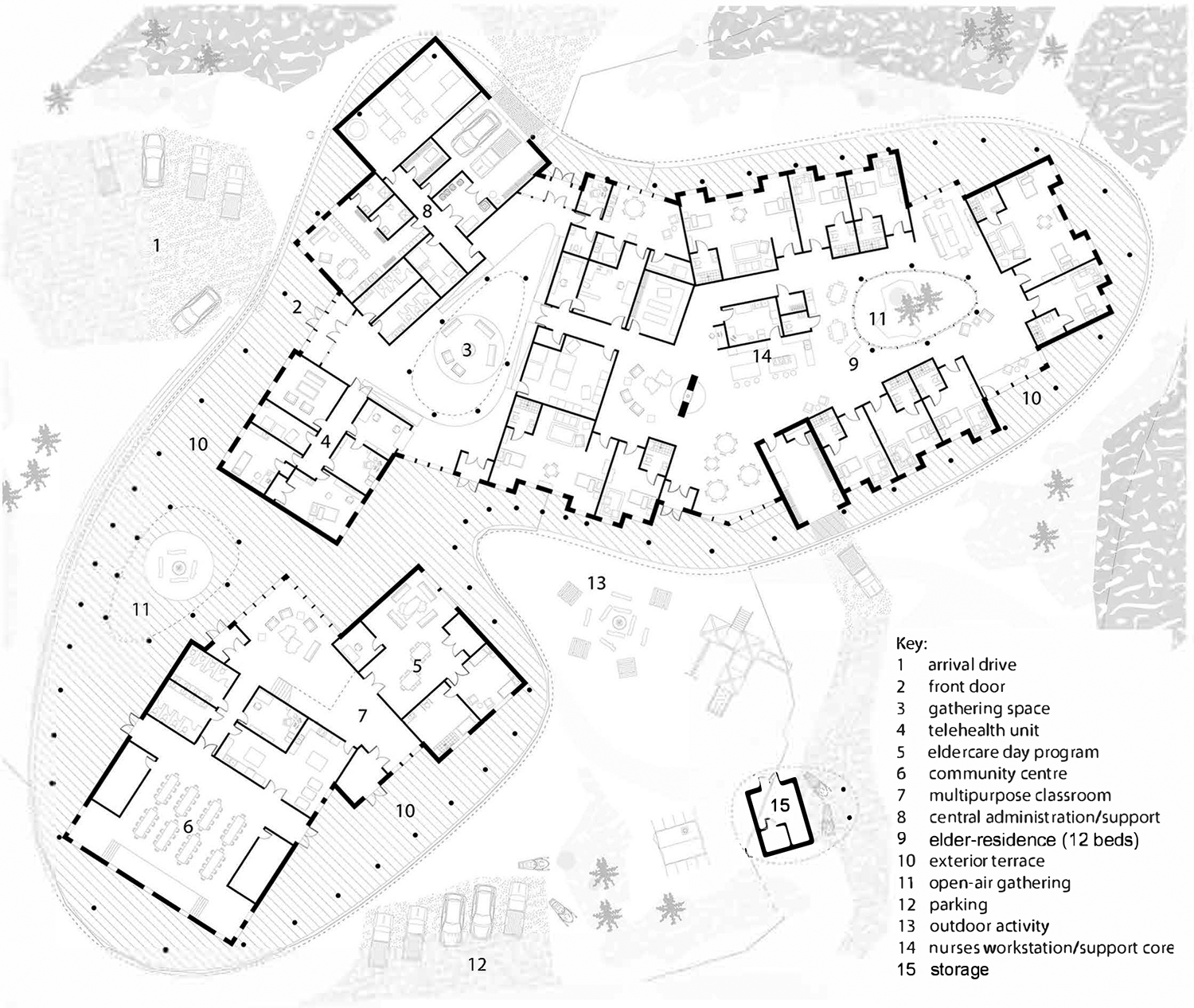
Elderhousing prototype 12-bed residence, plan.
Salutogenic Design Concepts
(1) Residential scale and imagery—These elderhousing prototypes are residential in scale and appearance and in addition house day “friendship centers,” the local community arts council, and rooms and outdoor space for local ceremonies, health-related or otherwise; (2) hybrid strategy—These small-scaled prototypes, built with a mix of local and nonlocal materials and methods, function as an alternative to large scale, impersonal, government-sponsored institutions. By contrast, they express openness, indoor–outdoor connectivity, and ecological concerns, that is, geothermal systems, entry vestibules functioning as thermal buffers, cisterns, and partial off-site prefabrication; (3) informal composition—Long, hospital-like corridors are eschewed in favor of short corridors accentuated by natural daylight and window alcove seating places. This is in direct contrast to the institutionalism of long-term care facilities in the Canadian far north; (4) involvement with nature—Site amenities include a firepit, garden in support of socialization, rituals, and traditional connections with the land. A wood deck surrounds the residence in support of nomadic camp traditions, special events, and amenities. An informal “camp” shed, teepee, parking spaces for trailers for visiting family members, garage for a transport van, and a small storehouse for food provisions. Walking paths and benches afford engagement with seasonal ponds, streams, and wetlands; and (5) hierarchy of interior space—Rooms with varied ceiling forms and proportions are aesthetically and visually stimulating. The private realm is arranged in small informal clusters in proximity to communal spaces, that is, kitchen/dining room, in support of ceremonial functions including caribou preparation for meals.
Convergences
The two case studies are inspired by anthropomorphic forms in nature, First Nations’ traditions, building performance objectives based on occupant needs and aspirations, and climate change–driven ecological determinants. In a parallel reappraisal process, psychiatry, social work, medical nursing, and physician geriatric contemporary approaches in diagnosis and treatment counseling are reappraised through the lens of traditional healing practices in far north Canada, and these best practices are increasingly of primacy in First Nations’ psychiatric, substance abuse treatment, and geriatric medicine. As such, they draw upon time-tested amenities, i.e. primacy of the outdoor firepit as an indigenous expression of theraserialization—a fusing of the words therapeutic and serialize—defined as the collaging, sequential layering, and superimposition of indoor and exterior realms along a single continuum from outdoors to indoors, and vice versa. It is an operative process centered on achieving indoor–outdoor connectivity, transparency, and maximizing the therapeutic affordances of visual and functional connectivity with nature; theraserialization is currently being expressed with respect to best practices in the design of nature-attuned healthcare facilities including hospitals, hospices, and long-term care environments for the aged (Verderber, 2010, 2018). An excellent example of this design strategy is expressed at the Hospice Djursland, in Rønde, Denmark, by C. F. Møller, completed in 2011. There, exterior–interior transparency is achieved as a series of superimposed layers, in plan, culminating in an interior landscaped courtyard. Other strong examples include patient rooms that open onto semiprivate gardens at the George Mark Children’s Hospice, in San Leandro, CA, by Remick Associates, completed in 2003, and the terraced residential units and multilevel therapeutic gardens at the Assisi Hospice, in Singapore, by New Space Architects, completed in 2016. Numerous hospices built in recent years in many parts of the world have utilized this design strategy to positive effect (Verderber & Refuerzo, 2020).
Accordingly, large, insulated windows are incorporated, affording unobstructed views without compromising thermal requirements. Second, a strategy of tempered modularity guides the use of off-site prefab construction (Verderber, 2016); significant portions of the structures as proposed would be manufactured off-site, balanced with on-site construction totaling as much as 50% of construction. These components would be transported by a combination of airlift, ship/barge, and truck, including bedroom/washroom modules, wood frame roof truss-wall systems, telehealth rooms apparatus, and counseling rooms and would be integrated with on-site construction by local tradespersons, that is, electrical, plumbing, wall systems, heating, foundation/flooring systems, exterior decking, and roofing. Modular building componentry is specified for extreme climatic and soil conditions including elevated piers to shield the building envelope from the permafrost while simultaneously being universally accessible for the physically restricted.
From the perspective of traditional healing techniques, methods of diagnosis and treatment vary greatly from tribe to tribe and from healer to healer. Such methods are especially subject to locally available food supplies, transportation supply chains, climate conditions, and time of year (World Health Organization, 2002). Regardless of whether the focus is mental health and substance abuse treatment or long-term care for the frail-aged, the focus of concern is restoring functional and cognitive capabilities and one’s outlook on life itself. Techniques for restoration of behavioral imbalances, cognitive, and physical abilities in indigenous healing may include divination or prediction to foretell or forecast events or situations, including interpretive dreams; fasting; exposure to natural elements such as water, fire, smoke, stones, or crystals as aids in seeing reason or the source of one’s imbalance; prayer, dance, chanting, use of music, singing, drums, and rattles; laying on of hands; talking and counseling; medicinal plants or botanical mixes made into teas, salves, ointments, or purgatives; rituals and ceremonies occurring around the firepit, in sweat lodges, shake tents; storytelling, stargazing, and substance smoking (Struthers et al., 2004).
Summary
The two case studies are grounded in normative traditions long retained by First Nations communities in Canada’s far north. CS1, a 24/7 behavioral health and rehabilitation residential center for persons suffering from psychiatric disorders and alcohol and drug dependency, is an inpatient facility located on a remote site near Yellowknife, NWT. CS2 consists of three alternative elderhousing prototypes for small communities in the far north. In both, the intent is to reject often ill-fated health policies perpetuated by mainstream Canada’s healthcare system with respect to planning, designing, constructing, and operating conventional evidence-based healthcare environments. The underlying assumption of this alternative strategy is that it can help overcome the unfortunate legacy of colonization and of forcing individuals into culturally inappropriate institutions. Both case studies consciously incorporate the operative inclusion of theraserialization as a design concept. In CS1, it is expressed in the main circulation artery encircling the courtyard, allowing views into and from it. In CS2, it is expressed in the relationship between the residential and adjacent exterior realm. In both, transparency and spatial layering is prominent with visual and functional connectivity tempered in order to retain thermal warmth and also to ensure safe, secure conditions.
Circumpolar regions across the globe share commonalities with regard to ill-fated government-imposed public health policies. In Canada, their impact has been 2-fold. First, traditional healing modalities and the resulting buildings were suppressed during colonialization. Second, colonialist government polices had devastating consequences on both the physical and mental health of First Nations populations. The influential 2002 Romanow Report on the future of Canada’s health system emphasizes that “The health system must (now) reflect the values, needs and expectations of all Canadians, including Canada’s aboriginal peoples. The poor health status of Canada’s aboriginal peoples is a well-known fact and a serious concern not only to aboriginal peoples but also to all Canadians. This situation is simply unacceptable and must be addressed” (Romanow, 2002, p. 12).
The result has been a reappraisal process debunking public health policies, a process referred to in the health sciences and the humanities literature as decolonialization. Decolonialization, as pertaining to evidence-based healthcare environments, is an innovative strategy affording much promise in circumpolar communities. Concurrently, the narratives of First Nations communities in Canada are just beginning to be told, in diverse forums including the Arctic Adaptations: Nunavut at 15 exhibit in the Canadian Pavilion at the Venice Biennale in 2014 (Martin, 2014). This relationship between health and the land in the far north was a principal theme. Related research is addressing the architectural history of indigenous health–centered typologies, a history only now being reexamined in earnest. Walker (2004) argues the main commonality across built environments in the circumpolar world is their universality in terms of severe land and climatological conditions. Locally time-tested methods and typologies maximize natural resources and vernacular traditions, as many situations remain where local materials and methods remain more practical (and available) than south-to-north importation. “The skills and ingenuity that inspired traditional circumpolar architecture have not yet been lost. They can continue to inform and inspire if circumpolar peoples are included among the experts that design their homes and communities” (Walker, 2004, p. 79). For example, the skill sets and construction materiality palette essential in the design and construction of the Mackenzie Inuit Winter House must not be allowed to disappear (Arnold & Hart, 1992).
As widely reported in the media, the climate crisis is exerting a toll on circumpolar regions (Paddison, 2019). The rate of temperature rise in the Arctic is disintegrating the permafrost, releasing methane and other toxigens into the atmosphere, and loss of myriad animal species (Franzen, 2019). Every building constructed in the far north must be more resilient in the face of these disruptions (Harvey, 2019). From this point, the challenge is to build healthcare architecture in far north regions equally salutogenic and ecologically sustainable and resilient—in short, ecohumanist (Peters & Verderber, 2017). LEED-inspired methods and tools developed in more temperate climates can be adopted to the far north (Verderber & Peters, 2019). To this end, off-site prefab modular construction is increasingly seen as a feasible building procurement strategy in terms of its transport costs, adaptability to local design determinants, and timeliness, or the ability to be assembled in a matter of days or weeks, versus months—a key advantage in light of the short construction season in the far north (Peters, 2019). This blend or balance between on-site and off-site construction methods must remain the primary concern, throughout. Any architectural interventions procured and constructed in this manner, however, must be supportive of Vitruvian principles. That is, utmost attention must be devoted to the ultimate responsibility of architecture to be supportive in terms of the concurrent provision of commodity, firmness, and delight for its inhabitants (Verderber, 2012, 2016, 2017). This goal is achievable, in part, through the aforementioned design concept of theraserialization in a judicious synthesis of indigenous peoples’ time-honored, spiritually based, nature-land design traditions. However, it is recommended that any syntheses of local with nonlocal construction expertise and building technologies are to be carefully balanced, monitored, and periodically reassessed from the earliest project planning stages to construction of the built facility and its exterior environs.
Finally, future evidence-based environmental design research is warranted to ascertain the efficacy of existing healthcare facilities for the medically underserved in Canada’s far north. Any type of comprehensive postoccupancy assessment surveying, however, is best conducted with the cooperation of the appropriate governmental agencies with jurisdictional oversight and guided by experienced in-house or external consultant teams. Issues investigated should include, at minimum, patterns of functional use, environmental control systems and human comfort, appropriateness of aesthetic vocabularies, and day-to-day maintenance and upkeep issues. Evidence-based precedents exist of this type of system-wide postoccupancy assessment, including the evidence-based longitudinal survey administered by the State of Louisiana; this statewide survey was completed in 2002 and again in 2012 by hundreds of facility occupants (staff and patients). It included all of the agency’s facilities, facilities principally dedicated to medically underserved populations (Verderber & Thomas, 2013). Evidence-based research such as this is key in exploring a therapeutic healthcare architecture for the circumpolar far north, as a process centered on the fundamental role of salutogenesis as a core ingredient within a broader manifold of ecohumanist concerns, that is, placemaking, attainment of genuine cultural resonance, and the maintenance (or reestablishment) of harmonious ecological relationships (Stout, 2018). Ultimately, the provision of supportive, ecohumanist healthcare environments in circumpolar communities, in Canada and elsewhere, needs to express a deep reverence for the land and its healing affordances.
Implications for Practice
Two case studies are presented—a behavioral health residential treatment center and three elderhousing residential care prototypes—that incorporate best practices in participatory design methods involving indigenous First Nations communities in Canada’s far north region.
The synthesis of ecological with salutogenic design concepts and strategies in extreme climatic conditions represents an innovative approach that design professionals can apply in daily practice in healthcare design.
The blend of off-site prefabrication with on-site construction in the two case studies illustrates for the practitioner how a noninstitutional healthcare setting is attainable—one that makes the best use of indigenous and nonlocal design traditions, cost-effective material palette resources, and building technologies.
Footnotes
Acknowledgments
The authors thank Christopher Clark, AIA, of the Northwest Territories Social Services and Health Ministry, and James Bird for their inspiration and guidance throughout this endeavor. The authors also thank Joshua Silver and Lucas Siemucha.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.