
Abstract
Objectives:
A methodology to assess the impact of involving end users in therapeutic activities to address the hospital physical environment is provided. The impact of participating in a recreational art creation program with the aim of developing an art installation on the immediate feelings of participants and their perception of the physical rehabilitation environment (PPRE) and motivation to participate in rehabilitation (MPR) is investigated.
Background:
Rehabilitation unit design has largely excluded the perspectives of end users with disability. Including their aesthetic design contributions moves beyond contemporary approaches where their perspectives are considered.
Methods:
A two-period, mixed-methods pre–post intervention design involving within and between group comparisons is proposed. During Period 1, program participants and nonparticipants completed admission (T1) and discharge (T2) surveys including PPRE and MPR measures developed by the authors. Surveys pre and post each art session were completed. The art installation will be implemented within unit corridors. Period 2 participants will complete a T1 survey and their physical environment perceptions compared to Period 1 participants.
Results:
Participating in the recreational art program significantly improved immediate levels of calmness, happiness, pain, and physical health. There is a positive relationship between environment perception and rehabilitation motivation.
Conclusions:
People with disability should be actively involved in healthcare environment design. Arts-based programs have relevance to people with neurological injury as it promotes essential sensory stimulation. The methodology and findings can encourage further work which involves end users in the design of healthcare environments and evaluates the impact of their involvement.
A growing body of research has investigated patient perspectives of the hospital environment and the impact of hospital design on patient outcomes. Literature reviews have concluded that hospital design is a crucial factor impacting the health of patients (Laursen et al., 2014; Ulrich et al., 2008). For example, design considerations contribute to patient stress and anxiety (Laursen et al., 2014), while also impacting patient safety (Ulrich et al., 2008). An evidence-based review investigating the impact of physical characteristics of healthcare environments on health and well-being found that acoustic and visual environments and ventilation impact patient health (Salonen et al., 2013). Investigating the impact of hospital environments on the health of inpatients with distinct conditions is a necessary and an emerging area of research. There is a paucity of research investigating the impact of rehabilitation unit physical environment design on the health and well-being of people who have experienced a traumatic injury and/or have a neurological disability (see reviews by Ulrich et al. [2008] and Salonen et al. [2013] where studies considering neurorehabilitation environments are largely absent).
Adjusting to traumatic injury and/or neurological disability (e.g., stroke, spinal cord injury, or traumatic brain injury) can result in adverse psychological consequences. For example, experiencing traumatic injury has been linked to increased levels of anxiety (Le & Dorstyn, 2016) and depression (Bonanno et al., 2012; Fann et al., 2011; Williams & Murray, 2015). This is especially problematic when we consider that many people who have experienced injury often receive initial rehabilitation in hospital environments which have been characterized as unsatisfactory and negatively impacting patient psychoemotional health (Caspari et al., 2007; Shepley et al., 2017). While there is a growing emphasis on designing hospital environments as healing environments, to date, there are no definitive design standards toward ensuring favorable psychological outcomes via health facility design (Shepley et al., 2017). Similarly, definitive design standards promoting learning in rehabilitation environments are nonexistent (Lipson-Smith et al., 2019). Regardless, a variety of design considerations including access to the natural environment and the outdoors contribute to positive psychoemotional outcomes (Lakhani et al., 2019; Shepley et al., 2013; Shepley et al., 2017).
Rehabilitation unit design has an impact on the mood of people who have experienced a neurological injury (Anåker et al., 2018). Recent research has confirmed that the aesthetics, versatility, and legibility of neurorehabilitation environments should be improved (Lipson-Smith et al., 2019). Additionally, outdoor and green spaces should be maximized (Lipson-Smith et al., 2019). Aesthetics refer to beauty in design (and considers the inclusion of artwork), and rehabilitation unit aesthetics are expected to have an impact on the emotional well-being of inpatients with neurological disability and their family and friends, while also supporting integration into the community (Lipson-Smith et al., 2019).
Previous research has confirmed that exposure to artwork can influence inpatient health and well-being outcomes (Salonen et al., 2013). Iyendo et al. (2016) produced a model for understanding factors contributing to therapeutic environments which promote healing within their narrative review of studies investigating the impact of environmental design interventions on wellness in healthcare settings. Within their model, interactive artwork was identified as a factor encouraging positive distractions for inpatients. Studies within their review generally confirmed that the inclusion of artwork contributes to the healing process. Karnik et al. (2014) investigated previous patient perceptions of a collection of contemporary artwork at a health facility offering both inpatient and outpatient services. Of the patients who noticed artwork, over 70% and over 60%, respectively, indicated that the artwork improved their mood and reduced their stress.
The genre of artwork may have an impact on patient health and findings suggested that realistic artwork could reduce stress and anxiety, improve inpatient perspectives of healthcare and recovery time (Salonen et al., 2013), and promote feelings of comfort (Aalto et al., 2019). Artwork of the natural environment has been identified as preferential to abstract art; however, significant differences in health outcomes between exposure to both types are nonexistent (Eisen et al., 2008). It is worthwhile to note that findings around the value of artwork are mixed, as research has also confirmed that restorative outcomes are best achieved for patients when their room does not include artwork (Gao & Zhang, 2020). Neurorehabilitation unit physical design understandably prioritizes hazard management, while giving less emphasis on promoting psychosocial health (Colley & Zeeman, 2020). Progressing robust research investigating the impact of including artwork throughout health facilities on the health and well-being of inpatients is a worthwhile endeavor.
A 2017 white paper commissioned by the National Organization for Arts in Health (2017) included findings from an evidence-based review and confirmed that using the arts in healthcare can improve patients’ overall health outcomes, treatment, and quality of life. Key benefits include “[i]mproved outcomes, such as reductions in anxiety, pain, length of stay, and readmissions in hospitals” (p. 8) and an “[e]nhanced effectiveness in health communication” (p. 8). For people in the community with a traumatic injury and/or neurological disability, making art has been identified as an activity contributing to favorable psychological and physical outcomes (Schreefel, 2015). Art making as a part of art therapy—an approach where art development processes and theories and practices from psychology are integrated toward a new practice (Bucciarelli, 2016)—can also improve the health of those who have experienced a neurological injury. For example, for stroke patients receiving rehabilitation, participating in art therapy has resulted in a significant reduction in depression and significant improvements in physical function, and quality of life, compared to a control group (Kongkasuwan et al., 2016). (It is important to note that art therapy is a distinct discipline which is facilitated by a mental health professional with art therapy training and differs from recreational therapy where visual arts programs can be utilized to promote the well-being of people with distinct conditions [Carnes et al., 2017].) Robust evaluations of hospital rehabilitation visual art programs for people with neurological disability are limited (Morris et al., 2019; Pang et al., 2021). Of the studies that exist, few have employed pre- post intervention methodologies (Morris et al., 2019; Pang et al., 2021); furthermore, due to heterogeneity of outcomes measured (Pang et al., 2021), drawing definitive conclusions around the immediate impact of participating in visual art programs on health outcomes is not possible.
The UN Convention on the Rights of Persons with Disabilities affirms that people with disability need to be centrally involved in decision making that concerns them (Nations, 2006). End users are often excluded from hospital health facility design processes. It is long-overdue that traditional processes of hospital design founded on precedence of health facility design teams are revised, so that inpatient perspectives are prioritized (Patterson et al., 2017). Work to date has generally excluded the perspectives of those who experience physical and/or cognitive disability (Patterson et al., 2017), and thus, future work should consider their perspectives. Research has already established that arts-based methods (Smith et al., 2017) in combination with consensus building methods (Lakhani et al., 2020) can ensure the perspectives of end users with neurological disability are considered toward inclusive housing development. Including the aesthetic design contributions (i.e., developed artwork) of people with disability moves beyond contemporary approaches where their perspectives are considered.
The Current Study
Corridors serve as an essential patient space—fulfilling social and health service delivery obligations—within neurorehabilitation units (Colley et al., 2017). Furthermore, people receiving rehabilitation can spend a considerable amount of time within hallways (Blennerhassett et al., 2018). Thus, within this article, a methodology to assess the impact of involving end users in a recreational art creation program with the aim of developing an art installation throughout corridors of a rehabilitation unit is presented. Findings from the first study period are also presented. The study aimed to answer the following research questions: (i) What is the impact of participating in a recreational art creation program on the immediate feelings, motivation to participate in rehabilitation (MPR), and perception of the physical rehabilitation environment (PPRE) of people receiving rehabilitation in hospital? (Period 1) and (ii) What is the impact of implementing an art installation developed by inpatients throughout hallways of a rehabilitation unit, on the perceptions that rehabilitation inpatients have about the hospital environment and how the environment impacts their rehabilitation motivation? (Period 2)
Method
The Austin Health Human Research Ethics Committee [HREC] provided approval for this Quality Improvement Activity [ID:39023]; furthermore, the La Trobe University HREC also endorsed this decision [ID:39023]. A mixed-methods pre–post intervention design involving within and between group comparisons is underway (see the study diagram [Figure 1]). The study takes place over two periods, within an Australian rehabilitation unit largely supporting people with neurological disability. The first research question is addressed via data collected throughout Period 1, while the second via data collected during Periods 1 and 2.

Study design diagram.
Data Collection
During Period 1, participants (15 who engaged in the recreational art program [Group 1] and 21 who did not [Group 2]) were requested to complete surveys upon entering (T1) and exiting (T2) the rehabilitation unit. T1 and T2 surveys included questions to measure PPRE, MPR, and anxiety symptoms. After the art installation has been implemented, during Period 2, inpatients who enter the rehabilitation unit will be requested to complete a cross-sectional survey identical to T1 surveys completed during Period 1.
An MPR measure was developed by the authors. The measure requires participants to respond to statements on a 5-point Likert-type scale (ranking from strongly disagree [1] to strongly agree [5]). Higher values are indicative of having a greater MPR (the maximum scale value is 25). An exploratory factor analysis using the principal components method was conducted for T1 values and all items loaded on a single factor with a value greater than .50. Furthermore, Cronbach’s α for the scale was .802, indicative of the scale being reliable. A PPRE measure was developed by the authors. The measure requires participants to respond to three statements on a 5-point Likert-type scale (ranking from strongly disagree [1] to strongly agree [5]). Higher values are indicative of having a favorable PPRE (the maximum scale value is 15). An exploratory factor analysis using the principal components method was conducted for T1 values and all items loaded onto a single factor with a value greater than .50. Cronbach’s α was .849, indicative of the scale being reliable. Items for MPR and PPRE measures have been provided in Table 1.
Motivation to Participate in Rehabilitation and Perception of the Physical Rehabilitation Environment Items.

Anxiety symptoms were measured via the General Anxiety and Depression Questionnaire-7 (GAD-7; Spitzer et al., 2006). The GAD-7 requires participants to indicate how often they experience seven symptoms on a scale of 0 (not at all) to 3 (nearly everyday). Higher values are indicative of having a higher frequency of anxiety symptoms. T1 values of the scale produced a Cronbach’s α of .834, indicative of the scale being reliable. In addition to the suggested measures, T2 surveys included open-ended questions to establish the recreational art program participants’ perspectives of the recreational art program.
Those who participated in recreational art sessions also completed brief surveys prior to and after each session. Surveys included four questions to establish an individual’s level of sadness/happiness, anxiousness/calmness, pain, and physical health. Turner-Stokes et al.’s (2005) Depression Intensity Scale Circles were amended to assess the four domains (approval to amend the Intensity Scale Circles from Turner-Stokes was received). The circles were coded, so that the most positive response was a score of “6” while the most negative response was a score of “1.”
The Intervention
Group 1 participants participated in recreational art sessions which involved painting, printmaking, collage development, and drawing. Each recreational art session was approximately 2 hours in length, involved four to eight participants, and was led by a leisure therapist. At the beginning of sessions, participants were requested to describe what they would perceive as welcoming artwork. (This request was a response to anecdotal historical feedback suggesting that the rehabilitation environment was not welcoming, thus the program aimed to develop user derived artwork which was welcoming.) After participants described what was welcoming (this could be in the form of colors, textures, and/or shapes), the leisure therapist provided activities (including modes of production and/or colors) which would support their development of welcoming art. The production of artworks was a result of collaborations between several participants working together at any one time and participants were encouraged to use their mobility aid toward the completion of artworks. The collaborative artworks will be implemented throughout rehabilitation unit corridors prior to Period 2. Figure 2 provides the examples of collaborative artworks which have been created during Period 1 sessions. While photographs of corridors which will serve as sites for these artworks are provided in Figure 3.
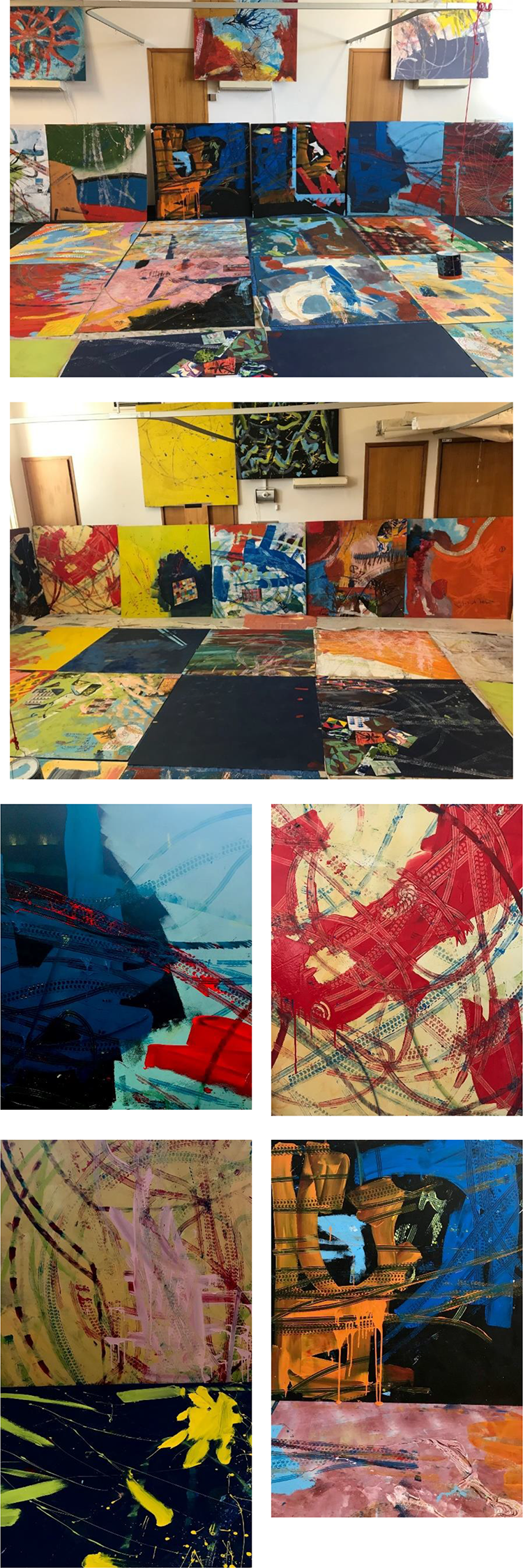
Collaborative artworks created during Period 1.

Corridors that will serve as sites for collaborative artworks.
Data Analysis
As all outcomes were not normally distributed, nonparametric tests for significant differences were progressed. To establish the impact of participating in the program on MPR, perception of the environment, and anxiety symptoms, Mann Whitney U tests for significant differences in MPR, PPRE, and GAD-7 difference sores (T2 − T1) between those who participated (Group 1) and didn’t participate (Group 2) in the recreational art program were progressed. To establish the impact of participating in recreational art sessions on the happiness, calmness, feelings of pain, and physical health of participants, the average prescore and postscore for all sessions that a participant engaged in was calculated, and Wicoxon Signed Rank tests conducted to test for significant differences between these pre- and postscores. Spearman’s rank-order correlations investigated whether a relationship between MPR, PPRE, and anxiety symptoms existed. The correlation between T1 and difference scores for each domain was tested.
Moving forward, after the art installation has been implemented, inferential analysis will establish if significant differences in inpatient perspectives of the physical rehabilitation environment exist between Period 1 and Period 2 participants exist, consequently clarifying the impact of the end-user developed art installation on inpatient perspectives of the physical environment.
Recruitment
During Period 1, inpatients who entered the rehabilitation unit between March and December 2020 were invited to participate in a quality improvement activity which consisted of them participating in a recreational art program with the aim of completing collaborative artwork which would be implemented throughout the rehabilitation unit. Recruitment was embedded into the operational process for those recently admitted to the unit. Upon admission, participants are oriented to the unit, and the extent of health and social services offered by a leisure therapist detailed. During this period, the recreational art program was introduced and inpatients were asked whether they would like to participate in the program. Both, inpatients who indicated that they were and were not interested in the program were provided the opportunity to participate in the evaluation component. Those who agreed to participate in the recreational art program and the evaluation completed surveys prior to and after each recreational art session and T1 and T2 surveys. Those who did not agree to participate in the recreational art program but were happy to complete T1 and T2 surveys were requested to complete T1 and T2 surveys only.
Participants
Fifteen inpatients participated in the recreational art program (Group 1) while 21 did not (Group 2). As one Group 1 participant did not complete a T2 survey, between groups analyses consider 14 Group 1 participants. Background information for Period 1 participants has been included within Table 2. Recreational program participants (Group 1, n = 14) spent a significantly longer time in hospital and had significantly lower FIM Motor scores (indicative of poorer function across this domain) upon entry, compared to those who did not participate in the program (Group 2, n = 21). Thus, it can be concluded that the groups differed.
Participant Background Information.
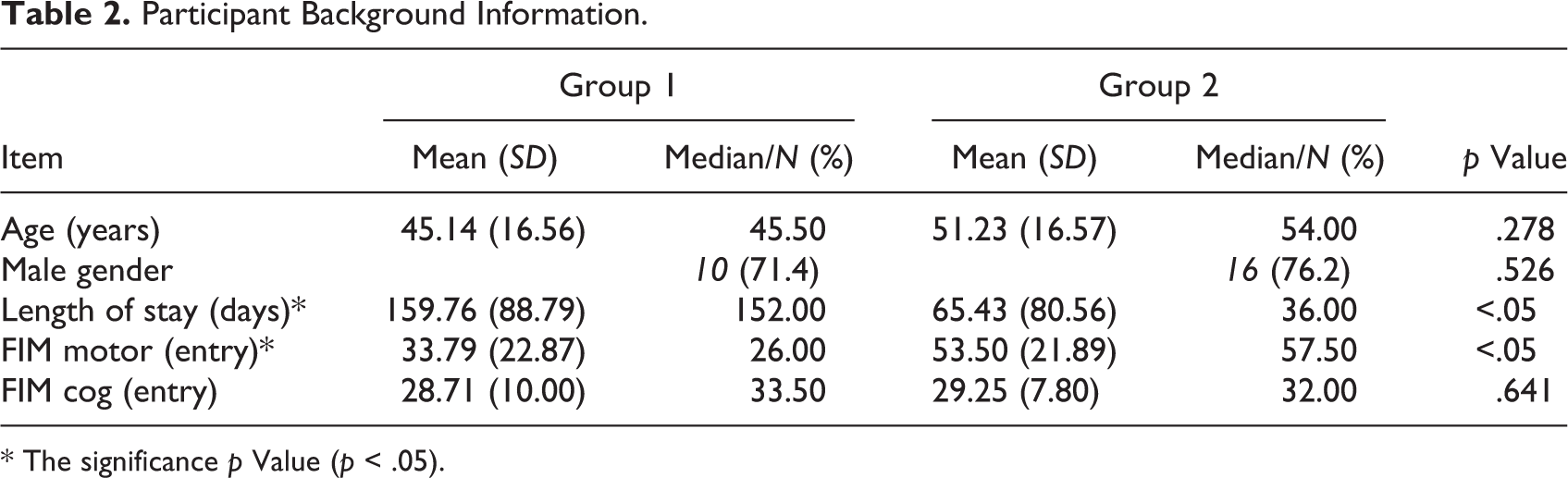
* The significance p Value (p < .05).
Findings
Impact on Immediate Feeling
Fifteen inpatients participated in the recreational art program (mean number of sessions = 3.6). Descriptive statistics for average pre- and postscores across the four domains have been included in Table 3, while median values illustrated within Figure 4. As clarified, postsession scores increased across all domains, indicative of improved outcomes across each domain after participating in recreational art sessions. Wicoxon Signed Rank tests confirmed that changes were statistically significant for all outcomes: happiness (Z = −2.521, p < .05], calmness (Z = −2.207, p < .05), pain (Z = −2.217, p < .05), and physical health (Z = −2.527, p < .05). Changes suggest significant improvement across the domains. Effect sizes across all domains were large (above .5) indicative of the intervention having a substantial effect.
Descriptive Statistics for Pre- and Postart Session Feeling Scales.

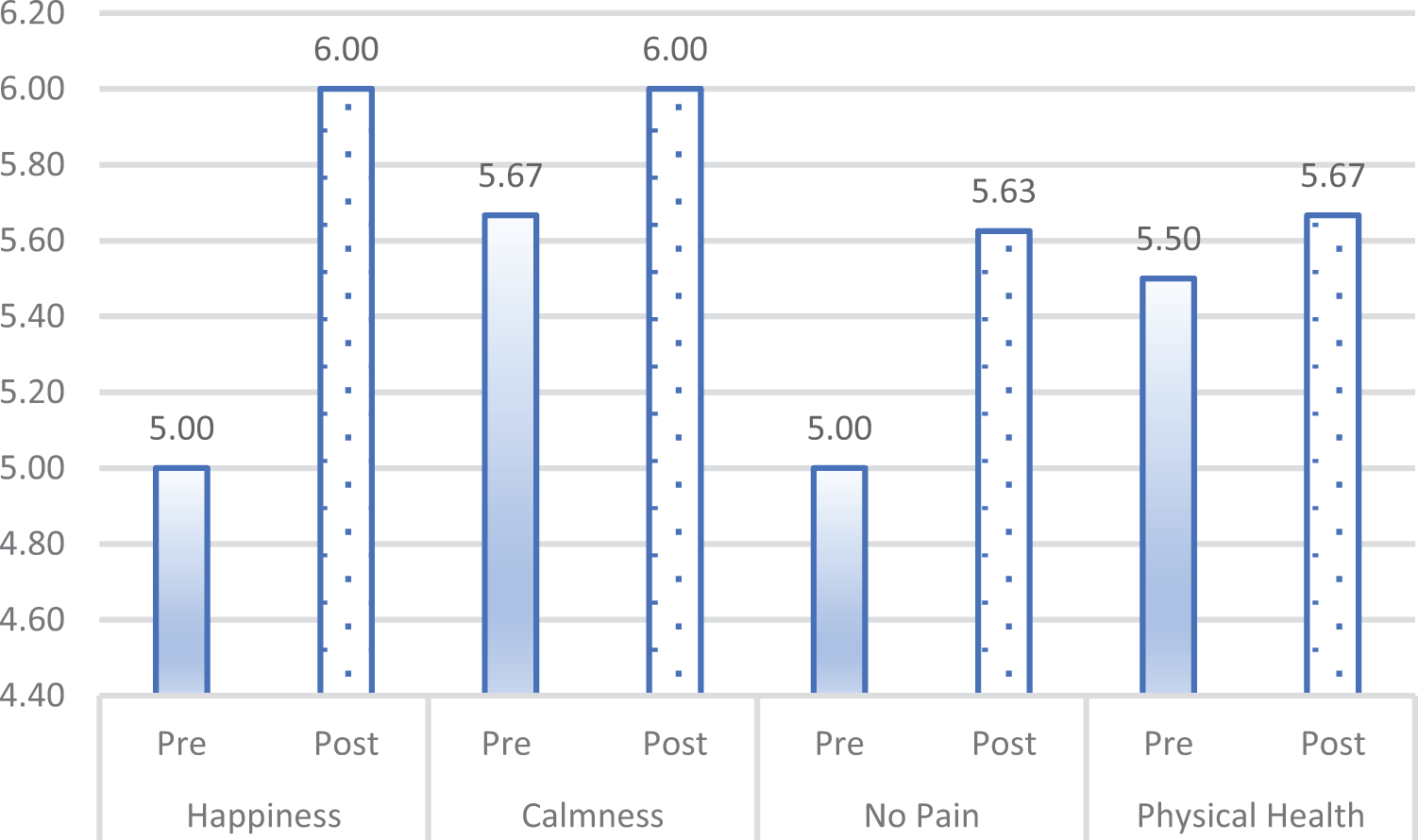
Median pre- and postart session feeling scores.
Impact on Anxiety Symptoms, MPR, and PPRE
Table 4 includes descriptive statistics and p values from Mann Whitney U tests undertaken to establish whether significant differences between groups existed across the three outcome measures utilized throughout T1 and T2 surveys, while Figures 5 and 6 illustrate pre- and postmean values for each MPR and PPRE item, for Groups 1 and 2.
Descriptive statistics and p Values From Mann Whitney U Tests.

T1 values for PPRE, MPR, and anxiety symptoms between groups were not significantly different, indicative of groups having similar feelings/perceptions across these domains. MPR slightly improved for those who participated in the recreational art program (T2 mean value of 22.21 vs. T1 mean value of 20.36) and motivation slightly declined for those who did not participate in the program (T2 mean value of 20.43 vs. T1 mean value of 20.90). Difference scores between both groups were not significantly different (Mann Whitney U = 93.00, p = .071), indicative of the changes between groups not being significantly different (however they did trend toward being significantly different). As illustrated within Figure 5, compared to T1 item mean values, T2 item mean values for Group 1 generally increased (for four of the five items), indicative of this group having improved motivation, while T2 item mean values generally declined for Group 2 (for three of the five items), indicative of this group experiencing a reduction in motivation.
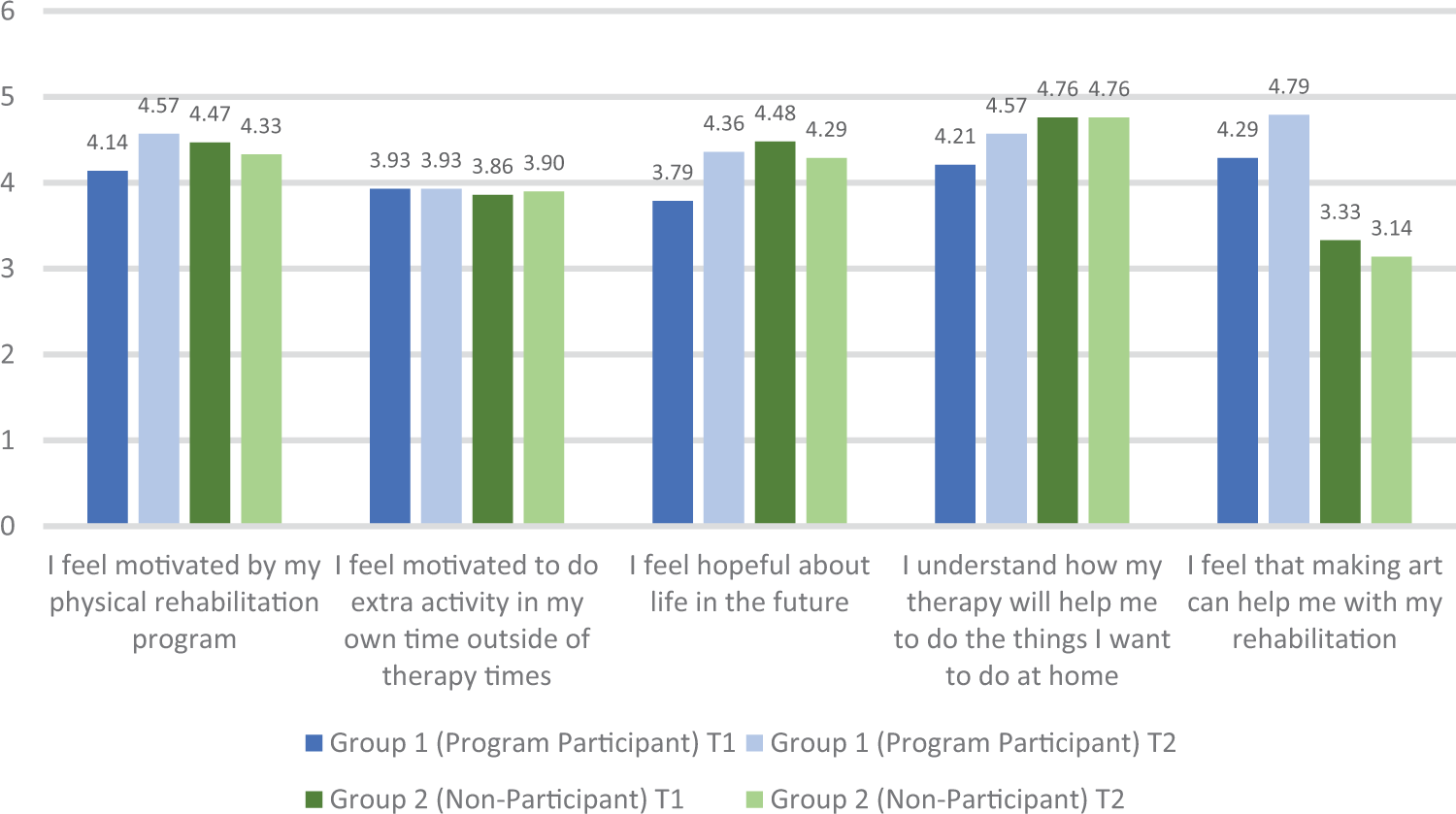
Motivation to participate in rehabilitation T1 and T2 item mean values for each group.
PPRE slightly improved for those who participated in the recreational art program (T2 mean value of 13.00 vs. T1 mean value of 11.50) and slightly declined for those who did not participate in the program (T2 mean value of 12.86 vs. T1 mean value of 12.47). Difference scores between both groups were not significantly different (Mann Whitney U = 102.50, p = .135), indicative of the changes not being significantly different between groups. As illustrated within Figure 6, compared to T1 item mean values, T2 item mean values for Group 1 generally increased (for all three items), indicative of this group having improved PPRE, while T2 item mean values marginally declined for Group 2 (all three items), indicative of this group having worsened perception of the rehabilitation environment.
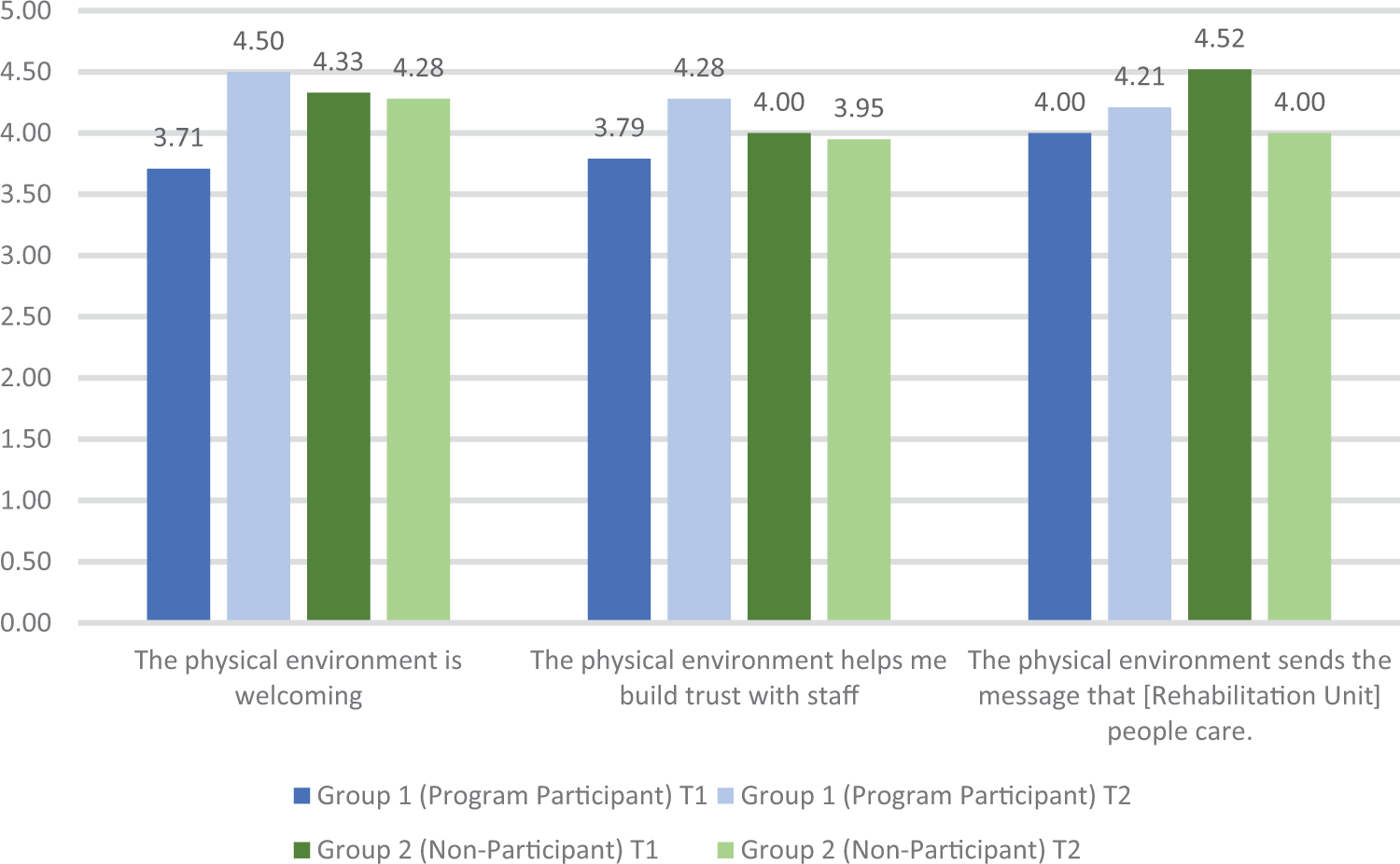
Perception of the physical rehabilitation environment T1 and T2 item mean values for each group.
For both groups, compared to T1, T2 GAD-7 scores decreased, indicative of participants across both groups having lesser anxiety symptoms approaching discharge. The changes in scores were not significantly different between groups (Mann Whitney U = 142.50, p = .881). Spearman’s rank-order correlations investigated whether a relationship between MPR, PPRE, and anxiety symptoms existed. Correlational coefficients (Spearman’s ρ) and p values have been included in Table 5. As clarified, T1 values of MPR and PPRE were significantly positively correlated, indicating that higher levels of initial motivation and having a favorable initial perception of the environment were associated. Similarly, difference scores were also positively correlated, indicating that improvements in motivation and an improved perception of the environment were also associated.
Correlational Matrix for Perception of the Physical Environment, Motivation to Participate in Rehabilitation, and Anxiety Symptoms.

Note. MPR = motivation to participate in rehabilitation; PPRE = perception of the physical rehabilitation environment; GAD-7 = General Anxiety and Depression Questionnaire-7.
* Correlation is significant at the .05 level (two-tailed).
** Correlation is significant at the .01 level (two-tailed).
Discussion
Preliminary findings confirm that participating in a recreational art creation program with the aim of developing an art installation which will be implemented in hospital has a significant impact on immediate levels of calmness, happiness, pain, and physical health of people who are receiving rehabilitation. Compared to levels measured prior to sessions, self-reported calmness, happiness, pain, and physical health of participants significantly improved after each session. The findings suggest that involving inpatients in therapeutic activities which aim to address the physical environment of the health setting where they receive support can provide therapeutic benefits while simultaneously involving them in healthcare physical environment design and decision making.
A methodology that aims to assess the impact of employing an art installation made by end users within the corridors of a rehabilitation unit has been provided. The design is rigorous as it includes control (Period 1 participants) and intervention (Period 2 participants) groups. Tests for significant differences in perception of the physical environment will confirm whether the art installation has an impact on participants’ perspectives of the environment. The distinct impact of the art installation will be established, as there is expected to be no other changes to the physical environment during the time period. The findings will clarify whether the revised environment including artwork developed by end users is perceived as promoting a welcoming environment, indicative of caring staff, and promoting trust between patients and staff.
The overarching two-period methodology could be employed for similar projects which aim to involve end users in therapeutic activities to address the hospital physical environment. For example, the methodology could test the impact of engaging participants in woodwork or woodcraft activities, with the aim of developing furniture for the environment, or gardening activities with the aim of improving the natural environment, on the immediate feelings of inpatients and their perspectives of the physical environment. The proposed approach fills a methodological void in research around patient perspectives of hospital or healthcare environments, which have largely investigated inpatient and/or staff perspectives (Douglas & Douglas, 2004; Kotzer et al., 2011; Xuan et al., 2021) or researcher observations of patient use (Colley & Zeeman, 2020). Such research has been valuable and highlighted domains which support (i) health service provision, (ii) promote patient safety, and (iii) are associated with patient health and well-being outcomes. However, research to date has not confirmed which elements within the environment have a causal influence on patient health and well-being. Furthermore, research has yet to investigate the impact of participant engagement in activities which aim to contribute to the physical characteristics of the hospital environment. The design proposed addresses these gaps and can be employed to confirm findings from research to date.
Findings also confirmed that there is a relationship between MPR and PPRE. Correlational findings confirmed that having an initial favorable perception of the physical environment is associated with a higher initial level of rehabilitation motivation. Changes across both domains are also associated, where an improved perception of the environment is associated with improvements in motivation. The findings are novel and add to research to date which has confirmed that aspects of physical healthcare environments are associated with mood outcomes (Goto et al., 2013; Laursen et al., 2014). The findings confirm that a physical environment which is perceived as welcoming, indicative of caring staff, and building trust between patients and staff can contribute to improved motivation for inpatients receiving rehabilitation. There is the potential that this increased motivation could contribute to greater improvements in functional rehabilitation outcomes and transition to the community. (Longitudinal studies will need to confirm if this is the case.) Regardless, the findings provide preliminary evidence in support of healthcare design decisions which prioritize features fostering welcoming and supportive environments.
Two measures valid for people receiving rehabilitation in hospital were developed as a part of this study: MPR and PPRE. The measures included five and three items, respectively, and factor loadings and measures of internal consistency suggest that they accurately measure the constructs they aimed to address. There is an absence of measures focusing on rehabilitation motivation and the perceptions that people receiving neurorehabilitation have of their physical healthcare environment. Given the distinct health consequences resulting from the onset of neurological disability and/or experiencing a traumatic injury, specific measures that are intelligible to end users are required. It is expected that the proposed measures can be used in further studies investigating perceptions that people receiving rehabilitation have around their physical environment and rehabilitation motivation.
Sensory stimulation—generally understood as a process and/or intervention where environmental stimuli are utilized to arouse the senses (Grieve, 2007)—may promote favorable rehabilitation outcomes for people who experienced a traumatic injury. Such stimulation involves activating auditory, kinesthetic, tactile, olfactory, and/or visual senses (Grieve, 2007). Creative practices are a form of sensory stimulation (albeit many involve patients participating in art creation rather than a form of stimulation facilitated by a health professional) which can stimulate neuropathways and promote neuroplasticity (Dieterich-Hartwell, 2017). This is especially important for people who have experienced a neurological injury. The recreational art program evaluated as a part of this study, and comparable programs, may have specific value to people who have experienced neurological injury, as visual art is a kinesthetic targeting strategy involving slow, coordinated, and mindful movements which can promote neuroplasticity (Doidge, 2016) and perhaps contribute to favorable physical rehabilitation outcomes. Furthermore, the creation of art can assist in addressing the trauma which at times accompanies a neurological injury (Jones et al., 2019) and thus promote psychological health. For these reasons, the program evaluated may have particular relevance to people receiving neurorehabilitation.
The study has limitations which are important to consider. The between groups component of the study tested for significant differences between those who participated in a recreational art program (Group 1) and those who did not (Group 2). These groups were not identical, and those who participated in the art program were in hospital significantly longer and had significantly poorer functional motor skills on admission. Inferential analysis did not yield significant differences in outcomes between groups; however, when compared to Group 2, descriptive findings suggest that Group 1 experienced improvements across motivation domains and an improved perception of the physical environment. These improvements may be due to Group 1 being in hospital longer and/or being motivated by experiencing increased functional gains. Future studies should consider a larger sample where both groups are comparable (perhaps by assigning people to groups based on functional level and estimated length of stay) and consider additional factors which may contribute to the domains measured (e.g., extent of family support in hospital and engagement in leisure activities). Regardless, as significant differences in T1 MPR, PPRE and GAD-7 scores between groups were not apparent, the authors are of the opinion that the groups are comparable under the context of the key outcomes included within this study, thus making the findings reliable.
Conclusion
People receiving healthcare should be actively involved in healthcare environment design. This is especially important for people with disability who may be excluded from such decisions. Including their perspectives is a human right and contributes to health service equity. The study and methodology proposed provide a framework to evaluate the therapeutic impact of interventions and/or activities which aim to amend the physical health service environment and evaluate the impact of environmental changes. It is expected that this methodology and underpinning research can encourage further work which involves end users in the design of health environments and evaluate the impact of their involvement.
Implications for Practice
– The two-period methodology presented could be employed to assess projects which aim to involve end users in therapeutic activities that address the hospital physical environment.
– Involving inpatients in therapeutic activities which aim to address the physical environment can provide therapeutic benefits while simultaneously involving them in healthcare physical environment decision making.
– Designing environments as welcoming can promote rehabilitation participation among people who have a neurological disability.
Footnotes
Acknowledgments
Dr. Ali Lakhani would like to acknowledge that the work of Dr. Jacinta Colley, Professor Heidi Zeeman, and Professor Elizabeth Kendall around hospital rehabilitation unit design has in part encouraged this work. Furthermore, Dr. Ali Lakhani would like to thank Professor Heidi Zeeman for providing consistent mentorship in this research area and Dr. Peter Grimbeek for consistent statistical advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a La Trobe University, College of Science, Health and Engineering Start-Up Grant.