
Abstract
Objective:
This article aims to investigate the impact of fine-grained differences in unit layout on care staff corridor communication.
Background:
Corridor design can be undertaken with greater emphasis on space and cost efficiency or with greater emphasis on affording quality knowledge workspace. Building on prior research on care team communication and inpatient unit design, this study aims to gain a better understanding of how corridor layout properties affect care team communication.
Method:
This study used space syntax analysis to characterize inpatient unit design, specifically floor-plan layout. Two approaches were used to capture care team communication: behavior mapping with recording of care team member locations and whether they were communicating and the HDR CARE Scale, Inpatient Version. The two units were part of a vertical tower expansion project, and, though constructed at separate times, they maintain the same organizational culture, floor plate, and location of key vertical elements.
Results:
The newer unit was found to be more visually open using three measures from space syntax. More nursing staff verbal communication was observed on this unit. Across both units, nursing staff were more likely to be observed verbally communicating in locations that were more visually connected (i.e., at locations with larger viewsheds). There were no significant differences between nursing staff self-report on work using the HDR CARE Scale, Inpatient Version.
Conclusion:
We conclude that care team communication may tend to be encouraged by visual connectivity that can be promoted through floor-plan layout.
Inpatient care staff communication has been characterized both as a source of annoyance to patients, staff, and visitors (e.g., Cordova et al., 2013) and as a valuable form of knowledge sharing (Carthey, 2008) that ultimately protects patients from harm. The purpose of this article is to investigate the impact of fine-grained differences in unit layout on care staff corridor communication. Specifically, this postoccupancy evaluation describes and compares two nursing units that have identical floor plates and organizational background variables but house different acuity-level patients and have subtly different floor-plan layouts, mainly at the core and team stations along the corridors. Three kinds of information are gathered and compared in the assessment: the visual openness of each unit, locations of care staff in unit corridors and whether they are verbally interacting, and care team assessments of how well the designed environment supports their work, especially for situation awareness, coworker interaction, getting help, and monitoring patients.
The potential implications of the study may improve understanding of the role and function of inpatient unit corridors and enhance understanding of how they should be designed. As hospitals face economic pressure to “right-size” facilities, it is important to understand whether unit corridors serve primarily to link spaces and thus should be designed with an eye toward size and cost efficiency. Alternatively, their perceptual and social functions may impact care teams in ways that warrant consideration in corridor design.
Background
Care Team Communication
Communication lapses are a root cause of many failures to protect patient safety, and strong and varied communication skills characterize successful nurse work (Apker et al., 2006). While the physical environment has been implicated as an obstacle to nursing care (Gurses & Carayon, 2007), research has established the importance of inpatient unit layout to care team communication (e.g., Kalisch & Begeny, 2005; Real et al., 2017).
Research studies from nursing, communication, and design indicate that care teamwork appears to be encouraged by the proximity and intervisibility of care team members to one another (Doede et al., 2018; Gharaveiset al., 2018; Gunn et al., 2015; Kalisch et al., 2013; Peavey & Cai, 2018). Corridors are recognized as potential key spaces for care team communication, with some commentators noting the potential of corridors to act as a mixing space of a uniquely egalitarian nature (Carthey, 2008; Iedema et al., 2010).
Space Syntax
This study uses space syntax methods to provide precise, quantitative measures of floor-plan layout attributes that allow us to measure conditions that are more or less conductive to proximity and intervisibility in inpatient unit settings. Space syntax is a set of theories and measures aimed at uncovering social dimensions of space (Bafna, 2003; Hillier & Hanson, 1984; Zook & Sailer, 2022), including in hospital spaces (Rafiq & Mustafa, 2021). A space syntax study of an intensive care unit (ICU) by Cai and Zimring (2012) linked the integration of assigned nurse workstations to patterns of nurse co-awareness. Other studies have found the size and properties of the viewsheds on various inpatient units to affect inpatient care processes and outcomes (Lu & Zimring, 2011; Ossmann, 2022; Ossmann et al., 2019; Pachilova & Sailer, 2020). Ossmann (2022) and Pachilova and Sailer (2022) have developed middle-range theory indicating that inpatient units with larger viewsheds support care quality and safety, possibly by promoting concurrent visual connections to both patients and care team colleagues, to at once enable patient surveillance and teamwork. The present study focuses directly on nursing staff, mostly registered nurses (RNs) and patient care assistants (PCAs), specifically observing where they communicate in inpatient unit corridors and how they evaluate the environments in which they work.
Care Team Member Assessments and Use of Their Own Environments
Postoccupancy evaluations commonly collect user assessments of how well their environment serves various purposes. Many architecture firms use their own instruments for such evaluations, sometimes customizing them for particular end-user concerns. The strength of such bespoke instruments lies in their specificity, which can allow designers to make needed changes, fine-tune their strategies, or demonstrate success to clients. However, bespoke instruments come at some cost to general knowledge because few such tools are validated, used across firms, or reported out using standardized measures, all of which hamper potential cross-case comparisons and long-term learning at the level of the profession. This study uses the validated HDR Clinical Activities Related to the Environment (CARE) Scale, Inpatient Version (Rich et al., 2021) to assess care team satisfaction with a range of functions and to describe correspondences with layout and behavior mapping data. This 9-item scale was developed for care staff, specifically nurses, to assess environmental affordances for efficient and effective work and was developed using a rigorous validation process as described by Rich and colleagues (2021).
This study aims to explore the issue of design and care team communication by focusing on the visibility properties of the floor-plan layout and on care team communication that occurs in unit corridors, including the spaces that are continuous with the corridor, such as team and decentralized nurse stations, and hallways that traverse the unit core. We compare viewshed sizes between two unit floor-plan layouts, testing for significant differences.
We then observe and report the locations that care staff occupy in corridors, noting whether they are engaged in verbal communication. We are particularly interested in whether the locations observed as hosting talking within the unit corridor system are characterized by larger viewsheds compared to locations recorded for care team members who are engaged in activities other than communication, following the literature cited above.
Prior research warrants looking at specific visibility conditions related to communication. In an empirical study, Lu and Zimring (2011) observed nurse locations as care team members engaged in various tasks (e.g., charting, medication administration). The authors characterize nurse conversation, as distinct from other care tasks (e.g., dispensing medications), as relatively portable, and thus they present aggregate patterns of communication locations as reflecting a degree of choice. Comparing the visibility properties of locations of care staff who are communicating versus those engaged in other activities can thus be taken to reflect, in aggregate, some degree of preference about locations for communication.
A novel aspect of this study is the direct querying of the care team assessments of space using a validated instrument. Care team responses to the HDR CARE Scale are expected to be of interest in their own right but also may correspond to or contradict the data gained by the other methods. Knowledge gained from these multiple data streams is expected to provide insights regarding functionally appropriate layout principles for unit corridor systems, specifically regarding the potential implications of designing and constructing inpatient units that are more visually open or more visually enclosed.
In sum, this study investigates the following: Whether there are differences in visual openness between the two units using precise, quantitative measures. Whether care team communication in corridors will occur more in locations with larger viewsheds compared to locations for care team members who are observed in corridors but are not talking. Whether items on the HDR CARE Scale that can be expected to be supported by visual connections will be rated more highly on the unit with greater overall visibility, greater patient visibility, and greater nurse station visibility. These specific scale items are related to (1) knowing what is going on, (2) interacting with coworkers, (3) getting help, and (4) monitoring patients.
Method
The method for this study was approved by Institutional Review Boards at Texas Tech University and Indiana University (IU).
Background and Description of the Facility and the Two Units
IU Health West Hospital is a community hospital campus located in Avon, IN, a suburb of Indianapolis. It is part of the Indianapolis Suburban Region of the IU Health system. IU Health West Hospital was originally constructed in 2004, and in 2017, it commenced the vertical expansion of one inpatient tower, adding a new floor, designed to be fully acuity adaptable, with 32 additional inpatient beds. This new inpatient floor, an acuity adaptable unit (AAU), sits directly above the existing inpatient floor, a medical–surgical unit (MSU), utilizing a stacked approach to patient rooms, infrastructure, and systems. With this approach, the floor plates were identical for each unit, which allowed the design team to explore the impact of changes within the unit core. The existing 32-bed unit was designed with one main, centralized care team station, a very small team station, and a decentralized care team station at each patient room. During the design process, project workshops uncovered anecdotal comments that the staff felt isolated during their shifts and wanted to feel more connected. The design of the new 32-bed unit resulted in four large, centralized care team stations with additional decentralized stations. This project provided the opportunity for a natural experiment to better understand how differences in the corridor and core layout affect patterns of care staff work.
Both the AAU and MSU are adult general units in a clinical hospital. All patient rooms on the two units are acuity adaptable and are basically similar. In this facility, the AAU admits both progressive and medical–surgical patients, while the MSU serves exclusively medical–surgical patients. The staffing ratio on the AAU is 4:1 (nurse-to-patient) with a round-the-clock cardiac monitor technician and an admission discharge transport RN. Ratios on the MSU are typically 5:1 on the day shift and 6:1 on the night shift.
The MSU has corridor-side windows to patient rooms with blinds that typically stay closed, except as needed to reduce the risk of patient harm (e.g., falls). The AAU uses the same privacy and safety practices. It has windows in the patient room doors and to the eight patient rooms that are located along the short corridors that extend from the corners of the unit. All patient rooms have decentralized stations nearby; these are generally two-seat stations in the MSU and single-seat stations in the AAU.
In terms of communication, staff use mobile communication devices. They have fixed workstations at team and decentralized stations on both units. The number and type of other team work areas (e.g., dictation rooms) are comparable across units, with the additional staff corridor through the core of the AAU used as a huddle space. The staff-oriented corridor through the core has also been observed to enable more open-door use of collaboration spaces, such as dictation rooms. The newer AAU had been in operation for over 2 years at the time of data collection. Staffing mix and experience and patient census for each of the observation days are reported in the Method section.
Space Syntax Measures
Two kinds of measures from space syntax floor-plan analysis are used to capture unit visibility: viewshed size and isovist connectivity. Viewshed size (technically, visibility graph analysis connectivity based on the isovist, Benedikt, 1979) measures the size of the 360-degree view for each point on a grid that covers the floor plan (technically, centroids of cells in a grid). For this analysis, the grid spacing is one foot and the viewshed sizes are reported in square feet. Space syntax analysis is usually relational in the sense that the properties of any specific location are always defined with respect to other locations in a spatial system. Although behavior is observed in the corridors only, space syntax analysis is undertaken for the continuous space of the unit floor plan, excluding chases, public bathrooms, stairwells, and structural elements or fixed furniture that are taller 5′0″. Comparing viewshed sizes between units captures their relative visual openness (see Figure 1).
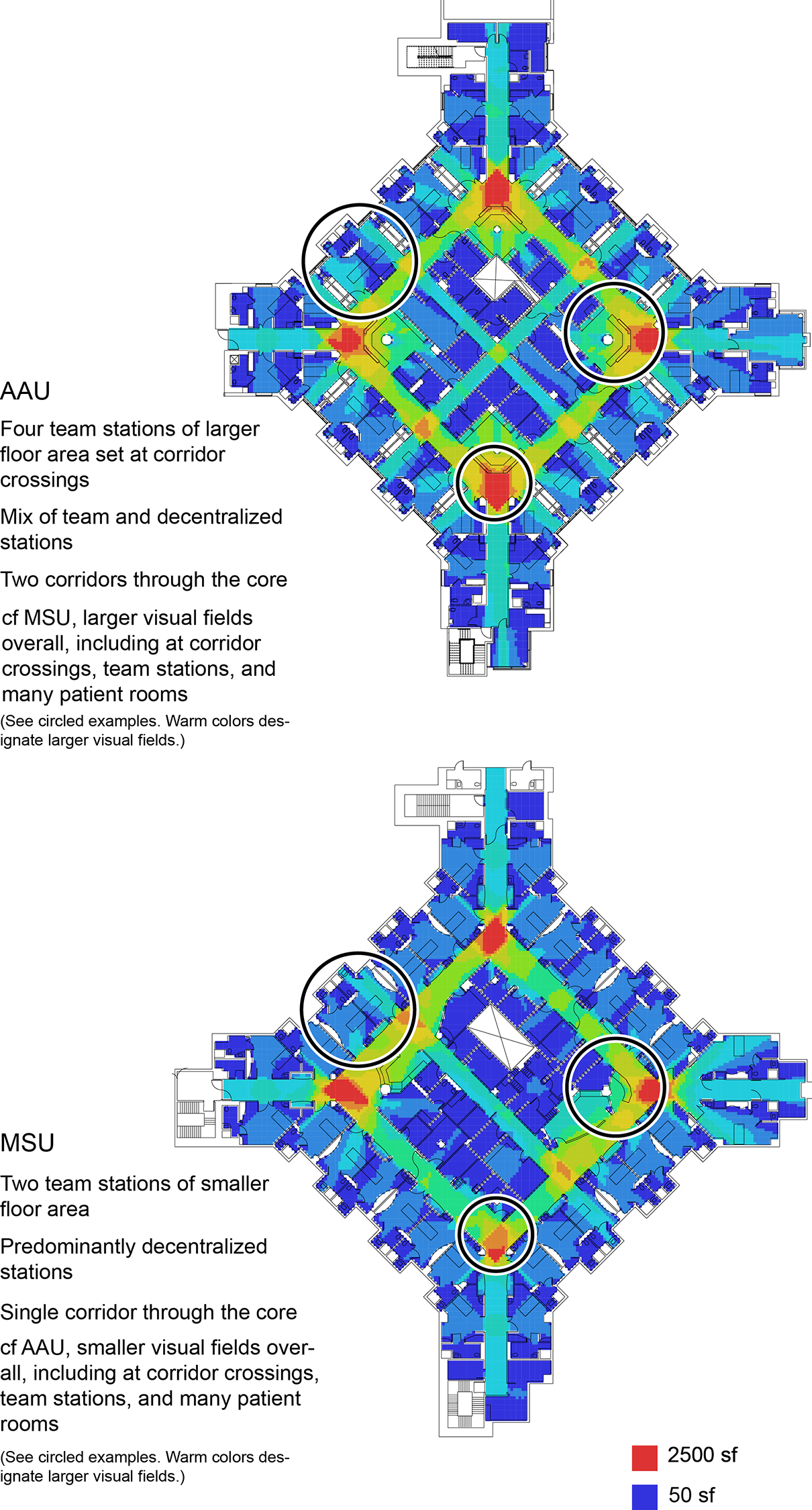
Two units in a vertical tower expansion: the same footprint and highly similar patient rooms but distinct corridor and core design.
The second measure, isovist connectivity, was taken for all patient heads-of-bed and for all nurse stations. Isovist connectivity was developed by Ossmann (2016, 2019, 2022) to capture the capacity for ICU nursing staff to surveil their patients while simultaneously staying visually connected to the unit at large. Isovist connectivity can be imagined as the sum of viewsheds built atop an originating viewshed. In Ossmann’s study, for example, she initially mapped the area visible from the patient head-of-bed as the originating viewshed. She then mapped all of the areas visible from this originating viewshed. The average of these areas is equal to the isovist connectivity of the patient head-of-bed in question. Such a measure allows us to assess the degree to which the initial viewshed reaches into the larger environment, in this case, the corridor system. A conceptual diagram of isovist connectivity appears in Figure 2. For this study, isovist connectivity is calculated and averaged on a per-unit basis for patient rooms and for nurse stations. Decentralized and team stations are pooled for purposes of the isovist connectivity analysis as they jointly act as a system of locations for care team work.

Isovist connectivity characterizes how robustly a location is visually integrated into the floor-plan layout.
For ICU heads-of-bed, published isovist connectivity ICU averages for patient heads-of-bed in square feet range from 618 to 1,333 sf (Ossman, 2016). For doctor workstations in emergency departments, isovist connectivity values in square feet range from 512 to 1,589 sf (Joshi et al., 2023).
The space syntax measure integration, especially of nurse stations, is cited elsewhere as associated with positive conditions for care activities (Cai & Zimring, 2012; Choi, 2011; Zook et al., 2019). However, the prior studies compared units with categorically different layout types, while this study looks at two instances of a basically similar layout with differences that may be too subtle to be reflected by integration values. In the preliminary analysis, integration values were nearly identical for each unit corridor system, as well as for team and decentralized nurse stations, and no additional integration analyses were conducted (see Table 1).
Integration Values for Two Inpatient Units.

a Integration is calculated here as the reciprocal value of mean depth (Hillier & Hanson, 1984); higher values refer to greater integration.
Behavior Mapping
Behavior mapping consists of the nonobtrusive recording of locations and behaviors of users in a given setting (Barker, 1976). In this study, a single investigator walked a predetermined route through each unit marking the location of all care staff on a floor plan when they passed or were passed by the investigator’s coronal plane. If the care staff was speaking (not via phone or other device) at the time the researcher passed by the individual, the individual was recorded as engaging in communication; if not, only the location of the individual was recorded. No communication contents or individual identities were recorded. Thirty-two behavior mapping sessions (16 per unit) were conducted over 2 weekdays and spanned the 7 a.m. to 7 p.m. shift. The researcher alternated between units at scheduled intervals, reversing the pattern on the second day. The end-of-day shift change was observed on both units. Coordinate locations were recorded for each observation and were matched with visibility graph analysis connectivity values associated with the same coordinates generated from DepthmapX (DepthmapX Development Team, 2017). Two sample behavior maps of locations are shown in Figure 3.

Two rounds of behavior mapping were conducted at around 12 p.m. in each unit.
Validated Survey
To capture care team evaluations of design support for inpatient work, licensed and unlicensed nursing personnel working on two inpatient units completed the HDR Clinical Activities Related to the Environment (CARE) Scale Inpatient Version. Additional questions were included on employment characteristics, including experience.
The HDR CARE Scale was delivered using two methods. One was via email with a direct link to the survey using Microsoft Forms. The other method was a printed survey that was made available to the care staff on both units participating in the research. The completed paper surveys were input into Microsoft Forms. Reminders occurred daily until a 60% response rate was achieved.
Results
Comparing Measures of Built Environment With Space Syntax
Visibility (viewshed size)
In comparing viewshed size between units, an unpooled two-sample t-test assuming unequal variances showed that the AAU had statistically significant larger viewsheds (M = 699; SD = 585) on the whole than the MSU (M = 608; SD = 531; for Welch’s test, F 254, 1 = 15.9, p < .0001).
Isovist connectivity of patient heads-of-bed
Though the patient room isovist connectivity data for each unit appeared to be roughly normally distributed, variances were found to be unequal. Therefore, in analyzing the head-of-bed isovist connectivity for each unit, an unpooled two-sample t-test assuming unequal variances was used. It showed that the AAU had greater isovist connectivity values at heads-of-bed (M = 825; SD = 318) than the MSU (M = 729; SD = 289; for Welch’s test, F 10, 1 = 3.11, p = .0027), though the difference was not statistically significant. These values are toward the low end of the range of unit averages identified by Ossmann (from 618 sf to 1,333 sf), although Ossmann studied purpose-built ICUs, which can be expected to be designed for greater visual openness.
Isovist connectivity of nurse stations
Though the nurse station isovist connectivity data for each unit appeared to be roughly normally distributed, variances were found to be unequal. An unpooled two-sample t-test assuming unequal variances showed that the system of team and decentralized nurse stations on the AAU had larger isovist connectivity values (M = 1,280; SD = 220) than the MSU (M = 1,269; SD = 189), though the difference was not statistically significant. A summary of visibility values is shown in Table 2. These nurse station isovist connectivity values track with the higher end of (1,589 sf) of doctor workstations identified by Joshi and colleagues (2023).
Visibility Values for Two Inpatient Units.

*p < .0001.
Comparing Where Care Team Members Communicate Using Behavior Mapping
Both units were staffed mostly by RNs, followed by PCAs, and included additional healthcare workers, such as sitters, unit secretaries, monitor technicians, and respiratory therapists (see Table 3). In comparing the two units, more staff were observed on the MSU (353 total observations) than on the AAU (324 total observations). However, the AAU nevertheless hosted a greater proportion of talking as observed, with 33% of care staff observed talking on the MSU and 46% observed on the AAU. It should be noted that the AAU has a larger and more occupationally diverse team with higher acuity patients (see Table 3).
Staffing and Census on Observation Days.

Note. RN = registered nurses; PCA = patient care assistant.
We further compared the viewshed size at locations where care team staff were observed talking and locations where care team staff were observed but were not talking. When we pooled the data from the two units and ran a logistic regression analysis, there was a whole-model statistically significant association between larger visibility and likelihood of talking (p = .0081). When we evaluated each unit individually, the association remained but was not statistically significant for either the MSU (p = .1465) or the AAU (p = .4760).
Comparing Responses to the HDR CARE Scale Inpatient Version
Forty-four of 73 possible respondents on the AAU completed the survey (60%), and 40 of 67 completed the survey on the MSU (60%). Nine surveys (four from the AAU and five from the MSU) were discarded for not completing one or more of the nine main items. For survey respondents on both units, the most common duration of working in one’s present role was 1–2 years. The AAU had a greater share of care staff in their role for less than 2 years (see Figure 4).

Both units skew toward new professionals, especially the acuity adaptable unit.
We report results for the following survey items that are expected to be impacted by visual connectedness:
How much effort does it typically take to know what is happening with my coworkers during my shift?
How much effort does it typically take to get help as soon as I need it?
How much effort does it typically take to frequently interact with my coworkers during my shift?
How much effort does it typically take visually monitor patients without disturbing them?
Because staff communication can act both as an aid to knowledge work and as a nuisance, we also report on an item wherein the care team member evaluates their overall sense of effort to achieve quality patient care:
How much effort does it typically take to provide high-quality care?
We constructed contingency tables to report on the survey data. No differences in patterns of response categories between units were statistically significant. “Requires little effort” was the most frequent answer for both units for “know what is happening with my coworkers,” “frequently interact with my coworkers,” and “visually monitor patients without disturbing them.” For two items, the most frequent response for the AAU represented a greater challenge than for the MSU. The most frequent response for “get help as soon as I need it” was “requires moderate effort,” while for the MSU, the most frequent response was “requires little effort.” Similarly, the most frequent AAU response for “able to provide quality care” was “requires much effort,” while for the MSU, the most frequent response was “requires moderate effort” (see Table 4).
HDR CARE Scale, Inpatient Version.

Note. Bolded items are modal (most frequent) responses.
Discussion
There were notable differences in viewshed size and visual connections between the two units, with the AAU being characterized by larger viewsheds and more robust visual links from patient heads-of-bed and nurse stations to the unit at large.
Across both units, care team communication was more likely to be observed in corridor locations with larger viewsheds compared to the viewshed sizes of locations for care team members who were using corridor space for other activities. Communication was observed to occur more frequently on the AAU.
Items on the HDR CARE Scale Inpatient Version that we expected to be rated more favorably on the higher visibility unit, the AAU, were mostly rated similarly and sometimes slightly less favorably compared to the lower visibility MSU.
This pattern of findings is summarized in Table 5.
Summary of Key Data.

a Mean depth (Hillier & Hanson, 1984) is the integration measure shown.
*p <. 0001.
This study analyzed the impact of relatively subtle differences in floor-plan layout on care team communication. High-visibility locations were associated with more likelihood of communication based on a statistical analysis of the behavior mapping data. The association of visual connectivity to care team communication is consistent with prior theory and empirical research (Cai & Zimring, 2012; Carthey, 2008; Lu & Zimring, 2011; Pachilova, & Sailer, 2020). The contradiction is that survey respondents from the more visually open AAU did not more favorably rate dimensions of work that would seem to depend on seeing one’s colleagues and patients. Observational data indicate that care staff may be sensitive to viewshed size for task locations, especially communication, while survey data does not necessarily bear out the significance of viewshed conditions on care staff evaluations of their inpatient work environment.
There are several possible explanations. We should first note that no survey response differences between units gained statistical significance because differences were small enough that they may have been due to chance. There is also a recognized tendency toward discrepancies between behaviors as observed and behaviors as self-reported, in part because observed performance assesses behavior under specific and definite circumstances, while self-reports gather reflections about a generalized and self-conscious sense of one’s performance (Dang et al., 2020). In terms of the impact of operations, we might consider the effect of care acuity. The AAU is a higher acuity environment, and the greater sense of challenge conveyed by AAU staff may derive from the more complex care they provide. The specific items that were slightly lower ranked by the AAU staff related to the effort needed for getting help right away and for providing quality care. The AAU patients by definition require more effort to provide care for. Potentially, the effort needed to get help right away may be affected by AAU care staff having greater obligations at bedside and thus being less available for instantaneous response to other members of the care team. Finally, the survey respondent characteristics reflect that while both units lean heavily toward new professionals, the AAU staff is predominantly new professionals. The prevalence of new professionals may generally increase workplace challenges. At the same time, this cohort may also stand to especially benefit from covisiblity to support tacit learning (Cai & Zimring, 2012). This article is, to the authors’ knowledge, the first published study to use the HDR CARE Scale (inpatient version), and future research publications may retroactively illuminate these findings.
While larger viewsheds appear to support conditions for care team communication, this phenomenon may play out differently under different conditions of acuity. Frequent care staff communication is fundamentally necessary in complex patient care. In lower acuity settings, less frequent communication may not only be adequate for the task at hand but also indicative that focus and work completion are well-accommodated. Locations that provide large viewsheds can be argued to afford better capacity to surveil while communicating. A potential reason for staff to position themselves in such spaces may be so that they can talk and simultaneously keep an eye on things. On the whole, we might infer that both operational aspects related to acuity and staffing and architectural aspects related to viewsheds and visual connections drive how members of the care team use and evaluate their workspace.
The cross-sectional nature of this study precludes causal inference. While the study associates larger viewsheds with a degree of support for care team communication, one limitation of the method is that it does not include a way to investigate either the potential nuisance or the potential social and clinical value of communication. In a separate study, the authors undertake a social network analysis of care team communication in these two units to better understand the structural features of care team communication. While there was a consistent association of locations of larger viewshed size with communication, the association only gained statistical significance when all observations were pooled, indicating a need for larger, better-powered studies to get a better sense of whether the effects replicate and, if so, what their magnitude may be. In a natural experiment, not all variables can be controlled. Greater communication may have been driven to some degree by higher acuity, newer professionals, and the involvement of more kinds of care professionals, among other potential factors.
Conclusion
Corridor space is a prime care team work space that warrants attention and consideration above and beyond its role in enabling connections between the parts of the program. This study lends support to the idea that more visually open corridors may contribute to care team communication. Building occupants can always, to some degree, overcome barriers to communication, but, in hospitals, the energy spent doing so may come at a cost to care team morale as well as to the quality and safety of patient care. Indeed, prior research has demonstrated subtle patterns of visibility register at the level of things as weighty as ICU survival (Leaf et al, 2010; Ossmann 2022).
One strength of using quantitative floor-plan analysis is that it enables specific design recommendations. This study demonstrated that a more generously sized corridor system can visually bind an inpatient unit together, making the patient heads-of-bed and the system of nurse stations more perceptually accessible. Pachilova and Sailer (2022) have noted that providing larger views for care teams can be achieved by such strategies as creating larger “clearings” in front of team nurse stations, creating larger team nurse station seating/work areas, and providing wider corridors. The analysis in this study also indicates that routing corridors through the core also creates greater visual openness.
Design alone does not determine the function of the care team work environment, especially when compared to the aspects of organizational culture recognized in the nursing literature, like qualifications; such variables lie beyond the control of the design team. There is nevertheless something in it for designers to better understand the ripple effects of layout decisions on the ecology of inpatient units, something that might enable better care of the care providers.
Implications for Practice
More visually connected inpatient units may promote communication among nursing staff.
Inpatient units corridors should be conceptualized and designed as key knowledge workspaces, and not just as spaces whose only value is that they connect one space to another.
Greater visual connections in inpatient units can be achieved by floor-plan layout strategies that create wider corridors, corridors through the unit core, and wider clear spaces at team nurse stations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a research grant from BSA LifeStructures to Texas Tech University.