
Abstract
Background:
Energy insecurity, the inability of households to meet their basic energy needs, can exacerbate adverse health conditions in residents of those households. This is a critical issue for many Maricopa County neighborhoods with high rates of heat-associated mortality.
Methods:
In 2021, the Maricopa County Department of Public Health and community partners launched a survey in a South Phoenix community (zip codes 85040, 85041, and 85042) aimed at examining the relationship between household energy burdens and demographic and physical housing characteristics. Chi-square and Fisher’s exact tests were used to examine sociodemographic and health correlates of energy burden.
Results:
Out of 145 respondents, 107 provided sufficient data to calculate energy burden (74%). Approximately 60.7% (n = 65) of participants were classified as having a severe energy burden (i.e., >10% of gross annual household income spent on energy expenses) and were more likely to report renting their homes than owning (p = 0.02). Severe energy burden was also associated with reduction of household expenses to pay energy bills (p = 0.04); experiencing stress related to energy issues (p = 0.03); and prior diagnosis of obesity (p = 0.03).
Conclusions:
These findings highlight the need for interventions to make rental housing more energy efficient and for increased access to and awareness of energy assistance programs, particularly for people with specific chronic health conditions who struggle to afford energy costs.
BACKGROUND
Energy insecurity, the uncertainty or inability of households to meet their basic energy needs such as heating, cooling, and powering essential devices, can exacerbate adverse health conditions such as respiratory disease and mental illness. 1 In cities such as Phoenix, Arizona, where average high temperatures in the summer exceed 105°F, energy insecurity increases morbidity and mortality from heat-related illness due to inadequate home cooling. 2 This is particularly dangerous for vulnerable populations, including older adults, children, and those with chronic health conditions.3,4,5
In 2006, the Maricopa County Department of Public Health (MCDPH) developed a surveillance system to monitor heat-related deaths. During 2006–2020, MCDPH investigators found that 61% of heat-related fatalities occurred indoors, with victims dying in homes without electricity, lacked air conditioning (A/C) units, or had underutilized or non-functioning A/C units. 6
The South Phoenix community, encompassing zip codes 85040, 85041, and 85042, is 60.7% Hispanic and has a median annual income of $66,466. From 2016 to 2020, this community experienced a higher rate of heat-associated deaths compared to the rest of Maricopa County overall (6.2 deaths per 100,000 vs. 4 deaths per 100,000, respectively). 7 In 2021, MCDPH, in conjunction with Unlimited Potential, the American Council for an Energy-Efficient Economy (ACEEE), and Columbia University, launched a survey in this South Phoenix community aimed at identifying the economic barriers preventing households from acquiring and maintaining an A/C unit or meeting their energy expenses. The present survey focuses on energy burden, defined as the proportion of household income spent on energy costs, and examines health and sociodemographic factors related to energy burden in this community.
METHODS
Funding from the Robert Wood Johnson Foundation’s Interdisciplinary Research Leaders program facilitated a collaboration between MCDPH, Columbia University, and the ACEEE. 8 From this collaboration, a team was formed to investigate energy insecurity in a South Phoenix community.
Survey
We partnered with a local community-based organization, Unlimited Potential, to survey residents in zip codes 85040, 85041, and 85042 in South Phoenix regarding household demographics, housing characteristics, monthly expenses, utility assistance program participation, personal health, and heat-related illness. The 80-question QualtricsXM survey, available in English and Spanish, included multiple-choice and open-ended questions. Community Health Workers from Unlimited Potential recruited participants through convenience and voluntary sampling of clients over the phone and visitors of a local farmer’s market during February–March 2021. Participants received a $50 gift card for completing the survey. This project was reviewed by the Columbia University Institutional Review Board and deemed not to be research.
Measures
Energy burden was calculated by dividing each participant’s self-reported annual energy expenses by their gross annual household income. Severe energy burden was defined as >10% of gross annual household income spent on energy expenses, high energy burden as >6%–10%, and low-moderate energy burden as ≤6% of gross annual household income spent on energy expenses.9,10
Demographics, including age, race/ethnicity, and household income, were analyzed in relation to energy burden. Housing characteristics, including the year the home was built and housing tenure (renting vs. owning), were also examined. Furthermore, analyses explored the relationship between energy burden and the energy efficiency of housing and appliances, as well as any limitations on using an A/C system. Limitation options that could be selected by respondents included lack of an A/C system, not being able to afford to run the A/C when needed, or poorly functioning or non-functioning A/C units (that respondents could not afford to repair). Lastly, we examined the relationship between energy burden and various comorbidities, including obesity, hypertension, diabetes, asthma, heart disease, and cancer.
SAS version 8.2 and Microsoft Excel 365 version 2108 were used to conduct analyses. Data cleaning included investigating response discrepancies and removing surveys for which energy burden could not be calculated using the previously described method. Chi-square and Fisher’s exact tests were used as appropriate to examine relationships between energy burden and other covariates.11,12
During the initial draft of this work, the principal author (
RESULTS
During February–March 2021 a total of 145 surveys were collected, of which there were 107 (74%) usable surveys for analysis. Among survey respondents, 98% identified as Hispanic or Latino, with a mean age of 43 years (range 19–75). Approximately 65% of participants reported living in single-family detached homes, 19% in apartments of multi-unit dwellings, and the remaining 16% in mobile homes. Among those living in single-family detached homes, 55% owned their homes. Approximately 48.7% of respondents lived in homes built before 1980, 21.4% in homes built in 1980–1999, and 28.6% in homes built between 2000 and 2020 (Table 1). Approximately 84.1% of respondents reported an annual household income of $36,000 or less, of whom 51% reported monthly housing costs greater than $1000 per month.
Survey Respondent Characteristics, Indicators, and Comorbidities according to Energy Burden; February 2021 to March 2021, Maricopa County AZ
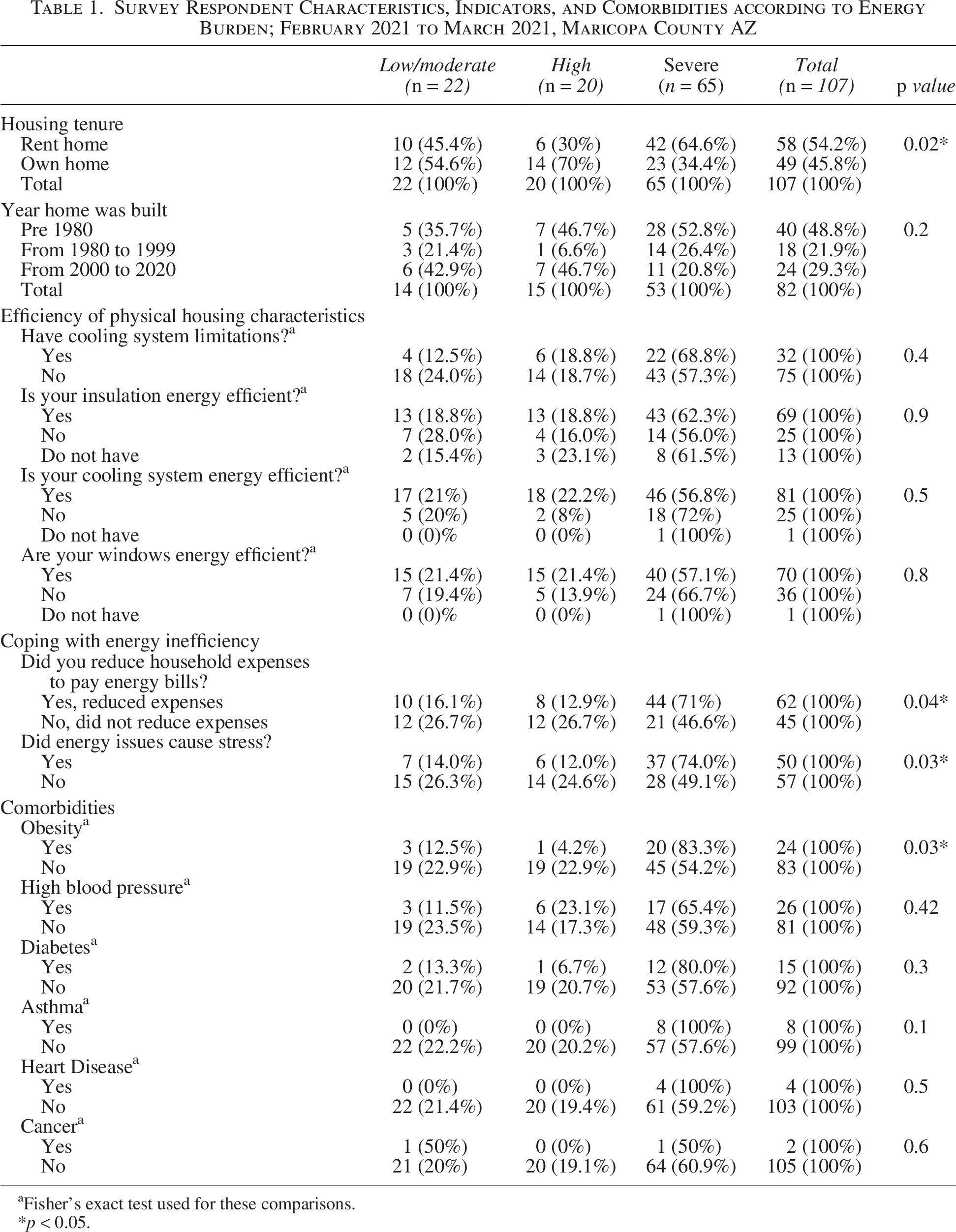
Fisher’s exact test used for these comparisons.
p < 0.05.
Of the 107 (74%) participants who provided sufficient data for energy burden calculations, 60.7% (65/107) were classified as having a severe energy burden, 18.7% (20/107) as having a high energy burden, and 20.6% (22/107) as having a low-moderate energy burden. Renters were more likely to experience severe energy burdens compared with homeowners (65% vs 35%; p = 0.02) (Table 1). In addition, 52.8% (28/53) of households with a severe energy burden lived in homes built before 1980, whereas only 21% (11/53) lived in homes constructed between 2000 and 2020. Among renters who provided information on the age of their home (n = 40), 22 (55%) reported living in pre-1980 housing compared to 5 (12.5%) who lived in housing built from 2000 to 2020. Mean household size was similar across energy burden categories: 4.3 people for low/moderate, 4.6 for high, and 4.4 for severe (p = 0.6).
Severe energy burden was further associated with the need to reduce household expenses to pay energy bills (p = 0.04) (Table 1) and experiencing stress related to energy issues (p = 0.03) (Table 1). A prior diagnosis of obesity (p = 0.03) was also significantly associated with increased energy burden (Table 1). Although not statistically significant, high blood pressure, diabetes, asthma and heart disease trended toward an association with high energy burden.
DISCUSSION
The results of this survey underscore the potential impact of energy burden on the health and well-being of this predominantly Hispanic/Latino community in South Phoenix. Energy burden is a critical issue for survey respondents in this community, with 60.7% of participants experiencing severe energy burden. This aligns with previous research demonstrating high prevalence of severe energy burdens among low-income and minority populations. 13 Additionally, the prevalence of severe energy burden in this study was higher than that reported for Phoenix as a whole (10%) and the national average (3.5%).14,15 This is likely due to a combination of factors, including low household incomes, high energy costs, and inefficient housing. 16
Several socioeconomic factors were associated with high energy burdens in the present analysis. Compared to homeowners, renters were more likely to live in homes built before 1980 and to experience severe energy burden. This finding is supported by national data showing that renters often face higher energy costs relative to their incomes due to less energy-efficient housing. 17 In addition, renters may also have limited control over making energy-saving improvements such as adding insulation or using LED lighting. Furthermore, most households in this survey earned less than $36,000 annually, with a majority dedicating over $1000 per month for housing, or a minimum of one-third of their pre-tax income. This disproportionate housing burden leaves these households acutely vulnerable to energy insecurity. Moreover, this study found a significant association between energy burden and both reduction of household expenses to pay energy bills and increased stress due to energy issues. This suggests a potential feedback loop, where the financial strain of high housing costs relative to income not only limits funds available for energy but may also contribute to a broader financial insecurity, amplifying the stress and hardship associated with meeting basic energy needs.
Housing characteristics may also play a crucial role in energy burden. Homes built before 1980 are generally less energy efficient, resulting in higher energy costs to maintain comfortable indoor temperatures. 18 Most survey respondents with severe energy burdens lived in housing built before 1980; however, no statistically significant relationship was observed between energy burden and year of housing construction. The likely reason is that of the 107 respondents for whom energy burden could be calculated, only 82 provided information on the year their home was built, resulting in reduced statistical power to detect an association. Moreover, landlords are generally not required to disclose the age of a property to tenants unless it impacts health or safety. As a result, many renters may never inquire about or be informed of the home’s age, which could have led to inaccurate or non-responses.
In the present analysis, having energy-efficient housing features such as cooling systems, insulation, or windows was not significantly associated with energy burden. Since energy efficiency can be a subjective concept and was not clearly defined in the questionnaire, respondents might have interpreted questions regarding the energy efficiency of their homes differently from one another. This might have affected the results of the analysis.
Energy insecurity can worsen existing health disparities, as individuals in households with severe energy burdens may have to choose between paying for energy and other essentials like medical care.19,20 This can lead to delayed or skipped appointments, untreated conditions, and ultimately poorer health outcomes, particularly for vulnerable populations already facing health challenges. In this analysis, a prior diagnosis of obesity was associated with severe energy burden. Obesity is highly prevalent in low-income communities doubly impacted by food insecurity and food deserts. 21 Obesity creates a combination of physiological challenges that make it harder for the body to cope with heat stress, increasing the risk of heat-related illness and death in households that cannot afford to maintain adequately cool temperatures.22,23,24 Although previous research demonstrated a relationship between energy insecurity and cardiovascular disease, respiratory and mental health conditions, we were unable to detect a significant association due to the lack of study participants reporting such diagnoses.25
Strengths
This survey has several strengths. It is the first community-scale survey to examine the prevalence of energy burden in South Phoenix. In addition, MCDPH investigators partnered with a local organization to recruit participants and collect data using a community-based participatory research approach, ensuring that the survey was culturally relevant and responsive to the needs of the community. The bilingual survey facilitated broader participation and more accurate data collection, while the provided incentive likely increased response rates and data completeness. Finally, this analysis utilized a previously validated and widely used method for the calculation of energy burden. 26
Limitations
This survey relied on self-reported data, which may be subject to recall bias. In addition, the sample size was relatively small and may not be representative of the entire South Phoenix community. Sufficient information for calculation of energy burden was provided in only 107 out of 145 surveys. Thus, a substantial proportion of participants were excluded due to missing data, which could have resulted in an under- or overestimation of the prevalence of severe energy burden in the survey population. Finally, the cross-sectional design of the survey limits our ability to draw causal inferences about the relationship between energy burden and health outcomes.
CONCLUSION
Local public health departments are increasingly recognizing energy insecurity as a critical social determinant of health and are implementing strategies to track its impact on communities. 27 Despite its limitations, this study provides valuable insights into the issue of energy burden in South Phoenix. Our findings underscore the need for assistance programs for low-income households and individuals with chronic health conditions could help offset the financial burden of energy costs. Public health campaigns could also raise awareness of the health risks associated with energy insecurity and help to promote behavior change and encourage individuals to seek assistance with paying their energy bills. Finally, future research should examine the longitudinal relationship between energy burden and health outcomes, as well as the effectiveness of interventions to reduce energy insecurity in low-income communities.
AUTHORS’ CONTRIBUTIONS
Conceptualization: V.B. and D.H. Methodology: V.B., D.H., S.M., and A.P.D. Formal Analysis: E.W. and T.B. Investigation: E.V. and T.B. Writing—S.M. and T.B. Writing—review and editing: A.P.D., D.H., and J.W. Supervision: V.B. and E.V. Project Administration: V.B. and D.H. Funding acquisition: V.B. and D.H.
Footnotes
ACKNOWLEDGMENTS
The Maricopa County Department of Public Health Climate and Health Team would like to thank the following persons and agencies for their contributions to this energy insecurity project: residents and respondents from the South Phoenix community, community health workers with Unlimited Potential, and Roxana Ayala and Lauren Ross (formerly) with the ACEEE.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
This publication and the project were supported by a Robert Wood Johnson Foundation Interdisciplinary Research Leaders Program award of $105,000 to the three partner organizations: the American Council for an Energy Efficient Economy (ACEEE; primary applicant), Maricopa County Department of Public Health, and Columbia University. The contents are those of the author(s).