
Abstract
Inhalation therapy has become a cornerstone in the treatment of respiratory diseases such as asthma, chronic obstructive pulmonary disease, and cystic fibrosis, owing to its rapid onset, direct pulmonary targeting, and avoidance of first-pass metabolism. Its clinical scope has expanded beyond conventional respiratory indications to emerging applications, including vaccine delivery, systemic disease management, and localized tumor therapy. However, traditional inhalation systems are often designed for the average patient, overlooking physiological variability that results in inconsistent drug deposition and therapeutic efficacy—particularly in children, elderly patients, and individuals with airway abnormalities. Additive manufacturing (AM), with its high design flexibility and capacity for personalization, offers new possibilities for structural optimization, particle engineering, and in vitro model fabrication in inhalation therapy. Growing evidence indicates that 3D-printed inhalation devices and formulation platforms can enhance drug deposition control, patient compliance, and delivery precision. This review provides a comprehensive overview of recent advances in AM applied to inhalation therapy, highlighting its roles in personalized device fabrication, microdose particle design, and in vitro model construction, as well as in the exploration of emerging therapeutic strategies. Furthermore, it discusses current technical challenges and translational barriers. Overall, AM is propelling the transition of inhalation therapy from standardized approaches toward intelligent, patient-centered delivery systems, offering both theoretical and technological foundations for next-generation respiratory healthcare.
Graphical abstract
Introduction
Inhalation therapy, as a primary route of drug administration, has become a first-line intervention for respiratory diseases such as asthma, chronic obstructive pulmonary disease (COPD), and cystic fibrosis, owing to its rapid onset of action, precise pulmonary targeting, and reduced systemic adverse effects. 1 –3 In recent years, its applications have expanded beyond traditional pulmonary indications to include vaccine delivery, systemic disease management, and localized tumor therapy. 4,5 Despite these advances, current inhalation strategies still rely heavily on standardized devices and dosage designs, often neglecting interindividual variations in age, airway anatomy, and inspiratory flow dynamics. This inherent tension between standardized design and patient heterogeneity not only compromises therapeutic consistency and efficacy but also constitutes a long-standing challenge in clinical practice. 6 Clinical evidence reveals that special populations—such as children, elderly patients, and individuals with airway abnormalities—frequently struggle to operate existing inhalation devices effectively. For example, many children are unable to achieve the minimum inspiratory flow required for dry powder inhalers (DPIs), while a substantial proportion of elderly COPD patients fail to use metered-dose inhalers correctly due to reduced joint mobility. 7 –10 At the same time, the pulmonary administration of innovative macromolecular drugs continues to face formidable barriers, including mucus entrapment, enzymatic degradation, and inefficient deposition, resulting in drug utilization rates below and compounding both clinical and economic burdens. 11 Collectively, these limitations underscore a growing contradiction: while traditional formulation and manufacturing paradigms prioritize scalability and uniformity, real-world clinical needs increasingly call for individualized, adaptive, and patient-centered inhalation solutions.
In recent years, additive manufacturing (AM; 3D printing [3DP]) has emerged as a promising solution to the challenges of inhalation therapy. 12,13 As a highly flexible manufacturing technology, 3DP not only addresses the dosage constraints of conventional mass production by enabling precise microdose control but also supports the customization of personalized devices based on imaging data. 14 –16 These advantages may enhance usability and patient acceptability, which are associated with adherence. Moreover, with the development of smart materials and the advent of 4D printing, inhalation devices are being endowed with the capability to respond to environmental or physiological stimuli, thereby offering more adaptive therapeutic strategies for specific patient populations. 17 At the same time, the integration of 3D-printed airway models with computational fluid dynamics (CFD) simulations has provided robust tools for in vitro evaluation and facilitated the clinical translation of inhalation formulations. 18 –20 Although the concept of personalized medicine has been discussed for decades, recent breakthroughs in AM and digital modeling technologies have reestablished the technical feasibility of patient-customized inhalation systems. 3DP technology holds promise to overcome the manufacturing limitations of traditional mass production, thereby providing a technical support platform for personalized treatment solutions that are clinically necessary. This review systematically summarizes recent progress in the application of 3DP for inhalation therapy, with a focus on personalized device manufacturing, dose modulation, in vitro evaluation systems, and novel therapeutic exploration. In addition, it discusses the prospects for clinical translation and the challenges that remain, aiming to provide both theoretical foundations and practical references for the development of more precise and efficient inhalation therapy systems in the future.
AM Technologies
AM, commonly referred to as 3DP, is an advanced manufacturing technology that fabricates 3D structures through sequential material deposition. Compared with conventional subtractive manufacturing, its advantages include controllable structural complexity, high geometric precision, and individualized customization. In recent years, AM has emerged as a critical enabling technology in pharmaceutical engineering and personalized medicine. 21 Within the pharmaceutical domain, the major 3DP technologies encompass fused deposition modeling (FDM), 22 stereolithography/digital light processing (SLA/DLP), 23 selective laser sintering (SLS), 24 inkjet printing, 25 and 3D bioprinting. 26 FDM extrudes thermoplastic polymers layer by layer to produce porous drug carriers, dry powder reservoirs, and customized inhalation interfaces. SLA/DLP employs ultraviolet or visible light to cure photopolymer resins, offering high printing resolution for fabricating intricate microfluidic inhalation devices and biomimetic airway models with optimized aerodynamic properties. SLS utilizes laser sintering of powdered materials to generate high-strength components suitable for pressure-resistant and moisture-tolerant inhaler cores. Inkjet printing, characterized by precise control over droplet volume and distribution, enables the fabrication of drug-loaded membranes, aerosolized droplets, and nanoscale drug delivery systems, thereby providing versatile platforms for controlled-release inhalation formulations. 3D bioprinting enables the fabrication of physiologically relevant airway and alveolar models through the layer-by-layer deposition of cells, bioinks, and hydrogels, thereby supporting studies on drug deposition, permeability, and toxicity responses. 27 –29 For example, by employing multimaterial jetting and hydrogel support strategies, Grigoryan et al. 30 successfully printed airway organoids containing human lung epithelial cells, which were subsequently applied for in vitro absorption assessment of inhaled drugs and nanoparticles. Such models hold significant promise for respiratory drug screening and inhaled vaccine development. In parallel, 4D printing—an extension of 3DP—leverages stimuli-responsive materials to impart adaptive deformation or functional regulation to printed structures in response to environmental factors such as temperature, humidity, or pH. 31 In the context of inhalation therapy, 4D printing has been utilized to fabricate airway stents capable of self-conforming at body temperature and to design angle-adjustable interfaces, both of which substantially improve personalized fit. 32
Overall, FDM and SLA are most effective for device structural optimization, SLS is well suited for producing robust functional components, and inkjet printing and bioprinting offer considerable potential for precise formulation control and advanced model construction. Meanwhile, 4D printing is driving the development of smart, responsive, and biomimetic systems. 14 With the convergence of materials science, Artificial intelligence (AI)-driven design, and CFD simulation, 3DP is increasingly positioned as a technological cornerstone for achieving precise and personalized inhalation therapy.
AM in Respiratory Sciences
Personalized and targeted inhalation therapy
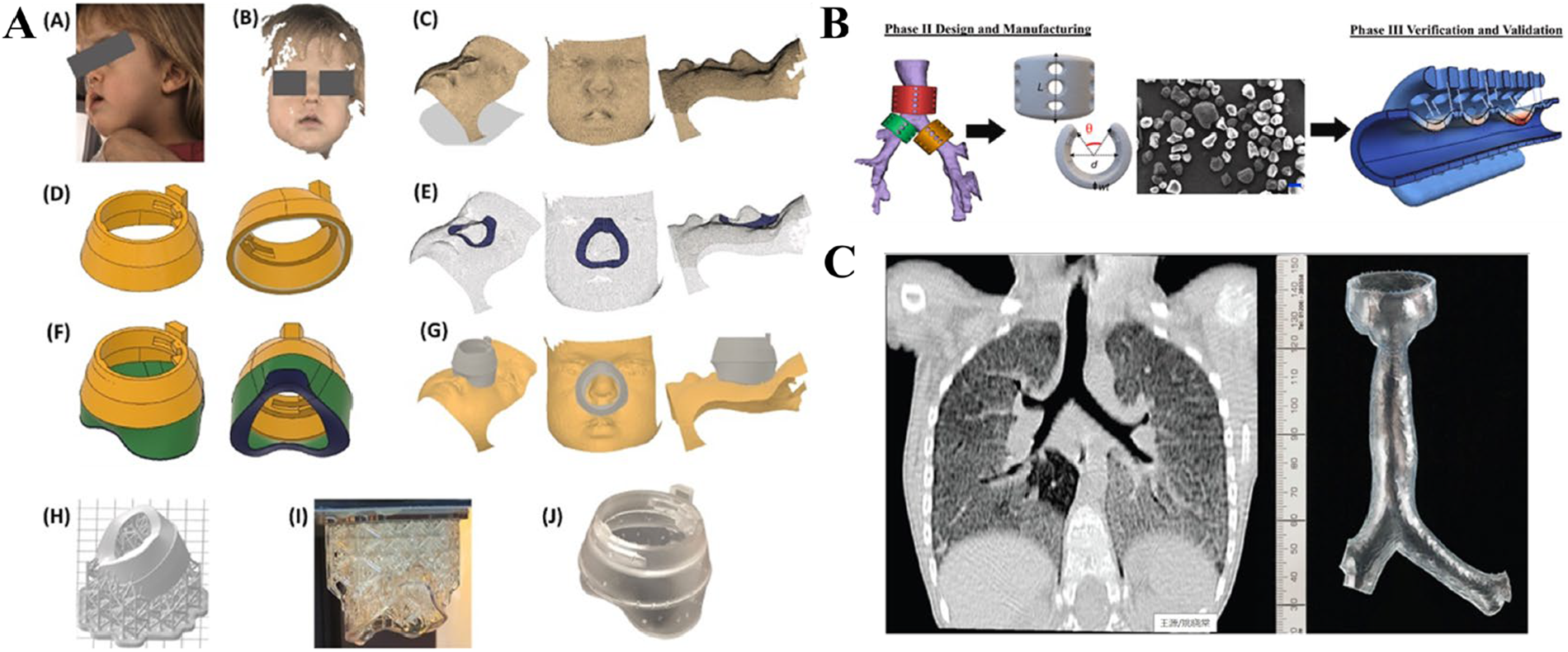
Inhalation therapy, a cornerstone in the management of respiratory diseases, is highly dependent on the patient’s inspiratory flow rate, pulmonary function, and ability to operate the device correctly. Traditional inhalation devices are designed for specific patient populations during development and validation, undergoing rigorous ergonomic testing. However, device performance standards are typically established based on representative demographic characteristics, and standardized device designs may not adequately accommodate significant physiological variations between individuals. For example, healthy females typically present smaller central airways than males (∼26%–35%), 33 –36 while even greater anatomical differences exist in pediatric, geriatric, and patients with abnormal airway structures. As a result, traditional inhalation systems frequently lead to dose variability, suboptimal drug delivery efficiency, and poor patient compliance. 37,38 3DP technology offers unique opportunities to tailor formulations and device structures to individual needs, such as age, lung function, and oral or nasal anatomy. Computed tomography (CT)-derived inhalation masks designed for pediatric patients have been shown to significantly enhance sealing performance and pulmonary deposition of nebulized drugs, thereby improving both compliance and therapeutic efficacy. 39,40 Interfaces and masks produced via SLA or FDM, based on facial scans of children, further enhance device fit, reduce operator dependency, and improve both delivery efficiency and adherence. Patient-specific airway geometries reconstructed from CT data obtained during actual inhalation sessions also provide realistic models for investigating aerosol transport and deposition in the upper respiratory tract. 41 In terms of protective strategies, Hu et al. 42 developed an intranasal mask composed of engineered microvesicles and thermosensitive hydrogels that form a sustainable barrier within the nasal cavity. This “internal barrier” strategy effectively blocked SARS-CoV-2 and influenza virus infections in both animal models and human airway systems, demonstrating a novel concept for personalized respiratory protection. Clinically, Bockstedte et al. 43 developed customized masks for patients with craniofacial anomalies using computer-aided design and manufacturing, achieving improved efficacy, comfort, and accessibility in noninvasive ventilation (Fig. 1A). Similarly, Naik et al. 44 reported a universal strategy for producing clinical-grade, patient-specific, biodegradable airway implants via SLS, exemplified by pediatric devices that restored airway patency in children with life-threatening obstructions (Fig. 1B). Collectively, these innovations reduce the invasiveness of respiratory interventions while establishing sustainable, patient-centered solutions for pediatric and anatomically diverse populations. 40,46
Customized tracheal models and scaffolds.
Beyond pediatric and craniofacial applications, patients with structural airway alterations caused by tumor resection, tracheotomy, or congenital anomalies often experience severely reduced deposition efficiency and are thus excluded from conventional inhalation therapy. 47,48 To address this challenge, 3DP based on high-resolution CT or magnetic resonance imaging data enables accurate simulation of upper airway features (e.g., uvula, epiglottis, soft palate) and facilitates systematic studies on deposition patterns in patients with abnormal airway anatomy. 49 –51 Ramaraju et al. 45 applied 3D-printed airway models for planning bronchial intubation, single-lung ventilation, and preoperative training. In infectious disease research, GóShaqour et al. 52 combined 3DP with hot-melt extrusion to fabricate antibiotic-loaded catheters and established a ventilator-associated pneumonia mouse model. This strategy not only inhibited bacterial biofilm formation but also verified the in vivo efficacy of anti-infective materials. In addition, SLS-fabricated tracheal and bronchial implants with anatomically customized interfaces and drainage channels have successfully restored airway patency in pediatric patients with tracheobronchomalacia, characterized by partial or complete airway collapse (Fig. 1C). Inhalation therapy requirements in such special populations exhibit pronounced heterogeneity in dosage, structural configuration, and delivery pathways, creating significant challenges for the adaptability and ergonomics of drug delivery systems. 53 By leveraging “patient-centric” reverse design, 3DP breaks the rigid framework of traditional industrial production, making personalized inhalation therapy a clinically feasible reality. Looking forward, the integration of AI-driven imaging modeling with print parameter optimization is expected to further position 3DP as a core technology for point-of-care manufacturing, offering highly adaptive, precision-tailored inhalation therapies for diverse patient populations.
Particle design
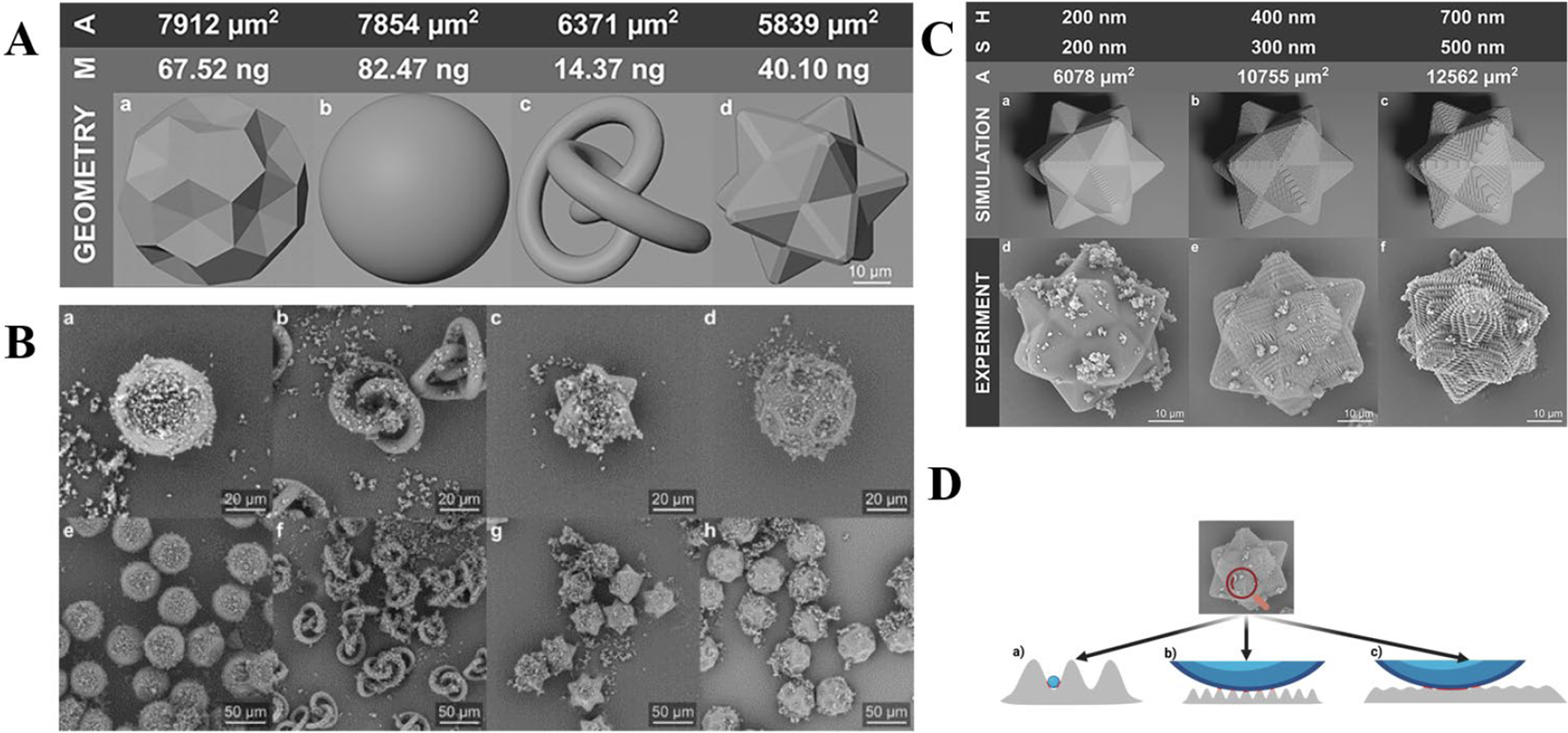
The clinical efficacy of inhalation formulations largely depends on the aerodynamic behavior, dispersion, and deposition characteristics of aerosolized particles within the respiratory tract. The geometric morphology and surface structure of particles are critical determinants of these properties. Traditional preparation methods, such as spray drying and spray freeze drying, have achieved significant success in producing dispersible inhalation powders, exemplified by commercial products like TOBI® Podhaler and Colobreathe®. These methods effectively address delivery efficiency and inhalation flow dependency issues cost-effectively. In contrast, AM enables deterministic, design-driven control over particle geometry and internal structure, allowing precise regulation of surface characteristics, porosity, and complex geometries. This controllability not only optimizes aerodynamic behavior and powder dispersion properties but also enables precise targeting of deposition locations and customization of drug release rates. Consequently, it facilitates more personalized and efficient inhalation therapy solutions tailored to diverse patient populations. Through jet printing or electrospray deposition, monodisperse particles with uniform morphology can be fabricated, while surface wrinkles or pores can be introduced by adjusting jet pulse frequency and solvent evaporation kinetics. Such roughened surfaces reduce effective contact area and agglomeration tendency, thereby enhancing powder dispersibility and pulmonary deposition efficiency. Digital modeling in AM further allows the creation of complex particle geometries—including spherical, star-shaped, tapered, or rolled structures—by modifying nanoscale surface topographies such as protrusions or grooves to optimize aerodynamic performance. Wostry et al. 54 demonstrated the use of multifocal multiphoton 3D laser printing to fabricate uniform, geometrically complex particles (∼50 µm diameter) as carriers for DPI formulations. This method enables precise control of particle morphology and surface texture to optimize inhalation performance. In their study, four geometries—Sphere, Soccerball, Rollingknot, and Pharmacone—were compared under three nanoscale roughness conditions (200–700 nm slice intervals). The Pharmacone particles exhibited superior aerodynamic behavior, achieving a fine particle fraction (FPF <5 µm) of 16.9%–18.1%, markedly higher than the 2.3%–3.8% observed for other shapes. This improvement was attributed to enhanced detachment of the active pharmaceutical ingredient (API, budesonide) during dispersion while maintaining uniform blending (API recovery 90%–110%, RSD <15%). Interestingly, surface roughness exerted minimal influence, as the API particles (mean diameter 1.43 µm) could not embed into surface grooves, highlighting particle geometry as the dominant factor governing dispersion and pulmonary deposition. These findings underscore the potential of high-resolution AM for rapid prototyping and optimization of inhalable particle systems (Fig. 2). However, it should be noted that the polymer employed in this study is not suitable for clinical inhalation applications, and the work primarily serves as a proof of concept for aerodynamic optimization rather than a demonstration of material compatibility with regulatory requirements for inhaled products. This limitation underscores the ongoing challenge of translating high-resolution 3DP approaches into clinically relevant respiratory formulations. However, Wostry et al. 54 carrier particles produced by 3D laser printing are therefore only used to investigate the influence of geometry on carrier particle performance. Because mass-produced particles consist of polymers, made by radical polymerization, and are not safe to be inhaled by humans, mostly due to possible residual photo initiator and the fact that they are not degradable. For inhalation drug delivery, inhalation materials must achieve targeted drug delivery without interfering with the normal physiological function of mucus. Otherwise, they may compromise barrier integrity or induce inflammation. 55 The success of inhalation materials lies not merely in enhancing delivery efficiency but in striking a balance between “enhancing therapeutic efficacy” and “maintaining pulmonary physiological function.” Nevertheless, research for noncytotoxic and possibly digestible photoresists, which could be mass produced with multiphoton 3D laser printing, is ongoing. 56 In another study, Zhang et al. 57 designed γ-cyclodextrin microrods and nanocubes for iodine delivery, combining potent antimicrobial activity with low inflammatory response, while Yu et al. 58 developed morphologically engineered nanovesicles for optimized insulin nebulization, achieving a bioavailability of 42.72% and reducing blood glucose to 50% of baseline. Additionally, low-density porous particles can enhance deep lung delivery by prolonging aerosol suspension time. López-Iglesias et al. 57 employed thermal inkjet printing combined with supercritical drying to produce alginate aerogel microparticles, achieving a superior FPF compared with commercial formulations, sustained salbutamol release over 10 hours, and excellent cellular compatibility. Overall, AM technologies hold significant promise for transforming the design of inhalable particles by enabling precise control over geometric structure, surface energy distribution, and internal porosity—attributes that remain challenging to achieve using conventional fabrication methods. Coupled with aerodynamic modeling and pulmonary deposition simulations, AM-driven particle engineering enables precise control over dispersion and deposition dynamics, paving the way for personalized inhalation therapy and multidrug synergistic delivery.
Particle design.
Design and development of inhalation devices
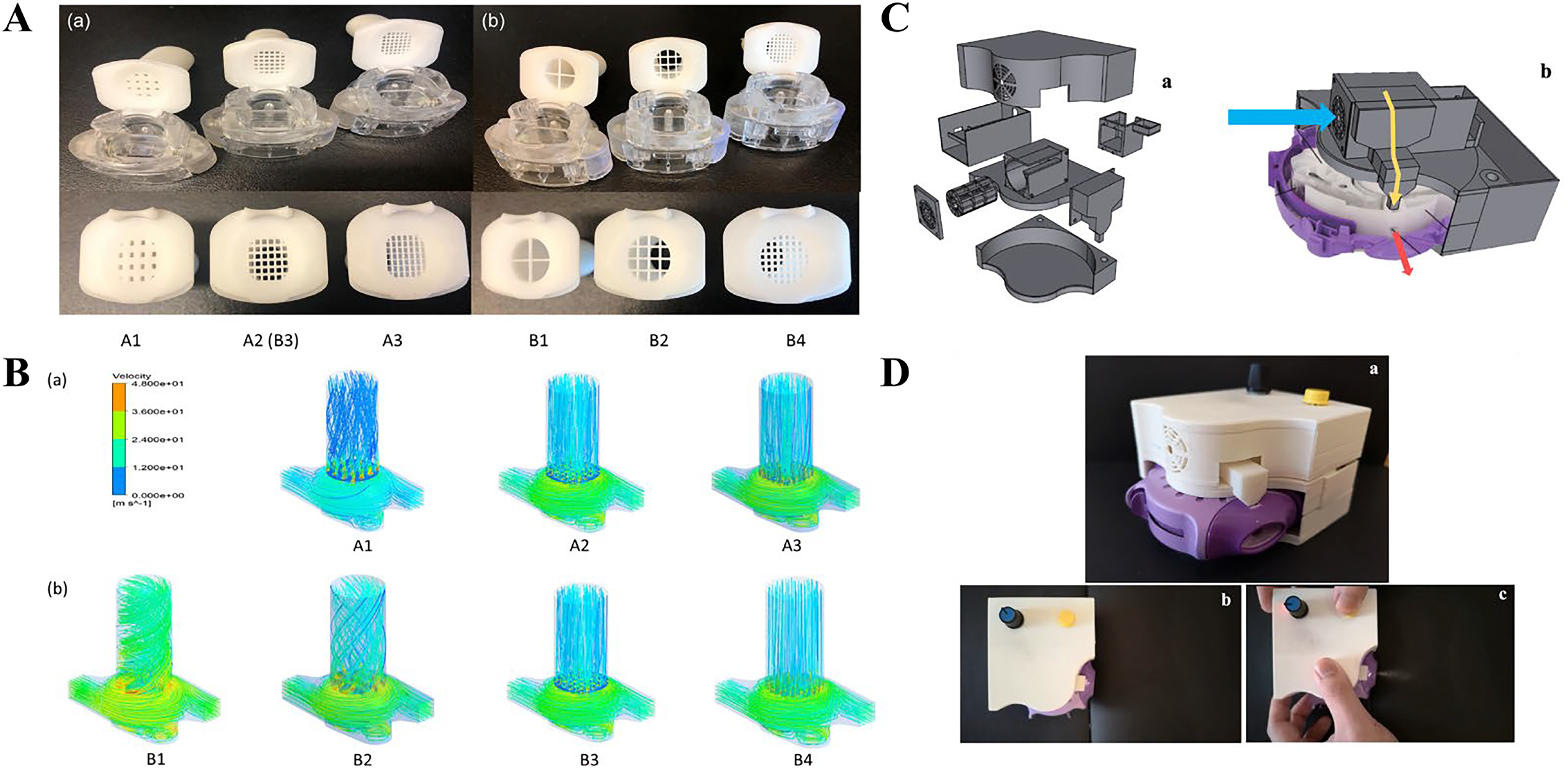
As a critical component of drug delivery systems, the structural design, nebulization efficiency, and aerodynamic characteristics of inhalation devices are closely linked to patient usage behavior, directly determining pulmonary drug deposition and therapeutic efficacy. AM technology offers unprecedented flexibility for designing and optimizing inhalation devices. Particularly in DPI design, its high-precision processing capabilities not only enable rapid prototyping of complex geometries but also support modular redesign of critical internal components. DPIs are typically categorized as single-dose devices and multidose devices, with the latter further subdivided into multiunit dose systems and reservoir-type systems. Although differing in powder storage format, dose metering mechanisms, and airflow path design, their fundamental operating principle is similar: during patient inhalation, inspiratory airflow generates turbulent and shear forces within the device that promote powder deagglomeration and aerosolization. Depending on the formulation type, this process may involve drug–carrier detachment in carrier-based systems or the dispersion of cohesive drug agglomerates in carrier-free formulations, ultimately enabling particle transport to the lower respiratory tract. Children, the elderly, and patients with chronic respiratory diseases often struggle to achieve optimal inhalation flow rates, leading to insufficient drug dispersion, particle deposition in the upper airways, and diminished therapeutic efficacy. Traditional device designs struggle to provide precise adjustments for different user groups, but the introduction of 3DP technology has transformed this landscape. Through 3DP, inhalation channels with varying geometric parameters can be rapidly manufactured to investigate how turbulence intensity, particle trajectories, and local pressure differentials affect powder dispersion efficiency. 59 Recent studies, for instance, have redesigned critical internal structures—including spiral channels, 60 mouthpiece dimensions, 61 gas inlets, grids, 62 and added supplementary components 63 to enhance device performance and improve drug delivery efficiency (Fig. 3). Additionally, researchers can guide the development of inhalation formulations and adjust inhalation therapies based on specific population-based lung function parameters or airway structural characteristics. For instance, in 2022, Ma et al. 48 systematically isolated distinct anatomical features of the human pharynx to investigate their independent effects on aerodynamics and particle deposition characteristics within geometrically realistic human airways. In 2025, Zhang et al. 50 examined how individual variations influence particle distribution and deposition mechanisms across different regions of the inhaler airway. Looking ahead, 3DP technology accelerates the manufacturing of numerically optimized devices and structural refinements, while subsequent feedback from in vitro data further drives product optimization.
Inhalation device design.
Establish in vitro evaluation models
The efficiency of drug delivery in inhalation therapy is constrained by the complex anatomical geometry of the airways, aerodynamic characteristics, and pulmonary barrier function. Traditional animal experiments and clinical evaluations are not only costly and poorly reproducible but also insufficient for systematically elucidating drug deposition and pharmacodynamic mechanisms. Consequently, in vitro models based on AM have become an emerging research focus in recent years. Broadly, these models can be divided into two categories: physical airway models—constructed using 3DP and CFD—to analyze aerodynamic behavior and optimize inhaler design; and bio-lung chip models—based on bioprinting and microfluidic technology—to reconstruct the air–blood barrier and simulate pathological conditions for drug screening and toxicological studies. Regarding physical airway models, researchers have developed structures that closely replicate real human airways using CT imaging combined with 3DP. For example, Lim et al. 64 demonstrated that their printed simulated airway model exhibits deposition patterns similar to in vivo human data, potentially providing a reference for in vitro–in vivo airway deposition correlation and offering opportunities for personalized deposition studies in specific populations or disease state (Fig. 4E). Salmanipour et al. 67 achieved over 50% deposition efficiency for dry powder formulations by integrating 3D-printed airway models with a “Trojan particle” strategy, validating CFD prediction errors below 10% across varying flow rates. Moreover, studies by Mirzaaghaian et al. 68 and Zhang et al. 69 revealed that transient breathing patterns and particle physical properties significantly influence deposition distribution. Earlier research, including Koullapis et al. 70 multiscale CFD modeling and Khalid et al. 71 review on airway scaffold fabrication, has provided methodological frameworks bridging simulation and clinical application. Overall, physical in vitro models offer excellent structural controllability and experimental reproducibility, serving as engineering platforms for inhaler design and pulmonary drug delivery assessment. However, their inherent limitation lies in the omission of biological elements such as mucus layers, epithelial cell barriers, and dynamic respiratory motion, necessitating integration with bioengineered lung models for a more physiologically relevant evaluation.
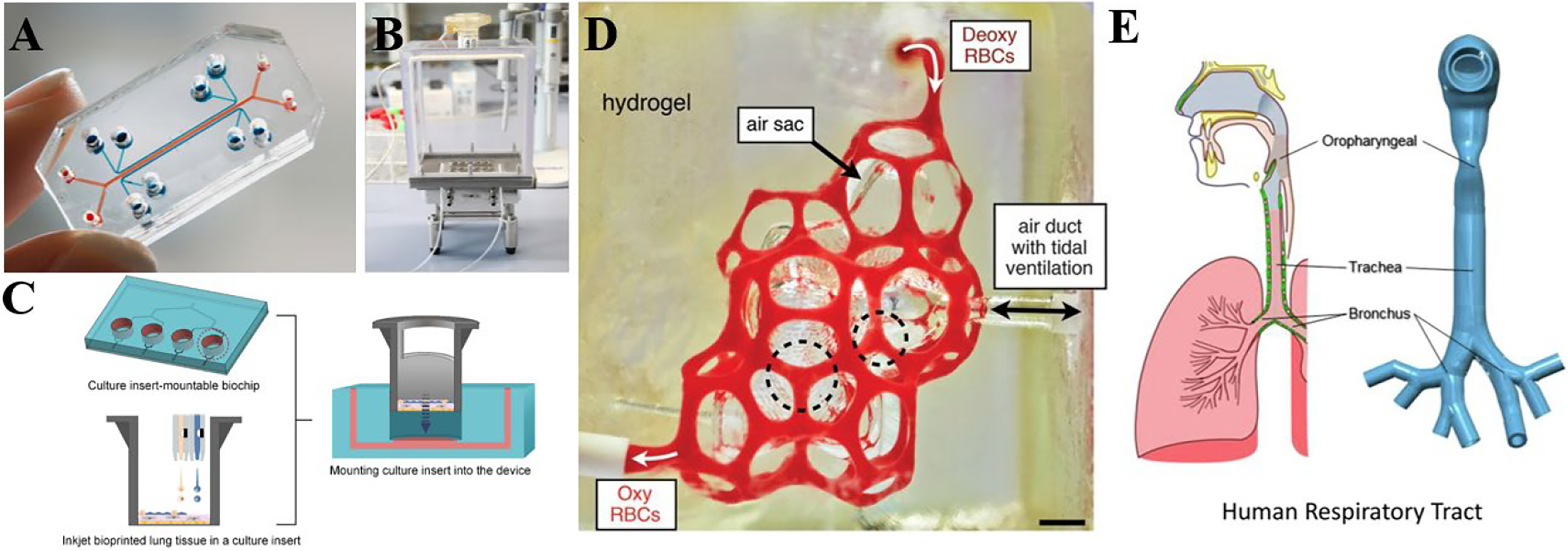
The “lung-on-a-chip” models.
Compared with physical in vitro models, research on bio-lung chip systems focuses on reconstructing the multicellular hierarchy and dynamic barrier functions of the lung within microfluidic environments, thereby more closely approximating in vivo physiological and pathological states. Their development can be broadly categorized into three dimensions: barrier reconstruction, functional biomimicry, and system integration (Fig. 4A, B). In terms of barrier reconstruction, Horváth et al. 72 demonstrated the feasibility of directly constructing an air–blood barrier via 3D bioprinting, providing a novel in vitro alternative model for inhalation toxicology. Kim et al. 66 developed a physiologically relevant alveolar lung-on-a-chip using 3D inkjet bioprinting. By fabricating micron-scale trilayer tissues and perfusing them at the air–liquid interface, they achieved structural integrity, tight epithelial junctions, and upregulation of key alveolar functional genes, highlighting the platform’s high customizability for diverse organ model studies (Fig. 4C). Functional biomimicry increasingly incorporates critical elements such as respiratory mechanics and vascularization. Grayson et al. 30 constructed complex vascular networks and validated oxygenation using photolithographic hydrogels, demonstrating the essential role of vascularization in maintaining pulmonary microenvironments (Fig. 4D). Shen et al. 73 enhanced barrier performance under cyclic respiratory stretching using a biomimetic hydrogel membrane, while Zamprogno et al. 74 developed a second-generation lung chip that maintained stable air–blood barrier function using primary human lung epithelial and endothelial cells. Tam et al. 75 introduced a photo-/enzyme-responsive hydrogel that provides a controllable and dynamic microenvironment, establishing a new material foundation for advanced lung tissue functionalization and personalized modeling. Overall, bio-lung chip research has evolved from single-layer barrier constructs to multifunctional platforms integrating vascularization, mechanical strain, and modular design. 76,77 Recent reviews have further emphasized their potential in modeling respiratory diseases such as bronchopulmonary dysplasia, COPD, and COVID-19, while also noting that the use of induced pluripotent stem cell–derived cells, achieving long-term culture stability, and establishing standardized protocols remain major challenges for clinical translation. 70,78 –80 In summary, physical airway models emphasize geometric reproduction and aerodynamic assessment, making them ideal for inhaler engineering optimization and deposition prediction. In contrast, biological lung-on-a-chip models prioritize biological fidelity and pathological simulation, offering unique advantages for drug screening and mechanistic studies. Future directions point toward integrating both approaches—using CFD and 3D-printed airway models to predict aerosol deposition efficiency, followed by validation of cellular-level toxicity and efficacy through lung-on-a-chip systems. This integrated strategy aims to construct a cross-scale, interdisciplinary lung modeling framework, thereby advancing inhalation therapy research from isolated physical optimization toward systematic biological validation and clinical translation.
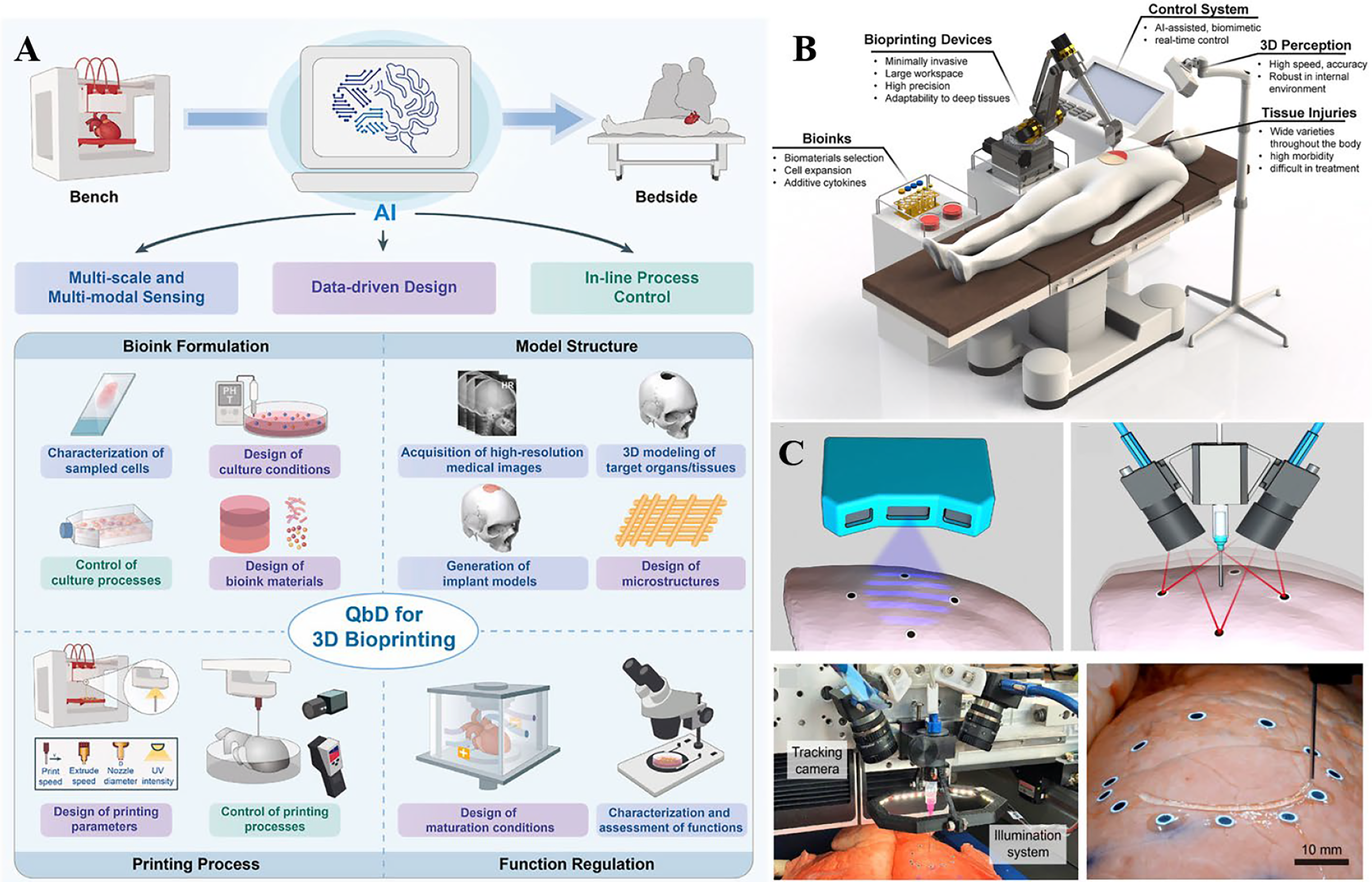
AI and machine-assisted printing
The advancement of 3D bioprinting technology requires the integration of biology, materials science, engineering, and computer science. Greater emphasis on interdisciplinary collaboration is essential to drive technological innovation and application. Emerging development directions include. The integration of artificial intelligence (AI) and intelligent robotics is propelling 3DP into the “5.0 era” (Fig. 5). Leveraging data-driven machine learning (ML) frameworks, AI enables optimization across design, process control, and material selection, substantially improving the precision and efficiency of complex tissue fabrication. 83,84 In the preprinting stage, AI contributes to bioink formulation design, composition screening, quality control, parameter optimization, and the development of adaptive printing platforms. 85 –87 During printing, AI enables real-time process monitoring, defect detection, and autonomous error correction. 88 Although its application remains in its infancy, AI demonstrates broad potential in 3D bioprinting—from material intelligence to process optimization and functional prediction. By leveraging ML algorithms, AI facilitates predictive modeling and adaptive control, leading to cost-effective, high-precision, and functionally enhanced constructs. 89,90 Xu et al. 91 used ML to develop a prediction model for cell viability by integrating neural networks, ridge regression, K-nearest neighbors, and RF. They investigated the performance of the model using three error metrics and used RF to determine the importance of each process parameter on cell viability. Their results indicated that the model could accurately predict cell viability and identify the critical process parameters in SLA printing. AI can also be used to predict the final performance of the design model. Barrera et al. 92 utilized hierarchical 2D images as input, with Young’s modulus, shear modulus, and porosity as outputs, to train a 3D convolutional neural network, ultimately achieving the prediction of the mechanical properties of scaffolds.
Artificial intelligence (AI) and machine-assisted 3D printing.
In parallel, the convergence of AI and closed-loop robotic printing has begun to redefine dynamic biomanufacturing. Zhu and McAlpine 42 developed an AI-assisted in situ 3DP system capable of adapting in real time to respiration-induced deformations of porcine lungs. This system directly printed ionogel-based flexible sensors on the lung surface, integrating electrical impedance tomography to produce high-resolution strain mapping. The mechanical compliance of the sensors matched that of native tissue, enabling continuous respiratory monitoring. This work highlights a paradigm shift—from static fabrication to adaptive, intelligent bioprinting—bridging AM with robotic-assisted pulmonary medicine. From a clinical application perspective, AI-enabled in situ bioprinting and flexible sensing introduce real-time feedback mechanisms to inhalation therapy. By dynamically monitoring lung deformation and ventilation status, AI continuously evaluates treatment efficacy and optimizes drug delivery strategies, propelling inhalation therapy from experience-driven approaches toward personalized, closed-loop precision interventions.
Overall, the integration of AI into 3D bioprinting and robotic manufacturing not only drives the intelligent evolution of tissue construction methods but also provides new technological support for the systematic optimization of inhalation therapy systems. By integrating AI-driven design and manufacturing with real-time physiological feedback, future advancements are anticipated in achieving refined optimization across multiple fronts: controlling inhalation particle size and morphology, predicting aerosol transport behavior, and designing personalized inhalation device structures. Coupled with dynamic modeling of patient respiratory patterns and pulmonary mechanics, AI can further enhance the precision and stability of respiratory disease treatments.
Discussion
The optimal efficacy of inhalation therapy depends on individualized drug selection, dose modulation, and precise pulmonary delivery strategies—requirements that apply to treatments for both localized airway and systemic diseases. AM offers innovative solutions in this process: by replicating patient-specific anatomy and respiratory patterns, it enables realistic device design and particle engineering during early R&D stages. Nonetheless, current advances in bioprinting and materials science remain insufficient to fully reproduce the complex physiological conditions of the human respiratory system, particularly in terms of airway elasticity, mucus layer simulation, and long-term model stability. In tissue engineering and in vitro modeling of airways and lungs, the lung’s intricate architecture—characterized by diverse cell populations, hierarchical airway branching, and complex vascular networks—poses formidable challenges for replication using current 3D bioprinting technologies. The scarcity of bioinks capable of recapitulating pulmonary microenvironments further limits the fabrication of structurally and functionally faithful constructs. 93 Moreover, the extended duration of the bioprinting process often compromises cell viability and biological function, reducing the performance of engineered tissues. 52 Post-print maturation into fully functional lung tissues remains a formidable task, while vascularization continues to represent a critical bottleneck; without sufficient perfusion, nutrient and oxygen diffusion within large constructs is inadequate, jeopardizing long-term cell survival. 94,95 These limitations collectively underscore the urgent need for advancements in bioink development, printing methodologies, and post-fabrication tissue maturation strategies to enhance the fidelity and feasibility of 3D-bioprinted airway and lung models. To address these challenges, AI- and robotics-assisted bioprinting are emerging as pivotal technologies that are propelling biofabrication toward an era of intelligent and adaptive manufacturing. AI-driven algorithms can analyze large-scale experimental datasets to optimize bioink compositions, predict printing outcomes, and enable closed-loop feedback during fabrication. When integrated with robotic systems, AI facilitates adaptive control of extrusion parameters, spatial alignment, and defect correction, thereby enhancing reproducibility and precision. These intelligent frameworks hold the potential to accelerate the realization of personalized, high-fidelity lung constructs.
However, the convergence of AI and 3D bioprinting also introduces new technical and infrastructural challenges. AI models require substantial computational resources to process complex geometries and multiparameter datasets, necessitating high-performance computing clusters or advanced cloud-based platforms. Moreover, the accuracy and reliability of AI predictions are inherently dependent on the quality and comprehensiveness of training data; incomplete, biased, or erroneous datasets can yield suboptimal or even flawed design outcomes. Addressing these issues demands not only technological innovation but also the establishment of standardized data frameworks, transparent model validation protocols, and interdisciplinary collaboration across engineering, computational science, and biomedicine.
Regulatory and standardization barriers continue to be major bottlenecks restricting clinical translation. 96 Current pharmaceutical and medical device regulations are not yet tailored to AM, underscoring the urgent need for unified standards on material selection, process reproducibility, and quality assurance. 97 Only through synchronized progress in regulatory science and technological innovation can personalized printed particles, tracheal stents, and inhalation devices achieve true clinical application. 98 Overall, AM is steering inhalation therapy toward intelligent, personalized, and biomimetic development pathways. From rapid device iteration to precision particle engineering, and from lung-on-a-chip platforms to digital health integration, its transformative potential is progressively unfolding. Future breakthroughs will rely on interdisciplinary collaboration, continuous innovation in materials and processes, and refinement of regulatory frameworks. 99,100 As these elements converge, AM is poised to redefine the research and application paradigms of inhalation therapy, ultimately establishing a new patient-centered model for respiratory health care.
Conclusion
This review summarizes the multilevel applications of AM in inhalation therapy. Covering personalized device design, particle engineering optimization, iterative device development, construction of in vitro evaluation models, and exploration of emerging therapies, AM demonstrates the unique potential to transcend traditional approaches. It enables precise geometric control, rapid prototyping, and iterative development, establishing a new paradigm for intelligent, personalized management of respiratory diseases. Nonetheless, current advancements remain constrained by several challenges, including limited biomimetic properties of printable materials, restrictions in printing efficiency and scalability, incomplete simulation of complex airway physiology, and insufficient long-term biocompatibility and clinical validation. Lagging regulatory standards and scarce clinical evidence further hinder large-scale implementation of personalized printed products. Looking forward, interdisciplinary collaboration will be pivotal in driving breakthroughs in this field. With the further integration of AI and computational modeling technologies, AM holds promise to enhance our understanding of the mechanisms underlying structure–airflow–deposition interactions. This advancement will improve quantitative prediction capabilities and design rationality in inhalation therapy development, thereby providing more interpretable technical support for precision treatment of respiratory diseases.
Authors’ Contributions
C.Z.: Writing—original draft preparation and finalizing the article. X.Z. and J.Z.: Collecting information. C.H.: Revising draft, supervision, and conceptualization.
Footnotes
Author Disclosure Statement
The authors declare that they have no financial or personal relationships with people or organizations that could inappropriately influence our work. There is no professional or other personal interest of any nature or kind in any product, service, and/or company that could be construed as influencing the position presented in, or the review of, the article entitled, “Applications of Additive Manufacturing in Inhalation Therapy.” This article does not have financial or other interests with any individuals or organizations.
Funding Information
This work did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.