
Abstract
Background:
Biobanks often lack standard mechanisms to keep donors connected to their biospecimens, reflecting a broken feedback loop that compromises trust, engagement, and scientific progress. Decentralized biobanking empowers patients to track their donations throughout the research journey, supporting personalized feedback and research collaboration via a privacy-preserving blockchain network. This case study explores operational feasibility of implementing decentralized biobanking for a large breast cancer biobank at a US academic medical center.
Methods:
A mixed-methods case study of the groundwork, implementation, and stakeholder feedback for a real-world decentralized biobanking app pilot was conducted. Biobank members were recruited from February to April 2023. Operational feasibility was assessed via analysis of institutional stakeholder perspectives, pilot engagement, and de-bi app activity.
Findings:
Physicians and other biobank stakeholders surfaced challenges surrounding managing expectations, balancing empowerment with clinical and research workflows, and navigating power dynamics between patients, physicians, scientists, and leadership. A total of 1080 participants enrolled over 10 weeks, including nearly 10% of the biobank with about 4000 biospecimens. During the pilot, biobank enrollment increased 65% versus the prior year, and there were no biobank withdrawals during or within 1 year following the pilot (p < 0.001 for both). The app, which facilitated biospecimen tracking and research engagement, was downloaded by 405 users. A total of 140 users tested the blockchain component, with 89% successfully claiming a nonfungible token representing their unique, immutable connection and access to donated biospecimens. Feedback was solicited to inform potential process improvements and risk assessments related to public relations, systems infrastructure, and ethical governance, illuminating next steps.
Conclusions:
We established operational feasibility for the first step toward decentralized biobanking, informed by requirements to manage expectations, workflows, and power dynamics. Our technical solution demonstrated robust participant engagement and compatibility with established biobanks, suggesting potential to build trust and align incentives and identifying next steps for communications, sustainability, and governance.
Keywords
Background
Biobanks acquire, store, and distribute biospecimens, such as tissue and blood from clinical procedures, for biomedical research.1,2 Typically, a one-time signature or waiver of consent grants broad permissions for biospecimen research, whereas donors’ identities are removed to protect privacy. 3 Under this model, there are no expectations or standard mechanisms for keeping individuals informed regarding the collection and use of their biosamples. 3 This broken feedback loop between patients and science undermines trust and disincentivizes research engagement, especially for marginalized populations.4,5 Continued reliance on outdated paradigms of deidentification and prospective informed consent is not only ethically insufficient in the era of mobile computing—it reinforces an unsustainable biobanking ecosystem that hinders data linkage, slows discovery, and misses opportunities to save lives.6–10
Interventions have sought to address different aspects of the problem, with notable efforts to enhance participant and community engagement.11–13 Digital solutions have been introduced to support patients’ rights to opt out or dynamically withdraw consent.14,15 Some biobanks build portals to “return results” that may be clinically actionable, for example, genomics.16,17 Others report aggregate-level progress and publications via newsletters or websites.18,19 Public and private marketplaces have been developed to match scientists with unmet biospecimen demand to biobanks with underutilized supply.20,21 National and international consortia have advanced infrastructure linking patient data, biospecimens, and derivatives across institutions.22–24 However, these well-intended efforts primarily address only a subset of biobank stakeholders and incur significant costs, and none have proved sufficiently valuable, sustainable, or scalable.25–27
Blockchain technology—an immutable, time-stamped shared ledger that decentralizes storage, verification, and exchange of digital data—has been proposed for biobanking solutions ranging from consent to biospecimen ownership.28–32 Building on broader ethical and sociotechnical shifts toward decentralization, 33 blockchain transfers decision-making power and ownership from centralized authorities to local, peer-to-peer networks reinforced by democratic consensus while maximizing security, thus enabling users to build cumulative layers of value.32,34–36 Despite their promise, blockchain-backed biobanking applications have functionally overlooked dimensions of the broader ecosystem in which they are implemented, 37 thus failing to sustainably align stakeholder incentives.38–40
To overcome these limitations, we are advancing decentralized biobanking as a solution that connects donors, biospecimens, biobanks, scientists, and physicians in a holistic biomedical metaverse (“biomediverse”).41,42 Our initial step toward decentralized biobanking is a patient-centered mobile application for donors to track their biospecimens, stay informed, and engage throughout the research lifecycle. The app lays the foundation for future decentralized governance by establishing ongoing, personalized communication between donors and biobanks. With patients and their biospecimens reunited, the decentralized biobanking platform can support the stepwise addition of mechanisms to facilitate shared allocation decisions, peer-to-peer communications, and efficient distribution of recognition, results, and other research benefits. 43
In this case study, we explore the operational feasibility of implementing a decentralized biobanking app for donor sample tracking for a breast cancer biobank. Building on our prior technical article detailing the app’s piloted development and deployment, 44 we provide expanded context on stakeholder requirements; explore quantitative pilot experiences encompassing app use, impacts on biobank enrollment, and blockchain proof-of-concept; and reflect on next steps.
Materials and Methods
Approach
Our approach is summarized in Figure 1, which illustrates the potential for decentralized biobanking to close the feedback loop between patients and scientists. Detailed descriptions of the app’s blockchain integration, architecture, and system components have been reported elsewhere. 44 Briefly, the mobile app integrated with existing institutional laboratory information management systems and leveraged a privacy-preserving blockchain infrastructure utilizing nonfungible tokens (NFTs). NFTs are unique, tamper-proof digital assets represented on a blockchain. 45 In our application, NFTs represent secure, nontransferable links between donors, their deidentified biospecimens, and associated research protocols, facilitating personalized updates without compromising confidentiality.5,46
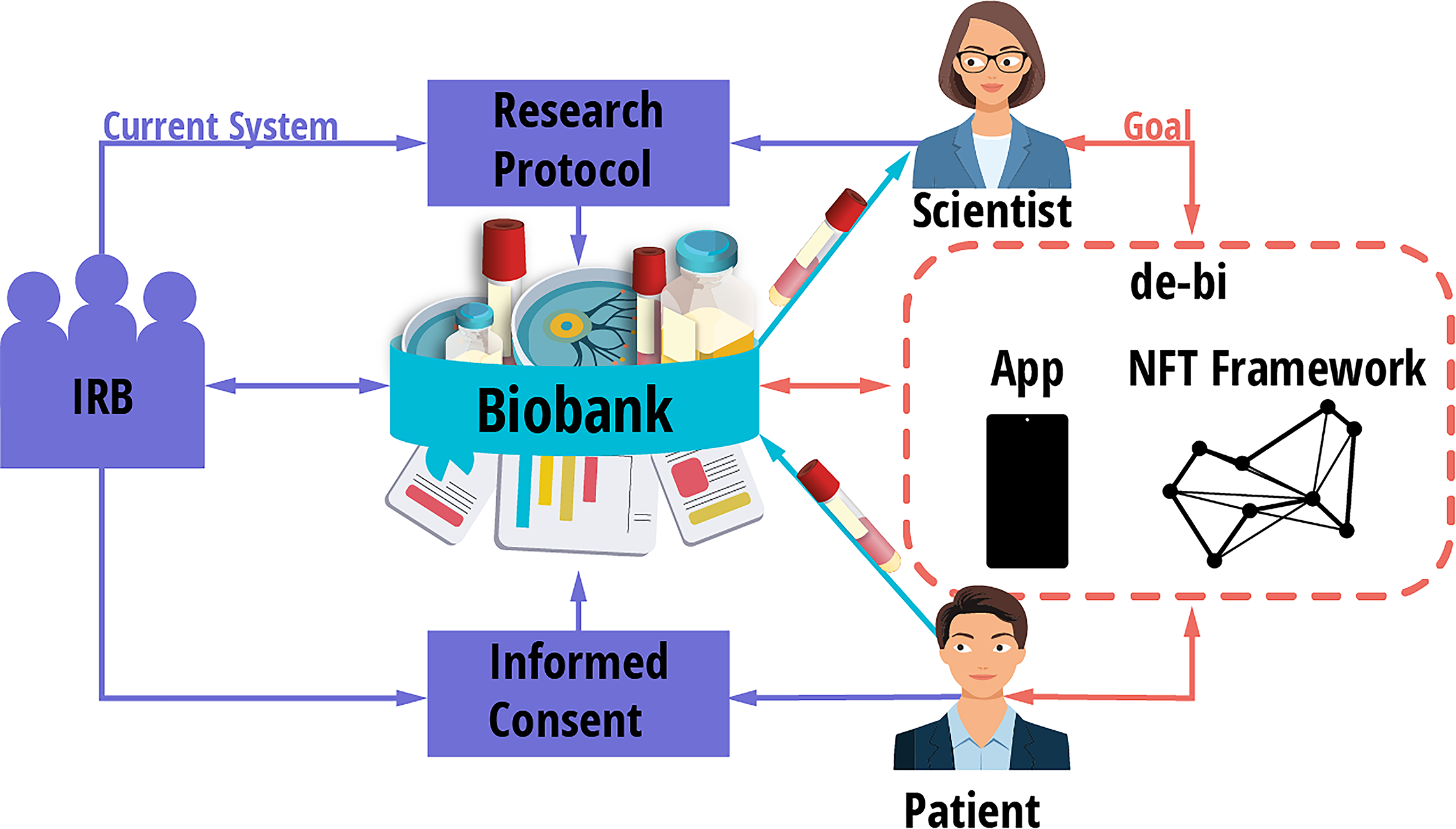
This diagram illustrates a traditional biobanking platform, wherein Institutional Review Boards approve biobanking protocols, patients provide prospective broad informed consent, prior to donating specimens, and scientists submit research protocols, allowing them to withdraw specimens from the biobank for designated purposes. It indicates the broken feedback loop between patients, biobanks, and scientists under the current system, as well as how decentralized biobanking “de-bi” may be implemented for existing biobanks, providing a privacy-preserving platform that combines a specimen tracking app with an NFT framework. NFT, nonfungible token.
Biobank context
As described in our prior technical feasibility study, the de-bi app was designed, developed, and piloted in the Breast Disease Research Repository (BDRR), a large university breast cancer biobank. Biobank consent is typically administered as a follow-on to surgical consent. Approximately 95% of those offered BDRR consent agree to participate; however, just 40–50% of eligible cases are enrolled, as surgeons do not universally perform biobanking consent. Over 10,000 consented to the BDRR between 2006 and 2023. Henceforth, we refer to the BDRR as “the biobank” and those who consented to the BDRR as “biobank members.” Biobank members are predominantly White (90.3%) and female (99.6%).
Biobank membership does not guarantee that biospecimens will be collected or that collected biospecimens will be utilized. As of May 4, 2023, nearly 61,000 biospecimens had been collected from 3940 members (mean = 15.5, range: 1–99 biospecimens/contributor). At that time, 9.6% of biobank biospecimens (5875/60,974) had been distributed to 45 principal investigators under 110 research protocols. See Supplementary Table SA1 for additional demographics and biospecimen inventory.
Case study methodology
We employed a mixed-methods case study approach to understand the affordances and constraints of the biospecimen supply chain, engage in participatory design with stakeholders, and execute a pilot of a de-bi app compatible with resources and regulatory frameworks.44,47 From 2021 to 2023, we performed ethnography of the breast cancer biobank, including site visits and participant observations, semistructured interviews, stakeholder alignment exercises, workshops, focus groups, presentations, and community engagement within or proximal to the breast cancer service line.
We engaged frequently with cancer care physicians; biobankers; scientists; research staff; ethics and compliance officers; nurses; IT and computer science experts; and university, hospital, and cancer center leadership. In 2023, we deployed the pilot and presented the live app and preliminary pilot data to biobank stakeholders. Multimodal qualitative data were captured systematically from stakeholder engagement, workshop archives, field notes, interview records, written correspondence, documentation, internal grant awards, protocols, and transcribed recordings of workshops and app demonstrations. See the “Human Research” section for all relevant Institutional Review Board (IRB)/QI protocols. 48
App design, development, and key features
Our software platform integrates with biobank databases to provide passive transparency for biospecimen donors without disrupting biobank workflows. 44 Technical details, participatory design, and usability testing are reported elsewhere.44,47 To summarize, privacy-by-design ensures compliance with preexisting biospecimen collection protocols, institutional biobanking regulations, and hospital policy. 44 A user-friendly app was designed utilizing anonymous biospecimen and organoid data from the breast cancer biobank and then validated via research surveys and interviews with the respective donor population. 47 The four key app screens were biowallet, biobank, labs, and profile (Fig. 2). Additional details on the app screens can be found in the Supplementary Material.

The four contexts introduced by the decentralized biobanking “de-bi” app and corresponding features providing community-level and personal-level transparency in an accessible manner, with unprecedented direct engagement of a biobank donor population. Reprinted from Sanchez et al., 2025, with permission. 44
Pilot procedures
English-speaking adults were eligible. Biobank membership was not required for participation in app testing, although feedback about personal biospecimens was limited to co-enrolled individuals. Recruitment occurred from February 16 to April 30, 2023, primarily via email and printed flyers. See Table 1 for demographics of pilot participants versus the biobank membership and Figure 3 for pilot workflow.
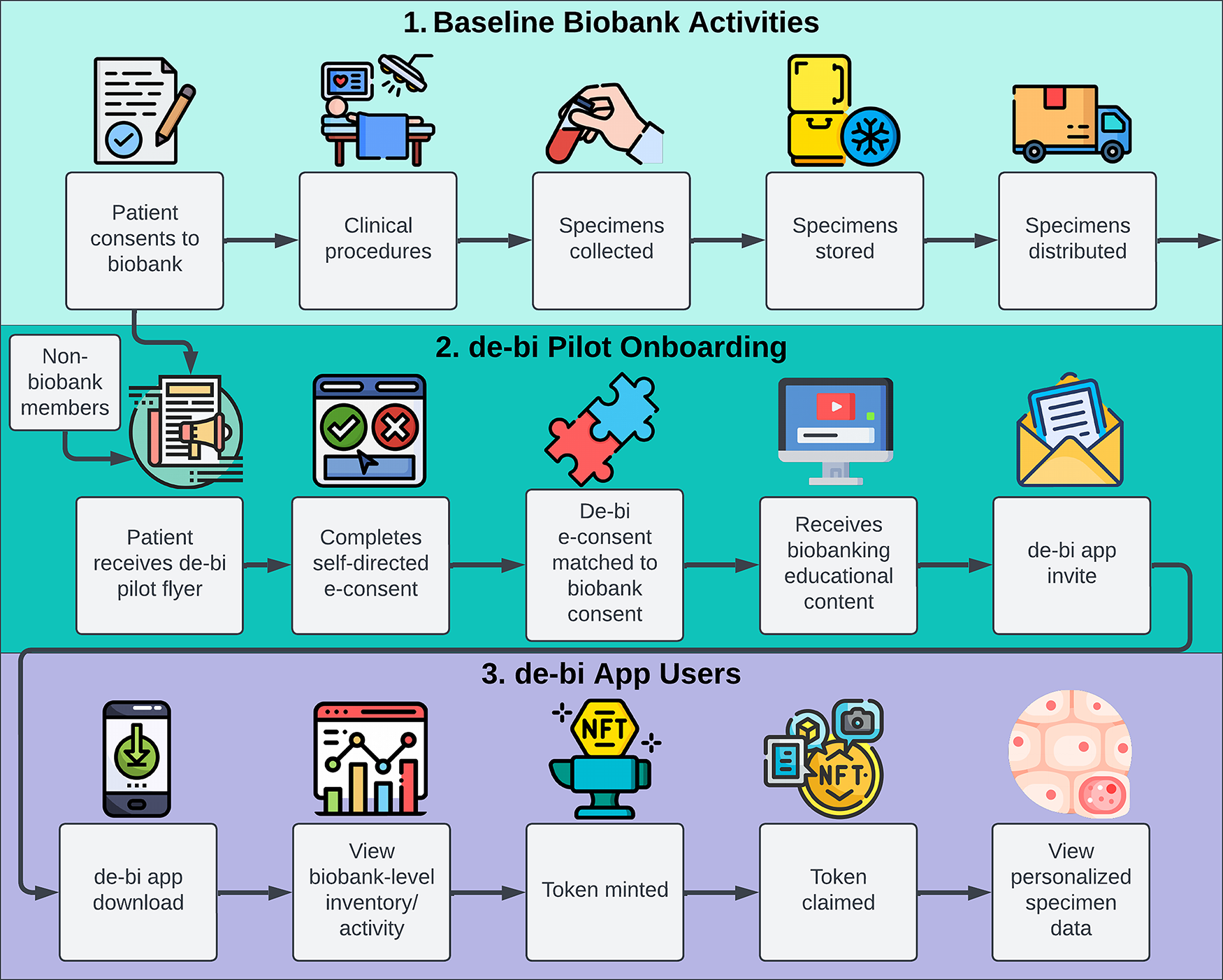
Retrospective and prospective recruitment of members from the source biobank for the pilot study, demonstrating how the de-bi app pilot and electronic consent process were integrated with the ongoing biospecimen collection activities. Participants who joined the pilot who were not consented biobank members (see row 2, far left) were able to participate in the pilot after receiving electronic or paper fliers from patient advocates, breast cancer clinic notices, although personalized specimen data were only available to co-enrollees of both the biobank and de-bi pilot protocols.
Demographics of de-bi Pilot Participants vs Full Breast Disease Research Repository Population
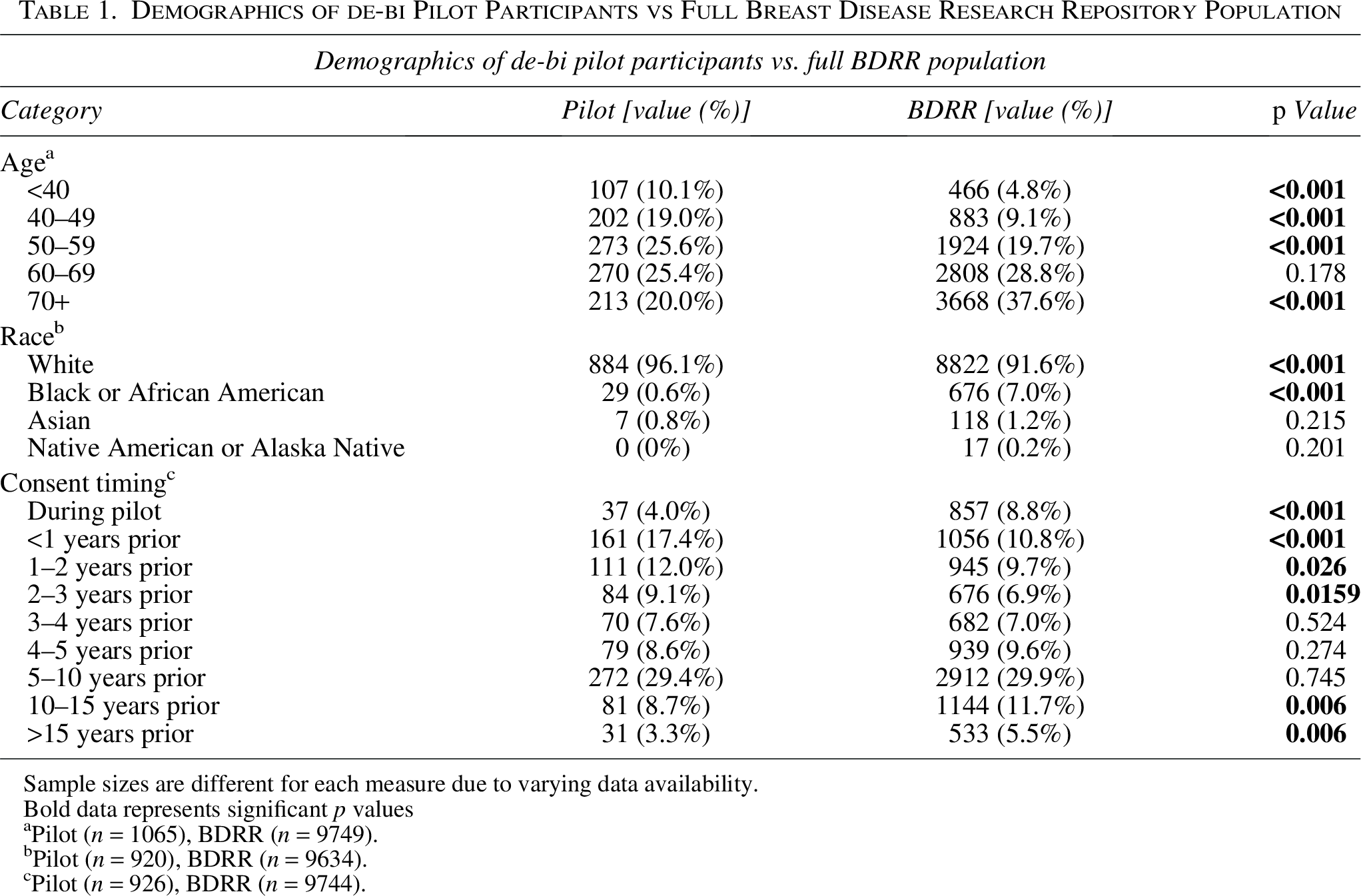
Sample sizes are different for each measure due to varying data availability.
Bold data represents significant p values
Pilot (n = 1065), BDRR (n = 9749).
Pilot (n = 920), BDRR (n = 9634).
Pilot (n = 926), BDRR (n = 9744).
App invites were distributed in batches. After downloading, users entered their name and birthdate, triggering verification of biobank membership (details available in the Supplementary Data). This was followed by matching donors to respective biospecimens via a unique anonymous study ID, which was linked to their app account. Participants were informed that finding and linking their biowallets to biospecimens may take up to 2 weeks.
Concurrently, biowallet NFTs were minted for each donor with biospecimens. Emails notified participants when their NFT was available, prompting login, whereupon the user experience simulated token-gated access to the biowallet and biospecimen data. In the interim, participants received access to educational materials, including an app user manual, links to video walkthroughs, and invitations to virtual and in-person orientation sessions. These resources stressed limitations, including the possibility of not having biospecimens banked or distributed, and limitations on available biospecimen information. App onboarding was aided by IT support.
Data analysis
We provide descriptive statistics from the quantitative datasets. Two-sided single rate ratio Z-tests, two-sided Z-tests for mean, and negative binomial regression were used to assess the impact of the de-bi pilot on biobank enrollment. Two-sided binomial exact and Fisher’s exact tests were used to evaluate the pilot’s impact on consent withdrawal. Emerging themes from qualitative sources were analyzed with grounded theory and triangulation to integrate insights. 47 Representative, deidentified quotes were selected to capture the full range of professional perspectives that emerged. Participant perspectives are addressed elsewhere.26,32,33
Findings
Requirements gathering: “how might we” implement decentralized biobanking?
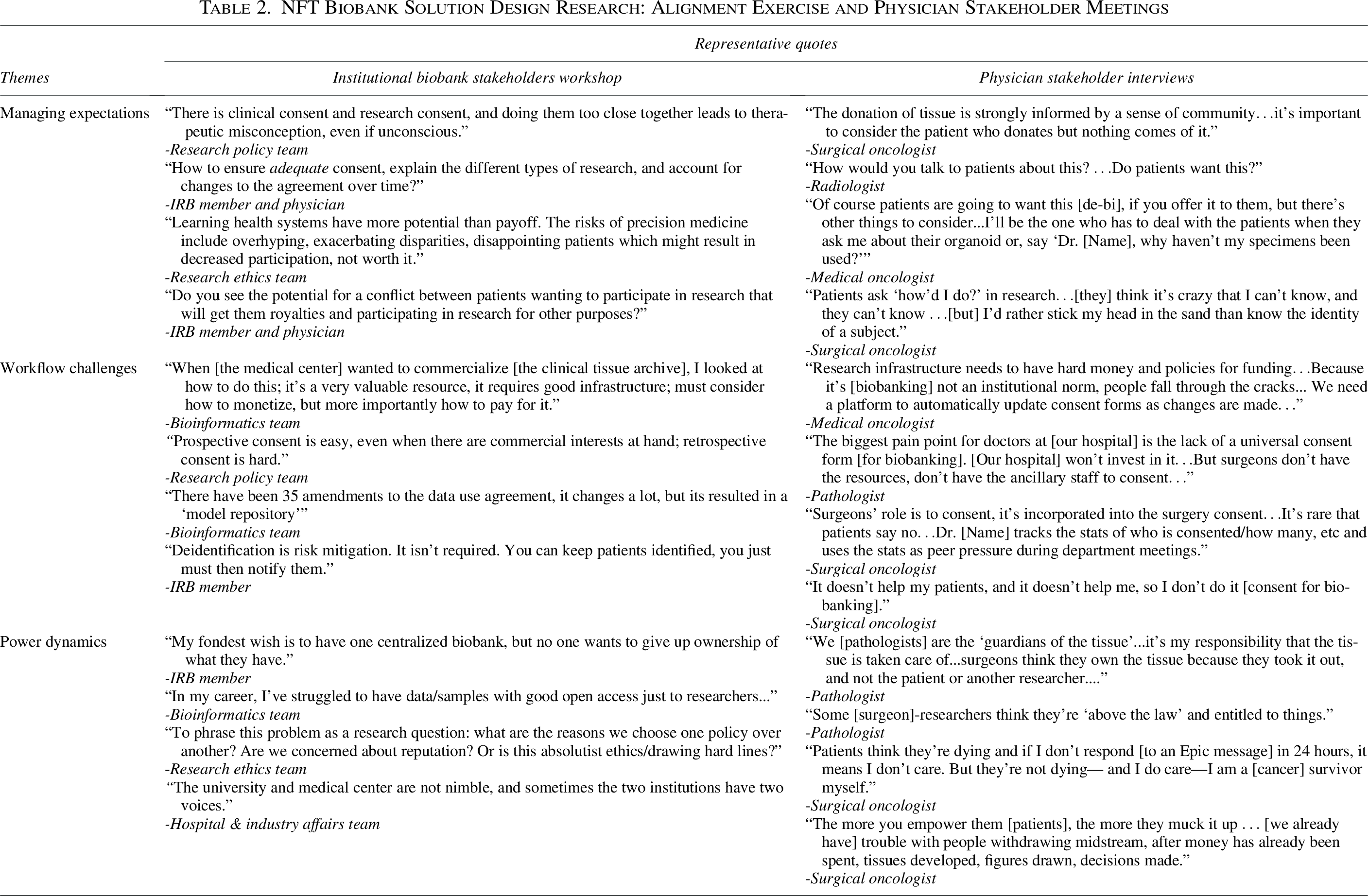
Table 2 highlights selected, representative quotes from a design workshop held with institutional biobank stakeholders (n = 10), during which the NFT-backed app prototype was demonstrated, 46 complemented by quotes from physicians (n = 10). Key themes surrounded managing expectations, workflow challenges, and power dynamics.
NFT Biobank Solution Design Research: Alignment Exercise and Physician Stakeholder Meetings
Managing expectations: “how would you talk to patients about this?”
Biobank leadership highlighted challenges for therapeutic misconception, particularly for biospecimens collected from clinical procedures. They noted the possible mismatch between anticipated and actual impact of research contributions, with potential for “disappointing patients which might result in decreased participation” as a consequence of revealing details of the biobanking supply chain and research process, “warts and all.” Early stakeholder interviews identified anxieties regarding patients who may consent, but never have biospecimens collected, or whose long-frozen biospecimens may be “like leftovers, picked at, but mostly forgotten.”
Clinicians broadly agreed that “patients are going to want this [sample tracking],” but they were apprehensive about how increased transparency might create duties to explain and interpret research processes and results. For example, a surgeon-scientist noted, “Patients ask, ‘how’d I do?’ in research…think it’s crazy that I can’t know and they can’t know…[but] I’d rather stick my head in the sand than know the identity of a subject.” Meanwhile, institutional leadership mused about the “need to consider public expectations of NFTs and blockchain,” and potential conflicts of interest, as in “How does commercialization fit into existing schemes of altruistic donation?”
Workflow challenges: “it doesn’t help my patients, and it doesn’t help me, so I don’t do it.”
Embedding biobank supply chains into clinical service lines demands standard procedures, integrated workflows, resources, funding, regulatory approvals, and coordination among many stakeholders, making operations vulnerable. Informed consent and institutional infrastructure were central challenges. For physicians, sample collection was a “nice to have,” if it could be done without disrupting clinical activities. For basic scientists, the “biobank is a lifeline.” Sample access requires “a good relationship with clinicians, [but] they don’t think it’s important, it’s not their job.”
In the pilot setting, it was “the surgeon’s role to consent,” but a pathologist noted, “the biggest pain point for doctors at [our institution] is the lack of a universal consent form…but surgeons don’t have the resources.” From the institutional perspective, “Prospective consent is easy, even when there are commercial interests at hand; retrospective consent is hard…some draw a hard line and say, ‘we won’t use old samples/data,’” and IRB leadership struggled with, “How to ensure adequate consent…and account for changes to the agreement over time?” An oncologist noted, “Research infrastructure needs to have hard money and policies for funding…Because it’s [biobanking] not an institutional norm, people fall through the cracks.”
Power dynamics: “who owns the tissue?”
Experts described a “Groundhog Day” of tension in which the hospital and affiliated university repeatedly fought over rights to control and profit from the biospecimen supply chain. Hospital leadership noted, “Sometimes the two institutions have two voices.” Frictions were exacerbated by differing values surrounding industry relations, with some trying to build a reputation for successful ventures and others fearing reputational damage from the same, invoking local headlines decrying, “How dare you make so much money?” Justifying resistance to monetization, a biobanker affirmed, “Patients donated their samples to be used for research, not sold for profit.” Put another way by a senior innovation officer, commercialization is “not the university’s business model—we rely on grants.” Pathology, surgery, and medical oncology departments were similarly described as “having different business models.”
Stewardship and rights to dictate the fate of biobank assets appeared to fall into the cracks between policies, norms, and powers across the academic medical center. Emphasizing this point, a cancer center leader posed the rhetorical question, “Who owns the tissue? The PI? The hospital, the university, the cancer center? What about the funders? What if it’s a private foundation?” Ambiguous ownership, coupled with burgeoning market opportunities, contributed to the “patchwork of workarounds,” wherein biospecimens are leveraged in one-off commercial collaborations, facilitated by “no one knowing what we actually have, or what it’s being used for.” Likewise, an IRB member summarized years of attempts to unify the university’s many siloed biospecimen collections, noting that “…no one wants to give up ownership of what they have.”
Decentralized biobanking was seen as empowering for patients but thereby seeded concerns about potential disruption of “researcher privacy,” academic freedom, and operational efficiency. Multiple senior investigators expressed the imperative to maintain control of their labs, for example, “I don’t need backseat drivers in my research.” Several worried that implementing transparency may provoke “trouble with people withdrawing midstream.” An ethics leader wondered about how engaging donors in this manner might “create pressures or new feedback loops?” Stakeholders recognized that providing transparency regarding donated biospecimens may have implications for power relations. Some focused on potential challenges for existing ownership models, whereas others found intuitive appeal in “the model of patient ownership of data…[although] the idea runs into legal interference and ethics barriers.” 49
Pilot participation
Pilot recruitment, consent, and app onboarding, and participation, biobank enrollment, and withdrawal details from before, during, and for 1 year following the pilot implementation are shown in Figure 4 and Supplementary Table SA2.
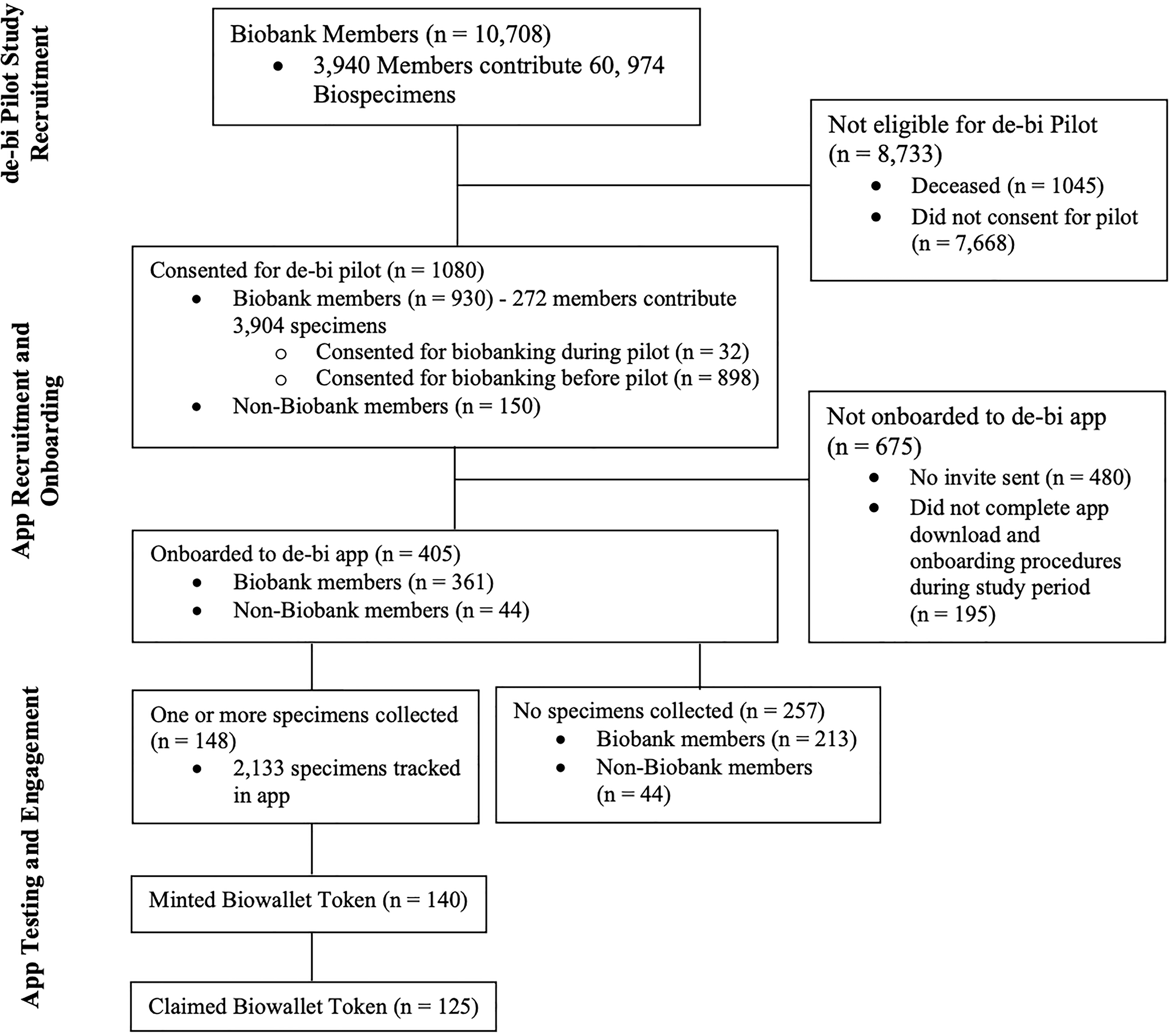
Decentralized biobanking pilot consort study outline from pilot recruitment to app onboarding, testing, and engagement.
Biobank donor recruitment
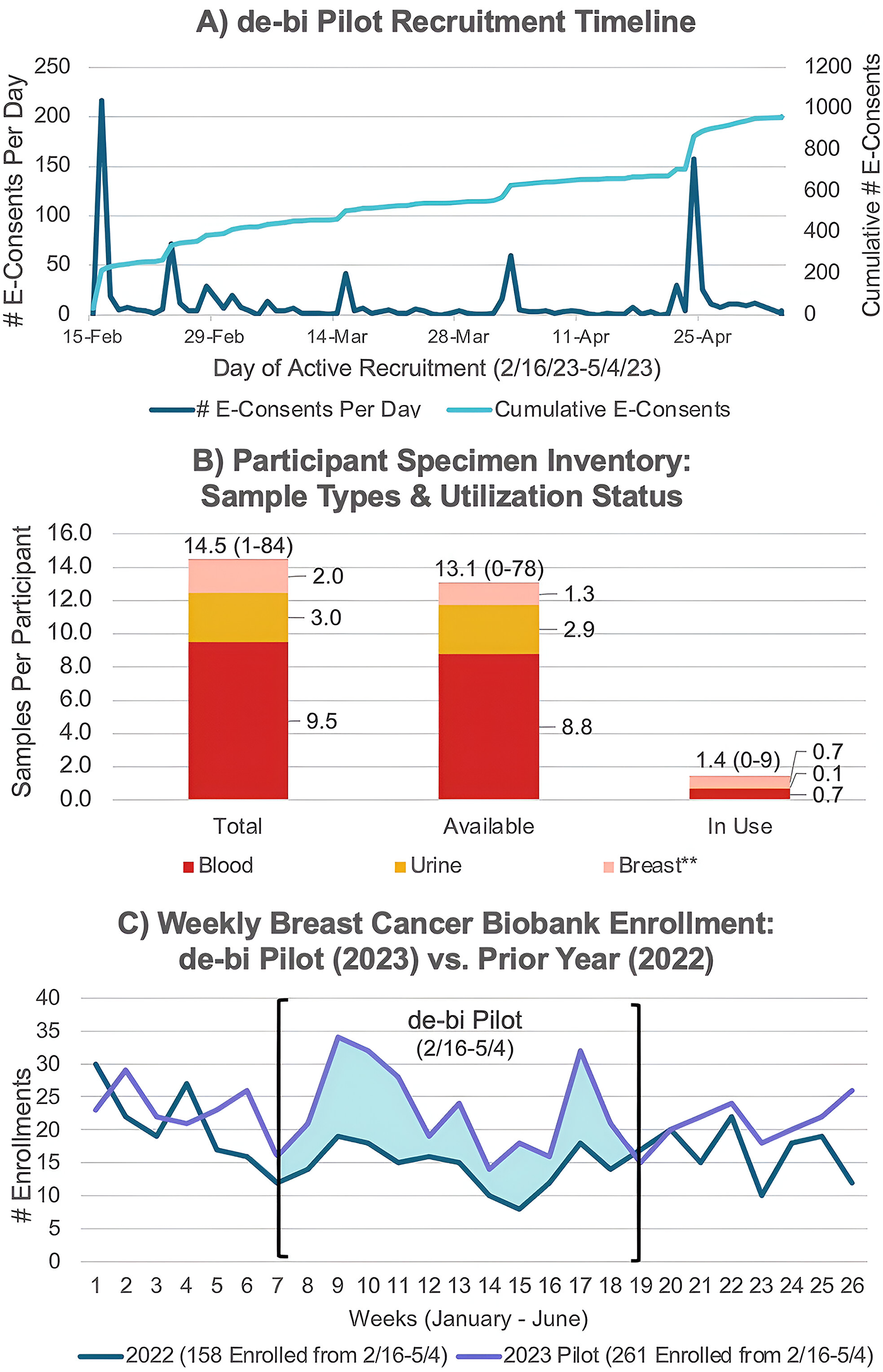
Over 10 weeks (2/16–5/4/2023), 1080 participants enrolled in the pilot (Fig. 5A). In total, 930 (86%) were confirmed biobank members. The mean age of pilot participants was 58 (range: 21–96), and 99% were women; see Supplementary Table SA3 for additional demographics. Among pilot participants, 32 enrolled in the biobank during the pilot, whereas the remainder were legacy biobank members. Among participants co-enrolled in the biobank, 29.2% (272/930) were linked with 3904 biospecimens (additional data available in the Supplementary Data). Figure 5B represents a descriptive snapshot of biospecimen status as visible to app users. Note: pilot participants could not influence biospecimen allocations via the app, although prior de-bi prototypes demonstrated how this feature may be enabled in the future.27,30
Biobank participation during pilot
From 2016 to 2022, excluding 2020, there was an average of 196 biobank consents during the corresponding 10-week pilot timeframe versus 261 in 2023, a 33% increase (p < 0.001). Compared with 2022, total biobank consents were 65% higher during the pilot (261 vs. 158, p < 0.001), and weekly biobank consent rates nearly doubled (23.6 vs. 12.3, p = 0.003; Fig. 5C). Biobank consent was stable in the year following the pilot (p = 0.862).
Pilot impact on biobank withdrawal
At baseline, biobank withdrawal is low, at 0.28% (28/9,881) of total enrollees. Among historical withdrawals, 10 (35.71%) were within 1 week of initial biobank consent, 22 (78.57%) within 1 month, 26 (92.86%) within 1 year, and just 2 (7.14%) over 1 year later. There were no withdrawals from the biobank during or in the year following the de-bi pilot (p < 0.001). Among the 5 years with over 1000 enrollments (2016–2018 and 2022–2023), 2023 was the only year with zero withdrawals (p = 0.028).
de-bi app activity
We briefly summarize below the key metrics described in our prior technical report to contextualize app engagement. 44 Approximately 600 app invites were distributed, with 405 downloading and completing app registration.
Biospecimen tracking
The “biobank” displayed 60,974 biospecimens from 3940 unique donors collected from February 1995 to May 2023. Around 318 new biospecimens were added during the pilot. Of biobank members using the app, 148/361 (41.0%) had their “biowallet” populated with a total of 2113 biospecimens (mean 14.4, range: 1–84), including 1414 blood, 419 urine, and 296 breast tissues. Additional details are available in the Supplementary Data.
Research engagement
Virtual “labs” included subpopulations for app users with “donor labs” representing six common diagnoses (e.g., ductal carcinoma), where individuals could learn about all donors, biospecimens, and research protocols relevant to their condition. App users tracked their biospecimens into 22 “scientist labs” and 38 unique research protocols, viewing a quantified overview of biospecimen collection and distribution activity. “Profiles” were completed by 153 users, annotating 886 biospecimens, including 760 “available” biospecimens.
Biowallet nonfungible token engagement
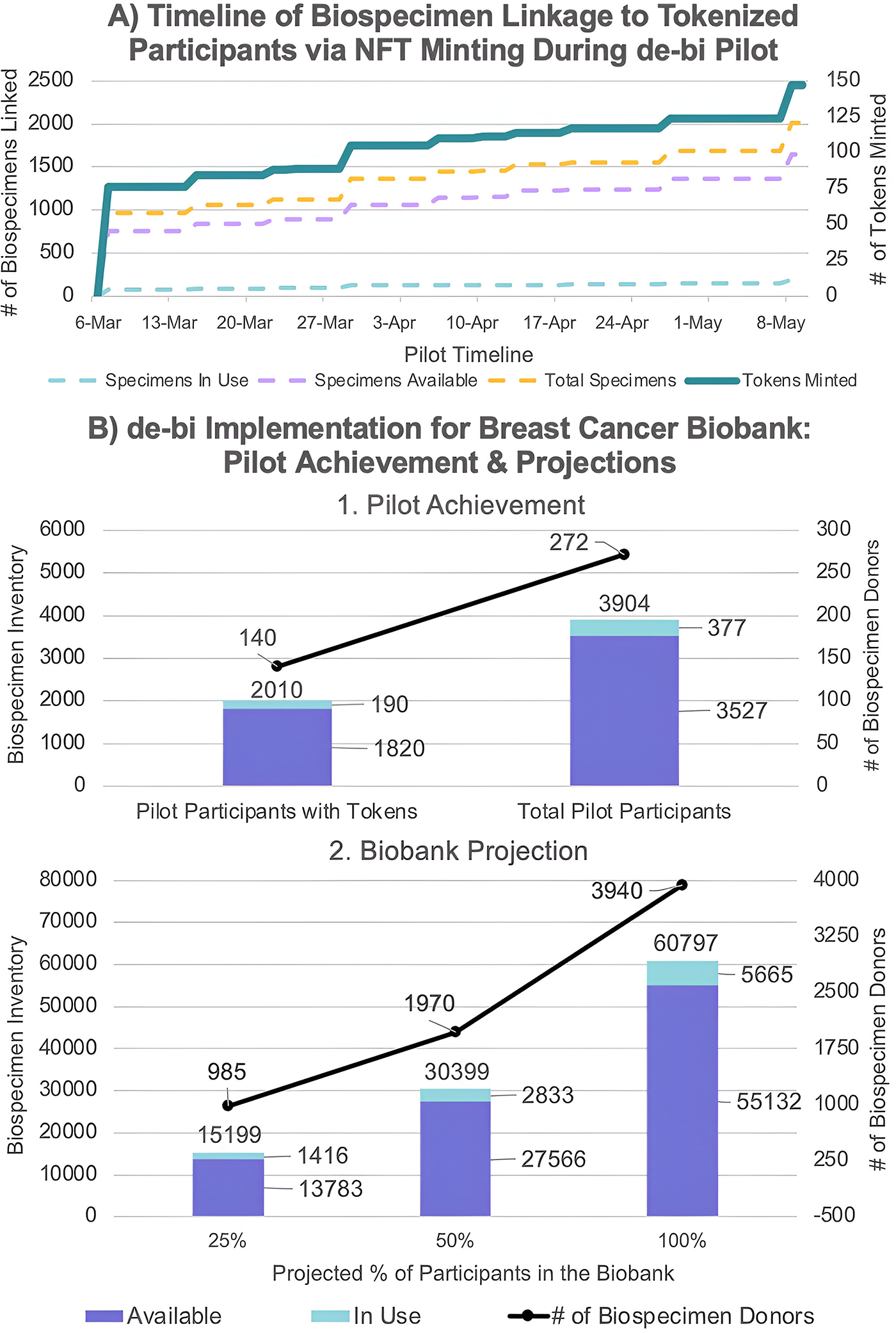
App users with biospecimens were eligible for biowallet NFTs. Of 148 app users with biospecimens, 140 initiated the biowallet token minting process. Of 140 tokens minted, 125 (89.3%) users returned to claim their tokens (median time = 1 day). Figure 6A illustrates NFT minting and access to biospecimens in participants’ biowallets over time. Figure 6B shows pilot achievement and projections for the number of biospecimens reconnected to respective donors. The piloted app was not configured to capture the frequency of page views following initial claiming. Details on biowallet claimants versus nonclaimants can be found in Sanchez et al. 44
Pilot and app demonstration feedback: Navigating implementation and next steps
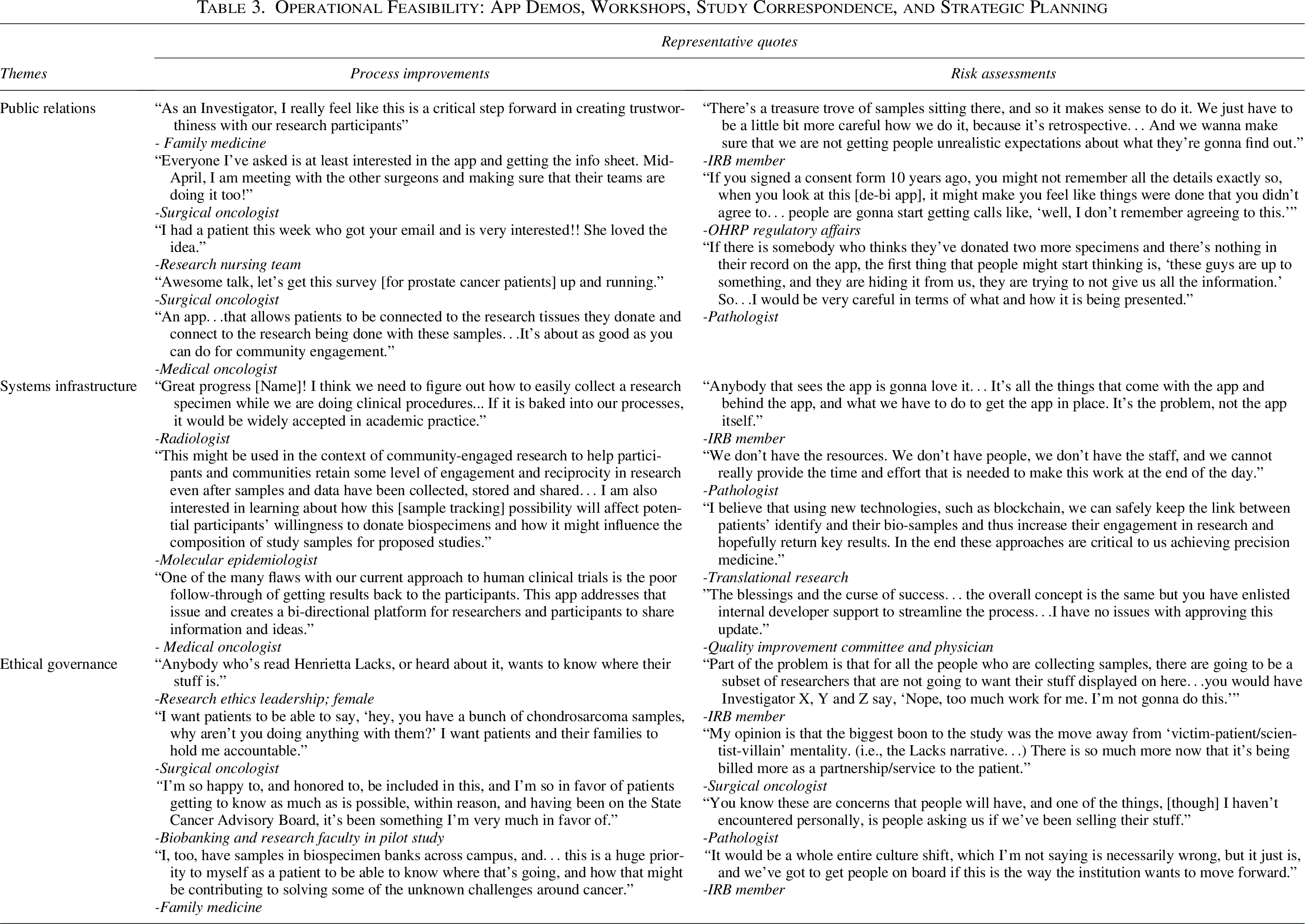
Operational feasibility was explored via representative quotes from a biobank pilot stakeholder workshop on next steps (n = 10) as well as physician, scientist, and biobanker engagement and correspondence during pilot execution and app presentations (n = 9; Table 3). All stakeholders whose perspectives were included viewed a live demonstration and/or tested the app on their personal device. Themes identified related to public relations, systems infrastructure, and ethical governance.
Operational Feasibility: App Demos, Workshops, Study Correspondence, and Strategic Planning
Public relations
Physicians highlighted the importance of implementing transparency of biobanking practices, especially for minority patients, sharing, “…this is a critical step forward in creating trustworthiness with our research participants.” A physician described the de-bi app as, “about as good as you can do for community research engagement.” Meanwhile, biobankers and regulatory personnel were apprehensive, stressing imperatives to “be very careful in terms of what and how it is being presented,” and “make sure that we are not getting people unrealistic expectations.” They expressed concerns about how the app may lead to misunderstandings which may fuel bad press, noting, “this is something that could be really great, or it could just blow up in our faces.”
Positive reception among participants and physicians stimulated prostate, sarcoma, and ovarian cancer biobanks to seek funding to expand the pilot to their use cases. Several suggested that our approach “will help us win grants,” by differentiating their community outreach and engagement strategy. The potential to enhance donor relations with disease-focused foundations was highlighted, for example, by a physician-authored grant application, which asserted, “de-bi will bring patients and their families closer to the research that would not exist without their generosity.”
Systems infrastructure
The broken feedback loop between patients and science was identified as, “one of the many flaws with our current approach,” framed as an infrastructure deficit that individual investigators and time-delimited grant-funded projects were not optimally suited to solve, notwithstanding many laudable efforts. The de-bi app was seen as an opportunity to embed community-engaged praxis, which may in turn “affect potential participants’ willingness to donate biospecimens and…influence the composition of study samples.”
Yet, operational barriers included lack of resources, staff, and time constraints. A biobanker noted limitations of the pilot, stating “we cannot really provide the time and effort that is needed to make this work,” emphasizing the imperative to advance technical integrations with the legacy systems for sustainable, scalable implementation. Likewise, a physician leader expressed that, if de-bi was adequately integrated into biobanking norms and technologies at the institutional level, “it may be widely accepted in academic practice.” Some recognized that decentralized biobanking, as a patient-centered approach to health data infrastructure, was “ultimately necessary for precision medicine.”
Ethical governance
Decentralized biobanking was seen as “the right thing to do” and “an inevitable consequence of smartphones,” although implementation posed questions for governance paradigms. An IRB member noted, “there are going to be a subset of researchers that are not going to want their stuff displayed.” Biobankers worried about patients attempting to dictate biospecimen distributions, seeking reassurance that “it’s not a free-for-all.” By contrast, several physician-scientists welcomed involvement of donors in biospecimen stewardship, particularly for the rare disease community: “I want patients to be able to say, ‘Hey, you have a bunch of chondrosarcoma samples, why aren’t you doing anything with them?’” Ultimately, decentralized biobanking calls for “a whole entire culture shift,” and a well-delineated governance framework is needed, “to get people on board.”
Discussion
Pilot summary
Decentralized biobanking enables donors to track biospecimens throughout the research journey via user-friendly apps. This case study examines considerations, experiences, and feedback from the first live pilot of a decentralized biobanking app in a real-world breast cancer biobank. We establish the operational feasibility of integrating this solution with biobank databases to provide transparency for donors without unduly burdening institutional stakeholders.8,50–52 Stakeholders identified challenges including managing patient expectations, integrating with complex workflows, and navigating sensitive power dynamics.
Biobank members were onboarded retrospectively and prospectively. Enrollment was robust: about 10% of biobank members (n = 1080) joined over 10 weeks—more than 200 within 24 hours of the first email. Over 400 app users viewed biobank activity and tracked over 2000 personal biospecimens. Beyond “returning results,” our approach implements openness of research processes and personalized research subcommunities.12,13,53–56 We also demonstrate proof-of-concept for a blockchain-backed solution: nearly 90% of eligible participants claimed an NFT that recognized donor contributions and simulated token-gated access to personal biospecimen data.49,57
Pilot participants learned that most consented members do not have biospecimens collected, and that most biospecimens reside in long-term frozen storage.58,59 Concerns that such disclosure may provoke disappointment or anger, potentially leading to lower biobank enrollment or withdrawals, were not substantiated by the pilot experience. By contrast, weekly enrollment during the pilot increased significantly, nearly double from the prior year, and there were zero withdrawals from the biobank during or within 1 year afterward, significantly lower than historically predicted.
Although the reason for increased enrollment is unclear—and no concurrent interventions were deployed—this aligns with design literature and stakeholder insights that timely, personalized feedback about biospecimen donations can drive participation and engagement. Pilot fliers showing the biowallet app were posted in clinics, shared by patient advocates, and the app was demonstrated at the breast cancer tumor board before launch. Patients likely inquired more about donation, and physicians may have been more motivated to consent patients given the promise of personalized feedback. Stakeholders identified potential to restore trust, boost competitive funding applications, and facilitate precision medicine. 60
Limitations
Due to outsized enrollment, app invites were not available to all pilot participants. Technical advancements in institutional database integration, automation of blockchain interactions, and enhanced in-app notifications are needed for durable implementation. Ongoing research is exploring how transparency and tokenization impact participant trust and engagement, and methods for improving blockchain infrastructure, for example, via account abstraction.11,31,61
While email was effective for retrospective enrollment, further evaluation is needed to ensure inclusion and accessibility and to optimize prospective recruitment.62–64 Most pilot participants self-identified as White, reflecting challenges observed across biomedical research.62,65 While not unique to this study, this limitation highlights broader concerns about insufficiently engaging diverse patient populations. 66 Current work is examining how to ensure operational viability of our approach for diverse populations, institutions, geographies, and socioeconomic settings.
Specimen tracking for donors is a new paradigm with the potential to revolutionize the biobanking research ecosystem. By keeping donors in the loop, our approach reenvisions biobanking in line with the ethos, affordances, and economics of blockchain systems. Further innovations in ethical biobank market design and governance strategies are needed to promote trust and ensure that decentralized biobanking safely unlocks value while aligning individual priorities, institutional incentives, and collective interests.46,67,68
Conclusion
This case study explores the operational feasibility of implementing decentralized biobanking for biospecimen donors. We demonstrate how a sample tracking app may be integrated with institutional biobank databases without compromising established protocols, privacy, or workflows. Importantly, the pilot experience suggested positive impact on biobank donors and potential benefits for research, countering concerns about bad press and withdrawal. Further development of decentralized biobanking technology and strategic investment in necessary infrastructure are crucial for the sustainability and scalability of our proposed solution. Likewise, implementing biospecimen tracking for biospecimen donors calls for new models of shared governance and profit distribution from biobank research. Moving forward, we are creating tools for scientists and roadmaps for institutions to catalyze cultural transformation and democratize biobanking as a foundation for a structurally just biomediverse.
Human Research
Mixed-methods research results described herein are enabled by a combination of several IRB-approved human subjects research protocols, coupled with ethnography and participant observational methods, as supported by a comprehensive quality improvement protocol, as listed below. The participants in each of the protocols below provided informed consent or waived informed consent, in accordance with the respective protocols. Conflict of interest disclosures were included in all consent procedures and reiterated as appropriate at each virtual and/or in-person encounter.
IRB00019273—Nonfungible Tokens for Ethical, Efficient, and Effective Use of Biosamples (Johns Hopkins University) STUDY22010118—Patient Views, Preferences, and Engagement in Next-Generation Biobank Research (University of Pittsburgh). STUDY22020035—Decentralized Biobanking “de-bi”: Exploring Patients Interests in Feedback, Education, Follow-up, Engagement, and Tokens of Appreciation Regarding Biobank Donation via Mobile and Web Applications (University of Pittsburgh). STUDY19060196—Breast Disease Research Repository (BDRR): Tissue and Bodily Fluid and Medical Information Acquisition Protocol (04-162) (Hillman Cancer Center). QRC 3958—Patient-facing Biobank Platform Development QI Proposal for Beckwith Award–Breast Cancer Supply Chain Analysis, Biobank Token Model Development, and Initial Pre-Pilot Testing with UPMC Patients (University of Pittsburgh Medical Center).
Authors’ Contributions
M.G. conceived, designed, and participated in all aspects of the pilot, collected qualitative data, cleaned the quantitative and qualitative data, coded and synthesized qualitative data, reviewed and contributed to quantitative analyses, wrote initial draft, led revisions, and prepared as well as takes responsibility for the final article; A.D. performed literature reviews, collected and coded qualitative data, contributed to thematic analysis, contributed substantively to development, organization and revision of article drafts, and managed citations; E.B. led to the quantitative analysis, prepared quantitative tables and graphs of quantitative data, contributed to writing methods and results pertaining to statistical analysis, and facilitated qualitative analysis and preparation of tables and figures; W.L.S. led to the technical development and IT support for the pilot, developed, formatted and prepared the quantitative data, reviewed qualitative codes, and participated in data analysis and synthesis; R.C.M. provided critical guidance on pilot execution, preparation of figures/tables, and article development, organization, and structure. J.K. provided conceptual input and ethical oversight for the pilot study, contributed to synthesis and discussions of framing and presentation of data, reviewed and provided feedback on article drafts, and M.M. contributed to conception of the work, participated in review, performed analysis of quantitative data, helped synthesize qualitative findings, helped to clarify methods, and providing critical input across the discussion. All authors reviewed and approved final submission.
Footnotes
Acknowledgments
The authors would like to thank the patients, physicians, scientists, and biobankers in the pilot setting who made this work possible. The authors specially thank Arvind Duhan, MBA, whose support was instrumental in pilot execution.
Author Disclosure Statement
Several co-authors (M.G., W.L.S., J.K., R.C.M., and M.M.) are shareholders in de-bi, co., a company created to advance decentralized biobanking to empower patients, accelerate science, and realize precision medicine. The pilot study described here was not sponsored by de-bi, co.; however, detailed conflict of interest disclosures were incorporated in all informed consent forms, quality improvement procedures, and verbal disclosures were made throughout ethnographic work. Conflict of interest disclosures were disclosed in accordance with the pilot protocol, under conflict management plans, and the principal investigator on the de-bi app pilot protocol was nonconflicted.
Funding Information
Foundational research on decentralized biobanking was generously supported by a grant from Emerson Collective/Yosemite to Johns Hopkins Berman Institute of Bioethics. The pilot feasibility study described here was enabled by grants from the UPMC Beckwith Institute, which supported app production and integration with the institutional biobank, Pitt Chancellor’s Gap Fund, which supported blockchain designs and technical development. Additional labor, materials, and resources were provided by the University of Pittsburgh and UPMC-affiliated Institute for Precision Medicine, Magee-Womens Research Institute, and David Berg Center for Ethics and Leadership at the Katz School of Business.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.