
Abstract
Background
Articular cartilage injuries often heal with fibrocartilage rather than native hyaline cartilage, resulting in inferior biomechanical properties and increased osteoarthritis risk. Curcumin has anti-inflammatory and antioxidant properties that may support cartilage repair; however, clinical use is limited by poor bioavailability. Micellar formulations enhance systemic absorption.
Purpose
To evaluate the effects of orally administered micellar curcumin on structural and molecular markers of osteochondral repair in a rat distal femoral defect model.
Methods
Thirty-two female Wistar rats were randomly allocated to 4 groups (n = 8 per group). Standardized 2-mm osteochondral defects were created in the distal femur. Animals received 250 mg/kg/day micellar curcumin or distilled water for 30 or 90 days. Macroscopic repair was assessed using the International Cartilage Repair Society (ICRS) scoring system. Histological evaluation followed ICRS guidelines and was performed in a blinded manner by 2 independent observers (intraclass correlation coefficient ICC = 0.89). Immunohistochemical analyses included SRY-box transcription factor 9 (SOX9), collagen type I (COL I), collagen type II (COL II), aggrecan, and matrix metalloproteinase-13 (MMP-13).
Results
Curcumin-treated groups demonstrated significantly higher macroscopic and histological scores than controls, particularly at 90 days. Increased expression of hyaline cartilage markers (SOX9, collagen II, aggrecan) and reduced collagen I expression were observed in treated groups. MMP-13 expression did not differ significantly between groups.
Conclusion
Oral micellar curcumin enhanced structural and molecular parameters of osteochondral repair in this preclinical model. Further translational and clinical studies are required before therapeutic application.
This is a visual representation of the abstract.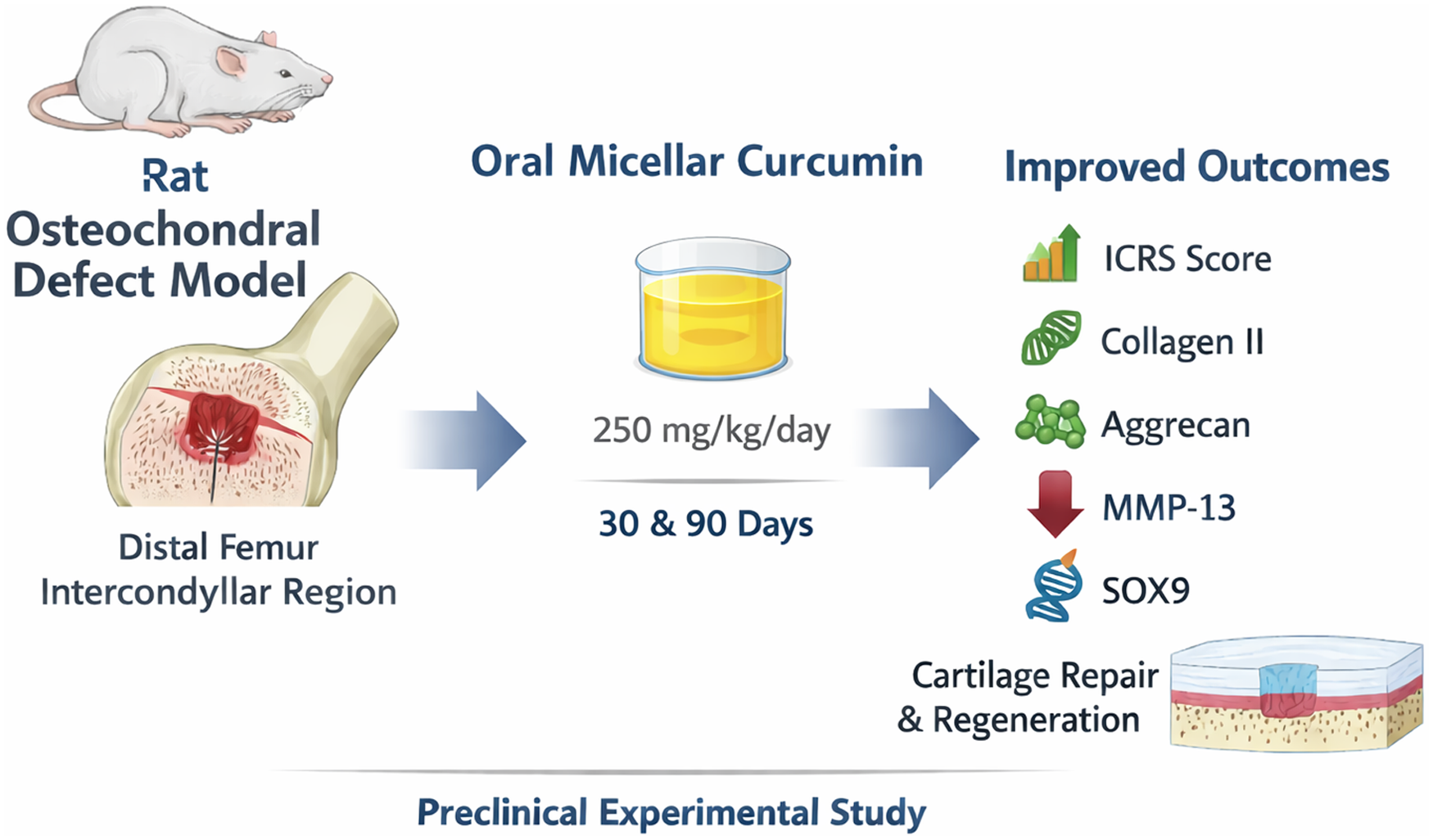
Keywords
Introduction
Articular cartilage injuries are prevalent and carry a considerable risk of progressing to osteoarthritis due to the tissue’s limited intrinsic healing capacity. Instead of regenerating hyaline cartilage, the reparative process often leads to fibrocartilage formation, which has inferior biomechanical properties and is more prone to degeneration. Osteochondral defects may arise from trauma, overuse, or conditions such as osteochondritis dissecans and are frequently encountered in athletes. 1
Treatment of these lesions aims to restore joint function and delay degenerative changes by promoting the regeneration of hyaline-like cartilage. While surgical techniques exist, they often fall short in terms of long-term outcomes and reproducibility. Consequently, there is increasing interest in adjunctive therapies to enhance cartilage repair. 2
Curcumin, the main polyphenol derived from Curcuma longa, has been widely studied for its anti-inflammatory and antioxidant effects, which are believed to support cartilage regeneration.3 -6 It modulates key inflammatory mediators such as tumor necrosis factor-alpha (TNF-α), interleukin-1 beta (IL-1β), and nuclear factor kappa B (NF-κB), and inhibits matrix-degrading enzymes such as matrix metalloproteinases (MMPs).7 -11 Moreover, curcumin enhances antioxidant defenses by upregulating enzymes such as superoxide dismutase (SOD) and catalase, thereby protecting chondrocytes from oxidative stress. 12
Curcumin has been explored using multiple routes of administration in both experimental and clinical settings. Intra-articular delivery of curcumin and curcumin-loaded nanoparticle formulations has demonstrated local anti-inflammatory and chondroprotective effects in osteoarthritis models, with improvements in cartilage structure and matrix integrity.6,13 Injectable scaffold-based and nanoformulated approaches have similarly shown potential in enhancing chondrogenesis and reducing cartilage degradation. 14 In addition, systemic and intravenous nano-curcumin formulations have been investigated to improve pharmacokinetics and bioavailability, particularly in early-phase clinical and translational studies.15,16 Clinical trials of enhanced-bioavailability oral curcumin have further supported its potential chondroprotective role. 17 Despite these advances, variability in systemic absorption and delivery efficiency remains a challenge.
However, native curcumin has poor bioavailability due to low solubility and rapid metabolism. 15 Micellar formulations have been developed to overcome these limitations, significantly improving curcumin’s systemic absorption and plasma concentrations. 18 These properties make micellized curcumin an appealing oral adjunct to conventional cartilage repair strategies.
The present study aimed to evaluate the effects of orally administered micellized curcumin on cartilage healing in full-thickness osteochondral defects created in the intercondylar region of the distal femur in a rat model.
Materials and Methods
Study Design
The study involved 32 female Wistar rats, aged 12 weeks, weighing between 275 and 315 g (mean: 295 g). Rats were housed in a controlled environment (22°C, 12-hour light/dark cycle) with ad libitum access to food and tap water. Animals were randomly divided into 4 groups (n = 8 per group). Full-thickness osteochondral defects were created in the intercondylar region of the distal femur on day 0. Evaluations were conducted at 30 and 90 days postoperatively, based on time points commonly used in the literature for assessing cartilage regeneration. 19
The required sample size was determined by an a priori power analysis using G*Power software (Universität Düsseldorf, Germany). Based on previously published data reporting differences in histological cartilage repair scores between treatment groups, a minimum effect size (f) of 0.40 was assumed.6,19,20 With a significance level (α) of 0.05 and a power (1-β) of 0.80, the total sample size required per group was calculated to be n = 7. To account for potential losses during the experimental period, n = 8 animals were included in each group.
The experimental protocol was approved by the Local Animal Experiments Ethics Committee of Istanbul Bağcılar Training and Research Hospital (HADYEK/2023-01; Approval No: 2023/37). All procedures were conducted in accordance with national regulations for laboratory animal care and complied with ARRIVE 2.0 guidelines.
Group Allocation
A total of 32 rats were randomly assigned into 4 groups, with 8 animals in each group. Group C1 (Curcumin – 30 days) received 250 mg/kg/day of micellized curcumin (NovaSOL Chemicals®, Belgium) via oral gavage for 30 days, after which samples were harvested. Group C2 (Curcumin – 90 days) received the same treatment as Group C1 for a duration of 90 days. Group K1 (Control – 30 days) received 250 mg/kg/day of distilled water via oral gavage for 30 days, and samples were harvested on day 30. Group K2 (Control – 90 days) followed the same protocol as K1 but for 90 days. Samples were collected at the end of each treatment period.
Randomization was performed using a computer-generated random number sequence prior to surgery. Group assignments were concealed using coded animal identifiers. Investigators responsible for macroscopic, histological, and immunohistochemical assessments were blinded to group allocation and were not involved in the randomization process.
Surgical Procedure
Rats were anesthetized using intraperitoneal injections of 10 mg/kg xylazine and 90 mg/kg ketamine. After shaving and antiseptic preparation with 10% povidone-iodine, a 2 cm longitudinal anterior incision was made over the right knee. A medial parapatellar approach was used to access the joint. Patella was dislocated laterally, exposing the femoral condyles. A 2 mm diameter, 1 mm deep cylindrical osteochondral defect was created using a low-speed drill

Osteochondral defect created in the intercondylar region of the rat distal femur.
Curcumin Administration
Micellar curcumin was used in this study due to its significantly higher bioavailability compared to native curcumin. In this formulation (NovaSOL®), curcumin is incorporated into surfactant-based nanosized micelles, enhancing aqueous solubility and intestinal absorption. Previous studies have demonstrated that micellar solubilization technology markedly increases systemic exposure and plasma concentrations compared to native curcumin.15,17,18,23
Curcumin was administered orally using a micellized liquid formulation at a dose of 250 mg/kg/day, in accordance with established literature and safety profiles for high bioavailability.18,23 Control groups received equal volumes of distilled water to mimic the same level of handling and stress

Oral administration of micellar curcumin via gavage.
The selected dose of 250 mg/kg/day was based on prior preclinical studies demonstrating anti-inflammatory and chondroprotective effects of orally administered curcumin formulations in rodent models.18,24 The micellar formulation used in this study (NovaSOL®) has been shown to significantly enhance systemic bioavailability compared to native curcumin.18,23 Using standard interspecies dose conversion based on body surface area (Km factor method), this dose corresponds to an approximate human equivalent dose of 40 mg/kg/day, which falls within the range evaluated in clinical trials of enhanced-bioavailability curcumin preparations.17,25
Sacrifice and Sample Collection
On day 30 or 90, animals were anesthetized as described. The distal femur was excised via a medial parapatellar approach, and animals were euthanized by cervical dislocation. The excised distal femurs were subjected to macroscopic evaluation

Excised distal femur and lesion site of the rat.
Macroscopic evaluation was performed under magnification using a surgical loupe to enhance visualization of the defect area. Although the defect size was 2 mm, this dimension is widely used in rat osteochondral defect models and has been evaluated in prior macroscopic scoring studies. 27 Macroscopic findings were interpreted in conjunction with histological data to ensure internal consistency between surface appearance and tissue architecture.
Histopathological Evaluation
Tissue samples were fixed in 10% formalin for 72 hours and decalcified in Morse solution. Samples were processed using standard histological protocols (alcohol, xylene, paraffin embedding), sectioned at 5 μm, and stained with hematoxylin–eosin (H&E), Masson’s trichrome (MT), periodic acid–Schiff (PAS), Safranin-O (SO), and Alizarin Red (AR). A comprehensive histological analysis was performed using multiple staining techniques to evaluate cartilage regeneration and tissue composition. H&E staining was used to assess general tissue architecture and cellular morphology. MT staining was employed to detect collagen fiber distribution and fibrotic changes. PAS staining was applied to visualize neutral polysaccharides and basement membrane structures. SO staining was used to evaluate glycosaminoglycan (GAG) content in the cartilage matrix. AR staining was performed to assess calcium deposition and tissue mineralization. 28
Histological evaluation followed the International Cartilage Repair Society (ICRS) histological scoring system. Histological scoring was conducted using the ICRS Visual Histological Assessment Scale, which evaluates parameters such as surface integrity, matrix staining intensity, cell morphology and distribution, structural organization, and integration with adjacent cartilage and subchondral bone. 29
Histological scoring was independently performed by 2 experienced histologists who were blinded to group allocation. All slides were anonymized prior to evaluation to ensure assessor blinding. Interobserver reliability was assessed using the intraclass correlation coefficient (ICC; 2-way random-effects model). The ICC value was 0.89, indicating excellent agreement between observers.
Immunohistochemical Evaluation
Slides were incubated with primary antibodies against SRY-box transcription factor 9 (SOX9), Collagen type I (COL I), Collagen type II (COL II), Aggrecan (ACAN), and MMP-13 at validated dilutions (SOX9: 1/250; COL I/COL II, ACAN: 1/100; MMP-13: 1/200). The avidin–biotin–peroxidase complex method was used with 3,3′-diaminobenzidine (DAB) chromogen and Gill’s hematoxylin counterstaining. Expression patterns were analyzed in a blinded fashion. 30
SOX9 is a key transcription factor in chondrocyte differentiation and cartilage regeneration. 31 COL II is characteristic of healthy hyaline cartilage, whereas COL I indicates fibrous tissue formation. 32 Aggrecan is essential for osmotic resistance and structural integrity; its decrease correlates with mechanical weakness. 33 MMP-13 is a matrix-degrading enzyme associated with COL II breakdown and cartilage degeneration. 34
Immunohistochemical scoring was likewise performed in a blinded manner using coded specimens.
Statistical Analysis
Data were analyzed using GraphPad Instat v3.06 (GraphPad Inc., CA, USA). Descriptive statistics included mean, SD, median, and range. Distribution was assessed via Kolmogorov-Smirnov test. Group comparisons were made using Kruskal–Wallis test followed by Dunn’s multiple comparison post hoc test. A P-value of <0.05 was considered statistically significant.
Results
Macroscopic Findings
The mean score for defect fill depth was significantly higher in curcumin-treated groups (C1 and C2) at both 30 and 90 days compared to controls (K1 and K2) (P = 0.0478). While border integration scores were higher in curcumin-treated groups, this difference did not reach statistical significance (P = 0.1622). The repair tissue quality score was significantly improved in the curcumin groups, especially in the 90-day treatment group (C2) (P = 0.0206). Overall ICRS scores were significantly higher in both curcumin groups compared to controls, with the highest scores observed in the C2 group (P = 0.0195). Mean macroscopic ICRS scores for each group are shown in
Histopathological Findings
Microscopically, curcumin-treated groups (C1 and C2) exhibited improved hyaline cartilage characteristics compared to controls. Cartilage surfaces were smoother, more continuous, and better preserved in the curcumin groups, particularly C2. Control groups exhibited fibrous tissue or fibrocartilage, while curcumin groups showed continuity of hyaline cartilage. Chondrocyte viability and columnar alignment were superior in curcumin-treated samples. Subchondral bone showed improved remodeling in curcumin groups versus necrosis, granulation, and callus formation in controls. Tidemark continuity and appropriate mineralization were better maintained in C2 animals.
Quantitative histological scores demonstrated significantly improved cartilage surface properties (P = 0.0016), matrix structure (P = 0.0047), chondrocyte distribution (P < 0.0001), cell viability (P = 0.0016), subchondral bone features (P = 0.0006), cartilage mineralization (P = 0.0002), and tidemark continuity (P = 0.006) in curcumin groups – especially C2 – compared to controls. Histopathological ICRS scoring values are presented in
Histopathological Findings of Groups in the Osteochondral Defect Model According to the ICRS Scoring System and Statistical Comparisons.

ICRS = International Cartilage Repair Society.
P < 0.01 vs K1.
P < 0.01 vs K2.
P < 0.001 vs K1.
P < 0.05 vs K2.

Quantitative histological evaluation scores across all groups.
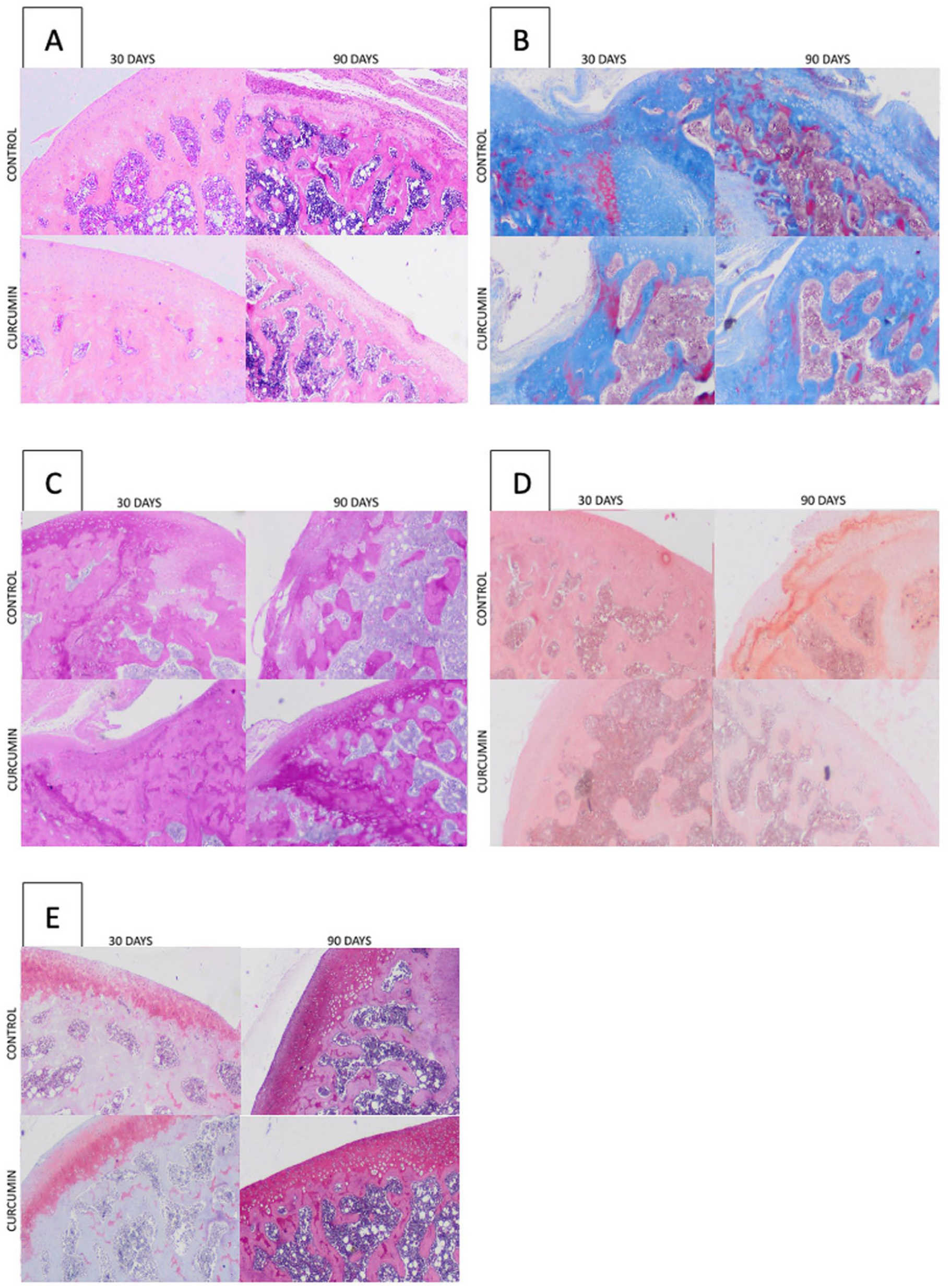
Histological images of cartilage tissue from all groups: (
Immunohistochemical Findings
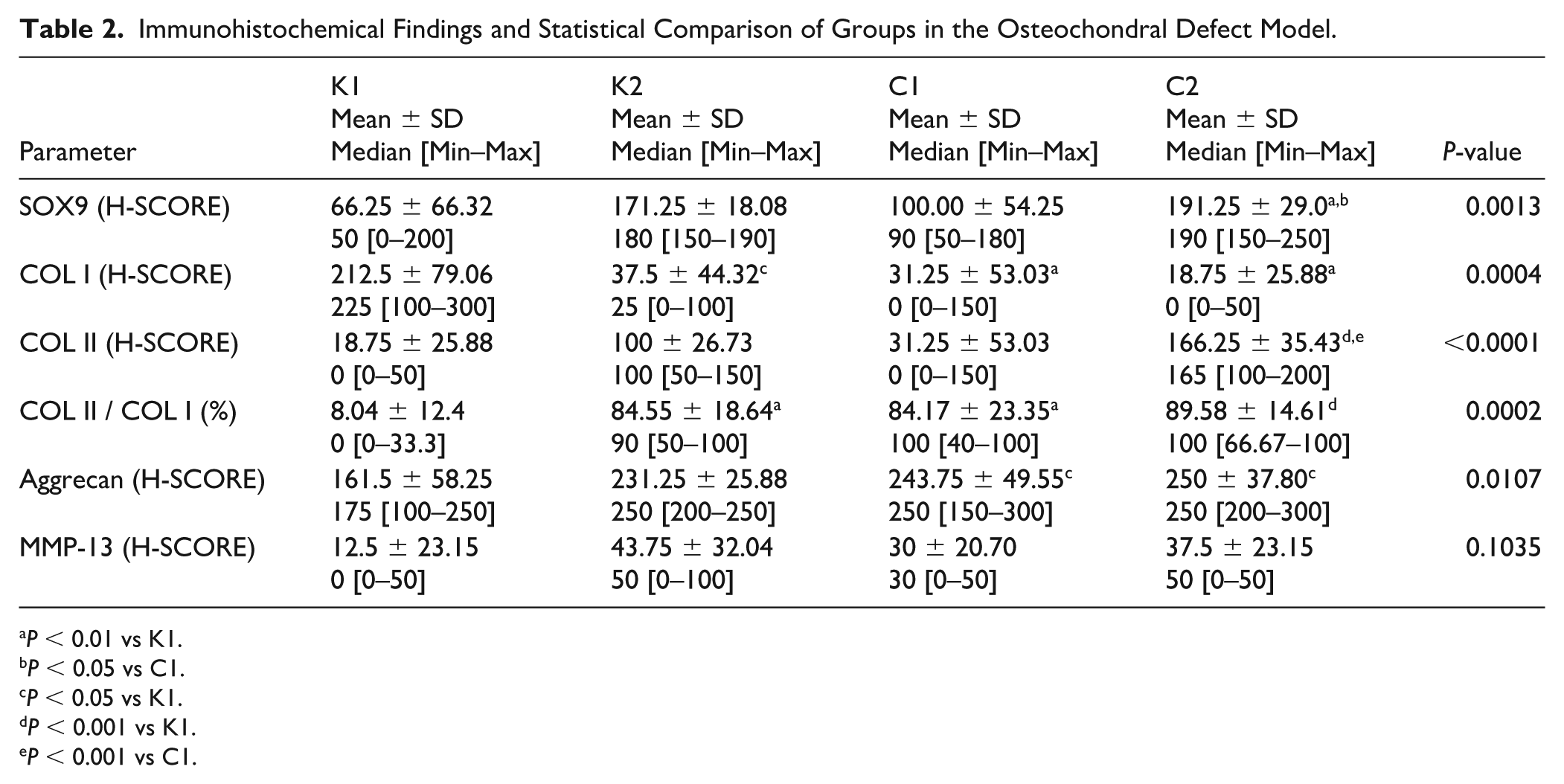
Immunohistochemical analyses revealed significant differences among groups. SOX9 nuclear immunoreactivity was significantly increased in the C2 group compared to controls (P = 0.0013). COL I expression, typically elevated in fibrocartilage, was significantly reduced in curcumin-treated groups (P = 0.0004), while COL II, characteristic of hyaline cartilage, was significantly increased in C2 animals (P < 0.0001). The COL II/COL I ratio, an indicator of hyaline-like repair, was highest in the C2 group (P = 0.0002).
Aggrecan immunoreactivity, reflecting proteoglycan content, was significantly higher in both curcumin groups than controls (P = 0.0107). Although MMP-13 immunoreactivity showed a mild increase in some groups, the differences were not statistically significant (P = 0.1035). Quantitative findings from the immunohistochemical analyses, including SOX9, COL I, COL II, Aggrecan, and MMP-13 expression levels, are summarized in
Immunohistochemical Findings and Statistical Comparison of Groups in the Osteochondral Defect Model.
P < 0.01 vs K1.
P < 0.05 vs C1.
P < 0.05 vs K1.
P < 0.001 vs K1.
P < 0.001 vs C1.
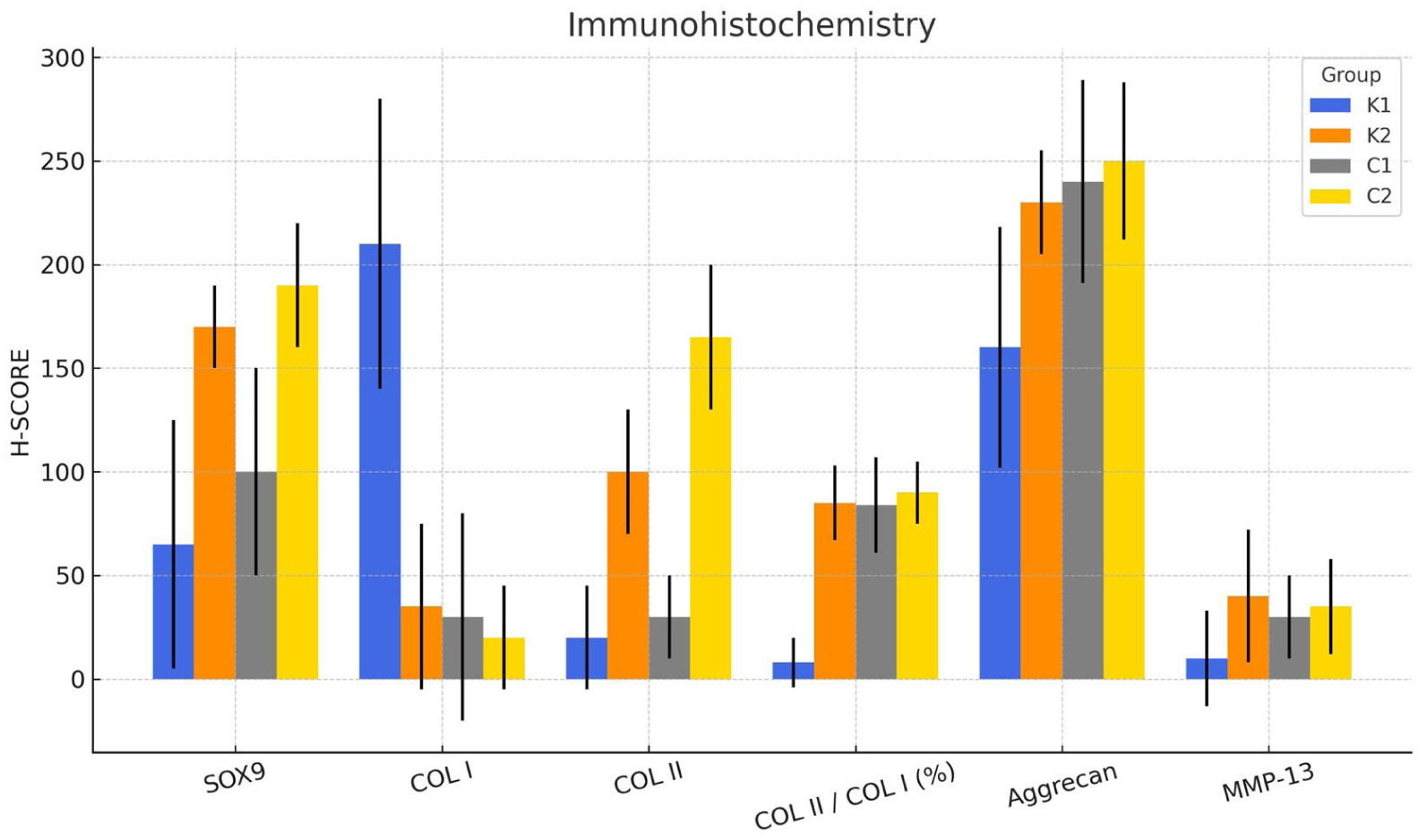
Immunohistochemical evaluation scores of all groups.
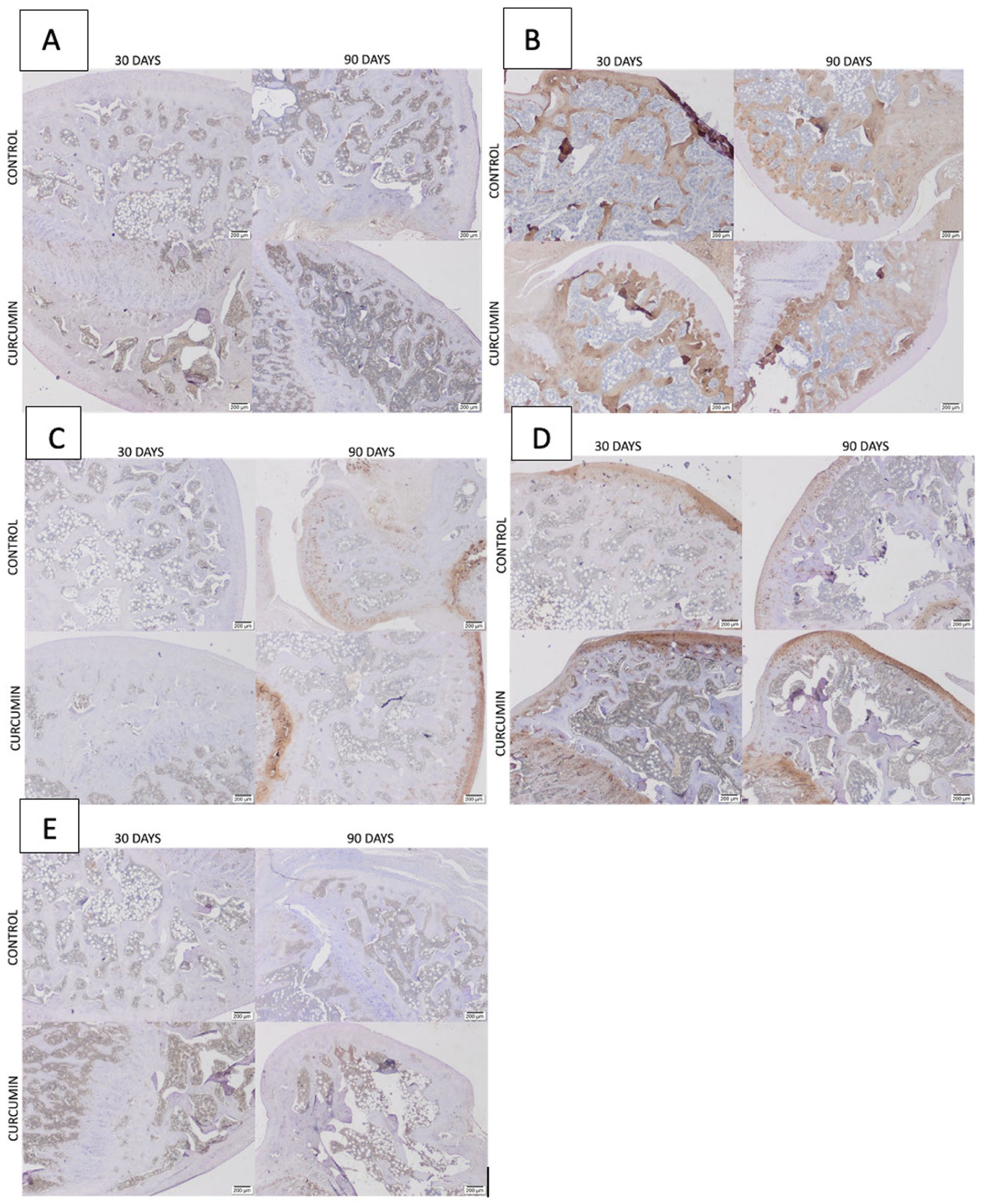
Immunohistochemical staining images: (
Discussion
This study demonstrated that orally administered micellar curcumin significantly enhanced osteochondral healing in a rat model. Particularly in the 90-day treatment group, curcumin improved macroscopic, histopathological, and immunohistochemical parameters of cartilage repair. The results indicated superior quality of the repair tissue, increased expression of hyaline cartilage markers, and more organized subchondral bone remodeling.
The use of separate 30- and 90-day sacrifice groups was intentionally designed to evaluate early and later phases of osteochondral healing. The 30-day time point reflects the proliferative and early matrix formation phase, whereas the 90-day time point represents a more advanced remodeling stage. Although extending all animals to a single 90-day endpoint could allow concurrent comparison, early-phase assessment provides valuable temporal insight into treatment responsiveness. This design is consistent with commonly used experimental cartilage repair models that distinguish between acute and remodeling phases. 19
Our macroscopic findings revealed significantly improved defect fill depth and repair tissue quality in curcumin groups, especially after 90 days. The high macroscopic ICRS scores suggest that curcumin promotes tissue regeneration and potentially accelerates the healing process. The improved macroscopic repair tissue in treated groups exhibited characteristics more consistent with native hyaline cartilage, such as smoothness, uniformity, and elasticity. 29 Curcumin exerts its regenerative effects by modulating extracellular matrix synthesis through chondrocytes via cytokine-mediated pathways. Nakagawa et al. 17 demonstrated that oral administration of highly bioavailable curcumin for 1 year following mosaicplasty significantly improved cartilage surface continuity and stiffness, as confirmed by second-look arthroscopic evaluations. These clinical findings support the potential chondroprotective and regenerative effects of curcumin observed in our study.
Chondrocyte distribution was also notably different between groups in histological evaluations. In curcumin-treated rats, chondrocytes were arranged in regular columns characteristic of healthy cartilage, while in control animals, they appeared irregular and clustered. The organization and alignment of chondrocytes are critical for extracellular matrix integrity and overall tissue architecture. Furthermore, chondrocyte viability was significantly higher in the curcumin groups, an essential factor for sustaining functional cartilage tissue.
Previous studies have demonstrated that curcumin significantly upregulates SOD activity, reduces intracellular reactive oxygen species (ROS), and suppresses chondrocyte apoptosis via extracellular signal-regulated kinase (ERK1/2) signaling pathways. These observations support the antioxidant–antiapoptotic mechanism that may underlie our findings.35,36 Consistent with our findings, Jin et al. 37 demonstrated that curcumin exerts chondroprotective effects in osteoarthritis by promoting AMPK/PINK1/Parkin-mediated mitophagy, a key pathway in maintaining mitochondrial homeostasis and preventing chondrocyte apoptosis. Similarly, Niazvand et al. 13 reported that curcumin treatment improved chondrocyte viability and enhanced extracellular matrix integrity in a rat model of osteoarthritis. These findings are in line with our histological observations.
Curcumin has been shown to modulate multiple signaling pathways implicated in cartilage homeostasis, including inhibition of NF-κB activation, suppression of pro-inflammatory cytokines such as TNF-α and IL-1β, and regulation of mitogen-activated protein kinase (MAPK)/ERK signaling cascades.8,35,36,38 Additionally, curcumin has been reported to enhance chondrogenic differentiation through SOX9 upregulation and to reduce extracellular matrix degradation by inhibiting MMP expression.34,38 These pleiotropic molecular effects provide a mechanistic framework supporting the structural and immunohistochemical improvements observed in our osteochondral defect model.
Immunohistochemical findings are consistent with previous experimental studies demonstrating that curcumin treatment enhances COL II expression and preserves proteoglycan content in osteoarthritic cartilage models.13,37,38 Zeng et al. found that curcumin significantly improved visual analog scale (VAS) pain scores in osteoarthritis patients through anti-inflammatory mechanisms. Although conducted in a clinical osteoarthritis population, these findings support the anti-inflammatory and cartilage-protective mechanisms observed in our experimental model. 39
Saber et al. investigated the combined effects of curcumin administration and swimming exercise in a rat model of monosodium iodoacetate (MIA)-induced osteoarthritis, and reported significant improvements in pain, joint stiffness, histological structure, and suppression of inflammatory markers compared to controls. The increased expression of SOX9 observed in this group further suggested enhanced chondrocyte differentiation and formation. 38 These observations reinforce the multimodal regenerative and anti-inflammatory potential of curcumin as observed in our osteochondral defect model.
The observation that certain control values at 90 days approached or, in some parameters, exceeded early curcumin-treated levels likely reflects the intrinsic time-dependent regenerative capacity of small animal osteochondral defect models, rather than absence of treatment effect.
Although these findings are preclinical, they suggest that enhanced-bioavailability curcumin formulations may merit further investigation as adjunctive strategies in cartilage repair research.
Several limitations should be acknowledged. The study evaluated early and intermediate healing phases only; therefore, long-term durability of the repair tissue remains unknown. Plasma curcumin concentrations were not measured, and the relationship between systemic exposure and local tissue effects remains speculative. Although micellar formulations enhance bioavailability in animal models, pharmacokinetic profiles in humans may differ. Furthermore, functional or biomechanical testing was not performed, limiting conclusions regarding the mechanical competence of the regenerated tissue. Future studies incorporating biomechanical analysis, pharmacokinetic assessment, and dose–response evaluation are warranted.
Conclusion
Micellar curcumin demonstrated favorable structural and molecular effects in this controlled preclinical model. While these findings are encouraging, further translational and clinical investigations are required before therapeutic application in humans can be considered.
Footnotes
Ethical Considerations
All experimental procedures involving animals were approved by the Local Animal Experiments Ethics Committee of the University of Health Sciences, Istanbul Bağcılar Health Practice and Research Center, Experimental Research and Skills Development Center (BADABEM) (Meeting date: May 26, 2023; Meeting No: 2023/37; Project No: 2023-01).
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.