
Abstract
Mobile technology shows great promise in resource-limited settings due to its low cost and pervasive nature. Early evidence-based studies have shown robust support for mHealth interventions implemented among people living with HIV (PLWH); however, this type of inquiry is lacking amongst the most vulnerable groups of PLWH such as men who have sex with men (MSM), prisoners, and those facing substance use disorders (SUDS) and structural instabilities. These populations face barriers more profound than the general PLWH population including social stigma and discrimination. In response to the lack of rigorous evaluation of mHealth implementation and the tremendous potential for mHealth tools in underserved PLWH, we propose a 3-pronged approach in rooting mHealth tools using evidence-based methodology—(a) assessing mHealth feasibility and accessibility through descriptive studies, (b) conducting pilot projects testing mHealth tools, and (c) integrating mHealth tools into existing large-scale studies. The set of research steps proffered here aims to build a solid body of evidence on mHealth interventions among underserved populations and the health conditions that disproportionately affect them.
Keywords
Introduction
Mobile phones and devices have become a ubiquitous part of society, traversing varied age groups, cultures, and socioeconomic backgrounds (World Bank, 2012). In healthcare, the use of mobile technology is viewed as an innovative strategy in governing personal healthcare and promoting preventive and treatment behaviors (Fjeldsoe, Marshall, & Miller, 2009; Katz & Nordwall, 2008; Lim, Hocking, Hellard, & Aitken, 2008). Mobile health (mHealth) interventions have already shown efficacy in improving treatment adherence in patients with chronic conditions such as diabetes, asthma, tuberculosis, and malaria (Asiimwe et al., 2011; Hanauer, Wentzell, Laffel, & Laffel, 2009; Hoffman et al., 2010; Ryan et al., 2009). It is now possible to have a tightly woven network of coordinated care by providing real-time data about dosing reminders (Pop-Eleches et al., 2011; Puccio et al., 2006), medication intake (Hardy et al., 2011; Harris et al., 2010), and solicitation of care (Lester et al., 2010) thus resulting in better feedback and improved communication between patient and provider. The fertile environment of near-ubiquitous access to mobile technology has encouraged entrepreneurs, nongovernmental organizations (NGOs), researchers, and governments to develop secure technologies for data collection that include secure servers, data encryption, and Health Insurance Portability and Accountability Act (HIPAA)-compliant security protocols.
The excitement around mHealth initiatives stems from mobile technology’s ability to address perennial barriers to health care access such as cost, infrastructure, and accessibility (Goel, Bhatnagar, Sharma, & Singh, 2013). The global health community has readily created and implemented a myriad of mHealth solutions in response to problems that previously seemed intractable; however, this surge in implementation lacks a thorough evidence base or rigorous evaluation (Tomlinson, Rotheram-Borus, Swartz, & Tsai, 2013). The mHealth community continues to lack a strong commitment to rigorous, peer-reviewed evaluation of interventions before pushing towards rapid scale-up (Franz-Vasdeki, Pratt, Newsome, & Germann, 2015). A recent systematic review has shown that most studies of mHealth implementation regarding mother and child health initiatives in low- and middle-income countries lacked methodological quality (Lee et al., 2016). While mHealth projects continue to garner significant attention and funding for implementation, the discipline continues to lack a consistent standard and culture of high quality, reproducible, rigorous evaluations of mHealth tools.
The Technical Evidence Review Group, convened by the World Health Organization (WHO), recently published the mHealth Evidence and Reporting Assessment (mERA) checklist that provides clear guidelines for evaluating the design and implementation of mHealth interventions as well as a set of standards for judging the quality of research methods (Agarwal et al., 2016). While the mERA checklist fits with a general trend in the mHealth sector towards better quality of reporting and improved reproducibility of studies (Labrique, Vasudevan, Chang, & Mehl, 2013), there is still a need to continue establishing peer-reviewed best practices and priorities for research methods. Moreover, the entrenched preoccupation of governments and funders with scale-up and broad-scope projects should not sideline initiatives that aim to develop and test mHealth tools for preventive care and treatment for highly marginalized populations.
Gaps and opportunities for mHealth in HIV
Mobile technology shows the greatest promise in resource-limited settings due to its low cost and pervasive nature (Atun & Sittampalam, 2006; Karanja et al., 2011; Leach-Lemens, 2009) making its use in these types of settings particularly impactful. Deployment of text messages in Africa, India, and South America has shown efficacious results specifically in the context of HIV/AIDS (da Costa et al., 2012; De Costa et al., 2010; Lester et al., 2010; Rodrigues et al., 2012) such that new WHO guidelines now strongly recommend texting to promote adherence and retention (WHO, 2013). Moreover, recent international guidelines suggest that the next generation of adherence interventions targeted to people living with HIV (PLWH) should be scaled back both in terms of cost and personnel (Thompson et al., 2012). Interventions that are informed by evidence and bolstered by mobile technology can offer the cost-effective and efficacious strategies that are needed to improve treatment adherence and optimize health outcomes among PLWH.
Early evidence-based studies have shown robust support for mHealth interventions implemented among PLWH in terms of increased medication adherence and viral load suppression (Dowshen, Kuhns, Johnson, Holoyda, & Garofalo, 2012; Hardy et al., 2011; Lester et al., 2010). Despite this promising trend, there has been an inability or unwillingness to examine the impact of mHealth tools on the most vulnerable groups of PLWH (Catalani, Philbrick, Fraser, Mechael, & Israelski, 2013)—prisoners, men who have sex with men (MSM), sex workers, individuals with substance use disorders (SUDs), injection drug users (IDUs), those with mental illnesses and neurocognitive impairment, and those facing structural barriers such as unemployment and homelessness. These populations face barriers more profound than the general PLWH population including social stigma and discrimination from society and healthcare providers (Earnshaw et al., 2014; Niang & Tapsoba, 2003). MSM, sex workers, and IDUs additionally are at higher risk of contracting and transmitting HIV (Beyrer et al., 2012), thus constituting a significant public health issue. Given that mobile technology holds great promise in enhancing traditional medical care, underserved populations with disease burden such as HIV can benefit enormously from evidence-based innovations that could mitigate their vulnerabilities.
In acknowledging the lack of rigorous evaluation of mHealth implementation and the tremendous potential of mHealth in underserved PLWH, we propose a three-pronged approach in rooting mHealth tools using evidence-based methodology constructed from our experiences in the field. It should be noted that these three “prongs” or approaches are not necessarily meant to be sequential but may be conducted independently of each other. The purpose of the prongs is to illustrate the variety of approaches that can be adopted to build up the literature on evidence-based mHealth in marginalized communities.
Assess accessibility of communication technology tools such as mobile phones and computers, and feasibility and acceptability of mHealth interventions through descriptive studies.
Conduct case studies, usability tests and pilot projects that implement mHealth-based protocols and interventions.
Integrate mHealth tools into existing large-scale clinical, pharmacological, or sociobehavioral randomized control trials.
In this critical paper, we will present examples of real-world projects and studies that we have conducted or been involved in as part of collaborative teams, as evidence of how this three-pronged approach can aid in filling the gap in mHealth research among historically underserved groups of PLWH. We will precede this with a theoretical model adapted from the public health and information systems literature, that can be used to examine the process of individual decision-making in an mHealth-based study.
Theoretical framework
A significant challenge to mHealth research has been the general lack of theory in guiding research design and implementation. This lack of theoretical framework was acknowledged in a systematic review of HIV-related mHealth studies (Catalani et al., 2013) where the authors note that mHealth researchers focus on user-centered design and health information systems over attempts to understand the health decision-making process. A strong set of theoretical frameworks will help “strengthen the mHealth evidence base” (p. 38). Early health behavior models were developed with predominantly linear and static methodologies; these have been insufficient when applied to innovative health interventions that incorporate information and communication technologies (Riley et al., 2011). An mHealth project that addresses preventive and treatment behaviors amongst vulnerable PLWH populations requires a framework that allows researchers to address the facets of health behavior change and communication as well as the technological components of service and communication delivery. We thus propose a theoretical framework—the integrated health and technology model (IHTM)—for examining mHealth among underserved PLWH that is rooted in the health belief model (HBM; Hochbaum, Rosenstock, & Kegels, 1952) but builds from this classical framework by incorporating the technology acceptance model (TAM; Davis, 1989; Davis, Bagozzi, & Warshaw, 1989).
The HBM provides us with a framework for examining individual health behaviors with respect to the specific variables that individuals assess when faced with a potential change in health behavior: their perceived susceptibility to ill health (i.e., their perception of personal risk), their perceived severity of ill health, perceived benefits of behavior change, and perceived barriers to taking action (Green & Murphy, 2014). This theory was subsequently amended to include self-efficacy as a core variable in behavior change (Rosenstock, Strecher, & Becker, 1988). The TAM is an information systems theory whose core tenet is that characteristics of any information system directly affect how motivated end users are to use the system (Davis, 1989). It posits that in designing a new information system, the two major determinants of end-user acceptance are the system’s perceived usefulness and ease of use (Venkatesh, Morris, Davis, & Davis, 2003).
The IHTM borrows key constructs from the HBM and the TAM into one comprehensive health–technology approach to individuals’ decision-making process (see Figure 1). With respect to mHealth-based studies, the IHTM takes into account health constructs regarding individuals’ perception of their disease severity and agency in mitigating illness while simultaneously establishing the mHealth intervention’s perceived usefulness and perceived ease of use on attitudes and consequently on behavioral change. The health-related constructs include demographics, personality traits, knowledge, and health self-efficacy that influence an individual’s perception of the seriousness of their health condition and lead them to make a cost–benefit analysis (the difference between perceived benefits and perceived barriers) of the proposed behavior change. This in turn influences the likelihood of behavioral change. Under the technology-related constructs of the IHTM, we include technology self-efficacy—perception of one’s ability to use the technology—that influences an individual’s perception of the ease of use and usefulness which in turn leads to positive attitudes towards and consequently likelihood of behavioral change. The construct “cues to action,” which is originally an HBM component, is adapted as a technology construct in the IHTM as the mHealth strategy that seeks to activate behavior change. By integrating key components from two established theoretical models, the IHTM offers a cohesive framework for understanding and predicting the effect of technology or mHealth interventions on health outcomes. As we describe the three “prongs” or approaches in what follows, we will connect the constructs considered in each of the types of studies to the constructs in the IHTM.

Proposed integrated health and technology model (IHTM).
Approach 1: Descriptive studies to assess access, feasibility, and acceptability
Technology-based studies that are conducted with the intention of influencing health outcomes can be unsuccessful if preliminary feasibility or acceptability studies are not conducted first (Black et al., 2011). In fact, formative research has been heralded as an integral first step in the design and implementation of HIV interventions (Gordon, Stall, & Cheever, 2004). Strong acceptability of the mHealth tool by the population in which it is to be ultimately tested is likely to be related to higher chance of successful implementation. Thus, to be able to design efficacious mHealth-based strategies, it is pertinent to gauge the adoption and use of the mHealth tool in question. Despite a lack of enthusiasm for this kind of descriptive work, there is a small yet burgeoning set of formative and multimodal evaluations of mHealth perceptions and attitudes (Chang et al., 2013; Curioso & Kurth, 2007; Haberer, Kiwanuka, Nansera, Wilson, & Bangsberg, 2010). The project discussed next is a prime example of this type of descriptive research.
In recent decades, the HIV epidemic has come to be concentrated among specific groups such as MSM (Alarcon et al., 2012). This is especially true in Peru where HIV rates among MSM range between 10% and 22% (Sanchez et al., 2007). There is also a high incidence of alcohol use disorders (AUDs) and risky sexual behavior in this group (Segura et al., 2008). Given that Peru’s telecommunication infrastructure is expanding rapidly and that LGBT and MSM have been identified as early adopters of emerging technology such as the Internet and cell phones (Bolding, Davis, Sherr, Hart, & Elford, 2004), we decided to conduct a descriptive study to gauge feasibility. In collaboration with a local NGO, we recruited 359 HIV-infected MSM and disseminated a survey that included measures of AUDs, risky sexual behavior, antiretroviral (ART) adherence, communication technology access and utilization, and mHealth acceptance.
Results showed that a majority of participants (86%) had daily access to cell phones with 30% having access to a smartphone. The most frequent activities reported were receiving and making calls followed by receiving and sending text messages. Specific responses to mHealth interventions showed that there was high interest in receiving medication reminders on cell phones either in the form of text messages or phone calls (Krishnan, Ferro, et al., 2015). This is promising since cell phone reminders have been successfully used in resource-constrained settings to improve ART adherence (Lester & Kariri, 2009; Lester et al., 2010). The sample showed high levels of AUD and risky sexual behavior mirroring previous findings and providing a justification for HIV prevention and intervention strategies that need to target multiple risk factors. Most importantly, the results showed that were no significant differences in technology use and mHealth acceptance among participants with varying levels of AUD, depression, and suboptimal ART adherence (Krishnan, Ferro, et al., 2015), thus indicating that an mHealth-based intervention is a feasible strategy in this population.
The authors have since conducted similar studies in Malaysia among MSM and in Indonesia among HIV-infected prisoners (see Table 1 for an example of survey items) to establish feasibility and acceptability. This step of evidence-based strategy is also essential in informing theory since constructs related to health (e.g., perceived severity) and technology (e.g., attitudes, self-efficacy), as proposed in the IHTM and assessed through the descriptive studies, can be used to predict likelihood of adopting the mHealth tool which has consequences for actual behavior change.
Example of survey items assessing interest in mHealth interventions.
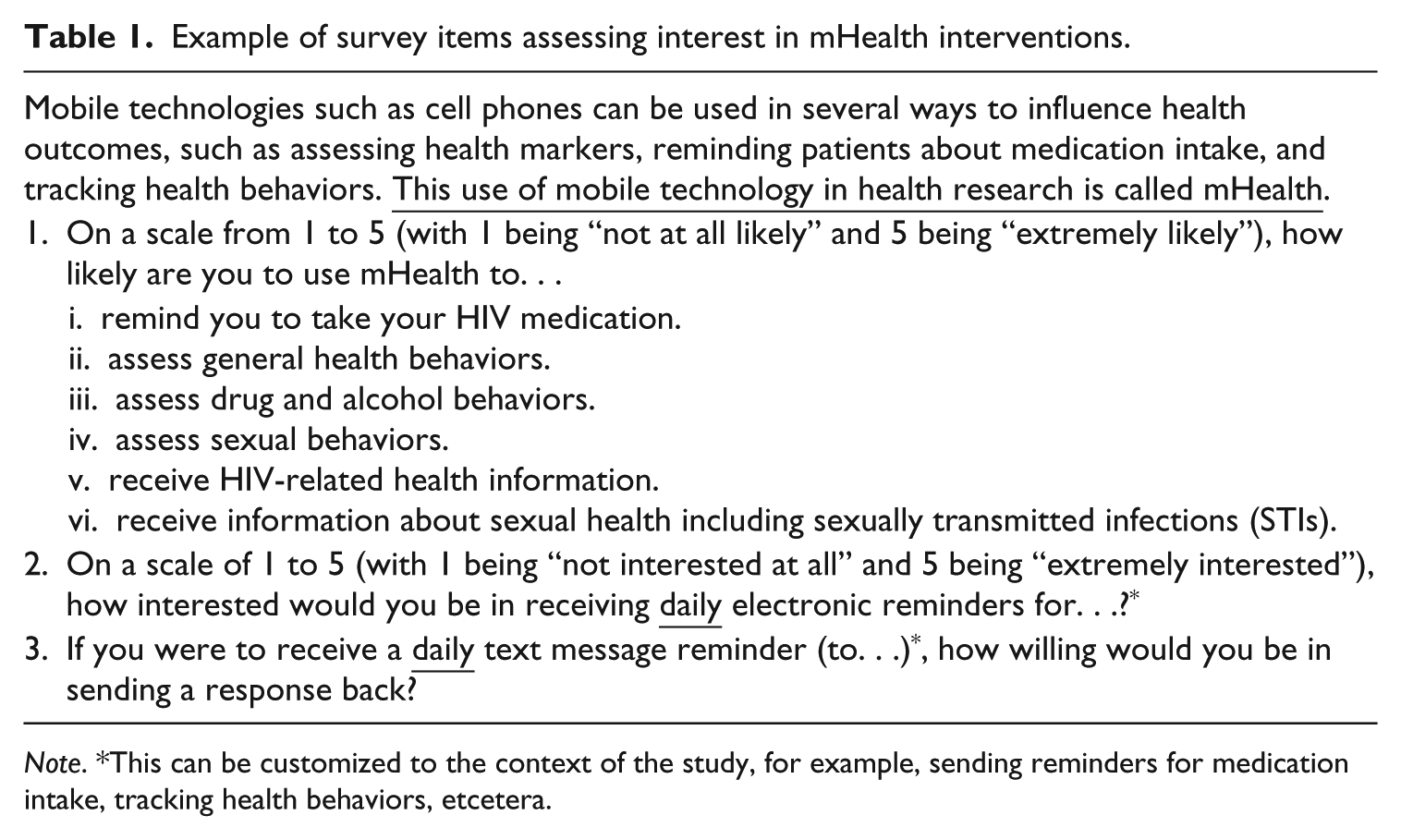
Note. *This can be customized to the context of the study, for example, sending reminders for medication intake, tracking health behaviors, etcetera.
Approach 2: Case studies and pilots
The implementation of case studies, usability tests, and pilots is an essential approach to building a body of evidence in order to inform scale-up (Tomlinson et al., 2013). In recent years, this approach has been deeply criticized due to the rapid proliferation of pilot mHealth projects that have failed to achieve efficacy and impact in real-world conditions (Labrique et al., 2013). There is however, an argument to be made for implementing pilots especially when considering the vulnerabilities of high-risk populations. Small-scale projects that are iterated in the early stages of development tend to maximize utility and acceptability to the end users (Dean, Makin, Kydd, Biriotti, & Forsyth, 2012). In this section, we leverage the technology components of the proposed IHTM model to examine the acceptability and utility that technology-enabled design protocols present to a specific group of end users. The section outlines the methodology and findings from two different pilots developed and tested for a specific subset of vulnerable PLWH—prisoners. These pilots demonstrate how researchers can and should leverage pilot phases in their studies to examine whether end users demonstrate self-efficacy and acceptance in using a mobile tool.
Developing and pilot-testing a text-messaging protocol to improve retention in care
PLWH transitioning from correctional settings to the community often encounter decreased access to ART, poor treatment outcomes, high HIV-risk behaviors, and social instability such as homelessness (Chen et al., 2013; Springer et al., 2004; Stephenson et al., 2005). Linking and retaining incarcerated PLWH to HIV primary care and other auxiliary services upon release is essential to improving their health outcomes (Springer et al., 2004). We developed a protocol incorporating text-messaging reminders and pilot-tested it among recently-released HIV-infected prisoners in order to improve medical appointment attendance (HIV, mental health, and/or substance abuse counseling) and retention in care. Three participants for the pilot study were recruited, each sourced from two large-scale clinical trials that were recruiting HIV-infected prisoners transitioning to the community (Di Paola et al., 2014; Krishnan et al., 2013).
Upon recruitment, participants were administered a baseline questionnaire and given a cell phone followed by a 10-minute information session by a research assistant (RA) on texting and setting up voicemail. Each participant was followed for 6 months; apart from baseline, they met with an RA in person at Months 1, 3, and 6, at which time they were administered a brief qualitative questionnaire gauging their reaction to the text-message reminders. The protocol composed of an RA sending text message reminders (e.g., “You have an appointment with Dr. _______ on [day of week, date] at [time]. Text “yes” to confirm or “no” if you don’t plan to attend”) 7 days, 3 days, and 1 day prior to participants’ medical appointment. If participants did not respond, the RA texted back within 2 hours and then waited 12 hours before placing a call to the participant. Prior to pilot-testing, an extensive mock-up session was conducted with the RAs to familiarize them with the study protocol and to troubleshoot potential problems. They were instructed to follow strict confidentiality rules such as saving ID numbers versus participant names in the phone directory and to avoid using real names in the text messages. In order to verify that the reminders were effective in improving appointment attendance and retention in care, the RAs communicated with the participants’ medical case manager to confirm attendance.
Qualitative interviews showed that the text messages were perceived as being effective in reminding participants to keep medical appointments; participants found them “useful” and “easy.” The RAs were able to confirm with the case managers that participants attended their HIV medical appointments, thus indicating successful long-term retention in care. In addition to the reminders, the cell phones enabled participants to contact the RAs with health-related concerns and questions thereby establishing bidirectional communication. Finally, qualitative interviews conducted with the RAs showed that they found text messaging to be a nonburdensome way of maintaining contact with study participants. Based on the efficacy of the pilot, the authors have adapted the findings to a recently funded larger scale randomized controlled trial examining the impact of automated reminders and feedback on ART adherence.
Piloting a mobile application to assess health-seeking behaviors among Indonesian prisoners
The following mHealth intervention piloted in Indonesia was a natural extension of the rapidly expanding ecology of telecommunications in this region. While Indonesia’s economic progress is clearly demonstrated in the telecommunication industry’s rising predominance in the region (Central Intelligence Agency [CIA], 2009), its underresourced health care system faces a worsening HIV epidemic (United Nations Programme on HIV and AIDS [UNAIDS], 2014). Currently, the HIV prevalence estimated in Indonesian prisons ranges between 1.1% and 6.5% (Culbert et al., 2016). In order to evaluate the continuum of care for HIV-infected incarcerated patients, we piloted an mHealth application (app) to evaluate health-seeking behaviors and continuum of care for prisoners, following their release.
The pilot was integrated into a larger survey concerning health-seeking behaviors and continuum of care access for 102 incarcerated PLWH in Jakarta. RAs conducted the survey using a mobile app built on the open-source platform CommCare. This app provided workflow support, skip logic, and automatic data capture synchronized directly with HIPAA-compliant servers via a secure cloud. The research team was able to reach 33 of the original 102-prisoner cohort after release. The patient data in addition to the user experience survey and metadata collected over the course of 33 interviews provided actionable pilot data regarding the feasibility and acceptability of the mobile intervention for this population. At the end of the survey concerning participants’ access to continuum of care, the RAs were prompted to ask two questions regarding the participants’ experience with the mHealth tool. Of the 33 participants in the pilot, a large majority (91%) indicated that they were either very comfortable or comfortable with the mHealth format for their adherence interview. When asked if they would prefer the interview to be conducted via a tablet, paper, or another format, 64% reported that they would prefer the tablet format.
After conducting each patient survey, the mobile app prompted the interviewer to complete an additional brief survey to evaluate their experience in administering the survey via the mobile tool. The RAs completed this form each time they completed an interview and results showed a 100% preference in using the app despite some technical issues such as battery life. Preliminary data from this pilot indicate strong evidence supporting the design of a scalable HIV continuum of care provision and consequently expand the app to nurses equipped to provide care directly to released prisoners. After multiple iterations to improve the usability and expand the scope of the services that the app supports, the lead researcher on this project intends to expand the app to several points-of-care and mobile care givers.
Pilots that allow researchers to test preliminary versions of technical interventions align with a core tenet of the IHTM which posits that exposing end users to a prototype or “façade” of a planned system allows them time to develop their perceptions of the new system’s usefulness and ease of use (Davis et al., 1989). Positive user experience with the piloted protocol or system thus leads to positive attitudes which consequently impacts likelihood of behavior change. This theoretical path to behavior change is of particular importance when dealing with marginalized populations as they are more likely to have other external barriers to care, for example, low socioeconomic status, and lower education and technology self-efficacy (Chen et al., 2013). By exposing underserved PLWH to pilot versions of mHealth systems and protocols, researchers can benefit from their feedback and in the same vein, increase their self-efficacy. This in turn is likely to influence them to adopt and maintain technology-enabled health behaviors.
Approach 3: Integration of mHealth into large-scale trials
This section discusses the strategy of integrating mHealth tools into already-existing large-scale pharmacological or sociobehavioral studies with the intention of maximizing study goals. Common issues with large-scale randomized control trials (RCTs) usually include failure in achieving adequate sample size (McDonald et al., 2006) and in studies with vulnerable populations, an inability to retain participants in the trial. It has been suggested that along with methodological innovation, information technology can aid in improving recruitment and retention (Bower et al., 2009). The study presented here is an example of integrating mHealth (in this case, cell phones) into a large clinical trial conducted among HIV-infected released prisoners with alcohol problems and severe structural barriers.
This was an RCT conducted among HIV-infected prisoners meeting DSM-IV criteria for alcohol dependence or problem drinking, who were transitioning to the community (Krishnan, DiPaola, Winn, Altice, & Springer, 2015; Springer, Altice, Herme, & Di Paola, 2014). Participants were randomized to either receive extended release Naltrexone (XR-NTX)—an FDA approved opioid antagonist—or a placebo injection once a month for 6 months and additionally followed for 6 months to examine the effect on HIV outcomes, alcohol use, and HIV-risk behavior. Like other large-scale clinical trials dealing with vulnerable populations, the study suffered from severe retention issues. Due to the transitory lives of the recently released participants, the RAs were unable to keep up with the constantly changing contact information. Many in the sample were homeless and were prone to “couch surfing.”
In an attempt to address retention, we decided to provide participants with cell phones. RAs contacted participants once a week on the cell phones for general inquiry, to assess alcohol craving and incidence of drinking, and to remind them about the monthly research interviews and doctor’s appointments. A total of 102 participants were recruited for the RCT, of which 34 were recruited after the decision to incorporate cell phones. Retention (defined as staying enrolled in the study and attending monthly interviews) prior to implementation of cell phones hovered between 54–67% between the first and final months of participation; drop-outs occurred at a higher rate during the first few months of being in the trial. This is likely an indicator of the difficult transition that incarcerated PLWH face from prison to the community.
Retention rates were noted for every month and calculated for the group as a whole (depending on which stage of the study they were in) and tracked for a year after implementation of cell phones. There was negligible improvement for the first 6 months after cell phones were introduced; however, retention improved drastically after that. There was an overall 8.9% increase in retention 9 months after cell phones with the most drastic improvement occurring among participants who were in the first 2 months of the trial (14% and 13%, respectively; see Figure 2). Retention continued to hover at similar rates—by the end of 1 year, the average increase in retention rate was 6.4% with the most significant effects felt on participants in the early stages of the trial. These results, though modest, point to the promise of mHealth in large-scale trials to improve retention and maximize study outcomes.
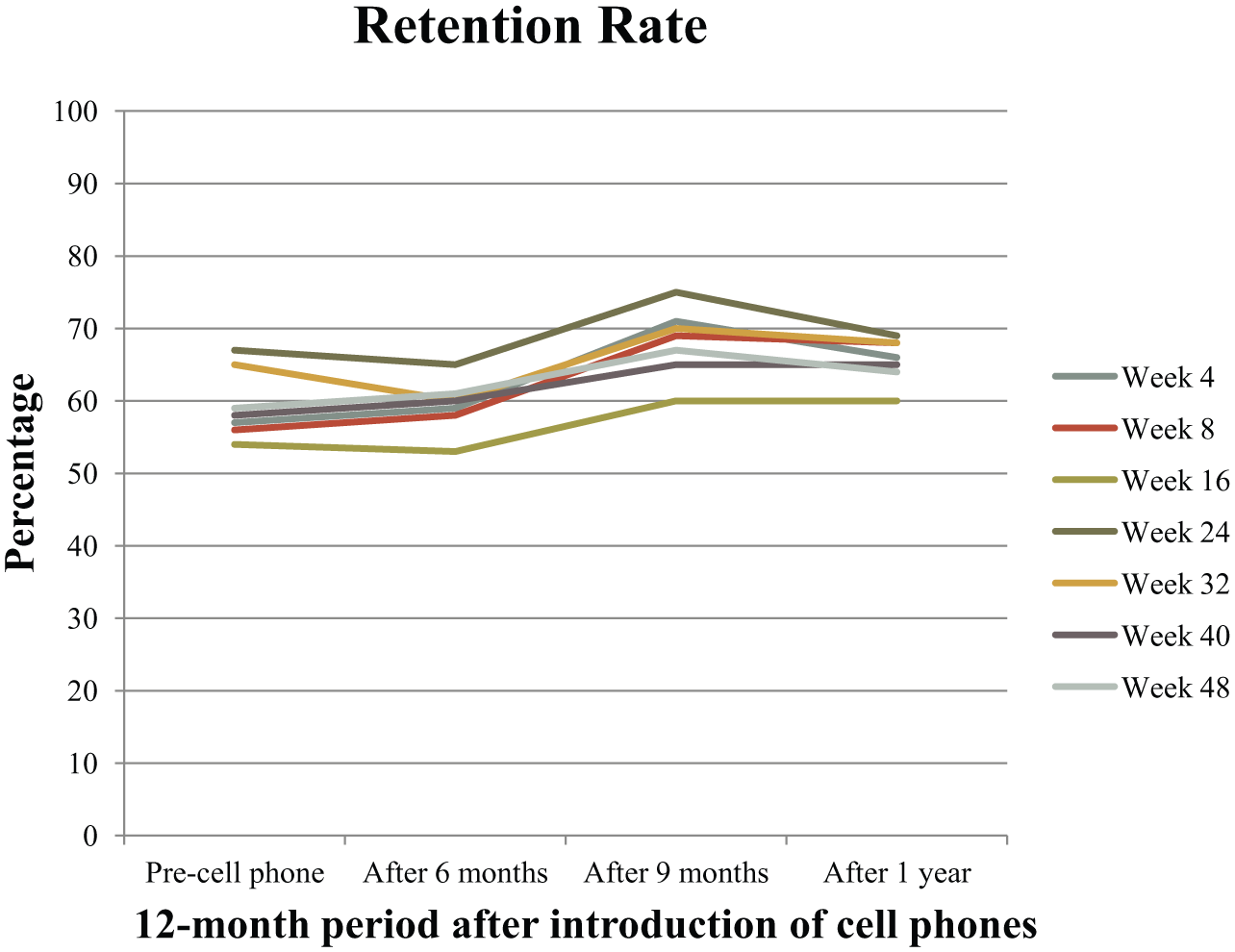
Participant retention rate postintroduction of cell phones.
In keeping with IHTM, the mHealth component discussed before (cell phones as a means to maintain retention in the trial) can serve as a cue to action that is likely to influence behavioral change. The mHealth tool may also influence how individuals carry out the cost–benefit analysis, that is, if the tool is easy to use and useful, the perceived benefits of adopting a health behavior change will weigh more than the potential costs (e.g., time, effort). This is turn will influence the likelihood of behavioral change such as improving medication adherence or reduction in alcohol intake, such as in the study discussed before.
Discussion
As the wider mHealth field matures from a period of myriad proof-of-concept and pilot projects towards projects built to scale, it is essential to build a solid body of evidence on mHealth interventions among underserved populations and the health conditions that disproportionately affect them, in a way that trends towards impactful and user-centered interventions. The multipronged strategy outlined in this article presents preliminary strides in integrating mHealth tools among underserved PLWH populations as a way to promote preventive behaviors and aid in positive health outcomes. This will ultimately allow for the scalability of mHealth interventions by focusing on content and user- and beneficiary-centered design.
While the physical geographic location of these studies ranges from South East Asia to Latin America and the United States, the technological context for these studies is remarkably similar. As detailed in the GSMA Mobile Connectivity Index, all the countries featured in this paper have remarkably similar mobile connectivity penetration, with the US ironically having a lower penetration rate (99.89%) than Peru, Malaysia, and Indonesia which all have over 100% mobile penetration. This is a clear demonstration of the “leapfrog” effect (Fong, 2009), that has allowed countries that are traditionally slotted as “developing” to leapfrog over the incremental steps that “developed” countries have had to follow; for example, transitioning from landline telephones to cell phones to phones with Internet capability and so on. Herein lies the promise of mHealth technology—access to mobile phones appears to be a converging factor among countries with otherwise divergent socioeconomic and health indicators. Previous research has noted that this leapfrog effect in technology can be linked to a leapfrog effect in preventive and curative care (Clifford & Clifton, 2012). This paper aims to equip researchers with these three approaches to mHealth so as to further explore whether leapfrogging in mobile connectivity can be leveraged among vulnerable HIV populations to better preventive and curative care.
Through the studies presented here, we have detailed the needs of highly vulnerable PLWH populations who have largely been ignored within the larger conversations around mHealth and HIV, but who can truly benefit from the convenience and discretion that mHealth tools provide. Unfortunately, these populations are perennially understudied and this insufficiency of evidence has implications for future implementation and scale-up of mHealth in these populations (Tomlinson et al., 2013). The study of technology access and mHealth acceptability among HIV-infected Peruvian MSM showed that this was a group that adopted smartphones faster than the general population. Without this descriptive study, researchers would be unaware of this trend and oblivious of the evidence that now supports the development of mHealth-based intervention strategies in this socially marginalized and understudied population. Similarly, the successful pilot-testing of text-message reminders and app-based surveys among recently incarcerated PLWH shows that future interventions targeting this group of PLWH can be designed using mHealth tools. An argument was also made for the implementation of mHealth tools into already-existing large-scale studies. It is not essential to develop interventions that are wholly situated around technology but rather that technology can be used to complement an existing study design or used to address issues of recruitment and retention.
In response to a lack of theory in the field, we structured our multipronged approach around a new integrated theory of mHealth. The IHTM has been adapted from existing health and information systems literature to explain the decision-making process of behavior change. By aligning the design of the technology with the utility it presents to the end user, the IHTM harnesses the power of user-centered design as evidence-based practice proposed by the TAM. This same alignment with self-efficacy extends to the health behavior component of the IHTM, where we discussed the specific variables that individuals assess when faced with a behavior change opportunity. Technology self-efficacy will determine a user’s likelihood to use a new technological intervention, and health self-efficacy will determine the likelihood of making a sustained change in adopting the technology to change one’s health behaviors. The theory though proposed for mHealth-based interventions for highly marginalized populations can easily be adapted for other mHealth studies. The IHTM presented here is purely a proposed theoretical model; future steps will be centered on testing the model.
Recommendations
The multiple approaches outlined here present preliminary strides in integrating mHealth tools among underserved PLWH as a way to promote positive health outcomes. The prongs are rooted in an integrated theoretical model that combines the constructs related to both health and technology—a combination that optimizes the model’s focus on efficacy and impact for the end user. Our recommendation is that future research be rooted in the testing of theoretical models that center on end users and beneficiaries in the development, implementation, and study of mHealth tools. This, we have found, is especially critical in the case of highly vulnerable populations such as drug users, prisoners, and MSM. Research design and testing must be tailored to their specific vulnerabilities, context, and preferences, no matter the scale of project, in order to design the most efficacious mHealth tool and intervention.
There is increasingly a push for scaled interventions and dissemination research; the 2015 mHealth Summit’s Global mHealth Forum focused on scale and evidence base as a central priority so as to better advocate to funders and governments for the integration of mHealth into systems in need of cost-effective solutions (Blynn, 2015). While scale should remain a central priority for the community of practice, the focus on scale-up and broad-scope projects risks sidelining mHealth projects that are necessarily smaller in scope. There is a limitation of course, in trying to influence scale-up of interventions developed for highly marginalized populations; this is because studies designed around vulnerable groups tend to be specialized (i.e., accommodative of multiple comorbidities) and hence are not always amenable to scale-up. However, rather than eschewing smaller scale projects to assess usability, this paper demonstrates that it is more important than ever to conduct systematic testing, evaluation, and review of interventions through well-designed case studies, usability tests, and pilot projects in order to reach particularly vulnerable populations The mHealth discipline needs an intentional framework for implementation and research regarding vulnerable populations such as underserved PLWH in order to adequately include them in the rapid evolution of the discipline.
Footnotes
Acknowledgements
The authors would like to acknowledge our mentors and colleagues Frederick Altice, Sandra Springer, Gabriel Culbert, Amy Althoff, Jeffrey Wickersham, and Angela DiPaola for giving us the opportunity to collaborate with them on the studies mentioned in this paper and encouraging us to develop an mHealth research agenda. Additionally, we would like to thank the numerous research assistants, international collaborators, and study participants who made possible the various projects that formed the basis of this paper.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Bristol-Myers Squibb Research Fellows Grant (AI424-954) awarded to Archana Krishnan.