
Abstract
Objective
To establish the endometrial cancer detection rate in women using hormone replacement therapy presenting with postmenopausal bleeding.
Study Design
Retrospective cohort study. Setting and population
Rapid access gynaecology clinic at a tertiary hospital. Women aged under 60 years referred with postmenopausal bleeding.
Methods
Retrospective study of referrals received between 1 January 2019 and 31 December 2020 including Hormone replacement therapy (HRT) use and histological diagnosis.
Main outcome measures
Histological diagnosis of endometrial cancer, borderline ovarian tumour or endometrial intraepithelial neoplasia.
Statistical analysis
Chi squared test
Results
1363 women were included. 214 women were using HRT when they experienced PMB and only one of these had endometrial cancer at histology (cancer detection rate 0.47%). 25 of the 1124 women who were not using HRT were diagnosed with endometrial cancer on histology (cancer detection rate 2.18%). Chi squared statistical analysis confirmed this was statistically significant (p value .0156).
Conclusions
The endometrial cancer detection rate in women aged under 60 years using HRT with PMB is very low. Referral on a two-week wait pathway for suspected cancer diagnosis induces stress and anxiety for the woman and may lead to more invasive initial investigation even though other diagnoses are far more likely. Women aged under 60 years with postmenopausal bleeding that have either commenced HRT or had a change to their preparation within the last 6 months should be seen on a less urgent referral pathway if necessary given the very low probability of endometrial cancer.
Introduction
Endometrial cancer is the most common cancer of the gynaecological tract in Europe. 1 Worldwide incidence is increasing due to rising obesity, increasing subfertility rates and an ageing population. These risk factors are largely based upon increased duration of oestrogen exposure. Raised BMI causing elevated circulating oestrogens released by adipose tissue can impact the endometrium and trigger bleeding. PMB is the main presenting symptom of endometrial cancer and results in large numbers of referrals to two-week wait gynaecology clinics to investigate suspected cancer.
Hormone replacement therapy (HRT) is widely used in the treatment of vasomotor symptoms, urogenital dysfunction and to reduce cardiovascular and osteoporosis risk among peri and postmenopausal women in the UK. A major side effect of HRT is irregular uterine bleeding. This can occur with both continuous and sequential regimens and is a significant reason for early cessation of treatment. 2 Irregular uterine bleeding is more common with continuous combined HRT in the initial year of therapy after which it is more common with sequential HRT. Few women have irregular bleeding after two years of using combined HRT. 3 Further studies demonstrated the risk of detecting pathology is low within the initial 6 months of using HRT when a large proportion of women reported breakthrough bleeding. 4 During the perimenopause, residual ovarian activity can promote uterine bleeding. Reduced compliance can also trigger bleeding. 5
Unopposed oestrogen therapy increases the risk of endometrial pathology. This has been strongly and consistently demonstrated in a Cochrane meta-analysis and subsequent studies with a strong dose- and duration-dependant relationship.3,6,7 NICE guidance recommends that all UK women with an intact uterus should receive combined HRT which reduces the risk of endometrial hyperplasia by comparison. There was no statistically significant difference between combined and sequential regimens in a meta-analysis. 3 When endometrial carcinomas do arise in patients on HRT, they are typically ‘type I’ (oestrogen-driven) cancers: well differentiated endometroid adenocarcinomas (FIGO grade 1). 8
In conclusion, unscheduled vaginal bleeding is very common within the first two years of commencing combined HRT. Combined HRT does not increase the risk of endometrial cancer. We receive a large number of two-week wait cancer referrals for women aged 60 years and under with PMB whilst using HRT. The large majority receive a final diagnosis of HRT-related bleeding. We suspected that cancer detection rates among this cohort was low and proceeded to evaluate this with the aim to ultimately guide clinical practice.
Methods
This was a service evaluation of a retrospective sample of 1363 women who were seen following a two-week wait referral in the gynaecology outpatient department of Sheffield Teaching Hospitals NHS Trust in the UK. All women aged under 60 years who were referred with postmenopausal bleeding between the 1st of January 2019 and 31st of December 2020 were included and outcomes analysed.
The following groups of patients were excluded: patient declined or did not attend appointment, referral downgraded or retracted and patient deceased prior to appointment.
A decision was made to include endometrial and ovarian cancers in the final analysis, but to exclude any other incidentally diagnosed malignancies. Current NICE guidance lists PMB as a possible symptom of ovarian cancer; therefore, we felt including these cases was appropriate. Data analysis was performed using Microsoft Excel.
Results
Patients under 60 years of age diagnosed with an endometrial or ovarian malignancy following referral for postmenopausal bleeding between 1 January 2019 and 31 December 2020 inclusive.
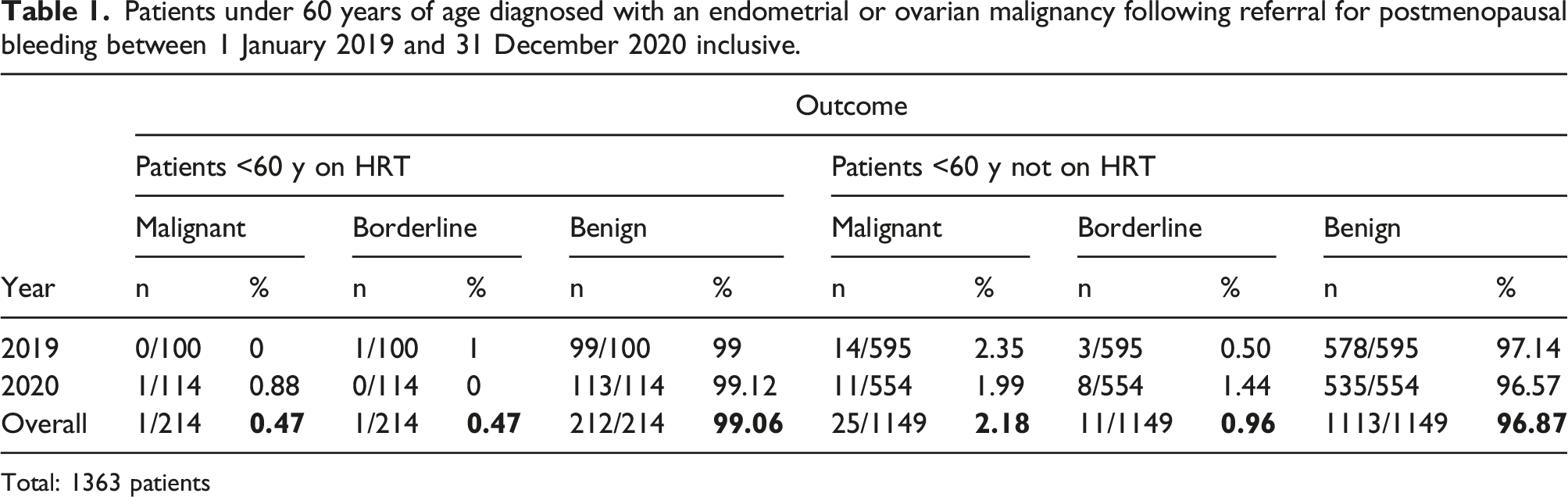
Total: 1363 patients
Table showing outcomes of patients under 60 years referred with postmenopausal bleeding while on HRT from 1 January 2019 to 31 December 2020 inclusive.
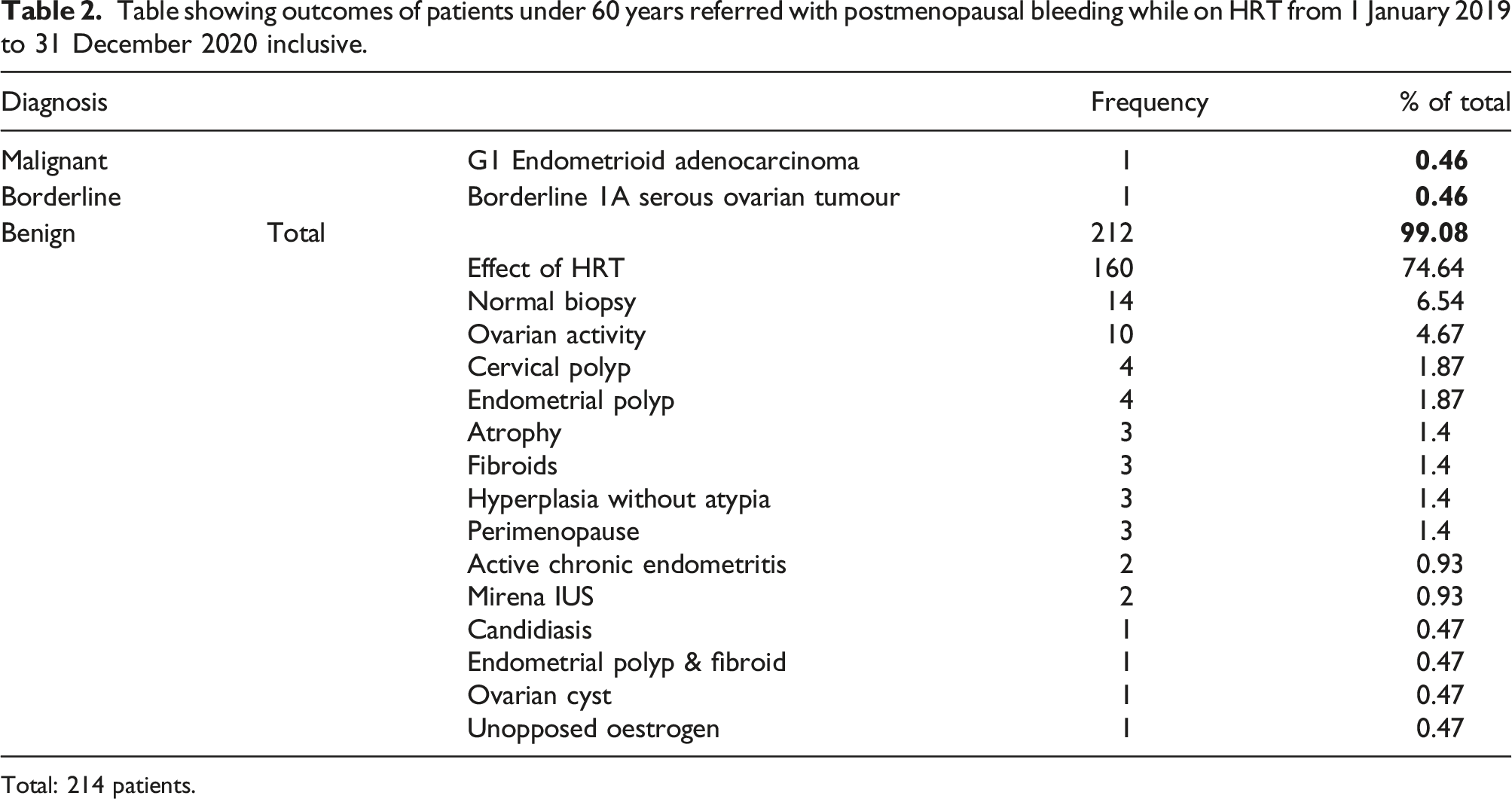
Total: 214 patients.
Table showing outcomes of patients under 60 referred with postmenopausal bleeding, not on HRT, from 1 January 2019 to 31 December 2020 inclusive.
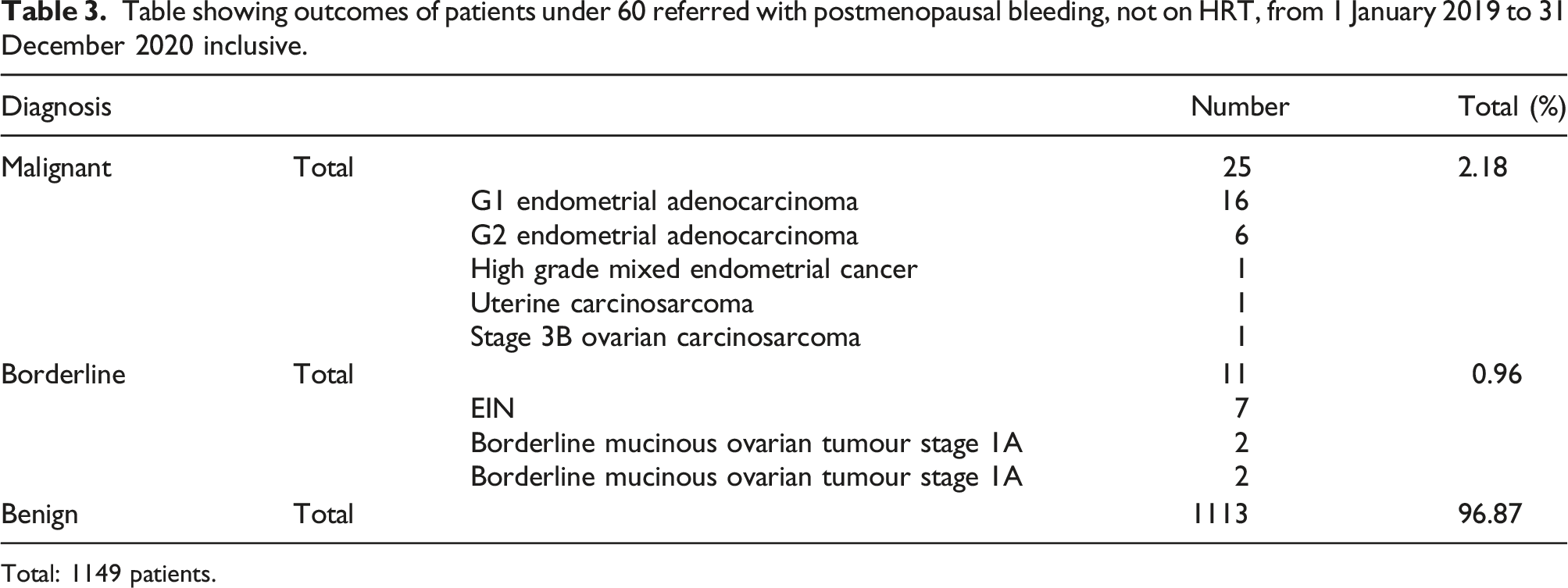
Total: 1149 patients.
Within the study 552 women were under age 55 years and of these 83 were taking HRT. 445 were classed as postmenopausal by the clinician reviewing the patient. One of these HRT users was the patient diagnosed with borderline serous tumour of the right ovary previously mentioned. No other HRT users under the age of 55 yrs were diagnosed with cancer or borderline tumours; however, in the non-HRT users aged under 55 yrs, there were 5 diagnoses of cancer and 3 borderline tumours (one of which was taking tamoxifen).
In subset data analysis of referrals between 1st January 2020 and 31st December 2020, a total of 114 referred women included in the study were using HRT and at least 12 reported a recent change of HRT within the last three months (11%).
Discussion
Main findings
The endometrial cancer detection rate was very low for patients under 60 years of age referred with PMB whilst using HRT. This knowledge could help triage referrals so that patients can be relatively reassured at presentation and directed to the clinic best suited to manage their presenting problem. This may be within the primary care setting involving a GP with a specialist interest in menopause or women’s health or by referring to a specialist menopause/HRT clinic in secondary care for patients with bleeding on HRT on a non-urgent basis, preserving the 2 week wait referral clinics for those most likely to have significant pathology. This is very dependent on the services available in the local area to determine the most appropriate setting for review and if necessary investigation.
Strengths and limitations
This study evaluated a large number of patients referred over a two-year period both before and during the COVID pandemic. All patient outcomes were analysed to determine the significance of HRT with regards to diagnosis. This study confirms previously published data regarding the frequency of irregular vaginal bleeding within the initial two years of use and when there may be changes to the preparation including type or dose of therapy.2,3 Other work also revealed similar very low detection rates of significant endometrial pathology in women using HRT. 4
This study was limited by its retrospective nature investigating referrals within a single unit. The numbers of patients on HRT were not matched to non-HRT but this was representative of our referral population. Review of patient case notes could provide limited detail of HRT use or recent changes.
Interpretation
Up to 77% of women commencing continuous combined HRT will report irregular bleeding within the first few months. This decreases to 10% after nine months unless using transdermal preparation when up to 20% may still report irregular bleeding.9–12 This is even more common with sequential users with up to 40% reporting irregular bleeding.10,13,14 The Million Women Study reported HRT had significant and contrasting effect on the risk of endometrial cancer depending on preparation and the women’s BMI over a follow-up period of 3.4 years. Continuous combined users had a reduced risk of endometrial cancer but for those on cyclical preparations the risk was not significantly different from non-users. 15
Feeley and Wells concluded in their review that there is a low probability of clinically relevant pathology when an endometrial biopsy is obtained from women using HRT. 16 This statement was predominantly based on a large UK multicentre study that demonstrated no endometrial hyperplasia or malignancy in women using combined continuous HRT, even after previous sequential HRT with a diagnosis of hyperplasia. 17 The ten year study by Mossa et al demonstrated a higher incidence of abnormal uterine bleeding amongst postmenopausal women using HRT as well as an increased endometrial thickness (ET). This was measured using transvaginal sonography (TVS) with 5 mm or more classed as increased. Despite these findings, there was no correlation with any significant difference in malignant endometrial pathology. 18
A randomised control trial of 246 patients aged 41–57 years with minimum 12 months amenorrhoea commenced on one of two HRT regimens. Vaginal bleeding was reported in approximately 40% at six months regardless of regimen used and 30% at nine months. This reduced to under 20% at one year. No endometrial cancer was detected with either regimen following endometrial sampling of all patients at 12 months. 4 In addition, a large cross-sectional study including 750 women using HRT demonstrated that they were significantly less likely to be diagnosed with endometrial cancer (odds ratio 0.229). 19 In a recent retrospective study comparing women with unscheduled bleeding on sequential or continuous HRT, the presence of hyperplasia without atypia was similar in both groups (0.5 and 0.4%, respectively). With regards to hyperplasia with atypia or endometrial cancer the incidence was 2% and 1%, respectively. 20
Lou et al conducted a review of the literature in 2017 regarding unscheduled bleeding on HRT and whether endometrial assessment is necessary. They concluded unscheduled bleeding is common with both sequential and continuous HRT at least within the initial 6 months of use. They also state two-week wait pathway referral is unnecessary given the low probability of malignancy; however, beyond the initial six months endometrial assessment is warranted. 21
NICE guidance for suspected cancer diagnosis recommends women aged 55 years and over with PMB are referred on a suspected cancer pathway for an appointment within two weeks. For women aged under 55 years, however, it suggests this referral pathway should be a consideration but is not mandatory due to the rarity of malignancy in these women. 22 Our data is supportive of this advice and may assist in providing reassurance both the patient and care provider regarding managing these symptoms within the primary care setting or by routine referral processes to specialist clinics if available. Many women will choose to commence HRT prior to a full year of amenorrhoea making it difficult to determine if they are truly postmenopausal or if their symptoms are due to ongoing ovarian activity or HRT itself. By NICE guidance, the definition is stated as unexplained vaginal bleeding more than 12 months after menstruation has stopped. This allows, therefore, some interpretation with regards to the use of HRT. The British Gynaecological Cancer Society (BGCS) recommends in addition to those with PMB as defined by NICE, women who have stopped HRT for at least six weeks presenting with persistent or new onset unexplained bleeding should be referred urgently. 23 Our study provides further evidence of the low cancer detection rate in HRT users under 60 years of age and may facilitate the production of clearer guidance regarding how these patients should be managed. Ideally this should be collaborative guidance from the BGCS and British Menopause Society as well as NICE for realistic expectation of how these patients can be managed.
The review article by Dave et al provides recommendations on the initial assessment plan for unscheduled bleeding on HRT. This specifies that with less than six months use of continuous combined HRT no investigation is necessary. Beyond this timeframe, transvaginal ultrasound (TVUSS) to evaluate ET should be requested. For patients on sequential HRT with heavy, prolonged or breakthrough bleeding in more than two cycles TVUSS should be requested. Different acceptable values of ET were specified with an ET of 5 mm or more requiring endometrial assessment (either biopsy alone or with the addition of hysteroscopy) for continuous combined HRT users and an ET of 7 mm warranting endometrial assessment in sequential HRT use. An endometrium of less than 5 mm does not require further investigation as the risk of endometrial cancer in this group is reduced by 90% regardless of the HRT regimen used. If bleeding persists or recurs this should be re-evaluated. Consideration is also required in the presence of high-risk factors including raised BMI or Lynch syndrome or a family history suggestive of Lynch syndrome. 24 The findings of our study with a very low rate of endometrial cancer concur with this review. The limitation of this review is that it is only available in The Obstetrician and Gynaecologist journal and is unlikely to be readily accessible by primary care providers. Incorporation of this review into new guidance would be beneficial to both primary and secondary care services to streamline referrals and manage patient ideas, concerns and expectations.
Conclusion
Endometrial cancer detection rate in women under 60 years referred with PMB is low. This is significantly lower if the woman is using HRT. Referral on a two-week wait pathway for suspected cancer diagnosis induces stress and anxiety for the woman and may lead to potentially unnecessary invasive uncomfortable investigations in a group of women with a very low risk of endometrial cancer. We propose women under 60 years with PMB on HRT or who have had a change to their prescription within the last 6 months should be seen on a non–two-week wait pathway and managed in a specialist menopause/HRT clinic instead. In the presence of significant other risk factors such as obesity, the decision to refer on the two-week wait pathway may still be appropriate and would be at the discretion of the referring clinician. Patients can be reassured however, that there is a low statistical probability of endometrial cancer. Referral on the two-week wait pathway should be reserved for those with persistent bleeding after six months of HRT, following cessation of HRT six weeks previously, and for non-HRT users who have PMB in accordance with NICE guidance.22,23
Footnotes
Acknowledgements
We would like to thank Lesley Mercer for assisting with the database to identify patients referred based on our inclusion criteria.
Author contributions
Charlotte Buchanan is a Specialty Registrar in Obstetrics and Gynaecology in South Yorkshire and was involved in the literature search, data analysis and writing up of the study.
Megan Robinson is a GP Registrar who completed a hospital rotation within the Obstetric and Gynaecology department at the Jessop Wing, Sheffield. She was involved in the literature search, data extraction and analysis.
Madeleine Macdonald is a Consultant Gynaecological Oncologist at the Jessop Wing, Sheffield and was responsible for the conception, planning, study selection and supervision.
Author’s note
The authors used the STROBE cohort reporting guidelines to complete this report. 25
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
CB.