
Abstract
Objective
To evaluate the impact of a short-term cognitive-behavioural therapy (CBT) protocol on menopausal symptoms and quality of life in women undergoing menopause.
Study Design
A short-term individual CBT protocol was developed. Peri- and post-menopausal women with symptoms were enrolled and assigned to either the experimental group (CBT) or the waitlist (CTL group) by patient’s decision.
Main Outcome Measure
Three validated questionnaires were used to assess psychological well-being before (T1) and after (T2) the intervention: the Menopausal Rating Scale (MRS), Clinical Outcomes in Routine Evaluation - Outcome Measure (Core-OM), and the World Health Organization Quality of Life in the short version (WHOQOL-BREF).
Results
Forty-eight women were included, 24 in each group. At T1, the CBT group had worse scores than the CTL group across all questionnaires. At T2, the CBT group showed significant improvement in all measures, while the CTL group experienced significant worsening in CORE-OM and WHOQOL-BREF scores, with stable MRS scores. In the MRS, at T2 the CBT group showed significant reduction in both the psychological and somatic sub-domains (<0.001), while the CTL group’s scores remained unchanged. In the CORE-OM, the CBT group showed significant improvement in the well-being (p = .002), problems (p = .005), and functioning (p = .001) sub-domains, while the CTL group had significant declines. In the WHOQOL-BREF, the CBT group demonstrated significant improvements in all domains (p < .001), while the CTL group declined.
Conclusion
A short-term tailored individual CBT protocol is effective in managing menopausal symptoms, helping women develop the resources and coping strategies needed to adjust to this complex period.
Introduction
The menopause and menopausal transition can be one of the most challenging times in a woman’s life, especially due to the onset of signs and symptoms resulting from the cessation of ovarian function.1,2
These changes can have a significant impact and may also make some women more vulnerable to the development of mental health issues.3,4 Furthermore, each of these symptoms can be greatly influenced by the emotional state.
Women’s experience of menopause and menopausal transition can significantly vary from person to person. Literature acknowledges that menopause is not a ‘universal’ syndrome 5 and the lived physical or psychological symptoms have different and unique patterns. 6
Menopausal hormone therapy (MHT) can help to overcome physical and psychological symptoms while also improving quality of life.3,7–10 However, in cases of clinical contraindication to the use of hormones or in the absence of medical indications to the prescription of MHT, medical alternatives may be limited and are usually focused separately on vasomotor or genital syndrome of menopause symptoms. Furthermore, even when MHT is prescribed, psychological distress may not always improve.
The possibility of psychological support in addition or alternatively to medical treatment may therefore be useful in symptomatic women.
Cognitive-behavioural therapy (CBT) has been proposed as a treatment for menopausal symptoms and its psychological effect on the quality of life is recognized by many authors and guidelines such as NICE. 11 CBT is a short-term therapy focused on modifying maladaptive thoughts and behaviours underlying emotional distress, including the patient’s dysfunctional attitudes, beliefs, and cognitive patterns. 12 The CBT protocol adapted for menopausal symptoms (CBT-Meno) includes psychoeducation sessions and cognitive and behavioural strategies. CBT-Meno has shown its effectiveness particularly in improving vasomotor, depressive, and sexual symptoms.13,14 Most of the studied CBT interventions are conceived as 6–8 weekly sessions of 90–120 minutes in small groups, while some authors also described individual sessions, CBT-self guide interventions, and online sessions.11,15,16
The aim of this study was to assess the effectiveness of a structured short-term individual face-to-face CBT protocol designed for women facing the menopause and menopausal transition. This tailored CBT intervention aimed to target both the cognitive and behavioural aspects of menopausal-related distress, helping participants develop adaptive coping strategies for managing physical symptoms and psychological challenges associated with this life stage.
Materials and methods
The study protocol was approved by the Medical Ethics Committee of IRCCS Azienda Ospedaliero-Universitaria S. Orsola Malpighi, Bologna, Italy (EU199/2017/O/Oss) and written informed consent was obtained from all participants in accordance with the 1975 Helsinki Declaration.
All subjects were recruited at the Outpatient Clinic of Gynaecology and Physiopathology of Human Reproduction Unit, IRCCS Azienda Ospedaliero-Universitaria of Bologna, Sant’Orsola University Hospital, between January 2019 and December 2019.
The inclusion criteria were: - Age between 40 and 60 years old. - Diagnosis of menopause or menopausal transition according to the criteria of the American College of Obstetricians and Gynaecologists (ACOG)
17
: menopausal state was defined as absence of menstruation for at least 12 months.
10
Menopausal transition was defined as the time that begins with the first onset of menstrual irregularity and ends 1 year after amenorrhoea has occurred.
18
- Absence of current psychiatric disorders or cognitive dysfunctions. - Reported psychological distress due to menopausal status and/or the related symptoms, assessed with validated questionnaires.
The exclusion criteria were the current use of MHT and/or psychiatric drugs.
During the routine gynaecological examination, a specifically trained gynaecologist evaluated the severity of menopausal and psychological symptoms reported by the women as reported in inclusion criteria, their medical conditions, and the presence of any contraindication. Subjects were informed about the possibility of undertaking a psychological support path with a specialized psychologist from our team.
The gynaecologist provided information material to the interested women concerning the general purpose of the research, the methods of data use, and the right to withdraw from the study at any time. Additionally, for those willing to participate, informed consent was obtained.
Each participant completed three questionnaires to assess her psychological well-being before receiving the treatment (T1).
Some additional data were collected from the subject by consulting medical records: • Age • Presence and duration of amenorrhoea • Medical conditions • Current or past therapies • Marital status and duration of the relationship.
The enrolment was progressive and included at least 48 women based on the power calculation (see 2.3 Statistics). After December 2019, we stopped enrolling due to the interruption of the psychological support service in our Menopause Clinic for organizational issues.
Women were given the possibility of undertaking psychological support (experimental group, named CBT group) or to return after 4 months (control group, named CTL group). Patients in both groups were then asked to complete three questionnaires to compare the results before and after CBT (T2).
Measurements
Three validated questionnaires were used to assess psychological well-being, menopausal symptoms, and quality of life: Menopausal Rating Scale (MRS), 19 Clinical Outcomes in Routine Evaluation - Outcome Measure (Core-OM),20–22 and the World Health Organization Quality of Life in the short version (WHOQOL-BREF).23,24 The detailed description of these scales is reported in Supplemental Materials S1. “MRS, Core-Om, WHOQOL-BREF description”.
Clinical intervention (CBT)
The clinical intervention proposed in this study was a short-term CBT, consisting of one individual face-to-face session per month, for four consecutive months. Each session was 1 hour (h) long, except for the first interview which lasted 1 h and 15 minutes, and took place in a dedicated room within our Clinic.
The intervention was conducted by a psychotherapist responsible for the Gynaecology and Obstetrics Unit, with clinical experience in CBT techniques in the gynaecological field, who relied on an individualized case formulation to adapt the focus of each session to the woman’s specific symptoms and priorities. This intervention focused on helping patients understand how their perceived emotional distress was triggered by their organic condition, in a bio-psychosocial perspective, thus considering not only hormonal changes but also expectations, symptom evaluations, and mood.
The treatment was centred on developing the patients’ ability to adapt to the physiological changes that menopause entails. Through psycho-educational interventions aimed at raising awareness of the meaning of menopause as a new life phase and cognitive-behavioural techniques to stimulate the skills needed to adapt to it, women were supported in responding to the experience of change, and in regaining control of their previous psychological function.
The first session started with a collaborative review of the woman’s responses to the administered psychometric scales, allowing for an objective assessment of symptom severity and self-reported psychological distress. This helped the clinician evaluate whether the subject perceived menopausal changes as a natural physiological transition rather than a pathological condition and identify key areas to focus on in subsequent sessions. A functional and fundamental approach is to help the woman develop a perspective focused on functionality rather than pathology, supporting her in understanding a new phase of life with its unique characteristics, as well as in recognizing the interconnection between the various symptomatic manifestations.
The focus of each structured session varied based on the woman’s menopausal stage and the symptoms experienced as most urgent and disruptive to quality of life. CBT targeted the restructuring of maladaptive thoughts and the modification of unhelpful behavioural patterns. For example, in women reporting significant sleep disturbances, cognitive restructuring was used to adjust unrealistic expectations about sleep patterns. Similarly, in cases of decreased libido, psychoeducation and cognitive reframing helped patients understand that this change could, at least in part, reflect a physiological response to the hormonal shifts typical of menopause. CBT thus supported the restructuring of dysfunctional beliefs – such as catastrophizing or attributing the decline exclusively to personal or relational dysfunction – and the emergence of behavioural patterns oriented towards restoring sexual quality of life. By promoting a cognitive shift towards viewing symptoms as part of a natural adaptation process, women reported reduced psychological distress and an improved ability to cope with menopausal changes.
At the end of each session, specific goals, exercises, and tasks were set which were then reassessed at the following meeting.
Statistics
Descriptive statistics for continuous parameters were reported as mean and standard deviation (SD) or median and interquartile ranges (IQ 25th–75th) upon verification of the normality of the distribution through the Shapiro-Wilk test. Categorical variables were expressed as absolute frequencies and percentages. Pairwise comparisons of independent observation were performed by the Student t test using the Welch correction where appropriate. Not normally distributed data were compared by the Mann–Whitney U test. The Chi-square test was used to compare proportions between the CTL and CBT groups. All tests were two sided and P-values <0.05 were considered statistically significant.
We performed a power analysis, so the number of subjects enrolled was based on a mean MRS change score of approximately 20% (2-point increase from baseline). Therefore, with an anticipated power of 80% and a significance level of 5%, at least 24 subjects in each group were enrolled.
Data analysis was performed using the Statistical Package for Social Sciences (SPSS) version 23 (International Business Machines Corp., Armonk, NY). The significance level was set at five percent, and pairwise deletion of missing data was used.
Results
Descriptive statistics
Fifty-two peri- and post-menopausal women were enrolled. Four women (one in the CBT group and two in the CTL group) did not complete the baseline or 4-month questionnaires and were excluded from the analysis. One woman from the CBT group dropped out after two CBT sessions.
Demographic characteristics of the study population.
Note. n, number; SD, standard deviation; CBT, cognitive-behavioural therapy; CTL, control.
Symptomatology of the study population at baseline (T1).

Note. Data are presented as mean and standard deviation (SD); CBT, cognitive-behavioural therapy; CTL, control; MRS, Menopause Rating Scale; Core-Om, Clinical Outcomes in Routine Evaluation - Outcome Measure; WHOQOL-BREF, World Health Organization Quality of Life in the short version.
Univariate analysis
Menopause Rating Scale (MRS)
Evaluation of MRS, CORE-OM and WHOQOL-BREF between T1 and T2 in the CBT and CTL groups.
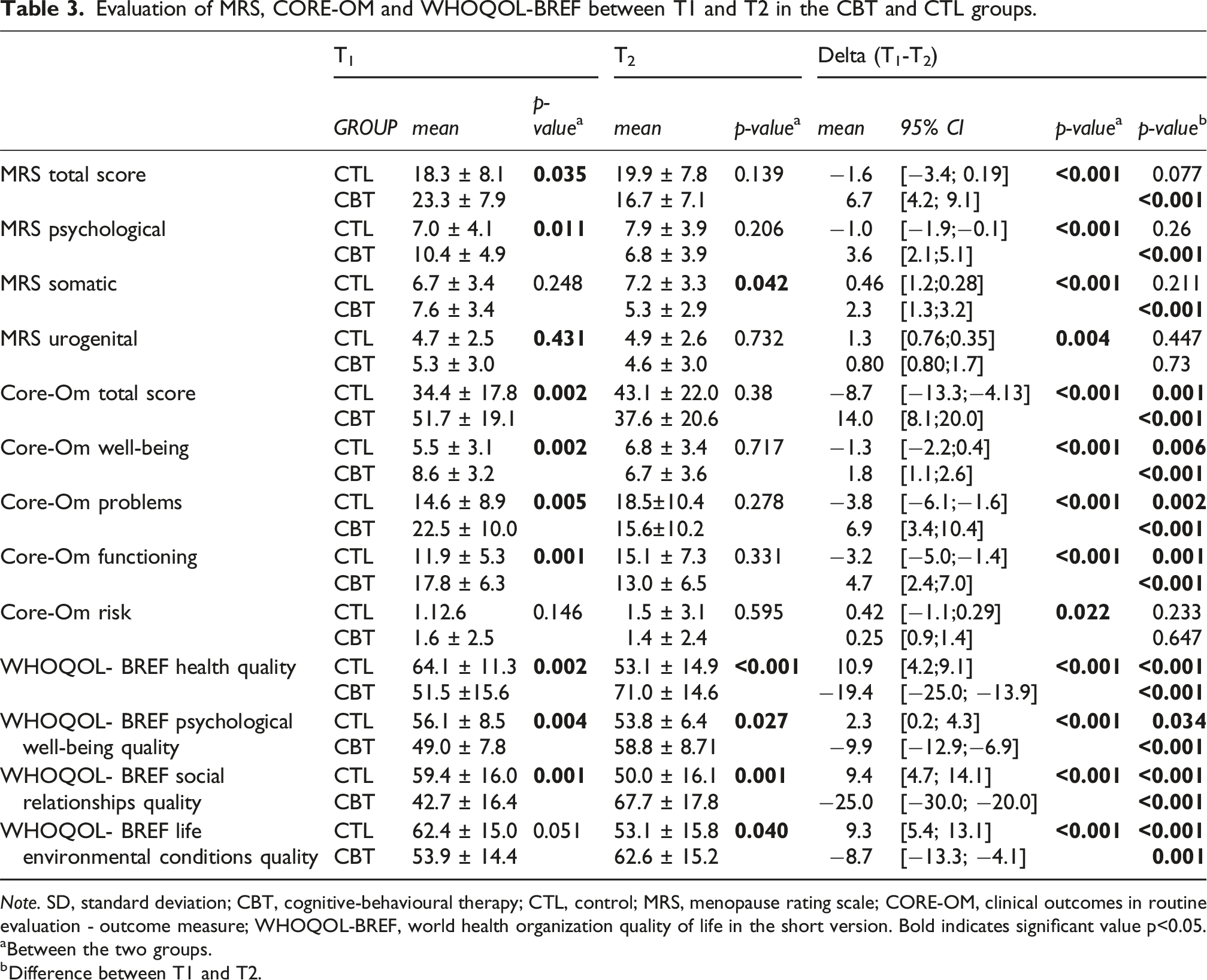
Note. SD, standard deviation; CBT, cognitive-behavioural therapy; CTL, control; MRS, menopause rating scale; CORE-OM, clinical outcomes in routine evaluation - outcome measure; WHOQOL-BREF, world health organization quality of life in the short version. Bold indicates significant value p<0.05.
aBetween the two groups.
bDifference between T1 and T2.
Analysing the MRS sub-domains, we found that at T1 the CBT group had a higher MRS psychological score (CBT mean score 10.4 ± 4.9 vs CTL mean score 7.0 ± 4.1, p = .011), while the somatic and urogenital sub-domains were not significantly different compared to CTL group at T1 (p > .05).
At T2, the CBT group had a significant decrease in both psychological and somatic sub-domains (respectively, mean score <0.001), while the CTL group scores remained substantially unchanged.
In both groups, MRS urogenital score did not change significantly from T1 to T2 and did not differ in any time point between the two groups (Table 3).
CORE-OM
Regarding the CORE-OM, at T1 the CBT group showed a significantly higher mean score compared to the CTL group (CBT mean score 51.7 ± 19.1 vs CTL mean score 34.4 ± 17.8, p = .002), indicative of the presence of greater issues.
Between T1 and T2, however, the CTL group showed a significant increase in the score (CTL mean difference T1–T2: −8.7 [CI –13.3; –4.13]), while the CBT group showed a significant reduction (CBT mean difference T1–T2: 14.0 [CI 8.1; 20.0]) (Table 3).
The same tendency was also observed in the Core-Om sub-domains, except for the Core-Om risk sub-domain.
At T1 the CBT group showed significantly higher scores than the CTL group in the well-being (p = .002), problems (p = .005), and functioning (p = .001) sub-domains. At T2, each group showed a statistically significant variation from baseline in the Core-Om well-being (CBT p < .001; CTL p = .006), problems (CBT p < .001; CTL p = .002), and functioning (CBT p < .001; CTL p = .001) sub-domains as well as in the total score. But whereas the CBT group showed a significant increase (and therefore an improvement), the CTL group experienced a significant decrease in the three aforementioned sub-domains.
The only sub-domain which did not change from T1 to T2 and did not differ between the two groups at any time point was the Core-Om risk score (Table 3).
WHOQOL-BREF
At T1, the analysis of the four WHOQOL domains scores showed significant differences between the two groups in the first three domains (quality of health, p = .002; quality of psychological well-being, p = .004; quality of social relationships, p = .001), while it was not as evident in the last domain (quality of environmental conditions of life, p = .051).
At T2, we recorded a significant increase in the mean scores of all domains in the CBT group, each with p < .001, and a significant decrease in the mean scores of all domains in the CTL group (quality of health, p = .0034; quality of psychological well-being, quality of social relationships and quality of environmental conditions of life, respectively, p < .001).
The significant difference between the two groups at T2 indicates that after 4 months the quality of life of those who had received psychological support was significantly higher, and the final scores at T2 in the CBT group were also significantly higher than those of the CTL group (Table 3).
Multivariate analysis
To determine whether age, duration of amenorrhoea, or the presence or not of a partner could influence the scores of the three administered questionnaires, multivariate analysis was performed. The only significant variable was the presence or absence of psychological support, except for two WHOQOL-BREF domains: quality of health and quality of environmental conditions of life, where the duration of amenorrhoea also had an effect (Table 1S Supplemental Material).
Discussion
Main findings
The aim of this study was to evaluate the effects of psychological support on a woman’s ability to manage the psychological and physical discomfort caused by menopause. In particular, we designed a structured short-term individual face-to-face CBT protocol (4 monthly sessions of circa 1 h each) for women facing the menopause and menopausal transition, while most of the studied menopausal CBT interventions are conceived as 6–8 weekly sessions of 90–120 minutes in small groups, CBT-self guided interventions or online sessions. 11
We evaluated peri- and post-menopausal women before and after CBT (CBT group) compared to women who did not immediately undergo psychological support (CTL group). At baseline the CTL group had better scores in the MRS, Core-OM, and WHOQOL-BREF compared to the CBT group. After 4 months, women who received psychological support (CBT group) scored better than women who did not receive any psychological support (CTL group). Furthermore, in the CTL group we recorded a worsening of many scores.
At the first evaluation (T1), the CBT group recorded worse scores in each questionnaire compared to the CTL group. This may explain why these women self-selected to undertake immediately CBT. As already mentioned, menopause is a multifaceted entity which may significantly differ in each woman6,25,26 Furthermore, the help-seeking attitude has been proven to vary too among women, according to their symptoms and experiences.27–29
At T2, CBT group had significant improvements in each questionnaire, reaching MRS scores similar to those of the CTL group, and better Core-Om and WHOQOL scores than those of the CTL group. These findings suggest that CBT helped these women improve their quality of life and manage menopausal symptoms better than women who did not undergo psychological support, despite their initial better scores.
Many authors have highlighted the effectiveness of psychoeducation and CBT in improving the quality of life in both men and women, and more recently it has been applied with promising results in post-menopausal women.6,13,14,30–32 In 2022, a systematic review and meta-analysis including 14 RCTs reported that CBT was superior to control groups in reducing menopausal symptoms and improving quality of life, although effects were generally small to moderate. 33
The only significant variable of our study which affected the measures of MRS, CORE-OM, and WHOQOL-BREF, as evidenced by the multivariate analysis (Supplemental Material), was the presence or absence of psychological support. The duration of amenorrhoea affected only the WHOQOL domains of quality of health and environmental conditions of life, probably due to the intensification of the menopausal symptomatology.34,35
In our study women in the CBT group experienced an overall improvement in their psycho-physical well-being thanks to the short-term CBT alone. In line with our results, a review by Samami et al., 36 found that menopausal women experienced an improvement in their well-being and quality of life with short-term CBT interventions. The results showed that the parameters measured by the MRS of the intervention group decreased after four psychological intervention sessions when compared to the control group.
In the studies about CBT-MENO,13,14 the authors demonstrated that their protocol improved menopause-specific beliefs, dysfunctional attitudes associated with depression, and menopause-specific behaviours.
Regarding the parameters more expressly related to psychological well-being evaluated in our study with CORE-OM and WHOQOL-BREF, our results showed that the CBT group had a significant improvement in the total scores as well as in most sub-domains. Conversely, the CTL group showed a significant worsening of the same scores. This finding could be explained by the fact that the women in the CTL group were not followed monthly but were seen directly at month four of follow-up. This waiting time may have led to the sensation of not being properly looked after. Since these women also showed some symptoms of discomfort related to menopause (as highlighted by the MRS scoring), these may have worsened due to the delay in access to the psychological support service.
In the administered questionnaires, the only sub-domains which did not vary significantly between the groups at T1 and T2 were the MRS urogenital sub-domain and the Core-Om risk sub-domain.
The first result could be expected, because the genitourinary syndrome of menopause (GSM) has a physical base, 37 not generally affected by the psychological sphere. Of course, a psychological intervention to better cope with the GSM issues may help to alleviate its burden however the symptoms can persist. Other somatic symptoms such as sleep disturbances and vasomotor symptoms are, on the other hand, strictly connected with emotive and psychological triggers.
The Core-Om risk sub-domain, which was not influenced by the time or the CBT intervention, is meant as an evaluation of the risk of harm to others or themselves. In our study sample, it appears to be low in both groups, consisting with the fact that these women experienced some psychological distress, but not as to be dangerous to their or others safety.
One important advantage of CBT compared to other psychological interventions is that it can be successfully delivered across a huge variety of settings, and that technology-assisted CBT and in-person CBT have shown to be as effective.11,38 In fact, technology-based interventions are intentionally designed to reduce barriers in mental health treatment particularly related to stigma and accessibility. 30
Zhang et al 38 suggested that CBT format (i.e. individual- or group-based CBT) and modality (i.e. CBT only vs CBT with adjunct techniques) can act as significant moderators of the effectiveness of CBT for depression and anxiety treatment, especially describing a significant overall treatment effect only for individual-based CBT studies. Furthermore, in the hospital context, CBT can be a valid option as it requires few sessions and therefore lower associated costs.
Strengths, limitations, and interpretation
One strength of our study is the choice of developing a short-term CBT protocol with four individual monthly in-person sessions of 1 hour each, in contrast to other CBT protocols which are typically delivered in groups.13,14,32 The individual format enables clinicians to tailor the intervention to the needs of the patients and may also represent a more acceptable option for women who prefer not to participate in group settings.
Another strength of this study, compared to previous research, is that we evaluated not only the menopausal symptoms but also the overall quality of life, highlighting the possible general effect of CBT on the well-being of peri/post-menopausal women.
However, we acknowledge that our study has some methodological limitations. The first is that the women were not randomly assigned and chose spontaneously whether to undergo CBT immediately or not, therefore the CBT group women may have been more receptive to managing their symptoms. This auto-selection also resulted in the fact that the two study groups were not homogeneous at baseline in terms of perceived severity of menopausal symptoms and quality of life, and therefore the comparison between the two groups is more challenging. Indeed, the CBT group had lower baseline scores on the questionnaires. However, the CBT group at T2 showed an increased quality of life while CTL group showed a worsened quality of life compared to T1, so this difference could be meaningful even though the starting scores were different.
Another limitation of the study concerns the limited duration of observation. It could be useful to perform a longer follow-up to investigate the duration of the benefits of the short-term CBT intervention. Longitudinal research with a larger sample and follow-ups to monitor the improvements in participants psycho-physical well-being could indeed be included in future developments. Implementing a more standardized CBT support protocol could represent a future research line that could improve the reproducibility and effectiveness of the intervention.
Conclusions
Our study shows that a short-term individual CBT protocol is effective in managing menopausal symptoms, helping peri- and post-menopausal women develop the resources and coping strategies needed to adjust to this complex period. These findings indicate that adapting CBT techniques to the needs of patients with dedicated sessions, is advantageous for women who are experiencing menopause or menopause transition.
Supplemental Material
Supplemental material - The effectiveness of short-term cognitive-behavioural therapy in women facing menopause and menopausal transition
Supplemental material for The effectiveness of short-term cognitive-behavioural therapy in women facing menopause and menopausal transition by Alessandra Lami, Chiara Ferracuti, Matilde Morelli, Maria Antonietta Giosa, Renato Seracchioli, and Maria Cristina Meriggiola, in Post Reproductive Health
Footnotes
Acknowledgements
We thank Julie Norbury for manuscript language editing.
Ethical considerations
The study protocol was approved by the Medical Ethics Committee of IRCCS Azienda Ospedaliero-Universitaria S. Orsola Malpighi, Bologna, Italy (EU199/2017/O/Oss), and written informed consent was obtained from all participants in accordance with the 1975 Helsinki Declaration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not openly available but are available from the corresponding author (AL) upon reasonable request.
Contributorship
All authors contributed to the study conception and design. The first draft of the manuscript was written by Alessandra Lami and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. CF and MCM: Validation and visualization. AL: Data curation and formal analysis. AL and AG: Writing – original draft. AL, MCM, FC, and MM: Writing – reviewing and editing. AG and CF: Investigation. MCM, RS, and CF: Supervision.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.