
Abstract
Background
Lifestyle optimisation and education plays a crucial role in the holistic management of symptoms during the menopause transition as well as reducing the risk of chronic diseases in the post-menopausal period. Provision of lifestyle education tailored to the menopause transition is limited in primary care, largely due to time pressures on general practitioners.
Objective
To upskill HWB coaches in primary care to deliver lifestyle advice and support as part of holistic menopause care.
Study design
A CPD and networking event aimed at HWB coaches was organised following engagement with all relevant stakeholders and collation of baseline data. This event focused on areas of highest demand according to a patient survey of women between the ages of 45 and 55 in a local GP surgery.
Main outcome measures
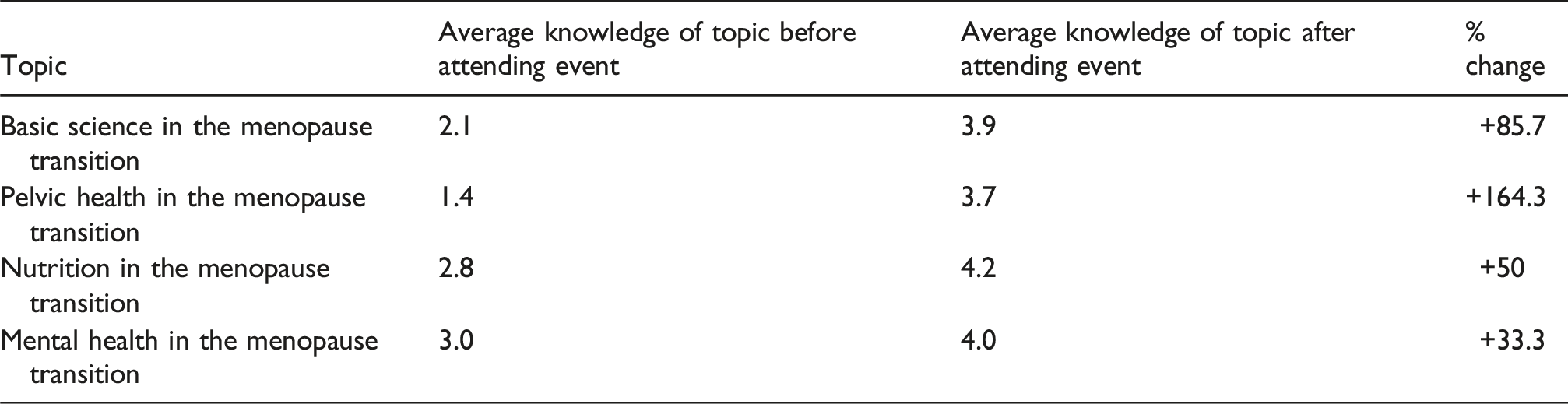
Pre- and post-event feedback was sought. All attendees were asked to rate their confidence on each topic presented at the event.
Results
An increase in confidence in the knowledge of each topic covered at the event was demonstrated by attendees.
Conclusion
This project demonstrated how a simple and focused education and networking event has promoted engagement and collaboration with local HWB coaches, and it has shown a clear increase in knowledge of key topics which can be transferred to their interactions with patients. It is hoped that this will serve as a foundation upon which further work can be done to expand the involvement of HWB coaches and the wider healthcare team to improve access to holistic menopause care in the community.
Keywords
What is the quality problem?
Pressures on primary care mean that lifestyle advice and education delivered to patients presenting to general practitioners during the menopause transition is very limited.
Why is it important?
Lifestyle optimisation plays an important role in the management of menopausal symptoms as well as reducing the risk of chronic diseases which are associated with menopause and post-menopause. Valuable opportunities are therefore currently being missed to improve the short-, medium- and long-term health outcomes of women who present to primary care during the menopause transition.
Aim
Primary aim
The primary aim was to upskill health and wellbeing (HWB) coaches and wellbeing (HWB) coaches in primary care to deliver lifestyle advice and support as part of holistic menopause care.
Achieving the aim will be demonstrated by an improvement in confidence and knowledge across a spectrum of topics relating to lifestyle advice in the menopause transition, as reported by HWB coaches in their pre- and post-event questionnaires.
Secondary aim
The secondary aim was to promote the engagement of HWB coaches in delivering patient education in the menopause transition. This resource can be harnessed to improve menopause care on a wider scale in future.
Background
Over 50% of people in the world will go through the menopause. Menopause is said to affect 13 million people in the UK at any given time and consumes 4% of the NHS budget. 1
In 2022, the British Menopause Society released ‘top ten tips’ – a tool which guides clinicians through evidence-based menopause management for their patients. Its first point is as follows:
‘All women should be able to access advice on how they can optimise their menopause transition and the years beyond. There should be an individualised approach in assessing menopausal women, with particular reference to lifestyle advice, diet modification as well as discussion of the role of hormone replacement therapy (HRT)’. 2
For NHS GPs, managing the menopause transition and the complications thereof are bread and butter. However, GPs rarely have the opportunity to provide the holistic level of care as is desired by them, their patients and the aforementioned standard guidance. A discussion which focuses on the importance of lifestyle is unfortunately the great exception rather than the rule. This is worrying – yet unsurprising – given that an average GP consultation is allocated only 10 min. As a result of this, lifestyle modification is often neglected in practice; particularly when media coverage in around HRT in recent years has prompted a sharp focus on pharmacological treatments in the menopause transition.
The role of hormone-replacement therapy HRT in menopause care is undisputed. It remains part of the first-line management of several menopausal symptoms and has proven benefits when used as recommended. 3 However, it is worth acknowledging that many women may not wish to use HRT – ‘it is neither needed nor required by every woman, and does not treat everything!’. 4 A recent study 5 found that 95% of women would prefer to use alternative therapies prior to HRT. Furthermore, there are a few cohorts of women in whom the risk of taking HRT outweighs the benefit, for example, those who have or have had an estrogen-dependent cancer.
Lifestyle modification is not only proven to help manage several common menopausal symptoms such as hot flushes, 6 but it also plays a crucial role in optimising a woman’s health during the menopause transition and her entire life thereafter, by limiting the adverse health implications seen after menopause.
Menopause, and the post-menopausal state, is associated with an increased risk of several chronic diseases such as osteoporosis, cardiovascular disease and type 2 diabetes. 5 Cardiovascular disease is the leading cause of morbidity and mortality in women.7,8 Osteoporosis is thought to affect over three million people in the UK, the majority of whom are post-menopausal women. 9 Similarly, symptoms of pelvic floor dysfunction often become more severe due to decreased estrogen in menopause, which can have a profoundly negative effect on quality of life. 10 Mental illness is also more prevalent during the menopause transition; and feelings of anxiety, low mood and brain fog can be as or even more debilitating than physical symptoms. 11 Modifiable risk factors for these conditions – for example, obesity – need to be addressed as part of holistic healthcare during the menopause transition.7,12 The menopause transition offers an opportune time to optimise lifestyle measures in order to minimise the risk of ageing-related disease. 13
Historically, discussion around menopause has been extremely limited due to a multitude of reasons including social taboo. Consequently, the lack of education and research around menopause has resulted in many women having limited knowledge of the topic. This can lead to confusion over how best to optimise their health during the menopause transition. 5 Delivery of reliable information from trustworthy sources is vital, particularly as we are already seeing this care gap being filled both by private practice as well as sources online which are of variable quality. 14
GP-led group consultations for menopause have been piloted in the UK – Sally Rushton has demonstrated the benefits of this in 2023. 15 Despite the encouraging outcomes, the main cited limitation was that it took up a significant amount of GP time, as no other team members felt confident to deliver relevant information to patients. Future aspirations from this pilot included linking in with other colleagues who may be keen to implement group consultations in this format. This prompted an interest trying to address this problem in primary care. Case studies on group consultations by NHS England refer to the benefits of integrating non-clinical professionals such as social prescribers into group consultation initiatives, highlighting the holistic approach this could offer participants. 16
HWB coaches are members of the primary care team who are contracted locally by Childwall & Wavertree Primary Care Network (PCN). Health coaches are already embedded in many primary care teams in Merseyside and around the country. Their role is defined as follows in the NHS Workforce Development Framework published in 2023
17
: Health and wellbeing coaches work with people with physical and/or mental health conditions, people with long-term conditions and those at risk of developing them. They focus on improving health related outcomes where lifestyle modification and self-management have a significant impact on outcomes and prognosis, by working with the person to set personalised goals.
The HWB coach profession has been shown to offer several benefits both for individual patients as well as wider teams and systems across healthcare. The scope of work of an HWB coach is continuously evolving; however, the framework provides a robust outline of the competencies and limitations of the role within the healthcare team. 17 The potential benefit that this role can bring to menopause care in the community has been explored in this project.
Method
Engagement of stakeholders and gathering baseline data
GPs
Once the main quality problem had been identified, a meeting was held with local GPs who have an interest in women’s health. This served as a brainstorming exercise around the obstacles faced by GPs in delivering good lifestyle advice to patients during a consultation relating to the menopause transition. Time constraint during a 10–15-min consultation was by far the biggest challenge. Information was also gathered on what relevant resources already exist locally in supporting patients with the menopause transition. Examples of existing support included a local ‘Menopause Café’, as well as Liverpool-based women’s charity ‘WHISC’. The discussion also highlighted a wider concern over the ongoing challenges faced in accessing weight management programmes and timely mental health support. The consensus amongst colleagues was that there is nowhere to signpost women in the menopause transition for support with obesity, given that the regional weight management services have very strict criteria for accepting patients. Similarly, long waiting lists mean that patients rarely access timely mental health support such as talking therapies and cognitive behavioural therapy (CBT). Finally, the brainstorming exercise also extended to discussing potential ideas for change. HWB coaches were identified as existing members of the primary care team who are well-placed to address some of the care gaps in the delivery of menopause care.
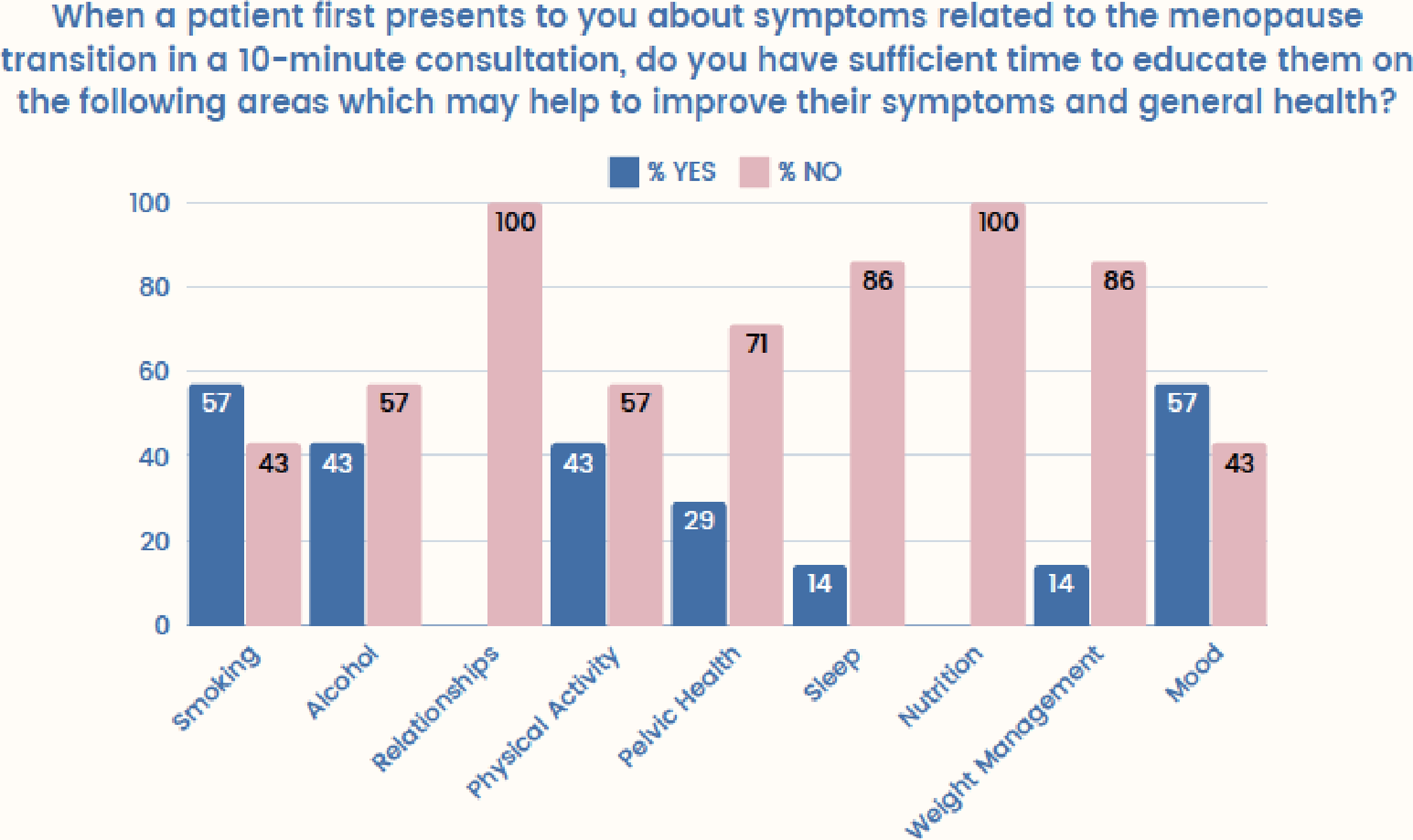
A short survey was also circulated to all GPs in the Childwall and Wavertree PCN, to establish which elements of lifestyle advice they would routinely incorporate into a consultation relating to menopause. This highlighted some clear areas of deficit.
Patients
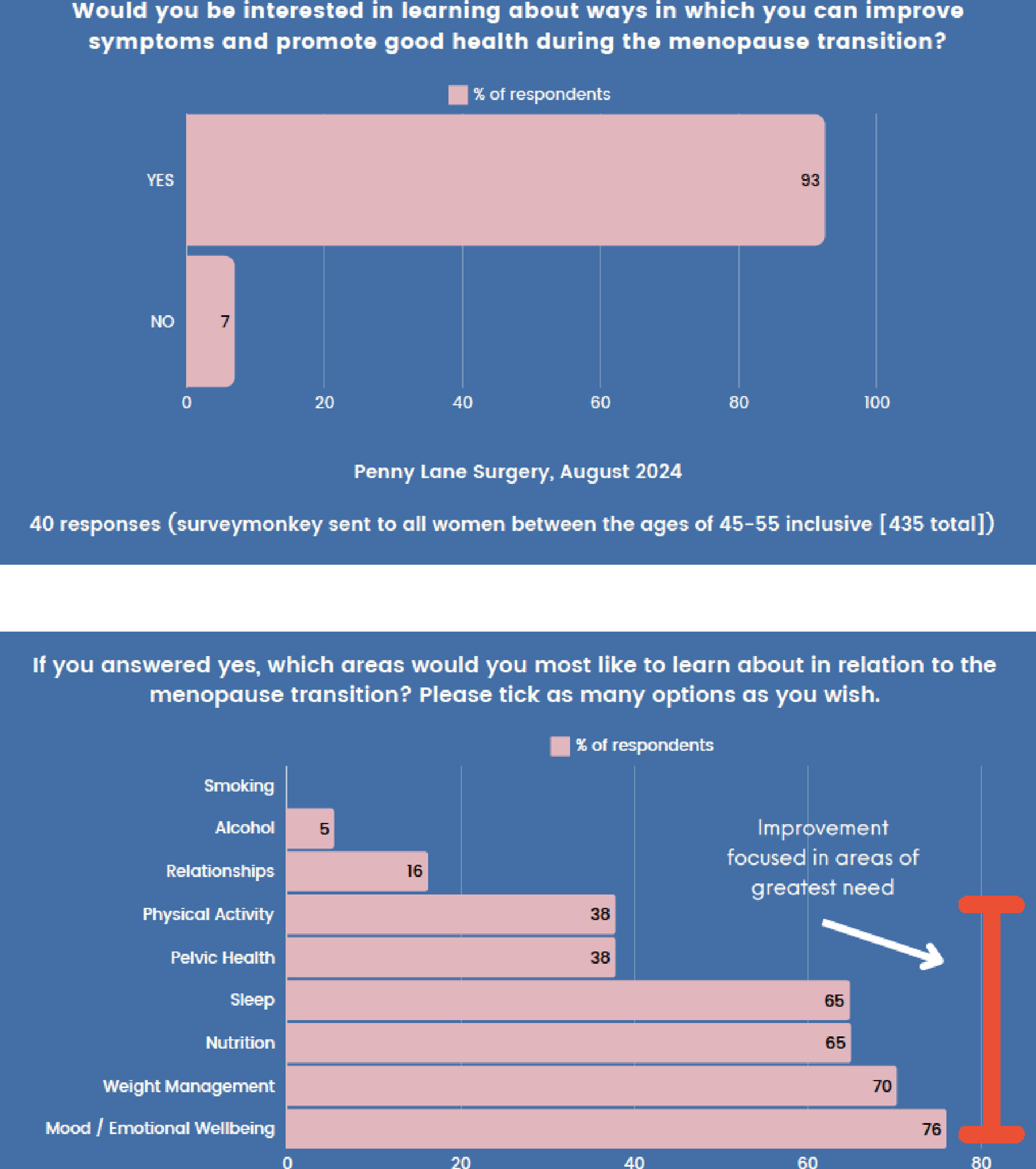
Female patients registered at Penny Lane Surgery between the ages of 45 and 55 were also sent a survey to establish the interest in lifestyle education during the menopause transition, and for which topics specifically there was the highest demand.
Health and wellbeing coaches
A meeting was then held with three HWB coaches employed by Childwall and Wavertree Primary Care Network. This enabled the quality problem to be presented initially to a small team of HWB coaches, and to canvas opinion and promote engagement with the project. It was felt by the whole team that HWB coaches are already supporting patients during the menopause transition in their existing roles by promoting a healthy lifestyle, including aspects of both physical and mental wellbeing. However, the team did not feel confident in their knowledge about aspects of lifestyle advice which are more specific to the menopause transition. This highlighted the need to obtain information on what they felt was required in order to upskill them in this area. The consensus was that a CPD and networking event with expert speakers would be valuable in improving knowledge as well as forming connections to allow collaboration with the wider multi-disciplinary team involved in menopause care. It was also acknowledged that within the team of HWB coaches there is a broad range of skill sets and prior experience across all aspects of lifestyle advice – for example, some HWB coaches have foundations in psychology and are skilled in managing mental health, whilst others have previously worked in the fitness industry.
Primary care network
Leaders of the Childwall and Wavertree Primary Care Network were consulted prior to and during the project. Their involvement and existing contacts enabled a suitable venue for the education event to be secured. Involvement of the care coordinator for the primary care network also ensured that sufficient protected learning time was allocated for HWB coaches to attend the education and networking event, and also benefited the advertising and communication leading up to the event.
Secondary care colleagues
Discussion with existing contacts in the menopause service at Liverpool Women’s Hospital enabled recruitment of expert speakers for the education and networking event, all of whom generously volunteered their time. The menopause service is experiencing enormous pressure due to the volume of referrals they receive. There was positive engagement from all specialists involved who were keen to support the project, acknowledging the potential benefit it would provide to our mutual patients as well as both primary and secondary care teams.
Quality improvement tools and techniques used
(1) Fishbone diagram – to establish root causes (see Appendix 1). (2) Stakeholder analysis (see Appendix 2). (3) Driver diagram – to generate ideas for change (see Appendix 3).
Implementation
The abovementioned steps resulted in the decision to host a CPD and networking event. Once a date and location were secured, the local primary care network care coordinator helped to advertise the event and facilitate protected learning time for attendees, and once all Health & Wellbeing Coaches from Childwall and Wavertree PCN were accounted for the invitation was shared more widely across HWB coaches in Cheshire and Merseyside. There were also some attendees from other disciplines such as nursing; however, the event was tailored specifically towards Health & Wellbeing Coaches. The event was held at Nuffield Health Fitness & Wellbeing Gym in Liverpool who kindly provided an event space with refreshments. Following a general practitioner introduction on the project, expert speakers were invited to educate attendees about topics which correlated with the topics highlighted as most in demand by patients – mental health, incorporating mood and sleep; nutrition including weight management; and pelvic health. Speakers involved were a Consultant Psychiatrist specialising in women’s health, Consultant Pelvic Physiotherapist and Dietetic Manager – all of whom are based at Liverpool Women’s Hospital Foundation Trust. Time was allowed for Q&A sessions, informal discussion and networking. Pre- and post-feedback was arranged.
Outcomes
The feedback questionnaire also asked whether the attendees enjoyed the event and whether they would recommend the event to a colleague. All attendees answered ‘yes’ to both questions. Open feedback and an opportunity to leave comments were also offered.
Discussion
Most menopause management in primary care is currently delivered by GPs. As demonstrated, advice and education around lifestyle modification is a neglected area of care.
It is clear that much needs to be done to train primary care teams in the management of menopause in order to respond to the enormous demands and pressure in this area.
The lifestyle advice and education surrounding the menopause transition does not require a general practitioner or clinical specialist to do so. It does, however, require a good understanding of menopause and menopause-specific education, as well as ongoing support from and collaboration with clinicians.
By including and upskilling our existing valuable HWB coach colleagues in our multi-disciplinary team approach to deliver holistic menopause care and targeting the crucial role of lifestyle modification, we may stand a better chance of achieving this, particularly where funding and resources are limited.
This project has demonstrated how a simple and focused education and networking event has invited HWB coaches across the city to engage proactively with providing lifestyle advice during the menopause transition, and it has shown a clear increase in knowledge of key areas which can be transferred to their interaction with our patients.
Developing this collaboration within our existing teams makes it possible for individualised and patient-centred care to be delivered efficiently to patients by those who are best-placed to do so, in locations which are familiar and accessible to patients. This should consequentially help to reduce load on clinical teams in both primary and secondary care.
It is hoped that this project has established the foundations for improving access to holistic menopause care in the community and will serve as a springboard for further collaboration with HWB coach colleagues and the wider MDT. It also opens the door to HWB coaches working towards delivering education in a variety of formats, including 1:1 and group consultation.
Aspirations and future plans: (1) Further education and networking events to educate the educators, covering different topics using a similar format to further upskill HWB coaches. (2) Trialling group consultations which could be led by HWB coaches and supported by GPs – see previous example piloted.
15
(3) Standard practice to offer patients who present during the menopause transition an opportunity to book in with an HWB coach to identify areas where lifestyle can be optimised – this may also be an opportunity to increase uptake of health screening such as cervical screening, breast screening and cardiovascular assessments. (4) Ongoing collaboration between primary and secondary/tertiary care to support further learning and nurturing relationships between all teams caring for women in the menopause transition. (5) Potential expansion of role of HWB coach into secondary care teams as well as primary care.
Balancing measures
Discussion during the event did highlight some unintended consequences of implementing the next steps of the project: (1) During informal discussion, there was concern about whether HWB teams are properly equipped and resourced for potentially higher referral rates from GPs and patients. (2) Discussion around the notion that delivery of lifestyle advice does not and should not replace a medical consultation with a GP – the intention is to improve and support delivery of the non-medical aspect of menopause care rather than replacing the discussions around medical issues.
Footnotes
Acknowledgements
We would like to thank Dr Nicola Thorbinson, Julie Clark and Nuffield Health Liverpool for their support in the organisation and hosting of our CPD event. We are grateful to the Health and Wellbeing Coaches working within Childwall and Wavertree PCN for their engagement during the early stages of the project, as well as local GPs with interests in women’s health – Drs Benazir Ansari, Helen Canning, Monica Khuraijam and Stephanie Cook – who also offered their ideas and support. Finally, we would like to express our thanks to Catherine Gallagher, Kate Walsh and Dr Helen Reynolds at Liverpool Women’s Hospital who shared their time and expertise as guest speakers during our CPD event.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
KL.
Appendix
(1) Fishbone diagram – to establish root causes.
(2) Stakeholder Analysis.
(3) Driver Diagram – to generate ideas for change.
(4) Event flyer.