
Abstract
Background
Care pathways are essential to ensure continuity, quality, efficient use of resources and positive patient outcomes. Although patient satisfaction is widely considered a major indicator of care quality, it remains largely unexamined in the context of care pathway implementation. The aim of this study was to assess patient satisfaction during implementation of a care pathway for recurrent surgeries.
Method
A newly designed questionnaire was utilized to examine patient satisfaction among adult patients hospitalized for visceral surgery at the University Hospital of Lausanne (CHUV). Analysis was conducted through nine care pathways frequently performed in visceral surgeries.
Results
Of the 280 patients surveyed, 258/280 (92%) of patients were satisfied with information received, 255/280 (91%) with the safety and 210/280 (75%) with their involvement in decision-making and care.
Conclusion
Patient satisfaction ratings of the care received during the care pathway were high. Complete and personalized information seems to be the key element for patients’ sense of safety and involvement in decision making and care.
Introduction
A care pathway is a method for managing care for a defined group of patients during a given period that specifies goals and key aspects of care based on available guidelines and evidence. Such pathways coordinate the roles and activities of health care teams to optimize the efficient use of healthcare resources. 1 Notably, the terms care pathway, clinical pathway and critical pathway are often used interchangeably in the literature.
Care pathways are implemented to improve continuity and quality of healthcare, patient outcomes and satisfaction, and efficient use of resources. 2 There is literature supporting the benefit of care pathways for reducing in-hospital complications, 3 developing outlines for the anticipated course of treatment, integrating evidence-based practice and guidelines, implementing structured clinical documentation, developing multidisciplinary documentation and facilitating day-to-day patient management. 4
Effectiveness of clinical care pathway is ensured by a process of continuous evaluation and follow-up of quality indicators. The predominant indicator for assessing the quality of care is patient satisfaction which can identify areas for improvement within the care process. 5 Increasingly there is a trend to involve patients in this process and use patient surveys to formally evaluate and measure patient satisfaction. 6
Satisfaction is a subjective, self-rated indicator. It has classically been, defined as an evaluation of the degree to which expectations are fulfilled. 7 A number of studies have highlighted that satisfaction greatly increases as care aligns with standardized clinical procedures.8,9 Others have demonstrated significant increases patient satisfaction for those experiencing a structured care pathway.10–13 Further, some investigators have noted the positive impact that satisfaction can have on therapeutic adherence.14,15 Moreover, another important aspect of patient satisfaction includes patient involvement, when desired, in the decision-making process and care.
A 2007 systematic review of 9 different patient-centred care models/frameworks identified 6 key attributes of patient-centred care: involvement, education, collaboration, sensitivity to nonmedical and spiritual dimensions of care, respect for patient needs and preferences, free flow and accessibility of information. 16 There is substantial literature supporting the benefits of patient participation in coordinating their own care. 17 Indeed, patient self-care and self-responsibility are integral components of care continuity. 18 A meta-summary of studies examining patient experiences with care revealed that many patients both desire and expect to be involved in their care. More specifically this includes communicating, monitoring, and self-management and patients want their role and ideas to be acknowledged. 19 Despite the available evidence that patient involvement is an important contributor to a successful care project,20 relatively limited attention has been given to developing guidelines that take the central aspect of patient-centred care into account. 16
Although care pathways are becoming more widespread, their impact on patient satisfaction remains largely unknown. Most studies have used existing tools to measure quality of care or health-related quality of life before and after care pathway implementation. 4 In contrast, relatively few have used patient satisfaction with care pathway experience. Research has also focused on changes in the process of care delivery and to a lesser degree on outcomes rather than on the patient experience.
Up until now, visceral surgery services have included patient needs and expectations implicitly in the development of a care pathway. The literature supports the notion that patient needs and expectations should be included in the development of the care pathway and the care pathway should have patient approval. 21 and that patient satisfaction is an essential element in assessing hospital-based care. 14
We aimed to evaluate patient perception and satisfaction with of involvement, information and safety related to a new care pathway.
Methods
Setting and context
The University Hospital of Lausanne (CHUV) is an academic, tertiary referral center in French-speaking Switzerland. Since 2006, the visceral surgery unit has implemented care pathways for 30 frequently conducted surgeries. Each care pathway was developed by hospital staff and relevant stakeholders to support continuity of care and guide treatment planning/care and provide evidence-based patient education promoting self-care. The care pathway document describes patient management before and during the hospital admission, medications/prescriptions and daily care practices validated by the healthcare team. It is intended to help the patient to visualize their entire support structure and to anticipate increasingly becoming involved in their daily care activities.
Sample
Adult patients 18 years and older admitted for one of nine elective surgeries supported by a care pathway. The nine surgical procedures included: inguinal hernia, abdominal hernia, laparoscopic cholecystectomy, sentinel lymph node dissection, total/partial thyroidectomy, gastric bypass, appendectomy, portal vein embolization and for certain types of lymph node resection (e.g. axillary or ilio-obturator lymphadenectomy). Consecutively patients who have hospitalized between June 2012 and September 2013 received the questionnaire. Patients with questionable literacy, or who could not read and understand French or who were discharged from the unit on the same day of surgery were excluded from the survey.
Instrument
The 27-item questionnaire was designed by the author (LC) and derived from the institution (CHUV) global survey patient satisfaction questionnaire. The overarching goal was to explore three dimensions of patient satisfaction: information, safety and involvement in care before/during/at hospital discharge. A 4-point Likert scale from “strongly agree” to “strongly disagree” was used to assess answer. The information must be given by the health care team to the patient to ensure guidance, involvement and anticipation of health care needs during hospital stay. Patient satisfaction relating to information assessed whether the information provided by the care team was specific, care-centred and adapted to individual patient health literacy. Perceptions related to safety evaluated perceptions regarding the adequacy of working conditions, environment to provide quality care and that nursing staff had the necessary knowledge to deliver safe care. Patient involvement is consequence of complete information given by health care team and their willingness. A content validity was conducted with two clinician nurses and the head of the department of surgery (ND). Comprehension testing was performed to examine patient understanding of the questionnaire items was conducted with 10 patients and no changes were made to the instrument and the final questionnaire was approved by the chairman of Visceral Surgery. Ethical considerations for the project and questionnaire were reviewed and approved by the Nursing Direction of the University Hospital of Lausanne (CHUV), Lausanne, Switzerland.
The Table 2 assesses three discrete periods of the care pathway (pre-hospitalization, hospitalization and discharge). In total, nine questions (1, 4, 5, 7, 8, 20, 21, 23, 24) refer to the dimension of information, 14 questions (2, 6, 9, 10, 11, 12, 14, 15, 17, 18, 19, 22, 26, 27) concern patient safety including pain management, and four questions (3, 13, 16, 25) indicate the degree of patient involvement (see supplemental materials).
Procedures
This cross sectional health survey was carried out in the visceral surgery service of the University Hospital of Lausanne (CHUV). The questionnaire was distributed to patients by a study investigator 1–2 days prior to discharge. Oral and written explanation about the study were provided and instructions were given on how to complete the questionnaire (4-item Likert scale). Patient participation was voluntary and questionnaires were collected by a study investigator prior to discharge to maximize the return rate.
Data analyses
The results for each question are the sum of two responses of 4-point Likert scale (i.e. “strongly agree” and “somewhat agree”). For example, if 84% of patients strongly agree and 15% somewhat agree, the overall rate is 99% (84 + 15%) patient satisfaction.
Responses were analyzed and are reported using descriptive statistical techniques. Non-parametric statistics were used in cases of skewed distributions. The relationship between different score of the questionnaire was assessed using Spearman rank correlation (R2). For the association of the questionnaire score with personal and clinical characteristics, explorative univariate analysis was performed using Pearson correlations, Phi correlation and ANOVA. Data analysis was performed with Stata version 13.1. 22 A P-value < 0.05 was used as the significance level.
Results
A total of 280 patients completed the questionnaire. Patients ranged in age from 18–90 (mean age 55.5), 54% of whom were female. The most frequently used care pathways were cholecystectomy, gastric by-pass, treatment of inguinal hernia and thyroidectomy (Table 1).
Satisfaction with information
Overall patient satisfaction on the 9 questions concerning information ranged from 80–99%. Patients were satisfied with the information given by the medical staff (277/280, 99%) and by the nursing staff (266/280, 95%) in preoperative consultations. In total, about 80% of patients (224/280) reported being informed during the preoperative consultation by a team member (physician or nurse) regarding the anticipated length of hospitalization. During the hospitalization, 96% of patients (274/280) were satisfied with the amount and quality of information given by the nurse and 95% for the preparation of the operation. For the overall hospitalization concerning the discharge planning, 87% of patients (244/280) received the information early enough from the physician to anticipate their discharge and the information given by the nursing staff was clear enough for the 89% (250/280). In a final summary, 97% (272/280) of patients were satisfied with the information given by the physicians and at 96% (269/280) with the information given by the nurses.
Satisfaction with safety
Patient satisfaction with safety ranged from 82–98% across the 14 questions addressing safety. In preoperative consultations, 98% (274/280) of patients were satisfied that their concerns were taken into account by the physician. At admission, 97% (272/280) of patients felt welcomed by the nursing staff and 89% (250/280) of patients said the nurses appreciated their concerns concerning health and treatment. Most of patients’ needs and expectations were taking into account by physicians in 97% (272/280) and for the nurses in 96% (269/280). Ninety-eight percent (274/280) of patients said they received quality care from nurses. Patient satisfaction with moral support provided by the health care team was 82% (230/280), while 97% (272/280) of patients reported feeling in safe hands during their hospitalization. Finally, 92% (258/280) of patients felt safe to leave the hospital. In a final summary, 98% (274/280) said they felt secure during hospitalization and 94% (263/280) would come back if necessary.
Concerning pain, 59% (165/280) of patients experienced pain after surgery. Women expressed more pain than men during the hospitalization (65 vs. 52% respectively, p = 0.002). The healthcare team, physicians (255/280, 91%) and nurses (260/280, 93%) did everything possible to relieve the pain. Of note, 91% (255/280) of patients how expressed pain received less information than the 94% (263/280) patients without pain (p = 0.1943). As a consequence, patient 90% (252/280) with pain felt less safe than patients who were not in pain (93%, 260/280) (p = 0.2231). The involvement of patients feeling pain (76%, 213/280), in decisions and care, is higher than the 74% (207/280) without pain, but not significant (p = 0,55). In a final summary, 88% (246/280) patients were satisfied with the care received when reporting pain and 90% (252/280) were satisfied with the pain management.
Satisfaction with involvement
For the 4 questions examining patient involvement, satisfaction ratings were 82–89%. A total of 82% patients (230/280) felt involved in pain management and in care decisions 89% (250/280). Notably, a minority of patients (106/280, 38%) would have preferred to be more involved in decisions regarding their operation.
The patient satisfaction did not differ across the periods of care (preoperative consultation, hospitalization and discharge) and ranged from 85–89% (p = 0.16). For the preoperative consultation period, 85% of patients (238/280) were satisfied, hospitalisation 89% (250/280), and in the preparation for discharge 88% (246/280). The overall satisfaction rate was 91% (255/280).
The patient satisfaction per dimensions (information, safety, involvement) was 92% (258/280) for the information, 91% (255/280) for the safety and 75% (210/280) for involvement in decision-making and care.
When dimensions and periods are mixed, patients were satisfied with the information in the preoperative consultation in 94% (263/280), the hospitalisation in 93% (260/280), for discharge in 87% (244/280) and for the assessment of stay in 95% (266/280). For the safety, patients were satisfied in preoperative consultation in 94% (263/280), in the hospitalisation in 91% (255/280), for the discharge in 89% (250/280) and for the assessment of stay in 93% (260/280). For their involvement, patients were satisfied in the preoperative consultation in 58% (162/280), in the hospitalisation in 80% (224/280) and for the assessment of stay in 83% (232/280). The discharge was not measured. To measure discharge, other survey should be done at distance of hospitalization.
Interestingly, ratings of satisfaction with safety were positively correlated with the scores on the information dimension (rs = 0.65, p < 0.01). Correlation between involvement dimension and information dimension (rs = 0.37, p < 0.01), and safety dimension (rs = 0.36, p < 0.01), are lower.
Discussion
Herein we report the evaluation of patient satisfaction with care pathways for visceral surgery at a tertiary academic medical center. Overall, patient satisfaction with care received during hospitalization was high. These findings are in line with prior reports such as Webster et al. 21 who identified 94% patient (263/280) satisfaction in a clinical pathway for laparoscopic pyeloplasty and by Soria-Aledo et al. 23 who evaluated a laparoscopic cholecystectomy clinical pathway with high patient satisfaction (97%, 272/280).
Importantly, a focal point needing attention is the information given by the surgeon during the preoperative consultation concerning expected length of stay and information given by the nurses in preparation for hospital discharge. The aim is the increase fluidity of the organisation in the unit during the patient admission and discharge, as it which is congested chronically. Focused and personalized education is probably the key. “Every patient’s capacity to understand instructions must be assessed and appropriate time allocated to teaching to ensure preparedness for a comfortable discharge”. 25
Visceral surgery patients feel safe during the different periods of hospitalization and their discharge home. Discharge must be improved. However, they expected more moral support from the nurse and better listening related to difficulties they experienced. During hospitalization, more than 40% of patients declared to have no pain. The other patients expressed that their pain was supported adequately by the medical team nurse. Women expressed more pain than men. Psychological factors may in part explain this observation. Perception of pain is reported differently by women and men. Further, physical differences (i.e. ovulation or menstruation) could potentially contribute to this 24 and some have noted that women report more pain, compared to men, across a variety of conditions and diseases. 25
After examining satisfaction, patient involvement appears to be a target for improvement. But, only four questions were created. It is short to understand completely the dimension. Patients’ involvement in their health care should be a goal in itself. Patients are full partners in their care and should be allowed to question the decision or action of care.
Strengths and limitations
It is recommended that satisfaction questions should be context and objective-specific rather than generic. 26 Therefore, the questionnaire was developed by the first author (LC), and evaluated by a multidisciplinary team for concordance and consensus. The phrasing of questions was validated by the head of the institutional hospital quality surveys. Thus, the limitation of the present study is that the questionnaire has not been validated yet by other investigations. However, a vast majority of quality control questionnaire are not formally validated prior to their initial use.
Satisfaction is significantly influenced by clinical outcomes such as pain relief and avoiding of complications. However, it is also significantly influenced by the care pathway and the overall hospital experience. The relative proportions to which these factors contribute towards overall satisfaction are likely to differ by condition or treatment depending on multiple factors. For all studies like this, the optimal time point for assessing satisfaction has yet to be defined. This study was performed in a single surgical service and therefore the results cannot be generalized. Although the hospital has a university status, types of surgery chosen in this study were relatively straightforward, common surgical procedures. Thus, data collection form regional hospitals could help contribute to the generalizability of the findings. Though probably reflective of other interventions, the actual generalizability of these findings to other surgical procedures is not known.
Clinical recommendations
Although the majority of patients are satisfied with the care, we identified two areas for improvement. First, information about the length of stay and the organisation of the discharge should be more specific. A simple intervention could include providing a handbook containing information and organisation of the admission, preoperative consultation, hospitalisation and discharge supplemented by dedicated time with a nurse to individualize the information and assess comprehension and literacy issues. Second, patients have unmet needs concerning moral and emotional support. Sensitizing the nursing staff to the expectations of visceral surgery patients and emphasizing the importance of listening to patient concerns, providing psychological comfort, and using presence to engage in moral support and diminish feelings of isolation.
Research recommendations
The results of this survey may serve as an initial basis to assess the improvement of patient satisfaction for new surgical care pathways. Before-after analysis will be important and may provide insight into the impact of planned interventions. Periodically re-surveying visceral surgery patients can be part of a continuous quality improvement program enabling more patient-centred approaches to care and better meeting the needs of visceral surgery patients.
A longitudinal study would be informative for examining the predictive validity of the questionnaire. Further, evaluating adverse events occurring within 15 days post-discharge would provide insight regarding possible links with levels of satisfaction. In this way, one might be able to identify at-risk patients and plan and implement corrective actions before hospital discharge.
Conclusion
Descriptive scores by item (n = 280).
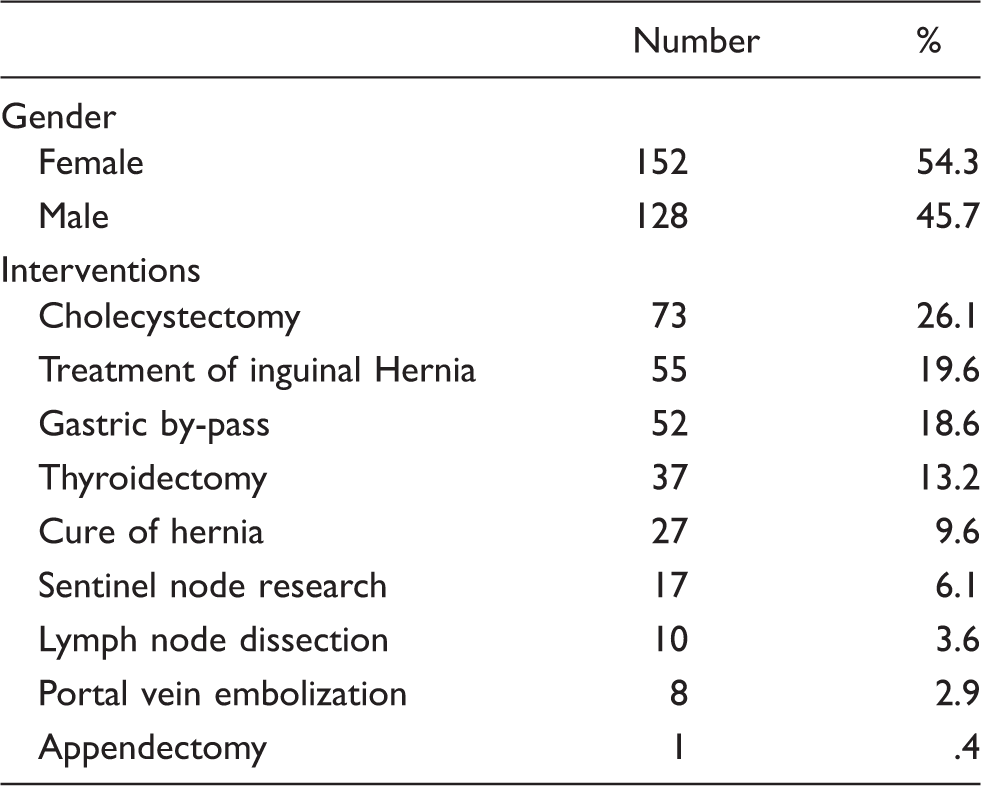
Demographic and clinical characteristics (n = 280).

Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.