
Abstract
Background
Multiple sclerosis (MS) prevalence has increased across Europe, yet contemporary population-based data from southern Europe remain scarce.
Objectives
In this retrospective population-based cohort study conducted in a healthcare area of the Basque Country (Barrualde-Galdakao Integrated Healthcare Organisation [BGIHO]), northern Spain, we estimated prevalence, incidence, and clinical characteristics of MS. Prevalence was estimated on 31 December 2023 using the 2017 McDonald criteria, and incidence was assessed from 1 January 2009 to 31 December 2023 using both symptom-onset and diagnosis-based definitions.
Results
Prevalence was 131.8 per 100,000 inhabitants (95% CI 119.6–145.2); age-adjusted prevalence (European Standard Population [ESP2013]) was 125.4 (95% CI 113.3–138.1). Mean annual incidence (2009–2023) was 4.4 per 100,000 person-years (95% CI 3.9–5.1) by symptom onset and 5.3 (95% CI 4.7–6.0) by diagnosis date. Relapsing–remitting MS (RRMS) accounted for 67.1% of cases; secondary progressive MS (SPMS) for 18.6%; and primary progressive MS (PPMS) for 14.2%. Median EDSS was 2 (IQR 0–5).
Conclusions
MS prevalence in this healthcare area is high. The findings reflect an aging MS population with evolving clinical characteristics. The use of complementary incidence definitions provides insight into disease occurrence and healthcare detection. Continued epidemiological monitoring is warranted.
Introduction
MS is a leading cause of neurological disability in young adults in Europe and North America. 1 In recent decades, prevalence and incidence have increased in many regions, likely reflecting improved magnetic resonance imaging (MRI) access, earlier diagnosis, therapeutic advances, and environmental changes. Increasing mean age and female-to-male ratios have also been reported. 2
In Spain, MS prevalence exceeds 100 per 100,000 in the most recent studies. The highest rates have been reported in northern regions such as Galicia and Asturias (110–198/100,000; 2015–2022; 42°–43°N),3–7 whereas lower figures have been described in southern areas, including Murcia, Alicante, and Lanzarote (50–112/100,000; 2014–2018; 29°–38°N).8–10 Incidence also varies between 2.5 and 8 per 100,000 person-years depending on geography and case definition. 7 These variations underscore the need for updated studies.
Despite a well-developed public healthcare system, contemporary population-based MS data from this part of the Basque Country remain limited. The only previous study, conducted in 1999 in western Bizkaia, excluding Bilbao municipality (adjacent to the present study area), reported a crude prevalence of 47.7 per 100,000 and an incidence of 2.76 per 100,000 person-years.11,12 The absence of updated data over 25 years limits the assessment of current disease burden and healthcare needs.
This study aimed to describe the contemporary epidemiology of MS in the BGIHO, and to compare the results with historical regional and recent Spanish data. Comparisons with previous studies considered differences in diagnostic criteria, study periods, and case ascertainment methods.
Methods
Study design and setting
We conducted a retrospective, population-based cohort study in the BGIHO from 1 January 2009 to 31 December 2023. The study population was dynamic and included patients with MS residing in the catchment area for ≥6 months. Prevalence was estimated on 31 December 2023, and incidence was assessed from 1 January 2009 to 31 December 2023. The study followed STROBE reporting guidelines.
BGIHO is one of several integrated healthcare organisations in the Basque Country, northern Spain (Figs. 1–2), covering 1577 km2 and serving 309,566 inhabitants (50.8% female; 1 January 2024, Eustat – Basque Statistics Office). The Basque public health system (Osakidetza) provides near-universal coverage in the area; potential non-public cases were explored through regional patient associations.

Geographical location of the study area. The Basque Country is highlighted in red within Spain (beige) and Europe (grey). Created by Enrique San-Martín using mapchart.net. CC BY-SA 4.0. Used with permission.

Study area within the Basque Country. The Barrualde-Galdakao Integrated Healthcare Organisation (BGIHO) catchment area is shown in slate blue, covering municipalities in the provinces of both Bizkaia and Araba/Álava. Provincial and regional boundaries are indicated. Map created by the authors using QGIS.
Case definitions
Prevalent cases were defined as patients alive, residing in the catchment area on 31 December 2023, and diagnosed with MS according to the 2017 McDonald criteria. 13 Crude prevalence was calculated per 100,000 inhabitants; age-adjusted prevalence used direct standardisation to the 2013 European Standard Population. An exploratory recalculation of crude prevalence was performed applying the 2024 revision of the McDonald criteria. This included review of the identified MS cohort as well as patients previously classified as radiologically isolated syndrome (RIS) and clinically isolated syndrome (CIS) using the same data sources as for primary case ascertainment (Osakidetza administrative database and the specialised MS clinic registry). Patients fulfilling the 2024 but not the 2017 criteria were reclassified as MS cases. This approach did not involve systematic population screening and may underestimate the impact of the revised criteria 14 at the population level.
Incident cases (2009–2023) were defined using two reference dates: symptom onset and diagnosis (McDonald 2005, 2010, or 2017). Onset-based incidence reflects disease occurrence, whereas diagnosis-based incidence reflects healthcare detection. For onset-based incidence, patients whose first clinical symptom occurred between 1 January 2009 and 31 December 2023 were included, even if diagnostic confirmation was established subsequently (up to 31 December 2024); these cases were included in incidence analyses but excluded from prevalence estimates. Annual incidence rates were calculated by dividing the number of new cases in each calendar year by the corresponding population at risk, using official population counts recorded on 1 January of the following year. Thus, the 2011 incidence rate, for example, was calculated using the population count dated 1 January 2012. Cases were assigned to each year according to either date of symptom onset or date of diagnosis.
Data sources
Cases were identified through multiple complementary sources. An initial list of potential cases was obtained from the Osakidetza administrative database (ICD-10 code G35), including all individuals with a recorded diagnosis of multiple sclerosis who had resided in the study area. Everyone was identified using a unique personal identification code (CIC; corporate identification code), which uniquely identifies each patient within the Osakidetza healthcare system, allowing data-source linkage.
This initial list was reviewed to exclude miscoded cases, alternative diagnoses, individuals not meeting residency criteria, and deceased patients. It was cross-checked with the specialised demyelinating diseases clinic registry (MS clinic database), enabling identification of additional confirmed cases and removal of duplicates.
Additional validation included consultation with regional MS patient associations to identify potential cases managed outside the public system, and verification with hospital pharmacy records of disease-modifying therapies to ensure complete case capture.
All potential cases underwent validation through review of electronic medical records. Cases identified in a single source required clinical confirmation. Only confirmed cases fulfilling diagnostic and residency requirements were included in the final cohort.
Variables
Demographic variables included age, sex, and country of birth. Clinical variables included dates of symptom onset and diagnosis, clinical phenotype (2013 Lublin classification 15 ), EDSS score at last follow-up, disease-modifying therapy exposure, diagnostic delay, relapse history, MRI activity, and cerebrospinal fluid oligoclonal bands when available. Disability was categorised as mild (EDSS 0–3), moderate (3.5–5.5), or severe (≥6). Age was analysed both as a continuous variable and categorised into predefined 10-year age groups, and additionally as <50 versus ≥50 years. Clinical data were available for most patients. Analyses used available-case data, with denominators specified where appropriate.
Statistical analysis
Analyses were performed using R (version 4.5) and Excel 365. Continuous variables were summarised as mean (SD) or median (IQR); categorical variables as frequencies and percentages. Ninety-five percent confidence intervals (95% CIs) for prevalence estimates were calculated using the Clopper–Pearson method for small samples (counts < 5), or the Wilson method for larger samples (counts ≥ 5), whereas Poisson distribution methods were used to estimate CIs for incidence rates. Temporal trends in incidence were analysed using Poisson regression models with the logarithm of the population as an offset variable. Incidence rate ratios (IRRs) with 95% confidence intervals were estimated, and model assumptions were assessed. Time to EDSS ≥4 was analysed using Kaplan–Meier curves and log-rank testing. Statistical significance was set at p < 0.05. Correlations between continuous variables (e.g., year of symptom onset and age at onset or diagnostic delay) were assessed using Pearson's correlation coefficient (r), given its robustness to moderate deviations from normality in large samples. Analyses were conducted using available-case data; no imputation was performed.
Results
Prevalence and incidence
Among 474 MS cases identified during the study period, 408 fulfilled the 2017 McDonald criteria and were alive and residing in the BGIHO on 31 December 2023 (267 women, 141 men; female-to-male ratio 1.9). Exclusions were due to death (n = 47) or relocation outside the catchment area (n = 19). Main epidemiological indicators are summarised in Table 1.
Summary of prevalence (31 December 2023) and incidence (2009–2023) of multiple sclerosis in Barrualde-Galdakao Integrated Healthcare Organisation catchment area.
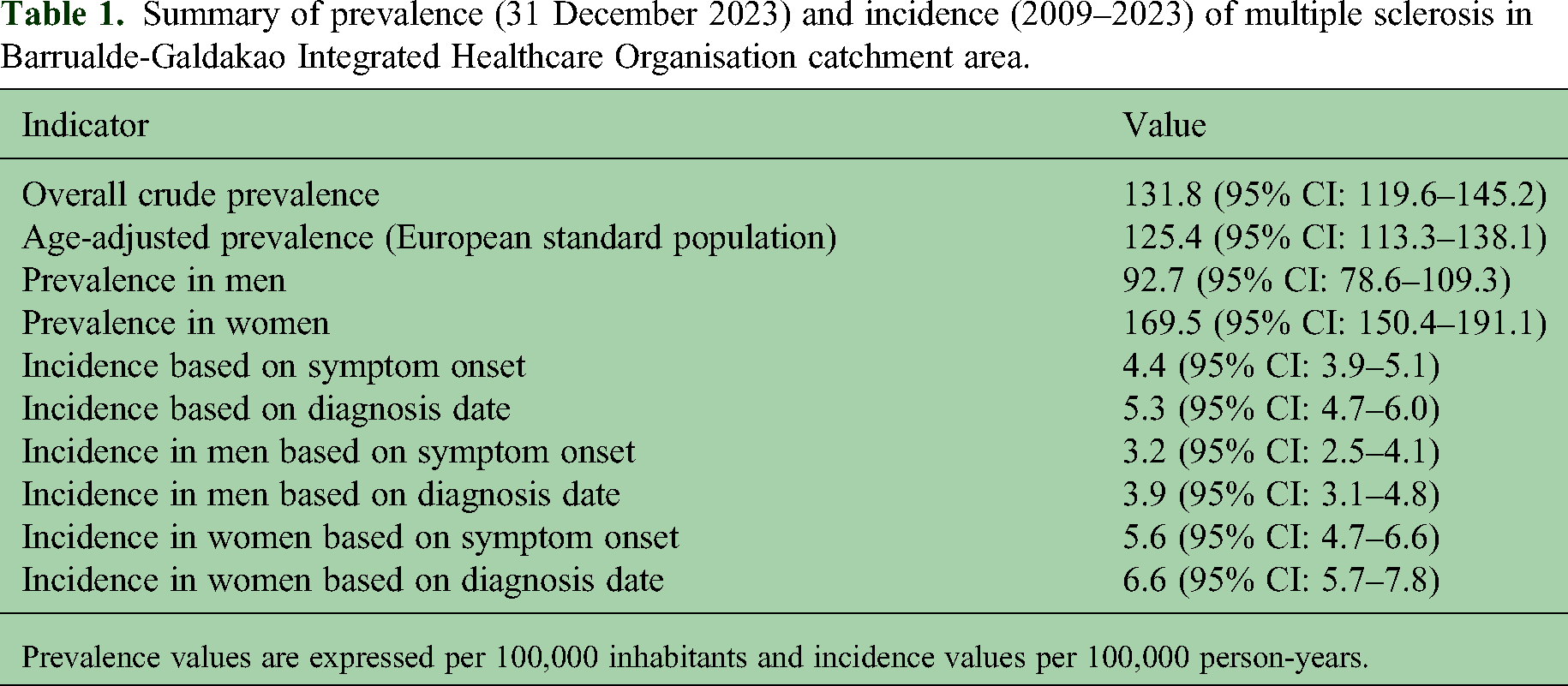
Prevalence values are expressed per 100,000 inhabitants and incidence values per 100,000 person-years.
Crude prevalence was 131.8 per 100,000, and age-adjusted prevalence (ESP2013) was 125.4. Prevalence was higher in women and in individuals aged ≥50 years (145.5 vs. 119.5 per 100,000; p = 0.047 for age comparison).
Age-specific prevalence increased with age, peaking in middle-aged groups (Table 2).
Age-specific prevalence of multiple sclerosis (31 December 2023).

Prevalence rates are expressed per 100,000 inhabitants. Confidence intervals (95% CI) were calculated using the Clopper–Pearson method for groups with fewer than 5 cases and the Wilson method for groups with 5 or more cases.
Patients born outside Spain represented 4.9% of the cohort, versus 11% in the regional population. Among native-born residents, crude prevalence was 140.9 per 100,000.
Application of the 2024 McDonald criteria identified 12 additional cases (11 radiologically isolated syndrome and one fulfilling dissemination in space through optic nerve involvement), increasing the number of prevalent cases from 408 to 420. Crude prevalence rose from 131.8 to 135.7 per 100,000.
Between 2009 and 2023, 205 incident cases were identified by symptom onset and 245 by diagnosis date. Mean annual incidence was 4.4 per 100,000 person-years by onset and 5.3 by diagnosis (Table 1).
Using onset date, Poisson regression showed a slight downward trend over 2009–2023 (IRR 0.9631; 95% CI 0.9328–0.9943; p = 0.021). This pattern was confined to 2021–2023; excluding these years, incidence remained stable (IRR 0.9911; 95% CI 0.9500–1.0339; p = 0.6775). No significant temporal trend was observed using diagnosis date (IRR 0.9801; 95% CI 0.9520–1.0090; p = 0.1751).
Diagnosis-based incidence was 19.5% higher than onset-based estimates, although not statistically significant (incidence rate ratio 1.20; 95% CI 0.99–1.44; p = 0.06). Among 40 patients with symptom onset before 2009 but diagnosis during the study period, 18 had PPMS.
During 2009–2023, 47 patients died and 19 relocated. The cumulative proportion of deaths in the cohort was 9.91% (95% CI 7.29–13.19).
Clinical characteristics
Clinical and demographic characteristics are summarised in Table 3.
Clinical and demographic characteristics of the multiple sclerosis cohort.
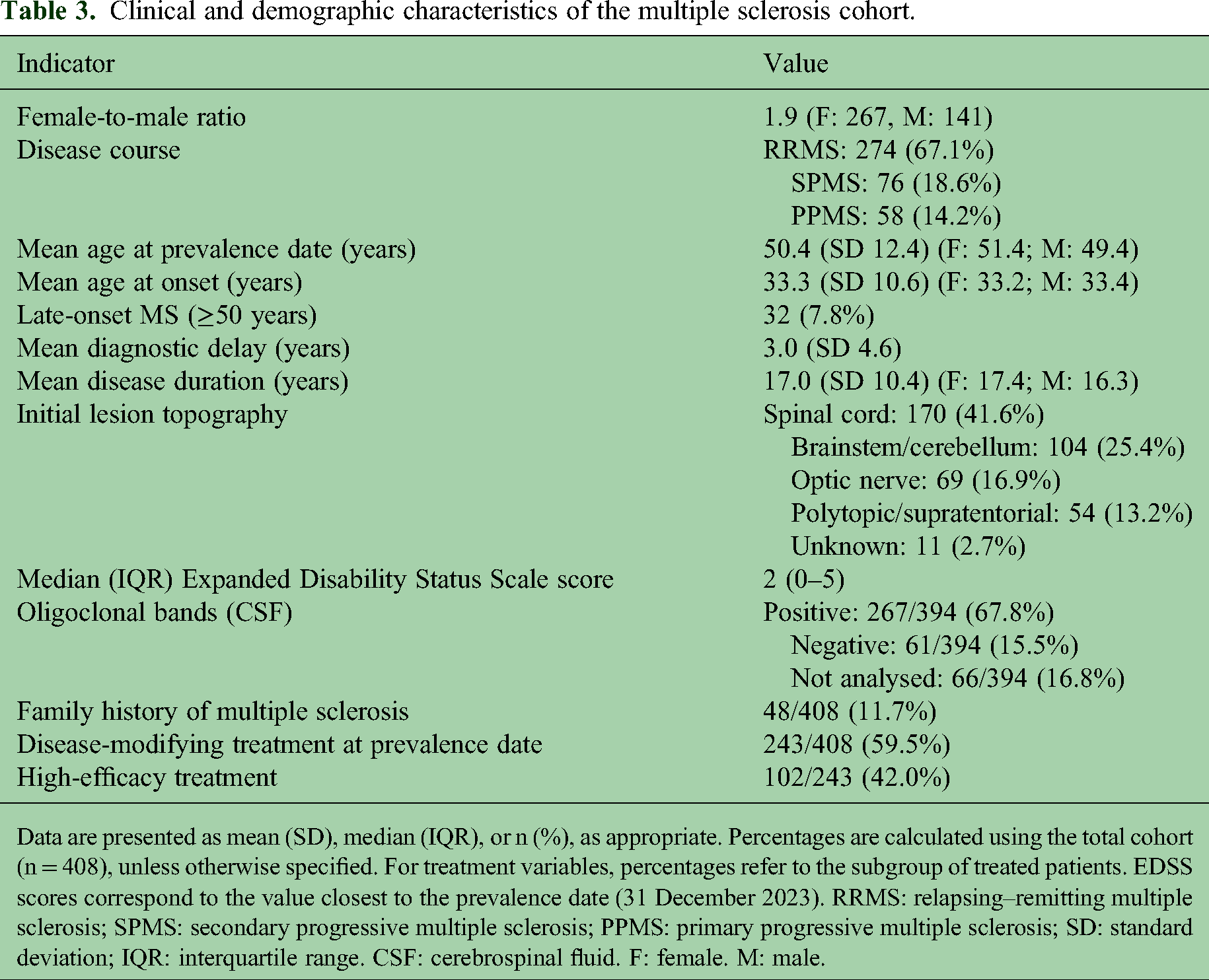
Data are presented as mean (SD), median (IQR), or n (%), as appropriate. Percentages are calculated using the total cohort (n = 408), unless otherwise specified. For treatment variables, percentages refer to the subgroup of treated patients. EDSS scores correspond to the value closest to the prevalence date (31 December 2023). RRMS: relapsing–remitting multiple sclerosis; SPMS: secondary progressive multiple sclerosis; PPMS: primary progressive multiple sclerosis; SD: standard deviation; IQR: interquartile range. CSF: cerebrospinal fluid. F: female. M: male.
The most frequent disease course was RRMS (67.1%), followed by SPMS (18.6%) and PPMS (14.2%).
Mean age at prevalence was 50.4 years, with no significant sex differences. Just over half of the patients were aged ≥50 years.
Mean age at symptom onset was 33.3 years and was significantly higher in PPMS (44.1 years) than in RRMS (32.4 years) (p < 0.001). Late-onset MS (≥50 years) accounted for 32 cases, half of whom had PPMS. Age at onset showed a modest but significant increase over time (r = 0.302; p < 0.001).
Mean diagnostic delay was 3 years; 208 (51%) were diagnosed within one year and 76 (18.6%) after ≥5 years. Diagnostic delay was longer in PPMS (mean 4.9) than RRMS (mean 2.5; p < 0.001) and decreased over time (r = −0.325; p < 0.001). Mean diagnostic delay declined from 2.4 years in 2009 to 0.5 years in 2023.
Mean disease duration at prevalence was 17.0 years, longest in SPMS (25.9 years; p < 0.05). Among SPMS patients, the mean time to secondary progression was 14.2 years and was significantly shorter in men than women (11.7 vs. 16.5; p = 0.0067).
Spinal cord involvement was the most frequent site of initial presentation (41.6%), particularly in PPMS (79.3%).
Disability was lower in women (mean 2.43 vs. 3.21; p = 0.0033, median 1.5 vs. 3). Disability was mild (0–3) in 264 (64.7%), moderate in 55 (13.5%), and severe (≥6) in 89 (21.8%). EDSS was higher in progressive phenotypes (median 6 in SPMS and PPMS vs. 1 in RRMS) and increased with age (median EDSS 0 in patients <40 years, 2 in those aged 40–59 years, and 5 in those ≥60 years).
Kaplan–Meier analysis estimated a median time to EDSS ≥4 of 22.8 years overall; women reached this milestone later than men (27.5 vs. 17.7 years; log-rank p = 0.0004).
Among patients with available cerebrospinal fluid studies, oligoclonal bands were positive in 81.4% of those analysed.
Treatment rates differed by phenotype (RRMS 68.6%, SPMS 52.6%, PPMS 25.9%), and treated patients were younger than untreated patients (mean age 46 vs 58 years).
In 2023, 23 relapses were recorded (annualised relapse rate 0.056; 95% CI 0.036–0.084), with higher relapse activity in RRMS (0.077) and in patients aged <50 years (0.082).
Among 328 patients with EDSS recorded in both 2022 and 2023, disability remained stable in 71.0%, improved in 4.3%, and worsened in 24.7%. Of the 81 patients with worsening, only 5 (6.2%) had experienced a relapse in the preceding six months. MRI activity was present in 39/236 patients (16.5%). NEDA-3 status could be assessed in 218 patients; 132 (60.6%) met NEDA-3 criteria in 2023. Disability progression was the principal driver of NEDA-3 loss.
Discussion
This population-based study provides updated epidemiological data on MS in a defined healthcare area of the Basque Country, 25 years after the reference study conducted in Bizkaia in 1999.11,12 The two areas are geographically adjacent and demographically comparable. Key epidemiological indicators from both studies are summarised in Table 4. The earlier study used Poser criteria and defined incidence according to symptom onset, an approach replicated in the present study to improve comparability.
Comparison of epidemiological indicators: Bizkaia 1999 vs BGIHO 2023.
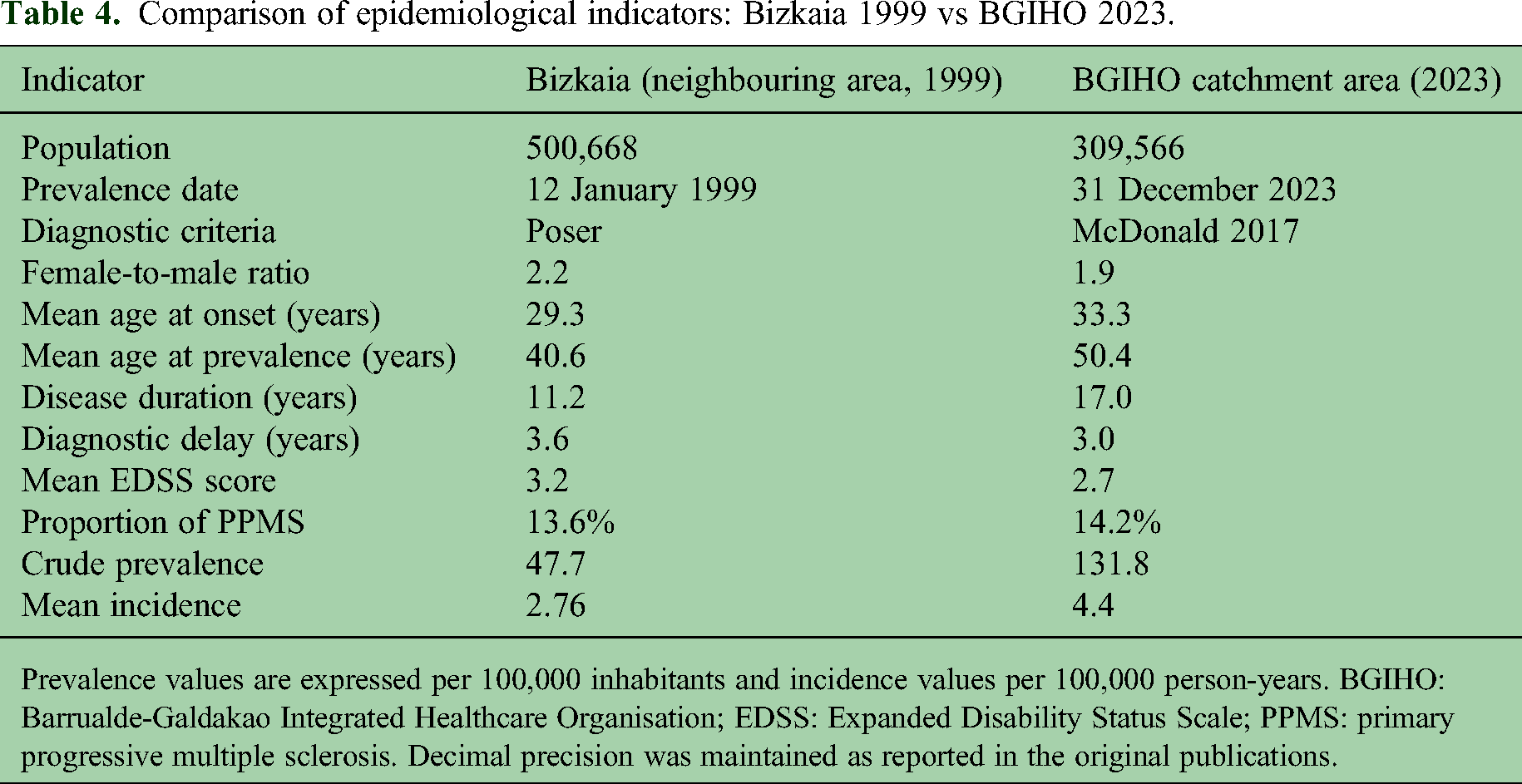
Prevalence values are expressed per 100,000 inhabitants and incidence values per 100,000 person-years. BGIHO: Barrualde-Galdakao Integrated Healthcare Organisation; EDSS: Expanded Disability Status Scale; PPMS: primary progressive multiple sclerosis. Decimal precision was maintained as reported in the original publications.
Compared with the 1999 cohort, the current population is older, with later disease onset, longer disease duration, lower disability, and shorter diagnostic delay. In contrast, the proportion of PPMS and the female-to-male ratio remained broadly similar over time.
Crude prevalence increased markedly compared with the 1999 study (2.76-fold). This change is likely multifactorial and may reflect improved case ascertainment, earlier diagnosis related to wider MRI availability and more sensitive McDonald criteria, longer survival, and potentially increased disease occurrence. Mean incidence based on symptom onset also increased over time, although methodological differences between studies should be considered when interpreting these findings.11,12 Diagnosis-based incidence was approximately 20% higher than onset-based estimates, likely reflecting the temporal lag between symptom onset and diagnostic confirmation. Onset-based incidence may more closely approximate biological disease emergence, whereas diagnosis-based incidence better reflects healthcare system detection.
The modest increase after applying the 2024 McDonald criteria suggests relatively comprehensive ascertainment under the 2017 criteria. However, this estimate was based on registry and clinical data rather than systematic population screening and may underestimate the full impact of the revised criteria.
Incidence remained broadly stable between 2009 and 2020. The lower incidence observed during 2021–2023 coincided temporally with the post-COVID period and was no longer significant after excluding these years. Similar temporal patterns have been reported in Denmark 16 although causality cannot be inferred. Healthcare disruption during the post-COVID period may have delayed neurological assessment and MRI access. However, whether these findings reflect delayed diagnosis, temporary healthcare-related effects, or sustained incidence changes remains uncertain and requires continued epidemiological surveillance.
Crude prevalence in our study is among the highest reported in Spain (Table 5). Recent studies from Asturias, Ourense, and Santiago (42°–43°N) have shown similarly high rates,4–6 whereas lower figures were reported in Lanzarote (29°N), Murcia (37°N), and Alicante (38°N).8–10 Although comparisons between studies should be interpreted cautiously because of methodological differences, these findings may support the persistence of a latitudinal gradient in Spain, despite evidence that the classical north–south gradient may be attenuating in parts of the Northern Hemisphere. 17
Comparison of clinical characteristics in epidemiological studies of multiple sclerosis in Spain (2015–2023).
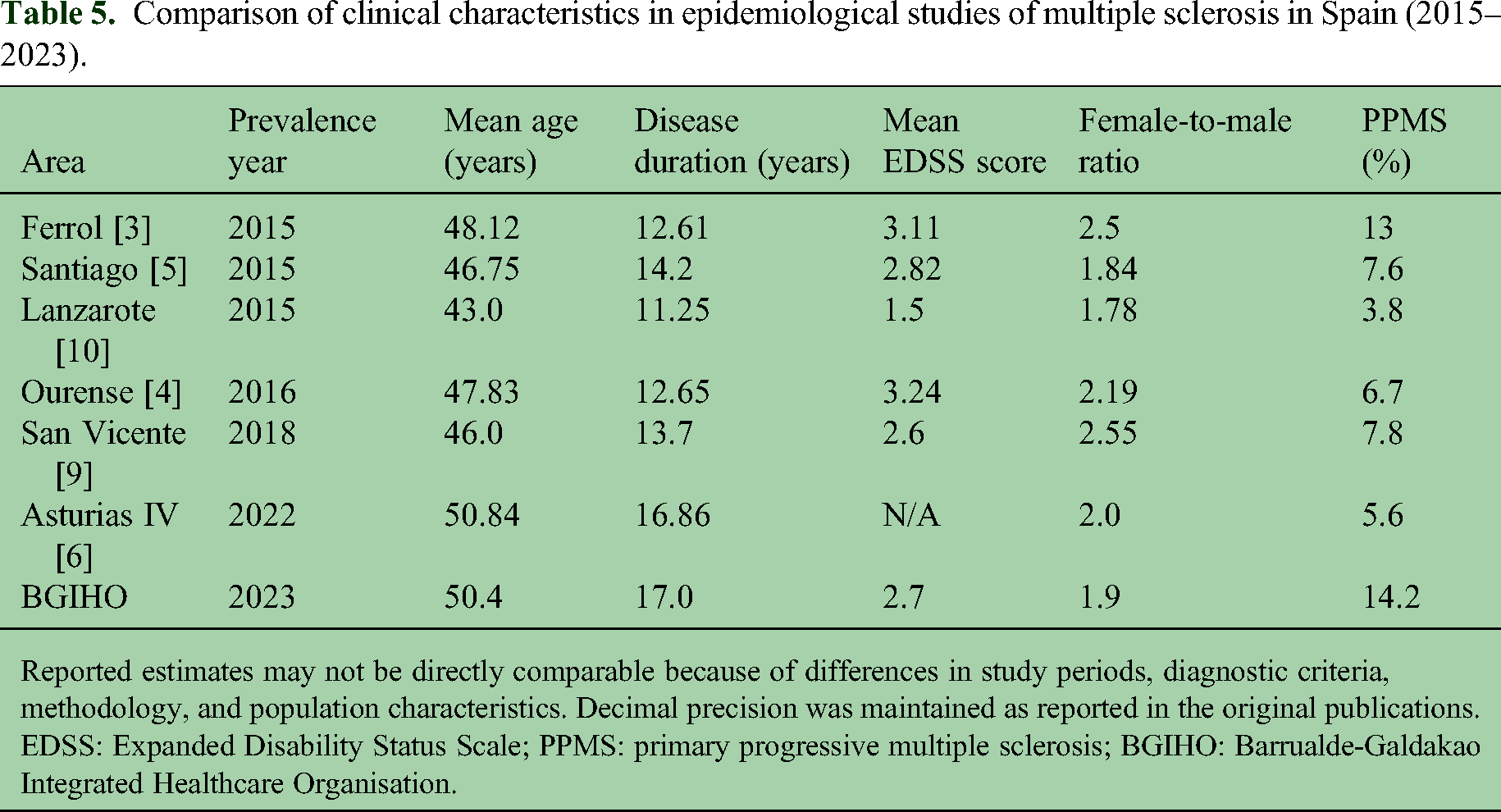
Reported estimates may not be directly comparable because of differences in study periods, diagnostic criteria, methodology, and population characteristics. Decimal precision was maintained as reported in the original publications. EDSS: Expanded Disability Status Scale; PPMS: primary progressive multiple sclerosis; BGIHO: Barrualde-Galdakao Integrated Healthcare Organisation.
PPMS accounted for a relatively high proportion of cases compared with most recent Spanish epidemiological series (Table 5) and was similar to both the 1999 Bizkaia study11,12 and classical natural history estimates (∼15%). 18 This stability over 25 years contrasts with the declining frequency of PPMS reported in some contemporary epidemiological studies. 19
In Asturias, PPMS represented a substantially lower proportion of cases despite similar latitude and broadly comparable demographic characteristics. 6 The reasons for these regional differences remain uncertain and may reflect methodological, environmental, or population-related factors.
The Basque population has distinctive genetic characteristics within Europe, including higher frequencies of blood group O and Rh negativity. A study conducted in the Basque Country found that O-negative blood may be protective against MS (odds ratio 0.49; 95% CI: 0.31–0.80), whereas Rh positivity in groups A or B may increase risk.20,21 However, the potential contribution of genetic background remains speculative and was beyond the scope of the present study.
Inflammatory activity in 2023 was low, and approximately 60% of evaluable patients met NEDA-3 criteria. Most patients were receiving DMTs, with a substantial proportion treated with high-efficacy agents. Although treatment rates appeared lower than in some recent Spanish cohorts,4,9 this may partly reflect the older age of the population and the relatively high proportion of progressive phenotypes in the present cohort.
Despite low inflammatory activity, disability progression was common, and the vast majority of disability worsening occurred without recent relapses. Although retrospective classification precludes definitive PIRA designation, this pattern is consistent with disability progression largely independent of relapse activity, particularly in an aging cohort with long disease duration.
Men showed greater disability accumulation, reached EDSS milestones earlier, and converted to SPMS sooner than women. These findings are consistent with classical natural history studies18,22 and support the relevance of sex differences in disability progression. However, these results should be interpreted cautiously, as this epidemiological analysis was not adjusted for potential confounding factors such as disease duration, treatment exposure, or baseline disability.
Compared with the 1999 cohort, the current population was older and had longer disease duration despite lower overall disability levels. This pattern may reflect improved long-term outcomes associated with earlier diagnosis, reduced diagnostic delay, broader access to DMTs, and advances in multidisciplinary care. Similar trends towards milder disease expression have been reported in other contemporary cohorts. 23
However, aging introduces important challenges including comorbidity burden, infection risk under immunosuppression, and complex care needs. These findings highlight the challenges posed to healthcare systems, and clinical trial design must adapt to an aging MS population.
Strengths of this study include the population-based design, comprehensive case ascertainment from multiple complementary sources, a 15-year study period, detailed clinical characterisation with EDSS available for all prevalent cases, dual incidence definitions, and the ability to perform a 25-year regional comparison.
Limitations include the retrospective design, potential imprecision in symptom onset dating, inherent survival bias in prevalent cohort designs, the dynamic cohort structure affecting cumulative measures, and differences in diagnostic criteria and methodology limiting direct comparability with historical or regional cohorts. Although multiple ascertainment sources were cross-validated to maximise case capture, the exact quantitative overlap between individual data sources was not formally quantified. The post-COVID decline in onset-based incidence is based on only three years of observation and should therefore be interpreted cautiously. In addition, the mean diagnostic delay observed in the cohort may contribute to underestimation of recent onset-based incidence, requiring longer follow-up to determine whether this trend persists over time. The exploratory application of the 2024 McDonald criteria was based on registry data without systematic population screening, which may underestimate its full impact. In addition, relatively small numerical changes in case ascertainment may influence epidemiological estimates in studies based on moderately sized populations.
MS prevalence in this healthcare area of the Basque Country is high and substantially exceeds historical regional estimates. The findings reflect an aging MS population with evolving clinical characteristics and provide updated population-based epidemiological data in a well-defined healthcare setting. The use of both symptom-onset and diagnosis-based incidence definitions offers complementary insights into disease occurrence and detection.
Supplemental Material
sj-docx-1-mso-10.1177_20552173261458067 - Supplemental material for Epidemiology of multiple sclerosis in a healthcare area of the Basque Country, Northern Spain: A population-based study (2009–2023)
Supplemental material, sj-docx-1-mso-10.1177_20552173261458067 for Epidemiology of multiple sclerosis in a healthcare area of the Basque Country, Northern Spain: A population-based study (2009–2023) by José Luis Sánchez-Menoyo, Sabas Boyero-Durán, Cristina Llarena-González, Natalia Roncero-Colina, Mar Mendibe-Bilbao, Silvia Vázquez-Picón, Urko Agirre-Larrakoetxea, Itxaso Azkune-Calle, Enrique Valdeolivas-Urbelz and Alfredo Rodríguez-Antigüedad in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgements
The authors thank the patient associations ADEMBI and AEMAR for their support. We acknowledge Karmele Zubizarreta and Karmele Garro for their collaboration, and Enrique San Martín for designing the geographical map. The authors received professional language editing assistance from Ideas Need Communicating Language Services. The company had no role in the study design, data analysis, interpretation of results, or manuscript content. The authors take full responsibility for the work.
Author contributions
JLSM conceived the study, collected and curated the data, performed the main analyses, and wrote the manuscript.
ARA contributed to data collection and provided critical revisions to the manuscript.
UAL participated in the statistical analysis and supported the methodological design as a member of the Research Unit.
SBD, CLG, NRC, SVP, IAC, and EVU contributed to patient identification and clinical data collection and reviewed the manuscript, providing relevant suggestions.
All authors read and approved the final version of the manuscript.
Consent to participate
Written informed consent was obtained from patients residing in the BGIHO area and receiving care at Galdakao-Usansolo University Hospital (HGU). A partial waiver of written informed consent was granted for patients residing outside the BGIHO area or receiving care in other hospital centres.
Conflict of interest statement
José Luis Sánchez-Menoyo received travel expenses from Novartis, Merck, and Biogen, and speaker fees from Biogen, Novartis, Sanofi, Merck, and has participated in clinical trials funded by Merck and Roche outside the work described in the manuscript submitted.
Alfredo Rodríguez-Antigüedad has participated in scientific consultancy or as a speaker in scientific meetings organised by Merck, Biogen, Novartis, Roche, Sanofi, Teva, and Bristol-Myers Squibb.
Sabas Boyero-Durán received research grants, travel expenses and/or speaker fees from Biogen, Bristol Myers Squibb, Merck, Novartis, Roche, Sanofi-Genzyme, and Neuraxpharm.
Cristina Llarena-González has participated in scientific meetings, scientific consultancy, and clinical trials organised by Almirall, Biogen, Bristol-Myers Squibb, Merck, Novartis, Neuraxpharm, Roche, Sanofi, and Teva.
Natalia Roncero-Colina, Silvia Vázquez-Picón, Mar Mendibe-Bilbao, Urko Agirre-Larrakoetxea, and Itxaso Azkune-Calle have no conflicts of interest to declare.
Enrique Valdeolivas-Urbelz received speaker fees from Novartis.
Data availability statement
The datasets generated and analysed during the current study are not publicly available due to ethical and legal restrictions related to patient confidentiality and data protection regulations. The data are stored within the secure electronic health record system of the BGIHO and are not transferable outside the institutional framework. De-identified data may be made available from the corresponding author upon reasonable request and subject to approval by the BGIHO Research Ethics Committee, in accordance with applicable data protection legislation.
Ethical considerations
The study protocol was approved by the BGIHO Research Ethics Committee (reference number 03/22) and conducted in accordance with the Declaration of Helsinki. Patient confidentiality was ensured, and all data were anonymised and stored in secure, password-protected databases accessible only to authorised study personnel.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: 2021 and 2023 internal calls for “Contracts for the Intensification of Research Activity” from Biobizkaia Health Research Institute. 2023 call for “Grants for Research Projects in Multiple Sclerosis” from the Basque Foundation for Health Innovation and Research (BIOEF)-EITB maratoia. Project file number BIO23/EM/004. The funders had no role in the design, data collection, data analysis, or reporting of this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.