
Abstract
Background
Accurate tracking of skeletal muscle mass (SMM) and fat mass percent (FM%) is central to evaluating obesity treatment. The InBody H20N bioelectrical impedance analysis (BIA) device could offer a scalable, lower-cost alternative. However, its accuracy compared to dual-energy X-ray absorptiometry (DXA) and research-grade BIA in adults with obesity is unknown.
Methods
Baseline SMM and FM% was measured in 55 participants with obesity (62.6±7.6 y, 67.3% female, BMI: 37.6±5.7 kg/m2) enrolled in a behavioral weight-loss program using three modalities: the InBody H20N, InBody S10, and DXA. Agreement was assessed using intraclass correlation coefficients (ICC) analyses with two-way mixed-effects and absolute-agreement, Bland-Altman plots with limits of agreement, and Lin’s concordance correlation coefficients.
Results
For SMM, agreement was good between H20N and DXA (ICC 0.78; 95% CI -0.15-0.94) and excellent between H20N and S10 (ICC 0.93; 95% CI 0.87–0.96). For FM%, agreement was excellent between H20N and DXA (ICC 0.93; 95% CI 0.79–0.97) and good between H20N and S10 (ICC 0.81; 95% CI 0.66–0.89). All ICCs were statistically significant (p<0.001).
Conclusion
Results indicate that the H20N provides clinically useful estimates of body composition relative to DXA and research-grade BIA, supporting its potential in resource-constrained environments.
Introduction
Accurate assessment of body composition is essential for evaluating cardiometabolic risk and monitoring treatment progress in individuals with obesity.1-3 Obesity is widely recognized as a major driver of chronic diseases including cardiovascular disease and type 2 diabetes1,4 and it also contributes to reduced mobility, diminished quality of life, and increased risk of premature mortality.4,5 It is shaped by an interacting set of biological, environmental, and socioeconomic factors, and its impact is often magnified in resource-constrained settings where access to longitudinal care and structured weight management support may be limited. In many communities, logistical and financial barriers (e.g., transportation, time off work, and limited availability of specialty services) reduce opportunities for regular in-clinic monitoring. These constraints underscore the value of approaches that enable reliable monitoring in the home and other non-clinical settings, supporting continuity of care when clinic-based resources are difficult to access.6,7
One promising approach to address this gap is the use of accessible body composition assessment tools, such as bioelectrical impedance analysis (BIA) devices. These devices are portable, cost-effective, and easy to use, making them well-suited for either home-based or resource-constrained settings where advanced imaging technologies like dual-energy X-ray absorptiometry (DXA) or magnetic resonance imaging are not applicable. By providing accurate estimates of body fat and muscle mass, BIA devices can support personalized interventions by clinicians or help individuals monitor their own progress, ultimately improving obesity management in underserved communities. 1
DXA is widely regarded as a reference method for measuring fat mass (FM) and fat-free mass (FFM) due to its high precision and ability to differentiate between bone, fat, and lean tissue. 8 However, several practical limitations restrict its uptake in routine clinical practice and limit its access in rural communities including high equipment costs (∼ $70,000), the need for trained personnel, and the requirement for a dedicated space to house the scanner. DXA is further constrained in individuals with obesity due to reduced accuracy when the entire body cannot be positioned within the scanner field. These constraints make DXA impractical for many outpatient clinics, field-based research studies, or at-home monitoring.
In contrast, BIA offers a more accessible and user-friendly alternative for body composition assessment. Many BIA devices are portable, relatively inexpensive, and easy to operate, making them suitable for use in a variety of settings. BIA estimates body composition by measuring the resistance and reactance of electrical currents as they pass through the body. 9 These measurements are then used in proprietary algorithms to predict FM, lean mass (including skeletal muscle mass (SMM)), and other body composition parameters. BIA was previously considered less precise than DXA due to its reliance on single-frequency methods. 10 However, technological advancements, including the adoption of multifrequency approaches, have significantly improved its accuracy and reliability, especially when standardized protocols are followed. 11 Research-grade BIA systems more often incorporate segmental, multifrequency measurements, which employ low and high frequencies and can improve estimation of fluid compartments compared with single-frequency approaches. 12 Even so, accuracy and agreement can degrade when measurements are taken under uncontrolled conditions (e.g., variable hydration, recent meals, or exercise), reinforcing the need to evaluate device performance across the continuum from tightly controlled to pragmatic protocols. 12
Among available BIA devices, the InBody S10 and InBody H20N (InBody, Cerritos, CA, USA) have gained popularity due to their user-friendly design and detailed output. The S10 is designed for clinical and research environments and supports measurements in supine, standing, or seated positions. Although it has demonstrated excellent agreement with DXA when used in the supine position, 13 its high cost (∼$15,000) limits its practicality in many clinical and community-based settings. In contrast, the H20N is a consumer-grade device intended for home or community use. It is battery operated, lightweight, relatively inexpensive (∼$350), and requires minimal training which altogether makes it a more feasible option for use in the home and resource-limited settings. Importantly, while both devices use an 8-point electrode system and segmental measurement, they differ systematically in measurement features that may influence performance, particularly the frequency set and number of impedance measurements collected. The S10 uses a wider range of measurement frequencies (six frequencies), whereas the H20N uses two frequencies, which may influence how each device estimates fluid compartments and thereby lean/muscle outputs. 14 These design differences help distinguish a “research-grade” platform optimized for clinical detail and flexible testing positions from a consumer platform optimized for usability, portability, and cost. This research aimed to evaluate the agreement between DXA and the InBody S10 to the InBody H20N for fat mass percentage (FM%) and SMM in adults with obesity to evaluate whether the H20N could serve as a practical and accessible alternative to the S10 and DXA, including for use outside of clinical settings.
Methods
Participant Characteristics at Baseline
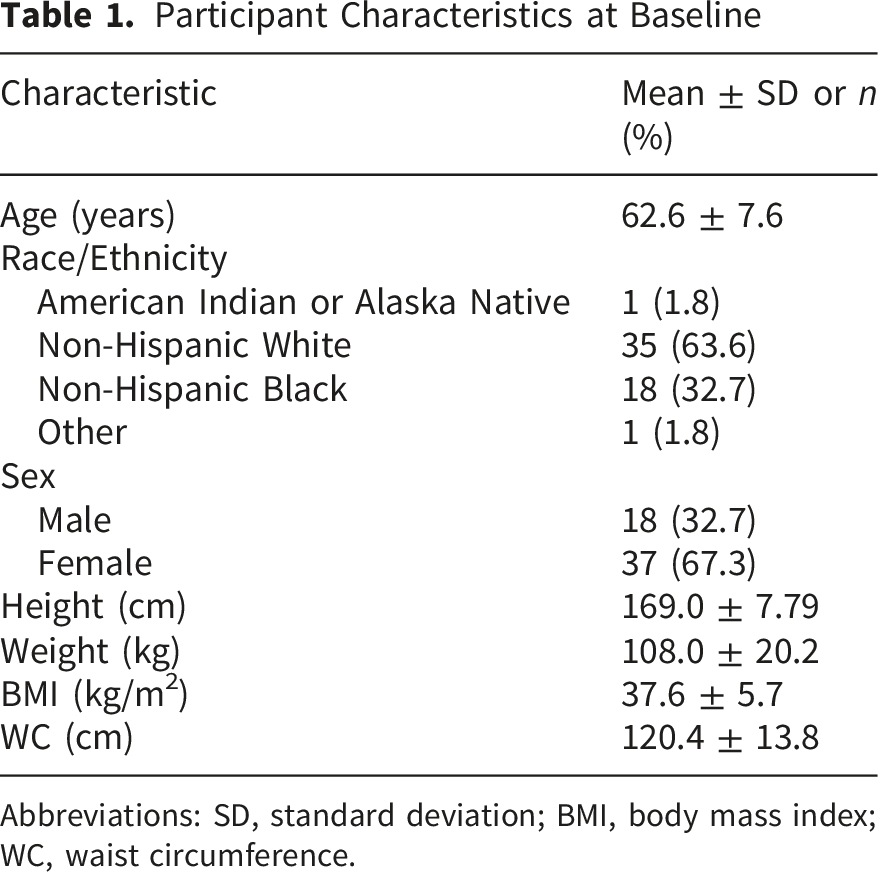
Abbreviations: SD, standard deviation; BMI, body mass index; WC, waist circumference.
Body composition was first measured using the InBody H20N (Figure 1) InBody H20N body composition analyzer. Image courtesy of InBody Co., Ltd.
SMM refers specifically to muscle tissue attached to the skeleton, whereas lean mass, as measured by DXA, includes SMM, connective and soft tissues, and body water. 17 Both the InBody H20N and S10 devices provide estimates of SMM which are estimates by a proprietary algorithm. DXA however, does not estimate SMM and instead provides appendicular lean mass (ALM), so we applied a validated prediction equation to estimate SMM from ALM (SMM = 1.12 × ALM - 0.63). 18 This approach ensured consistent estimates for comparison of SMM across devices.
To provide a comprehensive assessment of whether these devices can be used interchangeably, agreement was evaluated using complementary metrics that address distinct aspects of measurement performance. Bland–Altman analyses quantified mean bias and the limits of agreement (LoA), depicting the distribution of individual-level differences between methods (Figure 2).
19
Agreement was evaluated using intraclass correlation coefficients (ICCs) with a two-way mixed effects model and absolute agreement.
20
Agreement was interpreted as poor (<0.5), moderate (0.5–0.75), good (0.76–0.90), or excellent (>0.90). Cronbach’s alpha was calculated for internal consistency (i.e., reliability) of the device’s measurements. Higher values (typically ≥0.80) indicate strong consistency, and lower values suggest greater variability in results.20,21 Lin’s concordance correlation coefficient (Lin’s CCC) was also performed to assess the degree to which pairs of observations fall on the 45° line of agreement, thus evaluating both precision and accuracy.
22
Concordance was classified as very good (0.81 -1), good (0.61 -0.80), moderate (0.41 -0.60), fair (0.21- 0.40), and poor (<0.2).23,24 Bland–Altman plots comparing the agreement between dual-energy X-ray absorptiometry, the InBody H20N, and the InBody S10 for fat mass percent (A-C) and skeletal muscle mass (D-F). Dashed lines indicate the mean difference (bias) and the 95% limits of agreement (mean difference ± 1.96 SD). For each plot, the difference between methods is shown against the mean of the two methods.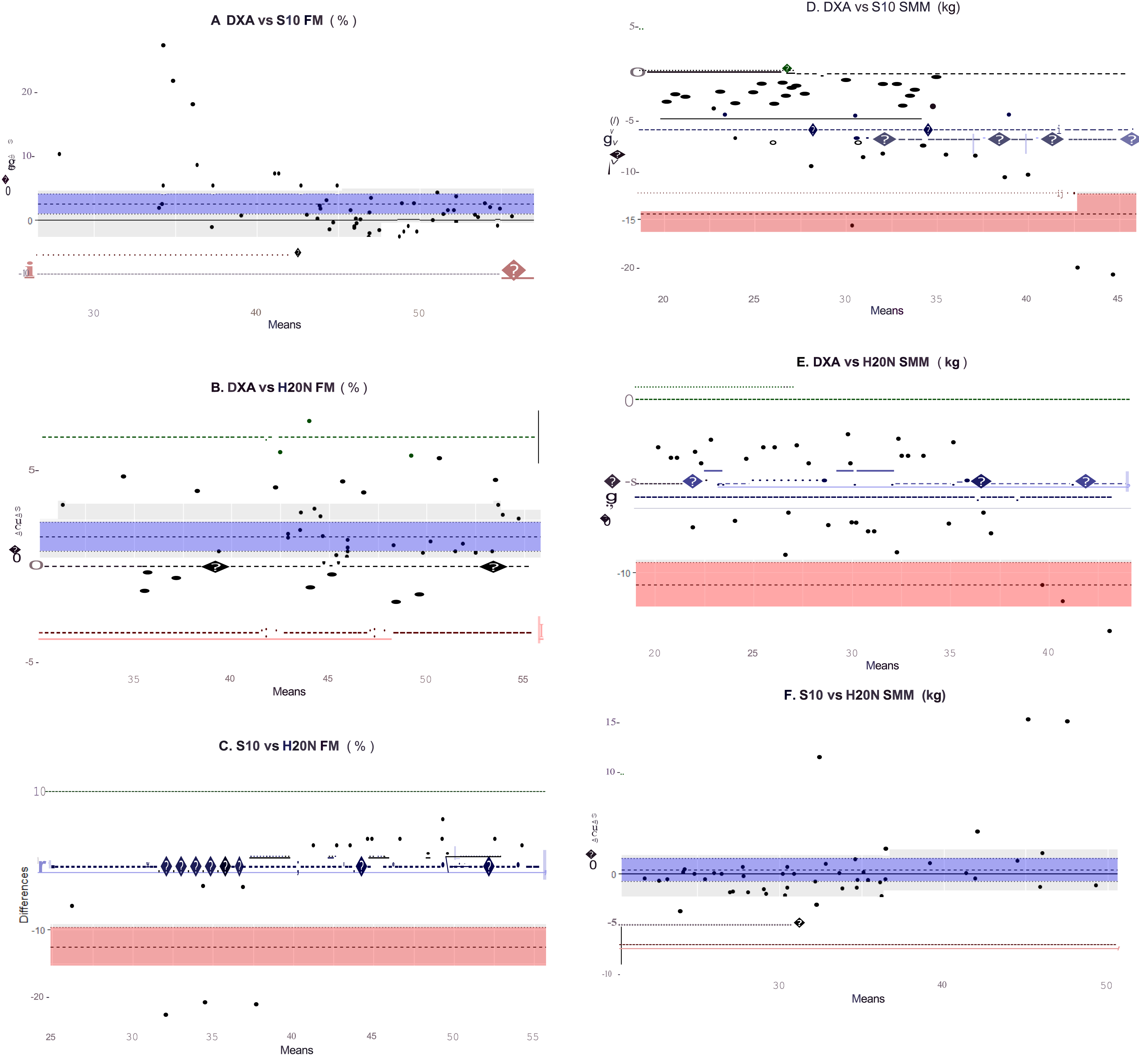
Results
Results of Intraclass Correlation Coefficient and Reliability Analyses
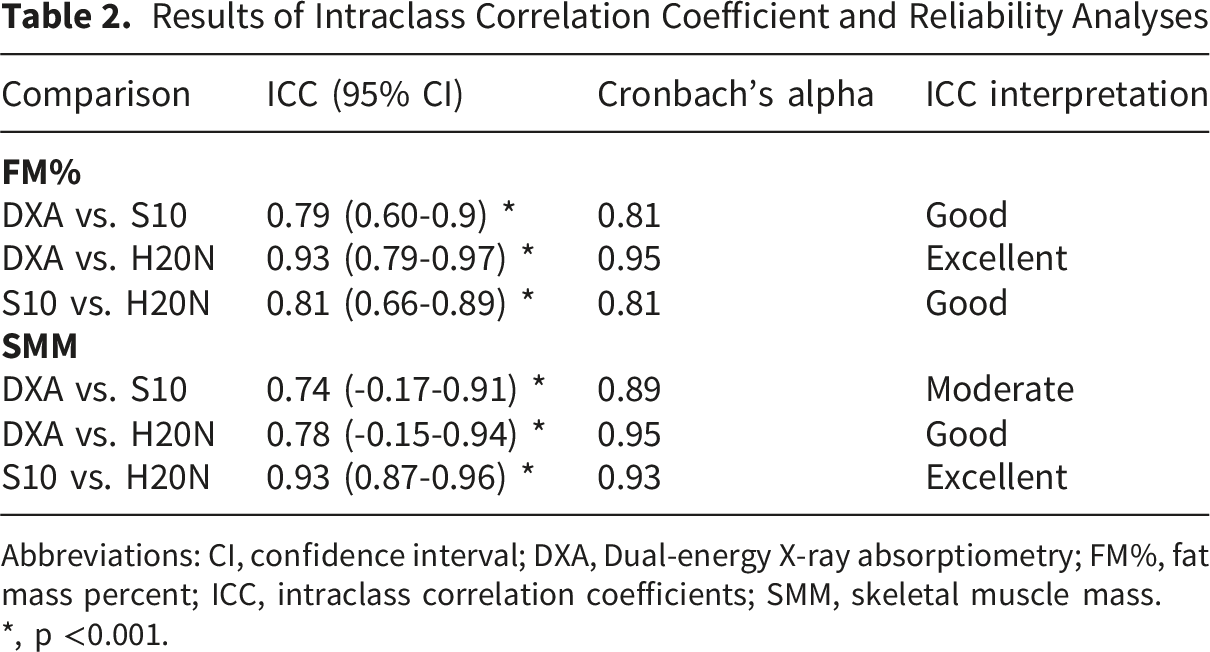
Abbreviations: CI, confidence interval; DXA, Dual-energy X-ray absorptiometry; FM%, fat mass percent; ICC, intraclass correlation coefficients; SMM, skeletal muscle mass.
*, p <0.001.
Lin’s Concordance Correlation Coefficient of FM% and SMM Between DXA, the InBody S10 and the InBody H20N
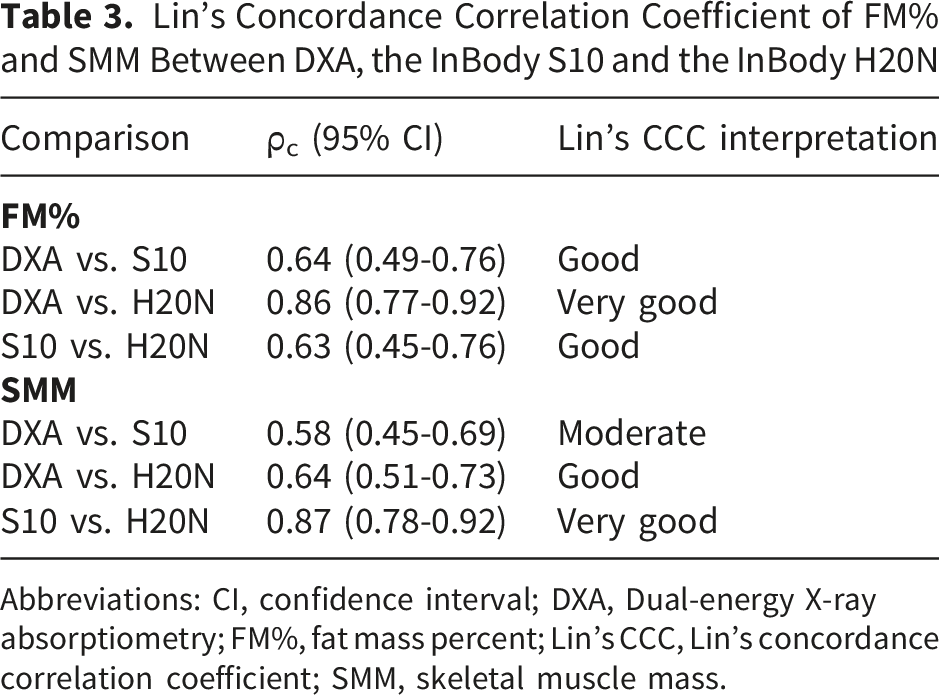
Abbreviations: CI, confidence interval; DXA, Dual-energy X-ray absorptiometry; FM%, fat mass percent; Lin’s CCC, Lin’s concordance correlation coefficient; SMM, skeletal muscle mass.
Cronbach’s alpha values ranged from 0.81 to 0.95 for FM%, indicating strong internal consistency across devices, particularly for H20N compared with DXA. For SMM, alpha was also high across comparisons (ranging 0.89-0.95) supporting good-to-excellent reliability. These findings reinforce that both BIA devices provide reproducible estimates, with the H20N showing the highest reliability for both FM% and SMM.
Lin’s CCC indicated varying levels of agreement across devices. For FM%, concordance was highest between DXA and the H20N (ρc = 0.86), reflecting very good concordance, while DXA and the S10 (ρc = 0.64) and the S10 and H20N (ρc = 0.63) showed good concordance. For SMM, concordance between the two BIA devices was very good (ρc = 0.87) whereas concordance between DXA and the H20N was good (ρc = 0.64) and moderate between DXA and the S10 (ρc = 0.58). These findings align with ICC results and reinforce that the H20N performs well for FM%, while SMM estimates remain less concordant with DXA and better between BIA devices.
Mean Differences, Standard Deviations, and Limits of Agreement (kg)

Abbreviations: DXA, Dual-energy X-ray absorptiometry; FM%, fat mass percent; LoA, limits of agreement; SD, standard deviation; SMM, skeletal muscle mass.
Discussion
Across devices, agreement was generally stronger for FM% than for SMM. For FM%, agreement ranged from good to excellent, with DXA vs H20N demonstrating the strongest performance and the highest concordance by Lin’s CCC. In contrast, SMM agreement was more variable where DXA-based comparisons were moderate-to-good whereas agreement between the two BIA devices was excellent. Lin’s CCC results generally aligned with ICC interpretations, showing strong concordance between the two BIA devices for SMM and the highest concordance between DXA and H20N for FM%. However, Lin’s CCC values for DXA comparisons indicated weaker concordance, particularly for SMM. This is expected because concordance correlation coefficients account for both correlation and systematic bias. Even a single outlier can dramatically reduce concordance whereas ICCs primarily reflect consistency across measurements. 25 Concordance correlation coefficients should be interpreted alongside other agreement and reliability measures (i.e., ICCs and Cronbach’s alpha) to provide a more complete assessment of interchangeability. 24 A critical finding in this research was the wide confidence intervals (CI) observed in the SMM comparison between DXA and the S10 (95% CI: -0.17 to 0.91) and between DXA and the H20N (95% CI: -0.15-0.94). This indicates low precision, meaning that while the average agreement is moderate to good, the potential for error in an individual measurement is large. Both CIs cross 0, suggesting the estimate is less precise in this sample (potentially due to sample size and/or high variability), and therefore warrant cautious interpretation.Several methodological features are likely to contribute to this. First, BIA is fundamentally grounded in estimating total body water (TBW) from impedance and then inferring FFM using hydration assumptions (e.g., FFM is 73% water), after which SMM is typically derived via proprietary, segmental algorithms. In people with obesity, there is a greater expansion of extracellular fluid (ECF) relative to intracellular fluid (ICF) which varies substantially among individuals at higher BMIs. 14 Variability in the ECF/ICF ratio can distort inferred TBW and propagate error into FFM and downstream SMM estimates. Second, each additional modeling step compounds error; in our workflow, converting DXA-derived ALM measures to SMM introduces another layer of approximation. These features help explain why SMM can show moderate-to-excellent consistency (ICC) yet still produce wide LoA and lower Lin’s CCC.
Prior research evaluating the accuracy of the InBody S10 compared with DXA has generally shown good agreement for FM–related measures, but more variable performance for lean and SMM estimates. Previous research in our lab has shown strong agreement between DXA and S10 FM and FFM when participants with obesity were assessed in the supine position. 13 We reported that posture influenced impedance pathways and measurement precision resulting in the underestimation of FM and overestimation of FFM. 13 Other studies demonstrate that while BIA tends to accurately estimate FM% relative to DXA, predictions of lean mass components are less consistent when compared to other BIA devices and DXA with agreement ranging from moderate to strong depending on population characteristics, hydration, and electrode configuration.26-29 No previous studies have compared the InBody H20N with either DXA or the S10. Furthermore, this is the first study to apply a validated equation to derive SMM from DXA-based ALM, enabling direct comparisons across devices that would otherwise produce non-comparable outputs.
The portability and affordability of the H20N make it an attractive option for rural and resource-limited settings where DXA is impractical. For example, prior research conducted in rural adults consistently shows that rural adults have higher BMI, higher prevalence of severe obesity, and greater cardiometabolic risk compared with their urban counterparts, driven in part by geographic isolation, limited healthcare infrastructure, and reduced access to preventive services. 30 Studies of rural obesity interventions have highlighted the challenge of monitoring body composition over time, resulting in many programs relying solely on body weight to monitor progress.31,32 However, there is evidence that changes in FM and lean mass better predict metabolic status than weight alone.33,34 Community-based obesity programs in low-resource settings, especially those delivered through cooperative extension systems, primary care clinics, or telehealth-supported behavioral interventions, have repeatedly emphasized the need for low-cost, scalable tools capable of tracking meaningful body composition changes without requiring specialized equipment or trained technicians.32,35 By providing accurate estimates of FM and SMM, the InBody H20N could fill a critical gap in these environments, enabling more precise monitoring during chronic disease management and community health initiatives. Determining longitudinal agreement is therefore a critical future direction for validating the H20N as a tool for monitoring body composition changes in real-world settings.
Future studies should also test whether a device- and population-specific calibration (e.g., an intercept/slope “correction factor”) can be developed for BIA-derived SMM to reduce the systematic offset we observed and bring H20N SMM estimates into closer alignment with reference-based values for cross-sectional use. Prior work has successfully adjusted BIA-derived appendicular muscle indices to better match DXA,26,36 and modeling refinements that incorporate body geometry have been proposed to address bias introduced by differing body proportions. 9 However, calibration is most effective at correcting a fixed mean bias and may not fully resolve individual-level variability (i.e., the spread/LoA), which often reflects day-to-day hydration shifts, posture/fluid shifts, electrode contact, and algorithmic estimation noise. Investigators should define acceptability thresholds a priori. In the absence of established minimally important differences for BIA-derived outcomes, the “acceptable” magnitude of disagreement will necessarily depend on the intended clinical or research application. It is also plausible that BIA accuracy could improve over the course of a weight-loss intervention. As body mass decreases, fluid distribution and TBW compartment ratios may become more stable, which could enhance the precision of SMM estimates. 13 Nonetheless, DXA may be commonly used as a reference method, but it is not error-free. Large -scale comparisons with magnetic resonance imaging (MRI) show DXA can overestimate lean mass and may miss longitudinal changes in lean tissue detected by MRI. 37 Accordingly, it is important to 1) further evaluate the H20N’s performance, including whether calibration or correction factors can meaningfully reduce systematic bias, and 2) during real-world use, explicitly define the minimum standardization needed to achieve measurements that are “good enough” for the intended purpose, recognizing that inter- and intra-individual variability is inherent to real-world settings. Future studies should also evaluate the H20N’s performance across different body sizes, racial and ethnic groups, and limited resource settings.
This study has several notable strengths. First, it directly compares a consumer-grade portable BIA device (H20N) and a research-grade BIA system (S10) with DXA, providing a comprehensive evaluation across multiple reference points. To our knowledge, this is the first study to assess the H20N against DXA or any clinical BIA device, highlighting its novelty and practical relevance. Second, the use of standardized measurement protocols and validated equations for estimating SMM from DXA-derived ALM strengthens the reliability of each comparison. Third, including adults with obesity enrolled in a structured behavioral weight-loss intervention represents a clinically meaningful group in whom accurate body composition assessment is particularly relevant and serves as preliminary evidence of the H20N’s clinical implementation. Several limitations should be considered. First, this was a convenience sample and was not designed or powered specifically to test agreement across body composition devices. Additionally, the study sample was drawn from a single weight-loss trial in Alabama, which may limit generalizability to broader or more diverse rural populations. Finally, the present research was conducted under moderately controlled conditions. Although hydration status and recent activity were standardized via pre-visit instructions, these factors could not be biochemically verified or otherwise rigorously controlled. Accordingly, these results should be interpreted alongside evidence that BIA can remain highly reliable yet show systematic bias when key real-world factors (hydration, meals, exercise, time of day) are not standardized 38
Conclusion
This study demonstrates that the InBody H20N, a portable and affordable BIA device, shows excellent agreement with DXA for FM% and good agreement for SMM comparable to a research-grade BIA system. These findings suggest that the H20N may serve as a practical alternative to DXA and clinical or research-grade devices in settings where cost, space, and accessibility are barriers. By enabling accurate assessment of fat and muscle, the H20N could support obesity management and chronic disease prevention in resource-limited environments.
Footnotes
Acknowledgements
The authors would like to thank the University of Alabama at Birmingham Nutrition Obesity Research Center, the research team involved in the parent study, and the participants and collaborative staff at the Wellness, Health, and Research Facility on the Lakeshore Foundation Campus for their collaboration.
Ethical Considerations
This research was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the University of Alabama at Birmingham under protocol code 30003818 on 4 April 2020.
Consent for Publication
Written informed consent to participate and for publication was obtained from all subjects involved in this research.
Author Contributions
RDS designed the original research; KME conducted research; RDS provided resources; KME performed data and statistical analyses; KME wrote original draft; WG, JW, CL, and RDS reviewed and edited the paper; RDS was primarily responsibility for the final content; KME and RDS administered the project. All authors have read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The parent study was funded by the National Institutes of Health, National Institute for Diabetes, and Digestive, and Kidney Diseases (K01DK124244) and the University of Alabama at Birmingham (UAB) Nutrition Obesity Research Center (P30DK056336).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Data Availability Statement
The original data presented in the study are openly available in PubMed Central.