
Abstract
Background:
Dissemination of evidence-based intensive health behavior and lifestyle treatments (IHBLTs) to families from low-income communities was the primary objective of the CDC Childhood Obesity Research Demonstration (CORD) 3.0 projects. The goal of RI CORD 3.0 was to adapt and test the effectiveness and context for remote implementation of an IHBLT, JOIN for ME.
Methods:
Children aged 6–12 years with body mass index (BMI) >85th percentile and a caregiver (N = 111) were recruited through a federally qualified health center (FQHC) or community setting and participated in an immediate or 4-month delay condition. Child and caregiver weight status, Family Nutrition and Physical Activity (FNPA), and child weight-related quality of life were assessed at baseline, 4 months, and at the end of the 10-month remotely delivered intervention. Program acceptability and intervention fidelity were assessed to inform subsequent implementation.
Results:
Analyses comparing active and delayed treatment groups at 4 months showed significant improvements in FNPA for the active treatment group compared with delayed group. Groups did not differ significantly on child or caregiver weight status. Ten-month treatment effects in the combined sample showed significant effects of time on child relative weight status, with children who initiated the program demonstrating decreases of 2.90% median BMI, 3.89%BMIp95, and 0.16 zBMI units. Session attendance and food security at baseline were related to greater changes in weight status.
Conclusions:
The adapted version of the JOIN for ME was successfully implemented and shown to be associated with significant, modest changes in child weight status.
Introduction
Childhood obesity is a significant public health concern associated with high rates of morbidity and mortality,1,2 including both physical and psychosocial health consequences.3–7 Children from low-income backgrounds are at particularly high risk 8 due to a multitude of environmental factors, 9 while also having less access to evidence-based interventions.10–12
Both the American Academy of Pediatrics (AAP) and the U.S. Preventive Services Task Force (USPSTF) have identified intensive health behavior and lifestyle treatment (IHBLT) as the recommended first-line intervention for youth with obesity.6,13 IHBLTs are multicomponent family-based interventions (>26 contact hours) that include attention to nutrition and physical activity combined with behavior change strategies and remain the treatment of choice for school-aged children for whom obesity medications are not typically approved by regulatory agencies or commonly prescribed. 14 While numerous studies document the effectiveness of IHBLTs for youth, 15 few of these explicitly focus on children from low-income backgrounds. 16 In research that has examined economic disparities, low income is a predictor of poorer outcomes.17,18
JOIN for ME is an evidence-based IHBLT for youth ages 6–12 years delivered in a group setting. JOIN for ME is consistent with AAP and USPSTF guidelines, and is supported by a strong body of evidence demonstrating clinically meaningful reductions in child weight status in open trials 19 and randomized controlled trials with school-age children and adolescents.20,21 JOIN for ME was adapted for delivery to children and families from low-income backgrounds living in urban cores in Rhode Island as part of a CDC-supported Childhood Obesity Research Demonstration project (RI CORD 3.0; U18 DP006429). 22
A combination of a priori and stakeholder-informed intervention adaptations were made to improve uptake of the JOIN for ME program in low-income settings. An intensive developmental formative evaluation phase, including interviews with key stakeholders and focus groups with caregivers and children, was conducted to obtain feedback on engaging with the community, adapting specific intervention components to improve implementation, and modifications for virtual delivery.23,24 Utilization of Proctor’s Implementation Outcomes Framework25,26 drove program adaptations to improve engagement,27–31 including updating materials to improve health literacy and transitioning from in-person to synchronous remote delivery.
The adapted program was tested in a type 2 hybrid effectiveness-implementation trial 32 in which outcomes of interest included both the effectiveness of the intervention (i.e., change in child weight status) and implementation of the intervention (i.e., acceptability and fidelity). We used blended facilitation, an implementation strategy in which the expertise of a facilitator within an external organization is combined with that of a member of the research team, to increase the uptake of JOIN for ME in community settings. 33
Materials and Methods
Study Overview
The study used a delayed treatment design, wherein a series of active/delayed treatment groups were conducted with participants recruited from community settings or an FQHC. One group of participants began treatment immediately following baseline assessment, while the second group waited 4 months (i.e., length of time of the intensive intervention phase), at which time they completed a second baseline assessment and began treatment. This design allowed all participants to receive the intervention, while providing a comparison of active and delayed treatment conditions at 4 months. The final enrolled cohort was only offered the intensive treatment phase due to time limitations. A Community Advisory Board (CAB) 34 was convened at the start of the project to ensure broad representation of the community and the study population 35 and met routinely throughout the duration of the study to provide high-level guidance related to project implementation.
Procedure
The internal facilitators or “champions” in each recruitment setting were coached to lead recruitment efforts. Inclusion criteria included: (1) child 6–12 years of age with BMI >85th percentile for age and sex, (2) at least one caregiver (parent or legal guardian) available to provide consent and participate in sessions, (3) ability to speak English or Spanish, and (4) agreement to study participation and delayed treatment onset. Children were excluded if: (1) either the child or the caregiver was currently involved in another weight management program, (2) they had a medical condition that would interfere with the prescribed dietary plan or participation in physical activity, (3) they were developmentally delayed such that the intervention materials would not be appropriate, or (4) they were in treatment for or diagnosed with a major psychiatric disorder that prevented group participation.
Interested families completed a brief telephone screen, followed by baseline assessment for eligible families. Caregiver consent was obtained at the start of the assessment, as was assent for children ≥8 years. Subsequent assessments occurred at the end of the intensive treatment phase (4 months) and at the end of maintenance sessions (10 months). Participants assigned to the delayed treatment condition completed a second baseline assessment at the end of the 4-month delay and prior to initiating treatment. Brief monthly calls were conducted with families during the delay period as a retention strategy.
At each assessment visit, children and caregivers were weighed and measured and completed brief questionnaires. As seen in Figure 1, a total of 111 families were consented, 8 of whom did not move forward to treatment assignment. Assignment to active or delayed treatment was based on the preferred language for intervention delivery, or in the case of cohorts in which all dyads had the same preferred language, day of the month on which the child was born. Of the 103 participants assigned to a condition, 44 in the active group and 39 in the delayed group initiated treatment. All study procedures were approved by the institutional review board at The Miriam Hospital.
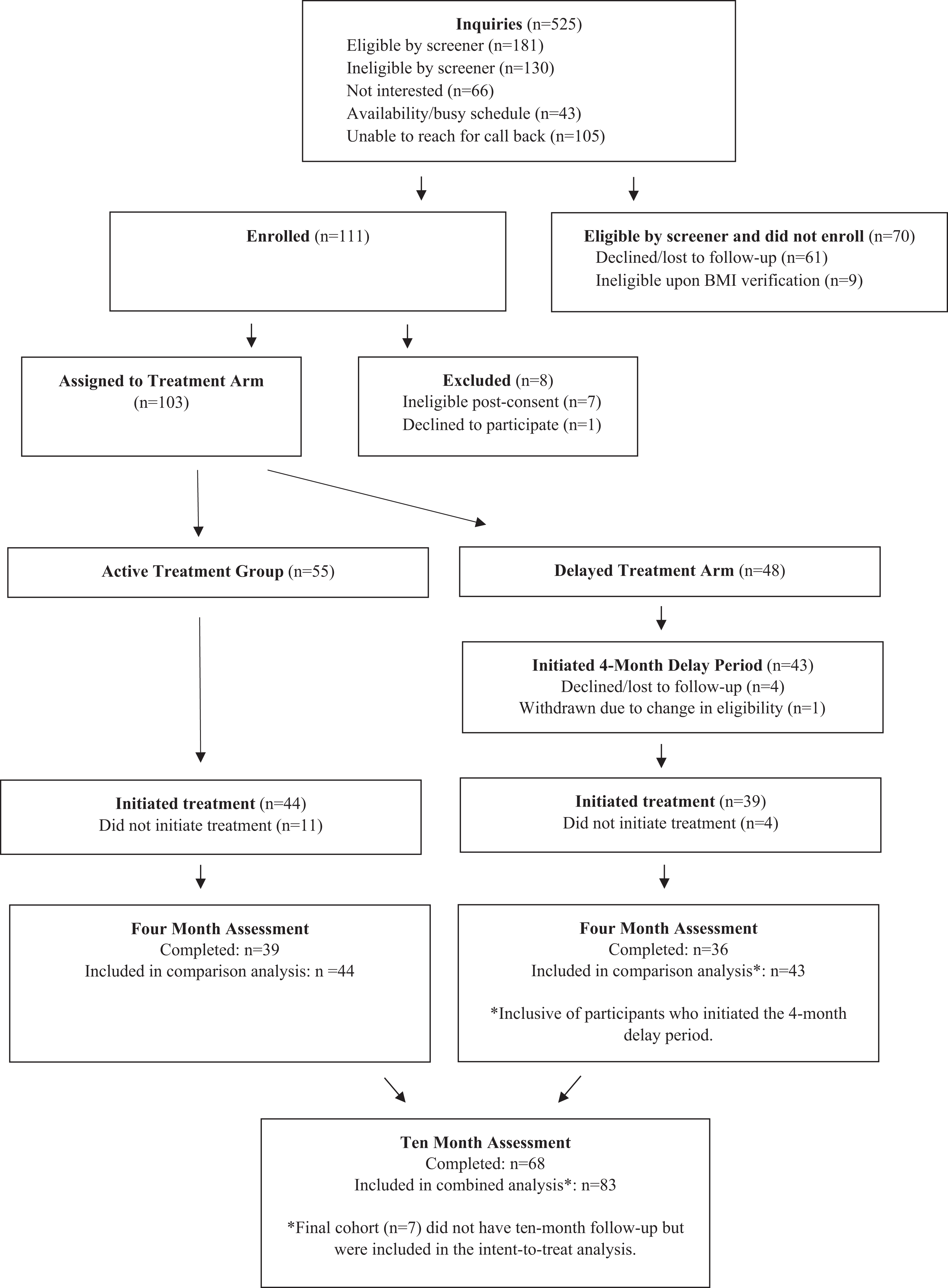
Participant flow through the study.
Intervention
Intervention targets
Intervention content of the JOIN for ME program is consistent with USPSTF recommendations and has been previously described. 22 Key concepts of the 16 core sessions include: self-monitoring, reducing LESS foods (e.g., cookies, sweetened beverages, fried foods) and increasing YES! foods (i.e., nutrient-dense foods such as fruits and vegetables), reducing screen time, increasing physical activity, and obtaining social support. Core content is reinforced during eight maintenance sessions conducted on a biweekly and monthly basis for total potential contact time of 30 hours (24 sessions × 75 minutes). Lesson format: Each dyad had a brief check-in with the coach (including virtual weigh-in and discussion of self-monitoring) followed by a group lesson that was divided into: (1) Connect—review successes and challenges in meeting goals from the previous week, (2) Learn—introduction and practice of a new skill, and (3) Go! Goals—setting goals relevant to the week’s specific content.
Coach Training and Supervision
Intervention was delivered by a trained community health worker or dietitian (i.e., coach) bilingual in English and Spanish using HIPAA-compliant Zoom. Coach training included seven self-guided modules with interactive learning opportunities followed by brief knowledge checks requiring a minimum of 80% correct responses prior to advancing to the next module. Modules covered determinants and treatment of childhood obesity, program curriculum, group facilitation skills tailored to remote intervention delivery, and addressing weight bias. Completion of self-guided lessons was followed by a remotely delivered group training session to review key content. Trained coaches participated in weekly remote supervision meetings led by a clinical psychologist or registered dietitian with expertise in the JOIN for ME curriculum.
Measures
Baseline assessments included brief caregiver interviews focused on sociodemographic variables and the child’s medical and psychiatric history. Standard demographic information was collected, including child and caregiver age, racial and ethnic background, and socioeconomic status. Food insecurity was assessed via the 18-item USDA Household Food Insecurity Survey. 36
Treatment Effectiveness
Anthropometric variables
Child and caregiver weight was obtained in person on a digital scale in street clothes without shoes, and height was obtained using a stadiometer. Weight and height were used to calculate body mass index (BMI; kg/m2), percentage of the 95th BMI percentile (%BMIp95), 37 percent over the median BMI (% median BMI, defined with reference to BMI at the 50th percentile for child’s age and sex), 38 and extended BMIz for children.
Secondary Outcomes
The Family Nutrition and Physical Activity (FNPA) screening tool was completed by caregivers to assess family behavioral and environmental factors related to obesity risk.39,40
Health-related quality of life (HRQoL) was measured via an obesity-specific child self-report measure, Size Me Up, 41 as well as the caregiver proxy, Sizing Them Up, 42 both of which have documented reliability and validity.
We administered four subscales of an adapted version of the NEWS-Y 43 to caregivers to assess perceived proximity to resources related to physical activity and diet, which has been related to increased physical activity, 44 cardiovascular fitness, 45 and increased fruit and vegetable intake in low-income neighborhoods.46,47
Implementation Metrics
We collected multiple implementation outcomes derived from Proctor’s Implementation Outcomes Framework, 25 including Acceptability, Adoption, Feasibility, Fidelity, and Costs. Here, we report information about program acceptability and treatment fidelity. Program acceptability was measured with an adapted self-report measure of program satisfaction administered to caregivers at 4- and 10-month assessments. 48
Treatment fidelity
Weekly group sessions were recorded, and approximately 20% of the 416 recorded sessions (n = 57 intensive treatment, 28 maintenance) were randomly selected and coded by an independent coder who was not part of the research team. Following a previously developed coding format, 49 each session was coded for: (1) adherence to the JOIN for ME curriculum (rated yes, partial, or no for each key topic within the Connect, Learn, and GO! portion of the session); (2) general coach characteristics (i.e., interpersonal skills and management of group interactions), rated on a scale from 1 (not at all) to 5 (a lot); and (3) overall coach expertise, rated on a scale from 1 (novice) to 9 (advanced). Each coach provided a self-rating of fidelity of intervention delivery mirroring the observer rating, allowing for examination of convergence between observer-coded and self-assessed fidelity.
Statistical Analysis
Intention-to-treat analyses were conducted using two separate multilevel models with random intercepts nested within person over time. Only individuals who initiated treatment were included in the analysis. Demographics of participants who did and did not initiate treatment were compared. Baseline participant characteristics were also compared between groups using chi-squared tests, Fisher’s exact tests, and t-tests. SPSS Version 28 was used for all analyses, with alpha set to 0.05.
The first set of analyses compared outcomes between individuals in the active versus delayed condition over 4 months. Variables that were significantly different at baseline between groups were included as covariates. The second set of analyses focused on the effects of JOIN for ME over the 10-month treatment period and included combined data from participants in both conditions aligned by treatment timepoint. The sample for this analysis was slightly smaller than the between-group comparison as it did not include individuals from the delayed treatment arm who did not initiate active treatment. Sensitivity analyses were conducted by including and not including the last cohort of participants (n = 7) who were only offered the intensive treatment. Results were not different, so these individuals are included in the presented models. Percentage of sessions attended, food security status (high and marginal food security operationalized as food secure, and low and very low food security operationalized as food insecure), and proximity to general resources and recreational resources were examined as predictors of change in relative weight outcomes over 10 months in separate models.
Results
Participants
Participant demographics are provided in Table 1. Child participants were equally distributed across males and females and averaged approximately 9 years. The sample largely identified as Hispanic or Latino, and 88.5% of children had a BMI >95th percentile. Caregivers were primarily women and had an average BMI (33.2 ± 6.8) in the obese range. Nearly half of the participants met the criteria for low or very low food security at baseline. The only significant difference between treatment groups was that the delayed group had a greater percentage of child participants who identified as Hispanic or Latino than the active group (90.7% vs. 72.7%, respectively). No differences in demographics were found between individuals who initiated treatment and those who did not. Of participants who initiated treatment, 90% completed 4-month and 89% completed 10-month assessments (n = 7 not included because they were only offered 4 months of treatment).
Baseline Demographics of Participants by Treatment Assignment
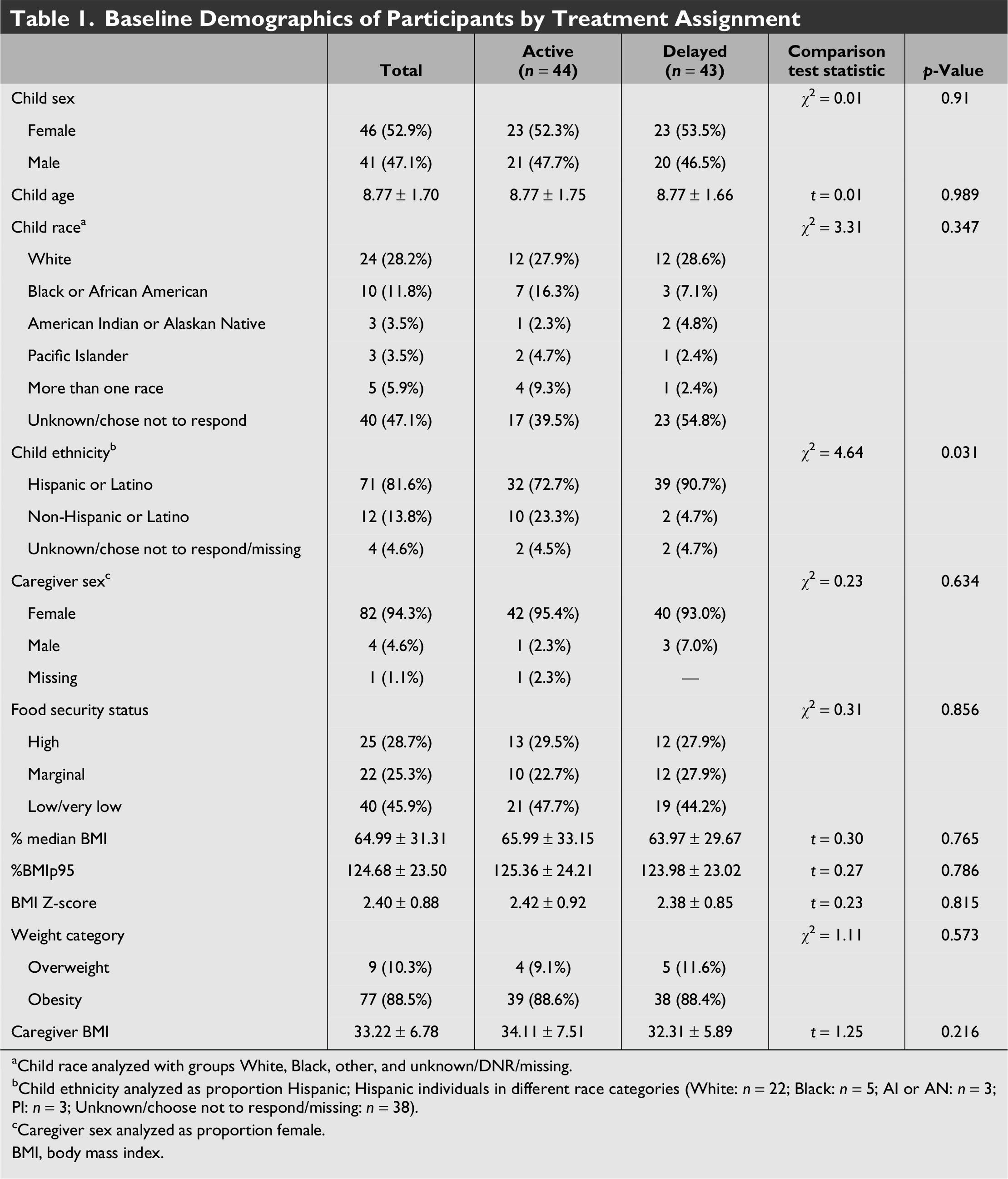
Child race analyzed with groups White, Black, other, and unknown/DNR/missing.
Child ethnicity analyzed as proportion Hispanic; Hispanic individuals in different race categories (White: n = 22; Black: n = 5; AI or AN: n = 3; PI: n = 3; Unknown/choose not to respond/missing: n = 38).
Caregiver sex analyzed as proportion female.
BMI, body mass index.
JOIN for ME Effectiveness Outcomes
Given differences in Hispanic/Latino ethnicity between groups at baseline, ethnicity was included as a covariate in analyses examining differences between groups. Analyses between active and delayed treatment groups over 4 months showed significant improvements on the FNPA in the active treatment group compared with delay. Child relative weight (all three metrics), caregiver BMI, child-reported health-related quality of life (HRQoL), and caregiver-reported child HRQoL were not significantly different by condition over 4 months (see Table 2 and Fig. 2A).
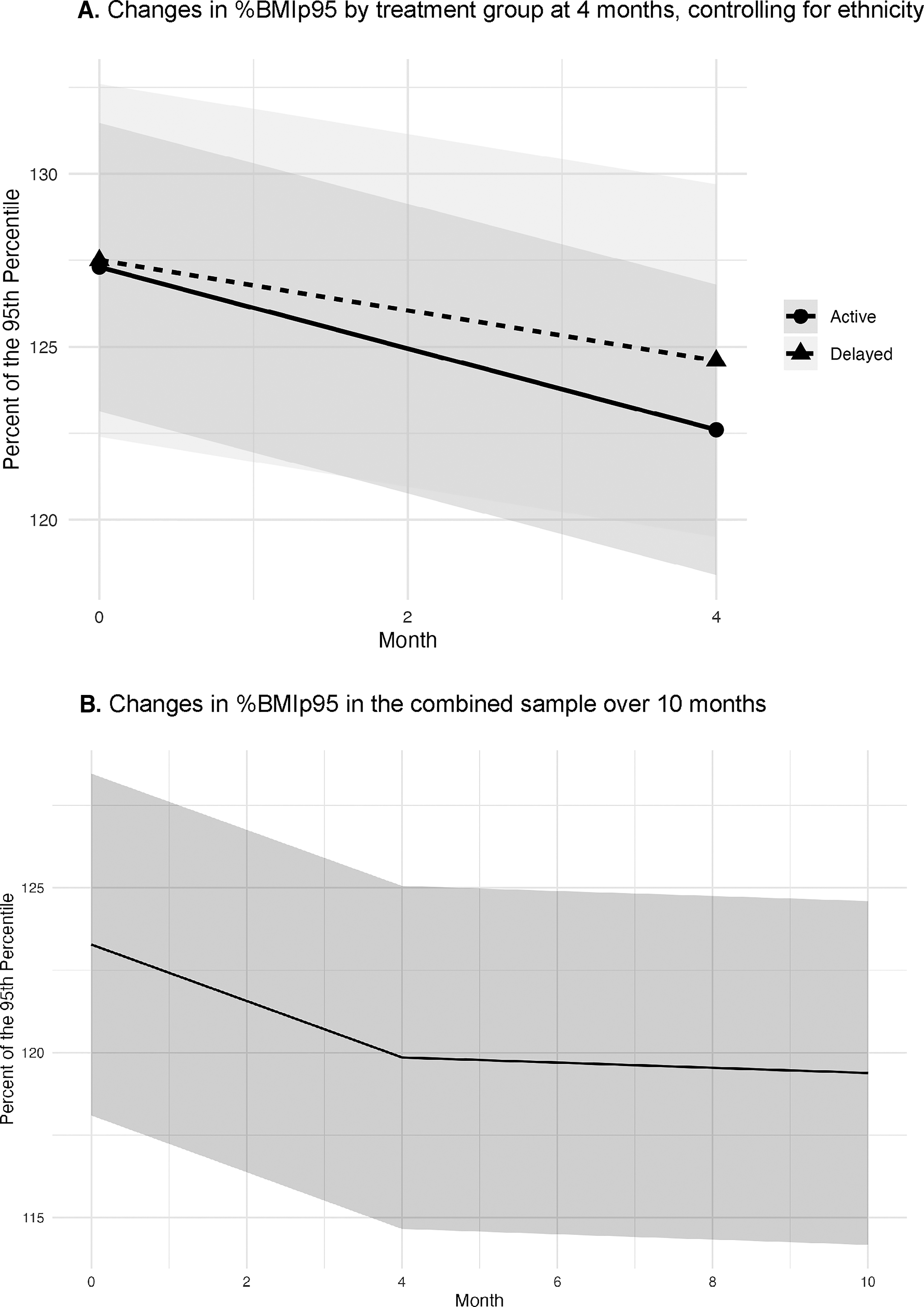
Changes in %BMIp95 at (
Estimated Marginal Means from Mixed Models of Between-Group Differences Between Active and Delayed Groups
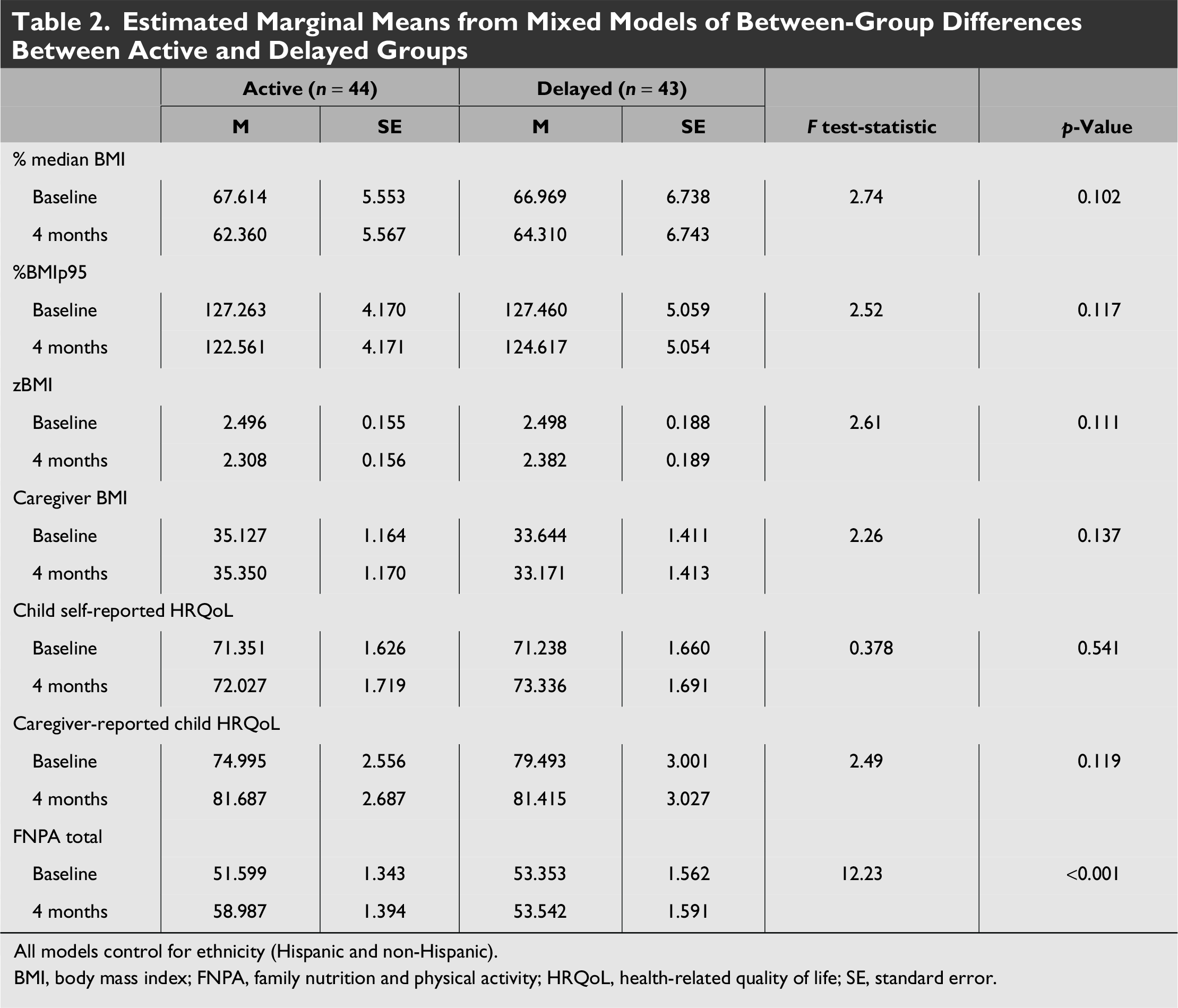
All models control for ethnicity (Hispanic and non-Hispanic).
BMI, body mass index; FNPA, family nutrition and physical activity; HRQoL, health-related quality of life; SE, standard error.
Analyses of 10-month treatment effects in the combined sample showed significant effects of time on all three metrics of child relative weight. Children who initiated JOIN for ME demonstrated decreases of 2.90% median BMI, 3.89%BMIp95, and 0.16 zBMI units over 10 months (see Fig. 2B). Caregiver-reported child HRQoL and scores on the FNPA total also improved over the 10-month treatment period (p < 0.05). No significant changes in caregiver BMI or child self-reported HRQoL were observed (see Table 3).
Estimated Marginal Means from Mixed Models of Changes at 10 Months (n = 83)
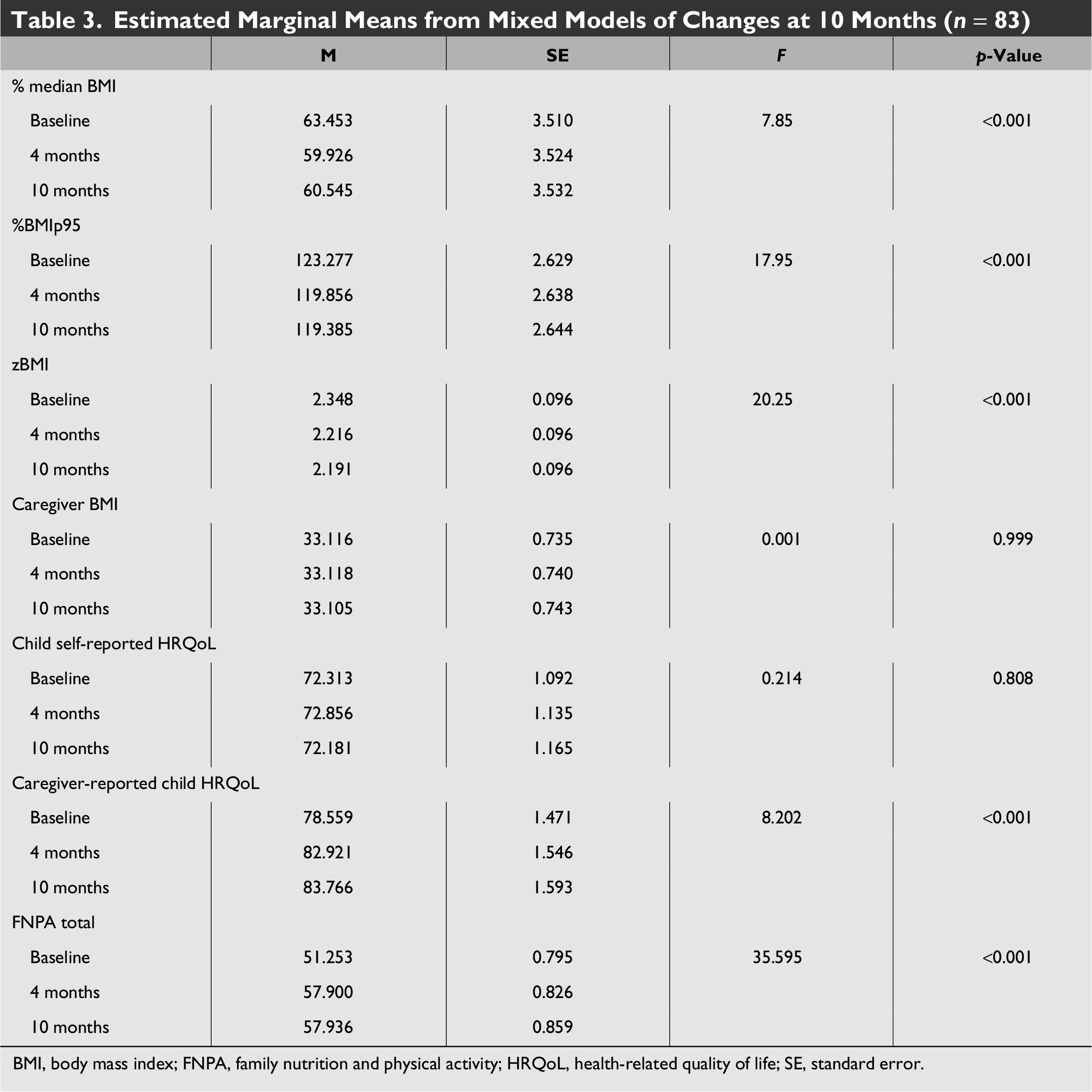
BMI, body mass index; FNPA, family nutrition and physical activity; HRQoL, health-related quality of life; SE, standard error.
Participants attended an average of 9.82 ± 4.89 of the 16 intensive sessions (61.5%) and 3.3 of the 8 maintenance sessions (41.28%). Attendance at a greater number of sessions was related to larger decreases in % median BMI (β = −0.01, p = 0.004) and %BMIp95 (β = −0.007, p = 0.005; see Fig. 3A). Food security was also found to be a predictor of change in child weight over time (β = 0.357, p = 0.034). Children from food-secure households showed greater reduction in %BMIp95 in comparison with children from food-insecure households (see Fig. 3B). Proximity to general resources (β = −0.11, p = 0.215) and recreational resources (β = −0.10, p = 0.248) did not predict change in child weight over time, though scores for proximity to general resources (β = 0.03, p = 0.002) and recreational resources (β = 0.04, p < 0.001) both significantly increased over time.
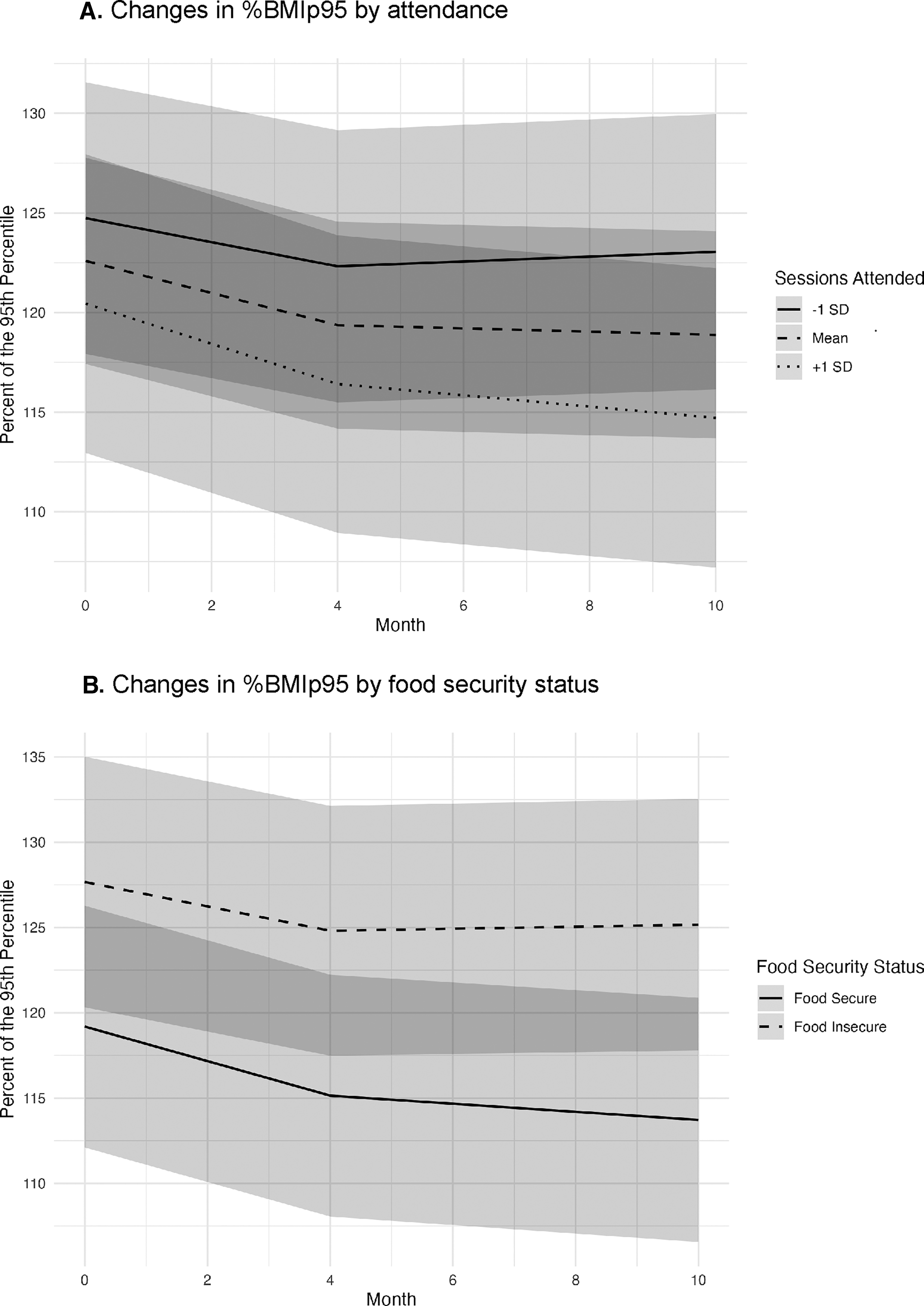
Changes in %BMIp95 at 10 months by (
Implementation Outcomes
Program acceptability
At the 4-month assessment, average scores were 4.6 ± 0.5 out of 5 on the treatment satisfaction questionnaire. 97.3% of caregivers indicated they would recommend JOIN for ME to another family, and 91.9% indicated that they “pretty much” or “very much” liked participating in JOIN for ME. At the 10-month assessment, average scores were 4.5 ± 0.6 out of 5 on the treatment satisfaction questionnaire. 94.1% indicated they would recommend JOIN for ME to another family, and 95.6% indicated that they “pretty much” or “very much” liked participating in JOIN for ME.
Treatment fidelity
98.8% of sessions selected for fidelity coding were rated, with the remaining sessions unavailable due to missing audio. Coaches were 98.1% adherent to session content material, received an average skills rating of 4.11 ± 0.39 out of 5, and had an average expert rating of 6.23 ± 1.10 out of 9, placing them at the high end of the intermediate skill category. Overall, coaches self-rated 95.5% of items as completed, 3.3% as partially completed, and 1.2% as not completed. Strong interrater agreement was identified between coach self-report and observer report across intervention content (91.2% overall).
Discussion
This is the first implementation of the JOIN for ME program adapted for families from low-income backgrounds. Participants found the program acceptable, and it was delivered with a high level of fidelity. The intervention was related to significant improvements in caregiver-reported eating and activity habits and children’s HRQoL. Changes in child weight status between the active and delayed treatment conditions were nonsignificant at 4 months, and a modest reduction in child weight status was observed at 10 months. The nonsignificant differences at 4 months may have resulted from small decreases in weight status within the delayed condition during the delay period. While intervention content was not delivered, it is possible that brief contacts with a study team member led families to begin making changes in eating and activity behaviors based on the anticipation of program start.
Of note, the change in standardized BMI is comparable with what was observed in the in-person open trial of JOIN for ME 19 and in a remotely delivered group-based intervention in rural settings. 50 However, the reduction in child weight status is less robust than that observed in other IHBLTs. It is unclear whether this resulted from transition to remote intervention delivery or challenges with program participation experienced by families from low-income backgrounds. While not uniformly the case, 51 dose as measured by attendance at treatment sessions has commonly been related to treatment outcome. 13 Remote intervention delivery addressed commonly cited transportation barriers; however, participants continued to experience challenges with engagement (61.5% attendance at intensive treatment sessions). We also observed challenges with engagement at the stage of program enrollment, which was most notable with community organizations (32% of recruited participants). It is possible that the blended facilitation strategy was less effective in this context compared with health care settings.
The other significant predictor of outcome was food security, with children from food-secure households demonstrating a greater decrease in weight status. Approximately 70% of enrolled families endorsed marginal, low, or very low food security. Food and nutrition security are significant social determinants of health, related to disparities in diet-related diseases52–56 as well as less robust outcomes in implementation of IHBLTs.57–59 These findings reinforce a recent call 15 highlighting the importance of research to address food security as a critical contextual variable in implementation of IHBLTs.
Consistent with the hybrid study design, next steps include integrating current findings with additional measures of program implementation, including cost of implementation delivery and post-intervention formative evaluation, to make further program adaptations and identify pathways for larger-scale dissemination. Critical elements of this plan include consideration of previously identified factors relevant to scaling the JOIN for ME program, such as highlighting return on investment and maintaining connection to the local community, 60 and identification of opportunities within the health care setting. The latter are being explored through ongoing discussions with members of our CAB, which include leadership within the Rhode Island Department of Health and a clinical care network of pediatric providers.
Conclusions
Remotely delivered adaptation of the JOIN for ME program was found to be acceptable, delivered with high fidelity, and associated with modest reductions in child weight status and improvements in child HRQoL in children from low-income backgrounds. Priorities for future work include identifying effective strategies for addressing food insecurity, increasing participant engagement, and securing pathways for larger-scale program dissemination.
Impact Statement
A remotely delivered adaptation of the JOIN for ME program was found to be acceptable, delivered with high fidelity, and associated with modest reductions in child weight status and improvements in child health-related quality of life in children from low-income backgrounds. Next steps include further adaptation and larger-scale dissemination.
Authors’ Contributions
E.J.: conceptualization, funding acquisition, methodology, supervision, writing—original draft, writing—review and editing; J.H.: conceptualization, data curation, formal analysis, visualization, writing—original draft, writing—review and editing; K.E.D.: conceptualization, data curation, formal analysis, project administration, writing—original draft, writing—review and editing; R.S.: conceptualization, formal analysis, funding acquisition, methodology, supervision, writing—review and editing; D.S.S.: conceptualization, methodology, writing—review and editing; A.G.: conceptualization, data curation, investigation, project administration, writing—original draft, writing—review and editing; W.E.: conceptualization, funding acquisition, project administration, writing—review and editing; A.R.E.: conceptualization, funding acquisition, methodology, supervision, writing—original draft, writing—review and editing.
Footnotes
Acknowledgments
The authors would also like to acknowledge all of the families who participated in the study as well as the incredible commitment of research staff, interventionists, and community collaborators.
Author Disclosure Statement
None reported by any of the authors.
Funding Information
This study was supported by the Centers for Disease Control and Prevention (CDC; Award No. U18 DP006429 to E.J.). This work is solely the responsibility of the authors and does not represent official views of the CDC. Dr. Elwy is supported by a VA Health Systems Research (HSR) Research Career Scientist Award, RCS 23-081.