
Abstract
Background:
Although intensive health behavior and lifestyle treatment (IHBLT) is effective for treating youth obesity, it is not accessible to many. Our objective was to examine the implementation of Fit Together, an evidence-based IHBLT clinic–community model delivered by health care and local parks and recreation.
Methods:
This study used a hybrid type 3 implementation-effectiveness design to examine uptake and implementation of the Fit Together model in eight North Carolina counties from 2016 to 2021. Each Fit Together partnership was provided with an implementation manual, training, technical assistance, and financial support. Implementation outcomes included partnership characteristics and program delivery (e.g., hours, referrals, attendance). Effectiveness outcomes included engagement (dose received), changes in child lifestyle habits, quality of life, and body mass index (BMI). Descriptive statistics described implementation outcomes, and linear regression models examined changes in participant-level outcomes.
Results:
All eight locations implemented Fit Together (range: 5–18 months). A total of 1193 youth with obesity (12 years ± 3.0, 52.4% female) were referred to a Fit Together program. Of referred youth, 20% (241/1193) attended ≥ 1 session, of which 85% (205/241) attended ≥2 sessions. Nearly a third of engaged participants (29%, 70/241) received ≥26 treatment hours. For each additional session attended, BMI percent of the 95th percentile declined (β = −0.12, p = 0.06).
Conclusions:
The Fit Together model can be delivered in diverse settings, engage priority populations, and deliver IHBLT in a variety of locations. Future work should test scalability and dissemination strategies for clinic–community models of child obesity treatment.
Keywords
Introduction
The 2023 American Academy of Pediatrics (AAP) clinical practice guideline for the treatment of child and adolescent obesity recommends intensive health behavior and lifestyle treatment (IHBLT), pharmacotherapy, and surgical approaches based on individual patient criteria, including age and obesity severity. 1 Among those treatment options, IHBLT is the cornerstone of treatment, with the AAP and the United States Preventive Services Task Force (USPSTF) recommending IHBLT for children aged 6 years and older with body mass index (BMI) ≥ 85th (AAP) or 95th (USPSTF) percentile. 2 IHBLT is defined as receiving a “dose” of ≥26 hours of face-to-face skills-based intervention including a combination of nutrition and physical activity, delivered by health professionals over a 3–12 month period.1–3 However, IHBLT is challenging to implement in clinical and community settings; thus, access remains low, particularly for populations who have a high risk for poor health due to environmental factors. 4
“Fit Together” partners health care organizations with local parks and recreation departments to deliver the components of IHBLT. Across the US, over 10,000 parks and recreation departments oversee 40 million youth participating in structured activities. Nearly 75% of Americans live within walking distance of a parks and recreation site, and these centers represent the diversity of the communities they serve. 5 The mission of Parks and Recreation includes improving community health for families, thus representing an aligned community partner.
In the Fit Together model, clinician partners screen for obesity, provide lifestyle counseling, and treat comorbidities, while the recreation partner offers family-based physical activity and nutrition sessions. Fit Together has demonstrated feasibility 6 and effectiveness in reducing BMI 7 and improving quality of life 8 among diverse and low-income youth with obesity and the ability to meet the IHBLT dose threshold (≥26 hours over 3–12 months). However, implementation in diverse settings has been less investigated. The main objective of this study was to examine implementation of Fit Together within eight geographically diverse counties representing rural and urban settings in North Carolina.
METHODS
Study Design
We used a hybrid type 3 design to evaluate the implementation (primary) and participant-level effectiveness (secondary) of the Fit Together model (clinicaltrials.gov ID: NCT03246763).9,10 All study protocols were reviewed and approved by the Duke University Health System Institutional Review Board.
Study Setting and Participants
The selection of program sites was informed by the Healthy People, Healthy Carolinas Initiative (HPHC), launched by the
ARCHES Site County-Level Descriptors
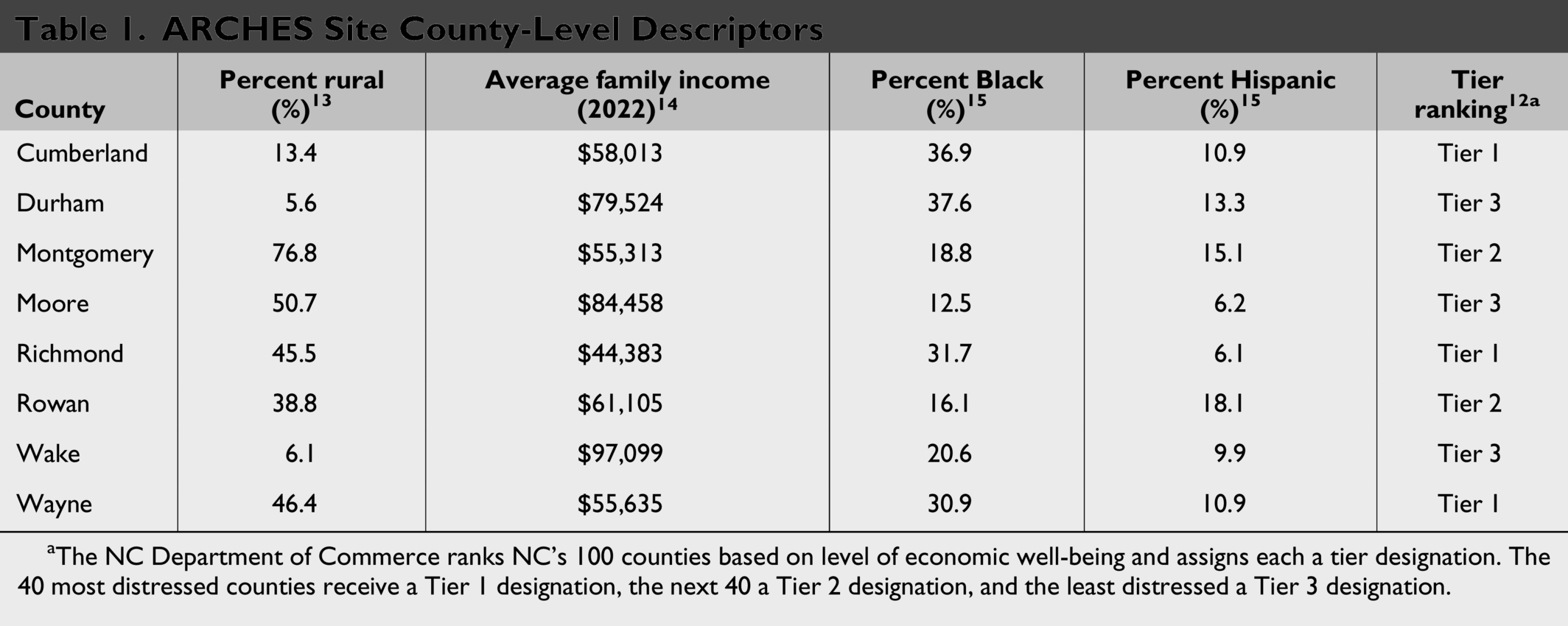
The NC Department of Commerce ranks NC’s 100 counties based on level of economic well-being and assigns each a tier designation. The 40 most distressed counties receive a Tier 1 designation, the next 40 a Tier 2 designation, and the least distressed a Tier 3 designation.
Within each county, the HPHC initiative helped to identify potential partners for the implementation of Fit Together. The clinical partners varied (e.g., pediatrics, family medicine), as did the recreation partner (e.g., local parks and recreation, YMCA, or other entity with space). The study team visited local sites to provide orientation and technical assistance. The HPHC coordinator determined which individuals should be involved in this meeting.
The Fit Together program offers broad criteria for participation: children must be referred by a primary care provider, be school-aged (5–17 years old), and have an age- and sex-specific BMI ≥ 85th percentile. We selected the age range prior to current AAP guidelines that recommend IHBLT for ages 6 and older. Each county was permitted to narrow participation criteria to their local needs and capacity, such as a targeted age group or severity of obesity.
Fit Together
Fit Together was developed over a period of 8 years prior to the start of this study as a partnership between the Duke Healthy Lifestyles clinic and Durham Parks and Recreation. For this study, we utilized primary care rather than tertiary obesity care as the clinical partner.
During routine well-child visits, providers screen patients for obesity using age- and sex-specific BMI curves and provide obesity counseling. The clinician refers the patient to the Fit Together “Connector,” a position that could be within the health care setting (e.g., community health worker) or in the recreation setting (e.g., recreation professional). The Connector receives the referral, contacts the caregiver, and invites the family to participate. The operational process was developed by each site to fit their needs, though contact was most commonly by phone. The child, caregiver, siblings, and other household family members are invited to attend Fit Together sessions for up to 12 months, free of charge. Children with disabilities were welcome to participate with accommodations as available by site. Parent and sibling participation was welcomed, and parental supervision was required.
Fit Together sessions are 90–120 minutes in duration and occur 2 to 3 days per week with at least 1 weekend session and 1 weekday evening. Connectors lead the sessions, which include stretching, sports and games, hands-on nutrition education, and unstructured playtime. All activities are tailored and adapted for low-income, culturally diverse families and children with obesity-related physical limitations.
Implementation Support
Fit Together sites received a comprehensive implementation guide, known as the “Playbook.” The Playbook (see Supplementary Data) was developed around the constructs of the Consolidated Framework for Implementation Research, 16 providing guidance on assessing and leveraging characteristics of the intervention, outer and inner settings, and individuals. Specifically, the Playbook included information on the development of referral strategies, partner engagement, identification of space and equipment requirements, staff hiring and training, and session planning. It also included materials for planning program sessions, such as examples of group-based activities, individual activities, and a nutrition curriculum.
The research team provided the Playbook, referral, and data management technical assistance to ensure consistency of attendance tracking, quarterly in-person training, financial support, and adaptation guidance as key implementation strategies to support the uptake of Fit Together. This assistance was provided to local sites through phone calls and monthly meetings as they developed their relationships locally, moved through the pre-implementation phase, and implemented their Fit Together program. In addition, Each program location also received a $5000 one-time stipend to purchase the necessary equipment for Fit Together sessions (e.g., balls, mats, cooking utensils). Sites had the flexibility to adapt and tailor the program to fit their local needs and resources.
Measures and Data Collection
Proctor’s Implementation Outcomes for Implementation Research framework 17 was used to inform measure selection. We focused primarily on adoption—successfully starting a program—and fidelity—delivering an adequate number of sessions for children to achieve the 26-hour dose. Table 2 shows the constructs, measures, and data sources. Data were collected using surveys of clinic and community partners and families, administrative program data, and observational assessment of programs.
Measures

Implementation outcomes
Sites were responsible for tracking referrals from the clinical staff, contacting families to introduce the program, and conducting sessions. Referral data were entered into a REDCap database, which sites used to manage contact information. At the end of each session, the site Connector entered individual-level attendance into REDcap. In addition, they provided data about the types of activities offered at each session, approximate session length and frequency offered (“dose delivered”), and total number of children, siblings, and caregivers in attendance. These data were all collected continuously throughout the study period.
Individual outcomes
Participant-level individual data were collected via survey of parents, site-based attendance logs, and referral information. After referral data were entered into REDCap, participants were sent a survey via email or text at baseline, 3, and 6 months.
Baseline clinical data included height and weight measured in clinic and recorded in the child’s health record. These measures were collected again at 3 and 6 months, as available, via request to the clinic, though, in practice, time between measures varied. Obesity severity was indicated by BMI percent of the 95th percentile. 18 Limited demographic data were collected via the provider referral form, including age and sex. Additional demographic data, such as race and ethnicity, were collected via baseline participant survey. Quality of life was assessed through the “Sizing Me Up” survey; 19 self-reported nutrition and physical activity questions were derived from the Family Life, Activity, Sun, Health, and Eating Study; 20 and food insecurity was assessed through a two-item screener. 21 Participant/family satisfaction and a social cohesion (peer support) survey were assessed at 6 months. Surveys were provided electronically through REDCap, but sites could provide paper versions and enter data themselves. Attendance logs were completed by on-site coordinators.
Completion of study surveys was not required for program participation. Families typically would not complete a survey unless they attended the program at least once and inconsistently completed the intended 3- and 6-month surveys. In addition, while the referral forms included sex, age, height, and weight, programs could proceed with the referral even if data were missing. Because this was primarily an implementation study, no data were retrospectively abstracted. Results are presented with sample sizes included for each measure.
Caregivers who participated in the surveys provided informed consent at that time. Children did not provide assent because they were not questioned. Participants who did not complete surveys have data included through a waiver of informed consent—no identifiable information was available to the researchers.
Data Analysis
Implementation outcomes
We used descriptive statistics to report overall and site-specific implementation characteristics, including total sessions offered, mean number of participants per session, session length, physical activity minutes per session, and nutrition minutes per session. We also described overall program-level implementation outcomes, including total referrals and attendance.
Individual outcomes
We used descriptive statistics to report baseline participant-level characteristics, including sex, age, weight class, race/ethnicity, food insecurity, quality of life, and nutrition and physical activity behaviors, and examined changes over time using standard t-tests. The primary effectiveness outcome was achieving 26 contact hours. We examined the relationship between program attendance and BMI using a linear regression analysis, with clustering by site, controlling for time between BMI measurements. We report satisfaction with the program at 6 months (no baseline). We do not use a prespecified alpha (commonly 0.05) to avoid the artificial binary of significant or not significant. Instead, we report p-values to three significant digits and allow the reader to draw conclusions using both effect sizes and p-values. All analyses were performed using Stata 17 (College Station, TX).
RESULTS
Implementation Outcomes
The clinic–community partnerships represented diverse geographical settings in North Carolina (Table 1, Fig. 1). All eight clinic–community partnerships were successful in establishing and implementing a Fit Together program, though the length of time between pre-implementation (planning) and implementation varied from 5 to 18 months.
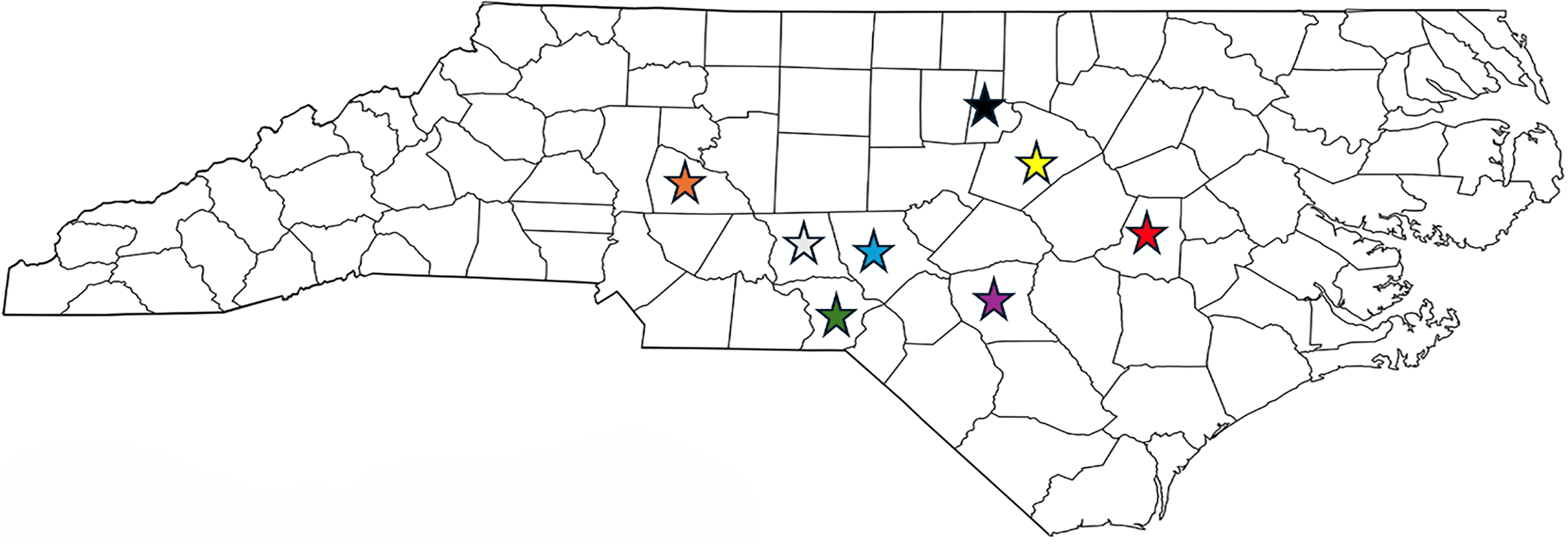
Map of locations.
All programs delivered sufficient hours of programming (“dose delivered”) for children to achieve the 26-hour recommended dose (range 30–203). Program session lengths were intended to be 90–120 minutes, and actual mean session length was 93 minutes (Table 3). The mean number of participants per session ranged from 2.1 to 14. There was significant variability in the average session length and time spent on physical activity and nutrition. Of the activities provided in the Playbook, Fit Together sites most commonly included indoor team games (58.5%) or indoor individual activities (54.8%). Only ∼43% included any outdoor activity and <40% included any type of nutritional activity.
Site-Specific Session Characteristics
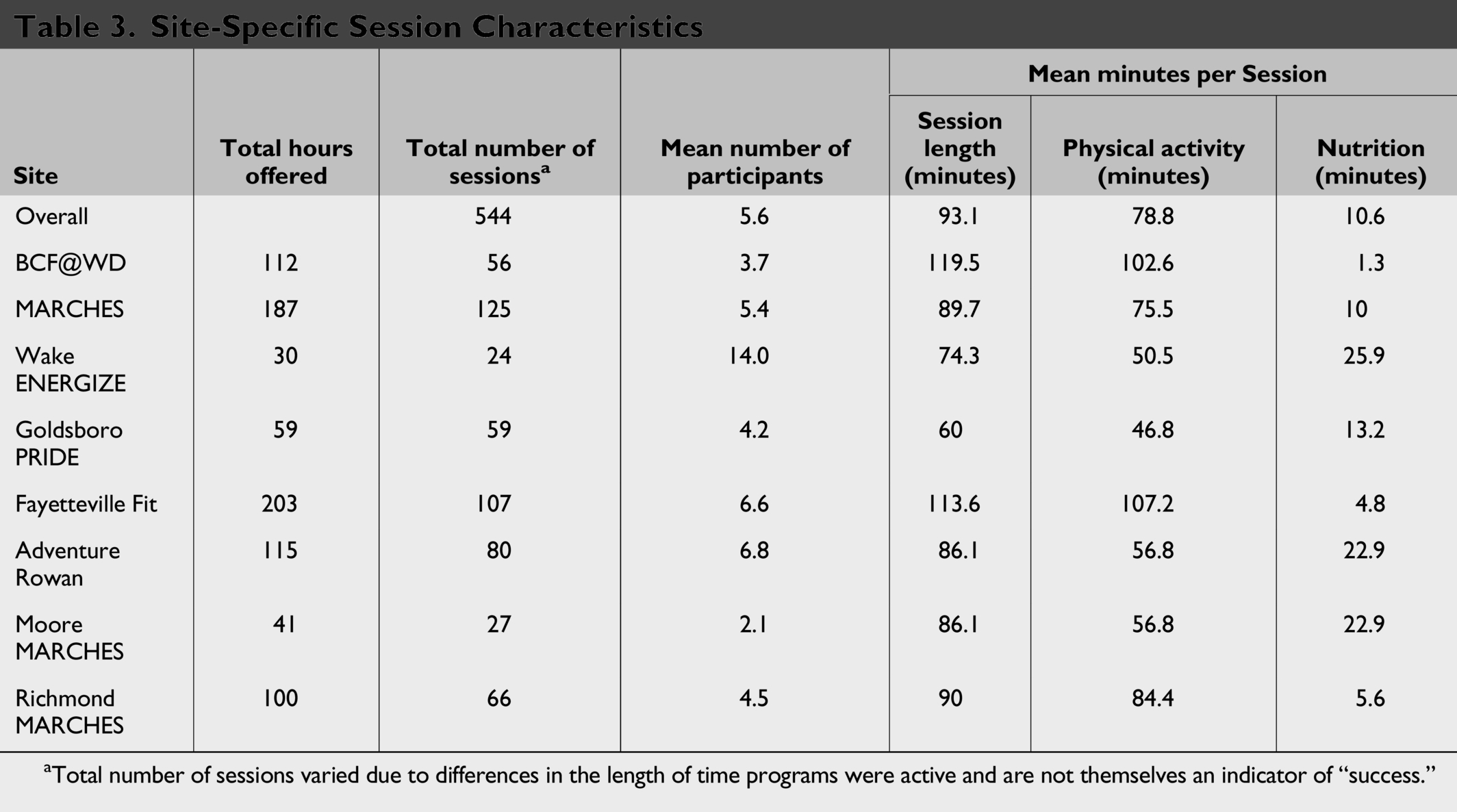
Total number of sessions varied due to differences in the length of time programs were active and are not themselves an indicator of “success.”
Participant-Level Outcomes
Participant demographics
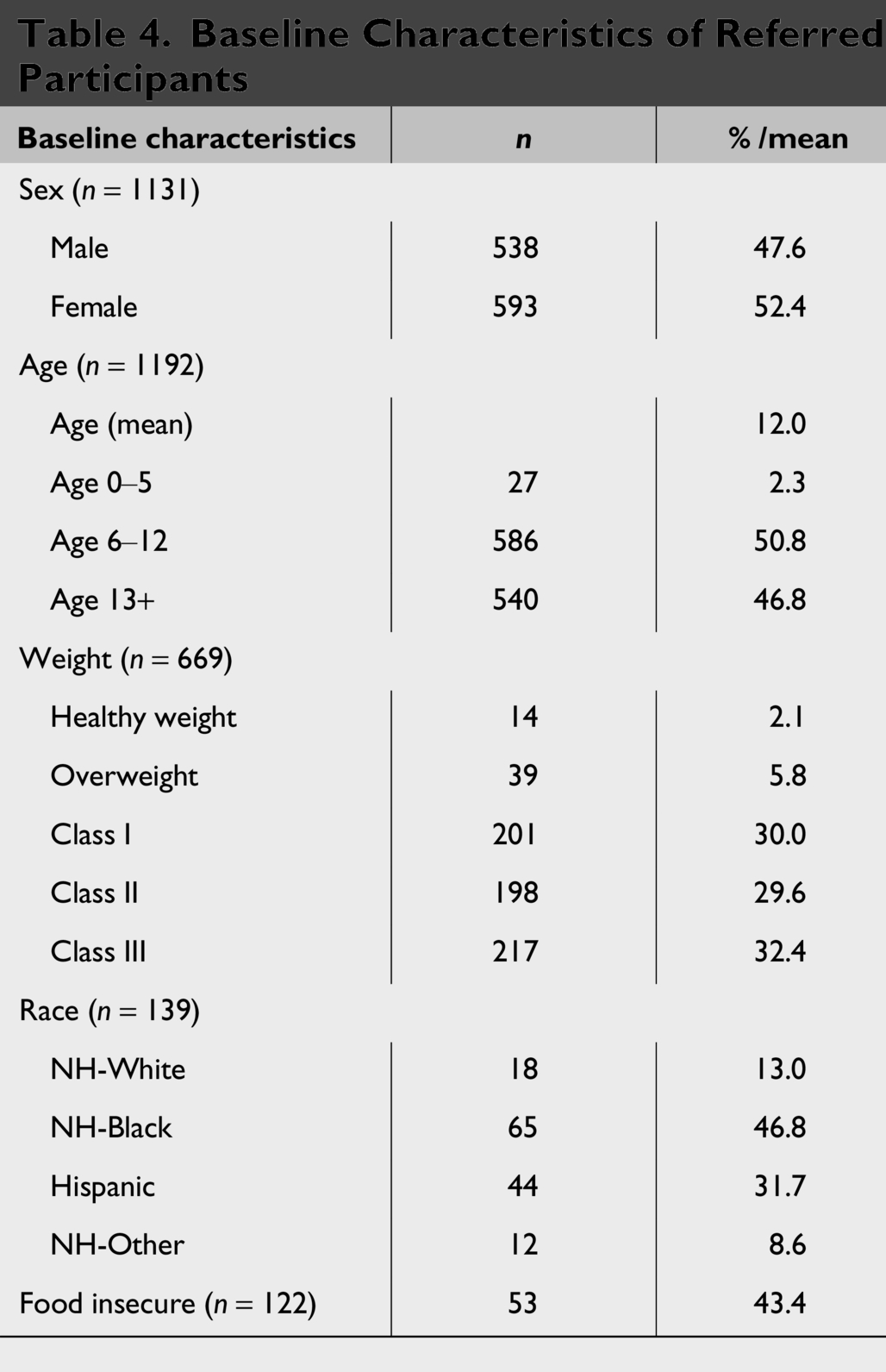
Referred participants (n = 1193 total) were 52.4% female, with a mean age of 12.0 ± 3.0 years old (Table 4). Among referred participants with complete baseline height and weight measurement data (n = 669), 61.8% of participants had severe obesity and were evenly distributed across obesity classes. For participants who completed demographic surveys (n = 139), 46.8% of participants identified as non-Hispanic Black, and 31.7% identified as Hispanic. Those completing food insecurity questions (n = 122, 88% of survey respondents) indicated that 43.4% reported having food insecurity.
Baseline Characteristics of Referred Participants
Dose received
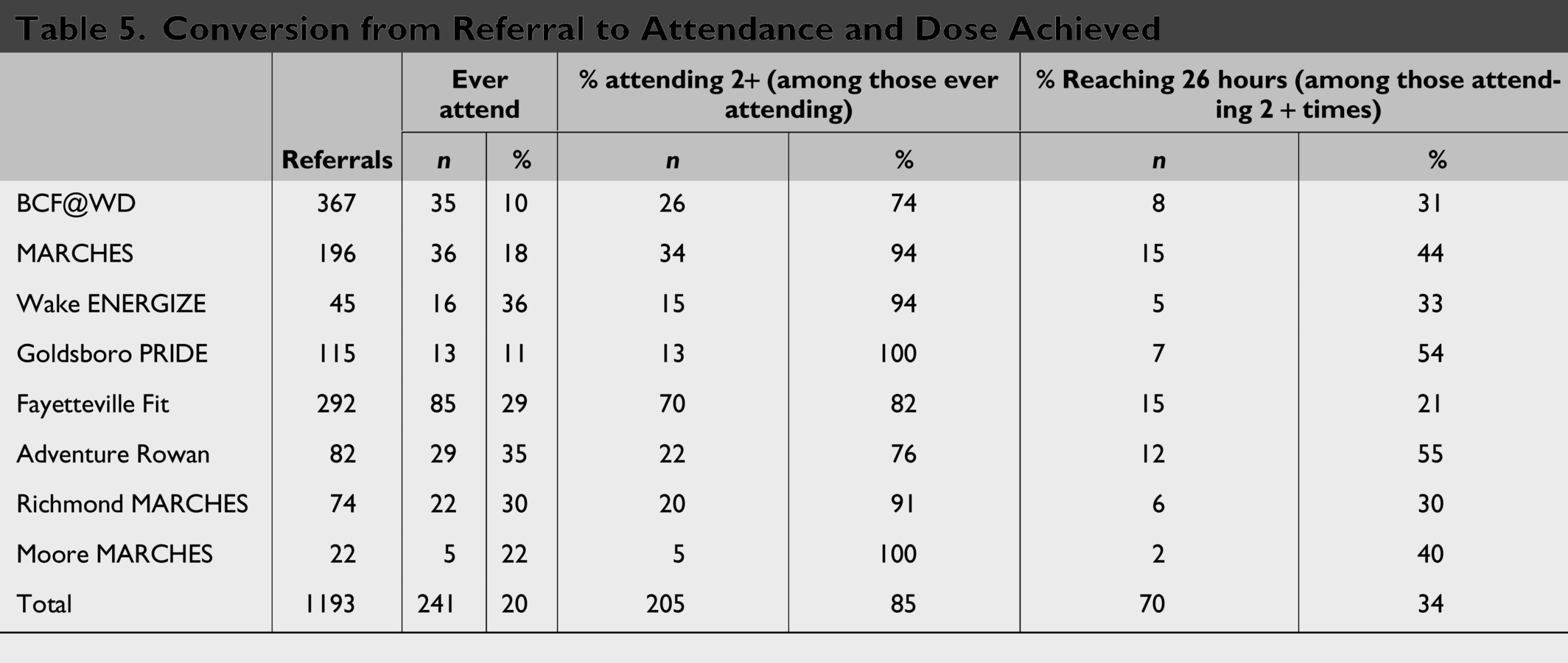
A total of 1193 children were referred to one of the eight Fit Together sites, and 241 (20.2%) attended at least one session (Table 5). Given that significant attrition from referral to attending a community-based program is expected, 22 we further examined only the “engaged” participants to assess effectiveness of the program itself. After attending their first session, most participants (n = 205/241) returned for at least one additional session, ranging from 74% to 100% of participants across sites. Of those who attended two or more sessions, 34% (n = 70/205) met the 26-hour treatment recommendation, ranging from 21% to 55% across sites. Overall, 4.2%–11% (mean 6%) of referred patients receive 26 hours of intervention in a 6-month period.
Conversion from Referral to Attendance and Dose Achieved
Health behaviors
Among health behavior survey respondents (n = 120) at baseline, 43% reported being confident eating fruits and vegetables, 68% reported being active 3 days a week, 82% watched 2 or more hours of television per day, and 81% played video games 2 or more hours per day. Among the 22 participants who responded to the post survey, there was an increase in confidence in eating fruits and vegetables. There were no significant changes in activity, sedentary time, or obesity-related quality of life.
BMI
Thirty-four participants had complete height and weight at 3 months, and 46 had complete height and weight at least one post time point, up to 6 months. Those (n = 34) with complete measures at baseline and 3 months had a significantly lower BMI percent of the 95th percentile at 3 months as compared with baseline (129.5% vs. 126.2%, p = 0.002). Those (n = 46) with any follow-up height and weight had a lower BMI percent of the 95th percentile (125.3% vs. 123.4%, p = 0.065). Examining those with any follow-up BMI, program attendance was associated with change in BMI percent of the 95th percentile (β = −0.12, p = 0.063), indicating that each additional day of program attendance was associated with a reduction of 0.12 in BMI percent of the 95th percentile.
Response to the satisfaction survey was low (n = 18). At 6 months, survey respondents reported agreeing or strongly agreeing that the referral process was easy (93.8%), program hours and location worked well for the family (94.1%), and the program helped their child become healthier (82.4%). Social cohesion survey respondents (n = 28) indicated strong social cohesion at the programs. Most respondents agreed or strongly agreed that they can count on (92.9%) or trust (96.4%) individuals at the program and felt a sense of belonging at the program (82.1%).
DISCUSSION
This study provides evidence for a real-world implementation model of IHBLT for youth with obesity in a variety of priority populations, through clinic–community partnerships. IHBLT is recommended by the USPSTF, the Centers for Disease Control and Prevention (CDC), and the AAP as a first-line treatment for obesity in children ages 6 and older. However, access is limited by multiple structural barriers such as high operating costs, issues with insurance coverage and reimbursement, and insufficient capacity. 7 Among primary care providers, barriers to addressing weight management include limited time, perceived environmental barriers, and limited knowledge of community resources. 13 Several existing interventions have been developed to meet this need. The Bright Bodies/Smart Moves for Kids program is a 12-week program for diverse children aged 7–18 with overweight or obesity. 23 The YMCA’s “Healthy Weight and Your Child” program is a real-world implementation of the Mind, Exercise, Nutrition, Do It (MEND) child obesity intervention. The program is for children aged 7–13 with obesity, and while the original MEND studies lasted 10 weeks, 24 the YMCA program is designed over 4 months, with 25 two-hour sessions in total. 25 By comparison, Fit Together is longer in duration (12 months vs. 3–4 months), requires a clinical partner, was offered in this study to a wider age range (5–17 years), and was conducted in mostly rural counties. All eight counties included in this study successfully implemented Fit Together, and both the settings and the populations of children were diverse.
While overall fidelity to the intended intervention was maintained at all sites in terms of number and duration of sessions offered (“dose delivered”), adaptations were common and favored indoor physical activities over nutrition. Although the AAP guidelines for IHBLT do not specify amounts of physical activity, nutrition, or any other component, this may indicate limited availability of facilities for nutrition education. Even so, 40% of sessions included some nutrition component, consistent with a weekly nutrition lesson. Adaptations are a critical part of implementing community-based interventions, although studies evaluating real-world implementation of the Diabetes Prevention Program caution that some adaptations may compromise fidelity to key components and limit effectiveness. 26 As noted in the AAP guidelines report, future research should better quantify the duration and quality of specific components needed for effectiveness.
In the IHBLT literature, dose appears to be the strongest predictor of participant-level outcomes; interventions that achieve more hours of face-to-face contact are associated with greater improvements in health behaviors, reductions in BMI, and improvement in overall health status.1, 3 Interestingly, while only 1:5 children who were referred to Fit Together in this study ultimately attended, ∼4:5 who attended once then attended multiple sessions. Among those who attended at least twice, 34% met the IHBLT “dose received” threshold, and among those with follow up data, children reduced BMI by 2% to 3% over 1 year. From a public health perspective, an intervention that targets a common health condition and improves outcomes for a third of participants is likely to have a positive impact at the population level if implemented at scale. Potential strategies to improve referrals, engagement, and frequent attendance may include optimizing workflows (e.g., electronic health record referrals), family navigation and support (e.g., programs on a bus line, integrating food insecurity resources into programming), and setting clear expectations for outcomes (e.g., orientation sessions). Future research—and future IHBLT programs—should focus on testing engagement-focused implementation strategies to improve conversion from clinician referral to program engagement.
One notable finding is the ability to reach high-need populations. The Fit Together programs in this study served populations that were rural, largely had severe obesity, and with a high prevalence of food insecurity. Future IHBLT programs should consider adaptations that further enhance the ability for communities to meet the needs of these children.
The study had several limitations. Because the focus was on implementation, only a fraction of those referred had complete data for our effectiveness endpoints. In addition, the opt-in nature of the surveys led to very low response rates to questions covering activity, nutrition, and quality of life. The individuals who responded were more likely to be engaged in the program and may not represent those who were referred. In addition, broader generalizability is limited, as these sites were across North Carolina.
Conclusions
The Fit Together model, a clinic–community partnership, can be delivered in diverse settings, engage priority populations, and deliver IHBLT in a variety of locations. Fit Together and the Playbook continue to evolve, integrating evidence from the AAP guidelines and incorporating new implementation strategies, such as online access, a more detailed and guided curriculum, and strategies for tightening clinic–community connections. Future goals include leveraging partnerships with parks and recreation departments to improve dissemination and reach a broader population of children needing obesity treatment.
Impact Statement
This study demonstrates that Fit Together, a model of IHBLT for child obesity treatment delivered through clinic–community partnerships, can be implemented across diverse settings, improving access to intensive health behavior and lifestyle treatment.
Footnotes
Acknowledgments
Colleen Toomey, Andre White, Michelle Wells, Dianne Ward, Cayla Treadway.
Authors’ Contributions
All persons who meet authorship criteria are listed as authors. All authors approved the final version.
Author Disclosure Statement
Dr. Heeren reports consulting fees from WW International Inc., outside the scope of the submitted work.
Funding Information
This work was supported by funding from The