
Abstract
Introduction
Pediatric obesity is a public health challenge, 1 impacting 14.1 million children in the Unites States. The Healthy Weight Clinic (HWC) is a Centers for Disease Control (CDC) recognized Family Healthy Weight Program (FHWP) that delivers Intensive Health Behavior and Lifestyle Treatment (IHBLT) for children with overweight or obesity in line with the American Academy of Pediatrics (AAP) Clinical Practice guidelines. 2 The HWC has been proven effective in reducing child BMI, sugary beverage, fast food intake, and screen time, while increasing sleep duration, physical activity, improving binge eating symptoms, 3 and parental stress.4-6 It has also been demonstrated to be cost-effective. 7
The aims of this study were to:
Package the HWC evidence-based FHWP to support implementation and adoption by health centers serving low-income children.
8
Conduct a Type III hybrid effectiveness–implementation study using a single-arm pilot trial to test implementation strategies and improvement in BMI over 1 year of the packaged HWC intervention.
9
Develop a sustainability and dissemination plan to accelerate adoption and scale of the HWC across health centers providing pediatric care.
8
In this type III hybrid effectiveness–implementation study, 10 the HWC was evaluated using a single-arm pilot trial that disseminated the HWC to four health care organizations with eight affiliated health centers: two federally qualified health centers in Mississippi (MS), one federally qualified health center in Massachusetts (MA), and an academic medical center in MA with five affiliated health centers. 8 This article presents implementation and effectiveness outcomes. The Mass General Brigham Institutional Review Board (IRB) approved all procedures (Protocol #s: 2019P001853; 2021P000258; 2023P003302). Quality improvement (QI) and evaluation data were also exempted by the AAP IRB (Protocol # 21 LI 01).
Methods
The HWC Package
The HWC package consists of (1) individual visits with a multidisciplinary clinical care team, (2) telephone check-ins, and (3) group sessions with other families to deliver 26 contact hours over 12 months (Fig. 1). It includes a HWC implementation and maintenance support: training modules, technical assistance (TA), and structured QI. A cost tool was developed to assist health centers in identifying the number of patients needed to be engaged in the HWC to be sustainable. 11
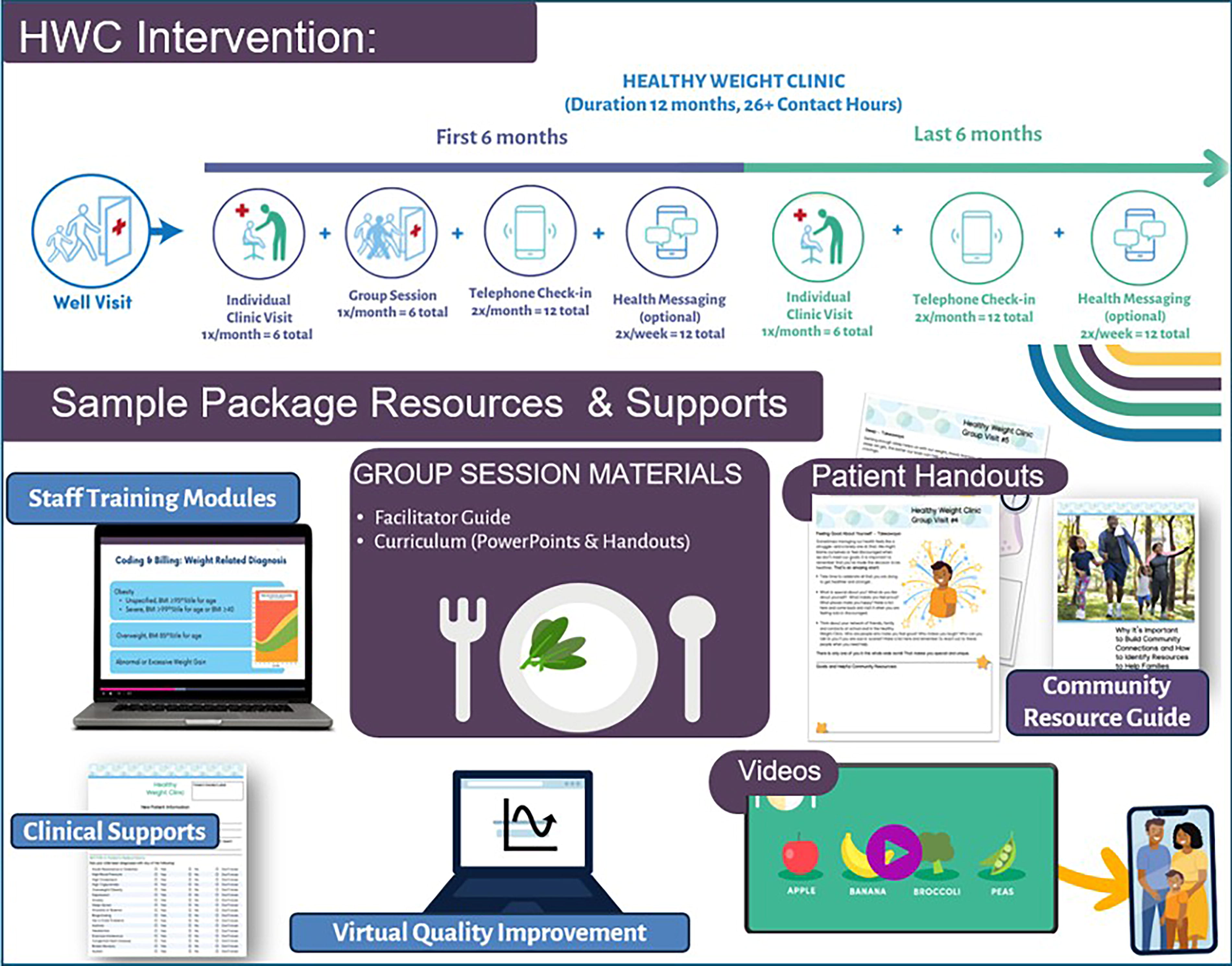
Healthy Weight Clinic package.
Evaluation Approach
The research team modified the Implementation Research Logic Model 12 to outline key elements of implementation and evaluation using both quantitative and qualitative approaches. Analysis was informed by Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) 13 outcomes and the updated Consolidated Framework for Implementation Research (CFIR). 14
Evaluation measures and timepoints are given in Table 1. Quantitative surveys and qualitative interviews were conducted with multidisciplinary personnel at the implementation sites in addition to a trial with HWC patients. These activities, along with monitoring utilization of HWC resources and ongoing technical assistance and structured QI, formed the basis of our sequential, explanatory, mixed methods design of the evaluation. 34 Reach was the number of enrolled trial participants, among those referred to the study. Effectiveness was captured by outlined outcomes below with our primary outcome being change in BMI, BMI z-score, percentage of the median, and %BMIp95 per year.
RE-AIM Outcomes, Data Sources, and Timepoints of Measurement
EHR, electronic health record; RE-AIM, Reach, Effectiveness, Adoption, Implementation, Maintenance; SDOH, Social Determinants of Health; SNAP, Supplemental Nutrition Assistance Program.
Caregiver Surveys and Child Electronic Health Record (EHR) Data (Effectiveness)
Inclusion criteria included: (1) child 2–18 years, (2) BMI ≥85th percentile, (3) caregiver English or Spanish speaking, and (4) child received care at one of the participating sites. Siblings were enrolled. Exclusion criteria included: (1) families planned to leave the health center in the next year or (2) child with chronic, growth interfering medical condition (i.e., congenital heart disease and inflammatory bowel disease), or antipsychotic medication. Referrals were made from August 2021 to August 2022; EHR data collection ended in December 2023. Children were referred to the study by their primary care provider. After referral, research assistants called caregivers to confirm eligibility, obtain verbal consent and complete a survey, and offered a $25 gift card for completing the baseline, 6-month, and 12-month surveys. The TREND flow diagram is in Supplementary Figure S1. This trial was registered on clinicaltrials.gov (NCT05020314).
Children with BMI ≥95th percentile at the health care organizations who were not enrolled and did not attend the HWC served as the comparison group. All BMI data from children aged 2–18 years were obtained from August 2019 through December 2023, matching the intervention participants’ timeline. As 91% of HWC participants displayed a BMI ≥95th percentile, this was selected as the criteria for the comparison group.
Primary effectiveness outcomes included change in BMI, BMI z-score, percentage of the median, and %BMIp95 per year calculated based on the CDC extended growth curves, within group and compared with the comparison group. 35 Linear mixed-effects models were used to evaluate differences in changes of BMI outcomes over time. To assess changes per year during the intervention period in the various BMI measures, a post-intervention time indicator was used as the primary predictor for within group analysis. In between group comparisons, an interaction term between post-intervention time indicator and group was included to assess differential change in outcomes between groups. Models also included fixed effects for sites, baseline BMI, race/ethnicity, and time since start of data collection in years to adjust for potential confounding. Models for BMI were additionally adjusted for child age and sex. The models used random effects to account for clustering of observations within individuals, who were nested within families and sites. Within-group analyses also included an intention to treat analysis for children enrolled in the intervention with BMI measurements at follow-up (n = 165, 86%). The MIXED procedure in SAS 9.4 (SAS Institute, Cary NC) was used to fit mixed linear regression models with random intercepts and slopes.
Secondary effectiveness outcomes included changes in child sleep, 25 screen time, 25 physical activity, 24 sugary beverage, fruit and vegetable intake,19B20 -23 binge eating symptoms, 17 obesity-related quality of life, 15 parental stress, 18 and food insecurity 26 and were reported at baseline, 6, and 12 months by the caregiver. Categorical questions were converted into numeric results for sugary beverage intake, fruit and vegetable intake, parental stress score, family-centered care, and satisfaction scores. For the outcomes that were asked with multiple questions, each question was first converted into a numeric value and then the sum or average of those questions was calculated as the final score. Mixed linear models were utilized for behavioral outcome changes and were adjusted for baseline BMI, child age, sex, and race/ethnicity. A random intercept was specified at the individual level, nested within family and site. There was no significant difference in baseline outcomes between those with 6-month (or 12-month) data vs. those without.
Training and QI Data (Adoption and Implementation)
Adoption was assessed at baseline by asking personnel if they participated in baseline HWC training, and how satisfied and prepared they felt to deliver the intervention.
Implementation from the provider perspective was captured with fidelity assessment: progress was documented at multiple timepoints through sources such as clinical measures/run charts and accompanying Plan Do Study Act (PDSA) forms/progress reports, as well as the Key Resources and Monitoring System Survey, which were integrated into regular PDSA forms/progress reports at baseline and each phase completion. Scheduled webinars were recorded and annotated by staff. Structured QI included regular training/TA calls, team, and individual level support for the utilization of the overall HWC package resources; information collected throughout is presented in Supplementary Figure S2 and in Results section Adoption and Fidelity.
Caregivers (Implementation)
Implementation was also assessed via patient engagement with the HWC, caregiver report of attendance modality (in-person, hybrid, and virtual), and satisfaction, as measured by a modified 8-item family-centered care assessment 36 and customer satisfaction scale, 37 assessed at 12 months. Caregivers were asked to report total HWC out of pocket costs over the past 12 months to inform sustainability. 38
Health Center Multidisciplinary Personnel Surveys (Implementation)
All HWC personnel (pediatric medical providers, community health workers, and nutritionist/dietitians) and administrative staff received invitations to complete post-training implementation surveys at baseline, 12 months, and 18 months. Surveys were 10–30 minutes in length, conducted from August 2021 to November 2023, and administered via a secure Research Electronic Data Capture link. Survey participants at baseline (n = 20) included eight medical providers, six community health workers, four dietitian/nutritionists, and two administrative leaders (Supplementary Table S1).
Implementation was measured by a 4-item Implementation Leadership Scale (ILS) 27 and 12-item Implementation Climate Scale (ICS) 29 at three time points and the 8-item Organization Readiness to Change Beliefs Scale (ORCBS) 30 at two time points, adapted for pragmatic use. 28 Acceptability, feasibility, and appropriateness 31 of the HWC package were assessed through 12 items (4 items per construct) at two time points. All questions were asked on a 5-point scale.
Health Center Multidisciplinary Personnel Interviews (Implementation)
Interview invitations were emailed to 30 HWC staff and administrators; 21 agreed to participate. Semistructured interviews were conducted at least 12 months following the implementation start date (Supplementary Table S2). The interview guide consisted of questions adapted from the CFIR interview guide 39 and RE-AIM framework40B41 -43 with overarching questions mapping to RE-AIM and follow-up questions and probes mapping to CFIR. Two researchers (IC and CR) conducted the interviews by audio-only Zoom. Verbal informed consent was obtained. Interviews were ∼45 minutes and participants were given $75. Audio was transcribed (Landmark Associates) and uploaded into NVivo QRS 14.0 for directed content analysis using the CFIR framework. Two researchers (IC and CR) independently coded transcripts and double-coded a random subset (24%) to ensure alignment with CFIR constructs and contextual relevance, reaching full consensus. Remaining transcripts were coded after establishing intercoder reliability. Themes were identified through iterative team discussions, with saturation guiding analysis. Emergent themes were incorporated, and illustrative quotes selected (Table 2).
Qualitative Themes and Representative Quotes Organized by CFIR Domain, Barriers, and Facilitators to Implementation
CFIR, Consolidated Framework for Implementation Research; CHW, Community Health Worker; FQHC, Federally Qualified Health Center; HWC, Healthy Weight Clinic; MA, Massachusetts; MS, Mississippi; RD, Registered Dietitian.
Maintenance and Sustainability
Maintenance was assessed by six subscales of the 21-item Clinical Sustainability Assessment Tool (CSAT) Short Form 44 at two time points, using an 8-point scale. Mean scores for each scale and subscale, and at each timepoint, were calculated.
Results (Grouped by RE-AIM Constructs)
Reach
There were 191 children enrolled in the trial (65% of the n = 295 referred). At baseline, children were a mean 10.78 ± 3.46 years of age, 44.5% identified as Hispanic/Latino, 52.9% Black, and 91% had a BMI ≥95th percentile (Table 3).
Baseline Characteristics of Healthy Weight Clinic Child Participants and Comparison Participants of the Effectiveness Trial
BMI, Body Mass Index; CHW, Community Health Worker; FQHC, Federally Qualified Health Center; HWC, Healthy Weight Clinic; MA, Massachusetts; MS, Mississippi; RD, Registered Dietitian; SD, standard deviation.
Effectiveness
In the fully adjusted model, HWC participants’ BMI decreased by −0.28 kg/m2 (95% confidence interval [CI]: −0.49, −0.06), percentage of the median decreased by −1.91 (95% CI: −3.13, −0.68), and %BMIp95 decreased by −1.06 (95% CI: −1.98, −0.14) per year compared with the comparison children. There was no significant difference in BMI z-score when compared with the comparison children (Table 4).
BMI Outcome Trend per Year at Postintervention Among Study Healthy Weight Clinic Participants and Comparison Group of the Effectiveness Trial
Random effects to account for clustering of observations within individuals, who were nested within families and sites. Models were adjusted for health organization, baseline BMI, time in years from data collection start date (8/2019), and race/ethnicity. Models for BMI were additionally adjusted for child age and sex. Bold denotes p < 0.05.
BMI, Body Mass Index; CI, confidence interval; HWC, Healthy Weight Clinic.
Secondary outcomes are reported in Table 5. Among children with clinical or subclinical binge eating disorder at baseline, there was a significant decrease from baseline to six months (b = −2.49; 95% CI: −3.68, −1.29) and 12 months (b = −2.65; 95% CI: −3.79, −1.51). There was a significant increase in obesity-specific health-related quality of life from baseline to 6 months (b = 3.74; 95% CI: 1.87, 5.62) and 12 months (b = 2.02; 95% CI: 0.25, 3.80). There was an increase in daily servings of fruits and vegetables (b = 0.30; 95% CI: 0.04, 0.57) from baseline to 12 months. There was a decrease in screen time (b = −1.04; 95% CI: −1.76, −0.31) from baseline to 6 months that was not sustained at 12 months. There were no significant differences in child sleep, sugary drink intake, physical activity, parental stress, or food insecurity at 12 months.
Healthy Weight Clinic Effectiveness Trial Survey Outcomes: 0–6 Months and 0–12 Months Adjusted Change
Missingness in baseline data: n = 3 missing BED score, n = 4 missing SSB intake, n = 4 missing physical activity hours, n = 6 missing fruit and vegetable intake.
Random effects to account for clustering of observations within individuals, who were nested within families and sites. Models were adjusted for health organization, baseline BMI, child age, gender, and race/ethnicity. Restricted to children with a baseline BED score of 8 or above (n = 78).
Restricted to participants who reported parental stress at baseline (n = 161).
CI, confidence interval; HWC, Healthy Weight Clinic; SD, standard deviation.Bold denotes p < 0.05.
Adoption
All eight sites conducted group and individual visits. Five sites struggled to hire and fully integrate the registered dietitian into the clinic. All 100% (18/18) health center personnel reported participating in baseline training related to the project, 79% (15/19) of surveyed were satisfied with the training, and 68% (13/19) reported feeling very or extremely prepared for their HWC work. From the package, 11 unique resources were identified as valuable. The resources most frequently identified (≥3 teams) were the HWC Recruitment Material, Handouts, Clinic Visit Intake Forms, Patient and Parent Educational Videos, Algorithm, and the Group Session Curriculum Guide.
Implementation
ORCBS and ICS scores declined or remained stable through 12 months, whereas ILS scores remained stable initially and showed an increase at 18 months, suggesting delayed improvements in implementation support. Feasibility, acceptability, and appropriateness of the intervention scales demonstrated upward trends, indicating consistent progress in perceived implementation. Health center staff survey results (baseline, 12, and 18 months) are summarized in Supplementary Table S3.
At 12 months, among caregiver survey respondents (n = 153), 89% reported attending a HWC visit—52% in-person only, 27% both in-person and virtually, and 21% virtually only. At 12 months, caregivers reported satisfaction with the HWC, including a mean satisfaction score of 4.44 (standard deviation [SD]: 0.79) and an average family-centered care score of 4.35 (SD: 0.84), with scores of 5 indicating greatest satisfaction.
Three of the four health organizations completed the structured QI. By the end of the QI, most teams were implementing or sustaining most resources/systems related to tracking HWC participation, monitoring no shows/sending reminders, monitoring HWC visit quality/coordinating care, and supporting key community partnerships (Supplementary Fig. S2).
Interview findings yielded six key themes, grouped by CFIR domains (see Table 2).
Maintenance/Sustainability
The CSAT subscales (Supplementary Table S3) showed increases from 12 to 18 months in engaged stakeholders and workflow integration. Several CSAT domains decreased, including engaged staff and leadership, implementation and training, monitoring and evaluation, and outcomes effectiveness. At 12 and 18 months, 50% or more of staff members reported the likelihood of sustainment over 2 years as very or extremely likely.
Caregivers reported a low out of pocket cost of the clinic, with 99% reporting that the intervention cost their family <$250 over the 12 months.
Discussion
In this Type III hybrid effectiveness trial, we demonstrated that the packaged HWC supported successful implementation of the HWC across eight health centers, reaching 191 children from diverse communities. The RE-AIM framework provided a systematic approach to evaluating multilevel outcomes in this pediatric weight management intervention, supporting a comprehensive assessment. The HWC was effective at reducing BMI compared with comparisons and showed improvements in healthy lifestyle behaviors, binge eating, and obesity-related quality of life. Mixed methods implementation showed positive trends, although staffing challenges (i.e., the dietitian/nutritionist role) persisted. Evidence of maintenance and sustainability was observed in seven of the health centers at 18 months post-training. Qualitative themes identified best practices and barriers informing the final HWC package, now in six new health centers and five additional states.
Implementation leadership support scores mirrored previous studies showing limited change. 45 The decline in organizational readiness is consistent with Rafferty et al., 46 potentially reflecting waning optimism due to structural and systemic challenges (e.g., IT and COVID-19). 47 Leadership engagement may bolster readiness in future obesity initiatives. 45
Implementation climate data showed declines in focus on and openness to evidence-based practice, highlighting opportunities to enhance communication and fidelity. 48 Despite declines, sustainability data showed stronger stakeholder engagement and workflow integration. Perceived acceptability, appropriateness, and feasibility increased over time, likely due to context-specific adaptations.
Qualitative findings echoed prior research stressing community partnerships, supportive environments, leadership, and cross-sector collaboration. 49 Themes aligned with earlier interviews, underscoring adaptable, evidence-based case, multidisciplinary models, and persistent challenges around social drivers of health and pandemic-related disruptions. 50
Our primary effectiveness findings align with prior HWC evaluations,4,5 demonstrating modest but significant BMI reductions within group compared with the comparison group. The reduction in %BMIp95 is similar to results from other intensive, multidisciplinary interventions such as the Bright Bodies program, which demonstrated modest reductions in BMI and %BMIp95 over 12 months. 51 The lack of significant change in BMI z-score compared with the comparison group could reflect limitations of z-score sensitivity at higher BMI percentiles, 52 underscoring the value of reporting on multiple BMI metrics in similar trials.
Secondary outcomes showed mixed findings. Binge eating symptoms improved, consistent with previous HWC studies 3 and similar trials.53-55 Improvements in obesity-related quality of life were also consistent with earlier HWC implementations. 5 Screen time decreased at 6 months but not at 12 months, suggesting potential dose-response effects tied to intervention intensity.
Although earlier HWC implementations saw reductions in parental stress, 6 baseline stress levels may have been elevated due to the pandemic, potentially masking effects. It is worth exploring how the pandemic impacted sleep and physical activity given lockdowns and access to school.
Strengths and Limitations
Strengths include a comparison group, diverse settings, and staff perspectives over multiple timepoints, enhancing our understanding of implementation over time. Limitations include staff turnover and small sample sizes limiting the power to detect statistical differences in implementation surveys. Secondary outcomes were only analyzed within person among intervention participants, without a comparison. Additionally, pandemic-related disruptions and site-level variation in staffing and infrastructure may have influenced implementation fidelity and outcomes.
While RE-AIM and our QI and TA efforts offered structure, fidelity and long-term maintenance were difficult to capture as precisely as on-site monitoring; however, this technique is helpful as we move to national dissemination and remote models for QI and TA as we did in this study.
Conclusions
This study informed the final HWC package and implementation supports (TA and QI) to facilitate spread and adoption of the HWC more broadly. Findings demonstrate that an evidence-based, scalable FHWP program using IHBLT can be effectively adopted and sustained in diverse settings. The HWC is a promising model to meet the urgent need for childhood obesity treatment in primary care.
Impact Statement
This study advances the field of childhood obesity by addressing critical gaps in intervention strategies. Findings support the effectiveness and feasibility of implementation of Family Healthy Weight Programs that deliver Intensive Health Behavior and Lifestyle Treatment, informing scalable, equitable models that align with best practices in implementation science.
Footnotes
Acknowledgments
The authors would like to thank our clinical partners at Holyoke Health Center, Delta Health Center, Aaron E Henry Health Center, and Mass General Brigham for Children, as well as all research participants and families.
Authors’ Contributions
I.C. and C.F.R.: Formal analysis; data curation; writing original draft; and writing—review and editing. M.L.: Formal analysis and data curation. J.D.S.: Methodology and writing—review and editing. M.E.P.: Conceptualization; writing—review and editing; and project administration. J.L.: Writing—review and editing and formal analysis. J.L.: Writing—review and editing. J.S.: Writing—review and editing and visualization. V.B.: Conceptualization and writing—review and editing. B.R., S.M., A.A.B., Y.C., and G.C.-S.: Writing—review and editing. E.M.T.: Conceptualization; writing—review and editing; and funding acquisition. L.F.: Conceptualization; writing—review and editing; and funding acquisition.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This publication was supported by the Centers for Disease Control and Prevention of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award (U18DP006424). Dr. Taveras was supported by grant number K24HL159680 from the National Heart, Lung, and Blood Institute.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.