
Abstract
Background:
This study leveraged a novel Missouri Medicaid (MOHealthNet) benefit to adapt and implement evidence-based family-based behavioral treatment (FBT) within health care settings in alignment with policy requirements.
Methods:
In a nonrandomized matched-comparison trial, 108 parent–child dyads participated in FBT, and 92 dyads attended at least one session. Licensed Clinical Social Workers or Registered Dietitian Nutritionists offered 26–33 FBT hours delivered virtually over 6–12 months to Medicaid-insured patients in an urban and rural pediatric health system in Missouri. The matched-comparison group included 186 participants. The Reach, Effectiveness, Adoption, Implementation, and Maintenance framework (RE-AIM) framework was used to evaluate effectiveness (primary) and reach (secondary) and explore adoption, implementation, and maintenance.
Results:
Children in the FBT group reduced their percent over median body mass index (BMI) compared with the matched comparison group (mean reduction: −3.9 ± 1.4, d = −0.42). Within the FBT group, participants also demonstrated improvements in coping with teasing, health-related quality of life, and family health habits (all p < 0.05). Families rated the program as highly acceptable. Reach data indicated enrolled patients had similar BMI, sex, and ethnic backgrounds compared with eligible but non-enrolled patients (ps > 0.301).
Conclusions:
Data demonstrate the feasibility of adopting and implementing FBT within health care systems and inform efforts to support maintenance. FBT reached a diverse population of families receiving Medicaid in pediatric primary care settings and was associated with greater improvements in youth weight outcomes compared with a matched comparison group. Adaptations made to align with the benefit may have reduced the magnitude of effects; however, this policy provides an opportunity to deliver FBT within primary care settings and expand access.
Introduction
Childhood and adolescence are critical periods for obesity development, necessitating interventions that equip children with skills to regulate their weight before adulthood. 1 Effective dissemination and implementation of efficacious treatments for children and families struggling with obesity are essential. Family-based behavioral treatment (FBT) is a multicomponent, evidence-based, cost-effective approach compared with individually delivered treatment 2 that is associated with significant positive changes in children and parents. FBT has been proven effective in reducing child weight in the short- and long-term by addressing dietary intake, physical activity, behavioral skills, positive parenting strategies, and fostering supportive family and peer environments.3–5
FBT aligns with the American Academy of Pediatrics (AAP) Clinical Practice Guidelines 1 and the United States Preventive Services Task Force (USPSTF) 6 recommendations that children with obesity be offered intensive multicomponent behavioral interventions to achieve body mass index (BMI) reductions. 7 BMI changes are associated with improvements in blood pressure, triglycerides, cholesterol, and insulin sensitivity, typically elevated due to childhood obesity.8–10 FBT also yields improvements in psychological well-being and health-related quality of life. 11
The availability of FBT has generally been low outside of regional Children’s Hospital-based health systems, largely due to costs for providing FBT and lack of insurance coverage. 12 In September 2021, MOHealthNet activated the Biopsychosocial Treatment of Obesity benefit, which covers intensive behavioral treatment and medical nutrition therapy (MNT). 13 This created a critical need for capacity building among health care systems in the state to provide FBT within primary care. For the current study, we adapted standard FBT, which is typically delivered through separate parent and child groups with individual sessions, to align with the MOHealthNet benefit, which specifies combined parent–child groups and fewer individual sessions. This study evaluated the adapted model in the medical home, leveraging available coverage to implement a more policy-aligned version of FBT. The primary study aim was to evaluate the effectiveness, and the secondary aim was to evaluate the reach of implementing FBT in accordance with the Medicaid benefit. Information on adoption, implementation, and maintenance was explored using the RE-AIM framework to further inform the feasibility of this adaptation for the policy benefit.14,15
Materials and Methods
Study Design and Setting
This study used a Type 1 hybrid effectiveness-implementation design to pilot the adapted FBT. 16 FBT was delivered in two health care systems serving large populations of low-income families with Medicaid insurance. 17 Partnerships were established through a statewide health coalition. Sites were selected to reflect diverse implementation contexts, including a large metropolitan system already providing FBT that sought to expand reach under the new Medicaid benefit, and a rural system without prior FBT experience that sought to implement FBT for the first time under the same benefit. This approach allowed evaluation of the adapted, Medicaid-aligned model across settings with differing baseline capacity and experience. 18 The study used a nonrandomized design with a matched comparison group extracted from the electronic health record (EHR).
Participants and Recruitment
A total of 108 children were recruited into the study. Eligibility criteria were designed to be policy-aligned and included children aged 5–12 years with a BMI ≥ 95th percentile.19,20 Eligible participants were enrolled in MOHealthNet, were comfortable speaking English, had cellular service access and data, attended a primary care visit at a participating site during the study period, and lived with the participating parent/caregiver >50% of the time. Exclusion criteria included family living or planning to move over 1 hour from the clinical practice, child being a ward of the state, and child exhibiting purging behaviors. The Washington University in St. Louis Institutional Review Board approved procedures, previously published in detail.17,21 Parents provided written informed consent and permission, and children provided written or verbal assent.
Patients were recruited into the study via referral by a primary care provider (N = 54) or through outreach from the site interventionists or staff. For patients who were eligible but did not receive a referral, interventionists/staff mailed a letter about the study, followed by a phone call to offer enrollment. Additional recruitment strategies included mailed postcards, a website, and flyers posted in clinics.
Treatment Program
The study included capacity building 22 among the health care settings to identify, refer, recruit, and enroll patients; to deliver FBT; and to collect study measurements. Interventionists (behavioral health providers and registered dietitians, referred to as “coaches” in interactions with families) were identified within each health system to deliver the intervention to enrolled patients. At the rural site, the interventionist (N = 1) was an existing behavioral health provider who was colocated within one of the participating clinics, while at the urban site, the interventionists (N = 1–2 at a given time) were new staff members but were not colocated within the clinics. The interventionists were trained in FBT and received ongoing supervision, including weekly individual supervision with expert study staff. They were trained to use the EHR to identify patients and send an EHR alert each week to the primary care provider to flag eligible patients. The study team used workshops, check-in meetings, a bulleted referral guide, and a patient handout to train and encourage providers to refer.
An evidence-based FBT package was adapted to meet the Medicaid benefit’s billing structure, which supports a predominantly group format for delivery of the intervention in the initial 6 months. Along with the long history of research supporting FBT in specialty settings,3–5 three recently completed randomized clinical trials have found that FBT for childhood overweight and obesity could be successfully implemented in pediatric primary care settings.3,14,23 Adaptations are reported in detail using the Framework for Reporting Adaptations and Modifications-Enhanced. 24 Adaptations included changes to intervention format to align with Medicaid billing requirements, such as combined parent–child groups and fewer individual sessions (Fig. 1).
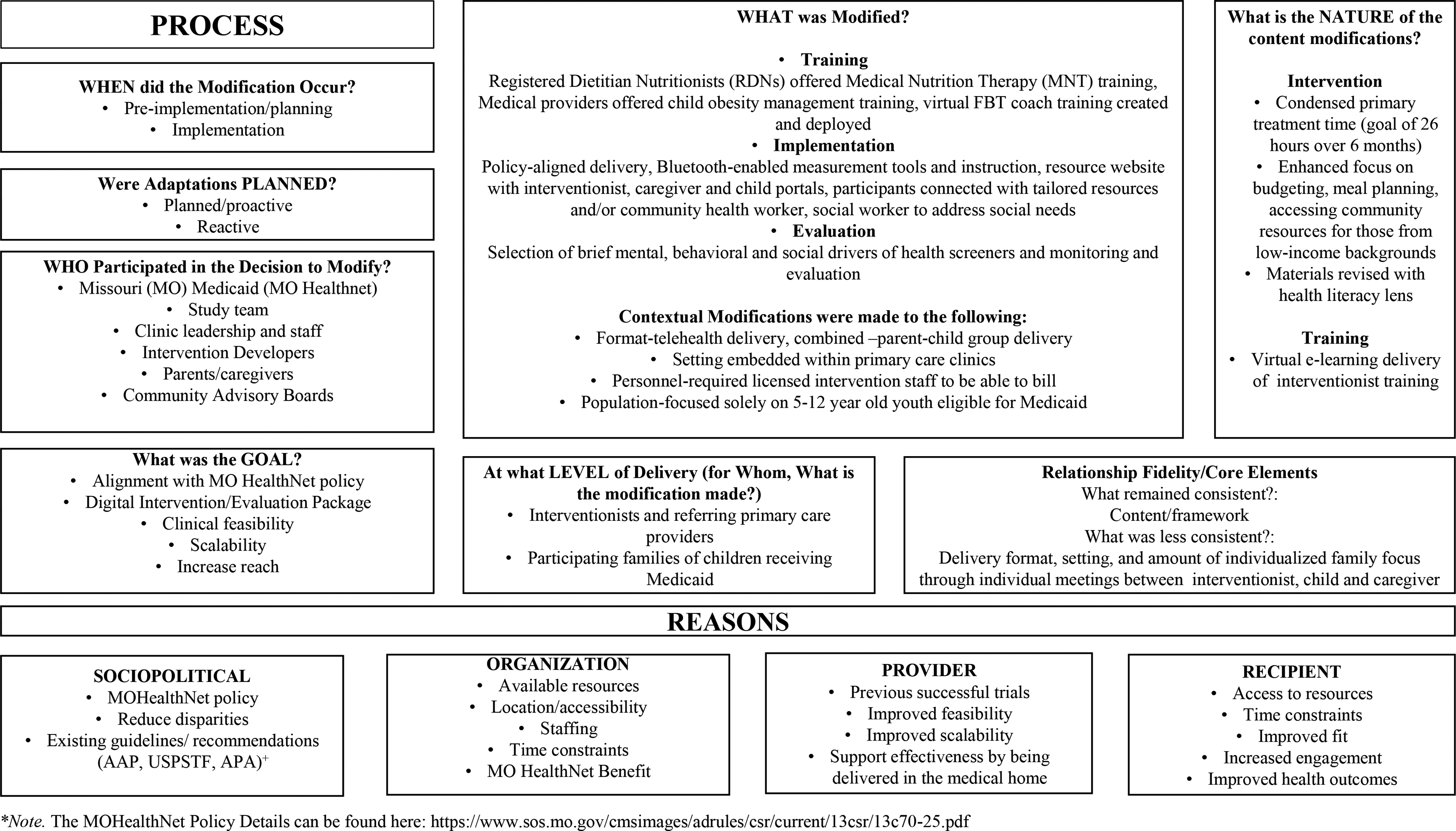
FRAME Adaptations to FBT to Improve Fit with the MOHealthNet Medicaid Benefit*. *Adapted from the FRAME (Wiltsey Stirman et al, 2019); +AAP, American Academy of Pediatrics; USPSTF, United States Preventive Services Task Force; APA, American Psychological Association; FBT, family-based behavioral treatment; FRAME, Framework for Reporting Adaptations and Modifications—Expanded.
A digital FBT provider training and participant resource platform was developed by the study team in collaboration with 3C Institute, Durham, NC. The platform provided training for interventionists and gave participants direct access to program support resources aligned with the focus of FBT. An interventionist portal hosted all program materials needed to guide treatment sessions and support families in areas such as positive parenting, food choices, and social facilitation.
Following completion of the digital FBT training, interventionists completed live virtual simulations and certification evaluations with the training team. FBT-trained supervisors provided ongoing supervision and virtual monitoring of interventionist treatment delivery and consultation on group-based delivery of intervention. Core components of FBT include: (1) the Traffic Light Eating Plan, which uses color-coding to guide increased intake of high-nutrient, low-energy-dense foods (GREEN) and reduced intake of low-nutrient, high-energy-dense foods (RED); (2) the Traffic Light Activity Plan, which promotes increased physical activity (GREEN) and reduced sedentary behavior (RED); (3) parenting strategies (e.g., modeling, reinforcement, environment shaping, limit setting, and routines); (4) behavioral strategies (e.g., self-monitoring, stimulus control, goal setting, and problem solving); and (5) social facilitation, a socioecological approach that supports parents in building positive family and peer environments and helps children develop skills to manage negative social interactions and engage in healthier alternatives. 25 Social drivers of health were also assessed to support engagement in treatment.
While designed to be delivered in-person, this treatment was adapted for telehealth, a modality offered through the MOHealthNet policy with demonstrated success in other FBT trials. 3 Most participants began treatment within 2 weeks of consent and baseline measurements. The initial phase involved one to two individual FBT sessions for each child, followed by placement into a group with other families for 15 weekly group sessions, each lasting 90 minutes. Additionally, families were eligible for eight additional 30-minute individual sessions throughout the 6-month period. To align with the benefit, which supports multidisciplinary care, families were encouraged to meet for an initial MNT assessment (45 minutes) and two follow-up MNT sessions (30 minutes each) with a registered dietitian nutritionist (RDN; Fig. 2, Table 1). These MNT sessions helped provide additional nutrition interventions catered to the child’s specific needs and helped empower families to make individualized nutrition changes. The RDN shared visit findings and goals with the FBT interventionist, who then utilized this information in individual and group FBT sessions with the family. Follow-up measurements were collected at month 12.

Family-Based Approach for Healthy Lifestyles (RYSE) FBT Program Timeline. Green squares indicate RD/MNT visit (registered dietitian/medical nutrition therapy visit), which is part of the benefit but is provided by a registered dietitian nutritionist (RDN) and is billed differently than FBT sessions. Check-ins at 3, 6, and 12 months are research visits. RDNs can deliver group FBT and MNT. LCSWs can deliver group and individual FBT sessions. MNT, medical nutrition therapy.
Individual and Group Participant Session Descriptions
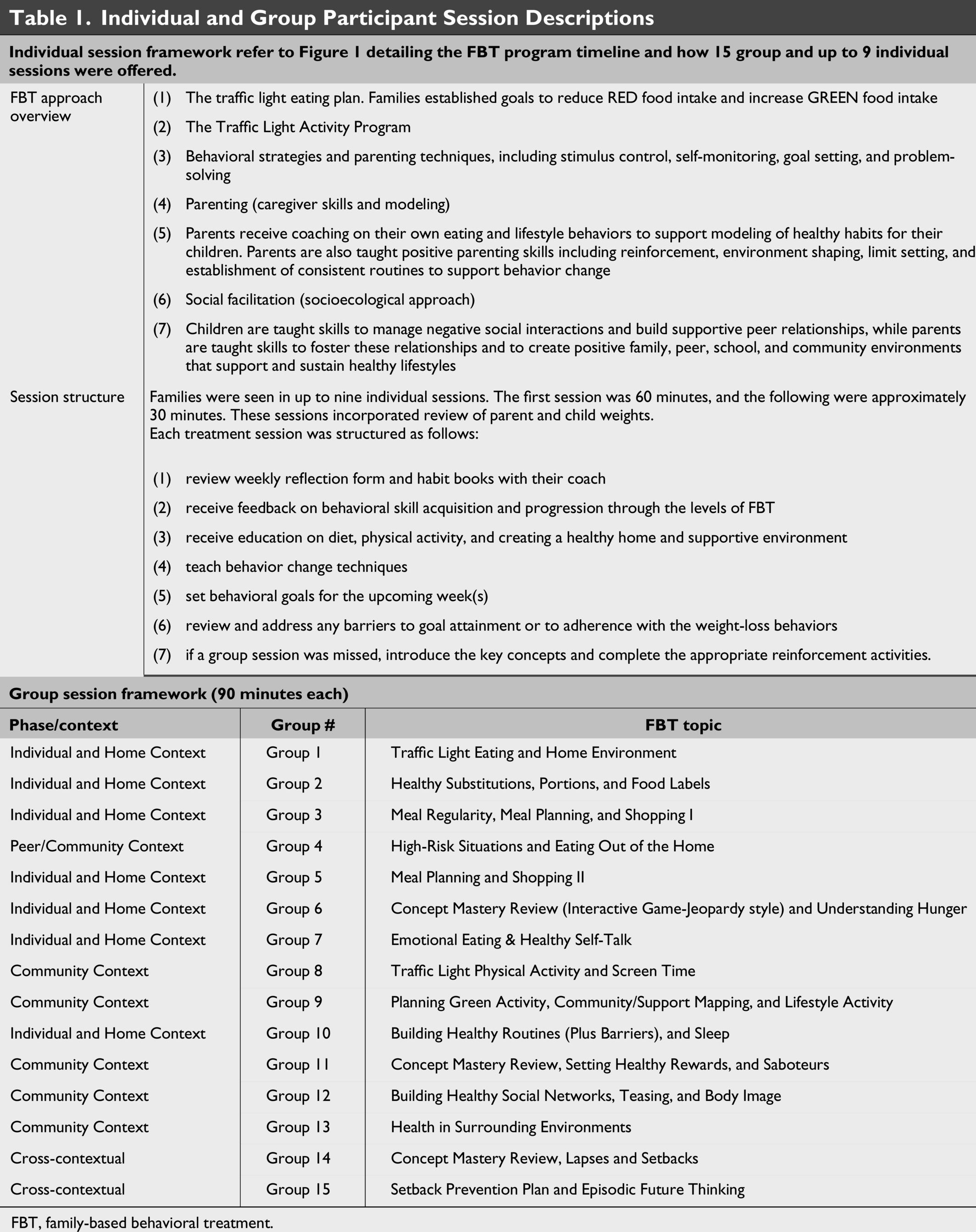
FBT, family-based behavioral treatment.
Group sessions typically began with a review of families’ prior week’s goals and progress on weight change, including review of dietary intake and physical activity self-monitoring and linkage of weight changes to energy-balance behaviors, followed by a brief psychoeducational topic, interactive skill-building and problem-solving (e.g., role plays, applied strategies, parent–child activities to reinforce key skills, strategies to enhance family and peer support, and in-session physical activity), and concluded with goal setting. This group-based delivery format was adapted from standard evidence-based FBT to align with the MOHealthNet benefit. Parents and children were expected to complete weekly weight measurements and ongoing behavioral monitoring at home. However, the combined parent–child group format and reduced number of individual sessions limited interventionists’ capacity to conduct consistent weekly weight checks and individualized behavioral check-ins. As a result, interventionist-led monitoring was less consistent, reflecting feasibility constraints inherent to group-based delivery rather than intentional modification of core FBT components.
Families participated in individual sessions (in person or via telehealth) lasting approximately 30 minutes. Sessions included measurement of parent and child weight; review of dietary and physical activity self-monitoring; linkage of weight changes to energy-balance behaviors; problem-solving of barriers; and goal setting for the time between sessions. These sessions also incorporated interactive, individualized skill-building tailored to the family using session-specific treatment content (e.g., building social support and modifying the home environment), including observation of parent–child interactions, coaching on effective reinforcement, therapist modeling, and tailored problem-solving for family-specific challenges to support behavior change and sustained focus on treatment goals. Sessions provided individualized feedback and support, emphasizing self-monitoring, adherence to treatment and homework, and behavioral goal setting. Each session included a review of parent and child progress in weight and self-monitoring, with adjustment of behavioral goals based on progress. Behavioral goals included daily calorie targets; reductions in RED foods/drinks and sedentary behavior; increases in GREEN foods and physical activity; self-monitoring; and completion of daily parent–child check-ins. To support fidelity, interventionists used session checklists and a family dashboard to track cumulative behavioral and weight changes and guide treatment delivery. For care coordination, interventionists communicated with the child’s primary care provider at least quarterly regarding patient progress, attendance, and medical concerns.
The initial MOHealthNet benefit provided FBT for 6 months, thus group sessions ceased after this period. However, some individual treatments (22% of all individual sessions) were delivered between months 6 and 12, depending on family circumstances. All group sessions and almost all individual sessions were delivered via HIPAA-compliant Microsoft Teams.
Matched Comparison Group
The historically matched comparison group consisted of patients from geographically proximal, nonparticipating practices. This cohort, obtained from the health systems’ EHRs, was stratified by sex and matched in a 2:1 ratio with the FBT participants based on percent over median BMI ranking. Patients were identified and matched based on their enrollment in MOHealthNet, age, sex, and weight. There was a 22-month window for data collection. For both the FBT participants and the comparison group, the mean time between baseline and 12-month measurements was 1.1 ± 0.2 years.
Measures
The demographic questionnaire assessed household income, parent educational attainment, parent and child sex, parent/child medication use, child age, race, and ethnicity. Items adapted from the 26-item Accountable Health Communities Health-Related Social Needs self-report screening tool were used to measure several social needs, including housing, food, transportation, and financial strain.26,27
Effectiveness
Effectiveness was examined at months 3, 6, and 12 as change in child’s percent over median BMI, 28 or “percent overweight” serving as the primary outcome. Robustness of findings was confirmed on additional BMI metrics (BMI percentile over the 95% [BMIp95], BMI percentile [BMI%ile], BMI z-score [BMIz], and BMI). 29 Height was measured for the child and parent using a wall-mounted stadiometer in the clinic. Weight was measured for the child and parent using a digital scale. 29 BMI was calculated, and the child’s percent over median BMI, BMIp95, BMI%ile, and BMIz were calculated in accordance with the Centers for Disease Control and Prevention extended BMI-for-age growth charts. 28 For secondary effectiveness outcomes, all psychosocial surveys were collected via the secure surveying platform REDCap30,31 and were completed by the participating parent/caregiver or child. Child weight-related quality of life was assessed using the Sizing Them Up 32 (parent-report) measure. Psychosocial functioning was evaluated using the Pediatric Symptom Checklist (parent-report) to screen for symptoms of emotional and behavioral disorders. 33 Ability to cope with teasing was measured using the 6-item problem-focused subscale of the Coping with Teasing Scale (child-report). 34 Family eating and activity habits and household practices were evaluated using the Family Nutrition & Physical Activity Screening Tool (FNPA; parent-report 35 ). The Combined Therapeutic Alliance Scale for Caregivers and Children 36 was used to measure parent and child-report of acceptability of the intervention on a scale of 1 (low acceptability) to 4 (high acceptability). Adverse events were measured using a parent-report change in health history questionnaire. Responses were reviewed by an independent medical monitor every 6 months for adjudication and then shared within 1 week of review with PIs for assessment of relatedness, severity, and categorization.
Analyses
The targeted sample for the FBT arm was based on a review of seven studies 37 demonstrating that those who received FBT experienced an overall change in percent over median BMI of −10.6 ± 15.3 at 24 months. This sample was powered at 96% to detect a reduction in excess weight in children and parents between 6% and 6.5% with the ability to detect between sex differences at 80%. While the final sample does not allow for these sensitivity analyses, power for change in the overall percent over median BMI is retained. 38 Originally, a 1:1 matched comparison was selected with the expectation that there would be more variability in the treatment group. Due to the smaller-than-expected sample size, the original comparison group size was maintained to capture additional variability, thus resulting in a 2:1 ratio to maintain a similar standard deviation estimate. All analyses were completed using Statistical Analysis System v9.4.
Descriptive analyses were utilized to present summary statistics such as means and percentages. Linear and logistic regression were used to compare enrolled and non-enrolled but eligible patients on BMI, age, sex, and race/ethnicity.
For effectiveness analyses, participants with complete baseline data (n = 92) were included. Time was included as a categorical covariate since all participants had equal time between visits, allowing for a nonlinear relationship in changes of the outcome. Models with the matched comparison group used time as a continuous covariate to account for individual differences in time to follow-up. Random effects were used to account for both within-subject correlation over time and site effects.
Secondary analyses were conducted within the FBT group based on available data. High versus low thresholds for FBT session attendance were based on average attendance values in other similar trials. 15 Clinically meaningful changes were considered weight-related changes that have been previously shown to be associated with cardiometabolic improvements (≥5 BMIp95; ≥0.25 BMIz)39–41 or previously shown to be achieved with FBT (≥9% median BMI; ≥1.3 BMI).42,43 Normality of the responses was checked using the Shapiro–Wilk test. Chi-square analyses were used to compare whether those in the lower versus higher attendance groups achieved changes at these clinical magnitudes.
Results
The 108 children enrolled had a mean age = 9.3 years, 54.6% were female, 31.5% were Black, were 35.2% White, and 25.9% were Latino/a. Of these, 92 attended at least one FBT session, and 89 had complete data at 12-month follow-up. Compared with the matched comparison cohort, FBT participants in the analytic sample were slightly older (mean age = 9.0 years vs. 8.5 years, p = 0.02) but similar in percent over median BMI. A sizable portion of FBT participants reported experiencing food insecurity (37.0%) and income volatility (29.3%). See Table 2 for detailed demographic information.
Participant Characteristics and Representativeness in the MO-CORD 3.0 at Baseline
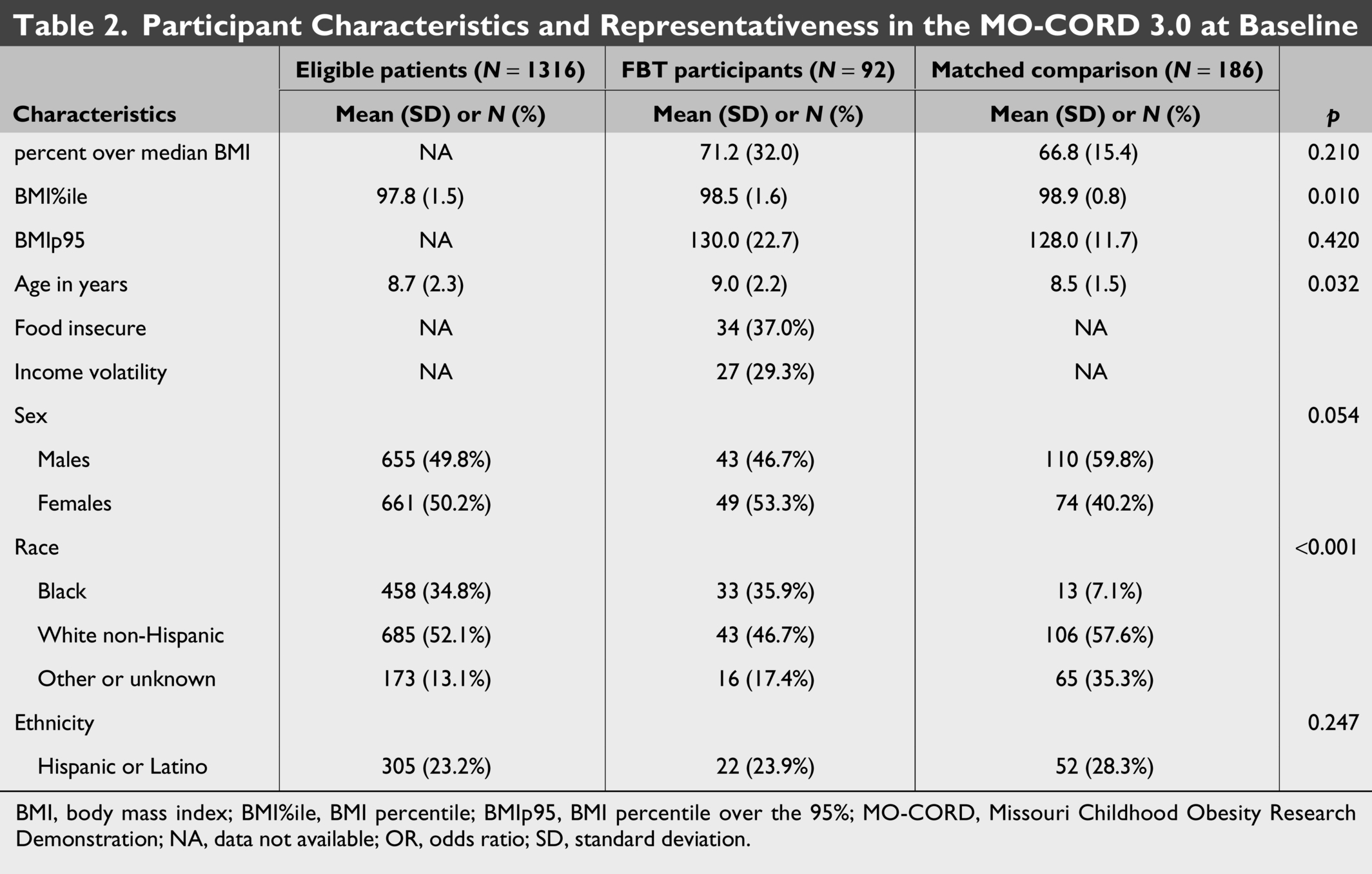
BMI, body mass index; BMI%ile, BMI percentile; BMIp95, BMI percentile over the 95%; MO-CORD, Missouri Childhood Obesity Research Demonstration; NA, data not available; OR, odds ratio; SD, standard deviation.
Reach
The enrolled patients were similar to the entire pool of patients who were eligible but did not enroll (Table 2) with regards to percent over median BMI (p = 0.210), sex (p = 0.054), and ethnic background (p = 0.247), though they were older by 0.3 years (p = 0.032) with differences in self-reported racial background (p < 0.001). Mean number of FBT sessions attended was 10.5 ± 9.2 out of 22 (M = 8.5 ± 5.9 group, M = 4.4 ± 3.9 individual) across participants, with an average total session time of 10.2 ± 4.1 contact hours across the intervention.
Effectiveness
Primary outcomes
At 12 months, children in the FBT group demonstrated a significantly greater reduction in percent over median BMI than the matched comparison group (mean change: −0.8 ± 1.2 vs. 3.1 ± 0.7; p = 0.007; d = 0.42), with an overall mean reduction of −3.9 ± 1.4 in the FBT group. Similar findings were observed for BMIp95, BMI%ile, BMI, and BMIz (Table 3). Sensitivity analyses further indicated a dose–response pattern: children who received a higher dose of FBT (≥17 hours) were more than four times as likely to achieve a clinically meaningful reduction in percent over median BMI as those not enrolled, while those receiving lower doses were more than twice as likely to do so (Supplementary Table S1).
Effectiveness Outcomes—Change Within and Between Groups at 3-, 6-, and 12-Month Timepoints
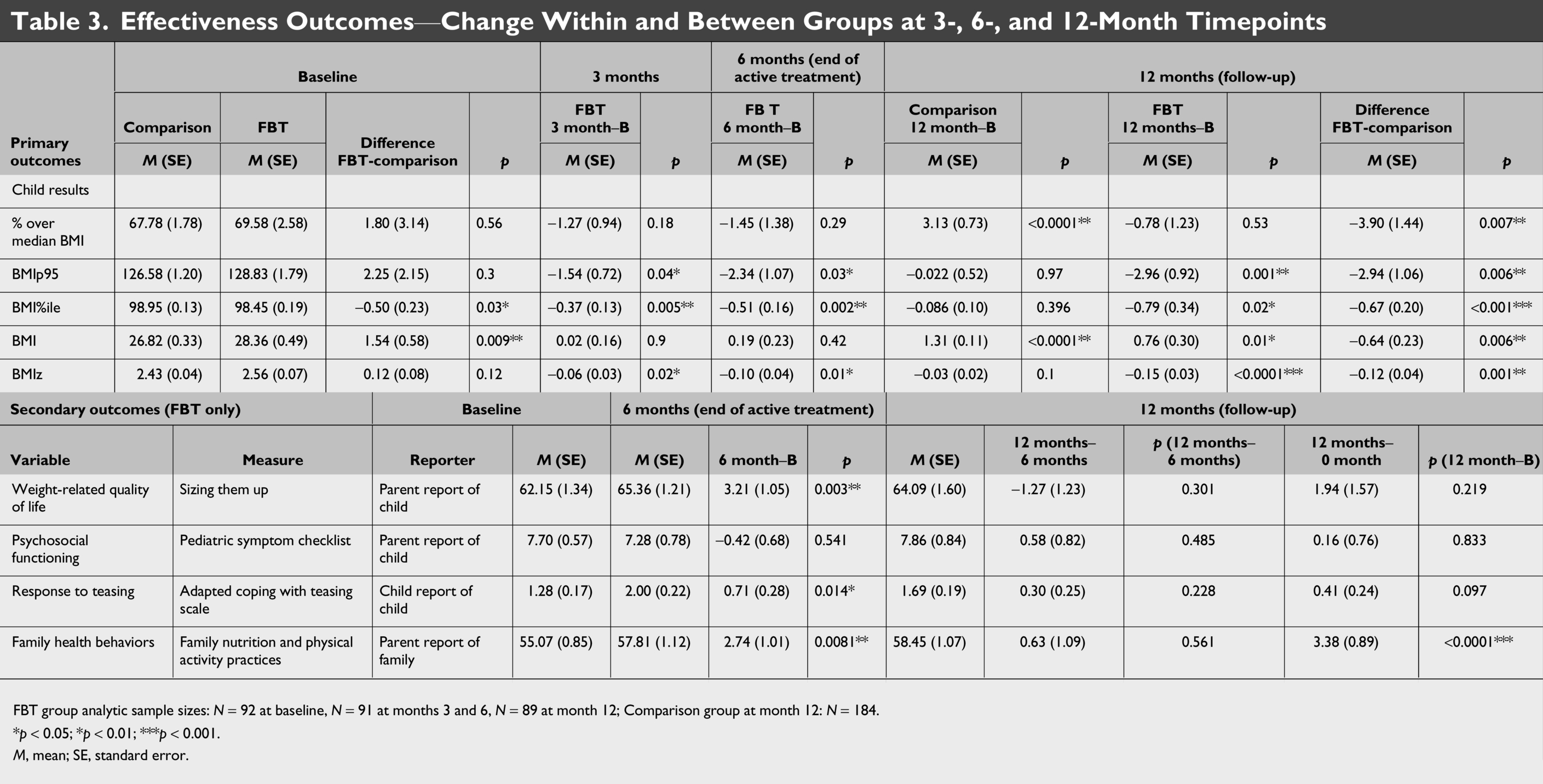
FBT group analytic sample sizes: N = 92 at baseline, N = 91 at months 3 and 6, N = 89 at month 12; Comparison group at month 12: N = 184.
*p < 0.05; *p < 0.01; ***p < 0.001.
M, mean; SE, standard error.
Additional outcomes
Participants demonstrated improvements across the 6-month intervention and maintenance through month 12 for adapted coping with teasing, health-related quality of life, and FNPA activity habits (all p < 0.05, Table 3).
Adoption
Interventionists served a substantial percentage of low-income children. One health care system was primarily urban, and one served a rural catchment area. Fifty-four primary care providers made 161 total referrals, 37 (68.5%) of whom referred ≥1 patient. Enrollment rates were higher among those who were referred (N = 63 of 161, 39.1%) than those recruited by the interventionist/staff (N = 45 of 587, 7.7%).
Families reported that they highly liked their interventionist (child M = 3.6 ± 0.6, parent M = 3.6 ± 0.8; Likert scale 1–4), worked well with the interventionist on solving their problems with a healthy lifestyle (child M = 3.6 ± 0.9, parent M = 3.6 ± 0.7), and felt like their interventionist was on their side and tried to help (child M = 3.5 ± 0.7, parent M = 3.5 ± 0.7; Supplementary Table S2). No adverse events were determined to be related to the study, including any development of disordered eating symptoms.
Maintenance
In both the urban and rural settings, FBT delivery has been successfully maintained, with Medicaid billing procedures fully established and sustained. At the rural site, FBT is primarily delivered in individual sessions, reflecting clinic preferences for scheduling during regular daytime hours and providing families with greater flexibility to participate.
Discussion
This trial evaluated the implementation of FBT, an evidence-based behavioral treatment for childhood obesity, adapted to align with a novel Medicaid benefit and delivered in real-world clinical settings. FBT was significantly superior to the matched comparison group in improving child percent over median BMI, with participants receiving FBT demonstrating reductions in relative weight at 3, 6, and 12 months, whereas those in the matched comparison group showed continued increases across the intervention period. Participants in FBT also demonstrated improvements in psychosocial and behavioral outcomes, including coping with teasing, health-related quality of life, and FNPA habits. The findings suggest that this scalable policy-aligned approach is feasible, highly acceptable, and associated with improvements in child relative weight and family health behaviors.
At the same time, the magnitude of weight change observed in this implementation trial was smaller than that reported in prior efficacy trials of standard FBT. This difference likely reflects adaptations made to align with Medicaid policy requirements, including delivery in combined parent–child groups and fewer weekly individual sessions. Individualized FBT sessions typically allow interventionists to observe parent–child interactions, assess use of positive reinforcement, and provide corrective feedback—elements that were reduced in the adapted model. Standard FBT is typically delivered in separate parent and child groups, an approach associated with stronger outcomes; prior work suggests that mixed-format approaches yield greater improvements in relative weight than group-only approaches, although group-based delivery may offer cost efficiencies.44,45 Together, these findings suggest that adaptations made to align with the Medicaid benefit may support scalability and reach; however, they may reduce treatment potency.
Patients enrolled in FBT were generally representative of the eligible patient population, showing good equity in who was being reached. The focus on the Medicaid population, through the new provision and partnerships with health systems that engage primary care providers in patient referrals, also appears promising for expanding access to FBT. Given the positive impact of provider referrals on enrollment, these partnerships may be an important mechanism for increasing reach. However, because referrals can be challenging to facilitate,46,47 further research is needed to identify strategies that support referral processes while minimizing burden on providers. Future studies might also explore whether referral rates improve over time as providers become more familiar with FBT.
Adoption and implementation success were reflected in each site’s ability to refer, recruit, and enroll patients; deliver the intervention sessions; and maintain attendance and acceptability among families. These findings support the feasibility of training interventionists within health care systems to deliver FBT and bill for these services through Medicaid. Notably, adaptations made to align with the Medicaid benefit resulted in a lower dose, averaging 10 contact hours, primarily in group sessions, compared with the 26 hours recommended by USPSTF. 48 Given that larger effects are observed in interventions providing greater contact hours (≥26), 49 more research is needed to identify strategies to increase the amount of support families receive through this delivery model. Parents reported time constraints as a primary barrier, with some families needing to pause and resume treatment due to external stressors. Offering an individual session format or increasing the proportion of individual sessions relative to group sessions may help address these barriers and better meet families’ needs.
Moreover, standard FBT is designed as an individualized behavioral health treatment; however, adaptations made to align with the Medicaid policy shifted delivery toward a predominantly group-based format, which may have decreased treatment effects. This shift limited individualized attention to changes in weight, energy-balance behaviors, and parenting, a hallmark of standard FBT.3,14,23,50 Policy changes to the Medicaid benefit may help support a higher dose of individual treatment sessions while accommodating the diverse needs of families, as well as extending the 6-month window for completing treatment. Ideally, this treatment session time would include opportunities for child-only and parent-only group sessions, consistent with standard FBT, to maximize effectiveness. Based on feedback from this pilot, MO has revised the policy, with a recent MoHealthNet amendment increasing flexibility and allowing delivery of the intervention over a 12-month period.
While FBT delivery was maintained in both health systems, patient volume decreased from levels observed during the study. At the urban site, the number of interventionists was insufficient to support higher volume, whereas at the rural site, referrals declined following a change in clinic location for the interventionist. Strategies to support the sustainment of FBT may include expanding insurance coverage beyond Medicaid and increasing reimbursement for individual FBT sessions. Greater payer diversity would allow clinics to serve a higher volume of patients eligible for FBT, thereby improving clinic capacity, stabilizing staffing, and supporting financial sustainability. Additionally, allowing interventionists to deliver other reimbursable behavioral health services during daytime hours may further support workforce retention and clinic-level sustainment of FBT.
Study limitations included the necessity of adopting a completely virtual model of delivery, reducing the sample size during COVID-19, and the broader context of pandemic-related increases in child weight. 51 While the virtual/telehealth format reduced the burdens of transportation and childcare and allowed for convenient evening sessions, it may have limited social connectedness among group members. Moreover, participants who volunteered to participate, relative to the matched cohort, may have had unmeasured characteristics that facilitated participation. Similarly, families who had higher attendance may have been more activated at baseline, and their percent over median BMIs may have improved without intervention. However, evidence summarized in the AAP clinical practice guideline indicates that trial participation alone is unlikely to produce meaningful or sustained BMI reductions, suggesting that baseline activation alone does not fully explain the observed improvements. 1 A key strength of the study is its position as the first evaluation of a Medicaid benefit covering obesity treatment for children, supporting the sustainability of the intervention beyond the study period.
Conclusions
This project demonstrated the successful implementation of FBT using a combination of group and individual sessions for families receiving Medicaid services under a novel benefit. Primary care clinics adopted the intervention, supporting multidisciplinary collaboration and expanding access to this evidence-based treatment through provider referrals. A demographically diverse sample of children participating in FBT achieved significantly greater reductions in percent over median BMI and a higher proportion of children achieving clinically meaningful weight outcomes compared with a matched comparison group. Participants in FBT also demonstrated improvements in psychosocial and behavioral outcomes, including coping with teasing, health-related quality of life, and FNPA habits. Families also reported high acceptability of the intervention. As an early evaluation of Medicaid-covered obesity treatment for children, this pilot supports a scalable, sustainable model for service delivery and informs future implementation.
Impact Statement
FBT delivered via telehealth within health care settings under a novel Medicaid benefit improved youth weight outcomes compared with a matched comparison group. Medicaid-funded FBT was feasible and acceptable, and although adaptations made to align with the benefit may have reduced the magnitude of treatment effects, these findings highlight the potential to expand the reach of FBT through health care settings.
Authors’ Contributions
M.L.D.G., A.M.B., A.E.S., L.C.N., J.A.C., S.E.B., L.T.M., S.E.H., and D.E.W. drafted and edited the article. D.E.W., S.E.H., A.E.S., M.L.D.G., L.C.N., R.R.W., R.B., and J.A.C. obtained grant funding, designed the study, executed the project, and conducted study analyses. All coauthors reviewed a final draft of the article and approved the submission.
Footnotes
Acknowledgments
The following individuals and institutions constitute the Missouri Childhood Obesity Research Demonstration (MO CORD) Research Group: (*indicates principal investigator or director): Washington University in St. Louis: Denise E. Wilfley, PhD*, R. Robinson Welch, PhD, Genevieve Davison, PhD, Fanice Thomas, PhD, (Centers for Disease Control and Prevention), Sherri L. Gabbert, PhD, (University of Virginia), Andrea K. Graham, PhD, (Northwestern University), Tina Day, BS, CCRP, Aubrie Hampp, MSc, Anne Claire Grammer, PhD, Lawrence T. Monocello, PhD, (Texas A&M University).Children’s Mercy Kansas City: Sarah E. Hampl, MD*, Meredith Dreyer Gillette, PhD, Jordan A. Carlson, PhD, Helena H. Laroche, MD, Kelsey M. Dean, MA, RD, LD, Sarah Bullard, MS, RD, LD. Pennington Biomedical Research Center: Amanda E. Staiano, PhD, Alyssa M. Button, PhD, Robbie Beyl, PhD, Peyton Murray, MA. Freeman Health System: Paul Petry, DO, Lisa C. Nelson, MA, Sarah Willoughby, LCSW.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was primarily funded by the Centers for Disease Control Childhood Demonstration Research Grant 3.0 (U18DP006425). Research reported in this publication was supported by the Washington University Institute of Clinical and Translational Sciences grant # UL1TR002345 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH); the Pennington Biomedical Research Center grant # U54 GM104940 funded by the NIH National Institute of General Medical Sciences (NIGMS), NORC Center Grant # P30DK072476 titled “Nutrition and Metabolic Health Through the Lifespan” sponsored by the NIH National Institute of Diabetes and Digestive and Kidney Diseases. Lawrence T. Monocello, Genevieve Davison, Anne Claire Grammer, and Fanice Thomas were funded by the T32 Pre- and Postdoctoral Research Fellowship in Washington University in St. Louis Transdisciplinary Pre- and Postdoctoral Training Program in Obesity and Cardiovascular Disease (T32 HL130357; National Heart, Lung, and Blood Institute). The content is solely the responsibility of the authors and does not necessarily represent the official view of the NIH.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.