
Abstract
Therapeutic hypothermia is widely used as a neuroprotective intervention in infants with hypoxic-ischemic encephalopathy (HIE); however, limited data exist regarding the long-term neurodevelopmental outcomes of different cooling strategies. The aim of this study is to compare the long-term neurodevelopmental and cognitive outcomes of combined hypothermia (CH) and whole-body cooling (WBC) treatments in children diagnosed with HIE with each other and with a healthy control group without an HIE diagnosis. This retrospective study included a total of 50 children diagnosed with HIE and treated with cooling therapy, who were followed in the Neonatal Intensive Care Unit of Mersin University between 2015 and 2021. Additionally, a control group was formed from healthy children of a similar age group who attended outpatient clinic checkups between these dates and whose archive records were accessible. We used the Wechsler Intelligence Scale for Children-IV (WISC-IV), the Stroop Test, and the Denver II Developmental Screening Test for neurodevelopmental assessments. Neurodevelopmental outcomes were generally found to be similar between the two groups. However, the Full Scale IQ of the CH group was found to be significantly lower compared to the control group. The groups that underwent cooling treatment showed more abnormalities in the Stroop and Denver tests compared to the control group. Although no significant difference was found between the CH and WBC methods in terms of overall results, weak outcomes in some cognitive subdomains in the CH group were noteworthy. Larger sample sizes and prospective studies are needed.
Introduction
Neonatal encephalopathy is a heterogeneous clinical condition characterized by loss of consciousness, convulsions, respiratory depression, and hypotonia, typically developing in the early neonatal period, usually after the 35th week of gestation. The most important cause is perinatal hypoxic-ischemic encephalopathy (HIE), which is one of the main causes of neonatal deaths and can lead to disabilities in the long term. Its incidence ranges from 2 to 9 per 1000 live births, while in Turkey, it has been determined to be 2.6 per 1000 births (Grubu, 2008).
The pathophysiology of HIE begins with the development of hypoxemia, hypercarbia, and acidosis due to inadequate gas exchange in the placenta or postnatal ventilation disorders. While the cerebral blood flow tries to increase, cerebrovascular autoregulation is disrupted, leading to cerebral damage. Cell death occurs in two stages; the first stage is characterized by energy deficiency, while the second stage is marked by damage that develops after oxygenation (Chalak et al., 2018).
Today, the routinely applied treatment method for moderate or severe HIE is therapeutic hypothermia (TH) (Victor et al., 2022). In some centers, selective head cooling (SHC) is applied, while in others, whole body cooling (WBC) is used. (Abate et al., 2021; Basiri et al., 2021; Gunn and Gluckman, 2007; Shankaran et al., 2005). WBC is easy to use, but there is no clear answer as to which method is best. (Wassink et al., 2019). However, there are significant technical differences between these two cooling therapy strategies. In the WBC method, the body is cooled to maintain a rectal temperature of 33.5 ± 0.5°C. (Azzopardi et al., 2009). In the SHC method, the head is cooled to maintain a rectal temperature of 34.5 ± 0.5°C (Gluckman et al., 2005; Zhou et al., 2010). Since the main cause of disabilities in HIE is brain damage, SHC, where the primary goal of treatment is cooling the brain, appears to be more advantageous. On the contrary, when head cooling is applied to SHC treatment, more pronounced hypothermia occurs in the superficial regions of the brain, while a milder hypothermia occurs in the deeper regions. (Gunn and Gluckman, 2007; Tooley et al., 2005). In this case, while the brain cortex would theoretically be better protected with SHC, the deeper parts of the brain, such as the basal ganglia and thalamus, would not benefit sufficiently from hypothermia. In the WBC method, however, hypothermia occurs to a similar extent in both the superficial and deep parts of the brain (Gunn and Gluckman, 2007; Tooley et al., 2005). Therefore, although WBC does not provide additional benefit for the superficial regions of the brain, it is better for the deep regions. As seen, theoretically, both strategies have their own potentially advantageous aspects. Another important issue to consider is that, although TH is an effective treatment method for HIE, neither SHC nor WBC is sufficiently effective for all patients, and nearly half of the patients either die or continue their lives with significant disabilities. In this case, the SHC and WBC methods have their pros and cons, but neither is sufficiently effective alone. So, can we combine them? In other words, while cooling the head as in the SHC method, can the rectal temperature be maintained at 33.5 ± 0.5°C as in the WBC method? Wouldn’t combined hypothermia (CH) applied in this way be the best cooling method?
According to our knowledge, there is no study in the literature that seeks answers to these questions. In this study, we aimed to find answers to these questions. Subsequently, we induced moderate systemic hypothermia (SH) by cooling the head and compared this method with the traditionally applied SHC or WBC methods.
In this study, we compared the long-term neurodevelopmental and cognitive outcomes of patients who received combined cooling therapy with those of patients who received whole-body cooling (WBC) therapy and with a healthy control group for both groups. We made this comparison by administering the Denver II Developmental Screening Test (DDST) and the Wechsler IV Intelligence Test to the patients.
Materials and Methods
This retrospective cohort study was conducted on newborns diagnosed with HIE who underwent cooling therapy in the Neonatal Intensive Care Unit of Mersin University Faculty of Medicine Hospital between 01.01.2015 and 31.12.2021. The study was conducted by reviewing the archived records of patients diagnosed with HIE according to the Sarnat&Sarnat staging and the American College of Obstetricians and Gynecologists 2004 criteria, who underwent cooling therapy (CH and WBC). In the CH group, the head was cooled to maintain a rectal temperature of 33.5 ± 0.5°C, while in the WBC group, the body was cooled to maintain a rectal temperature of 33.5 ± 0.5°C. Patients whose archival records were fully accessible and who underwent the DDST or the Wechsler Intelligence Scale for Children IV during follow-up were included in the study. Patients with a birth weight of less than 2000 grams, a gestational age of less than 37 weeks, congenital heart disease, multiple congenital anomalies, or congenital metabolic disease were excluded from the study. The demographic (birth information, gender, birth weight, head circumference, gestational week, mode of delivery, APGAR score) and clinical data (Thomson score, Sarnat&Sarnat staging, cerebral imaging [Magnetic Resonance Imaging (MRI)], and seizure activity with Amplitude-Integrated Electroencephalography [aEEG]) of the patients included in the study were recorded.
For the purpose of neurodevelopmental assessment, the WISC-IV (Wechsler Intelligence Scale for Children) was used to evaluate the intelligence level in children aged 6.5 years and older, the Stroop Test to assess cognitive control and attention levels, and the DDST scale scores to evaluate language, motor, and social development in children aged 3 months to 6.5 years. According to the applied hypothermia method, the patients were divided into two groups: CH (n = 17) and WBC (n = 33). Additionally, a control group was formed from healthy children who had come for outpatient clinic checkups, were not diagnosed with HIE, were of the appropriate age group, and whose archive records were accessible. Based on the recorded data, the long-term neurodevelopmental outcomes of these two groups were compared to each other and to the control group.
Statistical analysis
While calculating the statistics for continuous variables, the mean and standard deviation, median, minimum, and maximum values were used; for categorical variables, counts and percentage values were used. In evaluating the relationship between categorical variables, the chi-square test was used, and the student’s t-test was used to compare the means of continuous measurements between two independent groups. The researchers used the one-way ANOVA test statistic to compare the means of continuous measurements between more than two independent groups, and they applied the post hoc Tukey test statistic for pairwise comparisons when significant differences were found. The findings were analyzed using IBM SPSS version 25 software, and a statistical significance level of p < 0.05 was accepted.
Ethics committee approval
The study was initiated after obtaining approval from the Mersin University Ethics Committee, dated 18.09.2024 and numbered 2024/879.
Results
The study included a total of 50 children with HIE. The age of the children included in the study ranged from a minimum of 48 months to a maximum of 108 months, with an average age of 85.8 ± 15.9 months and a median age of 38 months. 72% of the children were boys, and 28% were girls. Cooling therapy was administered in the form of CH in 34% of the cases and WBC in 66% of the cases.
Demographic and clinical characteristics between the two groups formed according to the type of hypothermia treatment are presented in Table 1. There was no statistically significant difference between the groups in terms of both demographic characteristics and clinical features such as the Thomson score, Sarnat&Sarnat staging, blood gas parameters, aEEG, MRI results, or discharge with anticonvulsants (p > 0.05).
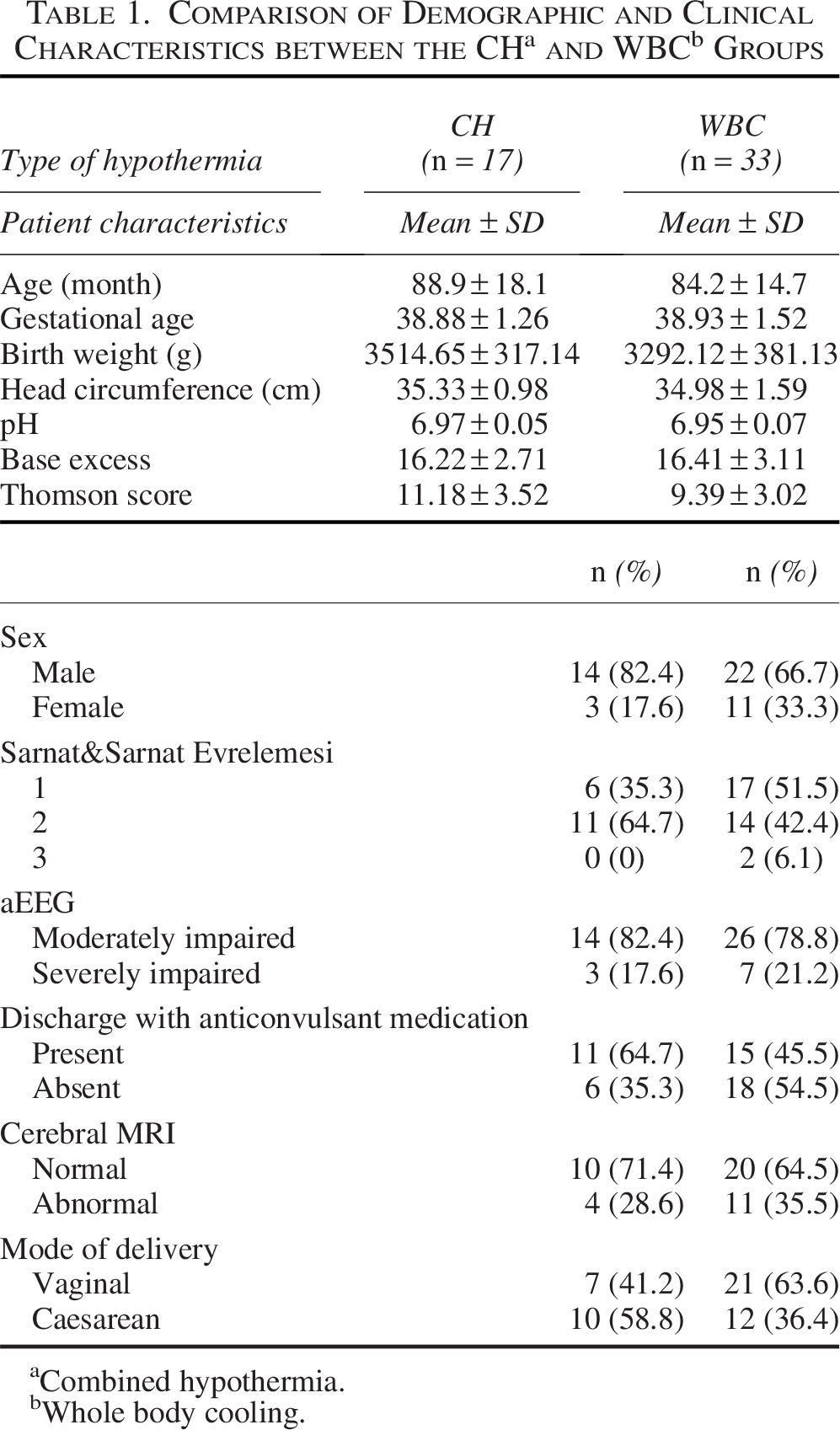
Combined hypothermia.
Whole body cooling.
When the CH and WBC groups were compared based on DDST and DDST subscale results, there was no significant difference between the groups (p > 0.05). The results of both groups (CH and WBC) were significantly different from the control group (Table 2).
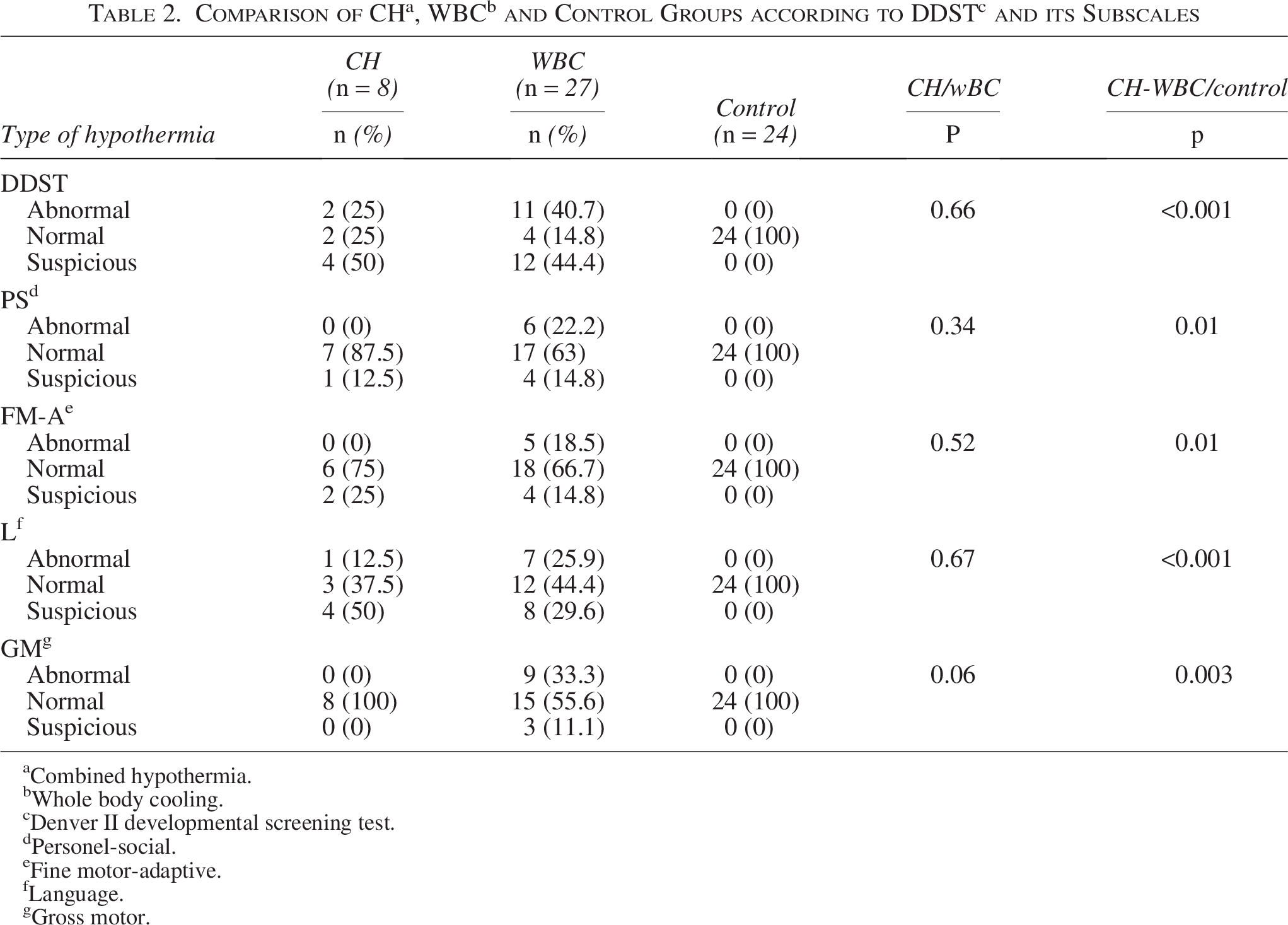
Combined hypothermia.
Whole body cooling.
Denver II developmental screening test.
Personel-social.
Fine motor-adaptive.
Language.
Gross motor.
There was no significant difference in WISC-IV test results between patients who underwent CH and those who underwent WBC (p > 0.05) (Table 3). Since an adequate control group could not be provided for the patients who underwent WISC-IV, these patients could not be analyzed with a control group.
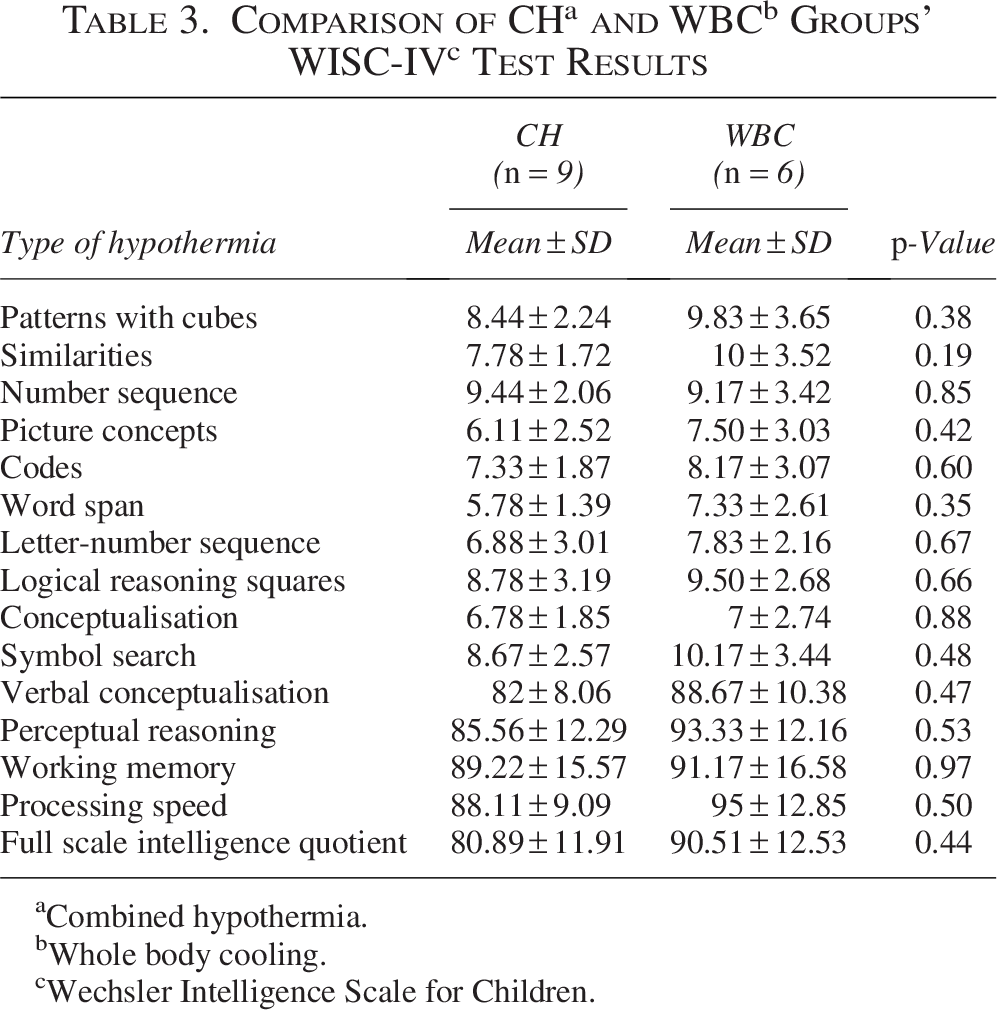
Combined hypothermia.
Whole body cooling.
Wechsler Intelligence Scale for Children.
There was no significant difference in Stroop test results between patients treated with CH and those treated with WBC (p > 0.05). The Stroop test results of both groups were significantly lower compared to the control group (p < 0.05) (Table 4).
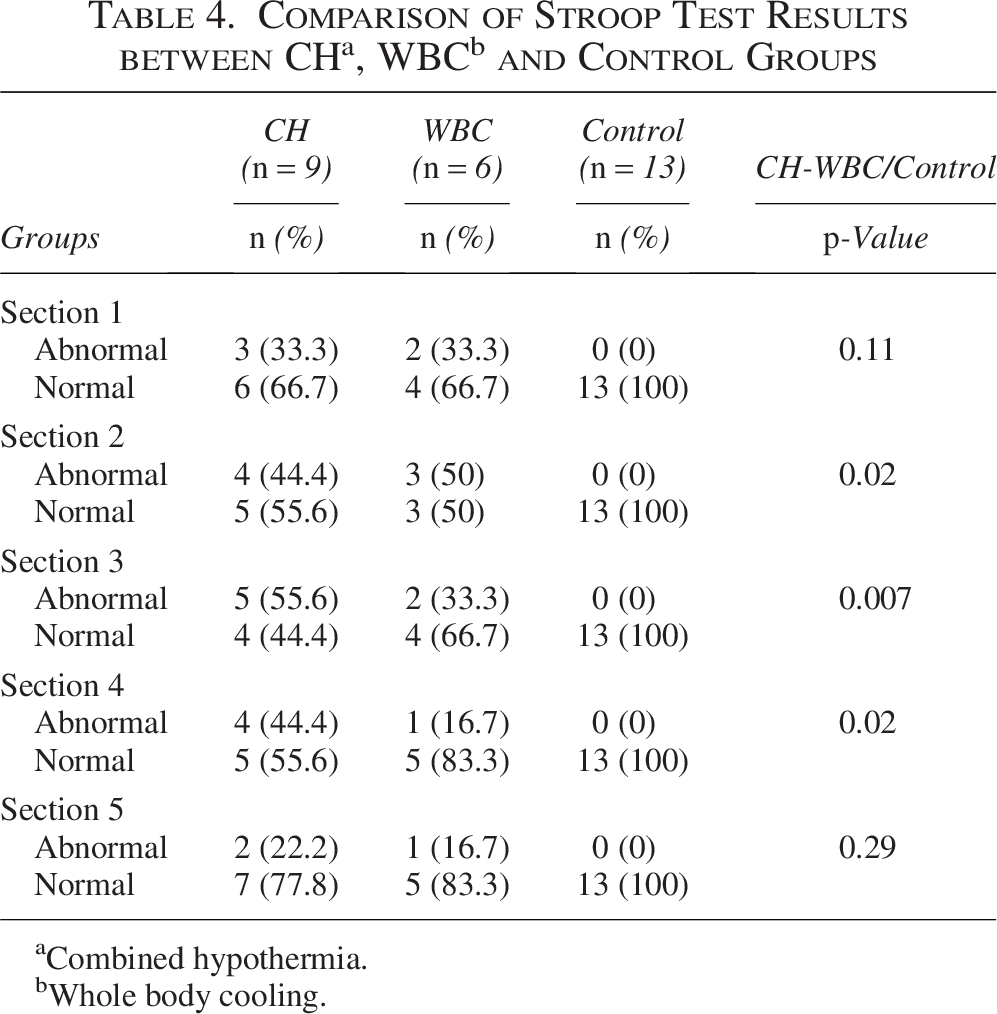
Combined hypothermia.
Whole body cooling.
Discussion
TH is an established neuroprotective treatment for infants with moderate to severe HIE and is currently applied mainly using WBC or SHC strategies (Azzopardi et al., 2009; Gluckman et al., 2005; Shankaran et al., 2005; Wassink et al., 2019). More recently, a CH approach—integrating local head cooling with systemic temperature control—has been proposed as a theoretically advantageous strategy aimed at optimizing both cortical and deep brain cooling (Celik et al., 2023).
In the present study, we compared long-term neurodevelopmental and cognitive outcomes of children with HIE treated with CH or WBC and found no statistically significant differences between the two groups across multiple validated developmental and neuropsychological assessments. To our knowledge, this is the first study to evaluate the long-term outcomes of CH relative to WBC. These findings suggest that, despite its theoretical neurophysiological advantages, CH did not demonstrate superiority over conventional WBC in long-term neurodevelopmental outcomes within the limits of the current cohort.
The rationale for CH is largely derived from experimental and physiological data indicating that SHC produces greater temperature gradients between superficial cortical regions and deep brain structures, whereas WBC results in more homogeneous cerebral cooling (Gunn and Gluckman, 2007). Based on these findings, it has been hypothesized that enhanced cortical cooling might translate into improved cognitive outcomes. Supporting this hypothesis, some neuroimaging studies have reported reduced cortical injury in infants treated with SHC (Rutherford et al., 2005). However, other investigations have shown no advantage or even greater brain injury associated with SHC compared to WBC, and neurodevelopmental outcomes assessed using standardized scales such as Bayley-III have been reported as similar between the two strategies (Celik et al., 2016; Goenka et al., 2020). These inconsistent findings suggest that theoretical or regional temperature differences alone may be insufficient to predict long-term neurodevelopmental outcomes.
The only previous clinical study evaluating CH demonstrated that the method was safe and feasible and did not increase short-term adverse effects compared with SHC or WBC (Celik et al., 2023; Sarkar et al., 2009a, 2009b, 2012). Although no statistically significant differences were observed in short-term efficacy, the CH group showed lower MRI injury scores and shorter hospitalization duration, along with a reduced need for gastrostomy in the WBC group (Celik et al., 2023). However, these findings were limited to hospitalization outcomes. Our study extends these observations into later childhood and indicates that these short-term trends do not translate into clear long-term neurodevelopmental or cognitive advantages.
Several factors may explain the absence of long-term differences between CH and WBC. Neurodevelopment following HIE is a complex and multifactorial process influenced by injury severity, injury pattern, postnatal intensive care, rehabilitation, environmental factors, and neuroplasticity, all of which may attenuate or obscure subtle differences in early neuroprotective interventions. Moreover, experimental studies exploring deeper or prolonged hypothermia have demonstrated increased mortality and adverse outcomes, leading to the conclusion that temperatures below 33°C or cooling durations beyond 72 hours may be harmful (Shankaran et al., 2014). These data suggest that there may be a narrow therapeutic window within which hypothermia is beneficial, limiting the potential incremental gains achievable by modifying cooling strategies.
Importantly, in our study, children in both cooling groups demonstrated significantly poorer developmental and cognitive performance compared with healthy controls, reinforcing previous observations that TH, while neuroprotective, does not fully prevent long-term neurodevelopmental impairment in survivors of HIE (Azzopardi et al., 2014). This finding underscores the need for adjunctive neuroprotective or neurorestorative strategies beyond hypothermia alone.
Limitations
The most significant limitation of this study is that it is a retrospective study, not a prospective randomized controlled trial. However, the similarity in the general characteristics and HIE severity levels of the cases included in the study between the groups indicates that the study’s results cannot be disregarded. In addition, a very significant limitation of the study is the small number of cases in the groups. That is to say, the number of cases for the Wechsler IV intelligence test and the Stroop color and word tests is nine in the CH group and only six in the WBC group. The DDST could only be conducted on eight cases in the CH group. Therefore, as the power of the comparisons was very low, we cannot exclude the possibility that true differences in outcome were obscured by the small sample size. Another limitation of our study is that the WBC method was performed using a servo-controlled device, while the CH methods were performed using a manually controlled device. The ideal scenario is to apply TH with a servo-controlled device in all groups. Because with a servo-controlled device, rectal temperature can be maintained within a narrower range compared to manually controlled methods. Therefore, the WBC group may have benefitted unintentionally from the use of a servo-controlled device.
Conclusions
Although no statistically significant difference was found in the long-term neurodevelopmental outcomes of patients who received CH and WBC treatments included in the study, it was determined that the CH group showed lower performance in some cognitive subdomains (especially working memory and perceptual reasoning). However, considering the limitations of the study, it appears that prospective randomized controlled trials with larger sample sizes are needed to draw definitive conclusions between the CH and WBC methods. Consequently, our findings ought to be regarded as exploratory rather than conclusive.
Authors’ Contributions
N.I.: Conceptualization, methodology, literature search, writing; A.M.A.: Writing, literature search, resource, critical review; E.Ç: Writing, literature search, critical review; E.S.: Resources, materials, data collection and/or processing; K.M.: Resources, materials, data collection and/or processing; Ç.O.: Design, supervision, critical review; A.O. and Ç.O.: Design, supervision, critical review; Y.Ç.: Design, supervision, analysis and/or ınterpretation, critical review.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Data Availability Statement
All data generated or analyzed during this study are included in the submission. The raw data are available from the corresponding author upon reasonable request.
Ethics Committee Approval
Ethics Committee approval was obtained from Mersin University Clinical Research Ethics Committee with the board decision dated 18/09/2024 and numbered 2024/879.
Informed Consent
Written informed consent was obtained from all the parents before the participants were enrolled in the study.