
Abstract
Hypoxic–ischemic encephalopathy (HIE) is a critical neonatal condition for which therapeutic hypothermia (TH) remains the cornerstone of neuroprotective intervention. Clinical observations and prior studies note that electrolyte imbalances—particularly hyponatremia and hypokalemia—frequently emerge during TH. Therefore, this study explores how activation of the renin–angiotensin–aldosterone system (RAAS) may contribute to sodium (Na) and potassium (K) disturbances in asphyxiated neonates receiving TH. In this prospective study, 38 newborns with HIE treated with TH and 21 healthy term newborns were enrolled. Serum renin, aldosterone, Na, K, and urinary electrolyte levels were measured at 24, 48, and 72 hours postnatally. Receiver operating characteristic analyses assessed the diagnostic performance of renin and aldosterone. Renin and aldosterone levels were significantly elevated in the TH group compared with controls (p < 0.05). Serum sodium levels were consistently lower at all time points (p = 0.001), while potassium levels were significantly reduced at 24 and 72 hours (p < 0.05). Fractional excretion of sodium was increased at 24 hours, and potassium excretion remained elevated throughout the TH period (p < 0.05). Among the biomarkers, aldosterone demonstrated excellent diagnostic performance at 24 hours (AUC = 0.919). Activation of the RAAS is evident in asphyxiated neonates undergoing TH, with aldosterone playing a pivotal role in electrolyte disturbances. These results highlight the clinical importance of vigilant monitoring and timely correction of serum sodium and potassium levels during the hypothermia protocol.
Keywords
Introduction
Perinatal asphyxia (PA), also known as birth asphyxia, is a condition caused by an inadequate oxygen supply to multiple organs of the newborn. It is a major contributor to neonatal morbidity and mortality, with an estimated 900,000 deaths occurring worldwide each year (World Health Organization, 2025). Neonatal hypoxic–ischemic encephalopathy (HIE) refers to brain injury resulting from PA. The primary treatment for HIE is therapeutic hypothermia (TH), which reduces the risk of further neurological damage (Gillam-Krakauer et al., 2025).
Serum electrolyte disturbances, particularly hyponatremia and hyperkalemia, are common in affected infants. The severity of these imbalances is directly correlated with the severity of asphyxia (Thakur et al., 2018). In a separate study conducted on infants with PA, hyponatremia was prominent, whereas hyperkalemia was not observed; however, potassium levels were still higher in the PA group compared with controls (Basu et al., 2010).
Electrolyte imbalances may also occur in infants with HIE undergoing TH. Notably, fluid retention and hyponatremia have been frequently reported in this context (Prempunpong et al., 2013). Acute kidney injury and tubulopathy, indicated by increased fractional sodium excretion, are suggested as underlying mechanisms of these findings (Aydin et al., 2013). While infants with PA typically present with hyperkalemia, a transition to hypokalemia has been observed following the initiation of TH. This shift is attributed to the intracellular shift of potassium induced by hypothermia (Chiang et al., 2017; Thakur et al., 2018).
Cardiac arrhythmias may also occur in infants receiving TH therapy. Electrolyte imbalance (hyponatremia, hypokalemia, hypomagnesemia, etc.) also poses a risk for cardiac arrhythmias (Rogoff and Pride, 2022). Therefore, electrolyte levels should be closely monitored in infants receiving TH. Electrolyte imbalance affects patients’ morbidity and mortality (Thakur et al., 2018).
The primary function of aldosterone is to directly regulate sodium absorption and potassium excretion. It acts as part of the renin–angiotensin–aldosterone system (RAAS). Additionally, hyperkalemia increases aldosterone synthesis (Scott et al., 2023). Given the known association between RAAS activity and electrolyte regulation, aldosterone may be a key mediator linking hypothermia to sodium and potassium imbalance.
Based on the available data, we hypothesized that aldosterone is the most important hormone affecting serum Na and K levels in infants with HIE who receive TH therapy. We aimed to evaluate the RAAS in infants with HIE who receive TH therapy, and to investigate how it may affect hyponatremia and hypokalemia. We believe this approach could provide new insights into the underlying pathophysiology. We could not find any similar studies in the literature.
Materials and Methods
Study population
This prospective study included infants diagnosed with HIE who received TH at the Department of Pediatrics, 3rd Level Neonatal Intensive Care Unit (NICU), University of Health Sciences Kayseri City Hospital, along with healthy term newborns without a history of NICU admission (control group).
Therapeutic hypothermia criteria
Infants were eligible for TH if they met the following criteria:
≥36 weeks of gestational age and weight ≥2 kg, 2- Infant ≤ 6 hours of age at initiation, Cord pH of < 7.0 or pH of arterial blood withdrawn within one hour after birth of < 7.0 and a base deficit of ≥ 16 or more, Amplitude-integrated electroencephalography (aEEG) was recorded for 30 minutes in infants with a pH between 7.0 and 7.10 and a base deficit between 12 and 16. On aEEG:
Lower amplitude < 5 microvolts and/or Upper amplitude < 10 microvolts and/or Active convulsion, Moderate-to-severe HIE based on modified Sarnat and Sarnat staging criteria (Thayyil et al., 2017), and Thompson score > 7 (Thompson et al., 1997).
Exclusion criteria
Infants were excluded if:
More than 6 hours had elapsed since birth, Birth weight was < 2000 g, They had life-threatening cardiovascular (e.g., uncontrolled persistent pulmonary hypertension) or respiratory abnormalities, They had major congenital anomalies (e.g., trisomy 13, trisomy 18, or multiple organ malformations), or They had life-threatening bleeding (e.g., uncontrolled intracranial hemorrhage) (Mosalli, 2012). Infants requiring > 50% oxygen support at the onset of TH were evaluated with echocardiography to rule out cardiac anomalies prior to treatment.
Sample size determination
Sample size estimation was performed using G*Power software (version 3.1; Universität Düsseldorf, Germany). The calculation was based on a two-tailed independent samples t-test, with a Type I error (α) of 0.05 and a desired statistical power (1−β) of 90%.
Due to the absence of prior studies evaluating renin–aldosterone activation and urinary potassium excretion during TH in neonates with HIE, a large effect size (Cohen’s d = 0.9) was assumed. This assumption was based on the expected magnitude of physiological differences between asphyxiated infants undergoing TH and healthy term newborns, as well as feasibility considerations within the study period.
Based on these parameters, a minimum sample size of 32 patients was required for the TH group. During the study period, 55 eligible infants were identified; however, 4 died, 2 were excluded due to major congenital anomalies, and 11 were excluded due to lack of parental consent. Ultimately, 38 infants were included in the TH group, along with 21 healthy term newborns in the control group.
We acknowledge that if the true effect size is smaller than assumed, the relatively small control group may limit statistical power. This limitation has been addressed in the Discussion section.
Whole-body therapeutic hypothermia protocol
Infants aged 36 weeks or older with intrapartum moderate to severe hypoxia and weighing over 2000 g were included in the study. Whole-body hypothermia was performed using an Arctic Sun 5000 device (produced by Medivance, Inc. of Louisville, CO) with servo control. TH was initiated within the first 6 hours. Body temperatures were monitored using a rectal probe. The infants’ bodies were rapidly cooled, and rectal temperatures were maintained at 33.5 ± 0.2°C for 72 hours. Then, warming was applied at a rate of 0.25°C/h to bring their body temperatures to between 36.5 and 37°C within 12 hours.
Criteria for discontinuation of hypothermia
Cooling therapy was discontinued in infants who developed life-threatening bleeding, required 100% oxygen support due to persistent pulmonary hypertension, or developed arrhythmia or hypotension that could not be controlled with medical treatment during TH.
Supportive and adjunctive treatments
Infants who were intubated and monitored with mechanical ventilation or given nasal breathing support were provided with heated and humidified air for breathing.
No sedative agent was routinely administered to the patients. Morphine infusion (10–20 μg/kg/h) was preferred in cases of shivering, agitation, or incompatibility with mechanical ventilation. The infusion was discontinued after the resolution of the existing problems. Morphine infusion was discontinued in cases of respiratory or blood pressure problems. No paralytic agent was administered to any patient.
Dobutamine was the first choice as the inotropic agent. In cases of persistent hypotension, dopamine infusion was administered in addition to dobutamine. Adrenaline infusion was also administered to patients when necessary.
The patient population received fluid containing 10% dextrose within the first 24 hours, and 0.2% normal saline containing 10% dextrose (50–60 cc/kg/day throughout the TH therapy) on the 2nd and 3rd days. Patients were not fed during the TH therapy. Intravenous sodium supplementation (3% hypertonic saline solution) was administered to patients with serum Na levels below 132 mEq/L (unless dilutional hyponatremia was suspected). Intravenous potassium supplementation was administered to patients with serum K levels below 4 mEq/L.
For patients with convulsions, phenytoin was the first choice of anticonvulsant (since intravenous phenobarbital is not available in our country) if the patient’s hemodynamic values were stable and there was no arrhythmia, and levetiracetam was the first choice for hemodynamically unstable patients.
As part of our unit’s routine procedure for TH, all patients were administered ampicillin and cefotaxime to reduce the risk of infection. Antibiotics were discontinued in patients without signs of infection after warming was completed. Aminoglycosides were not used in any patients due to the potential risk of renal toxicity.
Laboratory evaluation
Electrolytes, renal function tests, complete blood count, and coagulation values of the patients were evaluated daily. In addition to these parameters, plasma renin and aldosterone, urine Na, K, and creatinine levels were also evaluated at the same time (at the 24th, 48th, and 72nd hours postnatally). Similar measurements were performed in the control group at the same time points: serum Na, K, creatinine, plasma renin, and aldosterone levels, and spot urine Na, K, and creatinine levels.
The concentrations of aldosterone, direct renin, and plasma renin activity were measured by isotopic methods (radioimmunoassay (RIA)/chemiluminescent immunoassay (CLIA)). Urine and serum electrolytes (sodium, potassium) were measured by indirect ISE and creatinine by the compensated Jaffe method on Cobas 8000c (Roche Diagnostics). Additional Na and K supplementation was provided to patients who required it.
In the TH group, urine samples were collected via urinary catheter in 30 infants as part of routine clinical monitoring. In the healthy control group, spot urine samples were obtained using sterile urine collection bags. All urine samples were collected at standardized time points corresponding to blood sampling and were processed promptly to minimize potential contamination or timing-related variability in electrolyte measurements.
Definition of acute kidney injury
Acute kidney injury (AKI) was defined according to the neonatal kidney disease: Improving Global Outcomes (KDIGO) criteria. AKI was diagnosed based on urine output <1 mL/kg/h and/or an increase in serum creatinine relative to baseline values during the first 72 hours of life. These criteria were applied to all infants in the TH group.
Ethical approval
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Erciyes University Ethics Committee, Kayseri, Turkey (Approval No: 09.01.2019/96681246). Written informed consent was obtained from a parent and/or legal guardian of each participant.
Statistical analysis
Data were analyzed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were expressed as mean ± standard deviation, median (min–max), or frequency (%), as appropriate. The Shapiro–Wilk test was used to assess normality. Normally distributed data were compared using the independent samples t-test; non-normally distributed data were compared using the Mann–Whitney U test. The chi-square test was used for categorical variables. Receiver operating characteristic (ROC) analyses were performed using SPSS and EasyROC (version 1.3). The Youden index was applied to determine optimal cut-off values. A p value <0.05 was considered statistically significant.
Results
Demographic and anthropometric characteristics were comparable between the TH and control groups (p > 0.05). As expected, Appearance, Pulse, Grimace, Activity, Respiration (APGAR) score were significantly lower in the TH group than in controls (p < 0.001) (Table 1).
Comparison of Demographic and Anthropometric Characteristics Between Infants Receiving Therapeutic Hypothermia and Healthy Controls

Statistically significant p-values (p < 0.05) are shown in bold.
Data are expressed as mean ± standard deviation, median (minimum, maximum).
TH, therapeutic hypothermia.
Serum renin levels at 24 hours and 72 hours were significantly higher in the TH group than in the control group (p < 0.05), whereas no significant difference was observed at 48 hours (p > 0.05) (Table 2).
Comparison of Serum Sodium, Potassium, Renin, Aldosterone, Fractional Sodium, and Fractional Potassium Levels Between Therapeutic Hypothermia and Control Groups at 24, 48, and 72 Hours
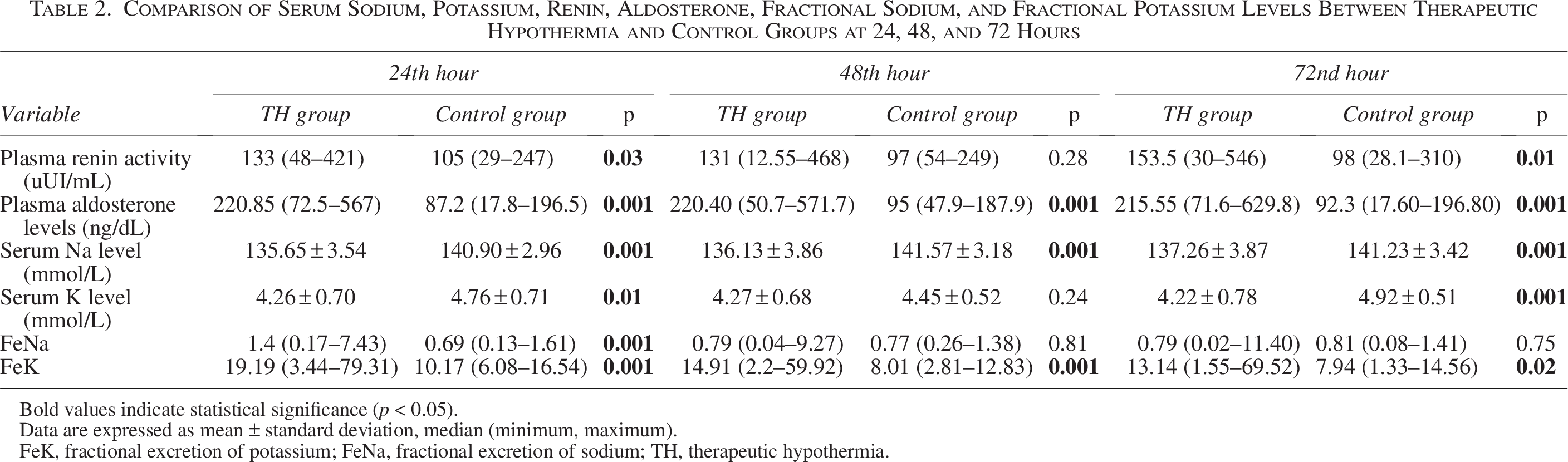
Bold values indicate statistical significance (p < 0.05).
Data are expressed as mean ± standard deviation, median (minimum, maximum).
FeK, fractional excretion of potassium; FeNa, fractional excretion of sodium; TH, therapeutic hypothermia.
Serum aldosterone levels were significantly elevated in the TH group compared with controls at all three time points—24 hours, 48 hours, and 72 hours (p < 0.001) (Table 2).
Serum sodium concentrations were consistently lower in the TH group at 24 hours, 48 hours, and 72 hours (p < 0.001). Serum potassium levels were significantly reduced at 24 hours and 72 hours (p < 0.05) but not at 48 hours (p > 0.05) (Table 2).
Despite the absence of a significant difference in serum potassium levels at 48 hours, intravenous potassium supplementation was administered to 26% of patients during the 24–48-hour period, while fractional potassium excretion (FeK) remained significantly elevated.
Fractional excretion of sodium (FeNa) was significantly higher in the TH group at 24 hours (p < 0.05) but showed no difference at 48 hours or 72 hours (p > 0.05). Fractional excretion of potassium (FeK) was significantly increased in the TH group at all measured time points (p < 0.05) (Table 2).
A total of nine infants (23.6%) in the TH group required intravenous sodium supplementation. Four infants received a median of 2 (1.4–5) mEq/kg within the first 24 hours, five received 5 (1.6–5.2) mEq/kg between 24 and 48 hours, and four received 3 (1.6–5.2) mEq/kg between 48 and 72 hours (Table 3).
Intravenous Sodium and Potassium Supplementation and Urine Output in the Therapeutic Hypothermia Group
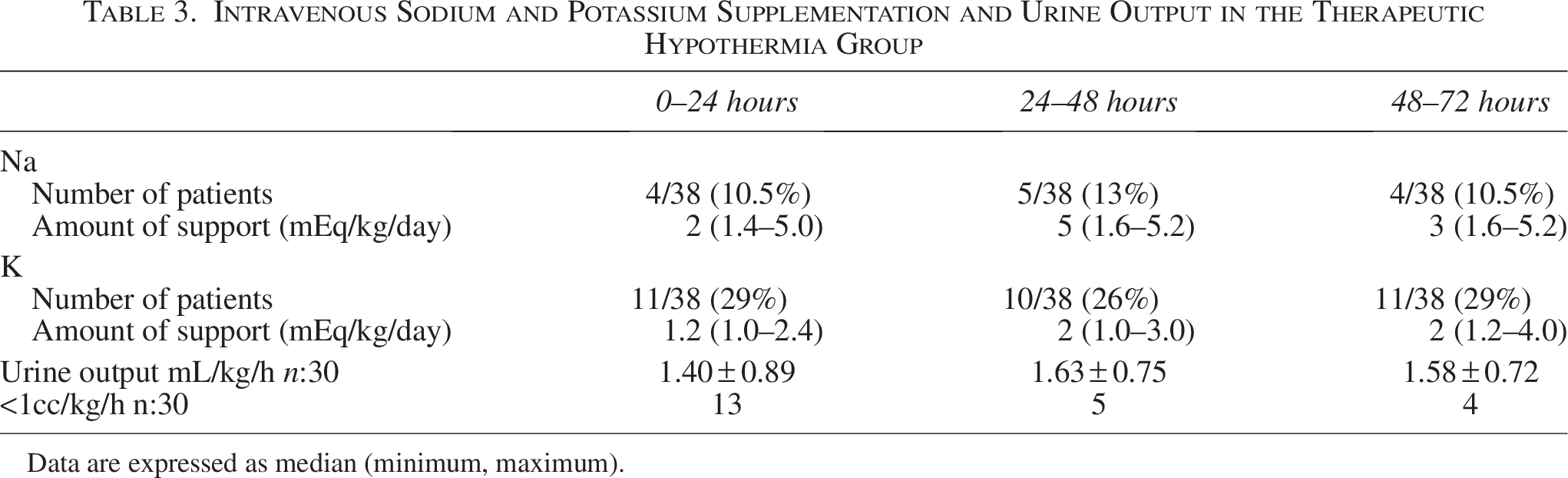
Data are expressed as median (minimum, maximum).
Intravenous potassium supplementation was administered to 22 infants (57.8%) in the TH group. 11 received 1.2 (1.0–2.4) mEq/kg within 24 hours, ten received 2 (1.0–3.0) mEq/kg between 24 and 48 hours, and 11 received 2 (1.2–4.0) mEq/kg between 48 and 72 hours (Table 3).
Ten infants (26%) in the TH group experienced seizures requiring treatment; six had severe and 32 had moderate HIE according to the Sarnat classification. Inotropic support was required in 24 infants (63%): nine received dobutamine alone, one dopamine alone, 13 dobutamine + dopamine, and one a combination of dopamine, dobutamine, and adrenaline.
Thirty infants were monitored with a urinary catheter. Oliguria (<1 mL/kg/h) was observed in 13 infants on day 1, 5 infants on day 2, and 4 infants on day 3.
According to the neonatal KDIGO criteria, 13 infants met the definition of acute kidney injury during the TH period.
ROC analyses: For renin, the area under the ROC curve (AUC) was 0.673 (p < 0.05) at 24 hours and 0.703 (p < 0.05) at 72 hours. For aldosterone, the AUCs were 0.919 (p < 0.05) at 24 hours, 0.903 (p < 0.05) at 48 hours, and 0.919 (p < 0.05) at 72 hours (Fig. 1).
Receiver operating characteristic (ROC) curves for renin and aldosterone levels at 24-, 48-, and 72-hours distinguishing infants with therapeutic hypothermia (TH) from controls.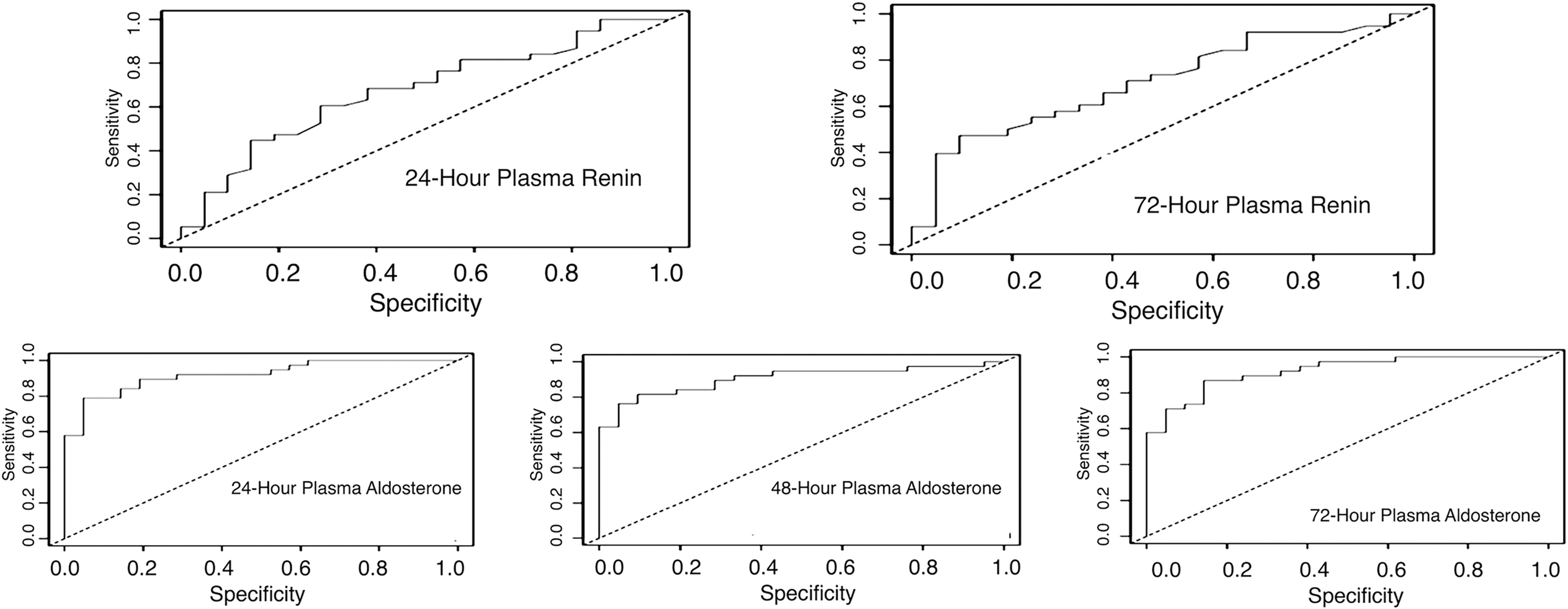
According to the Youden index, optimal cut-off values were:
Renin: 124 at 24 hours (>124 = patient, ≤ 124 = control) and 189 at 72 hours (>189 = patient, ≤ 189 = control); Aldosterone: 152.5 at 24 hours, 156.9 at 48 hours, and 146 at 72 hours.
Sensitivity and specificity values were as follows:
24 hours renin: 60.5% and 71.4%; 72 hours renin: 47.4% and 90.5%; 24 hours aldosterone: 78.9% and 95.2%; 48 hours aldosterone: 81.6% and 90.5%; 72 hours aldosterone: 86.8% and 85.7%.
These findings indicate that aldosterone demonstrated the highest diagnostic performance, particularly at 24 and 72 hours (AUC = 0.919).
Discussion
This study is the first to demonstrate activation of the RAAS in newborns with HIE undergoing TH. Our findings indicate that aldosterone levels are significantly increased in these infants and that this elevation contributes to alterations in serum sodium and potassium concentrations, as well as their urinary excretion patterns (Table 2).
Although TH is an established neuroprotective intervention that reduces mortality and morbidity in HIE, it may also induce complications involving multiple organ systems. Among these, renal function and electrolyte balance are particularly affected (Shah et al., 2007).
Kuroda et al. evaluated RAAS activation in patients undergoing open-heart surgery and found that both renin and aldosterone levels increased during hypothermia (Kuroda et al., 1983). Their study supports our findings, although their patient population consisted of postoperative adults, and measurements were taken before, during, and after hypothermia in the same subjects.
Pereira et al. demonstrated that there was a difference in cord blood aldosterone levels between patients with PA and healthy infants, with higher levels of aldosterone present in the cord blood of asphyxiated newborns (Pereira and Procianoy, 1997). Therefore, the elevated aldosterone levels we found in our study may be due solely to asphyxia. Otherwise, elevated aldosterone levels without hypothermia therapy indicate that aldosterone elevation may be due to hypoxia rather than hypothermia.
Previous studies have reported that infants with HIE frequently develop electrolyte imbalances—including hyperkalemia, hyperphosphatemia, and hypocalcemia—before initiation of TH, due to hypoxia-induced cellular injury. Following the onset of cooling, however, a transition from hyperkalemia to hypokalemia is typically observed. Eicher et al. (2005) first reported hypokalemia as a side effect of TH, a finding later confirmed by the Neonatal Study Group (Kwon et al., 2011). In animal models, Todd et al. (1977) observed increased hepatic potassium levels during cooling, likely due to catecholamine-mediated intracellular potassium shifts. Similarly, Koht et al. (1983) noted that hypokalemia in this context rarely reaches arrhythmogenic levels, whereas Boelhouwer et al. (1987) reported significant hypokalemia in adults after postoperative cooling, leading to cardiac complications, which they attributed to intracellular potassium redistribution rather than urinary loss. Conversely, Gluckman et al. (2005) found no significant increase in hypokalemia incidence among cooled neonates.
In our study, serum potassium levels were significantly lower in the TH group at 24 and 72 hours, whereas no difference was observed at 48 hours—possibly due to potassium supplementation during that interval. Importantly, the apparent normalization of serum potassium levels at 48 hours should be interpreted with caution, as it is likely attributable to iatrogenic potassium replacement rather than true physiological recovery. This interpretation is supported by the persistently elevated FeK during the same period, indicating ongoing renal potassium loss despite supplementation. Importantly, fractional potassium excretion was significantly elevated at all time points in the TH group compared with controls (Table 2), suggesting that increased urinary potassium loss contributes to hypokalemia. This finding contrasts with the observations of Boelhouwer et al. (1987), who reported no renal contribution, and supports the hypothesis that elevated aldosterone promotes renal potassium excretion during TH.
Fluid retention and hyponatremia are also well-documented during TH. Prempunpong et al. (2013) attributed these findings to inappropriate antidiuretic hormone (ADH) secretion and/or acute kidney injury, leading to dilutional hyponatremia. Aggarwal et al. (2005) similarly reported combined glomerular and tubular dysfunction in asphyxiated neonates, with reduced glomerular filtration rate, fluid retention, and hyponatremia, along with increased FeNa.
In our cohort, serum sodium levels were significantly lower in the TH group at 24, 48, and 72 hours, confirming these earlier observations. Although FeNa was elevated at 24 hours, it did not differ significantly thereafter. The interpretation of FeNa in this setting should also consider the presence of acute kidney injury, as hypoxia-related tubular dysfunction may limit the kidney’s ability to appropriately respond to aldosterone-mediated sodium reabsorption. We initially anticipated reduced sodium excretion due to elevated aldosterone; however, hypoxia-induced tubular injury may have impaired aldosterone responsiveness. The absence of persistently increased FeNa and the partial sodium retention observed could reflect a balance between aldosterone-mediated reabsorption and tubular dysfunction secondary to hypoxia.
Inotropic support represents another important potential confounding factor in the interpretation of RAAS activation. In the present study, 63% of infants in the TH group required inotropic support, most commonly dobutamine and dopamine. Both agents are known to influence renal blood flow, glomerular filtration, and renin secretion independent of hypoxic–ischemic injury or hypothermia. Therefore, part of the observed elevation in renin and aldosterone levels may be attributable to inotropic therapy rather than the hypothermia protocol itself. This interaction should be considered when interpreting RAAS-related findings in critically ill neonates undergoing TH.
Limitations
Several limitations of this study should be acknowledged. First, the TH group differed from the control group in two fundamental aspects: exposure to hypothermia and the presence of PA. Therefore, the current study design does not allow complete separation of the effects of ischemic renal injury from those attributable to TH itself. Although previous studies have demonstrated elevated aldosterone levels in asphyxiated neonates even before cooling, hypothermia-related physiological changes may further modulate RAAS activation. Accordingly, our findings should be interpreted as reflecting the combined effects of asphyxia and hypothermia rather than hypothermia alone. In addition, the high rate of inotropic use in the TH group may have contributed to RAAS activation and represents a potential confounding factor.
Conclusion
This study is the first to demonstrate activation of the RAAS in infants with HIE undergoing TH. Our findings emphasize the importance of vigilant monitoring for hyponatremia and hypokalemia in asphyxiated neonates undergoing TH, recognizing that both ischemic injury and hypothermia-related physiological changes may contribute to RAAS activation and electrolyte disturbances. Moreover, we provide the first evidence that increased urinary potassium excretion may contribute to hypokalemia in this setting. Further studies investigating the underlying mechanisms and clinical management of electrolyte disturbances in cooled asphyxiated neonates are warranted.
Authors’ Contributions
Conceptualization: O.B. and F.B. Methodology: O.B., B.İ., and A.Ö. Data curation: B.İ. and Ç.K. Formal Analysis: B.İ. and O.B. Investigation: O.B. and B.İ. Writing—original draft: B.İ. and O.B. Writing—review and editing: O.B. and B.İ. Supervision: O.B.
Footnotes
Acknowledgments
The authors sincerely thank all members of the neonatal research team at the University of Health Sciences, Kayseri City Hospital, for their invaluable assistance and collaboration throughout the study. The authors also express their gratitude to the participating families and the mothers who generously provided consent for their newborns to take part in this research.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. Furthermore, no specific funding was received for this study.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.