
Abstract
This study investigates the experiences and perspectives of Sikh caregivers of autistic children with respect to cultural awareness and educational support. Existing literature indicates that caregivers of autistic children already face systemic barriers in accessing appropriate services, and that for minoritized populations is often compounded. Data from a survey (n = 113) and focus groups (n = 11) in this study reveal a significant gap in autism knowledge between Sikh caregivers own beliefs and those that they perceive to be held broadly by the Sikh community. The results echo previous similar diaspora-related research, highlighting persistent cultural stigma and misconceptions surrounding autism, as well as language barriers and a lack of culturally relevant community resources. These challenges often hinder caregivers’ access to support services. This study underscores the need for cultural competence in educational practices and increased community awareness to foster understanding and improve support for autistic individuals and their caregivers within the Sikh community.
Caring for and advocating on behalf of a child with autism is often difficult and time-consuming, largely due to systemic barriers within educational and social support systems (Ishler et al., 2023; Krakovich et al., 2016; Samsell et al., 2022). While families encounter numerous challenges in rearing a child with a disability, these are often compounded for those from minoritized backgrounds. Specifically, researchers have found that minoritized caregivers often face higher levels of autism-related stigma, more negative experiences with medical professionals, and less access to information and supports (Iadarola et al., 2017; Khalil et al., 2025; Rivera-Figueroa et al., 2022). In addition, parents from immigrant or other ethnic minority backgrounds often find themselves needing to reconstruct their sense of identity following their child's disability diagnosis (Lee & Zhu, 2021). This process involves reexamining beliefs about disability within the framework of their cultural or religious background, which sometimes conflict with their own evolving beliefs. This can pressure caregivers to change the way they interact with schools and educators as they advocate for their child's needs (Lee & Zhu, 2021). These demands can be both emotionally taxing and isolating for families of autistic children.
While there is a growing body of literature exploring cultural, ethnic, and religious experiences and perspectives on autism, such as those of Lantinx, Black, Muslim, Jewish, Hispanic, and Chinese caregivers (Colbert et al., 2017; Gilligan, 2013; Jegatheesan et al., 2010; Rivera-Figueroa et al., 2022; Sakai et al., 2019; Sher et al., 2022), there remains a notable gap in research focused on Sikhism. Sikhism is a monotheistic religion founded in the fifteenth century in the Indian subcontinent and is deeply connected to the Punjabi language, culture, and ethnic identity, intertwining Sikh religion with Punjabi cultural identity (Cole, 2004). While the majority of Sikhs reside in India, the second largest population of Sikhs live in Canada and has done so for over a century (Johnson et al., 2024; Shahed, 2019). Today, approximately 2% of Canada's population identifies as Sikh, demonstrating a 130% increase over the past two decades (Statistics Canada, 2022).
The Sikh faith centers on the sacred scripture, the Guru Granth Sahib, and emphasizes values such as community, equality, and compassion. Researchers suggest myths about autism continue to circulate within Punjabi and Indian communities, leading to stigma and misconceptions (Iqbal et al., 2023; Vats et al., 2024). Common misconceptions include beliefs that autistic individuals prefer to be alone, cannot detect rejection, do not share feelings, lack emotional responses, or are incapable of participating in normal life or relationships (Iqbal et al., 2023). These misconceptions may be shaped by cultural norms regarding what is considered typical or atypical behavior (de Leeuw et al., 2020). Researchers indicate that strong cultural stigma, general misconceptions, and limited awareness often contribute to delayed diagnoses and reduced access to supports (Shafi et al., 2024; Turnock et al., 2022). South Asian families confirm pronounced stigma and a lack of understanding around autism within their communities have led to social isolation and stigmatization (Shafi et al., 2024). Similarly, researchers of the Punjabi community's perspectives on autism describes low levels of autism awareness and understanding as well as the prevalence of misconceptions or reinforcement of misinformation (Iqbal et al., 2023). As described in Crenshaw's (1991) intersectionality framework, the social, cultural and political identities of individuals can overlap and intersect to produce unique challenges or positions. For Sikh caregivers’, cultural, religious, linguistic, or social positions can overlap and result in unique challenges accessing knowledge and educational support for their autistic children. Researchers suggest South Asian cultures, including Sikhs, face challenges in integrating individuals with disabilities into their culture and mainstream society at large due to restrictive norms and limited information (Carruthers et al., 2018). Compounding the impact of community-based factors affecting the caregiver experience, autism research, assessments, and diagnostic tools, to date, have been overwhelmingly Western or Eurocentric, even within South Asian countries. Interventions often draw from European cultural frameworks, including those shaped by the legacy of the eugenics movement, focused on restrictive norms (de Leeuw et al., 2020; Fong et al., 2022).
Therefore, this study examines the perspectives of Sikh caregivers of autistic individuals in Canada. Such understanding of individual and perceived community beliefs on autism as well as perceptions of the educational system will help contextualize the role and experience of minoritization, specifically for Sikh caregivers. Specifically, this research addresses the following questions: a) How does the Sikh caregiver community understand autism? b) How do Sikh parents/caregivers perceive the Sikh community's perceptions of autism? c) What are the experiences, perspectives, and desires of Sikh caregivers of autistic children related to the educational support of their children?
Method
This research project used an explanatory sequential design starting with quantitative data collection (i.e., online survey) followed by qualitative data collection (i.e., focus groups) to further interpret and expand upon the initial findings (Creswell, 2013). Participants for both the quantitative and qualitative aspects of the study were Sikh caregivers of autistic children residing in Canada. The inclusion criteria for participation are individuals over 16 years of age that self-identifies as a Sikh caregiver of an autistic child. For the purposes of this study, a caregiver was defined as any individual self-identifying as playing a primary role in the daily care of an autistic person. Ethical approval for the study was granted by the General Research Ethics Board at Queen's University.
Measures
Researchers collected quantitative data using an online survey focused on caregiver experiences and perspectives on autism, as adapted from Kamei (2013), LaBarbera (2017), and Zuckerman et al. (2018). The survey consisted of three distinct sections, including demographics (e.g., caregiver age, home language), autism beliefs and knowledge, and educational supports. The demographic section included 15 closed-choice questions, autism beliefs and knowledge included 21 Likert scale questions, and the educational supports section included 11 Likert scale questions. Likert scales included the options, numbered from 1–5: strongly disagree, disagree, unknown, agree, and strongly agree. Questions assessing beliefs and knowledge contained two distinct segments—one on autism characteristics, adapted from Zuckerman et al. (2018), and the other on autism origins, adapted from Kamei (2013). Adaptations included the removal of one question from the characteristics section due to a lack of fit with the population and the addition of two question stems for all statements: “My belief of this statement” and “My community's belief of this statement.” The questions regarding caregivers’ perspectives on their educational support were adapted from the sensitivity to family needs and collaborative practices of the parents’ section from LaBarbera's (2017) survey on teacher and caregiver educational outlooks. Adaptations included changing the question starter from “My child(rens) teacher” to “As a Sikh caregiver, I feel that the autistic individual's teacher(s),” and the addition of the item, “is able to communicate with me with culturally responsiveness and in my choice language.” The scale for this section included unscored options for unsure and not applicable. The original survey instruments were validated (Kamei, 2013; LaBarbera, 2017; Zukerman et al., 2018) but our adapted survey was not validated prior to the study. To ensure valid survey submissions, we used Qualtrics spam prevention techniques including ReCAPTCHA, Fraud Score, ID Duplication (Qualtrics, 2025), as well as limiting included responses to those from within Canada and to those who self-identified as Punjabi or South Asian. The survey took participants between 20 and 30 min. The survey questions are available upon request from the first author.
Following the completion of the survey, the research team—together with community researchers (fourth and fifth author) and the partner organization leader (third author)—developed focus group questions informed by the survey findings and the study's guiding research questions. The whole team collectively created the focus group questions aligned to both the population and the study method. We also used versions of some of the survey questions to gain deeper responses. The focus group sessions included seven questions involving three themes: caregiver perceptions of autism, their perceived community's perceptions on autism, and their experience navigating religious and educational contexts. These questions are available upon request from the first author.
Data Collection Methods
The survey was distributed through social media platforms and the networks of the partnering organization, Sikhs for Autism, over a period of 2 months. All recruitment efforts led individuals directly to the online survey link. Following a research introduction and request for research consent, participants were required to confirm that they identified as a Sikh caregiver of an autistic individual in Canada. Following confirmation of their fit with these criteria, individuals were invited to begin the survey. Participants were permitted to complete the survey in one or more sittings. Data from incomplete surveys (n = 55) were calculated in the results where applicable. All submissions with at least two completed questions (n = 113) were used in the analysis. Following the survey completing, participants were invited to the focus group study and to submit their contact information to receive a $5 gift card incentive.
In addition to recruitment at survey completion, the partnering organization Sikhs for Autism shared invitations within their networks. Four focus groups were conducted online through Zoom. Each included two to four participants with a total of 11 participants across the four groups. Each focus group was conducted online over a 45 min to 1 hour span. All focus groups were facilitated by one of two community researchers. In terms of positionality, the community researchers, who conducted the focus groups, were both Punjabi and English-speaking female members of the Sikh community and with an undergraduate degree in social sciences and a particular interest in disability, inclusion, and autism in the Sikh community. The community partner (third author), who facilitated recruitment, was a Punjabi and English-speaking Sikh father of two children, one with autism, with over a decade of educational advocacy experience for Sikh autistic students and their families. The researchers (first and second author), who worked behind the scenes to prepare and lead the project, were white, English-speaking, and non-Sikh. The first author was a female PhD student in special education with a background in sociology and disability studies, and the second was a male professor in special education with over 20 years of experience in special education. Both community researchers received training in qualitative methods and focus group facilitation from the research team and were involved in the early development of the research project. They took turns leading groups and the non-facilitating community researcher was present to record the session or provide support as needed. Following data collection, participants received a $40 gift card for their involvement. Sessions were recorded and later transcribed verbatim for analysis. When the transcript included Punjabi words, the community researcher translated them into English for analysis.
Data Analysis
The survey data were analyzed using descriptive statistics and multiple one sample t-tests. Descriptive statistics, including frequencies, percentages, and means, were used to summarize the demographic data from the caregivers. A one sample t-test was used to examine the differences in means of the individual's perceptions and understanding of autism compared to their perceptions of their community's beliefs. This was used across each question and thematically based on the question focus (i.e., caused by parent or family, medical professionals or genetics, or other). The educational support questions were examined using descriptive statistics (i.e., frequencies, percentages, and modes) as they were not comparative to one another.
We conducted a deductive thematic analysis of the focus group transcripts, following the approach outlined by Braun and Clarke (2006). Researchers developed the codebook using themes identified in the survey results and refined for clarity and cultural fit through consultation with Sikh members of our research team. Two team members independently coded each transcript. Intercoder reliability was assessed via NVivo's coding comparison function (O’Connor & Joffe, 2020), yielding an unweighted Cohen's kappa of 0.40 and a percent agreement range of 92% to 100% calculated by NVivo. The difference between these two scores is attributed to the lack of discrete start and end points for coded segments; software-based calculations often penalize minor segmentation differences despite strong conceptual alignment (Gamarra & Heron, 2025). To ensure the rigor of our final analysis, all discrepancies were reconciled through dialogue (between the coders) until 100% consensus was reached.
Results
Participant Demographics
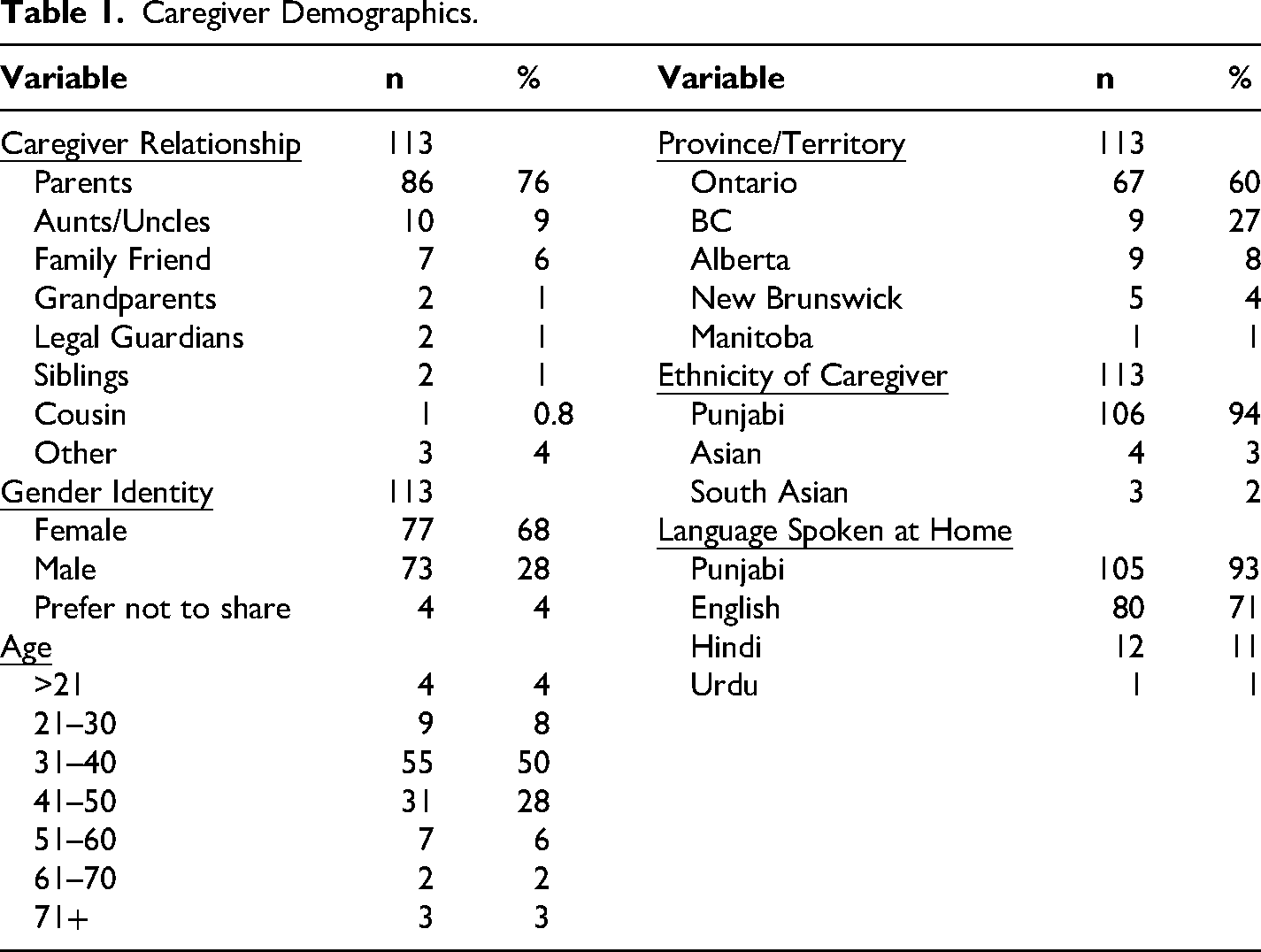
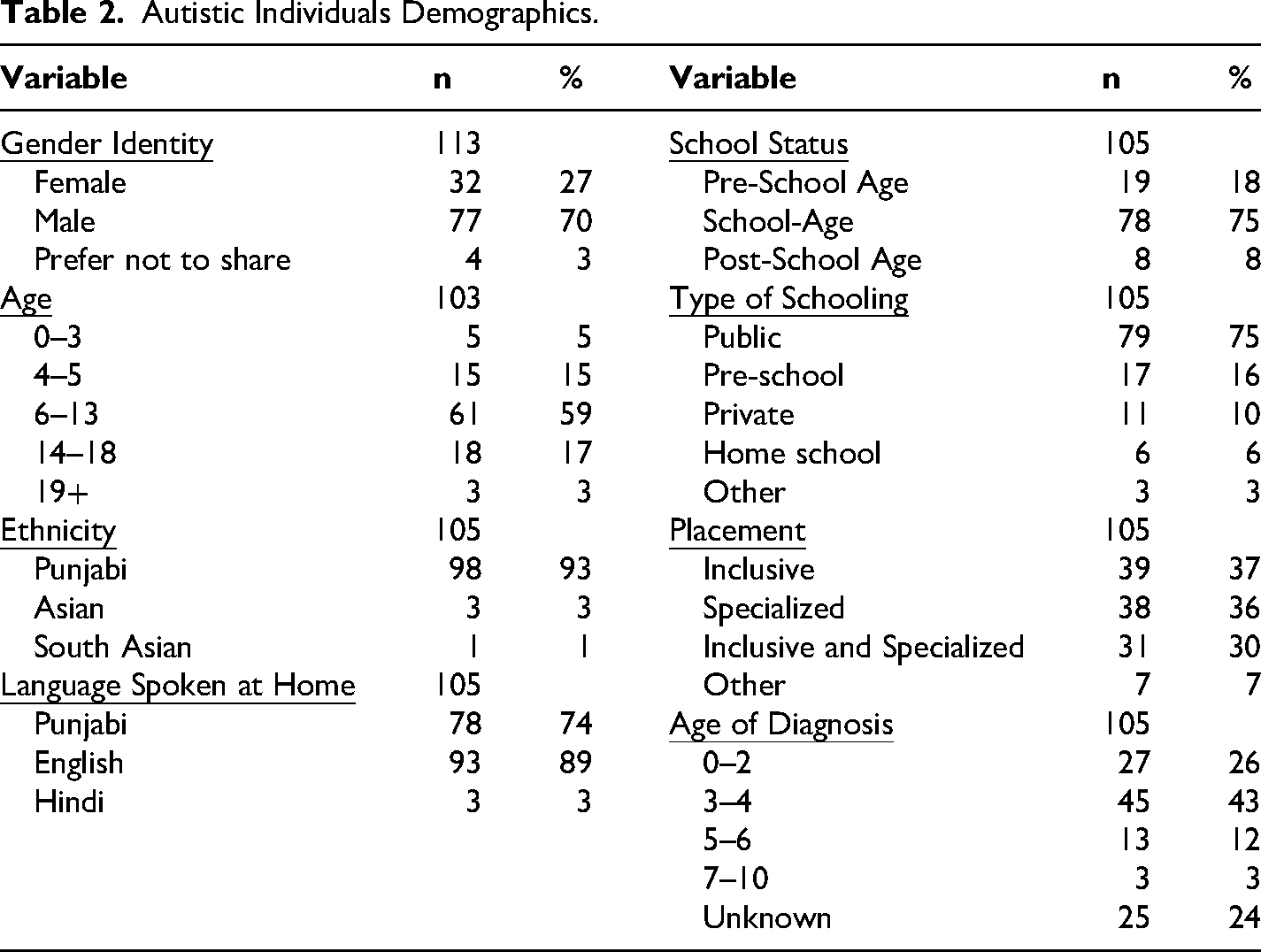
In broad terms, the caregiver participants for the survey (n = 113) were Punjabi (94%), female (68%), parents (76%), from Ontario (60%), who spoke Punjabi (93%) and English (71%), and on average, between the ages of 31–40 (see Table 1). Caregiver-reported demographics of the autistic individuals in their care, from the survey sample, included individuals who were school aged (74%), Punjabi (93%), males (70%), who speak Punjabi (89%) and speak English (74%), and on average, between the ages of a 6–13 years old. Of the sample, 37% were educated in inclusive settings, 36% in specialized programs, 30% in a combination of inclusive and specialized programs and 7% were in other formats (e.g., post school; See Table 2). Among the focus group participants (n = 11) were one father, two siblings, and eight mothers of autistic children. We did not collect full demographic information for the focus group participants.
Caregiver Demographics.
Autistic Individuals Demographics.
Quantitative Results
Sikh Caregivers and Perceived Community Beliefs on Autism
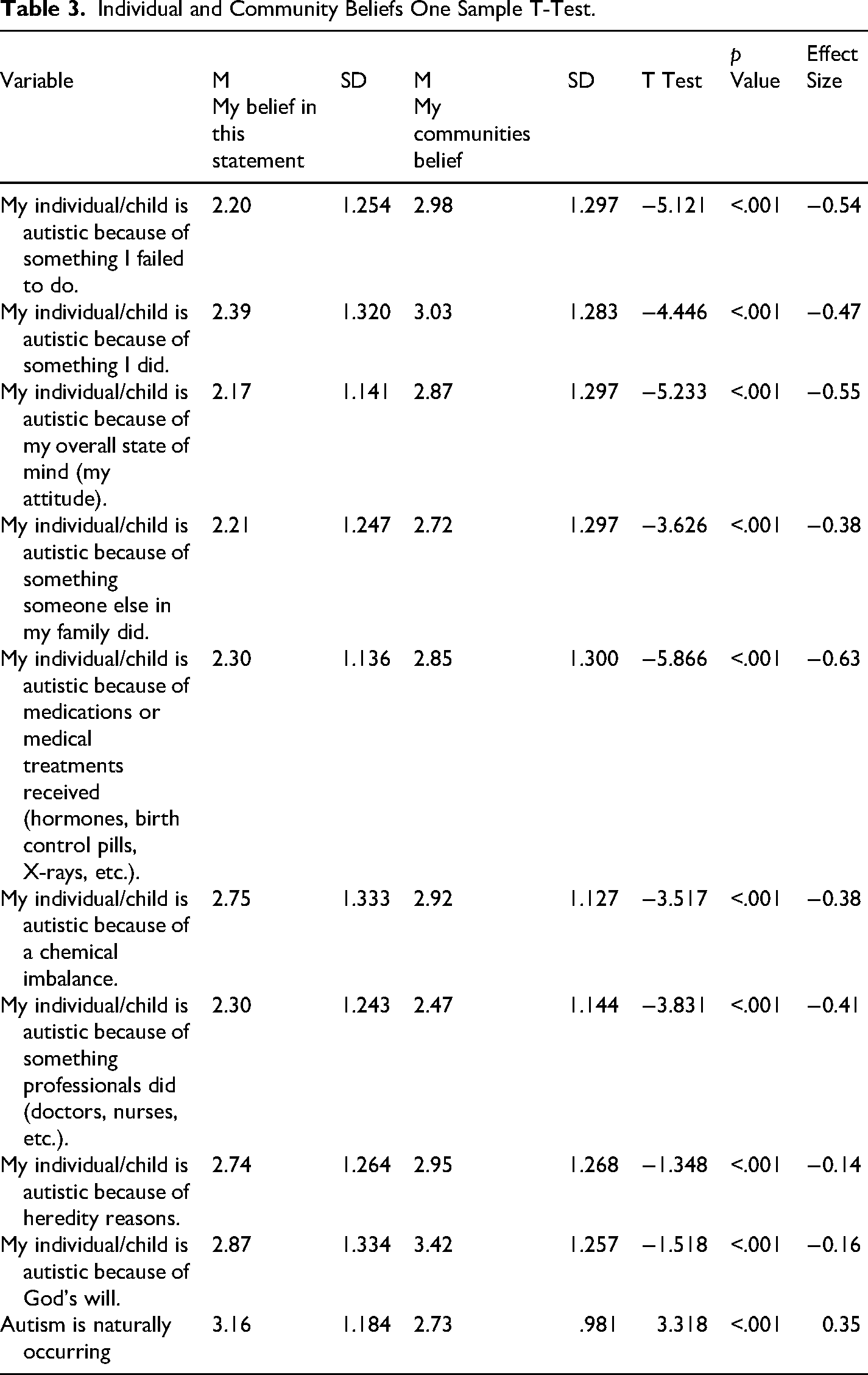
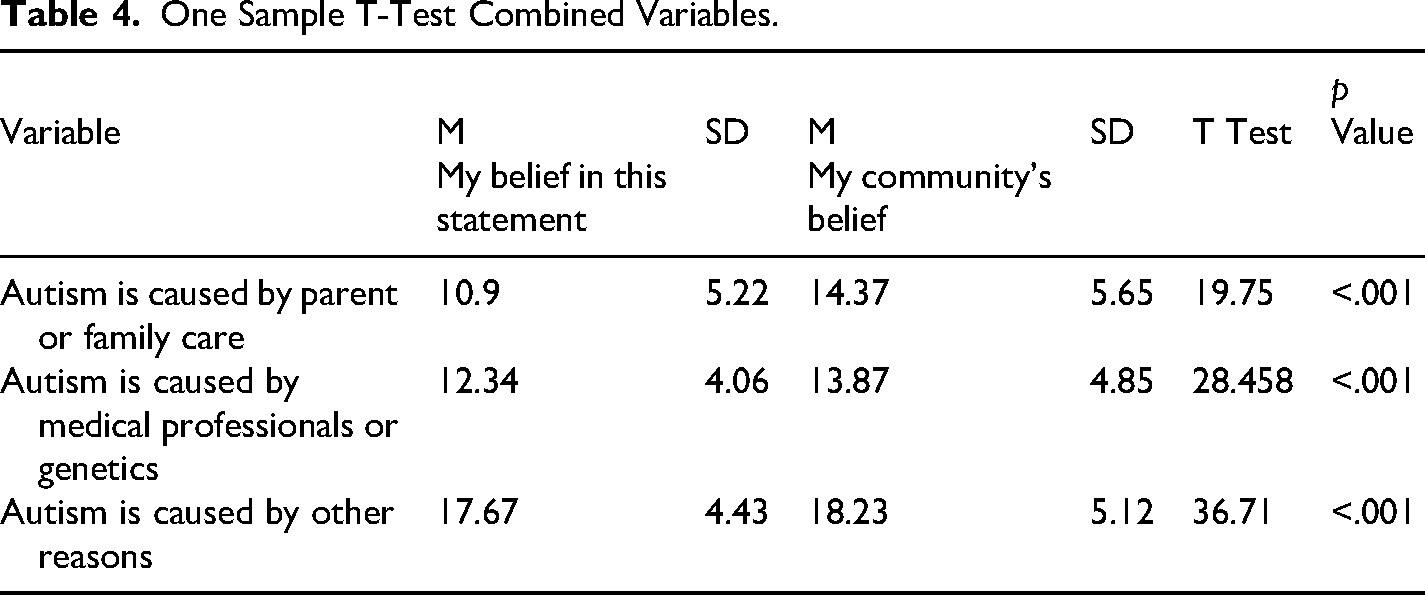
Quantitative analysis revealed a statistically significant difference in the caregivers’ perceptions of autism (causes, origin, and understanding) compared to their perceptions of their community's beliefs (see Table 3). To identify and understand any trends across the themes in the survey, we tested for significance between caregivers’ beliefs and those they perceived from the Sikh community, based on three broad themes of autism causes (i.e., caused by family, medical, and other causes) and all three themes revealed a statistically significant (<0.001) difference in the between caregivers’ own and the beliefs they perceived the Sikh community (see Table 4).
Individual and Community Beliefs One Sample T-Test.
One Sample T-Test Combined Variables.
Sikh Caregivers Perspectives on Educational Support
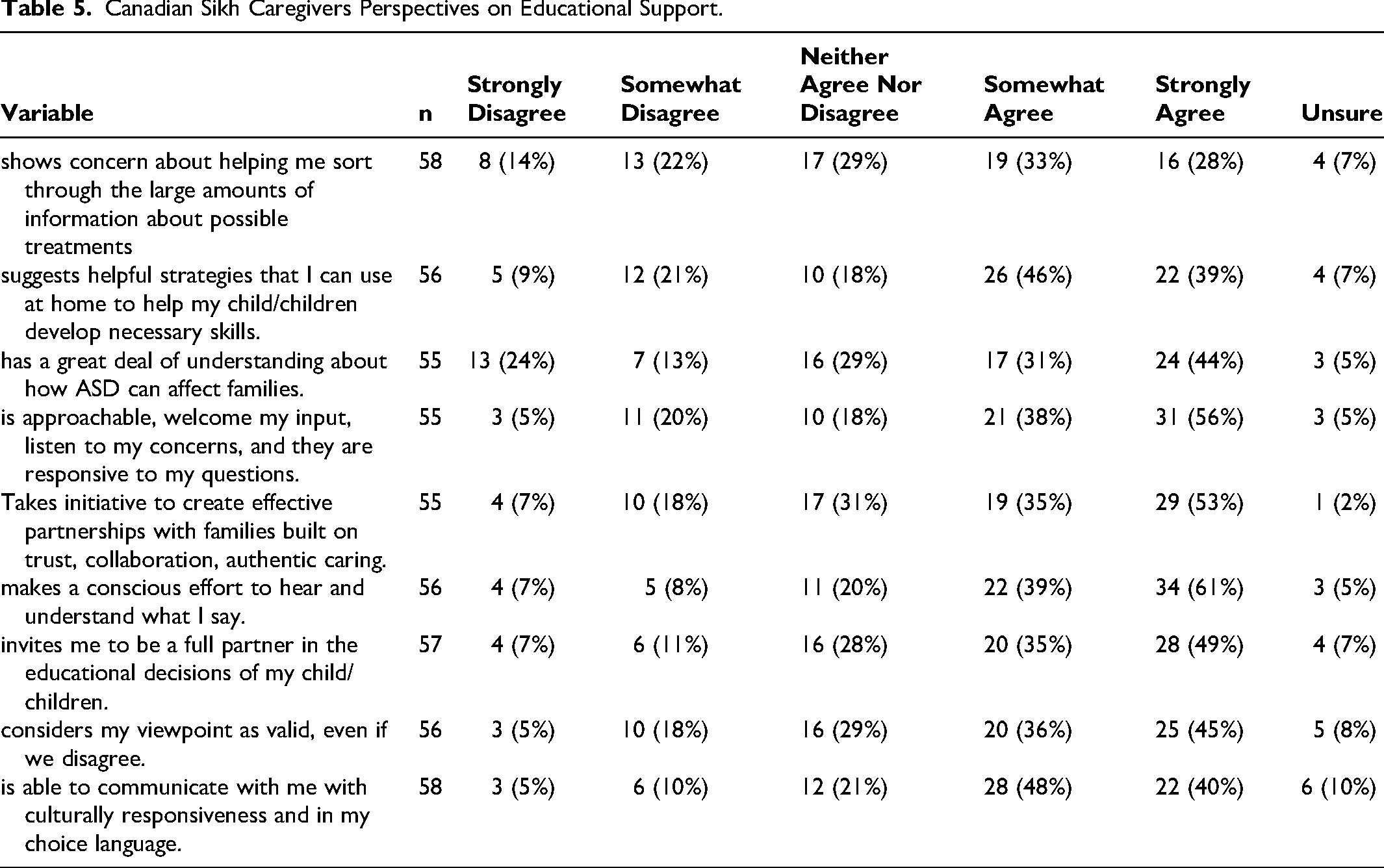
When asked about their perspectives on educational support and teacher attitudes, the caregivers reported generally positive relationships with their children's teachers, noting that teachers had made a conscious effort to hear and understand caregivers (61% strongly agree), were responsive to caregivers’ input (56% strongly agree), and worked to build teacher/caregiver partnerships (53% strongly agree or agree). In the area of culturally responsive teaching and communication, caregivers reported that teachers commonly communicated with cultural responsiveness and in the caregiver's preferred language (40% strongly agree and 48% somewhat agree, respectively). However, caregiver reported understanding of the impact of ASD on the family (24% strongly disagree) and in relation to support or treatment programs (14% strongly disagree) were variable (see Table 5).
Canadian Sikh Caregivers Perspectives on Educational Support.
Qualitative Results
The qualitative analysis revealed multiple intersecting themes that capture caregiver's experiences in the Sikh community. The three overarching themes included (a) stigma and acceptance, (b) religion and culture, and (c) system barriers. The theme of stigma and acceptance encompasses the sub themes of caregivers’ awareness and acceptance, cultural and generational awareness, and cultural stigma. The theme of religion and culture encompasses the sub themes of leaning into religion, leaning out of religion, and religious acts and autism. Lastly, the theme of system barriers encompasses the sub themes of culturally relevant support, barriers to Western systems of support, language barriers, and educational system barriers.
Stigma and Acceptance
Caregiver Awareness and Acceptance
The sub theme of caregiver awareness and acceptance captured participants’ articulation of their understanding of autism, which emphasized their knowledge both before and after their child's diagnosis. Most caregivers expressed limited to no knowledge of autism prior to their child's diagnosis, and many described that they only started to research autism supports after the diagnosis, which left them simultaneously searching for answers while also raising their autistic child. Some caregivers elaborated that accepting and understanding the child's autism diagnosis made them more compassionate towards others with less understanding of autism. One caregiver explained that, because the Sikh community generally has a limited understanding of autism, their child's diagnosis inspired them to become passionate about educating others in the community on autism and the challenges parents face. Similarly, another caregiver said, “my personal experience with autism has left me more empathetic toward others facing similar challenges.” Many of the caregivers resonated with this idea. When discussing the development of their own awareness and understanding of autism, many caregivers emphasized the need to accept autism in their own child in order to fully confront their own internalized stigma of disability. This then gave way for an expanded sense of openness and possibility. One caregiver shared by reframing the diagnosis as a part of who their child is, rather than something that needed to be “fixed,” they were better able to support their child. Many caregivers echoed the importance of awareness, acceptance, and understanding of autism in effectively support their autistic child.
In terms of information sources on autism, caregivers reported making use of various sources including online media (e.g., YouTube), parent support groups, and informal networks such as group chats or parent connections. These connective tools and experiences were found especially helpful for building an understanding of their child. The online resources also provided some helpful tools for behavioral support and communicating with educators to combat stereotypes for autistic students and families.
Generational Awareness
The sub theme of generational awareness includes caregiver discussions on autism awareness in their community across generations and the influences on their own experiences. Many caregivers mentioned generational differences in the acceptance of autism. They described younger generations as carrying less stigma and having more inclusive interactions with autistic children, whereas those from older generations generally focused on how autism should be cured. One caregiver explained it this way: My nephews, they're in their twenties now and dealing with [my autistic child] is perfectly normal for them. There's nothing wrong with him. He's just got a different way of doing things, and they have a better understanding of things than I think even what our generation did. Looking at our parents’ generation to them, it's like a complete taboo thing.
Cultural Stigma
The sub theme of cultural stigma, or negative attitudes held by members of a cultural group toward behaviors, conditions, or groups of people (Becker & Arnold, 1986) focused on the stigmatized perspectives, noted by caregivers, that persist in the Sikh cultural community. Cultural stigma sometimes contributed to caregivers’ own limited knowledge of autism. As one caregiver articulated, the lack of community awareness on autism contributed to his own initial difficulty in accepting his autistic child. As caregiver noted their child's autism would be described as a “mental issue” in India, their country of origin
Many caregivers sought support for their child outside of their culture because of the cultural stigma. One caregiver mentioned she had to look to places and people outside of the Sikh community, to gain knowledge and support for her autistic child as she wasn’t able to find resources within the community or religious centers like Gurdwaras (i.e., the Sikh's place of worship). Several described their attempts to “hide” their child's autism and their own feelings of blame when in Sikh community spaces. For example, one caregiver said, “The biggest thing with Sikhism is that whole thing of it's a taboo issue. Nobody wants to talk about it. Everybody just wants you to keep it hidden.” The stigma surrounding autism in the Sikh culture made it difficult for them to engage with the community.
Religion and Autism
Leaning Into Religion
Some caregivers felt they increasingly relied on, or leaned into, their religion for a sense of comfort by praying and relied on spiritual enlightenment, or Waheguru. As one caregiver said, I'm actually finding comfort and going back into the Gurdwara now, and like finding peace and praying, and just leaving it to Waheguru, and like just reconnecting with that part of my life.
Leaning out of Religion
In some cases, caregivers distanced themselves from, or leaned out, of their religion. This was often associated with a perceived lack of welcome or judgement of their child in religious spaces. One caregiver described Gurdwaras as not very accepting of her autistic daughter, noting there are “a lot of eyes rolling” when they are present. Another caregiver linked their own negative experiences to a belief held by some Sikh's that a mother's poor karma in a past life was the cause of autism. Several others echoed experiences with this karmic association and the resultant blame on mothers. One sibling caregiver shared that, while Sikhism was supportive of all, not all Gurdwaras or religious community members were. They highlighted a potential disconnect between the religion and common practice, noting that while Sikhism was supportive of all, not all Gurdwaras or religious community members were. She continued by describing the contradiction between religious teachings and practices that led her family to avoid going to the Gurdwara for some time. She says the religious teachings emphasize: Her wish was religious institutions and communities “just treat everyone equally. Give support to anyone who needs it. Some people need more support than others.”
Religious Acts and Autism
This sub theme highlights the intersection between religious acts and understandings of autism. One caregiver discussed how supporting her autistic child is an act of Seva, a core aspect of the Sikh religion that involves selfless service or acts of compassion for others. By engaging in acts of Seva, individuals receive raza, or acceptance in God's will. Although the Seva to raza connection is present in the religious teachings, caregivers did not always see it associated with support for autistic children. Seva is not just giving food. It's literally supporting people in any form possible. So, it's like, religiously, I think like there's nothing that's being like ‘don't support anyone who has mental health, illnesses, or health’, or anything like doing the complete opposite. It's just a good raza. Maybe like that focus a lot on the cultural norms of what the South Asian community expect when you go to a Gurdwara you're supposed to just have a certain etiquette there. That's more of the issue.
System Barriers
Culturally-Relevant Support
This sub theme focused on the barriers to accessing culturally-relevant support. Participants described a lack of culturally-relevant support and resources related to autism. Because many Gurdwaras were found to have limited to no resources on autism, caregivers sought resources outside of their cultural community. Therefore, they suggested bringing conversations about autism and disability (i.e., what they are, how to support) to religious places would create awareness and help create critical community connections. Specifically, they expressed a desire for resources within Gurdwaras such as information on autism, autism support groups, and more sensory-friendly physical spaces.
Barriers to Western Processes of Support
This sub theme highlighted the barriers Sikh caregivers face in accessing the Western-oriented systems of support in Canada. Despite mention of general system-level barriers for all autistic children, some discussed how being a Sikh caregiver could exacerbate those challenges. As a few caregivers noted, other, larger religions communities (i.e., Muslim, Christian) may receive more consideration in educational contexts, while the Sikh community is often not. As one caregiver noted, …I feel that if another community was stating this [cultural disconnect, limited educational support], I think their voice would be more heard rather than our Sikh [voices] are. You know they don't take our South Asian community that seriously, I would state. If it's somebody [else] or some other religion, [I’m] sure their voice would be heard, and changes would be made.
Language Barriers
This sub theme highlights the barriers some caregivers faced in supporting their autistic children due to language barriers, particularly in accessing information, support, and services. They noted issues in both verbal interactions and information access due to language barriers including both conventional English and specific educational jargon. Many desired both autism support services and informational resources in Punjabi. One caregiver described English as having a negative gate-keeping effect on support and resources acquisition. I do think being Sikh matters because I don't think the system is set up in our favor… because the people making the decisions don't look like us, so I think it does matter. And I have the privilege, I can speak English.
Discussion
Caregivers of autistic children commonly face systemic barriers to accessing supports and services, which is exacerbated for those from marginalized communities or diverse backgrounds (Iadarola et al., 2017; Khalil et al., 2025; Krakovich et al., 2016; Rivera-Figueroa et al., 2022; Samsell et al., 2022). But there is a lack of research focusing on the perspectives of Sikh caregivers of autistic individuals in Canada. We found that many Canadian Sikh caregivers described limited awareness of autism before their child's diagnosis, which they connected to the lack of awareness and cultural stigma in the Sikh community broadly. Canadian Sikh caregivers also felt their community stigmatized autism, which resulted in caregivers going outside of their community for knowledge and support. They emphasized Sikh religious teachings are inclusive, compassionate, and supportive of all individuals, but the challenge was the community's attitudes towards autism, where stigma and judgment persisted. Canadian Sikh caregivers discussed some barriers to accessing educational support, such as language barriers and the lack of culturally relevant supports.
From the results, Canadian Sikh caregivers primarily understand autism through their own lived experience with their child and post-diagnosis learning. Although cultural stigma existed, Canadian Sikh caregivers often developed more accepting and informed perspectives over time. Moreover, the findings highlight the complex interconnection of culture, religion, and stigma within the Sikh community. Across the quantitative and qualitative data, a consistent pattern of cultural stigma and the need for diverse culturally relevant support persisted. Quantitative results revealed statistically significant differences between the beliefs held by Canadian Sikh caregivers of autistic children and their perceptions of broader Sikh community beliefs. These findings, echoed in the qualitative data, underscore the need for greater community education on autism, including its origins and supportive strategies for families, to reduce stigma and debunk misconceptions. As noted in the literature, cross-cultural understandings of autism are shaped by social attitudes, stigma, and culturally defined norms of typical and atypical behavior (de Leeuw et al., 2020). Despite cultural stigma, Canadian Sikh caregivers agreed Sikhism's teachings reflect mutual support, equality, and acceptance and do not promote stigma. Rather, participants expressed that stigma surrounding autism was culturally rooted and not embedded in religious teachings. The experience of displacement in religious spaces is documented for autism parents of other faiths as well (Gilligan, 2013; Jegatheesan et al., 2010).
Canadian Sikh caregivers discussed some barriers to accessing educational support in Western systems such as language barriers and the lack of culturally relevant supports. As the literature suggests, immigrant and ethnic minority families often adapt or reconstruct aspects of their identity to align with Western educational norms (Lee & Zhu, 2021). The findings reflect broader evidence that minoritized caregivers frequently encounter structural inequities, including limited access to information and lack of equity in accessing institutions (Iadarola et al., 2017; Rivera-Figueroa et al., 2022). Engagement with the education system often requires families to navigate unfamiliar norms and expectations due to cultural mismatches and language barriers. For caregivers who already face systemic barriers such as limited institutional support and social isolation (Krakovich et al., 2016; Papoudi et al., 2021), the added burden of stigma, language barriers, or system barriers further exacerbates their challenges. While many caregivers described positive interactions with educators, suggestions for improvement included the provision of multilingual resources and increased cultural competence within school systems.
Implications for Practice
While many Canadian Sikh caregivers expressed positive relationships with their children's educators, there were inconsistencies in educators understanding of how disability and autism impact their lives, especially given their unique cultural identity. In addition to learning about autism in general, it is critical for educators to be sufficiently trained in intersectionality to fully understand how cultural stigma, religion, and community may impact families’ experiences and how they access services. For Sikh caregivers’, cultural, religious, linguistic, or social positions can overlap and result in unique challenges accessing knowledge and educational support for their autistic children (Crenshaw, 1991). Strengthening educator awareness on diverse experiences and intersectional challenges could equip educators with more tools and resources to support these families. Educators could work with cultural and religious institutions to create more community-based resources (Shurr et al., 2022). For example, for some Canadian Sikh caregivers, language is a barrier to accessing quality information about supporting autistic children, and providing translated materials to families could reduce these barriers. By developing authentic caregiver-educator relationships, both parties can benefit from developing understanding and empathy.
Limitations and Future Directions
This study has several limitations, including the sample size and reliance on self-reported data. While the survey received 113 responses and the focus groups included 11 participants, these numbers may not adequately represent the broader population of Sikh caregivers of autistic children in Canada. In addition, our recruitment strategy did not expand outside of the partnering organizations’ contacts, which may have limited the diversity of the sample and geographical scope, as they are mainly active in Ontario. Future researchers should aim to include a larger and more geographically diverse sample, with greater representation across North America to help capture a wider range of caregiver experiences across educational backgrounds, regions, and socio-economic statuses. In addition, although the focus groups were conducted with a community researcher fluent in Punjabi to translate if needed, the survey was not translated into other languages. This could potentially be a barrier for some individuals engaging in the survey portion of the study. Future research should offer translated versions of the survey to increase engagement.
With the online survey method, we could not verify the participants’ identities. Despite spam and bot protection protocols being followed, there may still be individuals who are not honest about their identity. Future research should more carefully consider the verification process and further ways to eliminate the risk of bots. Additionally, the survey relied on caregivers’ self-reports of perceived community beliefs and stigma. This approach places the burden of interpretation on the caregiver and may not fully capture how the broader community itself understands or expresses these beliefs. The caregiver's interpretation may not be accurate, and this limits the reliability of the data.
Footnotes
Acknowledgements
We would like to thank all of the participants for sharing their experiences with us.
Ethical Considerations
This study has been reviewed for ethical compliance by the Queen's General Research Ethics Board. Informed consent was obtained from each participant in the study. We gained consent for publishing the results.
Funding
This manuscript draws on research supported by the Social Sciences and Humanities Research Council Partnership Engage Grant [892-2023-2036].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
After the data has been held for 5 years, it will be securely deleted as per our letter of information to consenting participants.