
Abstract
Adolescents and young adults (AYA; ages 15–39) with acute leukemia have significant unmet supportive care needs. This pilot study integrated same-day palliative care (PC) into an AYA leukemia clinic, measuring symptom burden (SB) with validated symptom assessment tools at baseline, 3, and 6 months. Among 31 patients, moderate-severe symptoms included tiredness, anxiety, and poor appetite. AYAs experienced high SB and psychological distress, regardless of care phase or sociodemographics. With PC integration, tiredness and depression improved significantly; no symptoms worsened. Half of the PC visits led to management changes. Early integration of symptom-focused PC was feasible, value-adding, and well-received by patients.
Keywords
Background
Cancer in adolescence and young adulthood (AYA) is a non-normative life event with distinct long-term cognitive, physical, and psychosocial consequences unique to this age cohort. 1 AYAs with cancer, defined as ages 15–39 years at initial diagnosis, experience profound life interruptions including delays in educational and professional pursuits, 2 disrupted peer relationships,1–3 threatened fertility, sexual dysfunction, 1 financial toxicity, 4 and poor body image. 3 Despite survival gains within AYA oncology, underrecognized symptom burden (SB) and psychosocial challenges contribute to unmet supportive care (SC) needs, 1 leading to poor health-related quality of life 5 and high psychological distress. 6
AYAs with acute leukemia undergo highly intensive and lengthy treatments. However, comprehensive SB assessments and care models for delivering multidisciplinary SC in a non-end-of-life (EOL) setting have not been studied in this population. Early palliative care (PC) may help to identify and address unmet SC needs. Emerging adult7,8 and pediatric oncology9,10 literature shows benefits of early PC rather than initiation at the EOL. Early PC aims to identify psychosocial needs, guide symptom management, promote goal-concordant care, and assist with advanced care planning. This study aims to assess the feasibility of early PC integration with SB assessment in an AYA leukemia clinic.
Methods
Participants
Participants were recruited from the AYA leukemia clinic at the University of Chicago between February 2020 and September 2020. Eligible patients were diagnosed with acute leukemia between 15 and 39 years old and were undergoing active treatment or monitoring in survivorship. The University of Chicago IRB approved the study protocol. All patients provided informed consent.
SB assessment
Patient demographics and disease/treatment characteristics were collected via baseline survey and electronic medical records. The Edmonton Symptom Assessment System (ESAS), a 9-item instrument on a 10-point visual analog scale, assessed physical symptoms. Single-item symptom severity was scaled in the following manner: 0 = none, 1–3 = mild, 4–6 = moderate, and 7–10 = severe. 11 Psychological distress was assessed by the 18-item Brief Symptom Inventory (BSI-18), an instrument capturing symptoms related to the domains of depression, anxiety, and somatization. Items are rated on a 5-point Likert scale from 0 (not at all) to 4 (always). Domain scores (each with a maximum score of 24) are summed to determine the Global Symptom Index (GSI) of distress score (maximum score of 72) with gender-specific cutoffs for caseness correlating to GSI scores >10 in men and >13 in women. 12 Both instruments are validated within adult oncology populations and have been applied in AYAs.13–15 SB was assessed at baseline, 3 months, and 6 months from the initial survey. Responses were categorized by phase of care: intensive therapy (frontline or salvage chemotherapy), less intensive therapy (maintenance), post-SCT (<1 year postallogeneic transplant), and off-therapy (in survivorship).
Early integration of PC
A PC led SC team was embedded into the existing weekly AYA clinic infrastructure to provide symptom-focused care. Preexisting interdisciplinary clinic services included psychology, pharmacy, social work, and AYA navigation. All participants presenting for routine oncologic care were referred to the SC team for symptom management. A palliative medicine physician provided same-day PC consultation in a shared clinic space with options for as-needed follow-up, including embedded and stand-alone in-person return visits and telehealth.
Early PC integration was considered feasible if >75% of AYAs completed the initial PC consultation. A 7-item anonymous questionnaire on a 5-point Likert scale was administered after 6 months to assess AYAs’ acceptability of early PC.
Statistical analysis
We aimed to enroll all eligible AYAs from the AYA leukemia clinic, which sees approximately 60 new patients annually and had roughly 100 AYAs in curative treatment at the time of study enrollment. Enrollment was challenged by COVID-19-related restrictions, infection concerns, and health care system strains.
Descriptive statistics were calculated for patient demographics, disease characteristics, and symptom assessment scores. The nonparametric Wilcoxon rank-sum test was conducted to detect changes in SB scores between baseline and 6 months, as well as associations between demographic/disease characteristics and ESAS scores. To detect if there was an association between care phase and SB scores, a linear mixed-effect model accounting for intraclass correlation from repeated measures was conducted, utilizing predictor marginal mean values. The care phase was collected at every assessment. Statistical significance was considered as p < 0.05. Analyses were conducted using STATA 15.1.
Results
Patient demographics
Forty-six patients were approached for study enrollment. Thirteen (28%) patients declined participation, 2 (4%) consented but were later deemed ineligible, and 31 (67%) accrued onto the study. All participants completed the baseline symptom assessment surveys and 25 (80%) completed 6-month surveys; demographic characteristics are summarized in Table 1. Thirty (97%) patients completed the initial PC consultation; one patient died prior to consultation. The median age at baseline was 29 years (range 18–43), with a median age at diagnosis of 27 years (range 15–38). Most were male (52%), white (58%), or college graduates (51%). The most common diagnosis was acute lymphoblastic leukemia or lymphoblastic lymphoma, and the majority were receiving intensive frontline or salvage chemotherapy at baseline. Eighteen (58%) patients had relapsed or refractory disease at baseline.
Patient Characteristics at Baseline Assessment
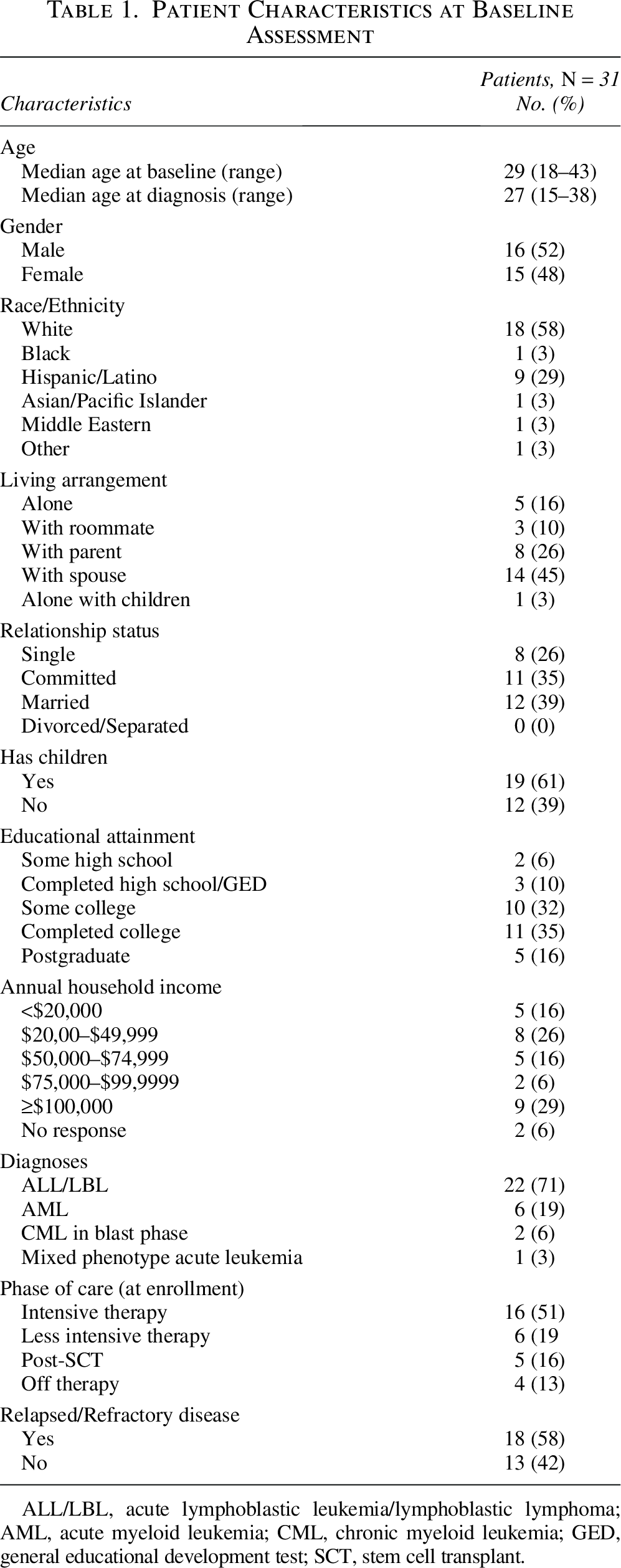
ALL/LBL, acute lymphoblastic leukemia/lymphoblastic lymphoma; AML, acute myeloid leukemia; CML, chronic myeloid leukemia; GED, general educational development test; SCT, stem cell transplant.
Symptom burden: ESAS
At baseline, 48% reported ≥1 severe symptom on the ESAS (defined as score ≥7), with poor feeling of well-being as the most reported severe symptom (n = 7/31, 23%). At 6 months, 56% reported ≥1 severe symptom, with poor appetite being the most common (n = 9/25, 36%). Breakdown of ESAS scores at baseline and 6 months is in Table 2. No median ESAS scores worsened at 6 months compared with baseline, while tiredness (p = 0.02) and depression (p = 0.01) scores significantly improved. At baseline, common moderate-to-severe symptoms (defined as ESAS score >3) included poor feeling of well-being (61%), tiredness (58%), poor appetite (45%), and anxiety (42%). At 6 months, these symptoms persisted at levels >40%.
Prevalence and Severity of Physical and Psychological Symptom Burden at Baseline and 6 Months
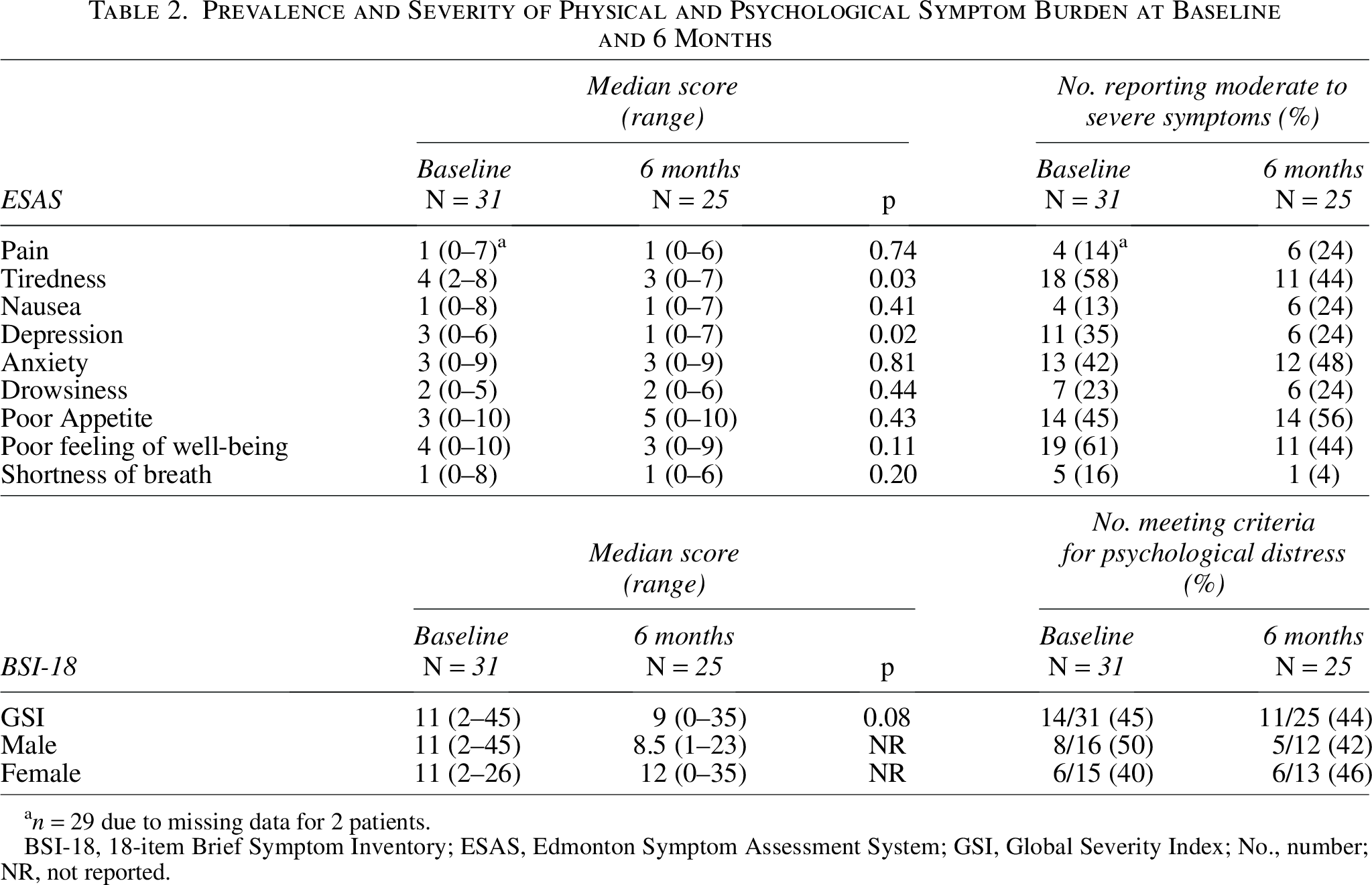
n = 29 due to missing data for 2 patients.
BSI-18, 18-item Brief Symptom Inventory; ESAS, Edmonton Symptom Assessment System; GSI, Global Severity Index; No., number; NR, not reported.
Symptom burden: BSI-18
BSI-18 GSI scores at baseline and 6 months are reported in Table 2. At baseline, 50% of men and 40% of women reported high psychological distress, with median GSI scores of 11 for both sexes. At 6 months, 42% of men and 46% of women reported high psychological distress with median GSI scores of 8.5 and 12, respectively.
Effect of phase of care on SB
The impact of care phase on SB is summarized in Table 3. Overall, ESAS scores were similar regardless of care phase. Patients in intensive therapy reported worse feelings of well-being than those in less intensive therapy (p = 0.02); however, being off therapy did not result in lower ESAS scores (p = 0.42). In fact, off-therapy patients reported more tiredness than those in less intensive therapy (p = 0.03).
Impact of Phase of Care on Physical Symptom Burden
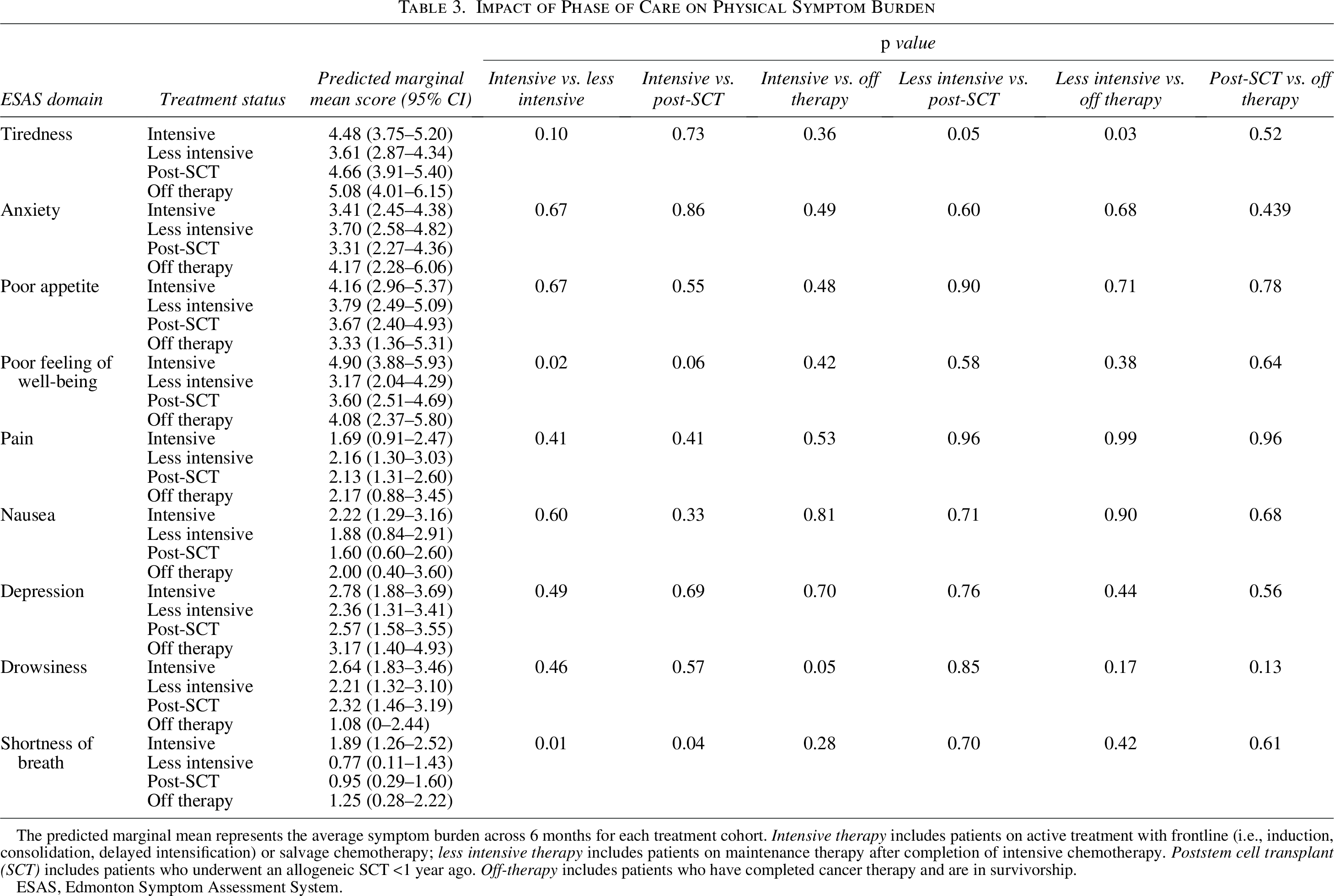
The predicted marginal mean represents the average symptom burden across 6 months for each treatment cohort. Intensive therapy includes patients on active treatment with frontline (i.e., induction, consolidation, delayed intensification) or salvage chemotherapy; less intensive therapy includes patients on maintenance therapy after completion of intensive chemotherapy. Poststem cell transplant (SCT) includes patients who underwent an allogeneic SCT <1 year ago. Off-therapy includes patients who have completed cancer therapy and are in survivorship.
ESAS, Edmonton Symptom Assessment System.
Effect of cancer and sociodemographic characteristics on SB
The impact of cancer characteristics and sociodemographics on the change in median ESAS scores from baseline to 6 months is summarized in Supplementary Tables S1 and S2, respectively. The change in ESAS scores was similar regardless of sociodemographic or baseline cancer characteristics, including race, level of education, relationship status, presence of children, living arrangement, household income, initial response to therapy, having relapsed/refractory disease, or having central nervous system involvement (all p > 0.05). Only age ≥30 was associated with a statistically significant worsening of anxiety (p = 0.02).
Impact of early PC integration
Over 6 months, 30 patients received symptom-focused PC. There were 81 total PC encounters over 16 combined clinics, with an average of 5 patients (range 1–8) per clinic. Patients received an average of 2.7 (range 1–6) PC visits. Approximately 50% of encounters resulted in adjustments to medical management, with the most common symptoms including pain, anxiety, neuropathy, insomnia, muscle cramps, depression, and nausea. The SC team identified critical issues unbeknownst to the oncology team, including medication dosing errors, serotonin syndrome, and medication nonadherence.
Fifteen patients (50%) completed the perceptions of PC survey. Most felt that PC was a positive addition to overall care (100%) and was helpful for treating symptoms (100%), making treatment decisions (n = 14, 93%), providing hope (n = 12, 80%), and coping with their illness (n = 13, 87%). Twelve patients (80%) recommended a SC visit near the initial diagnosis of serious illness.
Discussion
This is the first study to report trends and factors associated with high SB and integrate early PC into oncologic care for AYAs with acute leukemia in a non-EOL setting. It was feasible to characterize SB throughout the care continuum and introduce symptom-focused PC in an impactful way. AYAs reported high SB irrespective of care phase, including survivorship, and there was no significant difference by sociodemographic characteristics. Moderate-to-severe symptoms across the care continuum included tiredness, anxiety, poor appetite, and poor feeling of well-being, which is consistent with the literature in AYAs with cancer. 16 Although there was a trend toward GSI improvement on the BSI-18 (p = 0.08), psychological distress remained high at 6 months (44%) despite most having completed intensive treatment. This is also congruent with prior studies demonstrating substantial psychological morbidities in AYAs with cancer15,17 and higher burden of fatigue and anxiety in AYA survivors compared with older survivors and age-matched controls. 18 While high SB was anticipated during intensive chemotherapy, the persistence into maintenance therapy and survivorship was surprising and may reflect cumulative short and long-term toxicities associated with multiagent chemotherapeutic regimens,19,20 ongoing psychosocial challenges, 21 heightened fear of recurrence linked to greater distress and somatization, 22 and pandemic-related stressors.
Despite positive impacts on medical management and acceptability among AYAs, early PC did not improve most moderate-severe symptoms at 6 months, including tiredness, anxiety, poor appetite, and poor feeling of well-being. Several commonly addressed symptoms (e.g., neuropathy, muscle cramps) uncovered by PC were not represented on the ESAS. Notably, tiredness is prevalent and persistent among AYAs, with studies noting moderate fatigue lasting one year after diagnosis.16,23 Concurrent high anxiety, as seen in our cohort, has been associated with prolonged duration of other severe symptoms. 16
The above moderate-severe symptoms are nonspecific and often challenging to address pharmacologically, underscoring the need for a multidisciplinary approach that includes PC. One potential hypothesis for symptom persistence across different care phases is that the underlying mechanisms may shift over time; for example, a poor feeling of well-being may result from intensive chemotherapy side effects, hormonal changes, evolving psychosocial challenges, or increased anxiety during the survivorship transition.15,17
Extreme social isolation, disruptions in daily routines, fragmented oncologic care, and concerns related to contracting COVID-19 had a substantial impact on the mental health of AYAs with cancer, contributing to worsening psychological distress and anxiety, particularly among those with hematological malignancies. 24 It is plausible that PC integration with access to telehealth follow-up may have mitigated worsening SB that would have otherwise occurred during this time.
In general, early PC integration was well-received by most AYAs. Future research with extended follow-up is needed to determine whether clinic-based symptom assessments can appropriately cue providers to address unmet SC needs, identify barriers to care, and assess the longitudinal impact of integrated SC in AYAs with cancer. Larger studies exploring the impact of comprehensive AYA oncologic care models with embedded SC and psychosocial services on SB are warranted.
Strengths and limitations
Strengths of this study include the unique integrated clinic model of embedding PC services into a preexisting AYA-focused leukemia clinic and the use of validated SB measures across multiple time points. Limitations include the small sample size and limited power, data collection from a single institution, heterogeneous times of assessment relative to care phase, and use of English-only instruments. Study accrual occurred during the COVID-19 pandemic, which significantly impacted enrollment and may have confounded patient-reported SB. The lack of a randomized control group limits meaningful conclusions regarding the impact of early PC on SB.
Conclusion
AYAs with acute leukemia experience high SB independent of care phase or sociodemographic characteristics. This study highlights both the feasibility of early PC integration into routine oncologic care and the need for routine, standardized SB assessment in AYAs throughout the cancer care continuum, including during survivorship. There remains an unmet need for symptom management, and future research is needed on how to best deliver AYA-specific SC.
Authors’ Contributions
A.Y.W., C.D., and F.J.H. conceived the study. A.Y.W., F.J.H., K.S.H., and W.S. contributed to study design. A.Y.W., S.E.M., C.H., K.S.H., W.S., A.D., J.M., and T.H. contributed to data collection. A.Y.W., S.E.M., and C.H. contributed to data analysis and drafting the article. All authors contributed to article revisions and approved the final version for submission.
Footnotes
Author Disclosure Statement
No interests to disclose.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.