
Abstract
Purpose:
Adolescents and young adults (AYAs; 15–39 years) with sarcoma undergo intensive therapies during a vulnerable time in their lives. We aimed to characterize the unmet needs of AYAs with sarcoma to inform strategies that improve outcomes.
Methods:
We used purposive sampling to conduct semistructured focus groups of AYAs with sarcoma treated primarily at Dana-Farber Cancer Institute. Focus groups were conducted via Zoom by trained moderators and focused on experiences with treatment, decision-making, care communication, supportive care services, and the effects of cancer on daily life. Focus groups were audio recorded, transcribed, and thematically analyzed via a team-based approach.
Results:
We conducted four focus groups with 20 participants (16–34 years) adolescents, emerging adults, young adults, and those with recurrent/metastatic disease. Participants confirmed that sarcoma and its treatment affected their physical, emotional, social, and economic health. We identified three key overarching themes: (1) Disruption to agency and mobility negatively impacted well-being and social relations; (2) The transition from “active treatment” to “surveillance” was fraught as it often magnified challenges of “returning to normal” and loss of autonomy; and (3) Additional supports and services may help address identified unmet needs and gaps in care. Participants expressed a desire for support services to be introduced earlier to help facilitate independence.
Conclusion:
AYAs with sarcoma experience loss of agency, mobility, and impaired well-being due to their diagnoses and treatments. They desire early introduction of supportive services, and care teams can proactively address these challenges by connecting patients with targeted services, resources, tools, and community.
Introduction
Roughly 90,000 adolescents and young adults (AYAs; 15–39 years) are diagnosed with cancer each year in the United States. 1 AYAs face cancer during a critical period of personal and professional development, which can magnify the short- and long-term effects of treatment.2–7
Sarcomas are rare cancers of the connective tissues that disproportionately affect AYAs.8,9 AYAs with sarcoma have inferior survival compared with children10–14 or AYAs with other cancers.11,15,16 Sarcomas are commonly treated with intensive multimodal therapy including high doses of chemotherapies, which can predispose to heart disease, neuropathy, hearing loss, infertility, sexual dysfunction, and second cancers.17–19 Surgery and radiation often result in reduced mobility, imbalance, pain, and chronic wounds.17–19
AYAs with sarcoma often face functional disabilities that affect return to school and work.20–22 They are at high long-term risk for depression, anxiety, distress, fatigue, and poor quality of life.23–25 The informational, emotional, and practical needs of AYAs with sarcoma are frequently unmet.2,26 The specific effects of their diagnoses and treatments on their lives, as well as desired interventions to address them, are not well understood.
To address this knowledge gap and aid the development of patient-informed, multidisciplinary care strategies, we conducted a qualitative focus group study that aimed to explore and understand the unique challenges, existing supports, and unmet needs of AYAs with sarcoma.
Methods
Study design and participants
Focus groups were conducted with English-speaking AYAs diagnosed with sarcoma and treated primarily at Dana-Farber Cancer Institute (DFCI)—patients were recruited from both medical and pediatric oncology clinics. Exclusion criteria included non-English speakers or missing contact information. Purposive sampling was used to ensure a diversity of perspectives, including treatment location (pediatrics vs. medical oncology), life stage, and disease status. Eligible participants were approached by research staff after obtaining permission from treating oncologists. Informed consent was obtained from all the participants involved in this study. The study was deemed as Quality Improvement/Measurement activity by the DFCI Office for Human Research Studies and, therefore, exempt from full DFCI Institutional Review Board review.
Data collection
Four focus groups were conducted via a secure, HIPAA–compliant Zoom platform by trained moderators. The moderator guide was developed through an iterative team-based process based on a review of the literature and clinical and methodological expertise of the team (Supplementary Appendix A1). The guide focused on participants’ experiences with treatment, decision-making, care team communication, supportive care services, and the effects of cancer on daily life. As the goal across all groups was to explore and understand the unique challenges and unmet needs of AYAs with sarcoma, the same guide was used for all groups. With the guidance of clinical experts on the team, there were small adjustments made in wording to bring sensitivity to the topic of survivorship and treatment completion in the metastatic group.
Considering the sampling approach and exploratory nature of the research aims, the study team anticipated that four focus groups would be sufficient to achieve meaning saturation. 27 Because AYAs comprise multiple life stages, 28 patients were distributed into focus groups based on age/life stage (adolescence, emerging adult, and young adult), and a separate focus group for patients with recurrent/metastatic disease receiving treatment with noncurative intent. The composition of the four focus groups sought to best facilitate a meaningful discussion between participants by bringing together relevant subgroups, with goal to leverage similarities to build rapport among each focus group and allow the discussion to dive deeper into the diversity of their lived experiences and perspectives.
Focus groups were debriefed, and transcripts were reviewed by the team during data collection. Recruitment ceased when the team determined that meaning saturation was reached.29,30 Participants received a $25 Amazon gift card as a token of appreciation.
Data analysis
Focus groups were audio-recorded and transcribed. Data was analyzed via a collaborative team-based approach to thematic analysis.29,30 A combination of inductive and deductive approaches were used to code and analyze the data. 31 A comprehensive codebook was iteratively developed using deductive codes from the moderator guide, inductive codes from transcript review, and a review and discussion with the full team. 32 The codebook was then tested on two transcripts and discussed with the team to facilitate consistent interpretation and application. A finalized codebook was applied to all transcripts by a primary coder (BM) and reviewed by one of two secondary coders (AR, BNC). Coding uncertainties and discrepancies were addressed in recurrent coding meetings. Coded data were summarized, reviewed, and iteratively discussed. The team synthesized and analyzed the code summaries, identifying overarching patterns and themes and comparing themes across subgroups. Initial themes were discussed and refined through asynchronous review and edits, followed by synchronous team meetings. Coding and analysis were supported by NVIVO software (Lumivero).
Results
There were 20 participants (16–34 years) included in the four focus groups, with five participants per group: recurrent/metastatic (FG1), adolescent (FG2), emerging adult (FG3), and young adult (FG4). Participant characteristics are highlighted in Table 1.
Participant Demographics
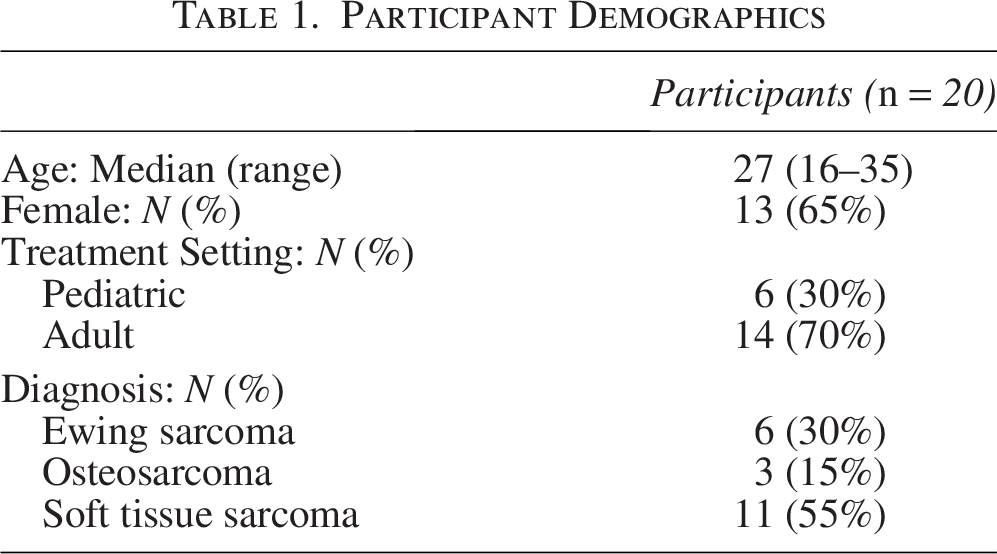
Participant Demographics
Participants came from pediatric or adult/medical oncology treatment settings. These different settings emerged as a key discussion point, where participants identified the pros and cons of each setting in relation to their overall treatment experiences. Some participants appreciated pediatric centers for their planned activities and interactive staff, which promoted a more cheerful and enjoyable treatment experience. However, sharing space with young children in a child-oriented environment that lacked privacy made some feel out of place. In the adult/medical oncology space, participants appreciated the approaches of the teams, perceived autonomy, and more individualized spaces. However, some noted a sense of loneliness and a lack of activities during long clinic days. Participants also observed that they were either the oldest or the youngest in their respective setting.
Across these care settings, we identified three key themes: (1) Disruption to agency and mobility negatively impacted well-being and social relations; (2) The transition from “active treatment” to “surveillance” was fraught as it often magnified challenges of “returning to normal” and loss of autonomy; and (3) Additional supports and services may help address identified unmet needs and gaps in care. Themes, subthemes, and representative quotes are shown in Table 2.
Themes, Subthemes, and Representative Examples
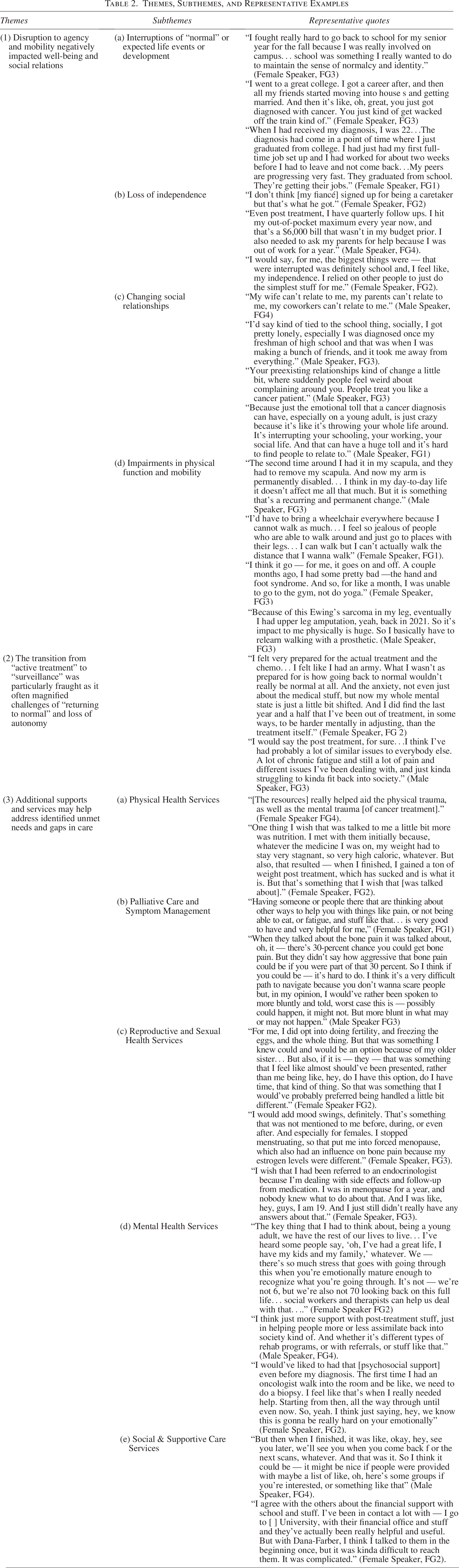
Theme 1: Disruption to agency and mobility negatively impacted well-being and social relations
Participants shared that their rare, life-altering diagnoses and their intensive multimodal treatments had negative impacts on their physical, emotional, social, and economic well-being. In particular, participants shared profound disorientation and distress from interruptions to meaningful, expected life milestones, a loss of independence, marked changes to relationships with family and friends, and impairments in physical function.
Participants across all groups described disruption to milestones commonly associated with adolescence and young adulthood and felt an inability to return to normalcy.
Treatment interrupted educational pursuits and careers. Prolonged absences led to challenges, such as needing to attend classes online. Participants also discussed interruptions to meaningful experiences, such as attending prom, joining a sorority, and traveling. Others shared difficulties beginning, remaining, and advancing in their careers, and some changed career paths. Those who returned to school or work found it difficult to explain time gaps, tell peers why they had left, or explain their altered appearance. Conversely, some participants viewed leaves of absence as opportunities to spend more time with family.
Participants shared that when it was possible, “continuing [to do] what [they] love doing,” helped preserve their identity outside of “cancer patient” (Female Speaker, FG2). Others shifted life goals, which gave participants a greater sense of autonomy.
Participants felt supported when clinicians tailored treatment and appointment schedules to accommodate for attending meaningful activities and milestone events. Other participants hoped to attend social milestones such as high school graduation, prom, and college activities. One participant said that attending his young daughters’ weddings in the future was a mantra throughout treatment. Clinician support was particularly meaningful when parents or caregivers were hesitant to support returning to school or other events.
Loss of independence
Participants described independence and self-sustainability as priorities, which were represented as living independently or having financial independence. However, many participants felt dependent on family for physical and financial support during and after treatment. Some previously independent participants moved in with their parents and received assistance with daily activities, such as bathing, walking upstairs, and traveling to appointments. Others described altered dynamics with significant others; one participant remarked that it was “humbling” to receive sponge-baths from his wife (Male Speaker, FG4).
Changing social relationships
Participants reported altered existing relationships and challenges navigating new ones. Many school-age participants experienced shifts in and loss of friend groups after prolonged absences from school, sports, and other activities. Some believed that friends distanced themselves due to discomfort in addressing their diagnosis and not knowing how to provide support. Some participants were reluctant to meet new people due to fear of being seen as a “sick person.” Rather, they “focused on other ways to stay connected” with those who “didn’t really treat [them] different” because it gave them a feeling of normalcy (Male Speaker, FG3). They felt the friendships that endured became deeper.
Participants also emphasized being supported and being understood were different, which contributed to feelings of isolation. They felt that despite loving support, many people were unable to relate to their experiences, and well-intentioned support was sometimes not helpful. One participant said that her family was in “denial of what [she] was going through, and they don’t know how to be supportive…”, attributing her chronic fatigue to laziness (Female Speaker, FG4).
Impairments in physical function and mobility
Key priorities for participants were being physically active and experiencing one’s youth free from disease and disability. Most participants were frustrated by the impacts of sarcoma treatment (e.g., amputations) on physical abilities. While some participants were able to resume previous activities with accommodations, others were unable. They described amputations, chronic pain, scarring, and bone pain as significantly impacting their ability to regain physical function. Some participants adjusted to physical changes more easily than anticipated; others were surprised by the magnitude of their pain or the extent of tissue removal. Participants felt these limitations challenged their sense of identity.
Theme 2: The transition from “active treatment” to “surveillance” was particularly fraught as it often magnified challenges of “returning to normal” and loss of autonomy
Participants felt underprepared for the prolonged and often non-linear nature of treatment and recovery that sometimes required additional surgeries, treatments, and potential relapse. Conversely, those who faced recurrence or metastasis felt more prepared for what to expect from subsequent treatments.
Post-treatment care was characterized as “murky.” Participants felt a lack of support and guidance and desired more structured follow-up. Some described health management challenges, including scheduling follow-up appointments, imaging, and re-establishing primary care. One participant remarked it became a “headache” to coordinate appointments between clinics (Female Speaker, FG3).
Physical effects such as pain, fatigue, hormonal changes, and weight gain were also highlighted as post-treatment struggles. A female participant experienced treatment-related menopause and felt she had limited support in management.
The emotional impact was particularly pronounced after treatment when participants were expected to return to “normal.” Many felt that they struggled to fit back into society. One male respondent discussed developing body dysmorphia due to scars from multiple procedures and loss of muscle mass. Another participant shared that his support networks understood his initial cancer diagnosis and treatment more than “some of these aftereffects people get from it… for whatever reason, it’s just harder for people to understand or to relate to” (Male Speaker, FG4). Recreating relationships was also difficult; one participant remarked that “creating that relationship [with her children] coming out of the treatment” was her hardest challenge (Female Speaker, FG4).
Theme 3: Additional supports and services may help address identified unmet needs and gaps in care
Participants identified helpful resources in addressing challenges; however, they were not introduced in a standardized manner and were used variably. Participants expressed a desire for supports and services to be introduced earlier, as well as revisiting/reoffering of supports over the disease trajectory.
Physical health services
Participants preferred physical support resources that promoted well-being and bodily autonomy. During long infusion days, they sought activities such as art therapy, yoga, massage therapy, and Reiki. They also expressed interest in services available on non-infusion days, including physical therapy, integrative health (massages, acupuncture), and nutrition services. Several participants noted that insurance coverage affected their ability to access physical therapy.
Palliative care and symptom management
Many participants described positive experiences with palliative care. However, utilization of these services depended on time of referral; those who did not receive referrals at time of initial diagnosis wished they were connected to palliative care earlier.
Reproductive and sexual health services
Participants discussed hormonal, sexual health, and reproductive issues, expressing a desire for more explicit discussion about treatment effects on fertility and sexual health. They struggled with low testosterone, menopause, and hormone fluctuations, and wished they had received more information, guidance, and support. Participants also wanted discussions on fertility options, with some recounting having to advocate for themselves regarding fertility and were surprised these conversations were not initiated by the care team.
Mental health services
The shock and uncertainty of having sarcoma took an emotional toll on participants; they expressed being scared, stressed, and suffering from anxiety. For some, the emotional impact was most pronounced after treatment, when they described that physical wounds may have healed, but their ability to return to “normalcy” was disrupted.
Participants wished that the emotional impact of cancer and its treatment was made more explicit. Mental health services that participants found helpful included social work, therapy, and care navigators. These resources helped participants process complex emotions, build coping strategies, and streamline health information. Multiple participants also described that mental health support was critical for adjusting to life after treatment. One participant explained that his therapist was essential in processing how cancer impacted his family because building a relationship with his children after treatment was “the most difficult part of my treatment, outside of the treatment itself,” (Male Speaker, FG4).
Survivorship groups were also helpful; one participant said the emotional support he received from the head of the young adult cancer program was “far and away the biggest and most helpful support,” (Male Speaker, FG1). Others described a similar sense of connection and community when forming relationships with other survivors, describing these connections as “a good feeling because it’s that not-alone feeling” (Male Speaker, FG4).
Introduction and utilization of mental health support varied. Some participants were referred to mental health services at time of diagnosis, while others did not receive referrals until later. One participant described being introduced to an “avalanche of information and things [they] could do to help [themselves],” early in their cancer journey, but opted out due to being overwhelmed (Female Speaker, FG3). Some participants also highlighted the desire for friends and family to receive psychosocial support.
Social and supportive care services
Even when a need was identified, participants said that discussions about support services were overshadowed by discussions about oncology care. Participants desired social services and resources to address life interruptions. These included financial services (e.g., guidance with insurance selection, support with out-of-pocket costs, and help maintaining higher education scholarships), accommodation support when traveling for appointments, and clear access to subspecialty and survivorship care. Similarly, suggested supportive resources included referrals to nutrition services, integrative medicine, support groups, and offering on-demand online content to introduce additional resources. One participant’s oncologist referred all patients to a social worker for an initial consult; the participant continued using this service “throughout treatment and that was really helpful,” (Female Speaker, FG2).
Discussion
In this focus group study, we found that AYAs with sarcoma experience loss of agency, mobility, and well-being as a result of their diagnoses and treatments. The transition from “active treatment” to “surveillance” was particularly difficult, highlighting the challenges of “returning to normal”. Participants also shared a desire for early introduction to and regular revisiting of supportive services, resources, tools, and community.
Prior work has established AYAs with sarcoma have reduced quality of life, poor psychosocial outcomes, and hindered social functioning.24,25,33 Our study identified drivers of these negative effects, including: loss of independence and autonomy, a lack of “return to normalcy,” changes to existing relationships and social behaviors, and challenges when transitioning from “active treatment” to “surveillance.” Chronic impairment to physical health, function, and mobility was recurrently expressed as a major challenge and unmet need that is potentially unique to AYAs with sarcoma, due to the debilitating and disabling nature of extremity and chest/abdominal wall sarcomas and the intensity of local therapies, which often includes high-doses of chemotherapy, radiation, and major limb-sparing surgeries or amputations.17–19 The loss of function and mobility is also directly related to the general sense of loss in independence and changing social relationships, such as with sports teammates. Understanding and addressing the complex interplay of these factors, with an emphasis on promoting long-term physical health and functional resiliency, can help AYAs with sarcoma and navigate their physical and psychosocial challenges.
Additionally, prior work has also established several unmet service needs of AYAs with cancer, including those with sarcoma, such as information resources and emotional and practical support.2,26 Our study adds valuable insights by collating recommendations directly from participants on how best to support them. Some of our results were similar to previous findings, such as the need for more reproductive, sexual health, and mental health services. However, some results were unexpected, such as participants expressing a clear desire for early involvement of palliative care and symptom management services. These findings signal that AYAs with sarcoma are at high risk, compared with other AYAs, for needing comprehensive support from pain and palliative care providers for cancer-related or chronic pain, due again to the nature of sarcomas and their treatments. In addition, AYAs with sarcoma may benefit from palliative care and mental health provider involvement given their high risk for recurrence and reduced overall survival compared to AYAs with other cancers and to children with sarcoma.11–13,16 Overall, AYAs with sarcoma emphasized the importance of early introduction of support services, to help maintain a sense of autonomy and normalcy, and address care needs that are less expected or unique to AYAs with sarcoma.
Oncology care teams can act on these findings to proactively offer individualized support in a standardized fashion to improve outcomes. However, while participants advocated for early introduction to supports, many were not ready to utilize them until later, suggesting that supports must be reintroduced during the treatment trajectory. At our institution, the data collected from these focus groups directly informed the creation and operation of our Adolescent and Young Adult Sarcoma Program (AYASP), which aims to assess patient-reported needs proactively, connect patients to helpful services, and develop evidence-based programs to address key areas of concern, such as early referrals to physical rehabilitation and to palliative care and development of personalized exercise programs to support physical function and autonomy. Every AYA with sarcoma in the DFCI AYASP is referred to an AYA patient navigator at time of initial consult, who reviews available resources specific to AYAs with sarcoma. These focus group findings will continue to inform future research and practice changes.
Our study has several limitations. Participants were recruited from a single, well-resourced cancer center, which may affect generalizability. Additionally, only English-speaking patients were eligible to participate, which may underestimate the needs of this population. However, as DFCI includes a pediatric oncology center (Jimmy Fund Clinic) and an adult sarcoma center, we were able to recruit patients treated in both pediatric and medical oncology treatment settings. Purposive sampling also aimed to ensure a diversity of perspectives, including treatment setting, life stage, and disease status. Interviews were conducted via Zoom to reduce challenges due to geography, and moderators were trained to ensure all participants felt valued and comfortable to elicit responses from everyone.
Conclusion
AYAs with sarcoma have rare, life-altering diagnoses and undergo intensive multimodal treatment that negatively impacts their long-term physical, emotional, social, and economic health. Their lives are interrupted and forever changed, they miss meaningful milestones, their independence and mobility are threatened, and their relationships are profoundly altered. By proactively addressing their unmet needs via connection to services, resources, tools, and community, providers may be able to help AYAs with sarcoma navigate these challenges, foster resilience, and preserve independence.
Authors’ Contributions
V.V.: Formal analysis, writing—original draft, writing—reviewing and editing. B.M.: Formal analysis, writing—original draft, and writing—reviewing and editing. A.R.: Conceptualization, methodology, formal analysis, and writing—reviewing and editing. B.N.-C.: Conceptualization, methodology, formal analysis, and writing—reviewing and editing. S.G.: Conceptualization, methodology, formal analysis, writing—reviewing and editing, and supervision. D.S.S.: Conceptualization, methodology, formal analysis, writing—reviewing and editing, and supervision. K.A.G.: Conceptualization, methodology, formal analysis, writing—original draft, writing—reviewing and editing, and supervision.
Footnotes
Acknowledgment
The authors would like to acknowledge Haley Szewczuga for her assistance in copy editing.
Author Disclosure Statement
We report no relevant conflicts of interest.
Funding Information
No funding was received for this article.
Prior Presentation
Preliminary analysis of this work has been presented as an abstract entitled “Independent, Not Alone: Balancing Support & Independence for Adolescents & Young Adults with Sarcoma; A Qualitative Study” at the American Society of Pediatric Hematology/Oncology (ASPHO) 2024.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.