
Abstract
Purpose:
Work ability and work-related outcomes (labor force participation, occupation, and educational attainment) are important for young adult-aged survivors of adolescent and young adult cancer (YAs). This study evaluates work-related outcomes and explores the role of workplace accommodations among YAs aged 25–34 years.
Methods:
For this cross-sectional study, YAs (N = 209) completed measures of educational attainment, labor force participation, occupation, work ability, and workplace accommodations. Work ability was assessed using the Work Ability Index and Work Limitations Questionnaire productivity loss index. We compared work-related outcomes with national benchmarks; analysis of variance models examined associations among work ability, work-related outcomes, and workplace accommodations.
Results:
Participant education and employment were greater than national benchmarks. Among employed cancer survivors (N = 176), individuals with less education reported lower work ability (F = 3.99, p = 0.004) and greater productivity loss (F = 4.21, p = 0.003) than those with higher levels of education. Workplace accommodations were a significant predictor of work ability; those with accommodations reported lower work ability (F = 3.99, p = 0.004) and greater productivity loss (F = 4.21, p = 0.003).
Conclusions:
While YAs in this sample generally demonstrated higher employment and educational attainment rates than the national average, those with lower educational levels face greater challenges in work ability. Workplace accommodations may only be provided to individuals experiencing the greatest deficits in work ability and productivity. This study highlights the need for additional data regarding workplace accommodations to enhance work ability and mitigate productivity loss among YAs.
Background
Annually, nearly 90,000 adolescents and young adults aged 15–39 are diagnosed with cancer. There are ∼680,000 adolescent and young adult cancer survivors (AYAs) in the United States, a number expected to grow due to rising incidence rates. 1 Research indicates that cancer negatively impacts work ability and work-related outcomes, including education, labor force participation, and job type. Work ability tends to be lower among cancer survivors than their same-age counterparts up to 6 years after diagnosis, and the financial cost of AYA cancers in the United States is $23.5 billion.2,3 Over $18 billion of these costs are attributed to absenteeism (i.e., time taken off/missing from work), presenteeism (i.e., working with altered performance), and reduced rate of employment. 3
Work ability and work-related outcomes are particularly important for AYAs, who likely have decades of work life years ahead of them after cancer. 4 Understanding the unique challenges faced by AYAs in returning to work is crucial, yet research in this area is limited. Work ability has only been examined using validated quantitative methods in three published studies focused on AYAs.5–7 Findings suggest that work ability is reduced in most AYAs in the 5 years following diagnosis and that lower work ability is associated with poorer quality of life.5–7
To address this gap, we developed the Work Ability in Young Survivors Study, focusing on young adult survivors (YAs) of AYA cancer aged 25–34. This age group allows for comparisons with national work-related benchmarks. This study integrated two bodies of emerging research in YAs: (1) long-term and late effects of cancer and its treatment and (2) work-related outcomes, guided by Feuerstein et al.’s Cancer & Work Model. 8 This proposed model postulates that cancer and its treatments impact work ability due to physical, cognitive, and psychosocial long-term and late effects. In turn, lower work ability leads to lower attainment of work-related outcomes. Workplace accommodations may serve to moderate the bidirectional relationship between work ability and work-related outcomes in cancer survivors.
Accordingly, this study has three objectives. First, we sought to document levels of labor force participation, occupation, and educational attainment following cancer treatment in YAs. We hypothesized that levels of labor force participation, occupation, and educational attainment in YAs would be lower than national benchmarks. Second, we sought to describe the relationship between levels of work ability and these outcomes and hypothesized that YAs in the workforce who report lower levels of work ability would also report holding occupations that require more manual labor (e.g., manual laborer v. managerial or professional) and lower educational attainment than survivors who report higher levels of work ability. Third, we explored whether workplace accommodations moderated the association of work ability with occupational category and educational attainment among YAs in the workforce.
Methods
This observational, cross-sectional study recruited YAs through the Wake Forest NCI Community Oncology Research Program (NCORP) Research Base. All study procedures were approved by the National Cancer Institute Central Institutional Review Board and registered on ClinicalTrials.gov (NCT03148080).
Study sample eligibility
To be eligible for the study, participants were (1) currently aged 25–34 years; (2) 2–10 years post-cancer diagnosis; (3) not in active cancer treatment (allowing for maintenance therapies); (4) diagnosed with first cancer (other than nonmelanoma skin cancer) at age ≥15 years; (5) able to read and understand English; and (6) able to understand and willing to sign a written informed consent document. Potential participants were excluded if they had a life expectancy of <6 months based on the opinion of the treating physician.
Recruitment
Potentially eligible participants were identified by research personnel via review of cancer registry, electronic medical records, or by response to flyers posted in clinics. Research staff contacted participants in alignment with site-specific recruitment protocols.
Participants were recruited by strata with equal allocation to each of four cells characterized by participant age group upon enrolling in the study (25–29 years, 30–34 years) and time since diagnosis (2 to <6 years, 6 to <10 years) to allow comparisons by current age controlling for time since diagnosis and by time since diagnosis controlling for age at diagnosis. Participants were required to be at least 2 years post diagnosis to allow the acute effects of cancer treatment to subside and increase the likelihood of having returned to work.
Study procedures
This observational study required participants to schedule a 45–60 minute appointment at a participating NCORP site to complete a survey via REDCap 9 with an NCORP staff member present. Participants received a $25 gift card for completion of study measures.
Measures
Cancer diagnosis and treatment information were collected from the medical record. Participants completed self-report measures in person at the study site. Work-related measures (e.g., occupational category) were only completed by individuals who reported that they were currently employed.
Demographic characteristics
Participants provided demographic characteristics, including sex, race, and ethnicity.
Educational attainment
Educational attainment was classified using the Current Population Survey (CPS) classifications to allow comparisons with US benchmarks and collapsed into ordinal categories. 10
Labor force participation
Participants were asked several questions from the General Social Survey and CPS regarding work for pay or profit during the survey reference week.10,11 For the analyses presented here, labor force participation was coded as employed, unemployed (not working but available and looking for work), or not in the civilian labor force (not employed and not looking for work, disabled, or active-duty military).
Occupational category
Occupational Category was summarized using the 2010 Standard Occupational Classification system. 12
Work ability
The 10-item Work Ability Index (WAI) is the most widely used measure of an individual’s ability to perform their work within available resources, in comparison with other times in life, and in relation to job demands. 13 Summed scores range from 7 to 49, with lower scores indicating poorer work ability. This measure has demonstrated adequate internal consistency among cancer survivors (Cronbach’s α = 0.89), 14 and in our study, the Cronbach’s α was 0.84. We also evaluated work ability using the 25-item Work Limitations Questionnaire (WLQ), 15 which assesses the impact of chronic health conditions and their treatments on job performance. Several scores can be derived from the WLQ, including at-work productivity loss (estimated percentage difference in at-work productivity compared with an external sample of healthy workers), the measure of interest in this study. Prior work suggests that for every 10% increase in on-the-job limitations, total employee work productivity declines 4%–5%. 16
Workplace accommodations
To evaluate workplace accommodations, employed participants were asked “Have any changes been made for you at your workplace due to your cancer?” (yes/no). Participants were also asked to report types of changes that were made (e.g., reduction in hours, reduction in tasks to reduce physical or mental strain, physical access aids). This strategy has previously been used with cancer survivors. 17
Data analysis
The planned sample size of the study was 200 participants, based on our ability to detect an effect size corresponding to a 15% lower proportion of employed cancer survivors. Planned stratification by age group (25–29 years, 30–34 years) and time since diagnosis (2 to <6 years, 6 to <10 years) was successful, with 47–66 participants allocated into each cell.
All participants who completed at least some of the study measures (N = 209) were included in the initial analytic dataset to describe educational attainment and labor force participation. For work-related measures (occupational category, WAI, WLQ, and workplace accommodations), the dataset included those participants who reported working in a civilian job. Categorical work-related outcomes were described using frequencies, while means and standard deviations were calculated for continuous measures. One-sample chi-square tests were computed to compare rates of educational attainment, employment status, and occupational category with national benchmarks from the 2018 CPS conducted by the US Census Bureau, treating these as historical fixed values. 10 Analysis of variance (ANOVA) models and linear contrasts were used to test whether work ability differed by levels of educational attainment or by occupational category. Both unadjusted and adjusted models are presented; adjusted models included sex, strata, and race/ethnicity (non-Hispanic white vs. all others). Finally, we evaluated whether the presence of workplace accommodations interacted with educational attainment or occupational category to predict work ability by using linear contrasts to estimate the effect of accommodation on work ability with adjustment for either educational attainment or occupational category and the interaction. Again, both unadjusted and adjusted models are presented; adjusted models included sex, strata, and race/ethnicity (non-Hispanic white vs. all others). To control for multiple comparisons, pairwise comparisons were only made if the overall test was significant (Fisher’s protected method).
Results
Participant characteristics
Two hundred fourteen participants were recruited between April 2018 and August 2020; 209 completed at least one measure. Study participants ranged from 25 to 34 years in age (M = 30.3, SD = 3.0) and were relatively evenly divided regarding time since diagnosis (Table 1). Most of the sample identified as female (64.1%) and white (83.3%). Most participants were married or living with a partner (60.8%). Total household income was most commonly between $50,000 and $74,999 (20.6%), with most participants reporting that they received insurance through an employer of themselves or a family member (71.8%). Most participants did not have children (61.2%). Lymphoma was the most commonly diagnosed cancer type (26.3%; Table 1).
Sample Characteristics

Participants could select more than one type of insurance, so the sum of the percentages exceed 100%.
Other cancer types included malignant carcinoid tumor of the midgut; malignant neoplasm of central nervous system, unspecified; malignant neoplasm of connective and soft tissue of left upper limb; malignant neoplasm of connective and soft tissue of the trunk; malignant neoplasm of connective and soft tissue unspecified; malignant neoplasm of the pancreas; malignant neoplasm of the pelvis; and solitary plasmocytoma.
Educational attainment, labor force participation, and occupation in YAs
Most participants (71.8%) reported some post-high school education. Rates of post-high school education were notably higher than those of 25–34-year-olds in the general US population (27.6% vs. 37.3%), 18 (Table 2). Most participants were employed (87.9%), again higher than the reported rate of employment among 25–34-year-olds in the general US population (79.2%). 19 The majority of employed participants were in management/professional roles (57.7%), compared with 41.5% of employed 25–34-year-olds in the general US population (Table 2).
Education, Employment, and Occupational Category of Cancer Survivors and Employed Individuals
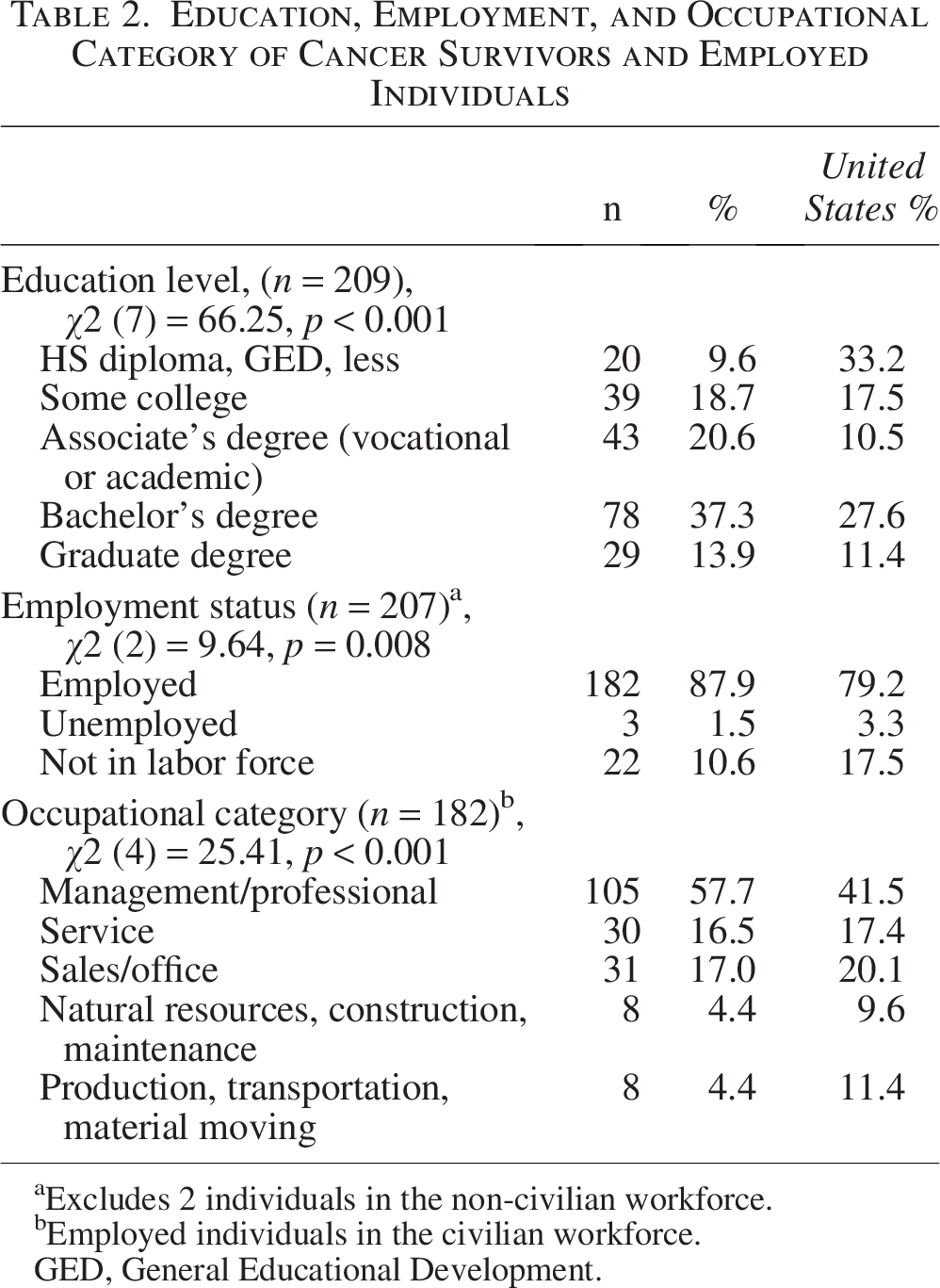
Excludes 2 individuals in the non-civilian workforce.
Employed individuals in the civilian workforce.
GED, General Educational Development.
Association of educational attainment and occupational category among YAs
Across categories of educational attainment, WAI scores ranged from 37.4 to 41.4, and WLQ productivity loss index ranged from 2.2% to 5.2%. Among employed individuals in our sample, work ability as measured by the WAI (N = 176) differed as a function of educational status (F = 3.99, p = 0.004 in unadjusted model; F = 5.63, p < 0.001 in model adjusting for sex, strata, and race/ethnicity) such that individuals with an associate’s degree reported lower work ability than those with a bachelor’s (sp’s < 0.001) or graduate degree (p = 0.019 for unadjusted model, p = 0.002 for adjusted model). Furthermore, individuals who had completed some college reported lower work ability than those who had earned a bachelor’s degree (p = 0.016 for adjusted model, p < 0.001 for adjusted model). Productivity loss among employed individuals as measured by the WLQ (N = 179) also differed as a function of educational attainment (F = 4.21, p = 0.003 in unadjusted model; F = 4.10, p = 0.003030 in model adjusting for sex, strata, and race/ethnicity). Individuals with a bachelor’s degree reported less productivity loss than individuals with an associate’s degree (p = 0.013 for unadjusted model, p = 0.008 for adjusted model), those who had completed some college (p < 0.001 for unadjusted model, p = 0.001 for adjusted model), and those who had obtained a high school diploma/General Educational Development or less (p = 0.019 for unadjusted model, p = 0.034 for adjusted model; Tables 3 and 4). Work ability and productivity loss did not differ as a function of occupational category in unadjusted models (Table 5) or adjusted models (Table 6).
Work Ability by Educational Attainment Among Employed Individuals (Unadjusted)
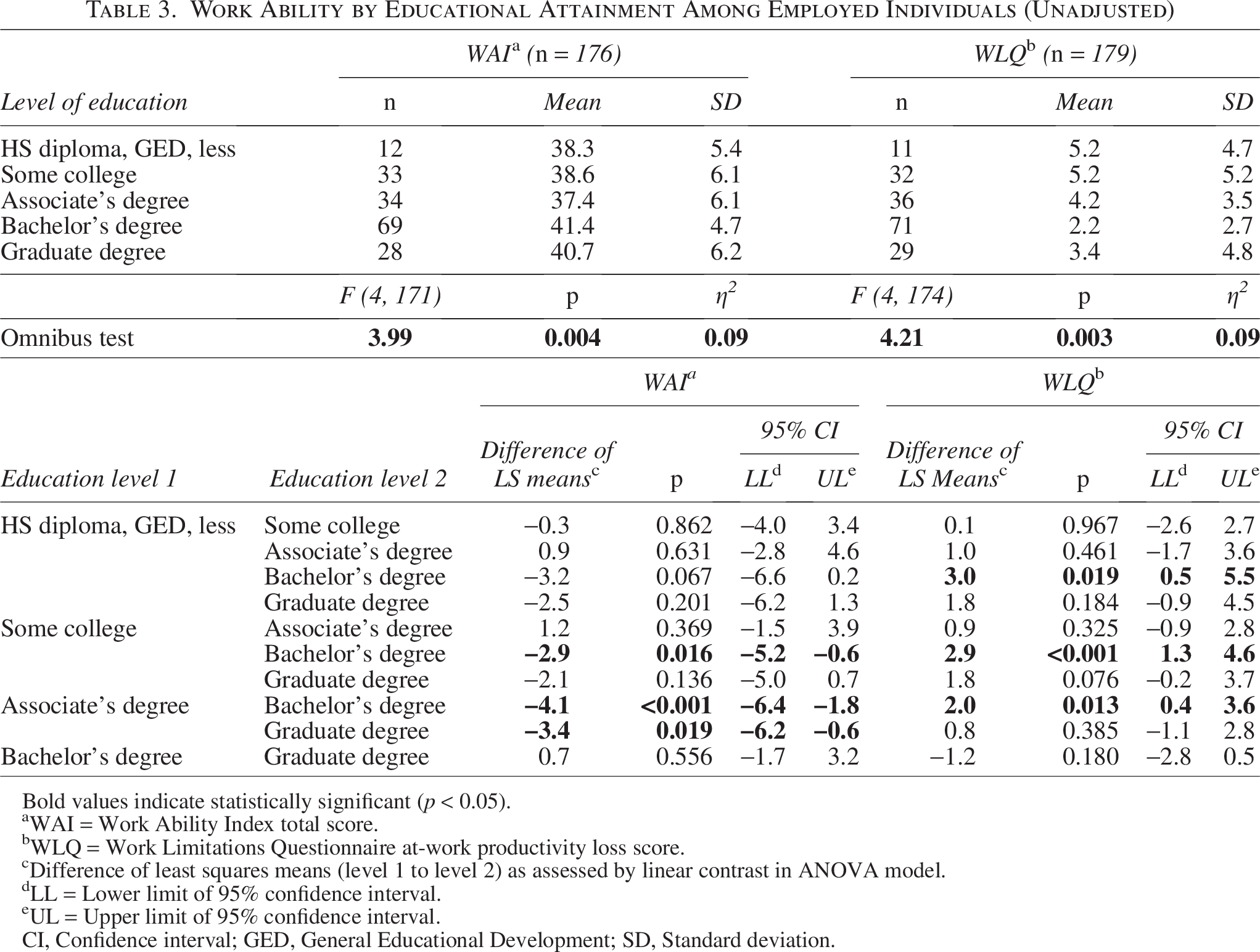
Bold values indicate statistically significant (p < 0.05).
WAI = Work Ability Index total score.
WLQ = Work Limitations Questionnaire at-work productivity loss score.
Difference of least squares means (level 1 to level 2) as assessed by linear contrast in ANOVA model.
LL = Lower limit of 95% confidence interval.
UL = Upper limit of 95% confidence interval.
CI, Confidence interval; GED, General Educational Development; SD, Standard deviation.
Work Ability by Educational Attainment Among Employed Individuals (Adjusted for Sex, Strata, and Race/Ethnicity)
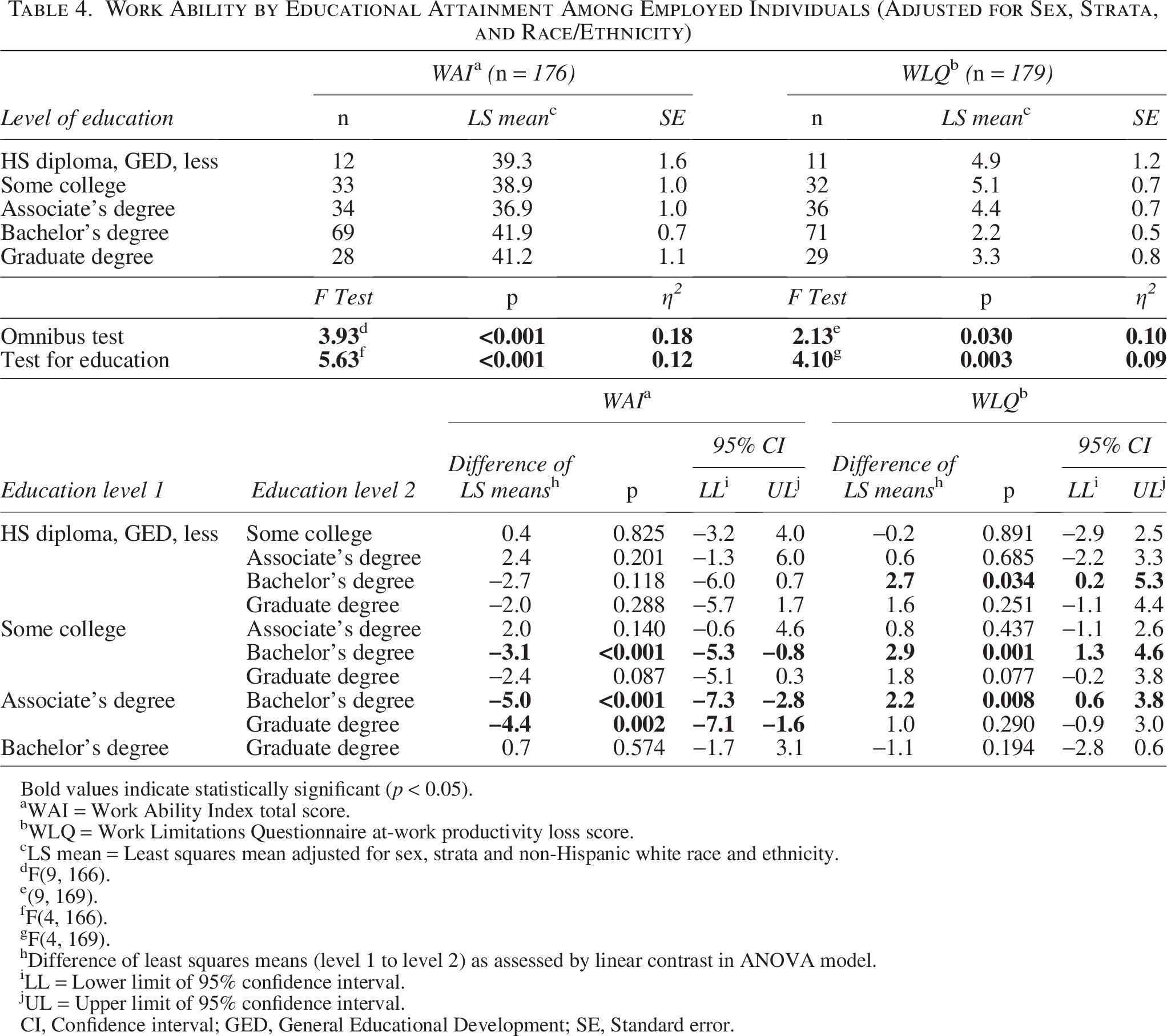
Bold values indicate statistically significant (p < 0.05).
WAI = Work Ability Index total score.
WLQ = Work Limitations Questionnaire at-work productivity loss score.
LS mean = Least squares mean adjusted for sex, strata and non-Hispanic white race and ethnicity.
F(9, 166).
(9, 169).
F(4, 166).
F(4, 169).
Difference of least squares means (level 1 to level 2) as assessed by linear contrast in ANOVA model.
LL = Lower limit of 95% confidence interval.
UL = Upper limit of 95% confidence interval.
CI, Confidence interval; GED, General Educational Development; SE, Standard error.
Work Ability by Occupational Category Among Employed Individuals (Unadjusted)
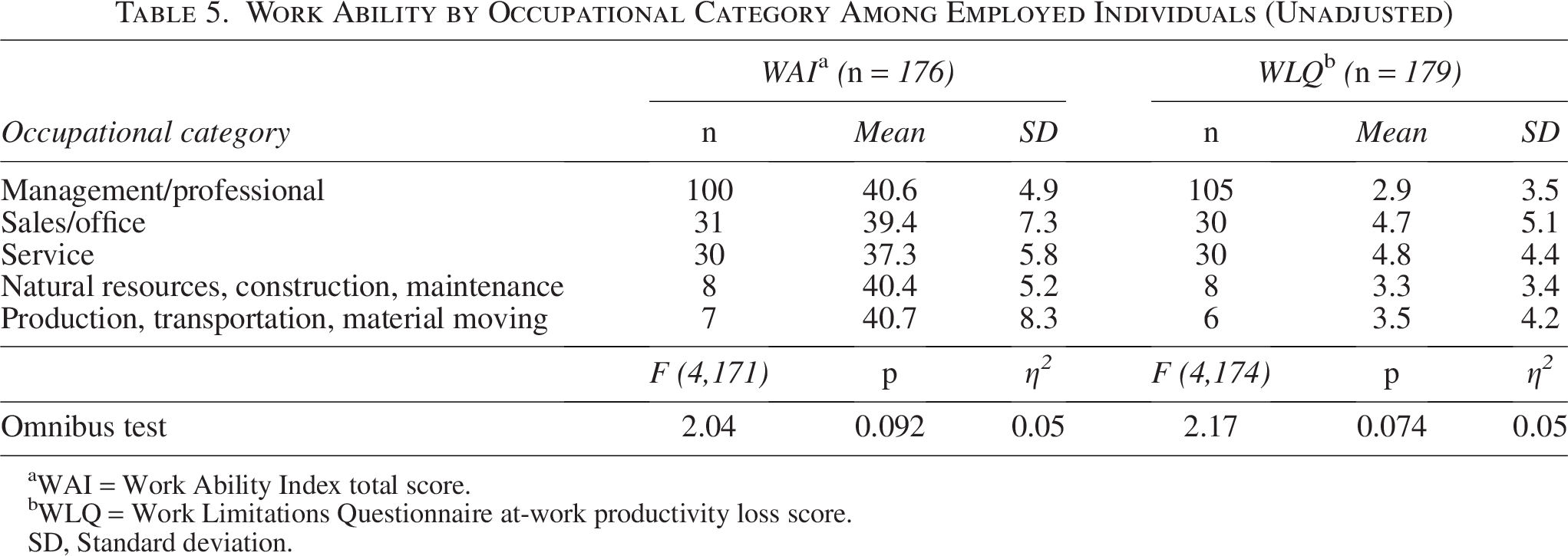
WAI = Work Ability Index total score.
WLQ = Work Limitations Questionnaire at-work productivity loss score.
SD, Standard deviation.
Work Ability by Occupational Category Among Employed Individuals (Adjusted for Sex, Strata, and Race/Ethnicity)
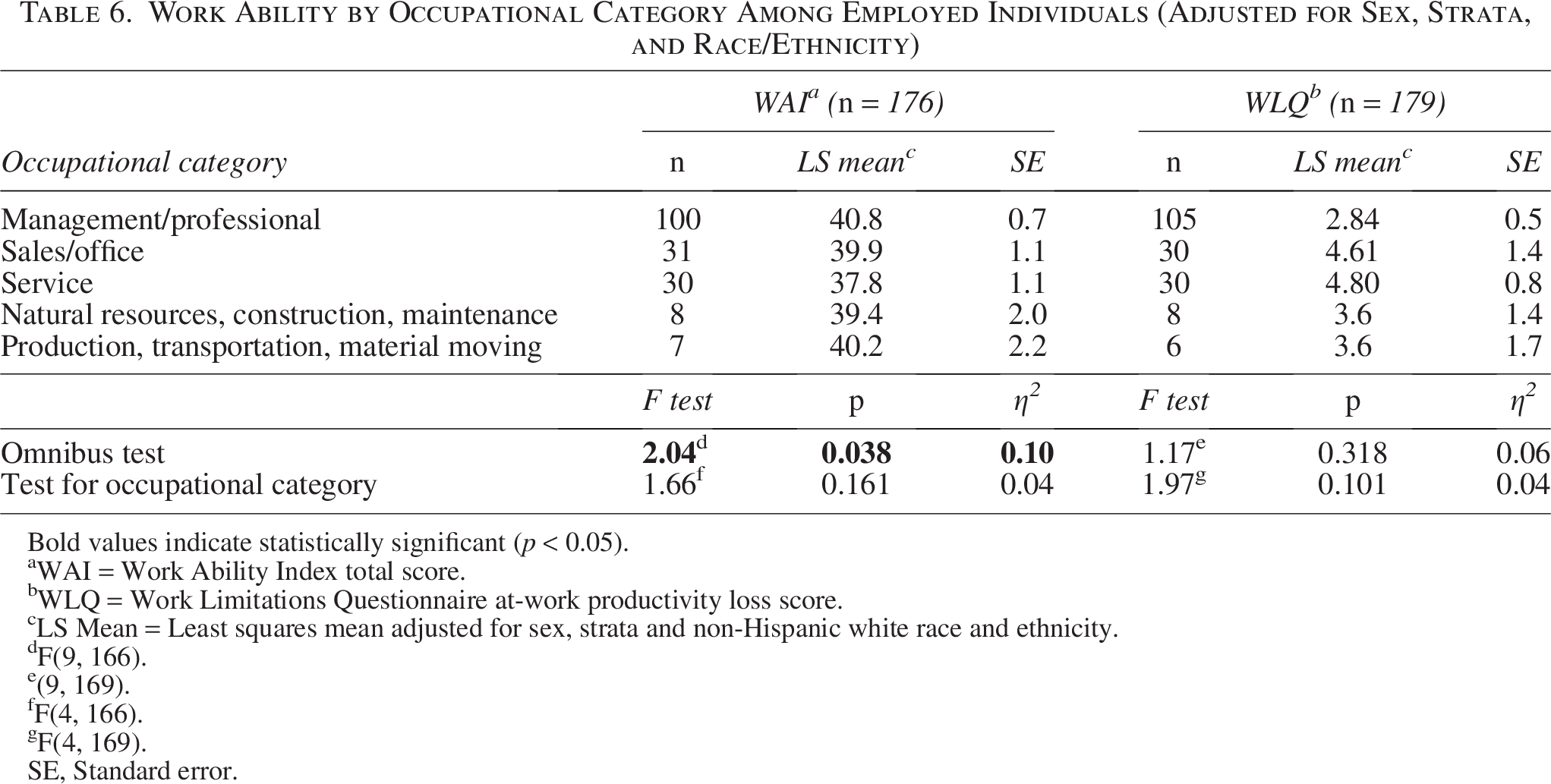
Bold values indicate statistically significant (p < 0.05).
WAI = Work Ability Index total score.
WLQ = Work Limitations Questionnaire at-work productivity loss score.
LS Mean = Least squares mean adjusted for sex, strata and non-Hispanic white race and ethnicity.
F(9, 166).
(9, 169).
F(4, 166).
F(4, 169).
SE, Standard error.
Workplace accommodations and the association of work ability with occupational category and educational attainment
Almost one-fifth of employed individuals in our sample reported that changes had been made for them at their workplace due to their cancer (N = 35/180, 19.4%). The most common types of accommodations were schedule changes, either to their number of work hours (n = 12/35, 34.3%) or to accommodate medical visits (n = 10/35, 28.6%). Changes to tasks to reduce mental strain (n = 10/35, 28.6%), reduce physical strain (n = 8/35, 22.9%), modify the physical work environment (n = 7/35, 20.0%), and other/unspecified types of changes (n = 11/35, 31.4%) were also reported.
We hypothesized that the impact of education on work ability would differ depending on whether or not accommodations were provided. However, workplace accommodations did not moderate the association between educational attainment and work ability (F = 1.39, p = 0.240 for the unadjusted model; F = 1.49, p = 0.206 after adjusting for sex, strata, and race/ethnicity) or productivity loss (F = 0.89, p = 0.474 for the unadjusted model; F = 1.13, p = 0.343 after adjusting for sex, strata, and race/ethnicity). Similarly, we wanted to evaluate whether workplace accommodations have a differential impact across occupational categories. The presence of workplace accommodations did not moderate the relationship between occupational category and work ability (F = 2.20, p = 0.072 for the unadjusted model; F = 1.97, p = 0.101 after adjusting for sex, strata, and race/ethnicity) or productivity loss (F = 1.36, p = 0.249 for the unadjusted model; F = 1.41, p = 0.232 after adjusting for sex, strata, and race/ethnicity).
While the hypothesized moderations were not present, these analyses demonstrated that the use of accommodations is an independent predictor of work ability and explains more of the variation in work ability than either educational attainment or occupational category alone in three of the four adjusted models. Specifically, those with accommodations reported lower work ability on average in both models of WAI (difference of least squares means for any accommodations: adjusted for educational attainment, sex, race/ethnicity, and strata: −3.3, 95% confidence interval (CI): −5.6, −1.0; adjusted for occupational category, sex, race/ethnicity, and strata: −5.1, 95% CI: −7.8, −2.4) and greater productivity loss in the model adjusted for educational attainment, sex, race/ethnicity, and strata (difference of least squares means: 2.8, 95% CI: 1.1, 4.6).
Discussion
In the present study, we described levels of work-related outcomes among YAs and compared them with national benchmarks. While previous data suggest that childhood cancer survivors achieve lower educational attainment than their non-cancer peers, 20 our findings are more consistent with a systematic review of studies on AYAs, which found that educational attainment did not differ from that of non-cancer peers. 21 One possibility is that because YAs experience disruptions to their education later in their educational trajectory or not at all (i.e., if their diagnosis occurs after they have completed their education), impacts on education are less common.
The racial and ethnic make-up of our sample may be a key factor that impacted this surprising finding. Racial and ethnic disparities in educational attainment are well documented. 22 The fact that our sample included less than 5% Black individuals and approximately 7% Hispanic individuals indicates that our sample was not representative of the US population, which as of 2018 consisted of over 12% Black individuals and over 18% Hispanic individuals aged 25–34. 23 Thus, it is possible that this finding is due to characteristics of our sample not directly related to late effects of cancer and cancer treatment. Future research on educational attainment in YAs should strive to obtain samples that are representative of the population to better understand how cancer impacts YAs educational attainment.
Similarly, rates of employment in our sample were notably higher than those in the US population. Notably, we required that measures be completed on-site with an NCORP staff member present. As a result, it is possible that our study procedures resulted in an increased likelihood that those who were less affected by the late effects of cancer and cancer treatment and those in occupational categories with greater flexibility or access to paid time away from work were more likely to participate. While greater-than-expected employment rates may be due, in part, to our sample’s characteristics, recent work suggests that it may not be an anomaly. A systematic review estimated that 75% of cancer survivors in North America return to work 2+ years post-diagnosis, 24 and it has been demonstrated that younger survivors are more likely to work than older survivors. 25 Indeed, the AYA-Leipzig study found that 88.8% of German AYAs returned to work after a cancer diagnosis, consistent with our finding that 87.9% of the YAs in our study were employed. 26 While the increased likelihood of YAs returning to work after cancer may, in part, be due to lower rates of comorbid conditions among YA survivors as compared with older survivors, 27 in the United States recent qualitative findings suggest that the need for medical insurance and the risk for financial toxicity that YAs experience may contribute to high rates of employment (often termed “job lock”). 28 Specifically, Ghazal and colleagues (2021) found that work-related goals changed significantly based on AYAs’ perceptions of the personal impact of financial toxicity. 29 Furthermore, YAs do not have the benefits of having been in the workforce for decades; they may lack sufficient savings or access to early retirement programs that may make leaving the workforce more feasible for older adults. Thus, the desire to reduce financial toxicity may also be driving greater-than-expected employment rates. 30
A secondary aim of this study was to evaluate whether work ability and productivity loss among YAs differed by educational attainment and occupational category. Our results suggest that YAs with higher levels of education may be protected from the negative impact cancer can have on work ability and productivity loss. This finding is consistent with a report of long-term YAs in Norway, which found that individuals with low work ability were more than twice as likely to have a low level of education. 6 In contrast, occupational category was not associated with these important work-related outcomes. This aligns with prior work, such as a study of long-term breast cancer survivors. 31 However, more research is needed to better understand this relationship.
Finally, we found that neither of these relationships differed as a function of workplace accommodations. Rather, our analyses revealed that use of accommodations is an independent predictor of work ability, such that those with accommodations reported lower work ability and greater productivity loss. It is notable that compared with the AYA-Leipzig study, a much lower proportion of participants in our sample reported obtaining workplace accommodations (82.3% and 19.4%, respectively). 26 This contrast may be the result of differences in social and economic norms between the United States and Germany. Consistent with previous research, individuals in our sample with low work ability were more likely to seek out and obtain formal accommodations at work. 17 In other words, accommodations are being provided to those who need them (i.e., those with low workability). However, it also suggests that such accommodations may not mitigate productivity loss effectively, which could be a concern for employers and employees. Beyond formal employer-provided accommodations, YAs may also benefit from job crafting, or self-initiated ways in which employees can change their jobs. 32 By adapting their work roles, YAs may be able to more effectively maintain productivity and well-being.
Limitations and strengths
This study is not without limitations. First, this research relied on cross-sectional data. As such, we were unable to evaluate work-related outcomes over time in cancer survivors. Future studies should consider employing longitudinal methodologies to better inform our understanding of how work-related outcomes change over time in YAs. Furthermore, our study was not powered to examine how clinical characteristics such as cancer type related to work-related outcomes. Future studies should seek to obtain larger samples to allow for subgroup analyses on key cancer and treatment-related variables. This issue is particularly important given the heterogeneity of cancer diagnoses in samples defined by age group, resulting in wide variability in treatment course, long-term and late effects, and trajectories of recovery that may differentially impact work-related outcomes.
This research also relied on self-report data, which may impact the validity of our findings. Specifically, respondents may not have accurately remembered and reported information about the impact of cancer on their work or provided answers they believed to be more socially acceptable, rather than reflective of their actual experience. Relatedly, when evaluating whether workplace accommodations acted as a moderator, we used only a single, binary item to model this. Furthermore, while this item has previously been used with cancer survivors, 17 the set of items it is part of has not been formally validated as a cohesive measure. Future research should utilize validated measures of workplace accommodations to more accurately characterize this construct in YAs.
Finally, our sample had limited racial and ethnic diversity, making it less representative of the YA population as a whole. While we recruited through the NCORP to ensure this study reached YAs receiving care in the community setting, the sites from which most patients were accrued did not have minority/underserved status, meaning less than 30% of the population they serve were racial/ethnic minorities or rural residents. While we attempted to improve representation of racial and ethnic minorities within our sample by extending the study to facilitate recruitment of these underrepresented groups, future studies should use established methods for purposive sampling from the outset to ensure a representative sample.
These limitations notwithstanding, this study also has several strengths. We used the NCORP infrastructure to obtain data from patients treated in community oncology practices across the United States. Use of this national network is notable given that the majority of YAs receive treatment and follow-up care in the community, 33 yet much research on this population has limited recruitment to academic medical centers. Second, our stratified sampling approach allowed us to ensure representation across age and time since diagnosis. Third, we created our age criterion to map onto national benchmark data for work and education outcomes.
Conclusion
This study adds to the scant literature on work-related outcomes in YAs by emphasizing the complexity of the relationships among educational attainment, occupational category, work ability, and workplace accommodations. While cancer, cancer treatment, and associated late effects certainly impact work-related outcomes, it is also important to consider the broader sociocultural context, which may also impact these outcomes, such as race, ethnicity, educational attainment, and cancer-related financial toxicity. As such, oncology teams might consider providing targeted, evidence-based interventions to YA cancer survivors at risk of poorer work-related outcomes, such as a referral to vocational counseling. Finally, while individuals with lower levels of work ability may be more likely to receive workplace accommodations, it is unclear if such accommodations are sufficient to improve work ability and reduce productivity loss in YAs. Further research is needed to determine which accommodations should be offered to whom and how the success of these accommodations should be evaluated.
Authors’ Contributions
K.M.M.: Writing—original draft and writing—review and editing. J.A.T.: Formal analysis, data curation, methodology, and writing—review and editing. S.M.C.: Conceptualization, methodology, and writing—review and editing. K.A.: Writing—Review and Editing. J.M.: Conceptualization, methodology, and writing—review and editing. L.V.G.: Writing—review and editing. H.M.: Investigation and writing—review and editing. J.L.: Investigation and writing—review and editing. R.J.: Investigation and writing—review and editing. J.C.: Conceptualization, methodology, and writing—review and editing. C.S.: Writing—review and editing. T.A.A.: Conceptualization, methodology, and writing—review and editing. G.J.: Conceptualization, methodology, and writing—review and editing. S.C.: Conceptualization, methodology, writing—original draft, writing—review and editing, supervision, project administration, and funding acquisition.
Footnotes
Acknowledgment
The authors would like to acknowledge the following NCORP sites for their participation: Cancer Research Consortium of West Michigan NCORP, Cancer Research for the Ozarks NCORP, Columbus NCORP, Essentia Health NCORP, Hawaii Minority Underserved NCORP, Heartland Cancer Research NCORP, Iowa-Wide Oncology Research Coalition NCORP, Kaiser Permanente NCORP, Metro Minnesota Community Oncology Research Consortium, NCORP of the Carolinas (Greenville Health System NCORP), Sanford NCORP of the North Central Plains, Texas Pediatric Minority Underserved NCORP, Southeast Clinical Oncology Research Consortium NCORP, Wichita NCORP, and Upstate Carolina Consortium Community Oncology Research Program. In addition, the authors would like to thank Wake Forest NCORP Research Base staff members Karen Craver, Julie Turner, Renee Glenn, Tammy Vogler (Site Coordinator), Eden Gurganus Wood (Data Management), and Jenna Gerosa (Regulatory).
Author Disclosure Statement
The authors declare that they do not have any interests, funding, or employment that may inappropriately influence or affect the integrity of this submission.
Funding Information
This study was supported by the National Cancer Institute of the National Institutes of Health under award number UG1CA189824 and the Biostatistics and Qualitative and Patient-Reported Outcomes Shared Resources of the Wake Forest Baptist Comprehensive Cancer Center’s NCI Cancer Center Support Grant, award number P30CA012197. Additional support was provided by the National Cancer Institute of the National Institutes of Health under award numbers R21CA191989 (PI: Danhauer) and K99/R00CA248701 (PI: Murphy). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.