
Abstract
Purpose:
Young adult (YA) cancer survivors aged 18–39 years face increased chronic disease risk. Although YA survivors prioritize health, structural barriers may limit their ability to maintain healthy lifestyles, particularly in culturally and geographically diverse regions. This mixed-methods study explored health priorities, social determinants of health (SDoH)-related barriers and facilitators to maintaining a healthy lifestyle, and intervention preferences for YA cancer survivors in New Mexico (NM) to inform future interventions.
Methods:
Descriptive statistics and thematic analysis were conducted on surveys and semistructured interviews with 17 YA cancer survivors and 11 YA cancer care providers in NM. Surveys assessed demographics and, for survivors, SDoH, and intervention preferences.
Results:
Social isolation was the most prevalent adverse SDoH, affecting 47% of YAs. YAs expressed interest in diet/physical activity-related programs (82%) and were flexible about group/one-on-one (59%) and in-person/online (71%) program formats. YA themes included: physical and mental health are priorities post-treatment; multilevel barriers and facilitators shape health behaviors; there is a lack of YA-specific resources; community building is key for peer support; support strategies to address psychosocial, behavioral, and health care navigation concerns are needed. Provider themes included: YAs have specific care needs during the survivorship transition to long-term wellness; collaborative, innovative organizational solutions are critical, peer and community support is effective, and integrating psychosocial and culturally informed care enhances outcomes; there is a need for empowering support tailored to the needs of YA survivors in NM.
Conclusion:
Physical, mental, and social health are priorities for YA cancer survivors post-treatment. Findings highlight the need for flexible, community-informed interventions that support holistic health and long-term survivorship.
Keywords
Introduction
Over 650,000 adolescent and young adult (AYA) cancer survivors live in the United States, a growing population with increasing survival rates but persistent health and quality-of-life challenges. 1 Although AYA is commonly defined as ages 15–39, this study focuses specifically on young adult (YA) survivors aged 18–39 due to consent requirements and interview considerations. As YAs transition into adulthood, they remain at risk for chronic conditions, including obesity-related diseases such as diabetes and cardiovascular issues. 2 Obesity is a modifiable factor linked to recurrence and mortality in several cancers.3–6 However, many YA cancer survivors’ lifestyles do not meet dietary or physical activity guidelines. 7 Health care providers can support behavior change through survivorship care plans, as recommended by the Institute of Medicine, 8 to improve health outcomes and quality of life. 9
Prior qualitative, mixed-methods, and population-based studies have documented that YA cancer survivors experience persistent physical and psychosocial challenges during and after treatment, including fatigue and sleep disturbance, anxiety and fear of recurrence, disruptions to work and relationships, and difficulties accessing coordinated survivorship support.10–12 Studies incorporating survivor and provider interviews have identified gaps in lifestyle counseling, inconsistent delivery of survivorship care plans, and limited access to health promotion resources following treatment.13–15 However, much of this work has focused on single stakeholder perspectives, specific cancer types, or clinic-based samples, often in urban or resource-rich settings, with limited attention to how social determinants of health (SDoH) and geographic context shape survivorship experiences and access to care in diverse or rural regions.16–18
Despite increasing awareness of health risks among YA survivors, few interventions specifically target dietary behavior change during this life stage19,20 marked by psychosocial transitions such as establishing independence, building careers, and forming relationships.19–20 These changes are often complicated by lingering effects of treatment, including stress, anxiety, and depression.21 SDoH—such as health care access and social support—may further influence their ability to maintain healthy lifestyle behaviors, particularly in rural and diverse populations where resources are more limited.
A critical gap remains in understanding how YA cancer survivors prioritize health behaviors within their lived contexts and what they prefer in a health behavior intervention, and how providers perceive survivorship-focused health promotion in culturally and geographically diverse settings. This convergent mixed-methods study integrated survivor-identified priorities and intervention preferences and SDoH-related barriers with provider perspectives on care delivery and resource availability in New Mexico (NM). Aim 1 (YA survivors) was to: (1a) quantify SDoH-related needs and intervention preferences using an online survey, and (1b) qualitatively explore health priorities, barriers and facilitators to diet and physical activity, and desired survivorship resources through semistructured interviews. Aim 2 (Providers) was to qualitatively explore perspectives on existing resources, gaps, and feasible health promotion strategies for YA cancer survivors. Findings will inform culturally responsive, community-informed intervention development in resource-limited settings.
Methods
We used a convergent mixed-methods design 22 ; surveys and one-on-one interviews were collected in parallel, analyzed separately, and integrated during interpretation. Integration relied on triangulation across data sources and joint team interpretation to identify convergence and divergence and to inform intervention implications. The guiding theoretical framework informed methodological decisions, including selection of survey measures aligned with stress, coping, and SDoH constructs and development of semistructured interview guides probing environmental stressors, coping strategies, and health behaviors. The framework also guided qualitative analysis, with coding and theme development conducted using an SDoH-informed deductive-inductive lens to capture emergent individual, interpersonal, and structural influences on survivorship experiences. The protocol was approved by the University of New Mexico Health Sciences Center Institutional Review Board.
Theoretical framework
This convergent mixed-methods study was guided by a theoretical framework informed by Barrington et al.’s model of the association between perceived stress and obesity, 23 Lazarus and Folkman’s Transactional Model of Stress and Coping, 24 and SDoH. Barrington et al.’s model conceptualizes perceived stress as a pathway linking environmental stressors to obesity-related behaviors (diet and physical activity). Lazarus and Folkman’s Transactional Model frames stress as a dynamic process of appraisal and coping that shapes behavioral and psychosocial outcomes. We situated these processes within an SDoH framework, conceptualizing rurality, cultural norms, language access, and local resource infrastructure as upstream determinants that shape stress exposure, coping capacity, and opportunities for health behavior change in NM (Fig. 1).
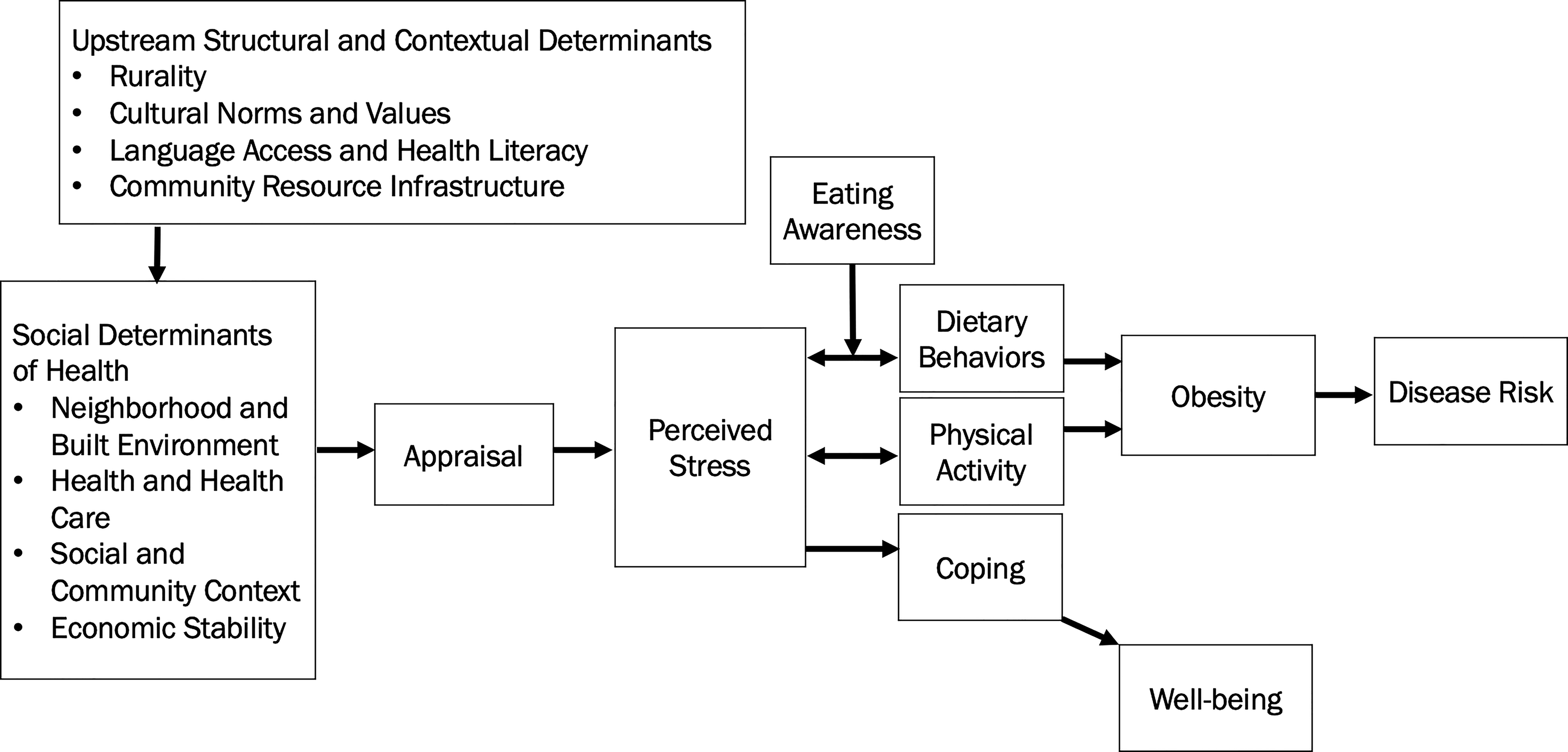
Theoretical framework. The integrated theoretical framework combines social determinants of health (SDoH), Lazarus and Folkman’s Transactional Model of Stress and Coping, and Barrington et al.’s biobehavioral model. SDoH-related stressors influence perceived stress, which affects dietary and physical activity behaviors. In our study, stressors, perceived stress, health behaviors, and coping were assessed using the Accountable Health Communities Health-Related Social Needs tool and semistructured interviews. Rurality, cultural norms, language access, and community resource infrastructure are depicted as upstream structural determinants influencing SDoH domains, stress appraisal, coping capacity, and health behaviors in culturally diverse and resource-limited settings such as New Mexico.
In alignment with this framework, SDoH-related stressors were assessed using domains from the Accountable Health Communities Health-Related Social Needs Screening Tool and explored qualitatively through survivor interviews. Upstream structural and contextual determinants were further explored through provider interviews. Coping processes were examined through interview questions about challenges and adaptation strategies. Health behaviors were assessed via survey items on physical activity and intervention interest and further explored in interviews addressing diet, physical activity, and related barriers and facilitators.
Participants and setting
Eligibility criteria for Aim 1 included: age 18–39, ≥1-year post-treatment, NM residency, and prior cancer diagnosis. Those aged 15–17 were not included due to regulatory and ethical considerations and different interview dynamics. For Aim 2, eligible participants were health care providers (e.g., physicians, nurses, social workers) working with YA cancer survivors in NM. Exclusion criterion for both aims: not English- or Spanish-speaking. Participants were recruited via nonprobability convenience sampling using a multipronged approach, including clinical outreach through oncology and survivorship clinics, community outreach, social media, and word of mouth. Because recruitment involved open community outreach and self-selection, a conventional response rate could not be calculated. Enrollment aimed to capture diverse survivor and provider perspectives across age, geographic context, and professional roles; however, no formal stratified quotas were enforced. Recruitment continued until thematic saturation was reached, defined as no substantively new themes emerging during team-based analytic review.
In NM, nearly half the population identifies as Hispanic or Latino, 25 and 26 of 33 counties are rural or frontier. 26 Almost all NM counties are health professional shortage areas. 27
Procedures
Participants were enrolled from May to November 2024. The study was discussed with the University of New Mexico Comprehensive Cancer Center Community Outreach and Engagement Community Advisory Board in June 2024 to obtain feedback on study procedures. All participants provided informed consent to participate and have deidentified data published. Participants completed an eligibility screener and online survey via REDCap 28 and were then contacted by email or phone to schedule an interview.
Survey measures
The survey included questions on age, gender identity, sexual orientation, race, ethnicity, and urbanicity. For YAs, the survey also included questions on age at diagnosis, relationship status, insurance status, cancer type, cancer stage, treatment type, and intervention interest and preferences (e.g., “Would you be interested in participating in a program to improve diet and physical activity?”), and the 26-item Accountable Health Communities Health-Related Social Needs Screening Tool. 29 The tool assesses five core domains (housing instability, food insecurity, transportation problems, utility needs, interpersonal safety) and eight supplemental domains (financial strain, employment, family and community support, education, physical activity, substance use, mental health, disabilities). This tool was selected because it captures upstream determinants of health relevant to cancer survivorship. Although not specific to YA or cancer populations, the tool allowed for systematic assessment of cross-cutting social and contextual factors that shape stress, coping, and health behaviors. The full survey instrument is provided in Supplementary Materials (Supplementary Appendix). Providers also had questions on provider type, years of experience, and interest in cancer support programs.
Qualitative interviews
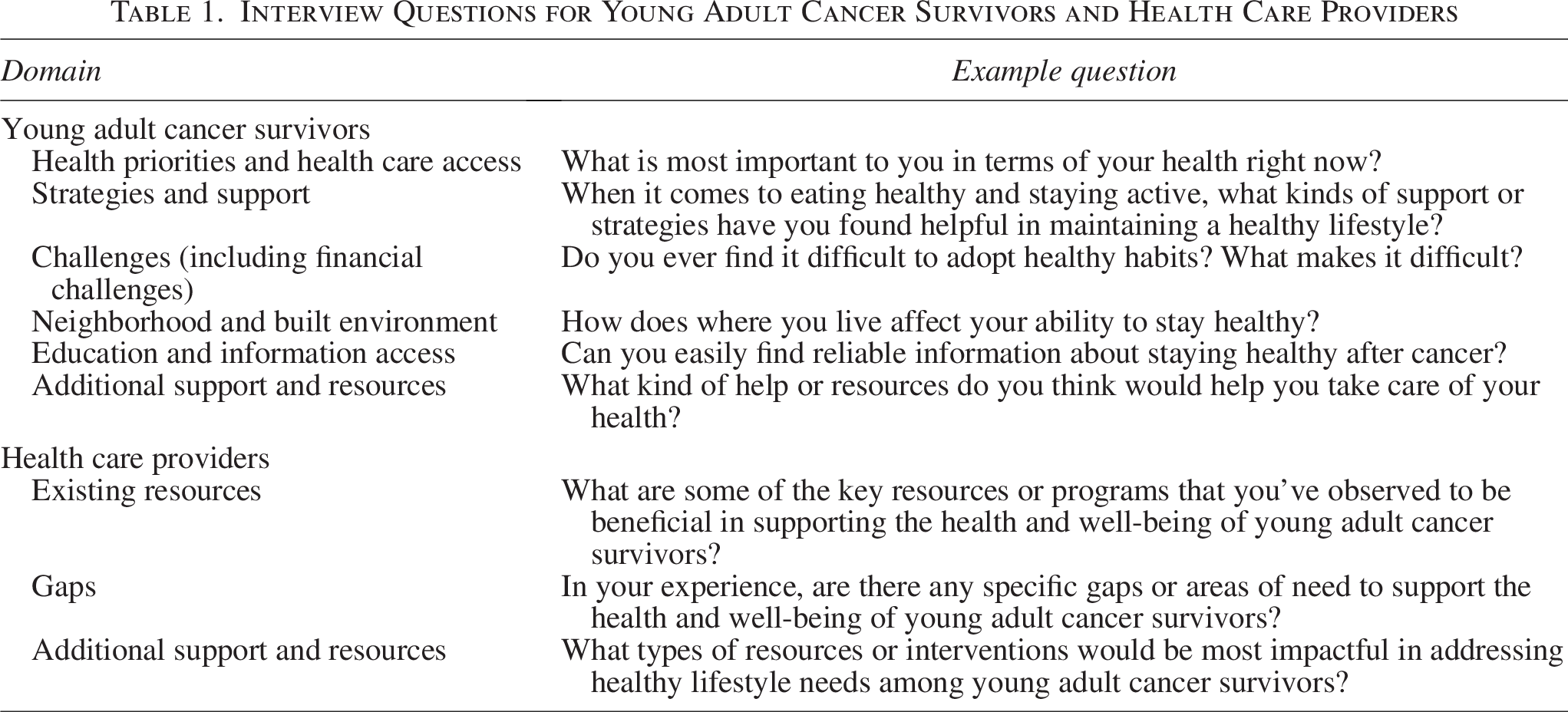
Participants completed a 45-minute semistructured interview via Zoom, phone, or in-person for a $50 e-gift card. One-on-one interviews were conducted by trained qualitative researchers (E.B., J.A.T., M.M.) using an interview guide developed with the team and were audio-recorded and transcribed verbatim. Interviews were conducted in small batches and reviewed iteratively by the research team to allow for ongoing reflexive discussion, refinement of probing strategies, and monitoring of emerging themes. The interview guides included questions on key domains with exploratory probes for each domain. Domains and example questions are depicted in Table 1. Separate interview guides were developed for YA survivors and providers based on the guiding theoretical framework; full interview guides are provided in Supplementary Materials (Supplementary Appendix).
Interview Questions for Young Adult Cancer Survivors and Health Care Providers
Data analysis
Descriptive statistics were conducted to summarize survey responses. For Accountable Health Communities Health-Related Social Needs domains, response categories were collapsed into binary indicators reflecting potential need (presence vs. absence) for interpretability given the small sample. Thematic analysis was used to identify, analyze, and report repeated patterns in the interview data. 30 Using the coding reliability approach, 31 a codebook was created after familiarization with the data using an SDoH lens. Over half of the transcripts were coded 32 by two researchers (A.W.B. and E.B. or M.M.), and the codebook was revised based on discussion. The remaining transcripts were coded by one researcher (A.W.B.) and reviewed by a second researcher (A.Z.R.). Data quality was ensured through an audit trail, triangulation, and member checking. 33 Triangulation compared patterns across survey findings, survivor interviews, and provider interviews and was discussed in reflexive team meetings. For member checking, we emailed participants summary tables and visual theme summaries (with an optional co-authorship invitation) and invited feedback; responses supported resonance and informed minor wording refinements.
Findings were integrated during interpretation by examining how survey patterns converged with interview themes. Interviews incorporated flexible probing to allow participants to introduce content beyond the guide. Analysis combined inductive theme development with attention to stress, coping, and social context, supported by triangulation and reflexive team discussions to mitigate confirmation and social desirability bias.
Results
Participant characteristics
YA cancer survivors (n = 17; ages 21–40; mean 7.8 years postdiagnosis) were mostly Hispanic or Latino (58.8%), women (88.2%), straight/heterosexual (70.6%), and from urban or suburban areas (82.4%). The most common cancer types were breast (23.5%), lymphoma (23.5%), and leukemia (17.7%).
Providers (n = 11) were all women and mostly straight or heterosexual (81.8%), Hispanic or Latino (90.9%), and working in urban or suburban areas (90.9%). Provider types included nurse practitioner or advanced nurse practitioner (27.3%), registered nurse (18.2%), social worker (18.2%), patient navigator (9.1%), therapist or counselor (9.1%), or dietitian (18.2%). Full demographic characteristics are depicted in Table 2.
Participant Characteristics for a Sample of Young Adult Cancer Survivors (n = 17) and Health Care Providers (n = 11)
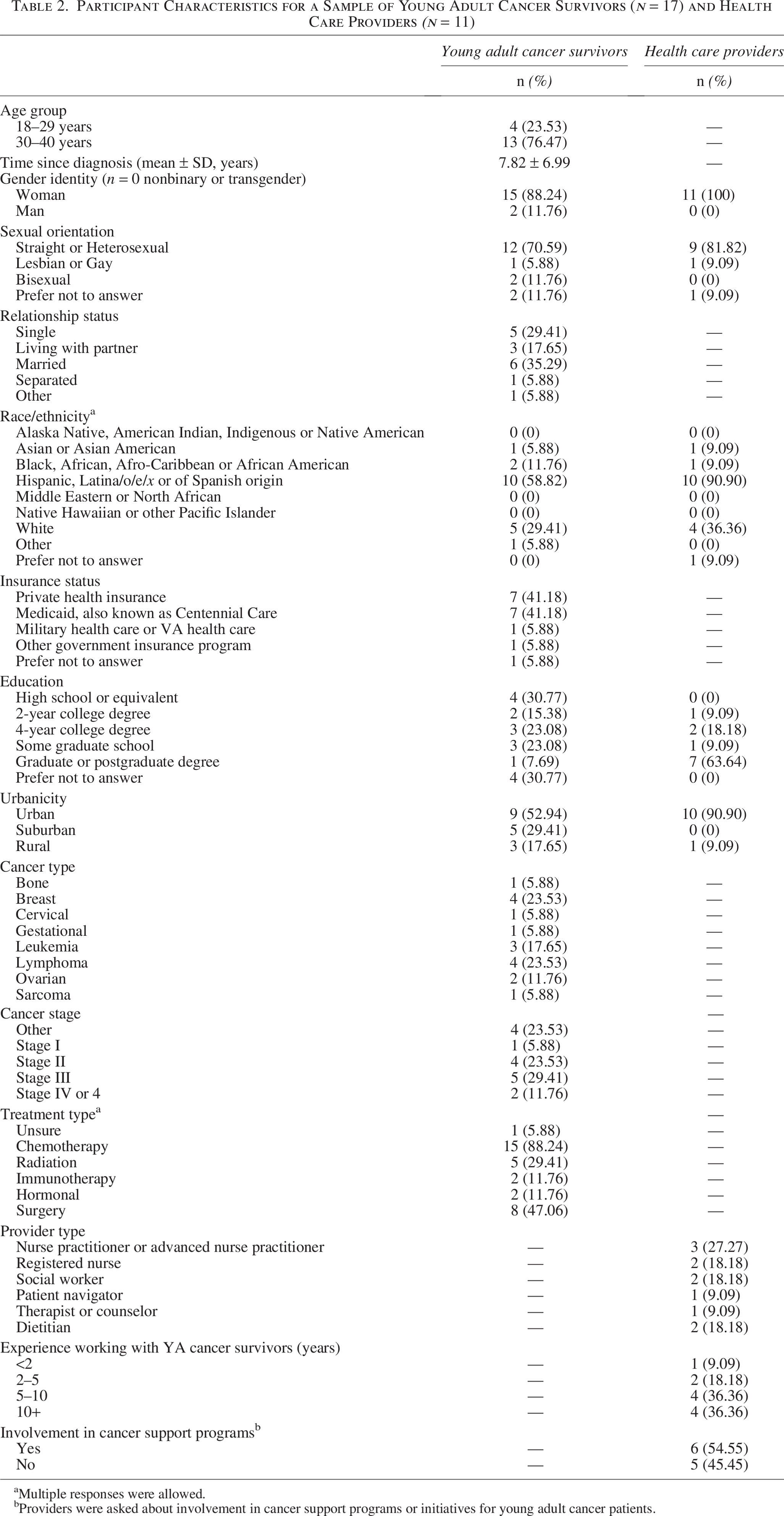
aMultiple responses were allowed.
bProviders were asked about involvement in cancer support programs or initiatives for young adult cancer patients.
Quantitative outcomes
Most YAs reported access to SDoH, including reliable transportation (94.1%), housing (88.2%), food access (76.5%), and utilities access (88.2%), and lack of financial strain (82.4%). However, nearly half (47.1%) reported feeling lonely or isolated. Eight participants (47.1%) met physical activity guidelines. Monthly or daily substance use was reported by four YAs (23.5%). Stress was moderate-to-high in 41.2% of participants, and 58.8% had experienced recent mental health concerns. Full results across all domains are presented in Table 3.
Social Needs in a Sample of Young Adult Cancer Survivors (n = 17)
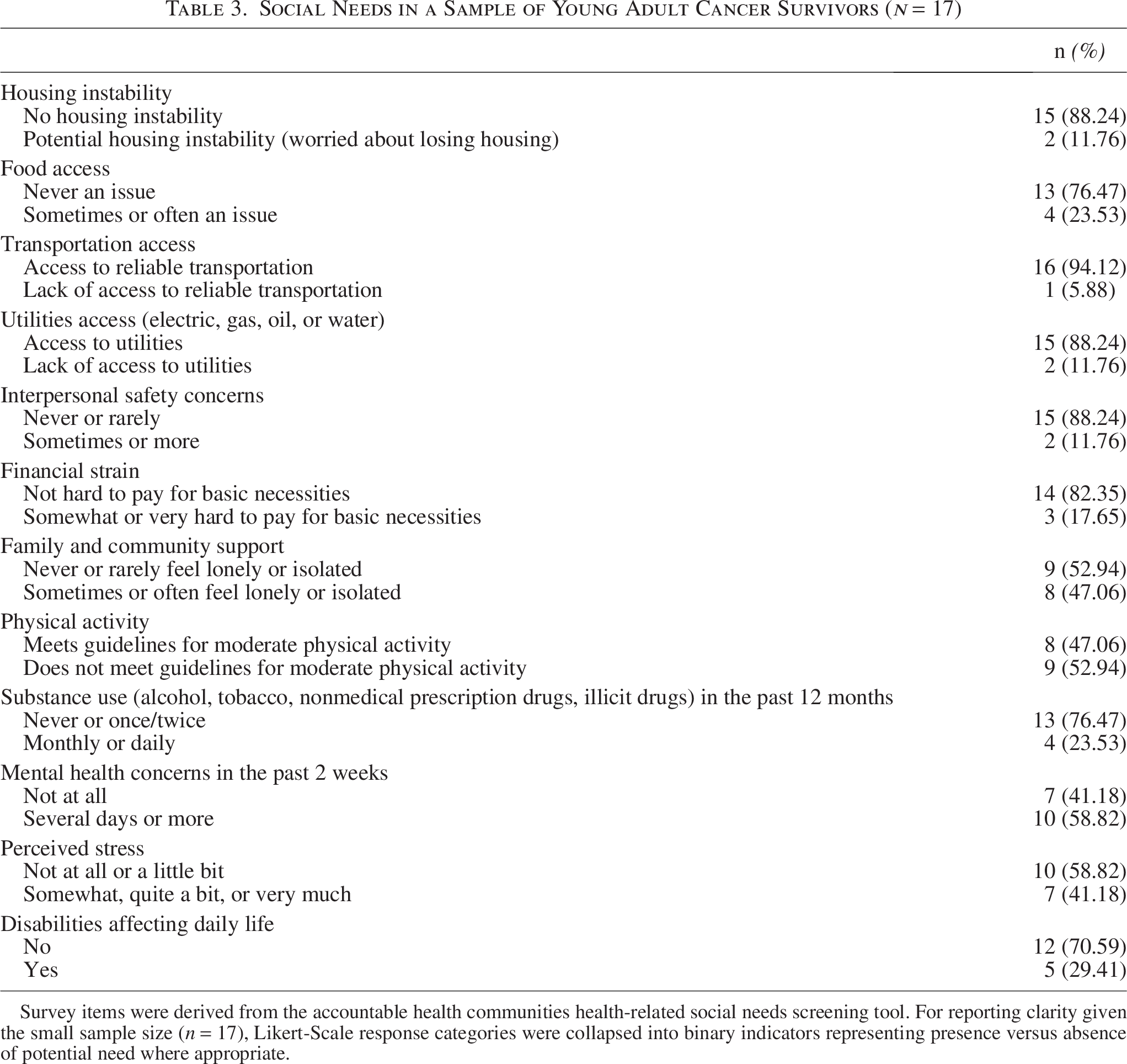
Survey items were derived from the accountable health communities health-related social needs screening tool. For reporting clarity given the small sample size (n = 17), Likert-Scale response categories were collapsed into binary indicators representing presence versus absence of potential need where appropriate.
Lifestyle intervention preferences are summarized in Table 4. Most YAs (70.6%) rated a healthy lifestyle (not explicitly defined) post-treatment as very or extremely important. Most expressed interest in diet/physical activity-related programs (82.4%) and were flexible about group/one-on-one (58.8%) and in-person/online (70.6%) formats. These quantitative patterns, particularly loneliness/isolation and flexibility in intervention preferences, converged with qualitative themes emphasizing community building, the need for tailored support, and adaptable delivery formats.
Lifestyle Intervention Preferences in a Sample of Young Adult Cancer Survivors (n = 17)

Qualitative outcomes
YA survivor themes
Qualitative data revealed the following higher-level themes among YAs: (1) physical and mental health are priorities after cancer treatment; (2) multilevel barriers and facilitators influence health habits; (3) there is a lack of YA-specific, evidence-based resources despite abundant health-related information; (4) community building is key for peer support and connection; (5) tailored support strategies to address psychosocial, behavioral, and health care navigation concerns are needed. Representative quotes are depicted in Table 5.
Themes That Emerged from Qualitative Interview Data from a Sample of Young Adult Survivors and Representative Quotes (n = 17)

Physical and mental health are priorities after cancer treatment. YAs reported a focus on self-care and well-being post-treatment, recognizing the importance of balancing physical and mental health. As one YA stated, “It’s become a more important thing to me to take care of myself and my mind” (1221). Many described learning to set boundaries and prioritize their health, sometimes for the first time, as they acknowledged the need to put themselves first in a demanding world. For some, treatment revealed or intensified challenges, such as executive functioning difficulties, highlighting the importance of self-compassion and tailored strategies for daily life. Others grappled with the emotional toll of disrupted life goals, such as starting a family, which compounded feelings of loss, isolation, and depression. Cancer treatment was described as a catalyst for embracing self-care as a lifelong priority, underscoring the need to address both physical and emotional well-being in survivorship care.
Multilevel barriers and facilitators influence health habits. YAs described how their health habits are influenced by multilevel barriers and facilitators, reflecting the broader social and environmental contexts of their lives and emphasizing the importance of addressing systemic obstacles while leveraging supportive environments to promote health. Subthemes included: (1) structural and financial barriers, (2) environmental context, (3) social and family influence, and (4) competing responsibilities and disruption in care.
Structural and financial barriers
YAs discussed challenges related to limited access to providers, financial stress, and logistical issues such as transportation and insurance. These barriers often constrained their ability to prioritize or sustain health-promoting behaviors and highlighted the need for more accessible, affordable systems of support.
Environmental context
YAs highlighted the dual role of their physical surroundings in shaping health behaviors. While many viewed nature and outdoor spaces as facilitators for physical activity and mental well-being, others described barriers such as excessive heat, lack of indoor space, or safety concerns that limited opportunities for building and sustaining an exercise program. One YA shared, “…it’s been too hot to exercise outside, and I don’t have any room inside. I’ve been trying to clean the house to make it possible for me to exercise. So I feel like that’s one thing that I would want to do for my health, but I can’t” (1226).
Social and family influence
Interpersonal relationships were described as both facilitators and barriers to healthy living. Some YAs credited partners and family members with supporting health behavior changes, such as adopting healthier diets or shared routines. Others, however, noted challenges when family norms or habits conflicted with their own health goals, contributing to frustration or feelings of isolation.
Competing responsibilities and disruption in care
Many participants described the challenge of balancing health goals with caregiving and work responsibilities. Others highlighted how frequent relocation, often for economic or family-related reasons, disrupted their continuity of care and required them to establish relationships with new providers. These transitions were particularly difficult for those also managing cancer-related fatigue, disability, or other lingering treatment effects, underscoring the need for coordinated and flexible survivorship services.
There is a lack of YA-specific, evidence-based resources despite abundant health-related information. Despite the abundance of health-related information available, YAs reported a lack of resources tailored to their unique needs, particularly for long-term health maintenance after treatment. As one participant noted, “I’m afraid to just grab it off the internet type thing because there’s a lot of misinformation” (1218).
Many expressed frustration with the scarcity of evidence-based, age-specific materials and instead turned to informal sources, such as social media, to fill these gaps, despite uncertainty and potential misinformation on these platforms. Accessible support groups for their age group were also identified as an unmet need, with some YAs describing how broader, mixed-age groups failed to meet their expectations for peer connection and relevance.
Additionally, unmet needs included critical life areas such as family planning and fertility preservation. YAs cited a lack of structured support or clear guidance from providers, leaving them to navigate complex, deeply personal decisions on their own. These challenges highlight the urgent need for reliable, YA-specific resources that not only address long-term health maintenance but also provide practical tools and peer support networks to empower YAs after cancer.
Community building is key for peer support and connection. YAs discussed thriving when they connect with peers with shared experiences, finding emotional validation and understanding that formal support structures often cannot provide. One YA reflected:
It was just so awesome, wholesome to find someone my age who has been through something… Our parents do try to comfort us, but they don’t know what it’s like to have third-degree burns on your neck and have to keep going to radiation day after day after day. They don’t know what it’s like to lose your hair that makes you have so much identity as a person or what it’s like whenever you take steroids for months because you’re going through chemo. So I found not only [redacted], but a bunch of people who understood me and validated me” (1205).
YAs reported that informal, peer-driven gatherings can foster a sense of belonging, shared resilience, and trust, offering a crucial space for navigating the challenges of life after cancer. Groups that encourage physical and social activities create opportunities for casual interactions and meaningful connections. YAs reported that such community-building efforts are essential for fostering peer support and connection, helping them feel understood and less alone in their journeys.
Tailored support strategies to address psychosocial, behavioral, and health care navigation concerns are needed. YAs discussed a need for programs that address their distinct physical and emotional needs, highlighting the value of inclusive, accessible, and individualized guidance. One participant described the burden of navigating follow-up care, stating, “…there was a lot of pushback, and I had to fight to get some of those follow-up scans” (1222).
Many acknowledged the challenges providers face in meeting patients’ diverse needs. Insights highlighted the need for psychosocial and behavioral interventions that address the real-world challenges of post-treatment life. Mental health emerged as a particularly critical area where tailored interventions are warranted, with additional mention of nutrition and the need for individualized guidance.
Participants emphasized that survivorship requires a high degree of agency, advocacy, and system literacy, skills that are not intuitive and are often unsupported. Many YAs were left to advocate for their own care, often without guidance. This self-advocacy extended to financial and insurance navigation, areas that shaped their ability to access consistent care. These experiences highlighted a need for developmentally tailored support strategies that build self-advocacy, provider communication, system navigation skills, and resilience in managing the emotional demands of survivorship.
Provider themes
The following higher-level themes emerged among provider interview data: (1) YAs need tailored resources and care that meet their evolving needs across the lifespan; (2) collaborative solutions and resource innovation are needed to overcome systemic and logistical barriers; (3) strong peer and community connections provide critical support for YAs navigating life after cancer; (4) integrating psychosocial and cultural strengths enhances care and support for YAs; (5) empowering YAs with education and individualized approaches supports their independence and resilience. Representative quotes are depicted in Table 6.
Themes That Emerged from Qualitative Interview Data from a Sample of Health Care Providers and Representative Quotes (n = 11)

YAs need tailored resources and care that meet their evolving needs across the lifespan. Complementary to YAs’ discussion of the need for YA-specific resources, providers described how YAs require health care systems that adapt to their evolving needs, bridging the gap between pediatric and adult care with comprehensive survivorship support. Providers reported that structured transition programs are critical for addressing the late effects of cancer treatments, which often manifest decades later. As one provider explained, “So just because they have pediatric cancers, like I say, their late effects are going to come later in adulthood…that’s why they need some kind of clinic or somewhere that can see them” (1505).
Collaborative solutions and resource innovation are needed to overcome systemic and logistical barriers. Providers discussed that addressing structural and logistical barriers in health care requires innovative approaches such as virtual care, stronger partnerships, and long-term investments in infrastructure. One provider suggested:
Offering different modalities for follow-up than rather just in-person only… continuing to offer tele-visits and virtual visits… I think it’s early education and I think it’s meeting them where they’re at rather than expecting them to meet us where we’re at (1516).
Building sustainable systems, particularly in resource-limited areas, demands creativity and a commitment to ongoing development. Providers also described how virtual care can offer a promising solution to improve accessibility and engagement.
Strong peer and community connections provide critical support for YAs navigating life after cancer. Like YAs, providers recognized that YAs thrive when given opportunities to connect with peers who share similar experiences. Social gatherings and community-driven initiatives offer valuable spaces for sharing their journeys and fostering a sense of belonging. These peer-centered spaces are crucial for addressing the emotional and social needs of YAs, providing a sense of community and shared resilience that complements traditional medical care. As one provider noted, “They don’t necessarily need an organized support group or a presentation. They need to talk to each other” (1514).
Integrating psychosocial and cultural strengths enhances care and support for YAs. Providers discussed that tailoring care to the cultural diversity, family dynamics, and psychosocial needs of YAs strengthens their health care experiences and outcomes, highlighting the importance of culturally sensitive, family-centered approaches that address the unique needs of YA survivors. Personalized approaches ensure that survivors feel understood and supported, even when health care resources are limited. Language and cultural barriers further underscore the need for compassionate, inclusive care.
Empowering YAs through tailored education, resources, and support is needed to navigate survivorship and establish independence. Providers mentioned that early and ongoing education tailored to the unique challenges YAs face is essential for fostering independence and a proactive approach to survivorship. Providing tools and guidance helps them navigate their care and thrive. Encouraging YAs to explore and personalize their resources was described as key to this empowerment, equipping them with the skills and confidence to take charge of their health and embrace survivorship with resilience and independence.
Mixed-methods integration
Quantitative and qualitative findings converged across key domains. Survey-reported loneliness aligned with survivor and provider themes emphasizing peer connection. Interest in diet/physical activity programming and format flexibility corresponded with qualitative accounts of competing responsibilities and care disruptions, supporting adaptable delivery models. Survey-reported stress and mental health concerns complemented themes describing psychosocial burden and navigation challenges.
Discussion
This study explored health priorities and intervention preferences among YA cancer survivors and their providers. Despite structural and psychosocial challenges, survivors reported motivation to improve their health, emphasizing self-care and the value of community support. Nearly half (47.1%) reported loneliness or isolation, reinforcing prior findings on disrupted social well-being among YAs and the need to integrate social support into survivorship care. 34 Findings support strengths-based, personalized interventions, as survivors described motivation to improve health, intentional self-care practices, and flexibility in preferred program formats, while providers emphasized building on survivors’ existing coping strategies and community strengths to support long-term survivorship.19,20
Interpreted through the guiding frameworks, convergent findings show how structural stressors and social context shape coping and health behaviors during YA survivorship. Social isolation functioned as both a stressor and a constraint on coping resources, highlighting an intervention pathway integrating social support and resource navigation. Survivors’ narratives reflected appraisal and coping processes (Lazarus and Folkman) and linked stress and constrained resources to challenges maintaining a healthy diet and regular PA (Barrington et al.), underscoring the need to address upstream SDoH in behavior-focused survivorship support.
Balancing survivorship with adult responsibilities (employment, finances, caregiving) often led YAs to deprioritize health behaviors. While prior research has identified these competing demands,34,35 our qualitative findings further highlighted relocation as a common survivorship challenge, with participants describing frequent moves related to employment, family needs, or access to care. Survivors reported that relocation disrupted continuity of care, delayed re-establishment of provider relationships, and made it difficult to maintain consistent health routines. Interventions must align with YAs’ life stages and context to be sustainable. 36 Additionally, environmental factors such as neighborhood safety and climate, elements often overlooked in survivorship studies, emerged as influences on health behaviors.
Our sample—predominantly female, over age 30, and Hispanic or Latino—closely reflects NM Tumor Registry data for YA survivors (70% female, 72% over 30, 43% Hispanic or Latino), except for Native American representation (8% in the registry vs. 0% in our sample). Despite most participants living in urban or suburban areas, care disruptions were common. Unlike studies that emphasize rurality as a key barrier, 17 our findings reveal that localized system-level issues can hinder access even in urban settings. This highlights the need for culturally responsive, community-based programs that account for geographic context and local resource availability, even in urban or suburban settings.37,38
YAs often found health behavior change isolating, especially when it conflicted with family or cultural norms, reinforcing the value of family- and community-informed interventions.39,40 Interest in both online and in-person formats points to the need for hybrid or flexible models that expand access while honoring personal preferences. Survey findings showing high interest in diet/PA programs and flexibility in format complemented interview data describing barriers such as competing responsibilities and access constraints, supporting the need for adaptable, community-connected intervention models. Such approaches may be particularly relevant in settings such as NM, where cultural values, connection to community, and geographic context shape survivorship experiences. 9
YA survivors and providers both emphasized a lack of YA-specific, evidence-based survivorship resources, particularly for nutrition, physical activity, and mental health, consistent with persistent resource gaps identified in YA survivorship research.41,42 Investing in community resources is essential, especially in rural, linguistically diverse areas with limited culturally tailored support. Strengths-based, community-based participatory action research-aligned approaches can leverage community resilience and existing assets.37,43 Providers identified a need for transition clinics and lifespan-oriented support, particularly for fertility planning, cognitive challenges, and identity development. In NM where many YA survivors and families follow traditional food practices, culturally and linguistically tailored care is critical for improving outcomes and trust. 44 A novel contribution of our study is providers’ emphasis on community partnerships and locally driven care models to address regional provider shortages. Casillas et al. similarly support the role of community-partnered approaches, reinforcing the value of local collaboration in resource-limited settings. 45
Limitations of this study include a lack of participation from Spanish-preferring, Native American, and rural survivors, groups that may face distinct challenges. Despite the use of flexible probing, inductive analysis, and triangulation, the use of semistructured interviews and self-reported data may have introduced confirmation or social desirability bias. Additionally, most participants received care at the study site, which may have influenced responses. Despite these limitations, the study provides rich, contextualized insights into the lived experiences of YA cancer survivors in a diverse, geographically unique setting.
Conclusions
YA cancer survivors’ health behaviors are shaped by structural, social, and individual factors, including provider shortages, relocation, cultural norms, and mental health needs. YA survivors are motivated to adopt and maintain a healthy lifestyle but lack tailored resources and support systems. Providers echoed the need for lifespan-oriented, culturally responsive care. Flexible, community-informed programs that are culturally responsive and contextually feasible may offer a model for improving survivorship in culturally diverse and resource-limited settings, including rural and frontier communities.
Authors’ Contributions
A.W.B., A.G., J.V., A.L.S., and C.K.B.: Conceptualization, methodology, and funding acquisition. E.B., J.A.T., and M.M.: Project administration and investigation. A.W.B., A.Z.R., E.B., J.A.T., and M.M.: Formal analysis. A.Z.R., M.M.S., and M.M.d.O.: Validation. A.W.B., A.Z.R., and M.S.S.: Writing—original draft preparation. C.K.B.: Supervision. All authors: Writing—reviewing and editing.
Footnotes
Acknowledgments
The authors thank the participants for sharing their time and experiences and the University of New Mexico Comprehensive Cancer Center Community Advisory Board for contributing their expertise.
Author Disclosure Statement
All authors declare that they have no conflicts of interest.
Funding Information
This research was supported by an Institutional Research Grant, IRG-21-146-25, from the American Cancer Society, by the University of New Mexico Comprehensive Cancer Center Support Grant NCI P30CA118100 and the Behavioral Measurement and Population Sciences shared resource, and REDCap DHHS/NIH/NCRR #8UL1TR000041.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.