
Abstract
Purpose:
Nasopharyngeal carcinoma (NPC) is a rare cancer, especially in nonendemic regions such as North America, occurring in a bimodal age distribution with the first peak in adolescents and young adults (AYA). Limited data exist on treatment outcomes in this group. The purpose of our study is to evaluate treatment outcomes of NPC in the AYA population in British Columbia, Canada, and evaluate late effects.
Methods:
We conducted a retrospective cohort study of AYA patients (ages of 15–39 years at diagnosis) diagnosed with NPC and treated between 2000 and 2015. Demographics, treatment outcomes, and late toxicities were collected. Overall survival (OS) and disease-free survival (DFS) were analyzed using the Kaplan–Meier and Cox regression. Locoregional recurrence and distant metastatic recurrence were evaluated using the competing risk method. Late effects were described qualitatively and quantitatively.
Results:
The cohort included 97 patients: 93 received curative intent treatment, 3 received palliative treatment, and 1 was excluded from survival analysis. Five-year OS rates were 81% (Stage I/II), 80% (Stage III), and 68% (Stage IV), with corresponding DFS rates of 78%, 77%, and 66%. The addition of neoadjuvant and/or adjuvant chemotherapy to radiotherapy was associated with improved survival. Advanced-stage disease had a higher incidence of locoregional relapse. Common late toxicities included xerostomia, hearing loss, epistaxis, and hypothyroidism.
Conclusion:
Although survival rates in our cohort were comparable to existing literature, the rate of late toxicities was high. These findings support the need for AYA-tailored treatment strategies and survivorship care to minimize long-term complications and optimize quality of life.
Introduction
Nasopharyngeal carcinoma (NPC) is considered an uncommon cancer in most parts of the world with an age-standardized incidence rate of 1.3 per 100,000 population. 1 However, NPC has a distinct geographical distribution, with Asia accounting for 83.3% of global NPC incidences; of those cases, 52.5% occurred in East Asia, with the highest incidence in Southern China, followed by 35.8% in Southeast Asia. In contrast, nonendemic countries such as Canada and the United States of America have an age-standardized incidence rate of 0.62 per 100,000 and 0.41 per 100,000, respectively.1,2
In endemic regions, the incidence of NPC increases gradually with age, with peak levels at 50–60 years; however, some studies have noted a bimodal age distribution in low-risk populations and nonendemic areas, with the first peak occurring in adolescents and young adults (AYA).1,3,4 The incidence rate of NPC in childhood is <1% among all childhood tumors, and multiple studies have noted that although the pediatric population tends to present with more advanced disease, younger age is associated with better prognosis and outcomes. Standard therapy for NPC includes a combination of chemotherapy and high-dose radiotherapy over several weeks. These treatments are associated with a high burden of late toxicities affecting quality of life (QoL), which include but are not limited to xerostomia, dysphagia, hearing impairment, and secondary malignancies.5,6
Due to the low incidence of NPC in the AYA population, there has not been published data evaluating survival outcomes of this population in North America. The purpose of this study is to evaluate treatment outcomes of NPC in the AYA population in British Columbia as well as to evaluate late side effects. This is the first provincial population-based study in a nonendemic region with systematic follow-up.
Materials and Methods
After obtaining institutional REB approval, a retrospective review of all adolescent and young adult patients ages 15–39 years treated for NPC between January 1, 2000, and December 31, 2015, in British Columbia, Canada, was conducted. Patient information was collected from the BC Cancer Agency (BCCA) electronic medical record. We recorded the following variables: Patient age, sex, ethnicity, Eastern Cooperative Oncology Group Performance Status Scale (ECOG), tumor histology, date of diagnosis, initial TNM staging, initial treatment, and dates of treatment—including surgery, radiation dose, fractionation, and the use of chemotherapy. All patients underwent staging according to the American Joint Committee on Cancer, seventh edition.
We also recorded the incidences of treatment-associated late toxicities, including xerostomia, dysphagia, dental caries, chronic nasal/sinus congestion, skin changes, neck fibrosis, thyroid nodules, hypothyroidism, secondary malignancy, cranial nerve injury, brain stem injury, infertility, carotid artery stenosis, and cerebral vascular accident by review of all medical notes from BCCA as well as specialist consultation notes.
Overall survival (OS) and disease-free survival (DFS) were analyzed using the Kaplan–Meier method, and locoregional recurrence and distant metastatic recurrence were evaluated using the competing risk method. Locoregional recurrence was defined as relapse in the nasopharynx (local) or in cervical or supraclavicular lymph nodes (regional). Distant metastatic recurrence was defined as any relapses outside of these regions. A two-tailed p value of <0.05 was considered statistically significant for all analyses. All analyses were conducted using R Statistical Software, Version 4.5.0. Late effects were described qualitatively and quantitatively.
Results
Patient characteristics
From 2000 to 2015, a total of 97 AYA patients diagnosed with NPC were included in this study. The baseline characteristics are shown in Table 1. The median age at diagnosis was 35 years, with an age range of 15–39 years. Among these patients, 41 (42%) were female. The median follow-up was 77 months.
Patient Demographic, Disease, and Treatment Characteristics
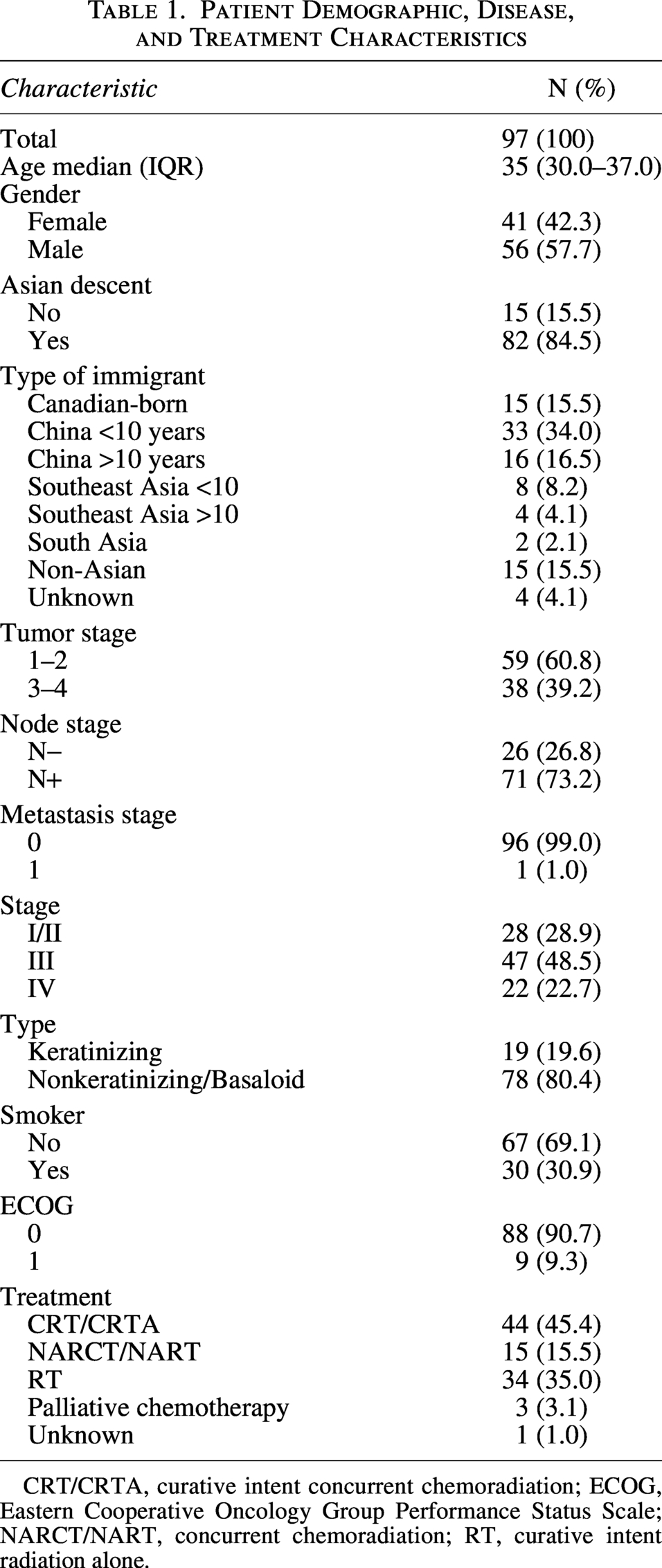
CRT/CRTA, curative intent concurrent chemoradiation; ECOG, Eastern Cooperative Oncology Group Performance Status Scale; NARCT/NART, concurrent chemoradiation; RT, curative intent radiation alone.
With regard to ethnicity, 82 (85%) were of Asian descent, and among those, 66 were Chinese, 13 were Southeast Asian, and 3 were South Asian.
In terms of immigration status, 15 (16%) were Canadian born, 49 (51%) immigrated from China with 33 (34%) before the ages of 10, and 16 (17%) after the age of 10, 12 (12%) immigrated from Southeast Asia with 8 (8%) before the age of 10, and 4 (4%) after the age of 10, 2 (2%) immigrated from South Asia, 15 (16%) immigrated from non-Asian countries, and 4 (4%) were unknown.
Out of the 15 Canadian-born patients, 13 (87%) were Chinese, 1 (∼7%) was Southeast Asian, and 1 (∼7%) was South Asian.
Sixty-seven (69%) were never-smokers, and all the patients had an ECOG status of 0 (91%) or 1 (9%).
In terms of disease characteristics, 61% had T1/T2 tumors, 73% were node positive, and 1% had metastatic disease at diagnosis. The predominant histological type was nonkeratinizing/basaloid carcinoma, accounting for 80% while the remainder were keratinizing-subtype. The distribution of disease stages was as follows: Stage I/II (29%), Stage III (48%), and Stage IV (23%).
Treatment at diagnosis included curative intent concurrent chemoradiation (CRT/CRTA) for 44 patients (45%), curative intent neoadjuvant chemotherapy followed by concurrent chemoradiation (NARCT/NART) for 15 patients (16%), curative intent radiation alone (RT) for 34 patients (35%), palliative intent chemotherapy for 3 patients (3%), and unknown for 1 patient (1%).
Survival analysis
One patient was lost to follow-up and excluded from the survival analyses. The remaining 96 patients were included in the survival analyses. As shown in Figure 1A, OS at 5 years was 81% for Stage I/II, 80% for Stage III, and 68% for Stage IV (p = 0.1). The Kaplan–Meier curve for OS by treatment (Fig. 2A) demonstrated OS at 5 years was 75% for CRT/CRTA, 93% for NARCT/NART, 79% for RT alone, and 0% for the palliative-intent chemo group (p = < 0.001).

Survival analysis based on disease stages ,  ,
,  .
.

Survival analysis based on treatment groups CRT/CRTA,  NARCT/NART,
NARCT/NART,  Palliative, RT.
Palliative, RT.
Multivariate analysis using Cox regression for OS demonstrated that patients who received palliative chemotherapy had an increased risk of death with a hazard ratio (HR) of 6.42, confidence interval (CI) of 1.21–34.0 (p = 0.029), as shown in Table 2.
Combined Multivariate Analyses for Survival Outcomes
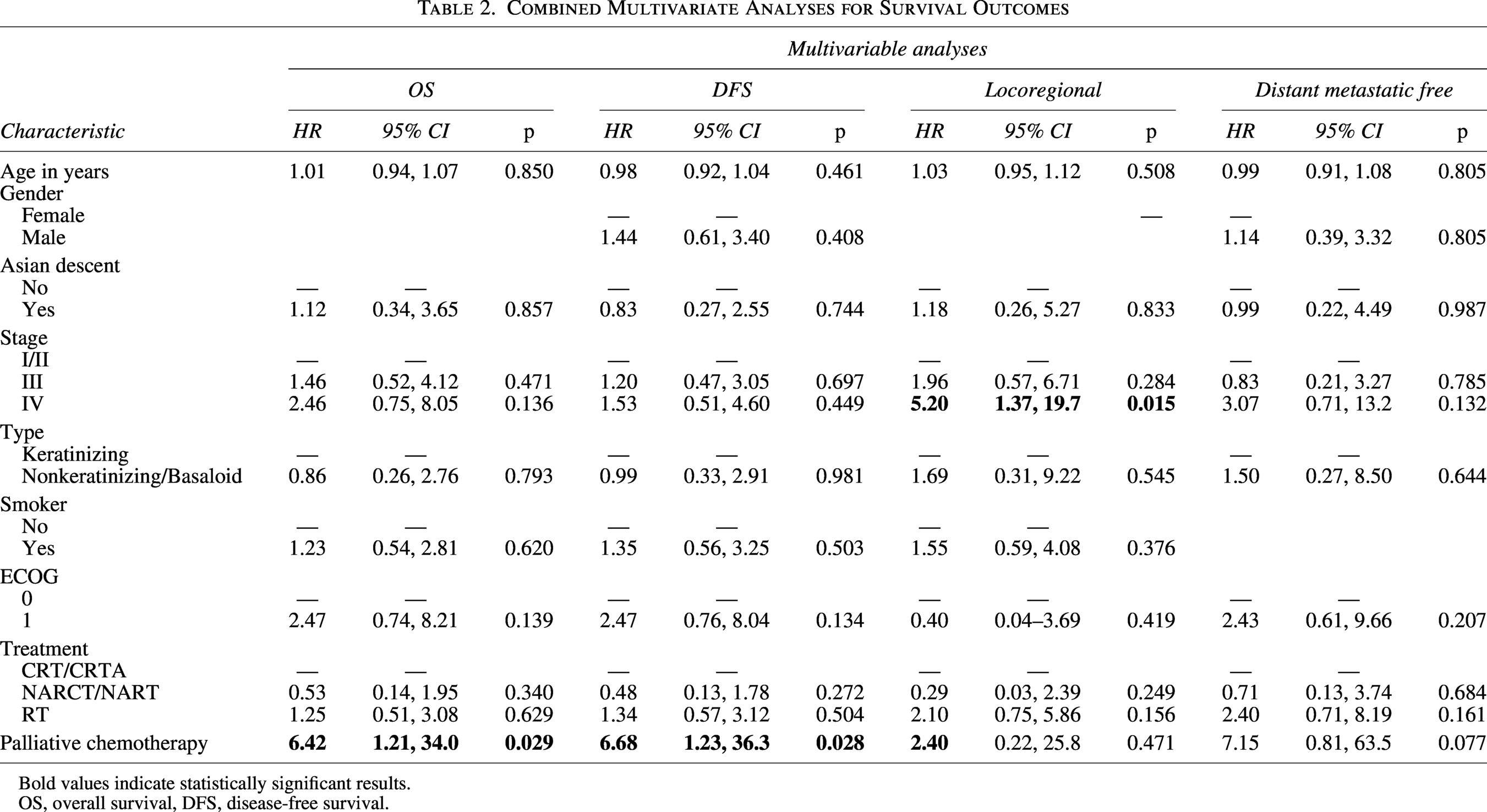
Bold values indicate statistically significant results.
OS, overall survival, DFS, disease-free survival.
DFS at 5 years was 78% Stage I/II, 77% Stage III, and 66% Stage IV (p = 0.4) as shown in Figure 1B. With regards to treatment groups, DFS at 5 years was 73% for CRT/CRTA, 85% for NARCT/NART, 79% for RT alone, and 0% for the palliative group (p < 0.001), as shown in Figure 2B.
Multivariate analysis using Cox regression for DFS demonstrated that patients in the palliative chemotherapy treatment group were more likely to have an increased risk of death from recurrence or disease (HR of 6.68, CI = 1.23–36.3, p = 0.028).
The cumulative incidence of locoregional relapse at 5 years was 4% for Stage I/II, 11% for Stage III, and 25% for Stage IV (p = 0.2) as shown in Figure 1C. With regards to treatment groups (Fig. 2C), cumulative incidence of locoregional relapse at 5 years was 14% for CRT/CRTA, 7% for NARCT/NART, 12% for RT alone, and 33% for the palliative chemotherapy group (p = 0.4). On multivariate analysis, patients with Stage IV disease had a higher risk of locoregional recurrence or death from recurrence (HR of 5.20, CI = 1.37–19.7, p = 0.015).
Furthermore, cumulative incidence of distant metastases at 5 years was 15% for Stage I/II, 11% for Stage III, and 36% for Stage IV (p = 0.04), as shown in Figure 1D. By treatment groups shown in Figure 2D, the cumulative incidence of distant metastases at 5 years was 14% for CRT/CRTA, 14% for NARCT/NART, 21% for RT alone, and 67% for the palliative chemotherapy group (p = 0.7).
There were no other significant variables for survival outcomes on multivariate analyses (p > 0.05).
Late effects
We defined late effects as side effects present 6 months and beyond post-treatment.
As shown in Table 3, in our cohort, the most common long-term toxicity was chronic xerostomia, reported in 67% of patients. In terms of other aspects of oral health or dental hygiene, 2% had dental caries, 8% of participants required dental extraction post-treatment, but only 1% of them required dental implants. Additionally, 20% reported ongoing trismus and 5% reported temporomandibular joint (TMJ) dysfunction.
Late Effects and Complications
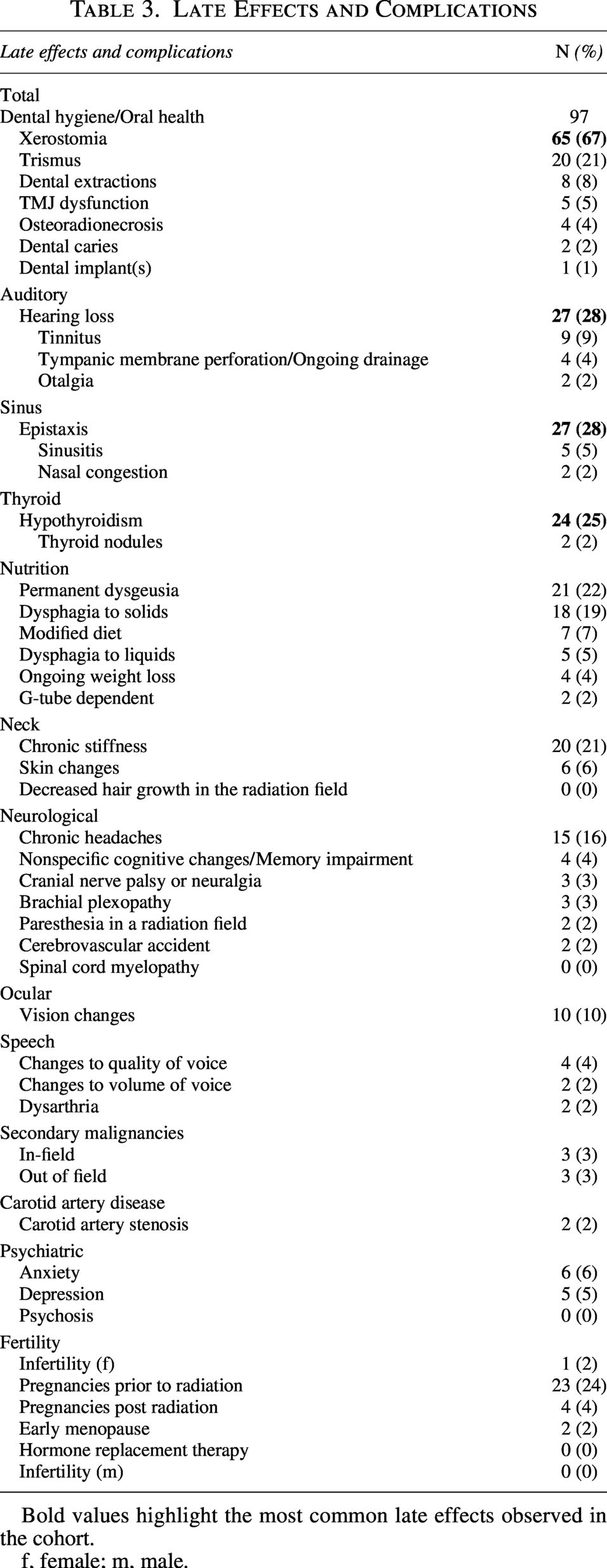
Bold values highlight the most common late effects observed in the cohort.
f, female; m, male.
The second most late side effects reported were chronic epistaxis and hearing loss, reported in 28% of patients. Other sinus-related toxicities include chronic sinusitis (5%) and nasal congestion (2%). Auditory-related toxicities included tinnitus (9%), tympanic membrane perforation/ongoing drainage (4%), and otalgia (2%).
With regard to thyroid function, 25% of patients went on to develop hypothyroidism post-treatment, and two other participants had documented thyroid nodules, which were benign on follow-up.
Twenty-one (22%) patients reported permanent dysgeusia. Following that, 19 (19%) patients reported persistent dysphagia to solids, and out of that group, 5 also experienced dysphagia to fluids. Furthermore, 6 out of those 19 patients required diet modification, and 2 patients had documented ongoing weight loss. Two patients were G-tube dependent, one secondary to dysphagia and the other secondary to severe trismus. Osteoradionecrosis was seen in 4% of patients.
With regards to speech, 4% reported changes to the quality of their speech, and two out of the four reported changes to the volume as well. Two participants reported experiencing dysarthria.
In terms of neurological complications, there were two cases (2%) of nonfatal cerebrovascular accidents recorded. Other relevant late toxicities include chronic headaches (15%), nonspecific cognitive changes/memory impairment (4%), brachial plexopathy (3%), cranial nerve palsy/neuralgia (3%), and paresthesias in the radiation field (2%).
With regard to effects on the reproductive system, there was one (1%) documented case of infertility in one female patient out of 41 patients. There were no documented cases of infertility in male patients. Twenty-three (24%) female patients had documented pregnancies prior to treatment, and four (4%) had pregnancies post-treatment. There was one (1%) case of pregnancy complication in a patient who was pregnant post-treatment. There were two (2%) patients with early menopause post-treatment, neither of which required hormone-replacement therapy (HRT).
Other late effects included two (2%) cases of carotid artery stenosis and ten (10%) cases of vision changes. Additionally, six (6%) patients reported skin changes in the radiation field.
There were three (3%) cases of in-field secondary malignancies: Bilateral squamous cell carcinoma of the external auditory canals, high-grade epithelioid sarcoma of the right paracervical muscle, and squamous cell carcinoma of the oropharynx. The median time for the development of these secondary malignancies was 20 years. Additionally, there were three (3%) cases of out-of-field secondary malignancies, which consisted of sigmoid adenocarcinoma, breast cancer, and dermatofibrosarcoma protuberans.
Lastly, we also investigated treatment effects on the patients’ mental health. Five reported depression and six reported anxiety. There were no reported cases of psychosis.
Discussion
While previous studies have explored outcomes of NPC in the AYA population, most have originated from endemic regions such as China. Given the rarity of NPCs, especially in AYA, very few have originated from nonendemic areas. Our study focused on the treatment outcomes of this specific AYA population in British Columbia, Canada, as well as treatment late effects.
Overall and disease-free survival
Previous larger studies on NPC in the general population in China have shown 5-year overall survival rates of 100% for Stage I, 94.3% for Stage II, 83.6% for Stage III, and 70.5% for Stage IV. 7 Survival outcomes of NPC in nonendemic regions have been noted to be slightly worse. On the higher end, a Canadian study published in 2021 analyzing 601 patients demonstrated 5-year OS rates of 90% for Stage I, 77% for Stage II, 72% for Stage III, and 42% for Stage IV. 8 On the lower end, a study based out of the United States demonstrated overall 5-year survival rates of 76.94% for Stage I/II, 78.92% for Stage III, and 41.69% for Stage IV. 9 Another study based out of Sweden demonstrated a 5-year OS rate of 83.6% for Stage I/II, 69.3% for Stage III, and 68.6% for Stage IV. 10 All the patients in the aforementioned studies were treated with RT alone or a combination of CRT (either concurrent CRT, neoadjuvant plus concurrent CRT, induction RT, or concurrent CRT plus adjuvant). The 5-year OS rate in our cohort was 81% for Stage I/II, 80% for Stage III, and 68% for Stage IV, which is in keeping with published survival outcomes in nonendemic regions.
When comparing our results with previous NPC in AYA studies, our survival outcomes are comparable. Other literature on NPC in pediatrics and adolescents based out of Sun Yat-sen University Cancer Center described a 5-year OS rates of 85.4% for Stages I–III, and 79.7% for Stage IV and 5-year DFS rates of 86.4% for Stages I–III, and 73.5% for Stage IV. 11 Another study also described a 5-year OS rate of 88.2% and 5-year DFS rate of 85.3%. 12 It is important to note that the current standard of care for Stage II+ patients includes neoadjuvant chemotherapy followed by chemoradiation for NPC, which is associated with improved overall survival; however, the majority of our cohort did not receive this treatment as it was not standard of care during that time, which may have resulted in lower 5-year OS rates compared to published literature. 13
Treatment modality effects
In our study, the addition of neoadjuvant and/or adjuvant chemotherapy with RT (NARCT/NART) conferred the best survival rate (5-year OS 93% and DFS 85%), followed by RT alone (5-year OS 79% and DFS 79%) and CRT/CRTA (5-year OS 75% and DFS 73%). The higher survival for patients receiving neoadjuvant chemo has been demonstrated in meta-analyses. 14 As expected, the patients receiving palliative-intent chemotherapy had very poor survival and DFS. These findings are consistent with existing literature in both pediatric/AYA and adult NPC.12,15
Locoregional relapse and distant metastasis
A large cohort study based out of China described a 5-year local recurrence-free survival of 89.7%, regional recurrence-free survival of 94.5%, and distant metastasis-free survival of 85.6%. 15 A separate study reported a 5-year occurrence rates of locoregional and distant failures of 7.4% and 17.4%, respectively. 16 Advanced-stage NPC is associated with a higher rate of locoregional and distant relapse, with the latter being the predominant mode of failure. The cumulative incidence of locoregional relapse at 5 years for our study was 4% Stage I/II, 11% Stage III, and 25% Stage IV (p = 0.2), which, although not statistically significant, shows a clear trend consistent with the literature. The cumulative incidence of distant metastases at 5 years was 15% Stage I/II, 11% Stage III, and 36% Stage IV (p = 0.04).
Late effects
Increasing age has been associated with a poorer prognosis and NPC-related mortality; however, younger age has been associated with a higher risk of long-term complications. Given improving survival outcomes, it is important to analyze survivorship in this population.8,17 In a head-to-head study comparing long-term QoL between pediatric and adult NPC patients, the former group reported significantly better outcomes in global health status but poorer cognitive function. 18
The most commonly reported treatment-related toxicities in NPC are xerostomia, neuropathy, and hearing loss or tinnitus.11,12 Along that same line, a study published in 2014 demonstrated that neuropathy, hearing loss, and xerostomia had a statistically significant impact on the general QoL of their cohort. 19 Another study also corroborated that the most common treatment late effect was xerostomia, with 605 out of 775 (78.1%) patients. 20 Following that, hearing loss is the second most reported toxicity in their study. These findings are consistent with our study.
Overall, the late effects of NPC treatment are comparable between the AYA and adult populations; however, the AYA population faces distinct vulnerabilities as treatment-related toxicities often surface during a critical period of life planning and identity formation. Furthermore, although the survival outcomes of AYA cancer patients are initially higher compared to the general population, their survival declines faster in the long term compared to the general population due to late toxicities and second malignancies. 21 Therefore, these factors underscore the need for more tailored treatment plans to help mitigate the associated toxicities and preserve long-term QoL. Previous smaller studies have explored the potential role of interferon ß as an adjunct in NPC in the pediatric and AYA population to reduce radiation dose and, as a consequence, treatment-related effects; however, there is still insufficient high-level evidence from large, randomized clinical trials to support its routine use. 22 Survivorship care clinics to provide specialized and long-term coordinated care have also shown to be beneficial for the AYA population.23–25
Strengths and limitations
The strengths of our study include its population-based design examining a relatively rare cancer in the AYA population within a nonendemic country. We had long-term follow-up on patients and were able to comprehensively evaluate treatment, survival outcomes, and late toxicities. Limitations include the long retrospective study period and the absence of systematically collected patient-reported outcomes.
Conclusion
Our study provides insight into the limited literature on NPC in the AYA population in a nonendemic region. Our cohort demonstrated survival outcomes comparable to the existing literature on the general population globally, with a clear trend toward worse outcomes with advanced-stage disease as well as improved outcomes with chemoradiation therapy. Furthermore, this study also corroborated the burden of late treatment-related toxicities seen in NPC survivors. These late effects may impact the AYA population more profoundly given the critical life stage during which they occur. Lastly, NPC survivors face a distinct subset of treatment-related toxicities, which is primarily driven by intensive head and neck radiotherapy, therefore underscoring the need for AYA-specific survivorship strategies focusing on minimizing late effects and preserving QoL. Further prospective studies focusing on risk-adapted therapy and long-term follow-up protocols are needed to achieve balance between oncologic control and long-term survivorship outcomes in this unique population.
Authors’ Contributions
S.H.: Investigation, writing—original draft, writing—review and editing, and visualization. A.D., M.C., K.G., N.C., J.W., E.B., E.T., and D.S.: Conceptualization and writing—review and editing. R.M.: Formal analysis and visualization. S.N.H.: Conceptualization, data curation, funding acquisition, methodology, project administration, resources, supervision, validation, and writing—reviewing and editing.
Ethical Considerations
This study was approved by the University of British Columbia—BC Cancer Research Ethics Board (UBC BC Cancer REB; Approval No. H23-03415).
Consent to Participate
The requirement for written informed consent was waived by the Research Ethics Board due to the retrospective design.
Data Availability
Aggregate data supporting the findings of this study are included in the article. Individual-level data are not publicly available due to ethical and privacy restrictions related to human participant data.
Footnotes
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.