
Abstract
Purpose:
This study aimed to explore sexual health among young Danish cancer patients aged 18–39 years and to generate exploratory insights into how sexual health may differ by age, gender, treatment status, and treatment type.
Methods:
A descriptive observational study was conducted from January 2023 to September 2024. Participants completed the European Organization for Research and Treatment of Cancer Sexual Health Questionnaire. Sexual health outcomes were compared across age groups and gender, between participants undergoing treatment with those post-treatment, and participants that underwent surgery only versus those who received systemic treatment or/and radiation, with or without surgery.
Results:
Fifty-eight young adults participated (60.3% male, mean age 29 years); 67% had oncological cancers. The most frequently reported challenges involved communication with healthcare professionals, perceptions of femininity, and treatment’s impact on sexual activity. Female participants reported lower sexual satisfaction, reduced libido, more sexual pain, treatment impact on sexual activity, and higher fatigue than male participants. Those undergoing active treatment reported greater reduction of libido, treatment impact on sexual activity, and partner-related insecurity compared to those post-treatment. No considerable differences were found between age groups or treatment type.
Conclusions:
Young adults with cancer face sexual health challenges, regardless of age and treatment intensity. Female participants and those undergoing active treatment report a higher sexual health burden. These findings underscore the need for tailored interventions to address and support sexual health throughout the cancer trajectory.
Introduction
In 2019, the global incidence of cancer among young adults aged 18–39 years was 44.99 per 100,000, and this number continues to rise. 1 This growing trend underscores the urgent need to understand and address the unique challenges faced by young adults with cancer. Young adulthood is a critical developmental stage marked by significant personal, social, and emotional milestones.2–4 In this period individuals often initiate and explore sexual and romantic relationships, develop sexual identity, and plan parenthood.2,4 A cancer diagnosis during this formative time can therefore have profound and lasting effects on multiple aspects of well-being, particularly sexual health.2,5 The World Health Organization (WHO) defines sexual health as a state of physical, emotional, mental, and social well-being in relation to sexuality—not merely the absence of disease or dysfunction. 6 Cancer-related sexual health challenges are often shaped by a complex interplay of biological, psychological, interpersonal, and sociocultural factors. 3 These challenges may affect multiple domains of functioning and lead to a significant reduction in overall quality of life.7,8
Previous research has shown that young adult cancer survivors commonly experience a range of sexual health issues, including pain during intercourse, reduced libido, body image concerns, vaginal dryness, fatigue, urinary incontinence, and difficulties in partner relationships.4,9 These disruptions can delay or inhibit key life experiences, such as the initiation of sexual intimacy and the development of romantic partnerships.8,10 Despite these challenges, the biomedical aspects of cancer care have historically taken precedence, and sexual health concerns in young adults have often been overlooked—due in part to their age, the prioritization of survival, and the intensity of treatment. 10
Young adults often receive aggressive treatment regimens, increasing the risk of acute and long-term side effects. 11 Studies indicate that young adults with cancer report lower satisfaction with their sexual lives than their healthy peers and continue to experience significant concerns related to sexual health well into survivorship.2,5 In a recent cross-sectional study, 22.3% of 776 young adults with cancer reported experiencing one or more sexual health issues within the previous week, including distorted body image and reduced sexual and romantic capacity. 12 These findings reinforce that sexual health is a key component of quality of life for young adults affected by cancer.8,10,13
International guidelines recommend that sexual health should be routinely addressed by health care professionals in oncology. 14 However, further clarification is needed regarding the appropriate timing within the cancer trajectory for initiating these conversations, as well as the specific topics that should be covered to ensure they are relevant and responsive to the needs of young adults with cancer. 14 In response to this need, the European Organization for Research and Treatment of Cancer (EORTC) recently developed the EORTC QLQ-SH22, a validated instrument designed to assess sexual health-related quality of life in cancer patients, both during treatment and in survivorship. 15 While this tool offers a valuable foundation, there remains a need to better understand how sexual health concerns manifest across different clinical subgroups of young adults with cancer. To our knowledge, this is the first study to apply the EORTC QLQ-SH22 to examine sexual health among young adults with cancer. Applying the EORTC QLQ-SH22 to identify specific sexual health challenges experienced by young adults with cancer offers valuable insights that can inform clinical practice. This study aimed to explore sexual health among young Danish cancer patients aged 18–39 years and to generate exploratory insights into how sexual health may differ by age, gender, treatment status, and treatment type.
Materials and Methods
Study design
This study is a descriptive observational study. The study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines 16 to ensure transparency and methodological rigor.
Setting
The study was conducted at the University Hospital of Copenhagen, Rigshospitalet, from January 2023 to September 2024.
Participant and recruitment
The inclusion criteria were as follows: aged 18–39 years, a confirmed cancer diagnosis, sufficient mental capacity to answer a questionnaire, ability to understand the language of the questionnaire, and having read and understood the information sheet. Purposive sampling was utilized to ensure variation in age, gender, tumor site, treatment and disease status. The sample size aimed for an equal distribution across four groups: (1) Patients treated with surgery only; (2) patients undergoing curatively intended first-line cancer treatment, with or without surgery; (3) patients in life-extending cancer treatment, with or without surgery; and (4) patients in follow-up after first-line therapy with or without surgery with no evidence of disease, spanning six months to 5 years posttreatment.
Participants were recruited between April 2023 and August 2024 through clinical staff at oncological or hematological units at Copenhagen University Hospital, Rigshospitalet, Odense University Hospital, Zealand University Hospital, Roskilde, and Aarhus University Hospital. Additionally, the patient organization Young Cancer posted information about the study and provided contact details for the research team on their Facebook page. No participants declined to participate during the recruitment process.
Assessment instrument
Participants completed the EORTC QLQ-SH22 questionnaire, a 22-item valid questionnaire designed for both male and female cancer patients, applicable at various stages of treatment and during survivorship. 15 The questionnaire aims to capture the quality of life related to sexual health as a multidimensional construct, aligning with the WHO’s definition of sexual health. It comprises two multi-item scales aimed at assessing sexual pain (e.g., item 8: Have you been worried that sex would be painful?) and sexual satisfaction (e.g., item 3: Have you been satisfied with your level of sexual desire?). Additionally, it includes 11 single items that evaluate sexual activity (e.g., item 1: How important to you is an active sex life?), treatment-related and partner-related questions (e.g., item 7: Has the treatment affected your sexual activity?), general questions about sexual health (e.g., item 9: Have you had communication with health professionals about sexual issues?), and four gender specific questions (e.g., item 16: Have you felt less feminine as a result of your disease or treatment?, item 15: Have you felt less masculine as a result of your disease or treatment?). 15 The responses were converted to continuous data ranging from 0 to 100 using the EORTC QLQ-SH22 scoring manual, where a high score represents a high level of symptomatology or problems. 15 In calculating the scores for the items, the following are reversed: sexual activity (item 1), communication with health care professionals (item 9), confidence erection (item 14b), and sexual satisfaction (items 3, 4, 10, 12, 17, 18a, 19a, and 21a) according to the scoring manual. 15 The multi-item scales consist of sexual satisfaction and sexual pain. Sexual pain comprises two questions (items 8 and 11) and one conditional item (item 20a), whereas sexual satisfaction consists of five questions (items 3, 4, 10, 12, and 17) and three conditional items (items 18a, 19a, and 21a). 15
Data collection
Data were collected face-to-face, where participants completed the questionnaires independently (N = 18), or via phone, where the interviewer read the questions aloud and recorded the participants’ responses (N = 42). Each participant was given the opportunity to choose their preferred data collection method. Sociodemographic data and clinical characteristics were collected using a questionnaire including, for example, age, gender, relationship status, diagnosis, treatment status, and treatment received.
Statistical analysis
Sociodemographic and clinical characteristics are presented as means, standard deviations (SD), and frequencies. Except for time since diagnosis, sociodemographic and clinical characteristics were treated as categorical variables in the statistical analysis. Age was categorized into two groups, 18–29 years and 30–39 years. Cancer diagnosis was classified as oncological cancer, hematological cancer and other. For each participant, scores for single items as well as the two multi-item scales, sexual satisfaction and sexual pain, were calculated. Participants who responded “not relevant” to a question were still included in the study; however, their multi-item scale score were calculated excluding the questions marked as “not relevant” in line with the scoring manual from EORTC. 17 The scores are reported as mean and SD for each item.
A comparison was made between participants currently undergoing treatment and those who had completed their treatment. In addition, we compared sexual health between participants who underwent surgery only and those who received systemic treatment and/or radiation with or without surgery. Results are reported as mean ± SD. Additionally, sexual health outcomes were compared across age groups (18–29 years vs. 30–39 years) and gender (male vs. female). To assess exploratory trends between age groups and gender, unpaired t-tests were used. 18 t-Tests were applied only in comparisons where the two groups were of sufficiently similar size to ensure stable variance estimates and adequate statistical power. For groupings characterized by very small samples, analyses were limited to descriptive statistics. A significance level of p ≤ 0.05 was considered statistically significant. 18 All data analyses were performed using STATA 16.0.
Ethics
All participants received verbal and written information about the study and provided informed consent after having the opportunity to ask questions. They were explicitly informed that participation was voluntary and that they could withdraw their consent at any time without any consequences for their cancer treatment in accordance with the Declaration of Helsinki. 19 The study was approved by the Danish Data Protection Agency on January 10, 2023 (ID: P-2023-39). Ethical approval was not required from the scientific ethical committee under Danish legislation, as the study involved cross-sectional questionnaires without any further intervention. 20
Results
Sociodemographic and clinical characteristics
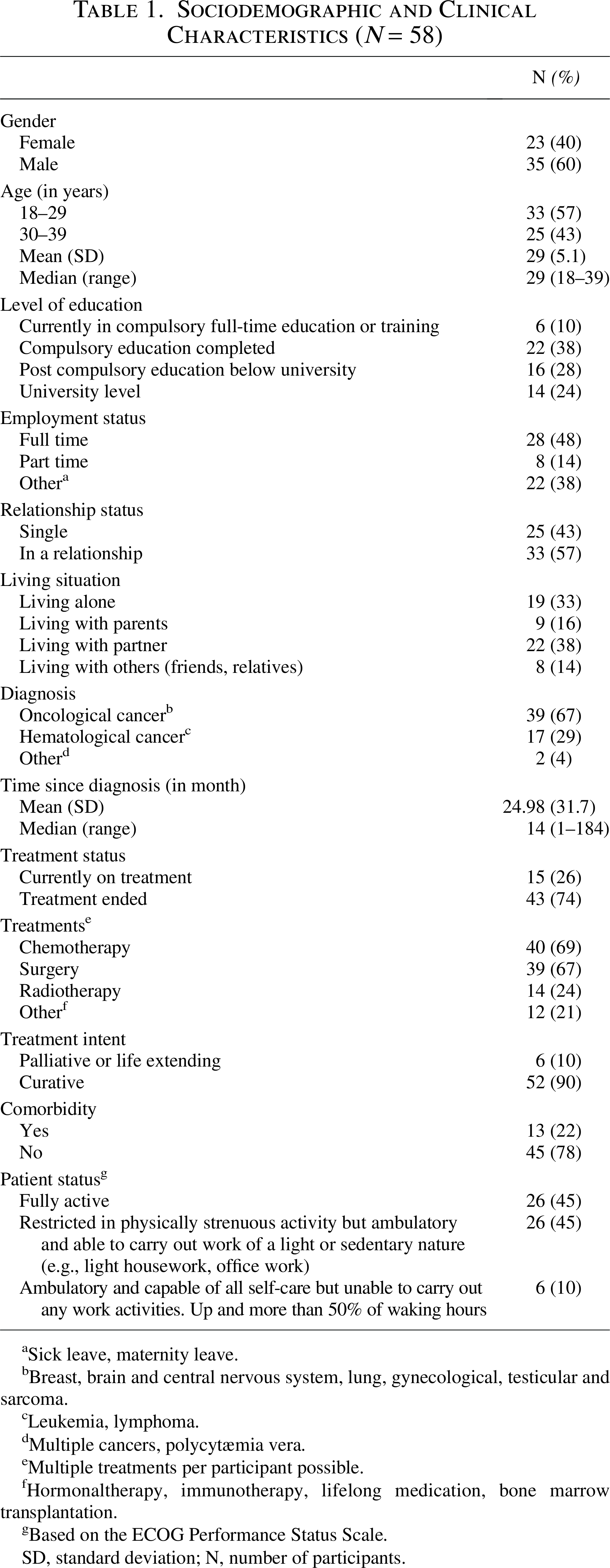
Sixty individuals were recruited, of whom 58 were included in the final analysis; one participant did not complete the EORTC QLQ-SH22, and one had five missing responses. Among those included in the analysis, the majority were male (60.3%) and had an oncological cancer diagnosis (67%). Approximately one-third were undergoing active treatment, and around half reported being in a relationship (Table 1).
Sociodemographic and Clinical Characteristics (N = 58)
Sick leave, maternity leave.
Breast, brain and central nervous system, lung, gynecological, testicular and sarcoma.
Leukemia, lymphoma.
Multiple cancers, polycytæmia vera.
Multiple treatments per participant possible.
Hormonaltherapy, immunotherapy, lifelong medication, bone marrow transplantation.
Based on the ECOG Performance Status Scale.
SD, standard deviation; N, number of participants.
EORTC QLQ-SH22 score
The EORTC QLQ-SH22 scores indicate that the most prominent issue reported by participants related to communication with health care professionals (mean = 87.5). This was followed by concerns about femininity (mean = 68.1), the impact of treatment on sexual activity (mean = 53.3), and fatigue (mean = 45.4). In contrast, worry about incontinence (mean = 6.3) and sexual pain (mean = 17.2) were among the least frequently reported symptoms (Fig. 1).
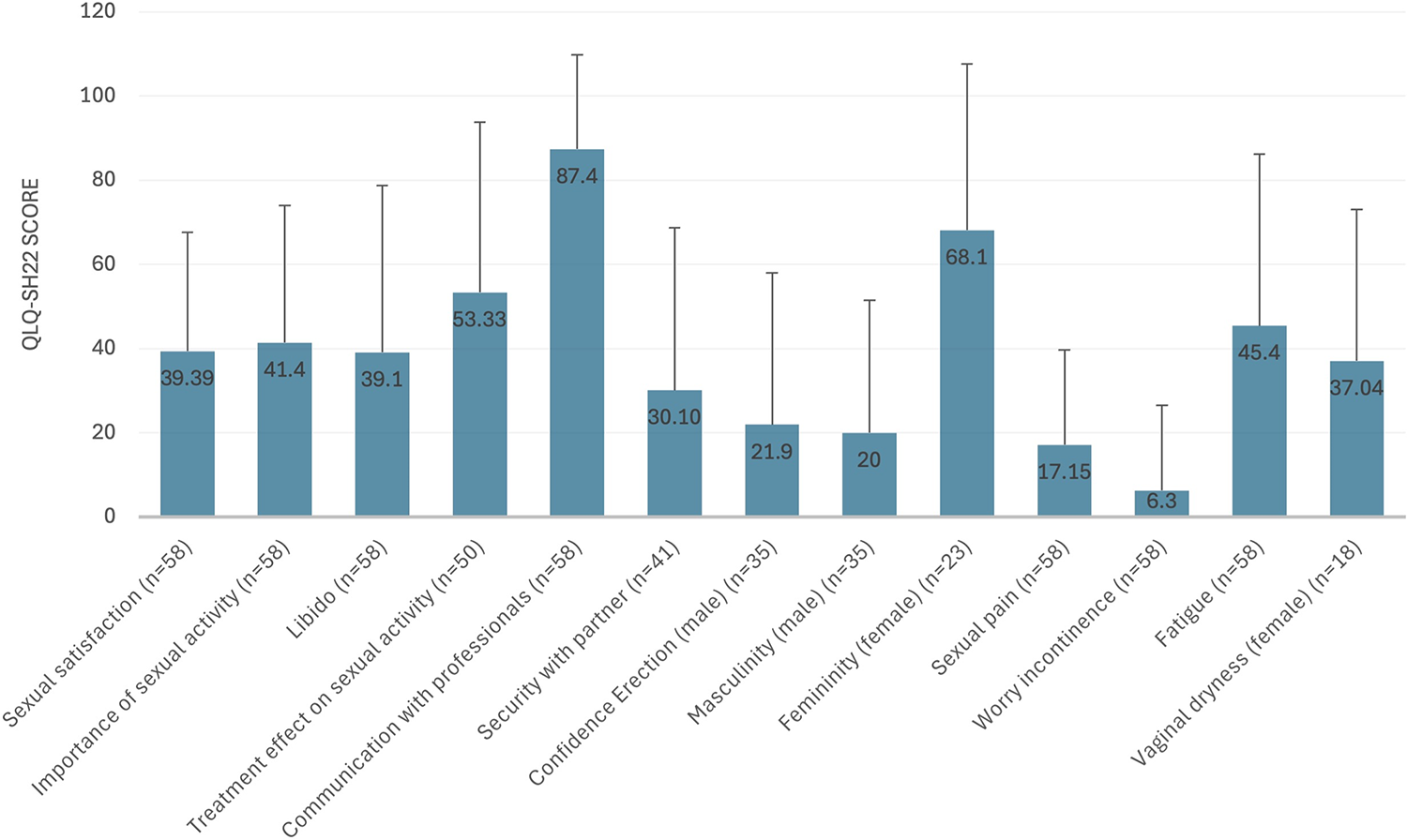
Mean item scores on the EORTC QLQ-SH22 (N = 58). EORTC QLQ-SH22, European Organization for Research and Treatment of Cancer Sexual Health Questionnaire.
Exploratory comparison of quality of life related to sexual health by age and gender
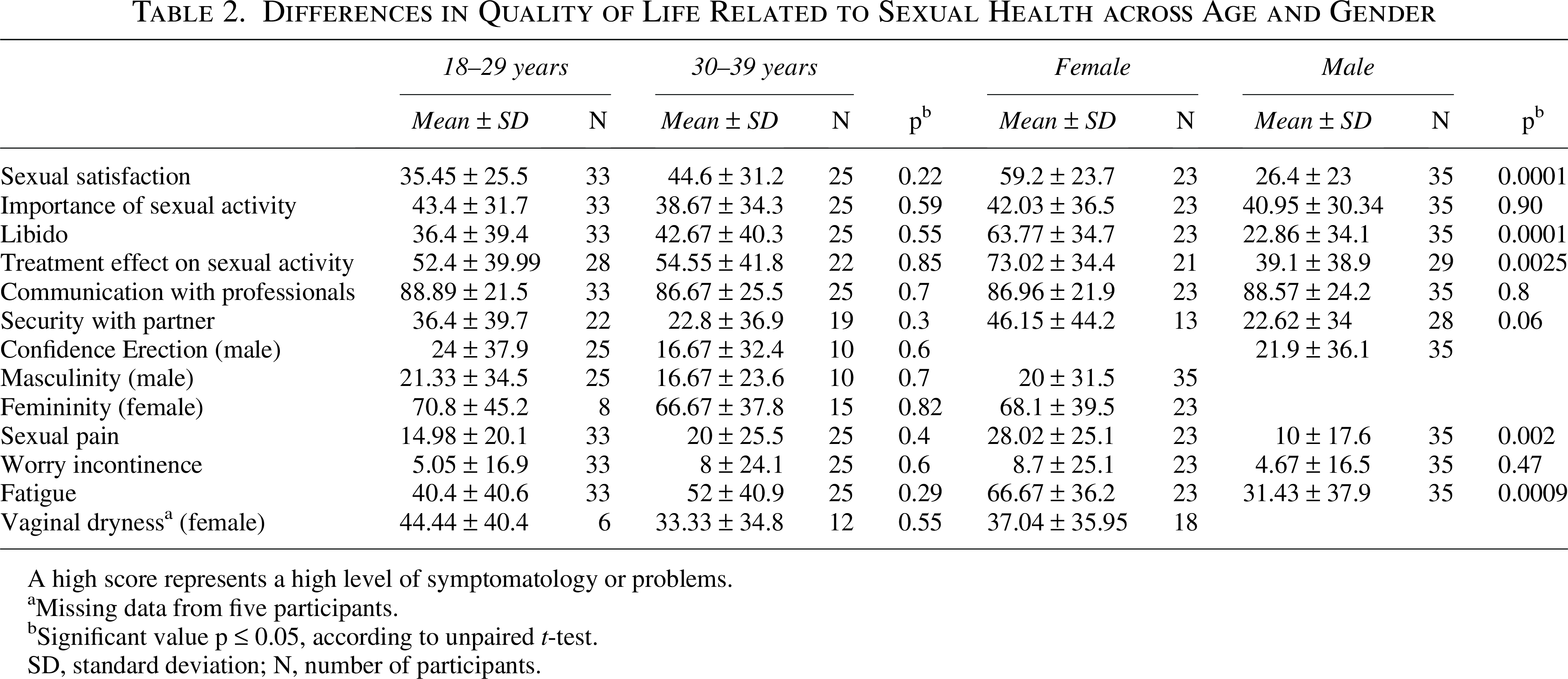
No statistically significant differences were observed between the two age groups (18–29 years vs. 30–39 years). However, female participants reported significantly higher levels of symptomatology and problems compared to males, indicating exploratory trends in several domains: sexual satisfaction (mean 59.2 vs. 26.4, p = 0.001), decreased libido (mean 63.8 vs. 22.9, p = 0.001), treatment impact on sexual activity (mean 73.0 vs. 39.1, p = 0.0025), sexual pain (mean 28.0 vs. 10.0, p = 0.005), and fatigue (mean 66.7 vs. 31.4, p = 0.0009). The least reported issue for both groups was worry about incontinence (mean 8.7 vs. 4.7, p = 0.47). No significant gender differences were identified in the remaining scales (Table 2).
Differences in Quality of Life Related to Sexual Health across Age and Gender
A high score represents a high level of symptomatology or problems.
Missing data from five participants.
Significant value p ≤ 0.05, according to unpaired t-test.
SD, standard deviation; N, number of participants.
Influence of cancer treatment on sexual health
Participants currently undergoing treatment reported higher levels of symptomatology and problems compared to those post-treatment. Notably, they reported greater issues related to libido (57.8 vs. 32.6), treatment impact on sexual activity (73.3 vs. 44.8), and feelings of insecurity with their partner (53.3 vs. 22.6). In contrast, post-treatment participants reported slightly higher levels of problems related to erectile confidence and perceptions of femininity (Fig. 2). A full overview of results is available in Supplementary Data.
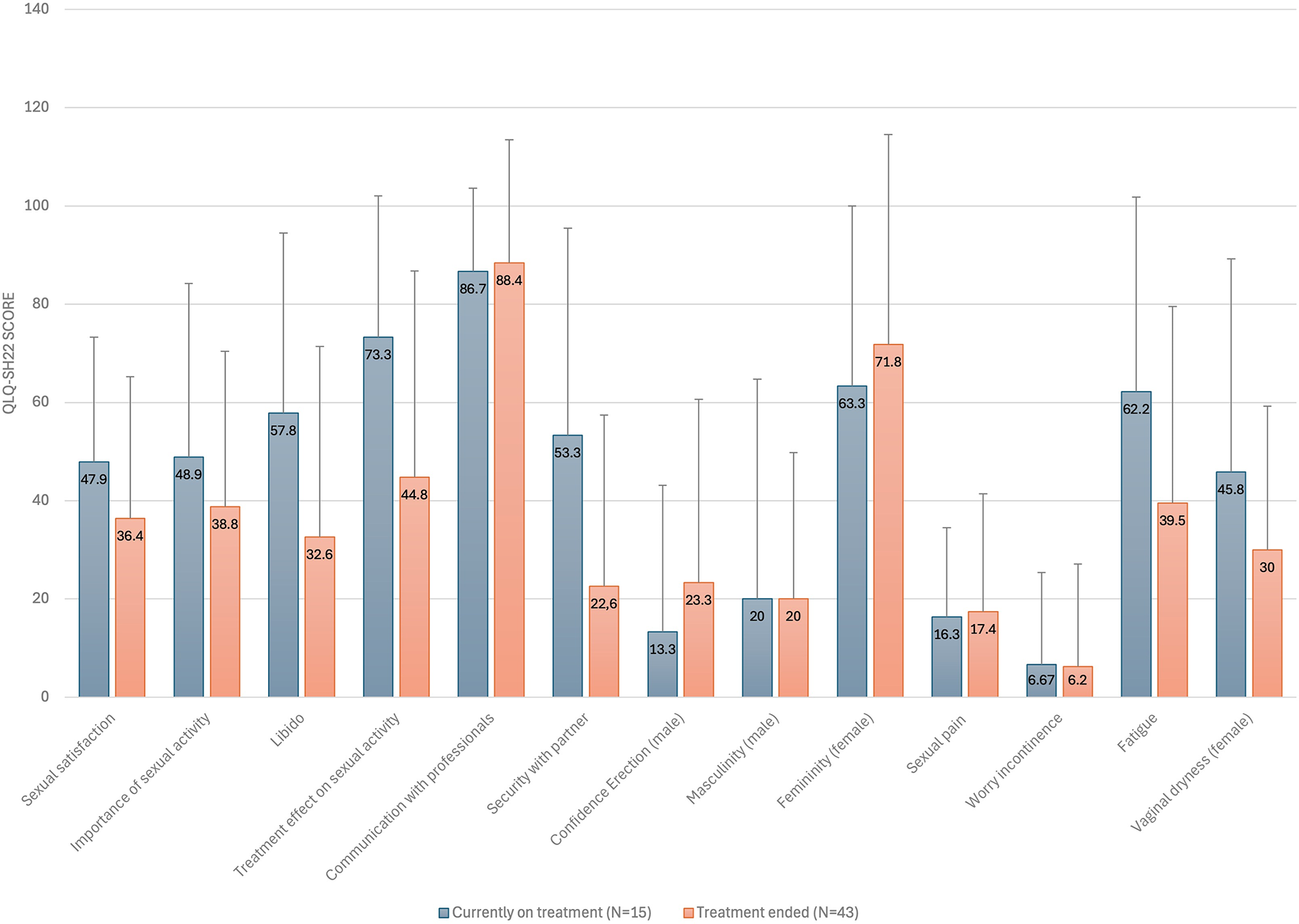
Differences in quality of life related to sexual health across treatment status.
Influence of treatment modalities on sexual health post-treatment
Participants who received systemic treatment and/or radiation with or without surgery reported higher levels of symptomatology or problems, particularly regarding the impact of treatment on sexual activity (54.5 vs. 28.2), than those who underwent surgery alone. In both groups, the most frequently reported issues were related to communication with healthcare professionals (90.1 vs. 85.4) and perceptions of femininity (73.3 vs. 66.7) (Table 3).
Differences in Quality of Life Related to Sexual Health Posttreatment Comparing Systemic/Radiation ± Surgery Versus Surgery Only

A high score represents a high level of symptomatology or problems.
Missing data from five participants.
SD, standard deviation; N, number of participants.
Discussion
This descriptive observational study represents the first application of the EORTC QLQ-SH22 questionnaire in a population of young adults with cancer. The findings show that young adults with cancer reported substantial sexual health challenges, with communication with health care professionals being the most prominent issue. The results suggested potential exploratory trends, with no age-related differences observed, but with female participants reporting higher symptom levels than male participants across several domains. Those undergoing treatment experienced greater difficulties with libido, sexual activity, and partner insecurity compared to post-treatment participants, who still reported ongoing concerns. No considerable differences were seen between current treatment and post-treatment, though systemic therapy was linked to slightly higher symptom burden. Ultimately, these findings contribute to the growing evidence base and offer important implications for improving sexual health among young adults with cancer. Insights gained from the EORTC QLQ-SH22 questionnaire may help refine clinical practice, supporting the development of more patient-centered approaches in oncology care.9,21,22
The EORTC QLQ-SH22 scores underscore the multifaceted challenges young adults with cancer face regarding sexual health. These findings align with prior work, including Åsberg et al., 23 who demonstrated poorer sexual health among cancer survivors compared with age-matched cancer-free controls, with particular differences in libido and partner-related insecurity. In their subgroup of young adults aged 18–39 years, the comparison included 24 cancer survivors and 1570 cancer-free controls. 23
Communication challenges with health care professionals emerged as a central issue, echoing previous literature.2,24,25 For example, Albers et al. (N = 56) found in a cross-sectional study that only 21% of young adults with cancer were satisfied with discussions about sexuality with health care professionals, despite over 90% valuing such conversations. 24 Barriers to initiating conversations about sexual health include lack of provider training, cultural taboos, and discomfort around the topic.24,26,27 Young adults report that they often feel dismissed when initiating sexual health discussions.2,26 Cultural differences may also influence how sexuality is perceived and whether patients feel comfortable discussing these concerns,2,28 but this does not diminish the importance of integrating sexual health into cancer care. A scoping review by Alqaisi et al. 29 emphasizes the need for educational and organizational strategies such as training programs, structured documentation tools, and system support to improve communication about sexual health. Frameworks such as Permission, Limited Information, Specific Suggestions, Intensive Therapy (PLISSIT) and Bring up, Explain, Tell, Time, Education, Record (BETTER) are highlighted as potential approaches to facilitate more effective communication about sexual health.29,30
Our study indicated no significant age-related differences in sexual health concerns, indicating that these issues are consistently relevant across the full young adult age range (18–39 years). This finding aligns with previous research by Graugaard et al., 12 (N = 822), who similarly reported no statistically significant differences in age in the negative impact of cancer on body image or sexual and romantic functioning among patients aged 17–36 years. 12 In contrast to age, notable gender differences emerged: female participants reported significantly higher levels of sexual dissatisfaction, fatigue, decreased libido, sexual pain, and negative treatment impacts on sexual activity compared to their male counterparts. However, the item on sexual activity does not clarify whether responses should reflect partnered or solo activity, which introduces ambiguity that may limit the measure’s content validity and the strength of the study’s conclusions.
Our results support previous research highlighting gender disparities in cancer-related sexual health outcomes. 9 While Greimel et al. 9 (N = 444) found no gender differences in specific domains such as libido and sexual satisfaction in a study primarily involving adults over 40 years of age, 9 our findings revealed significant gender disparities in these areas, suggesting that such differences may be more pronounced in younger populations. This pattern underscores the importance of integrating gender-sensitive approaches into sexual health rehabilitation for young adults with cancer.
Participants undergoing treatment experienced greater challenges, particularly in libido, partner security, and treatment impact on sexual activity, compared to those post-treatment. This supports findings by Oberguggenberger et al. 25 (N = 394) and may reflect the concept of response shift, 31 where patients adapt over time, altering their perception of QoL. Regarding partner-related security, our study found that participants currently undergoing treatment reported considerably higher levels of insecurity with their partner, an observation that contrasts with previous literature. 25 This finding may indicate a potential age-specific difference in how cancer treatment impacts relationship dynamics and sexual health-related quality of life in young adults.
Regarding treatment types, the results suggest that, for young adults, the impact of surgery only may be equivalent to that of systemic therapy and/or radiation (with or without surgery) in relation to the impact on sexual health. This finding contrasts with the study by Oberguggenberger et al. 25 (N = 394), which reported a greater symptom burden among older adults receiving intensified treatment compared to surgery alone, potentially indicating an age-specific difference in how treatment modalities affect sexual health. 25 The results indicated that the impact of treatment on sexual activity may be more pronounced among those receiving systemic therapy and/or radiation. However, others have found that both scarring and the physical demands of intensive treatments can adversely affect body image and overall sexual well-being.3,32
Strengths and limitations
A strength of this study is the use of a standardized, validated international questionnaire, which enables cross-country comparisons. Another strength is the heterogeneity of participants in terms of cancer types and the near-equal representation of the two age groups (18–29 and 30–39 years), enhancing the generalizability. Efforts to achieve equal distribution across the four predefined subgroups were not fully successful, possibly introducing selection bias and limiting external validity. Another limitation is the small sample size in some analyses of subgroups, which may reduce statistical power, increase susceptibility to outliers, and make subgroup comparisons more vulnerable to bias and overinterpretation. The sensitive nature of the topic may have introduced reporting bias, with participants potentially providing socially desirable responses. Although telephone surveys improved accessibility, discussing sensitive topics with a research coordinator may have introduced social desirability bias, potentially leading to underreporting of sexual activity or concerns. Such bias cannot be excluded, yet telephone-based data collection is well established in survivorship research and was chosen to support accessibility and participation.
Conclusions
This study indicates that sexual health challenges are common among young Danish cancer patients aged 18–39 years across the cancer trajectory. Inadequate communication with health care professionals emerged as the most frequently reported concern. Exploratory analyses suggested that female participants reported greater sexual health burdens across multiple domains and that those undergoing active treatment experienced more pronounced difficulties, particularly in libido, partner-related insecurity, and treatment impact on sexual activity. The lack of profound differences between treatment modalities may suggest that both surgical and systemic treatments have similarly negative influence on sexual health. The findings provide a preliminary indication of potential variations in sexual health among young adults with cancer; however, they should be interpreted with appropriate caution due to the exploratory study design and the limited size of the subgroups analyzed. To our knowledge, this is the first study to investigate sexual health among young adults with cancer using EORTC QLQ-SH22. The findings in this study underscore the importance of further research and the need for age-sensitive, gender-responsive, and phase-specific interventions to support the sexual health and overall well-being of young adults with cancer during and beyond treatment.
Authors’ Contributions
Conceptualization of the research project: L.B. and M.A.; methodology and recruitment; H.P., A.S.O., L.B., and M.A.; Formal analysis: S.M.H.; writing—original draft preparation: S.M.H.; writing—review and editing: L.B., A.S.O., H.P., and M.A.; supervision: L.B. and M.A.; project administration: M.A. and L.B.; All authors have read and agreed to the published version of the article.
Footnotes
Acknowledgment
The authors are deeply grateful to all the young adults who took part in the study and generously shared their valuable insights through the questionnaire. They extend their thanks to everyone involved in recruiting participants. Special thanks to nursing students Linnea Weis Pedersen, Cecilie Hobel, and Aja Lynghus Node for their support in coordinating and recruiting for the study.
Availability of Data and Materials
The data generated and analyzed in this study are not publicly available due to the Danish data protection rules but could be available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for the study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.