
Abstract
Background:
Adolescent and young adult (AYA) patients with cancer face numerous challenges, particularly at the end-of-life. However, little is known about how the patients and their families experience end-of-life care.
Objective:
We aimed to compare the quality of end-of-life palliative care and the levels of depression and grief among bereaved families of AYAs and middle-aged patients with cancer, and to identify associated factors.
Methods:
We conducted a secondary analysis of a nationwide mortality follow-back survey based on death certificates of patients who died from cancer in 2017 and 2018. Subjects were classified into two groups AYA (aged 20–39 years) and the middle-aged (aged 40–64 years). End-of-life quality was evaluated using the Care Evaluation Scale, Good Death Inventory, and Memorial Symptom Assessment Scale. Depression and grief levels among bereaved family members were also evaluated.
Results:
We analyzed 261 and 5790 bereaved families from the AYA and middle-aged groups, respectively. While the quality of end-of-life palliative care did not differ clinically significantly between the AYA and middle-aged group, the levels of grief and depression were significantly higher in the AYA compared with the middle-aged group (Effect Size [ES] = 0.57, p < 0.0001; ES = 0.22, p = 0.001, respectively).
Conclusion:
Although end-of-life care quality was comparable between AYAs and middle-aged patients, bereaved families of AYA patients experienced significantly greater grief and depression. These findings underscore the need for tailored bereavement support for AYA families.
Introduction
The adolescent and young adult (AYA) population, defined as individuals aged 15–39 years old, faces unique challenges when diagnosed with cancer. 1 These include interruptions in education or employment, increased dependency on parents or partners, financial difficulties, loss of fertility, and long-term health concerns. 2 AYA patients often experience a gap between pediatric and adult medical care, leading to discontinuous or inadequate care. 2
Palliative care aims to improve the quality of life of patients with serious illnesses and their families by recognizing and alleviating physical, psychological, social, and spiritual sufferings. 3 AYA patients with cancer commonly experience distress in all these areas, which affects their quality of life during and after treatment; therefore, palliative care particularly important for this group.4,5 While the benefits of palliative care in improving the quality of life for patients with cancer are well-established, evidence specific to AYA populations is limited and inconsistent across studies and settings. For example, a Canadian study has shown that health care providers are often reluctant or anxious about discussing palliative care with AYA patients. 6 In the United States, although AYA patients reportedly receive more aggressive treatment, they also engage in end-of-life discussions and receive palliative care.7,8 However, one study found that fewer than 20% of AYA patients at high risk of death received inpatient palliative care services. 9 These findings highlight the need for research based on nationally representative samples.
In Japan, Mori et al. found that the achievement of a “good death” was lower for AYA patients with cancer than among middle-aged patients, based on surveys of bereaved families of patients who died in palliative care units. 10 However, it remains unclear how AYA patients who die outside of palliative care units experience end-of-life care.
Grief is a natural response to the loss of a loved one, but bereaved families are at an increased risk of mental and psychosocial health issues, including depression and complicated grief disorders. 11 A qualitative study has reported intense grief among families of AYA patients 12 ; however, evidence on depression and grief levels in this group remains scarce.
Therefore, this study aims to compare the quality of end-of-life care and levels of depression and grief in bereaved families of AYAs versus middle-aged patients with cancer using a nationwide mortality follow-back survey based on death certificates. Our secondary aim is to identify factors associated with end-of-life care quality, depression, and grief among bereaved families of AYA patients.
Methods
Participants
We conducted a secondary analysis of data from a large-scale survey of bereaved families, based on death certificates provided by the National Cancer Center, Japan. The survey details are provided elsewhere. 13 Eligible participants were bereaved family members who had served as primary caregivers for patients with cancer aged 20–65 years at the time of death, identified from death certificates dated 2017–2018. The inclusion criteria were: (1) patient age between 20 and 65 years; (2) the patient was Japanese; (3) cancer was the cause of death; and (4) the place of death was a hospital, clinic, home, or nursing facility.
The upper age limit was set to exclude older adults, as end-of-life experiences differ significantly between geriatric and nongeriatric populations, making the former unsuitable as a comparison group for AYA patients.10,14
Procedure
Self-administered questionnaires were sent to eligible bereaved family members. Respondents were asked to return the completed survey anonymously within 2 weeks. A reminder was sent to nonrespondents 1 month after the initial mailing. The study protocol was approved by the National Cancer Center Japan, Institutional Review Board (reference number 2017-346).
Measurements
Care Evaluation Scale
The short version of the Care Evaluation Scale (CES; version 2.0) comprises 10 items evaluating the structure and processes of palliative care. 15 Responses were rated on a six-point Likert scale (1 = highly disagree to 6 = highly agree). We converted the total score to a 0–100 point scale, with higher scores indicating better care.
Good death inventory
A shortened version of the good death inventory (GDI) was used to evaluate perceived quality of death. 16 This 18-domain measure evaluates concepts relevant to a good death in Japanese patients with cancer and has sufficient reliability and validity. Bereaved family members were asked to rate the patient’s quality of death during their last month on a seven-point Likert scale (1 = strongly disagree to 7 = strongly agree), with higher scores indicating better perceived quality of death.
Memorial Symptom Assessment Scale
The Memorial Symptom Assessment Scale (MSAS) was used to evaluate the physical and psychological symptoms during the patient’s final week of life. 17 This measure comprises 32 items rated on a six-point Likert scale (0 = unknown, 1 = no symptoms, 2 = a little… 6 = very strong). It has been tested for its reliability and validity in patients with cancer. For this study, 11 representative symptoms were analyzed, including pain, fatigue, and anorexia.
Patient Health Questionnaire-2
Depression among bereaved family members was assessed using the previously validated Japanese version of the Patient Health Questionnaire-2 (PHQ-2), 18 short version of the PHQ-9, 19 which is a self-administered questionnaire based on the Diagnostic and Statistical Manual of Mental Disorders version IV’s criteria for depression. Items were rated from 0 = not at all to 3 = nearly every day. In this study, the sum of the two items was calculated, with higher scores indicating higher levels of depression.
Prolonged grief
We assessed two core symptoms of grief reactions using two items from the validated Japanese version of the Prolonged Grief Disorder (PG-13) scale, 20 a self-administered questionnaire that assesses the diagnostic criteria and symptoms of persistent grief disorders. The two items included, “In the past month, how often have you felt yourself longing or yearning for the person you lost?” and, “In the past month, how often have you had intense feelings of emotional pain, sorrow, or pangs of grief related to your lost relationship?,” each rated on a scale of 1 = not at all to 5 = several times a day. The sum of the two items was calculated, with higher scores indicating greater grief.
Patient and bereaved family characteristics
Data from death certificates were used to obtain the patient’s age, sex, and place of death. Questionnaire responses provided data on cohabitation status, duration from diagnosis to death, activities of daily living, communication ability, and oral intake. In addition, the questionnaire responses provided data on bereaved family members’ age, sex, relationship to the deceased, attendance with the patient, physical health, and mental health.
Statistical analysis
We compared the quality of end-of-life care for the bereaved families of patients aged 20–39 years (defined in this study as the “AYA population”) and those aged 40–64 years (defined as the “middle-aged group”). The outcomes of quality of end-of-life care, depression, and grief were analyzed using the total scores of the CES, GDI, MSAS, PHQ, and PG. Comparisons were performed using the Wilcoxon rank-sum test. Additionally, ES was calculated based on Cohen’s criteria: 0.2–0.5 indicates a small effect, 0.5–0.8 indicates a moderate effect, and above 0.8 indicates a large effect. In addition, we conducted adjusted analysis using multiple regression models with participants’ characteristics as adjusting variables.
To investigate the factors associated with the quality of end-of-life care in the AYA population, bivariate analyses were conducted using Wilcoxon rank-sum tests for categorical variables and Spearman’s correlation coefficients for ordinal variables. Moreover, we conducted multiple regression analyses to identify independent correlations. All statistical analyses were performed using SAS software (version 9.4; SAS Institute Inc.), with two-sided p values < 0.05 considered statistically significant.
Results
Questionnaires were sent to 110,990 individuals (25,974 in 2018 and 85,016 in 2019). Owing to undeliverable addresses, 14,658 forms (13.2%) were not delivered. In total, 60,797 forms (63.1%) were returned, including refusals, with 54,167 valid responses (56.2%). After excluding those who did not meet the inclusion criteria, 261 and 5,790 bereaved family members of AYA (aged 20–39 years) and middle-aged (aged 40–64 years) patients, respectively, were included.
Participant characteristics
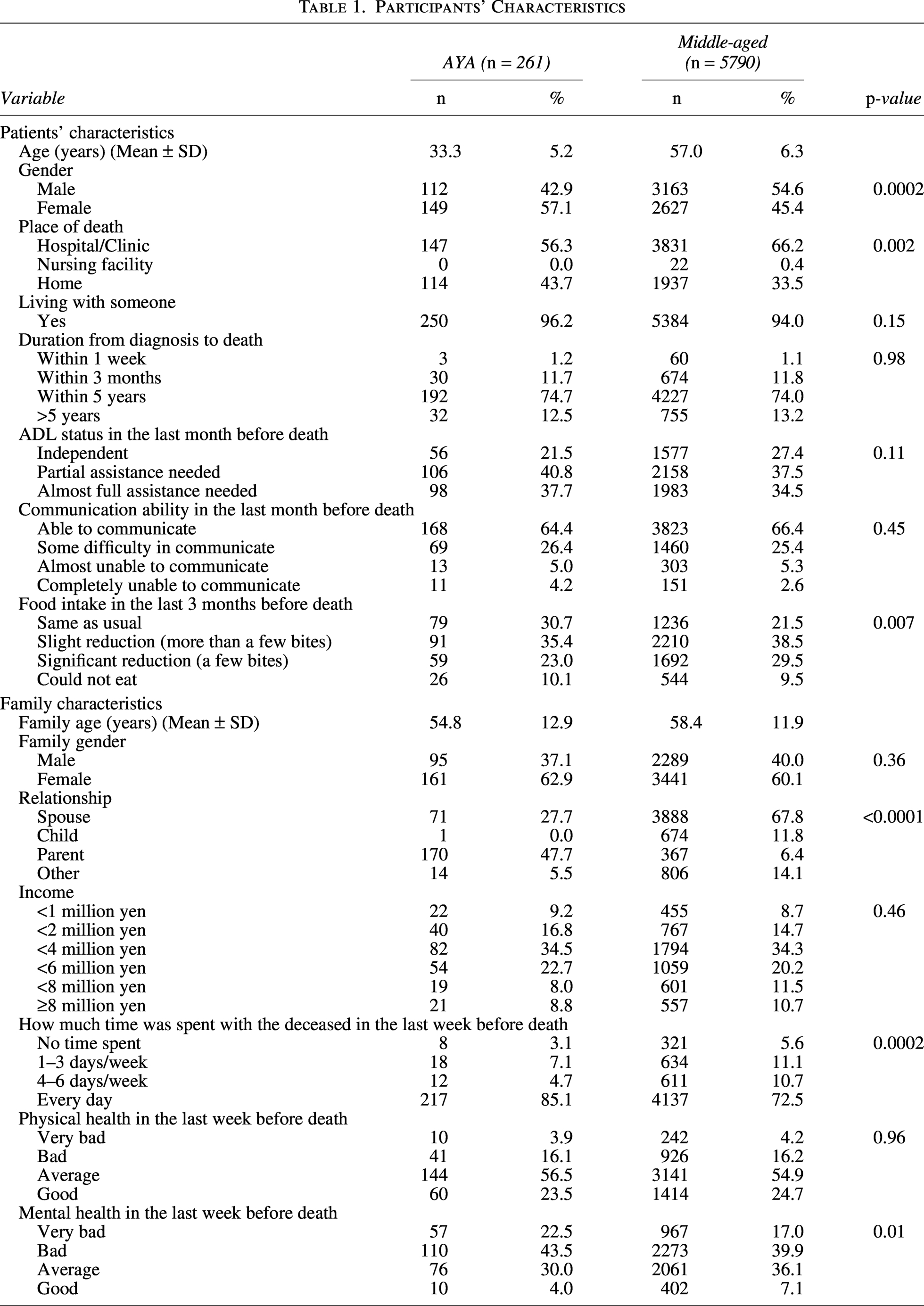
The participants’ characteristics are presented in Table 1. The average age of AYA patients was 33.3 ± 5.2, while that of middle-aged patients was 57.0 ± 6.3. AYA patients were more likely to be female (p = 0.0002), to have died at home (p = 0.002), and to have maintained oral intake near the end-of-life (p = 0.007). Among bereaved family members, the most common relationship to AYA patients was a parent, whereas for middle-aged patients it was a spouse (p < 0.0001). Bereaved families of AYA patients were more likely to have provided care at the end-of-life (p = 0.0002) and reported significantly poorer mental health (p = 0.01).
Participants’ Characteristics
Evaluation of the quality of palliative care by bereaved families of end-of-life
Comparisons of end-of-life care quality between AYA and middle-aged patients are shown in Table 2. The mean CES score (±SD) was statistically higher in the AYA group (76.3 ± 17.3) than in the middle-aged group (73.7 ± 17.0), with a marginally small ES (0.15, p = 0.01, adjusted p-value = 0.04). No statistically significant difference was observed in GDI score (ES = 0.00, p = 0.99, adjusted p = 0.94) between AYA patients (73.1 ± 17.5) and middle-aged (73.1 ± 17.9) patients, and the MSAS score was slightly higher among AYA patients (35.9 ± 10.3) compared with that among middle-aged patients (35.5 ± 9.8); this difference was statistically significant in adjusted analysis (ES = 0.08, p = 0.12, adjusted p = 0.01). The PHQ-2 score in bereaved families was significantly higher for AYA patients (4.1 ± 1.9) compared with that for middle-aged patients (3.7 ± 1.8), with a small effect size (ES = 0.22, p = 0.001, adj p = 0.02). The PG score was significantly higher in bereaved families of AYA patients (7.1 ± 2.1) compared with that in middle-aged patients (5.9 ± 2.2), with a moderate effect size (ES = 0.57, p < 0.0001).
Comparison of Quality of End-of-Life Care between AYA and Middle-Aged Patients with Cancer

Factors associated with the quality of end-of-life care, depression, and grief in the AYA group: Bivariate analysis
The factors associated with end-of-life care quality, depression, and grief among AYA patients are presented in Table 3. In the case of patients who died at home, GDI scores (p = 0.0004) as well as grief levels among bereaved relatives (p = 0.03) were significantly higher. Regarding patients who lived with their families, significantly higher grief levels were observed among bereaved families (p = 0.002). Food intake in the last 3 months before death significantly influenced MSAS scores (p = 0.01). Male family members had significantly higher MSAS scores (p = 0.01). Lower income was associated with significantly higher PHQ-2 scores (p = 0.02). Longer time spent with the deceased in the last week before death was associated with significantly higher grief scores (p = 0.0001). Poorer mental health among bereaved family members was associated with significantly higher MSAS scores (p = 0.04). Furthermore, poorer physical and mental health among bereaved family members was significantly associated with higher depression (p < 0.0001 and p < 0.0001, respectively) and grief (p = 0.02 and p = 0.01, respectively) scores.
Factors Associated with Quality of End-of-Life Care, Depression, and Grief among AYA Generation: Bivariate Analysis (N = 261)
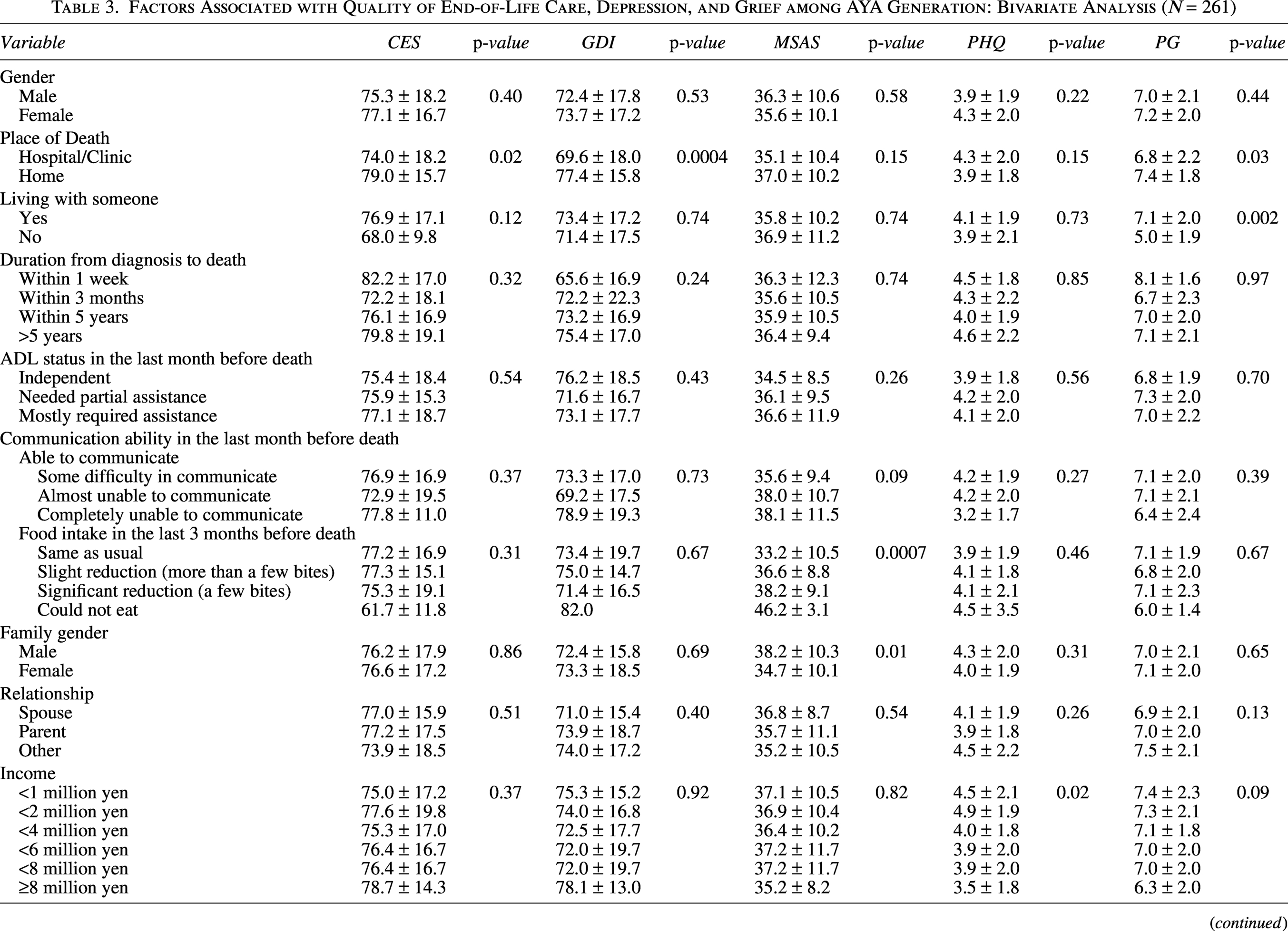
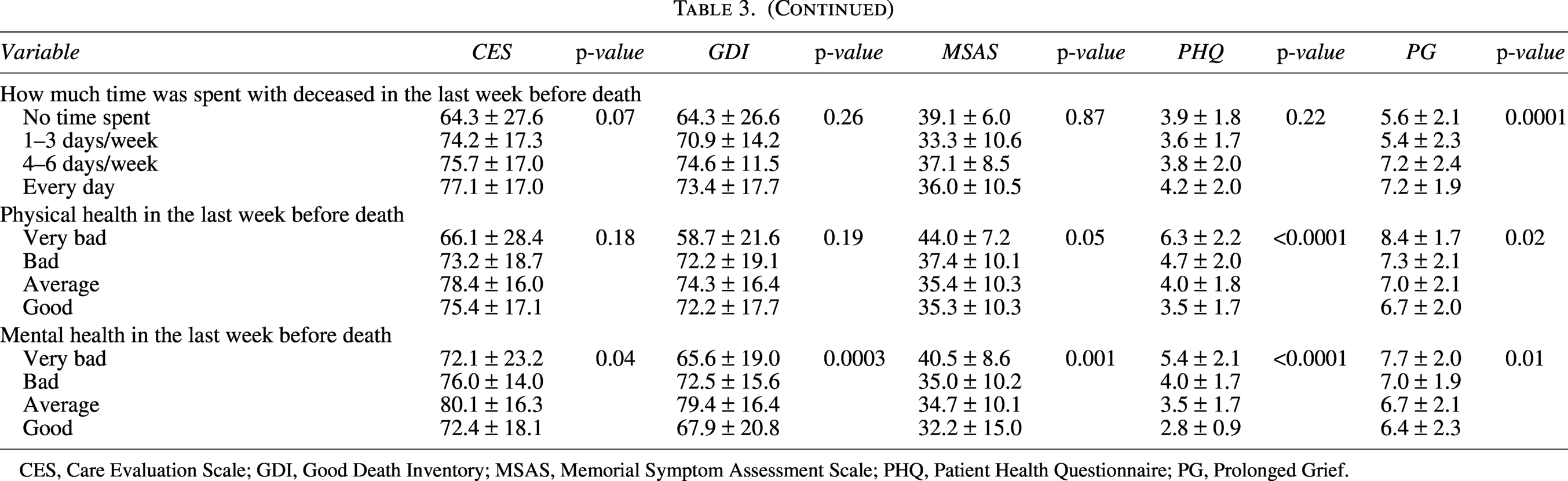
CES, Care Evaluation Scale; GDI, Good Death Inventory; MSAS, Memorial Symptom Assessment Scale; PHQ, Patient Health Questionnaire; PG, Prolonged Grief.
Factors associated with the quality of end-of-life care, depression, and grief in the AYA group: Multivariate analysis
The results of the multiple regression analysis are shown in Table 4. Patients who died at home had higher GDI scores (p = 0.001) and higher MSAS scores (p = 0.003). Regarding patients who lived with their families, significantly higher grief levels were observed among bereaved families (p = 0.002). Food intake in the last 3 months before death significantly influenced MSAS scores (p = 0.01). Poorer physical health among bereaved family members was associated with significantly higher PHQ-2 scores (p = 0.04) and higher PG scores (p = 0.04). Furthermore, poorer mental health among bereaved family members was significantly associated with lower GDI scores (p = 0.01) and PHQ-2 scores (p = 0.0003).
Factors Associated with Quality of End-of-Life Care, Depression and Grief among AYA Generation: Multivariate Analysis (N = 261)
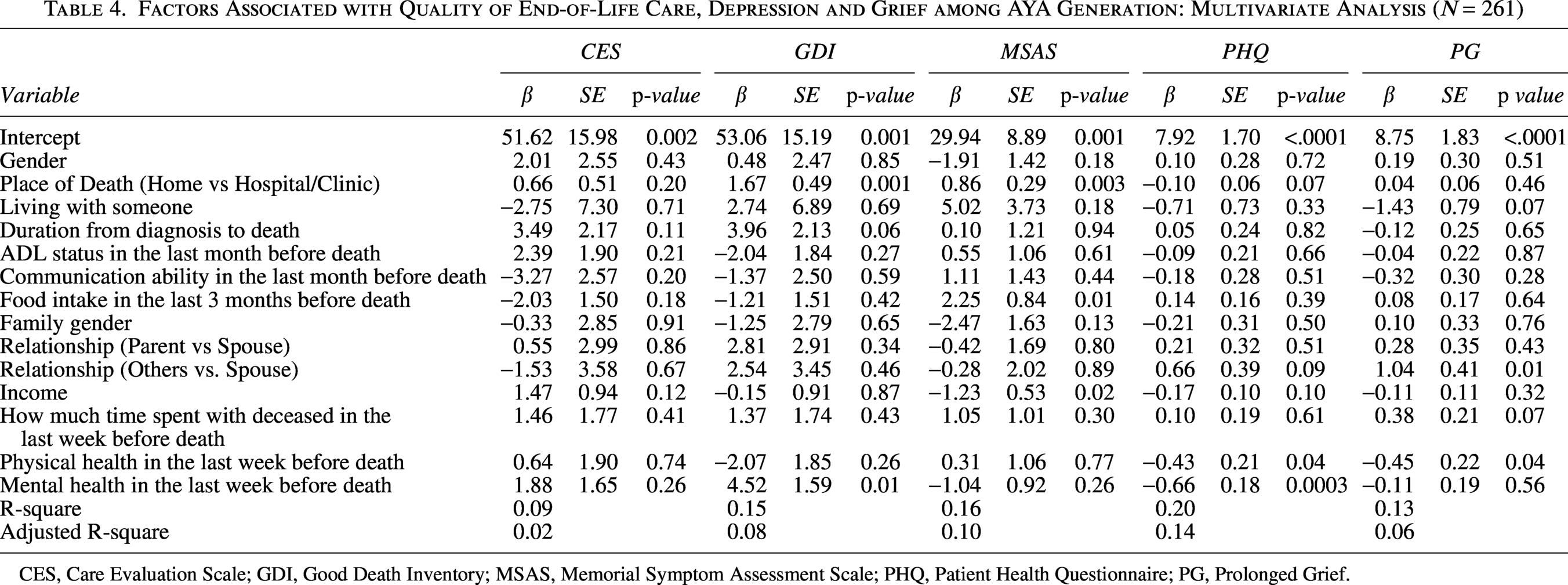
CES, Care Evaluation Scale; GDI, Good Death Inventory; MSAS, Memorial Symptom Assessment Scale; PHQ, Patient Health Questionnaire; PG, Prolonged Grief.
Discussion
This study compared the quality of end-of-life palliative care between AYA (20–39 years) and middle-aged cancer patients (40–64 years). To the best of our knowledge, this is the first study to explore the quality of end-of-life palliative care of AYA cancer patients in the representative sample.
The main finding was that grief levels in the bereaved families of AYA patients were significantly higher than those of the middle-aged group, whereas depression levels were not as high. The higher grief levels in the bereaved families of AYA patients could be attributed to the difficulty in losing a loved one at a young age. 12 Zebrack et al. emphasizes the importance of psychosocial care for AYA patients with cancer and their families, noting that this population group often face disrupted life trajectories and unfulfilled goals, potentially exacerbating grief among their families. 2 Furthermore, Choi et al. highlight that unmet needs in AYA patients with cancer can affect the grief and mental health of their bereaved families. 21 Moreover, Kingsley illustrates that religion/spirituality, maintaining a connection, and fulfilling parental roles are central elements of the grief processes in such contexts. 12
Despite the heightened grief, depression scores were not proportionally elevated for bereaved families of AYA patients. One possible reason for this is that grief is considered a normal response, and many bereaved individuals can process this grief over time, according to the Dual Process Model by Stroebe et al. 22 Since grief and depression follow different processes, high grief does not necessarily lead to high depression. Moreover, research by Bonanno has shown that grief experiences are diverse, and with a strong support network, bereaved families can effectively navigate the grief process. 23 Bereaved families of AYA patients often have greater familial and community support, which may help prevent the escalation of depression. Wright et al. have suggested that end-of-life discussions have cascading benefits for both patients and their caregivers, thereby improving their quality of life. 24 Appropriate interventions, such as end-of-life discussions, may lead to less aggressive end-of-life care and support the mental adjustment of bereaved families. 7 Moreover, personalized interventions before and after bereavement are preferable for family members.
In this study, AYA patients had significantly higher CES scores than middle-aged patients, with a small effect size. The relatively low prevalence and complex needs of AYA patients with cancer may have prompted care teams to deliver more individualized and concentrated care. 8 The higher CES scores in AYA patients might reflect the various efforts to support treatment in quality environments and preserve their quality of life.
This study further found that the achievement of a good death was not significant between AYA patients and middle-aged patients, which is inconsistent with previous research. 10 Mori’s earlier study, which focused on inpatient hospice deaths, found lower GDI scores in AYA patients. 10 However, the present study included a more representative sample, using death certificates, thus including home deaths.13,25 The increased prevalence of home deaths in this sample may explain the lack of a significant difference because home deaths are often associated with a higher likelihood of achieving a good death.13,25
The results of this study suggest that AYA patients with cancer who died at home had higher GDI scores, but also experienced greater physical symptom severity, as indicated by higher MSAS scores. Odejide et al.’s qualitative research suggests that while home care provides psychological stability, a lack of professional medical support could lead to worsening physical symptoms. 26 The burden on family caregivers—who often have to provide complex care at home without adequate information, support, or self-efficacy—highlights the need for improved home care services and psychological and social support to enhance the quality of life for AYA patients in their final days.
Overall, this study revealed that bereaved family members of AYA patients with cancer experience significantly higher grief and depression levels than those of middle-aged patients. Therefore, our results underscore the need for tailored psychological support and grief counseling that addresses the unique context of AYA. Specialized AYA palliative care teams can play a crucial role in delivering these services. 27 Further research is needed to understand the family grief of AYA patients with cancer and develop support interventions both pre and postbereavement for this vulnerable group.
Limitations
This study has several limitations. First, the response rate was not sufficiently high, suggesting the potential presence of nonresponse bias. Second, the outcome evaluations were conducted based on proxy assessments of bereaved family members, which may have been influenced by their subjective interpretation and emotional bias. Additionally, data collection occurred >6 months after patient death, introducing possible recall bias. Third, age-specific analyses were not conducted within the AYA group owing to the small number of participants in each subgroup. Fourth, the study did not include patients aged 15–19 years old, despite their inclusion in the definitions of the population in this study. Finally, as this was an exploratory study, adjustments for multiple comparisons were not conducted, and findings should be interpreted with caution.
Conclusion
This study compared the quality of end-of-life palliative care for AYAs and middle-aged patients with cancer and explored the associated factors. The results show that while the quality of end-of-life care was similar between groups, bereaved families of AYA patients reported significantly higher levels of grief, both statistically and clinically.
Authors’ Contributions
Conceptualization: Y.N. and M.M.; Methodology: Y.N. and M.M.; Investigation: Y.N.; Formal analysis: M.M.; Writing—original draft preparation: A.F. and M.M.; Writing—review and editing: Y.N., L.D., M.M., and C.S.; Supervision: C.S. All authors read and approved the final article.
Footnotes
Acknowledgments
The authors thank all the parties involved in this study for their cooperation.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This study was supported by the mortality follow-back survey project budget of the