
Abstract
Purpose:
To clarify communication preferences regarding the disclosure of bad news in adolescent and young adult (AYA) patients with hematological malignancies.
Methods:
A cross-sectional study was conducted from January 2021 to March 2022 using a five-point Likert-scale questionnaire. Participants were patients diagnosed between the ages of 15–29 years and aged <40 years at the time of the survey. Preferences regarding physician communication during the disclosure of bad news were assessed. Trend tests were performed for items showing substantial interindividual variability.
Results:
Data from 90 participants (49 male) were analyzed. Compared with adult cancer populations, AYA patients were less likely to prefer receiving bad news in the presence of family or to prioritize reassurance or emotional support. Over 90% preferred detailed and concrete information about their medical condition, including unfavorable information, and wanted physicians to listen to their distress and concerns. Seventy percent preferred receiving information about life expectancy. Participants wanted physicians to break bad news to them first while also valuing physicians’ consideration for their family members. Trend test results indicated that a preference for “Using indirect or softened wording” when delivering bad news was associated with younger age at diagnosis (<20 years), male sex, and shorter time since diagnosis (<5 years). Married participants more often preferred “Breaking bad news before it is fully confirmed.”
Conclusion:
AYA patients generally prefer clear and accurate disclosure of medical information while valuing physicians’ consideration for their family members. Many prefer factual information before or alongside emotional support, highlighting the need for flexible, individualized communication strategies.
Keywords
Introduction
Disclosing bad news regarding diagnosis, recurrence, or refractory disease is distressing for patients with cancer, altering their future and life prospects. 1 When delivering bad news to patients, a physician’s communication style can influence their subsequent stress levels.1–3 Therefore, medical professionals should consider patients’ stress and understand their communication preferences when delivering bad news. 4
The definition of adolescence and young adulthood (AYA) is generally considered to be individuals aged 15 years or older and under 40 years. This developmental stage encompasses major life transitions such as education, employment, marriage, and childbirth, and cancer treatment in AYA patients often coincides with these milestones. Compared with older adults, cancer incidence rates are relatively lower among the AYA population, 5 and hospitalization often limits opportunities for interaction with peers. Consequently, AYA patients may be particularly vulnerable to psychological distress, such as isolation and anxiety,6,7 underscoring the importance of developmentally and psychosocially sensitive communication strategies. 8
Previous studies have indicated that AYA cancer patients desire accurate and comprehensive information,7,9,10 including prognosis details,11,12 and wish to be involved in decisions regarding their treatment and care.13–15
Simultaneously, overly empathetic communication may unintentionally amplify anxiety in this population, 15 and expressions of empathy that are not well aligned with patients’ experiences may be perceived as unhelpful or difficult to accept. 8
Regarding decision-making, although guidelines recommend patient participation when developmentally appropriate,16,17 many AYAs—particularly adolescents—who are not fully independent—face challenges in making autonomous treatment decisions, and parental preferences often influence the process.18,19 These complexities, along with time constraints in clinical practice, can make it difficult for clinicians to provide fully individualized communication.20–23
Studies examining preferences regarding the disclosure of bad news have primarily focused on adult cancer patient populations.24–26 In Japanese adult cancer populations, 71 communication characteristics related to bad news disclosure have been identified and categorized into four domains: setting, information provision, communication method, and emotional support.25,27
However, research specifically examining preferences regarding bad news disclosure among AYA cancer patients remains limited. Furthermore, the extent to which these preferences vary according to psychosocial or clinical characteristics within the AYA population has not been fully explored. Given the relatively low incidence of cancer in the AYA population, 5 clinicians have limited experience and guidance regarding developmentally appropriate approaches for conveying serious information to this age group.7–9
Against this background, this study used a cross-sectional design to examine preferences regarding the disclosure of bad news among AYA cancer patients. Using the 70 communication characteristics identified by Fujimori et al. in Japanese cancer patients,25,27 the aim was to descriptively and exploratively characterize the bad news delivery approaches preferred by AYA patients and to examine associations with psychosocial and medical demographic variables.
Definitions of AYA cancer vary across studies. This study primarily included individuals diagnosed between 15 and 29 years of age, based on the definition used by the National Cancer Institute’s Surveillance, Epidemiology, and End Results program. 28 Because all respondents had experienced cancer treatment, individuals up to age 40 were also included, based on a broader definition of AYA.
In this study, “communication preferences” were conceptualized as the communication behaviors that AYA patients desire from clinicians when receiving serious or adverse information.
This study focused on patients with hematological malignancies, which account for approximately half of all cancers in the AYA population. Hematological malignancies are primarily treated with drug therapy, reducing the need to consider tumor site-specific factors or postoperative complications. Furthermore, these malignancies are often managed in different clinical settings, such as pediatric oncology and adult oncology, where communication practices may differ. This consideration also supported the selection of this study population.
Materials and Methods
Participants
Participants were approached by their treating physicians or clinical staff at participating institutions, including two general hospitals, two cancer centers, three university hospitals, and one children’s hospital, either during routine outpatient visits or inpatient care. In addition, study announcements were distributed through patient advocacy organizations (including the Tsubasa Non-Profit Organization and the Children’s Cancer Association of Japan), allowing interested individuals to voluntarily access the questionnaire.
To avoid making participation feel coercive, no reminders or follow-up contacts were conducted. No formal screening for cognitive impairment or psychological distress was conducted. No additional exclusion criteria related to comorbidities, treatment phase, or hospitalization status were applied. No formal sample size or power calculation was performed, as the study was exploratory and descriptive in nature.
Justification of survey design
This study employed a cross-sectional survey design to examine communication preferences regarding bad news disclosure among AYA patients with hematological malignancies. A questionnaire-based approach was selected to systematically assess preferences across multiple predefined communication domains, including setting, timing, information provision, manner of delivery, and involvement of family members.
Responses were primarily requested via the internet by scanning the QR code attached to the survey request form. Consent for participation and publication was confirmed through the questionnaire, and for 15-year-olds, parental consent was also confirmed according to the ethical guidelines of the Ministry of Health, Labor and Welfare of Japan. Participants completed the questionnaires either online or on paper.
This study was approved by the Institutional Review Board and Ethics Committee of the Hyogo Medical University (approved number: 3669). The study conformed to the principles of the Declaration of Helsinki. Each participating facility and patient organization cooperated in the study after receiving ethical approval from their respective facilities. Responses were processed centrally to identify duplicate submissions and confirm eligibility according to the study criteria.
Questionnaire
The questionnaire was based on a previously developed instrument consisting of 70 communication characteristics related to bad news disclosure, derived from in-depth interviews with Japanese cancer patients and physicians.25,27 The present study adopted these items without modification to explore preference patterns specifically within the AYA cancer population. The questionnaire items are provided in Supplementary Appendix. Validation and reliability testing of the instrument were not primary objectives of this study. Participants were asked to select the responses that best reflected how they would prefer to receive bad news, such as the diagnosis of cancer, recurrence, or progression of diseases (scored on a 5-point Likert scale; 1 = strongly do not prefer to 5 = strongly prefer).
The questionnaire also included questions regarding medical characteristics and demographics. Medical characteristics included age at diagnosis, years since diagnosis, diagnosis (type of hematological malignancy), recurrence, experience with stem cell transplantation, treating department, and current physical condition (performance score). Demographic characteristics included age, sex, education, occupational status, change in work and school life after cancer diagnosis, household size, marital status, having children, and caring for parents.
Questionnaires completed were returned either via a secure online platform or in sealed envelopes. Participants completed the questionnaire independently without assistance from clinicians or research staff. Missing data were handled using item-wise exclusion in descriptive analyses.
Data analysis
The primary outcomes were participants’ preference ratings for each of the 70 communication characteristics related to bad news disclosure. Secondary variables included demographic and medical characteristics examined in relation to preference variability.
The distribution of responses to all 70 questionnaire items was examined descriptively. For trend tests, the 5-point Likert scale responses were collapsed into three categories: “prefer,” “do not prefer,” and “no preference.” Communication style items for which more than 25% of respondents selected “prefer” and more than 25% selected “do not prefer” were operationally defined as having high interindividual variability in preferences.
We then validated internal consistency using Cronbach’s α coefficient, with the questionnaire comprising 70 communication characteristics. Cronbach’s α is an indicator of internal consistency, a value of 0.70 or 0.80 or more generally indicates internal consistency. 29
Trend tests (Cochran–Armitage trend test) were conducted with demographic and medical characteristics as independent variables and communication style items with high interindividual variability as dependent variables. Medical characteristics included age at diagnosis (<20 vs. ≥20 years), years since diagnosis (<5 vs. ≥5; <10 vs. ≥10), experience of recurrence, history of stem cell transplantation, and treating department (pediatrics or hematology). Demographic characteristics included sex, age at questionnaire completion (>25 years or not), marital status, and occupational status (working or not). Given the exploratory nature of the study, analyses were limited to bivariate trend tests, and multivariable modeling was not performed.
Statistical analysis
All statistical analyses were performed using Stata version 17.0 (Stata Corporation, College Station, TX, USA). All tests were two-tailed, and a p value < 0.05 was considered statistically significant.
Results
Response collection and study sample
A total of 235 patients were approached by participating physicians across eight institutions, and additional recruitment was conducted through patient organization websites, for which the total number of individuals reached could not be determined. Overall, 100 patients responded to the survey. After excluding nine respondents who were outside the eligible age range and one duplicate response identified during honorarium processing, data from 90 participants were included in the final analysis. Three participants completed paper-based questionnaires, and 87 completed the survey online. Responses were obtained for all variables except treating department (n = 88) and changes in employment after diagnosis (n = 58).
Participant characteristics
Of the 90 participants, 49 were male and 41 were female. The mean age at diagnosis was 21 ± 5 years (range, 15–29 years), and the mean age at survey completion was 27 ± 6 years (range, 16–39 years). Twenty participants were receiving active treatment at the time of the survey, 47 had undergone stem cell transplantation, and 66 had experienced disease recurrence. Most participants had a performance status score of 0–1 (Table 1).
Characteristics of the Study Participants
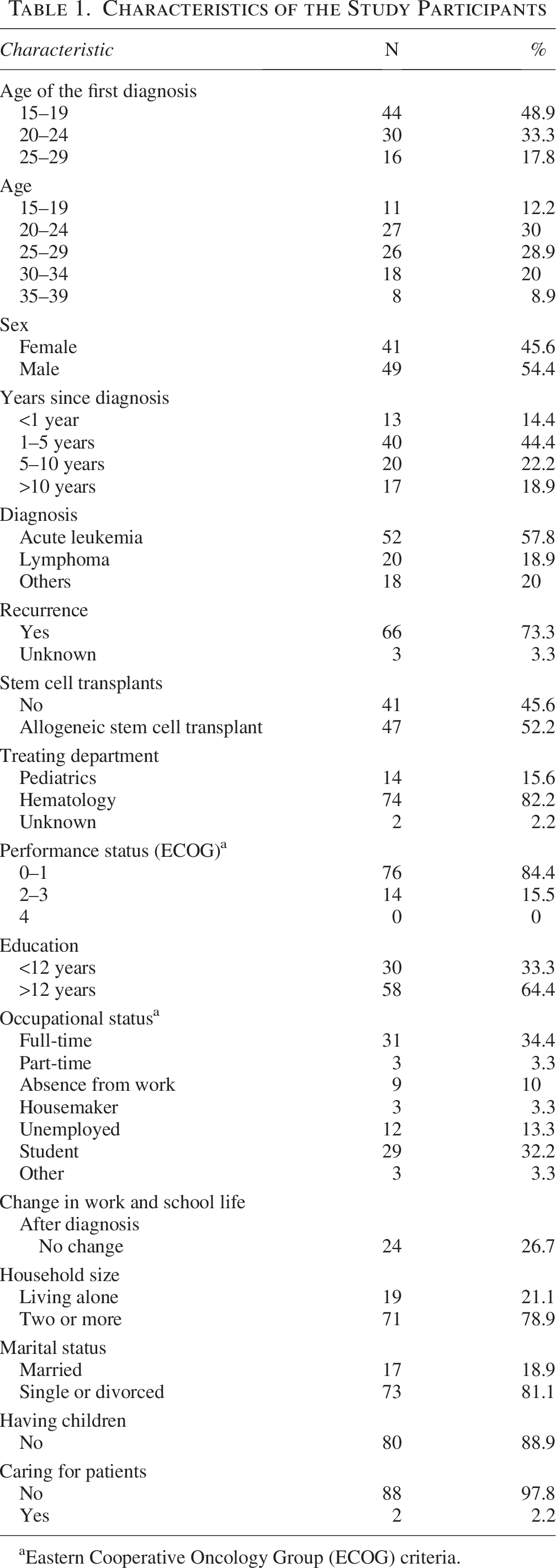
aEastern Cooperative Oncology Group (ECOG) criteria.
Preferred communication styles
Overall preferences for communication styles related to bad news disclosure are presented shown in bold in Table 2. Most participants expressed a strong preference for receiving detailed information regarding their disease, treatment options, side effects, and prognosis. Participants preferred communication conducted in a private setting with sufficient time, delivered by a trusted physician who explained information clearly, carefully, and repeatedly until the patient felt satisfied.
Descriptive Data on Patients’ Preferences for Communication Style
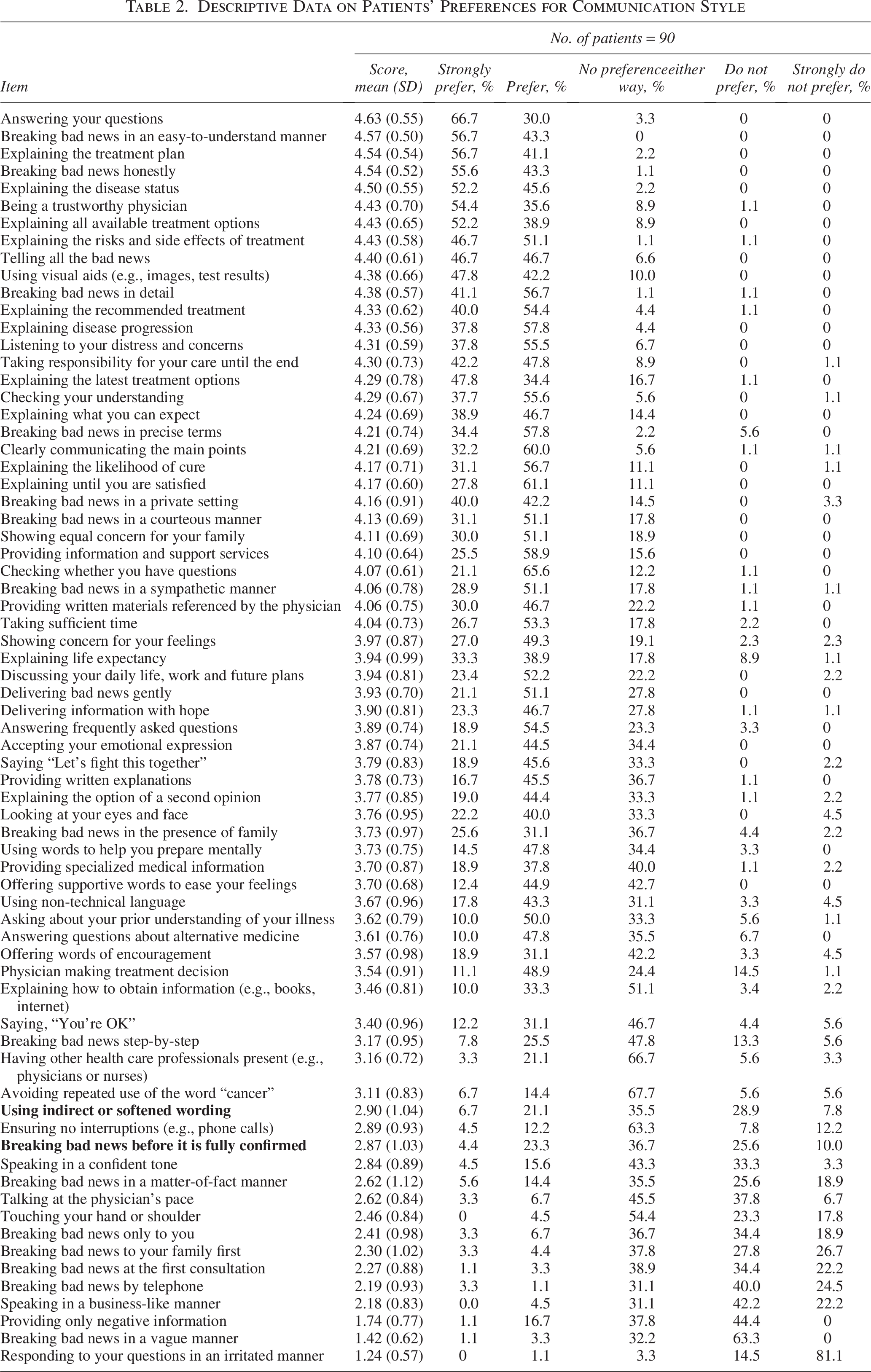
Few participants preferred several communication approaches, including “Talking at the physician’s pace,” “Touching your hand or shoulder,” “Breaking bad news only to you,” “Breaking bad news to your family first,” “Breaking bad news at the first consultation,” “Providing information at the first consultation,” “Breaking bad news by telephone,” “Speaking in a business-like manner,” “Providing only negative information,” “Breaking bad news in a vague manner,” and “Responding to your questions in an irritated manner.” Fewer than 10% of participants preferred these approaches.
Regarding family involvement, 57% of participants preferred to receive bad news in the presence of family members, and 80% desired physicians to show the same level of consideration toward their families. Only 7.7% preferred that physicians inform family members before informing the patient.
Two communication items met the predefined criteria for high interindividual variability in preferences: “ Using indirect or softened wording” when delivering bad news and “Breaking bad news before it is fully confirmed” (Table 2).
The Cronbach’s α for the 70-item questionnaire was 0.94.
Trend tests
The results of the trend tests are shown in Table 3. “Using indirect or softened wording” was significantly associated with male sex (p = 0.02), diagnosis before age 20 years (p = 0.02), and having received the diagnosis within the past 5 years (p = 0.003). “Breaking bad news before it is fully confirmed” was significantly associated with marital status, with married participants showing a higher preference (p = 0.01).
Results of Trend Test
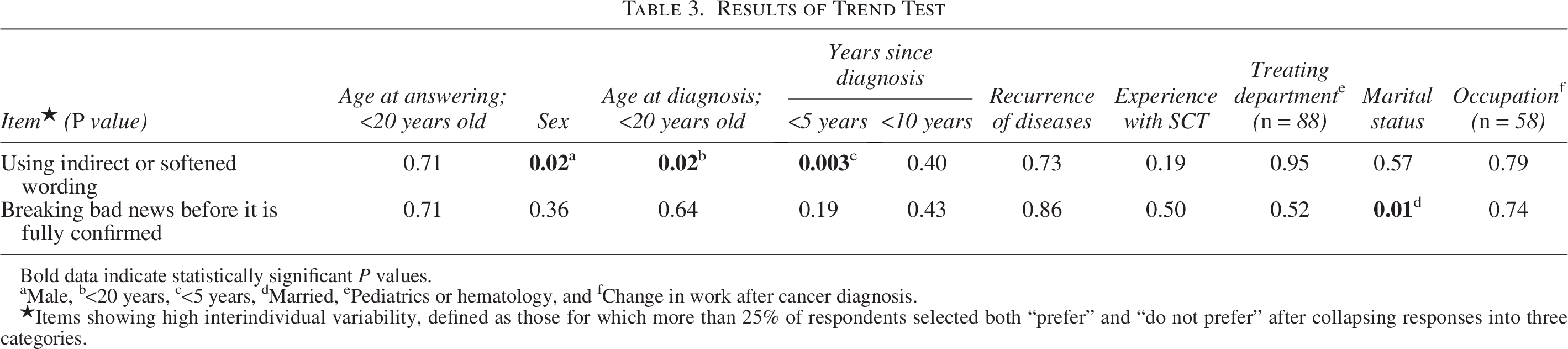
Bold data indicate statistically significant P values.
aMale, b<20 years, c<5 years, dMarried, ePediatrics or hematology, and fChange in work after cancer diagnosis.
★Items showing high interindividual variability, defined as those for which more than 25% of respondents selected both “prefer” and “do not prefer” after collapsing responses into three categories.
Discussion
This study examined preferences for disclosing bad news among AYA patients with hematological malignancies, focusing on specific communication domains. While AYA patients are known to value accurate information and involvement in decision-making,7,8 less is known about how these preferences translate into specific clinical behaviors. Our findings highlight both areas of consensus and substantial interindividual variability, particularly in comparison with the adult oncology population.25,30,31
Overall, most AYA patients preferred comprehensive and explicit disclosure, including detailed information about diagnosis, treatment, adverse effects, and prognosis. More than 70% of participants preferred receiving information about life expectancy. Although this proportion is slightly lower than that reported in some international AYA studies,7,12 the overall pattern is consistent with prior findings in both AYA and adult cancer populations. 25 These results suggest that many AYA patients prefer full disclosure rather than limited or selectively filtered information.
Participants also expressed clear preferences regarding how bad news should be delivered. Consistent with prior adult studies, AYAs preferred receiving information from a trusted physician in a private setting, with sufficient time for explanation and questions. In addition, many participants emphasized the importance of being listened to and understood.
Family involvement emerged as a nuanced and heterogeneous domain. Although family relationships play an important role in decision-making for AYA patients,18,19,22 particularly among younger individuals, more than 90% of respondents did not prefer that physicians disclose bad news to family members before informing the patient. In contrast, only about half preferred family members to be present during disclosure. These findings suggest that while AYAs value family involvement, they do not uniformly prefer family-centered communication at the time of receiving bad news. AYA patients also value consideration for their families, although some topics may be difficult to discuss in their presence. 32 Communication perceived as parent-centered may be disempowering, 22 whereas encouraging independence beyond patients’ preferences may increase distress. 33 These findings underscore the need to tailor communication to individual patient–family relationships. 34
Preferences regarding emotionally supportive language showed substantial interindividual variability. While most participants wanted their concerns to be listened to, fewer preferred reassurance-oriented expressions, such as words intended to use indirect or softened wording when delivering bad news. Compared with adult populations, AYAs appeared less likely to favor emotionally framed or potentially non–evidence-based reassurance. 25 This finding suggests a preference for authenticity and factual communication, highlighting the importance of calibrating emotional support rather than relying on standardized expressions. It has been reported that AYA patients do not prefer excessive empathy from physicians,8,15 which is consistent with our findings.
Notably, communication preferences varied according to patient characteristics.30,31,35 Preferences for certain communication styles differed by age at diagnosis, sex, time since diagnosis, and marital status. Although these findings should be interpreted cautiously given the exploratory design, they suggest that communication preferences among AYAs are not uniform and may be influenced by developmental stage and social context.
Cultural context may also influence communication preferences. In Japan, shared decision-making has historically emphasized family involvement, and clinicians may be more cautious about disclosing poor prognostic information directly to patients. 36 In addition, Japanese AYAs may be less accustomed to prioritizing autonomous decision-making compared with Western populations. 37 These contextual factors should be considered when interpreting the findings and their generalizability.
From a clinical perspective, these findings highlight the importance of avoiding assumptions about AYA patients’ preferences. While many patients prefer detailed and accurate information, preferences regarding emotional support and family involvement vary considerably. Because communication skills are modifiable, targeted training may help clinicians better respond to individual preferences and support decision-making in AYA patients.38,39
Communication skills training programs tailored to AYA populations have recently been developed, emphasizing the need to address developmental characteristics and complex psychosocial contexts specific to this age group. 40 However, evidence regarding their effectiveness remains limited, and further evaluation is needed. In contrast, communication skills training programs in adult oncology have demonstrated improvements in patient outcomes, 38 supporting the potential value of such interventions.
Taken together, these findings support the need for developing and refining communication training programs tailored to AYA patients to enhance patient-centered care in this population.
Limitations
This study has several limitations that should be considered when interpreting the findings.
First, the study employed a cross-sectional design and assessed communication preferences at a single point in time. Because patients’ physical condition, psychological status, and informational needs may change throughout the disease trajectory, the stability of communication preferences over time could not be evaluated. Therefore, the findings should be interpreted as reflecting self-reported preferences at the time of survey completion rather than stable or causal relationships.
Second, this study relied on a structured questionnaire and did not incorporate qualitative methods such as in-depth interviews. As a result, nuanced experiences, contextual influences, and ambivalence surrounding the disclosure of bad news could not be explored in depth. Future qualitative or mixed-methods studies are warranted to further elucidate these complex and context-dependent aspects of communication preferences.
Third, the sample size was relatively small and limited to Japanese AYA patients with hematological malignancies, which restricts the generalizability of the findings. Recruitment was conducted during the COVID-19 pandemic, when opportunities for in-person clinical follow-up were reduced. Participants were recruited through both clinical settings and patient advocacy organizations; however, the total number of eligible individuals approached and the response rate could not be precisely determined. Consequently, selection bias may have occurred, as participants who chose to respond may have been more motivated, engaged in their care, or particularly interested in communication-related issues.
Fourth, although hematological malignancies account for a substantial proportion of cancers among AYA patients, communication preferences observed in this study may not be directly applicable to patients with solid tumors, who may experience different treatment trajectories, symptom burdens, or decision-making contexts. In addition, because this study was conducted exclusively within a Japanese health care and cultural context, the findings may not be generalizable to populations in other countries, where norms regarding disclosure practices, family involvement, and physician–patient relationships may differ.
Fifth, the questionnaire consisted of 70 items, which may have imposed a considerable response burden and introduced the possibility of survey fatigue. Although most participants completed the questionnaire within a reasonable timeframe, variations in attention or interpretation cannot be excluded.
Finally, given the exploratory nature of the study and the modest sample size, statistical analyses were limited to descriptive and bivariate approaches.
Despite these limitations, the present study provides novel and systematically collected data regarding communication preferences among an understudied population of AYA cancer patients.
Conclusion
This study provides a systematic characterization of communication preferences regarding the disclosure of bad news among AYA patients with hematological malignancies. By translating previously described general principles into concrete communication behaviors, the findings highlight both areas of consensus and meaningful interindividual variability.
Further qualitative and longitudinal research is warranted to clarify how these preferences evolve over time.
Participating Research Facilities
Hyogo Medical University Hospital, National Cancer Institute for Cancer Control, St. Luke’s International Hospital, Osaka Women’s and Children’s Hospital, Gifu Municipal Hospital, Osaka International Cancer Institute, Mie University of Medicine, and Kyushu University Hospital.
Authors’ Contributions
All authors contributed to the study. Participants were recruited by Y.O., M.F., M.O., J.T., M.I., J.K., Y.T., K.A., Y.K., and K.I. Data analysis was performed by J.T. and supported by Y.O. The first draft of the article was written by Y.O., and all authors commented on the article. All the authors have read and approved the final article. Contribution statement based on the CRediT Taxonomy guidelines: Y.O.: Defined conceptualization (equal), methodology (equal), project administration (lead), funding acquisition (lead), investigation (lead), resources (lead), writing an original article (lead), supervision (lead), validation (lead), formal analysis (supporting), and visualization (lead). M.F.: Conceptualization (lead), methodology (lead), writing—review and editing (supporting), resources (supporting), and validation (equal). M.O.: Conceptualization (supporting), writing—review and editing (supporting), resources (supporting). J.T.: Formal analysis (lead), resources (supporting), visualization (supporting), and writing—review and editing (supporting). M.I., J.K., Y.T., K.A., and Y.K.: Resources (supporting) and writing—review and editing (supporting). Y.U.: Methodology (equal) and writing—review and editing (supporting). K.I.: Project administration (supporting), resources (supporting), and writing—review and editing (supporting).
Footnotes
Acknowledgment
The authors would like to thank the AYA patients and survivors who cooperated in the survey, Ms. Akiko Hashimoto of the nonprofit organization “Blood Information Plaza, Tsubasa,” who encouraged patient cooperation in the survey, and Mr. Kosuke Yamashita of the Children’s Cancer Association of Japan.
Data Availability Statement
Data supporting the results of this study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare no competing interests relevant to the content of this article.
Funding Information
This study was supported by the Grant-in-Aid for Scientific Research (Kiban-C; 20K10335, FY2020-
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.