
Abstract
Purpose:
Adolescents and young adults (AYAs) with cancer have unique physical, emotional, and social challenges. We aimed to identify key concerns among AYAs with cancer, evaluate pathways for connecting patients with resources, and inform the development of an AYA oncology program.
Methods:
This study was conducted at Mayo Clinic in Arizona and included English-speaking patients aged 18–39 years with recently diagnosed cancer. Participants completed a modified Needs Assessment Service Bridge questionnaire, which assessed patient-perceived needs with 39 items spanning 7 domains. An AYA nurse navigator discussed each participant’s results with them and connected them to the desired resources.
Results:
Of 52 eligible patients, 32 (62%) completed the questionnaire. Among them, 30 (94%) reported unmet needs in at least 1 domain and 19 (59%) reported unmet needs in 5 or more domains. The domains with the most frequently reported needs were health behaviors and wellness (81%), emotional health (72%), finances and everyday needs (59%), and work- and education-related assistance (56%). Younger participants reported more needs related to school life and scholarships/loans than did older participants. No significant differences were observed between the responses of men and women. Of 133 total needs identified by all participants, 93 (70%) were addressed by connecting patients to relevant resources.
Conclusion:
Systematic assessment of AYA needs and targeted connection to resources are essential for individualized and developmentally appropriate care. The current study identified key service gaps at our institution and will guide the continued evolution of our comprehensive AYA oncology program.
Keywords
Introduction
During the past 20 years, the global incidence of cancer in adolescents and young adults (AYAs) has increased, and efforts are being made to understand how the needs of this population differ from those of children and older adults with cancer.1,2 The complexity of coping with a life-threatening illness may be intensified for AYAs because they are also navigating crucial milestones such as establishing independence, pursuing education or career goals, exploring personal identity, and forming meaningful relationships. In the months after a cancer diagnosis, these stressors often lead to a wide range of unmet emotional, social, physical, and practical needs that may affect quality of life and clinical outcomes. Moreover, the developmental insecurity and instability caused by cancer exacerbate psychosocial distress, highlighting the need for targeted support for AYAs. 3
Despite growing awareness of the challenges encountered by AYAs with cancer, AYA-specific supportive care lacks consistent implementation among institutions and lacks systematic approaches to identify and address the needs of AYA patients in real time. To close this gap, our AYA oncology program implemented a structured, self-reported needs questionnaire, which was modified from the Needs Assessment Service Bridge (NA-SB). The NA-SB is a validated, age-specific questionnaire that assesses patient-perceived needs. 4 With the current study, we aimed to describe our experience with initial implementation of the questionnaire, to describe the most commonly reported concerns among AYAs with cancer, to evaluate the effectiveness of existing care-resource pathways, and to discuss how these insights could guide program development.
Methods
Participants and design
Eligible participants included English-speaking patients aged 18–39 years with a diagnosis of solid organ or hematologic malignancy, who had an initial consultation with an oncologist between March 1, and August 31, 2024, and who were prescribed cancer treatment (including radiotherapy, surgery, chemotherapy, immunotherapy, bone marrow transplant, or cellular therapy). To identify eligible patients, we ran a weekly electronic health record (EHR) report that filtered patients by age, visit type, and diagnosis. We reviewed the EHR of each patient identified by the report to verify they would be receiving cancer treatment at Mayo Clinic, had access to the patient portal, and spoke English.
Within 10 days of each patient’s initial consultation with an oncologist, the AYA oncology nurse navigator (AYAONN) called the patient to introduce the AYA oncology program and then sent them the modified NA-SB questionnaire via the EHR patient portal. The AYAONN role existed before this study was initiated and was staffed by a single navigator for the duration of the project. After the patient had completed the NA-SB, the AYAONN abstracted NA-SB results and demographic characteristics from the EHR, then called the patient again to discuss their responses and connect them with relevant resources on the basis of their identified needs. The following process-related outcomes were recorded: the proportion of patients who were connected to the needed resources, the number of days it took for patients to be connected to the needed resources, and the reason why a connection was not made.
Measures
The NA-SB is a patient-reported outcome measure for evaluating the physical, psychosocial, and practical needs of AYAs. 4 With permission from the original developer, we modified the questionnaire to retain six of its original domains (emotional health, sexual and reproductive health, health behaviors and wellness, work and education, peer support and programming, and finances and everyday needs) and to add one new domain (research interest) (Supplementary Data). The modified questionnaire included a total of 39 items: 15 about emotional health, 5 about sexual and reproductive health, 7 about health behaviors and wellness, 2 about work and education, 3 about peer support and programming, 6 about finances and everyday needs, and 1 about research interest. To reduce questionnaire burden, each item was converted into multiple-choice format that allowed patients to select specific needs within each domain.
We used two methods to evaluate patient experience with the NA-SB, a postassessment survey and a patient experience survey, which were both developed for the study. First, the AYA patient advisory council (comprising 12 current and former patients) completed the NA-SB and the postassessment survey. They rated the NA-SB as positive, negative, or neutral; offered open-ended feedback; and answered a question about frequency (“Currently, this questionnaire is being piloted one time at intake. In your opinion, how frequently do you feel this questionnaire should be sent to AYA patients?”). Second, study participants were given a brief patient-experience survey after they completed the NA-SB. The survey included three questions: (1) You recently completed a questionnaire about your needs as a young adult with cancer, do you recall this? (2) Was completing this form a burden? (3) Do you feel that your care was improved by completing this form?
Statistical analysis
Demographic and clinical characteristics of the study participants, such as age, race, sex, and cancer type, were summarized and compared between respondents and nonrespondents by using the Fisher exact test (for categorical variables) and the Wilcoxon rank sum test (for continuous variables). The p-values <0.05 were considered statistically significant, and all tests were 2-tailed. Domain scores were calculated as the sum of the number of needs indicated by the patient in each domain divided by the total number of possible needs in that domain. Pairwise correlations between domain scores were calculated by using Spearman rank correlation. Outcomes were summarized by domain. The proportions of respondents who indicated each specific need were compared according to age group (older vs. younger than the median age of 31 years) and according to sex by using the Fisher exact test. Analyses were performed with SAS version 9.4 (SAS Institute Inc) and R version 4.2.2. 5
Use of AI during article preparation
Portions of this article’s text were refined using an artificial intelligence language model (ChatGPT, GPT-5, OpenAI; October 2024). The tool was used to assist with grammar, clarity, and formatting improvements only. No content, data interpretation, conclusions, or analytic results were generated by the model. All factual and scientific content was reviewed and verified by the authors. Potential limitations include the risk of stylistic bias or inadvertent loss of nuance during rephrasing; these were mitigated through manual review and revision by the coauthors.
Results
We sent the NA-SB questionnaire to 52 patients; of these, 32 (62%) responded. The mean (SD) age of all patients was 30 (6.2) years, and the majority (56%) were women. Demographic and clinical characteristics were compared between those who completed the assessment and those who did not (Table 1); no significant differences were observed between the two groups (all p > 0.08). The mean (SD) time between completing the NA-SB and discussing the results with the AYAONN was 9.9 (5.5) days, and the mean (SD) time between discussing the results and being connected to resources was 6.1 (9.8) days.
Demographic and Clinical Characteristics of Eligible Patientsa
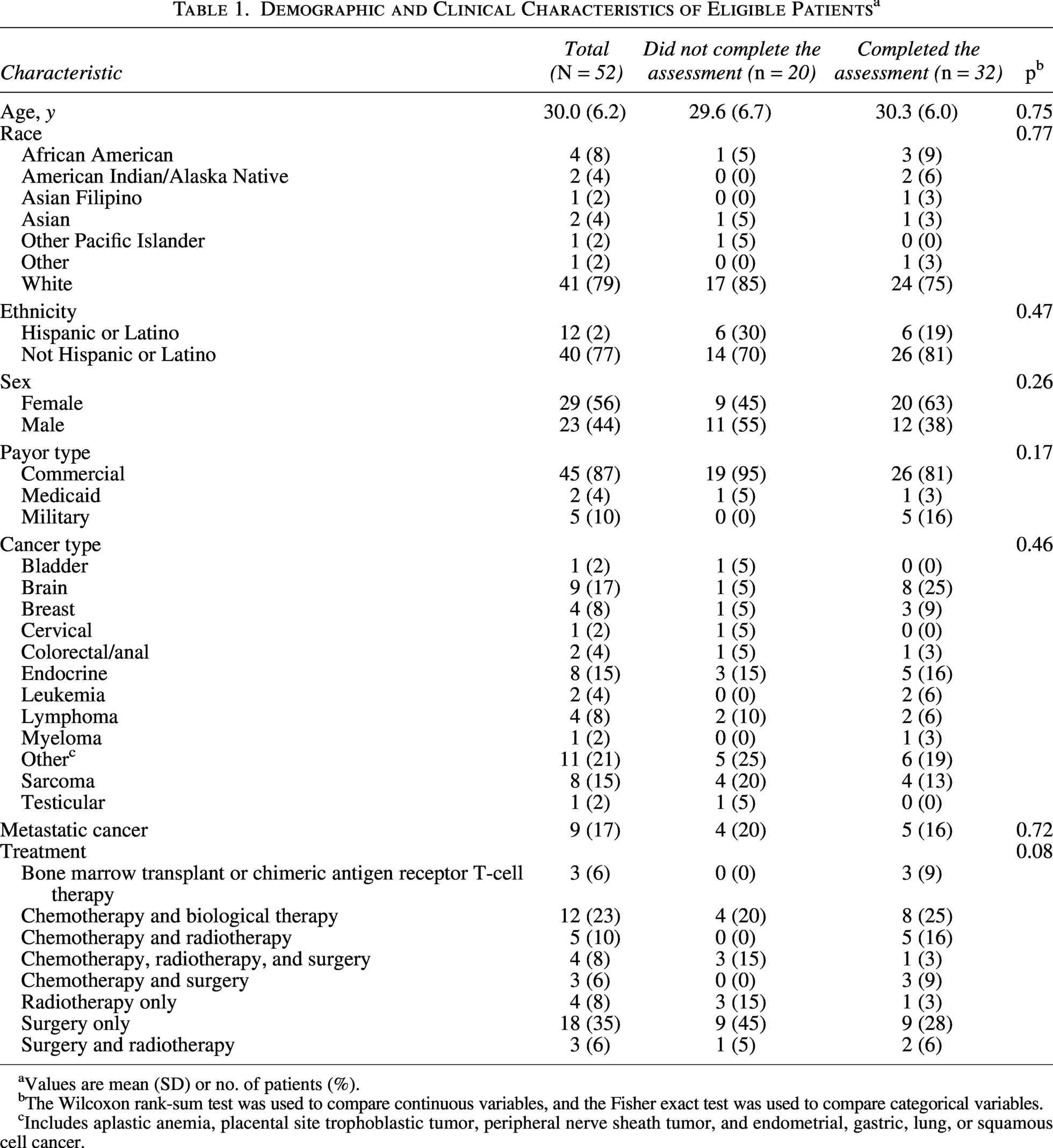
Values are mean (SD) or no. of patients (%).
The Wilcoxon rank-sum test was used to compare continuous variables, and the Fisher exact test was used to compare categorical variables.
Includes aplastic anemia, placental site trophoblastic tumor, peripheral nerve sheath tumor, and endometrial, gastric, lung, or squamous cell cancer.
Among the 32 patients who completed the NA-SB, 30 (94%) reported needs in at least 1 domain, and 19 (59%) reported needs in 5 or more domains (Table 2). Among all patients, 133 total needs were reported, 93 (70%) of which resulted in successful connection with resources. The domains with the most frequently reported needs were health behaviors and wellness (81%), emotional health (72%), finances and everyday needs (59%), and work and education (56%) (Fig. 1). Domains with less frequently reported needs included peer support and programming (50%), sexual and reproductive health (50%), and research interest (38%). Among the 40 needs that did not result in successful connection with resources, 17 (43%) had already been addressed through existing care pathways, 12 (30%) were due to the absence of an AYA-specific clinical trial-matching pathway, 4 (10%) were not clinically indicated (e.g., fertility counseling was requested by a patient who had not undergone gonadotoxic treatment), 4 (10%) were reported by patients who declined to participate, and 3 (8%) were reported by patients who were unreachable by telephone.

Radar plot of responses to individual items of the NA-SB Questionnaire. Colors indicate different domains. Numbers represent the number of patients who reported each need. NA-SB, needs assessment service bridge.
Domain-Level Results of the Needs Assessment Service Bridge Questionnaire
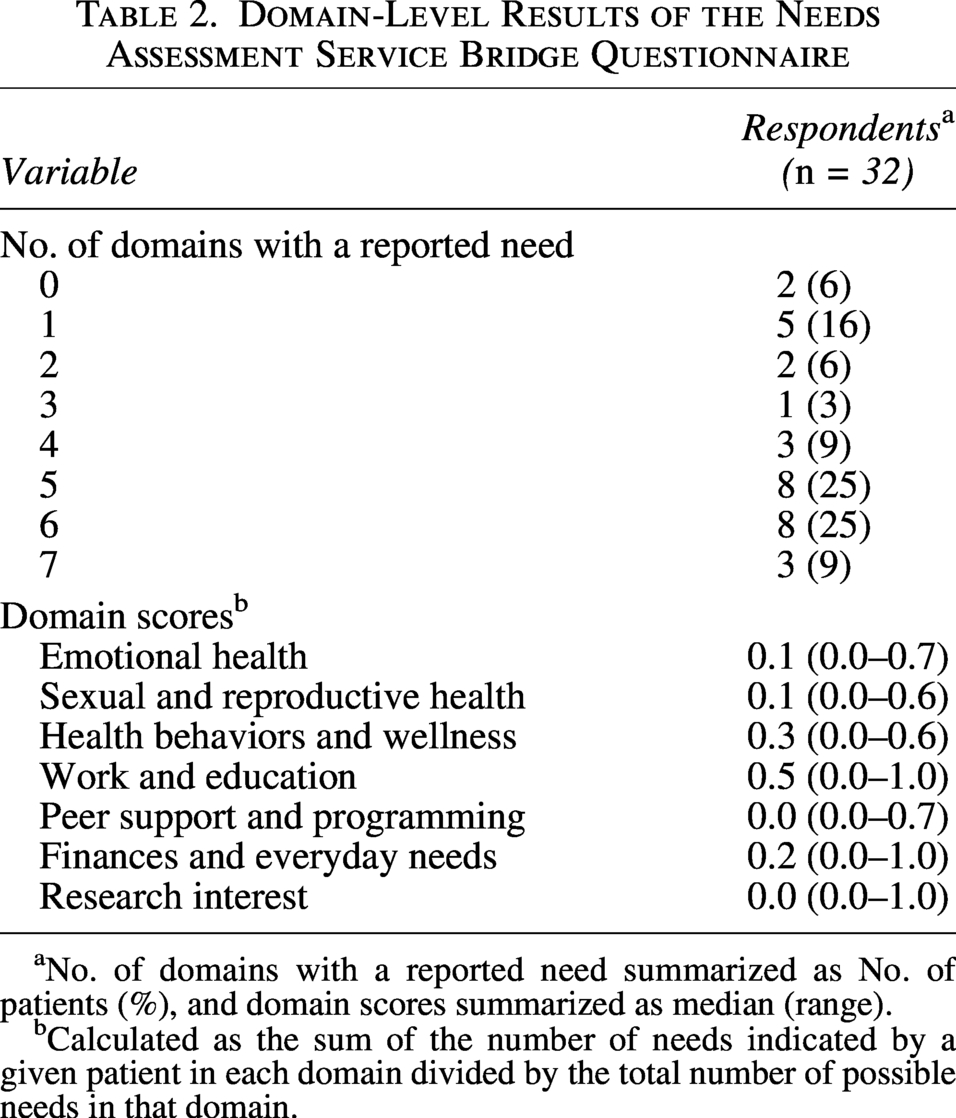
No. of domains with a reported need summarized as No. of patients (%), and domain scores summarized as median (range).
Calculated as the sum of the number of needs indicated by a given patient in each domain divided by the total number of possible needs in that domain.
Patient-reported needs were stratified by age (Supplementary Table S1) and sex (Supplementary Table S2). Younger participants reported needs related to school life more frequently than did older participants, but this study was underpowered to evaluate statistical significance.
Correlation analysis showed that finances and everyday needs correlated significantly with work and education needs (ρ = 0.66, p < 0.001) (Fig. 2). Finances and everyday needs also correlated significantly with research interest (ρ = 0.45, p = 0.01).

Correlations among domain scores. Spearman rank correlation coefficients between each pair of domains in the needs assessment service bridge questionnaire.
Evaluations of patient experience with the NA-SB yielded positive responses on both the postassessment survey and the patient experience survey. All 12 members of the patient advisory council (100%) rated the NA-SB positively and recommended that it be administered at least annually. Open-ended feedback from the council members indicated that early access to the NA-SB during their own treatment may have facilitated earlier identification of needs and enabled more personalized support. Of the 32 study participants who completed the NA-SB, 16 responded to the patient experience survey, 10 of whom recalled completing the NA-SB. Of those who recalled completing the NA-SB, 8 (80%) indicated that the NA-SB improved their overall care experience, and 0 (0%) indicated that the NA-SB was burdensome.
Discussion
The results of this study identified several of the most pressing needs of AYAs with cancer at our institution. The needs that were identified, including support for exercise, nutrition, anxiety, health insurance, and work-life balance, were consistent with those reported in other AYA-focused studies.6,7 Nearly all patients indicated at least 1 unmet need, and most indicated multiple needs spanning several domains. These findings will help bridge existing gaps in age-appropriate interventions and enhance our understanding of the lived experience of AYAs with cancer so that meaningful support and care can be provided. This work underscores the importance of dynamic, needs-informed care for building comprehensive AYA oncology programs.
Age and sex were not significant predictors of overall need, although school-related challenges and need for financial aid (i.e., scholarships or loans) were reported more by younger participants (≤31 years) than by older ones. These findings underscore the heterogeneity of AYA experiences and the need for caution against making assumptions based solely on age or sex. 8 Needs are complex; in addition to being influenced by age and sex, they may also be affected by psychosocial history, developmental stage, and life experience. For younger AYAs, concerns about school and financial insecurity highlight the value of early collaboration with social workers, vocational services, and financial assistance teams. 9
The strong correlation between financial/everyday needs and work/education needs suggests that these aspects of life are interconnected for AYA patients; disruption in one area most likely compounds challenges in the other. AYAs have greater financial strain than older adults and have higher health care costs and lower ability to work than their peers without cancer.10,11 A patient whose education or employment has been disrupted by cancer and treatment may also have loss of income (due to unpaid time off or employment termination), insurance instability or loss, difficulty maintaining living expenses, delayed financial independence, and interrupted educational pursuits. A multidisciplinary, team-based approach that integrates financial and vocational support may improve overall quality of life for AYAs with cancer and help them navigate life after cancer with greater stability and independence. 12
Recognizing the importance of clinical research for AYA outcomes, we modified the NA-SB to include an additional domain about research interest. Despite the lack of AYA-specific infrastructure for matching AYAs with relevant clinical trials at our institution, 38% of participants expressed a desire to learn about research opportunities. This level of interest is notable given the historically low participation rates of AYA patients in cancer-related clinical trials; AYAs represent only 8.4% of National Cancer Institute–sponsored trial enrollments. 13 Knowing that this level of interest exists, our institution may add an AYA-specific clinical research associate role; such roles have been shown to enhance research-related engagement. 9
The NA-SB results highlighted service gaps and enabled our institution to proactively identify patient needs and to connect patients with real-time, individualized support. In our efforts to connect patients with exercise-related support, we became aware that our institution offered no virtual or in-person exercise programs that were tailored to AYAs. This finding prompted us to develop an AYA-specific exercise initiative. In contrast, patients requesting nutritional support services were offered various options, including a self-guided nutritional e-learning module, a consultation with an oncology dietician, printed educational material, or a free virtual cooking class.
Financial concerns were a particularly important reported need that required real-time connection to an appropriate resource. When reviewing each patient’s NA-SB results, the AYAONN conducted a detailed assessment to determine the specific nature of financial concern. Patients who reported challenges with medical billing were referred to the financial concierge team, whereas those needing help with day-to-day expenses—such as rent, utilities, or other nonmedical costs—were directed to the AYA patient navigator, a nonclinical professional whose job is to connect AYAs with practical, financial, and logistic resources. Each patient received individualized counseling and resource referrals, and not all identified needs resulted in the same resource pathway; interventions were highly personalized.
Higher levels of clinician engagement have been associated with higher response rates to patient-reported outcome measures. 14 In the current study, the AYAONN introduced the NA-SB, explained its purpose, and engaged the patient in reviewing results and choosing the types of resources they wanted to be connected to. This collaborative model most likely enhanced the perceived value of the NA-SB and contributed to the study’s high rates of completion and satisfaction.
The NA-SB is useful for retrospective population-level analysis. When an AYA-focused, exercise-related clinical trial opened later in the study period, existing responses were used to identify interested patients, who were then contacted about participation in the trial. This highlights the potential of the NA-SB to not only improve patient well-being but also to identify and engage patients in relevant clinical research.
Implementation of the NA-SB was instrumental for assessing institutional readiness and uncovering service gaps, which are critical steps in AYA oncology program development. Results of the NA-SB offered insights into patient needs, service and resource availability, care gaps, and workflow challenges. The results also informed key decisions of our AYA oncology program, including the expansion of resource pathways and investments in peer support and clinical trial navigation. In the current study, we combined data about patient-reported needs with feedback from the patient advisory council to ensure that program development was aligned with patient priorities. This approach offers a strong, patient-centered strategy for guiding program development. 15
Use of an AYA-specific transdisciplinary team was previously reported to be an effective model of care 9 ; however, many health care systems are unable to support full-time dedicated staff. During NA-SB implementation at our institution, the AYA-dedicated team consisted of a medical director, social worker, patient navigator, and AYAONN (initially with limited time). The brief turnaround time from assessment to resource connection showed that NA-SB implementation was feasible and scalable, even with time constraints on the AYAONN. Given the success of this study, our AYA oncology program increased the AYAONN’s time and distributed NA-SB duties among other members of the AYA team.
The results of this study emphasize the importance of dynamic program evolution. Insights from the NA-SB prompted enhancement and advocacy across the full spectrum of AYA care, including targeted support for fertility services, expanded access to financial counseling tailored to young adults, creation of a structured pathway to psychosocial assessments, and improvement of peer support mechanisms. By evaluating resource pathways, even for less commonly reported needs, our program can now provide more comprehensive, tailored, and equitable support for all AYAs. As the program expands, the lessons learned from this NA-SB pilot study will continue to inform how we prioritize funding, training, and partnerships to ensure that all AYA patients receive timely, appropriate, and developmentally attuned support.
Limitations
This study has several limitations. The small sample size limits the generalizability of findings to the broader population of AYAs with cancer. The postassessment findings in particular should be interpreted with caution because survey responses were obtained from an even smaller subset of participants. The mean participant age was 30 years, suggesting that results may have been skewed toward the experiences of older AYAs. Racial and ethnic diversity was limited, with most participants self-identifying as White or not Hispanic or Latino. Although the questionnaire was only available in English, no non-English speakers were otherwise eligible during the study period, so this survey limitation did not result in exclusion of any additional patients. Additionally, most participants had commercial insurance, suggesting that socioeconomic diversity may not be fully represented. Finally, the study did not stratify needs on the basis of cancer type (hematologic vs. solid tumors) or treatment type (e.g., chemotherapy alone vs. multimodal therapy); these factors may influence the relevance of specific needs or resource gaps.
Future initiatives should focus on engaging more diverse AYA populations across racial, ethnic, and socioeconomic backgrounds, as well as across diagnoses and treatment types. Longitudinal assessments are also needed to evaluate how needs evolve over time and to better understand the long-term effects of individualized, developmentally appropriate interventions.
Conclusion
Together, these findings underscore the diverse and evolving needs of AYAs with cancer, identify key areas of unmet needs, and inform the future development and strategic prioritization of AYA-specific resources and services. At our institution, implementing a self-reported, age-specific needs assessment has become the standard of care for AYAs with cancer. This approach not only guides AYA-specific service development but also ensures that the program remains responsive and adaptable to the unique experiences and changing priorities of AYAs throughout their cancer journey.
Authors’ Contributions
E.M.C.: Conceptualization, funding acquisition, investigation, visualization, writing—original draft. M.A.G.: Writing—review and editing. W.L.A.: Data curation, methodology, writing—original draft. J.L.R.W.: Supervision, writing—review and editing. E.R.T.: Formal analysis, writing—original draft. A.R.: Supervision, Writing—review and editing.
Footnotes
Acknowledgments
The authors thank Emily R. Haines, PhD, for granting permission to use and modify the original Needs Assessment Service Bridge. The Scientific Publications staff at Mayo Clinic provided editorial consultation, proofreading, and administrative and clerical support.
Data Availability
The datasets generated and/or analyzed during this study are available from Mayo Clinic, but restrictions are mandated per institutional policies. Data may be available from the authors upon reasonable request and with documented permission from Mayo Clinic.
Ethics Statement
The Mayo Clinic Institutional Review Board deemed this study exempt from review because it is a quality improvement project.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This effort was supported by funding from the
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.