
Abstract
This study considers when, whether, and how spouses encourage professional mental health care by analyzing qualitative data from 90 in-depth interviews with gay, lesbian, and heterosexual spouses. Findings show that a majority of spouses are engaged in promoting each other’s mental health care but that the strategies used to promote care vary by gender and the gender composition of the couple. The majority of gay men and lesbian women promote care by framing mental health problems as largely biochemical, fixable only with professional care or medicine, and work to destigmatize this care. Lesbian women uniquely emphasize the influence of a spouse’s symptoms on marital quality as a reason to pursue care. Some heterosexual women and men also report seeing their spouse’s mental health care as something for them to deal with on their own and thus do not encourage care. This study has important implications for researchers looking to understand why some individuals seek mental health care and others do not and provides policymakers insight into mental health interventions via spouses.
The married experience a mental health advantage relative to the unmarried, including lower levels of depression and anxiety (Mernitz and Dush 2016; Van Hedel et al. 2018). This is in part because spouses provide emotional support to each other during times of stress (Holt-Lunstad, Birmingham, and Jones 2008), marriage provides access to health insurance and other resources that promote access to affordable mental health care (Walker et al. 2015), and those who are mentally healthier are more likely to get and stayed married (Tumin and Zheng 2018). Although emotional support, financial resources, and selection processes are key to the marital mental health advantage, we do not know whether and, if so, how spouses encourage or pressure one another to seek professional mental health care. For example, spouses may encourage one another to seek a therapist for counseling due to symptoms of anxiety or a primary care physician for medication due to depressive symptoms. Such encouragement may play a critical role in addressing mental health concerns among the married.
Additionally, how spouses encourage mental health care likely varies for men and women and by the gender composition of a couple (e.g., whether the couple is composed of two men, two women, or a man and a woman; Umberson, Thomeer, and Lodge 2015). Women typically take on the role of “health expert” and “emotion expert” within heterosexual marriage (Hochschild 1979; Risman and Johnson-Sumerford 1998), and thus women married to men may be especially likely to encourage their spouse to obtain mental health care (Reczek et al. 2018). In turn, research shows that heterosexual men often ignore their own and their wives’ health problems in general and mental health problems in particular (Addis and Mahalik 2003; Wendt and Shafer 2016), partially due to the stigmatization of professional mental health care. Stigmatization may be especially consequential for heterosexual men who are more likely to equate mental health care with weakness (Wendt and Shafer 2016). These gendered patterns may further depend on whether men and women are in a gay, lesbian, or heterosexual marriage (Scott, Pringle, and Lumsdaine 2004). For example, gay men are more highly attuned to their own health relative to heterosexual men (Tjepkema 2008), and gay and lesbian relationships are characterized by more equal divisions of labor, including around health problems, than heterosexual relationships (Reczek and Umberson 2012).
To examine how spouses influence each other’s use of professional mental health care, we analyze qualitative data from in-depth interviews with 90 midlife gay-, lesbian-, and heterosexual-identified spouses in 45 couples. Importantly, our sample of gay, lesbian, and heterosexual spouses makes it possible to consider variation in the dynamics around mental health care encouragement by gender composition of the couple. We ask: What are the processes through which spouses do (or do not) encourage one another to seek professional mental health care, and how do these processes differ by gender composition of couple?
Background
Mental Health in Marriage
Spouses are typically the first line of defense during the development, diagnosis, and progression of physical illness, wherein spouses notice and identify health symptoms, help each other decide whether physical symptoms warrant professional intervention, and facilitate formal and informal care in response (Chen, Waite, and Lauderdale 2015; Kiecolt-Glazer and Newton 2001; Reczek et al. 2018; Umberson et al. 2016)—a form of spousal interaction termed health care work (Reczek et al. 2018). While previous work has largely focused on how spouses monitor and promote medical engagement in response to physical health conditions, similar spousal interventions likely also occur for mental health symptoms. For example, spouses are highly attuned to each other’s mental health and attempt to alleviate mental health concerns within the home, such as by working together to reduce depressive symptoms and relationship strain (Sharabi, Delaney, and Knobloch 2016; Thomeer, Umberson, and Pudrovska 2013).
Missing are accounts of how spouses help one another determine whether mental health symptoms require professional care and whether and how spouses encourage one another to seek care. Mental health care provided by therapists, psychotherapists, psychiatrists, psychologists, counselors, and other medical professionals, along with prescriptions for medications to reduce mental health symptoms, have increased substantially over the past several decades (Mossakowski, Kaplan, and Hill 2011; Smith 2014). This has occurred partly due to the shift toward viewing mental health problems as having a treatable biochemical origin (Dincin 2001), increases in anxiety and depression in the general population (Centers for Disease Control and Prevention 2016), and decreases in the stigmatization of receiving mental health care (Mossakowski et al. 2011). The decision to seek mental health care is typically viewed as an individual decision (Moloney 2017), yet among the married, decisions of if and when to seek mental health care likely occur at the couple level, with spouses playing a key role in how individuals view and participate in mental health care.
Research on physical health shows that spouses co-construct physical illness to assess whether a problem is a minor condition that can be dealt with informally or whether it is a serious condition that should be managed within formal medicine (Reczek et al. 2018). Once the physical condition has been understood as posing a health risk, spouses facilitate care by encouraging or directly scheduling appointments for each other, driving one another to appointments, and following up to ensure medical compliance (Taylor and Quesnel-Vallée 2016). We theorize that spouses similarly co-construct the meaning of mental health symptoms to identify those symptoms serious enough to warrant professional intervention and encourage each other to seek professional care when deemed necessary. Moreover, because barriers in obtaining mental health care exist, such as the stigmatization of mental illness (Thoits and Link 2016), spouses may play a further role in the destigmatization of mental health problems by promoting or encouraging engagement in mental health care. Alternatively, some research suggests that spouses may reinforce the stigma of mental health care (Corrigan, Watson, and Miller 2006; Oestman and Kjellin 2002) and thus not encourage a spouse to obtain care. These possibilities have not been fully explored empirically.
Gender, Marriage, and Professional Mental Health Care
How spouses encourage one another to seek mental health care likely varies by gender due to long-standing and pervasive gendered social scripts, expectations, and roles regarding both marriage and mental health (Thomeer, Reczek, and Umberson 2015b; Schonbrun and Whisman 2010). These dynamics are further complicated by the gender composition of the couple as relationship dynamics depend on not only one’s own gender but also whether one is partnered with a man or woman (Reczek et al. 2018; Umberson et al. 2016). Research on heterosexual marriage has demonstrated that women and men have different expectations, skills, and experiences when one partner is physically ill (Calasanti and Bowen 2006; Pinquart and Sörensen 2006). For example, heterosexual women provide more emotional support for a physically ill spouse—known as emotion work (Hochschild 1979)—and do more health care work by facilitating medical care utilization and compliance than do men in heterosexual unions (Reczek and Umberson 2012). Further, past research suggests that in heterosexual relationships, men are not as attuned as women to their spouse’s emotional and physical needs, drawing on gender scripts that view men as emotionally incompetent (Thomeer et al. 2013; Umberson et al. 2016). When heterosexual women exhibit symptoms indicating mental health problems, heterosexual men may ignore these symptoms. For example, heterosexual men have been shown to deny their wife’s depression to avoid discussion of difficult emotions (Thomeer et al. 2013). Moreover, mental health care may be more stigmatized for men, and heterosexual men may not see mental health care as appropriate for either themselves or their spouse (Apesoa-Varano, Barker, and Hinton 2018; Wendt and Shafer 2016). Therefore, we expect that heterosexual relationships may be characterized primarily by spousal discordance, with women doing considerably more mental health care–promoting activities for their spouse than men.
How might marital dynamics around mental health care look in gay and lesbian couples? Gendered scripts casting men as emotionally self-sufficient and unskilled at understanding emotions and women as highly attuned to the emotional needs of others are prevalent in gay and lesbian relationships (Moon 2014; Rothblum 2009). Therefore, as in heterosexual couples, women married to women and men married to men may also engage in heteronormative gendered dynamics that shape efforts to promote mental health care. For example, lesbian women (much like heterosexual women) perform intensive emotional support for a physically ill spouse, relying on heteronormative constructions of women as emotional experts and innate nurturers (Simon and Nath 2004; Umberson et al. 2016). Lesbian women also appear to provide substantially more emotional support and desire fewer emotional boundaries in their intimate relationships than gay men (Rothblum 2009; Umberson et al. 2015). In turn, like heterosexual men, there is evidence that gay men minimize the significance of physical illness—their own and their spouses’—which is a process that may also extend to mental health symptoms (Umberson et al. 2016). Thus, we expect that gay men—like heterosexual men—may fail to exert effort to get their spouse to seek mental health care, whereas lesbian women—like heterosexual women—may engage in activities to influence and support their spouse’s mental health care use.
Yet, prior research suggests that men and women in gay and lesbian relationships do not necessarily conform to the same traditional gender norms as heterosexual men and women (Fish and Russell 2018; Kimport 2013; Oswald, Blume, and Marks 2005). Some research suggests a different dynamic of health care work for gay and lesbian compared to heterosexual marriages. For example, both gay men and lesbian women appear to promote their spouse’s healthy behaviors (e.g., decreasing alcohol use and smoking) in ways that are similar to those of heterosexual married women (Reczek and Umberson 2012; Umberson, Donnelly, and Pollitt 2018). Moreover, some research suggests that both lesbian women and gay men provide substantial emotional support to their depressed spouse, although lesbian women provide more extensive support in this context (Thomeer et al. 2015b). Additionally, while married heterosexual women with depression commonly conceal their depressive symptoms from their husbands in an effort to protect their husbands, gay men and lesbian women appear to do this rarely (Thomeer et al. 2013, 2015b). Thus, as an alternative possibility, it may be that due to alternative notions of gender in gay and lesbian marriages, gay men and lesbian women may be highly attentive to their spouse’s mental health symptoms and promote their spouse’s mental health care in an egalitarian and reciprocal fashion.
Taken together, research on marriage, mental health, and gender suggests that heterosexual women may encourage heterosexual men to obtain mental health care, but the ways in which this occurs are unknown. Further, the gendered dynamics of gay and lesbian couples suggest that lesbian women will likely encourage the mental health treatment of a spouse, while two alternative but equally plausible hypotheses suggest gay men may—or may not—encourage mental health treatment, dependent on their enactment of either traditional or innovative gendered norms.
Methods
Study Design
With approval from the first and last author’s Institutional Review Boards, data for this study were derived from qualitative in-depth interviews collected between 2012 and 2013 with 90 individuals in 15 gay male couples, 15 lesbian couples, and 15 heterosexual couples (45 couples, 90 individuals) who were legally married and living in Massachusetts. Massachusetts was chosen as the study site because it was the first state to legalize gay and lesbian marriage, thus yielding the largest populations of gay and lesbian married couples. In addition, Massachusetts residents have high rates of health insurance and relatively even access to quality medical care. This allows us to articulate differences across couple type in an environment with similar health insurance rates and care variation across the sample. First, gay and lesbian couples were recruited and interviewed. Next, heterosexual couples who were similar to gay and lesbian couples on age, relationship duration, race, and health insurance status were recruited and interviewed (discussed further in the following). We chose this approach to reduce potential bias in these factors across groups and thus more accurately assert differences across groups due to gender composition of the couple. The majority of gay and lesbian couples in the sample were identified through Massachusetts vital records. State of Massachusetts vital records were used in initial recruitment and yielded the names, birth years, addresses, occupations, and marriage dates from every gay and lesbian couple married in the state between 2004 and 2012, and recruitment letters were sent to these couples. This approach introduces bias because only individuals living in the same home since 2004 received the letters. Additionally, lower socioeconomic status individuals may be more likely to change residences and be harder to locate and are thus underrepresented in our sample.
Cisgender men and women aged 40 to 60 were included as our focus is on midlife married couples. We used a dyadic design wherein data were collected from both spouses. Interviews were conducted separately with each spouse to ensure confidentiality and privacy of each individual, and $50 gift cards were given to each respondent for his or her participation. The same interview guide was used for all respondents and included open-ended questions about general health, health care experiences within marriage, and mental health, and all were asked follow-up questions when appropriate. Open-ended interview topics included broad questions about interactions in mental health care settings, such as “Describe your mental health. Have you had any mental health problems? Has your partner? If so, what was your experience like?” Then, more focused questions were asked, such as “Did your spouse encourage you to go to the therapist? How so and did it work?” and “Did your spouse accompany you to the doctor? Why or why not?” and “If your spouse was present during this medical interaction, describe his or her influence.” We purposefully let respondents determine what types of mental health events were most salient to them to let the most central encounters emerge—overwhelmingly, depression and anxiety were discussed. Among our sample of 45 couples, at least one or both spouses in 37 couples reported periods of self- and/or professionally diagnosed depression or anxiety. Because we allowed respondents to define their own mental illness and do not have official medical reports, we discuss any accounts of mental health symptoms regardless of severity. Although respondents also encouraged informal supports (e.g., talking to a friend, meditating), our focus was on encouragement of formal mental health care, and thus these informal ties are beyond the scope of our study.
Analysis
All interviews were independently analyzed using a standardized method of inductive data analysis emphasizing the dynamic construction of codes for the development of analytical and theoretical interpretations as they emerged from the data (Silverman 2006). NVIVO qualitative software was used to house the data only. Using a standard approach to qualitative data analysis, each author read the transcripts multiple times to ensure understanding of interview content. Thereafter, consistent with standardized interpretivist and constructionist qualitative methodology and epistemology (Roy et al. 2015), the first author conducted the analysis (in consult with the secondary authors), constituting a three-step coding process. First, the first author conducted line-by-line, data-driven categorization to summarize each piece of data as it related to engagement in mental health care. Second, the first author performed “focused” coding to develop categories of professional mental health care initiation by connecting initial line-by-line codes together for conceptual purposes. Third, the first author, in consult with the other authors, created conceptual memos to develop categories and subcategories that related to one another on a theoretical level. Themes from this final stage are discussed in the following. The systematic and rigorous interpretation of conceptual findings by one data analyst is a highly reliable and valid approach to qualitative research (Esterberg 2002). While we analyzed the data for differences in how spouses approached mental health care across mental health symptom type, little variation emerged. Since there were no systematic differences between discussions of depression, anxiety, or other health problems, we do not distinguish between them in our discussion and refer to mental health symptoms and conditions broadly throughout the analysis.
Results
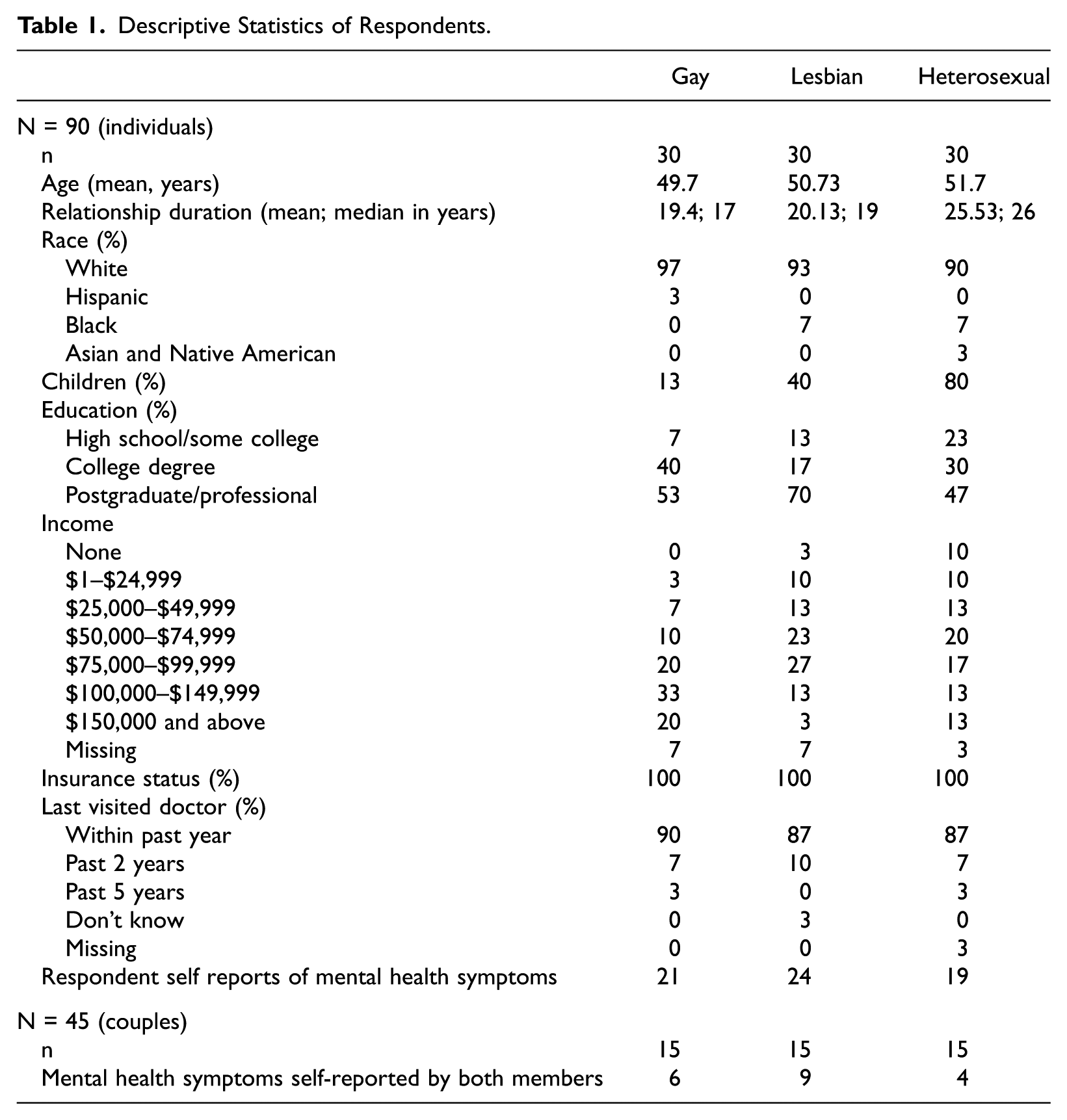
Table 1 presents the demographic data for our participants, showing an approximate average age at 50 for all groups. Consistent with population-level estimates, Table 1 shows average relationship durations between 18 and 23 years across groups, with lower relationship duration among lesbian couples (Carpenter and Gates 2008). Additionally, population-level research suggests that gay and lesbian married couples are more likely to be both white and more likely to be highly educated than their heterosexual counterparts, consistent with our sample composition (Liu, Reczek, and Brown 2013). Table 1 further shows that all couples in the sample have health insurance (required in Massachusetts, the study site) and a majority report seeing a doctor in the past five years. The number of respondents who report their own mental health symptoms and their spouses’ mental health symptoms affecting daily living at some point during their relationship is shown in Table 1, with the vast majority discussing one or more acute or prolonged bouts of depression or anxiety since they married. Spouses were highly congruent in reporting on each other’s mental health, wherein if an individual reported his or her own mental health problems, the spouse generally independently described the same problem. Because of space concerns, we do not report both spouses’ accounts of the same event, especially when they are consistent. We only report both accounts when they enhance the understanding and completeness of our findings (Reczek 2014). We use the term regulating spouse to distinguish the spouse who is promoting mental health care and symptomatic spouse to distinguish the spouse who is viewed as displaying mental health symptoms in a given example. In the following, we demonstrate the processes through which spouses attempt to get one another to address mental health symptoms in a formal setting.
Descriptive Statistics of Respondents.
Respondents often encourage mental health care when a spouse exhibits what is perceived to be a mental health problem. We identify two strategies described by a majority of gay and lesbian spouses and just under half of heterosexual spouses to encourage mental health care. We also identify one strategy of consciously avoiding recommending mental health care among heterosexual couples. These strategies are shown in Table 2, along with the couple gender composition most frequently reporting each strategy. In the first strategy, constructing individual symptoms as hurting individual well-being, we show how respondents construct mental health symptoms as biochemical in nature and serious enough to require medical care, reframing what could be interpreted as individual sadness, nervousness, or feeling “down” into a medical problem affecting the symptomatic spouse’s well-being to a degree serious enough to require medical intervention. We further discuss how this framing destigmatizes participation in mental health care. However, how spouses do this work varies by gender composition of the couple.
Strategies of Mental Health Care Promotion.

In the second strategy, constructing individual symptoms as hurting couple well-being, we discuss how regulating spouses—almost exclusively lesbian spouses—emphasize that the mental health of a symptomatic spouse influences the couple’s relationship quality and therefore individually focused mental health care is needed. In the third strategy, constructing individual symptoms as an individual-level problem for the symptomatic spouse to deal with alone, heterosexual men and women—but virtually no gay men or lesbian women—identified that their symptomatic spouse had a mental health issue but did not encourage that spouse to pursue mental health care. Men and women in heterosexual couples describe this dynamic in similar ways. We note that strategies are not mutually exclusive as the same couple and the same individual within a couple may use multiple strategies to encourage mental health treatment.
Constructing Individual Symptoms as Hurting Individual Well-being
Respondents constructed mental health symptoms as needing mental health care because symptoms negatively affected well-being of the symptomatic spouse. This occurred in two complementary ways—via (1) biochemical emphasis and (2) destigmatization and normalization. Gay and lesbian couples reported both types of strategies, whereas heterosexual men only reported the first strategy (biochemical emphasis) and heterosexual women only reported the second (destigmatization). More gay men than lesbian women reported using these strategies.
Biochemical emphasis
Regulating spouses often made the case that a symptomatic spouse’s mental health symptoms (e.g., not wanting to get out of bed, feeling depressed, trouble sleeping) were biochemical problems that were not the fault of the symptomatic spouse. This framing often involved making the case that biomedical problems needed to be outsourced to a medical professional. Many gay and lesbian respondents and some heterosexual men named a biochemical source and thus a biomedical solution to their spouse’s mental health problems. This typically occurred when a regulating spouse noticed that their symptomatic spouse’s mental health symptoms became more severe than typical. In this way, regulating spouses constructed an acceptable level of depression or anxiety for their symptomatic spouse. Symptoms occurring beyond that level prompted spouses to encourage mental health care.
As an illustration of this process, Sharon described how she convinced her wife, Sandy, that she needed mental health care by likening it to a broken bone: She was crying a fair amount and having a hard time sleeping, all those early signs to make sure you get help for yourself. To me it’s like you get a broken bone, you go to the doctor and you get it fixed. If you’re sad for a length of time and you have some indicators that could mean something else, you go see somebody who handles it.
Similarly, Dianne described how her husband attempted to help her address her mental health problems by suggesting that her problems were not an emotional issue but a biomedical issue requiring medical attention—specifically medication: He just really kind of presented evidence, information whatever, Internet stuff or whatever, or from books or from different philosophers whatever about where you know, hey it is chemical. You know it’s not you. It’s not you not being able to handle something. You know your brain is this whole different thing . . . he was the catalyst for change for me when I went, when I started going on medication.
David also described how his husband Michael was instrumental in him going on medication because Michael framed anxiety as a problem that could be addressed medically: He would say well why don’t you try it [antidepressants]? I know it’s a tough thing. Why don’t you consider it? And so finally one day I went into my therapist and said okay I’m ready to try it. And I went home and told Michael that and he said I’m so happy. He said I’m so relieved. He said, “Do you know how anxious you can be and da-da-da?” And I said, “No I didn’t realize that.” So, he was thrilled.
Michael provided David with an outsider’s perspective not only concerning the extent to which David’s anxiety was negatively affecting his life but also on the biomedical solution to that anxiety. Regulating spouses in this subtheme framed symptoms as medical problems that were both severe and beyond their control. These spouses constructed a new narrative of mental health symptoms as medical and biochemical and therefore requiring a medical solution.
Destigmatization and normalization
Respondents often described resistance from the symptomatic spouse to seek mental health care due to mental health care stigma. Thus, regulating spouses additionally encouraged mental health care via destigmatizing and normalizing therapy and medicine as legitimate and respectable solutions to the problem. The strategy of destigmatizing professional mental health care was pursued consistently by a majority of gay and lesbian couples as well as some heterosexual women and a few heterosexual men. For gay and lesbian couples, this strategy was often reported in tandem with the biochemical emphasis strategy described previously.
Destigmatization of therapy was common in the sample. Troy discussed the need for his husband to go to therapy as if it were asking him to go to the doctor for a physical health concern. Here, Troy normalized therapy as a part of being healthy: I approached it very bluntly, if I thought he needed to do something mental health wise I would tell him. So, I’ve been badgering him to go to individual therapy. . . . And finally he was ready to do it, but I, badgering is like mentioning it once every three weeks not every day. I’m not, I don’t think nagging helps but I think you do need to remind people sometimes that they need to take care of themselves.
Troy saw his process of “badgering” as part of his normal role as a spouse. This work of normalizing and destigmatizing was often discussed as a daily project, occurring continuously within the marriage by the regulating spouse.
Regulating spouses worked to normalize not only therapy but also medication as a necessary step to improve mental health or maintain well-being. For example, Alice described how her wife Maureen reminded her to take her medicine, vigilantly, each day as a normal practice like brushing her teeth: I think our commitment to each other is to be there for each other, period. And you know did you take your meds this morning? Okay cool, brush your teeth. You know, take your meds before you go to bed? Okay cool, brush your teeth. You know, checking in like how are you feeling? How are you doing? How are you sleeping because we’ve recognized that, you know, sleep patterns or eating patterns are definitely indicators of things that we need to be conscious of because that tells us if another shoe’s about to drop.
Maureen kept a close eye on any evidence that Alice’s mental health was declining, including sleep and food habits, as well as reminded her to take her medicine. These practices made Maureen’s care for Alice’s mental health, including medicine upkeep, a normal and everyday part of life. Similarly, Monica, married to Colleen, was resistant to Colleen’s suggestion to take antidepressant medicine. Colleen insisted on this mental health care, together with Monica’s therapist: I think the hard points are right before somebody says, “No, you really need to have the medication” discussion because we both get resistant. One of the features of my depression is I start thinking, “No it’s not that it’s not that bad,” I’ll start with “It’s not that bad,” and then I’ll go to “This isn’t depression” . . . and the people who I love, my sponsor, Colleen, my therapist would say basically, “Honey no this is depression you need to fix it.” . . . And finally I’ll be like, “Fine.” I’ll take the pills and guess what, you know keep going to therapy and then oh okay maybe you were right.
At times, this type of normalizing pressure occurred after the initial health care encounter in reaction to a symptomatic spouse’s resistance in order to promote continued care. Sue discusses how she is able to regulate her husband Henry’s medication uptake to keep him medically engaged: He’s on something for depression and that definitely helps him, I should know this ’cause I do the ordering. Celexa. And he was taking half a tablet and then he took one but he didn’t like being on it so he went back to half and I said, “Honey you really need to go back to one.” He’s like, “Okay.” [Chuckles] “It’ll calm you down a little.” I have noticed over the years when he’s gone back to a half tablet a day I’m like, “Honey did you change your medication a little bit?” He’s like, “Yeah.”“Well you need to bring it back.”
In this way, regulating spouses drew on their sense of trust and intimacy to convince a symptomatic spouse that receiving professional care or medication is necessary and legitimate. This normalization—and the daily enactment of these processes—was key to getting spouses to seek mental health care.
A subset of spouses pointed to their own experiences in pursuing mental health care to frame this care as normal and helpful. Sean recounted the process through which he followed his wife Wendy’s lead in getting on medication: She was helpful because she was on medication at the same time and she was telling me how it worked for her. She was on Zoloft, she saw a doctor first and was on medication first. She was first and then I guess even knowing that you could go to a doctor and talk about these things was helpful for me because I’d never seen a doctor about it before. She kind of took the lead on that, too . . . because it’s not a decision you take lightly I don’t think. I mean I don’t think the same way anymore but you think, “Oh I’m changing my personality or is this how I’m supposed to be?”
Any worries Sean had about being medicated for mental health problems dissipated when his wife Wendy went on antidepressants and was open about her experiences with him. In this way, a reluctance or fear of getting mental health care was reduced by spouses’ work to frame mental health care as valid, normal, safe, and health promoting.
Constructing Individual Symptoms as Hurting Couple Well-being
A majority of lesbian couples but only two gay couples and two heterosexual women encouraged a symptomatic spouse to seek professional care—most often individual therapy but also couples’ therapy—because their spouse’s symptoms were influencing the marriage. In this theme, regulating spouses framed relationship problems as a consequence of a symptomatic spouse’s individual mental health symptoms. Donna discussed how early in their relationship, Lisa’s mental health problems significantly affected their relationship and Donna successfully demanded Lisa receive mental health care: When Lisa and I got together, we would get into unbelievable fights. And, so I would, so I’d be like what is going on? And so she was talking about it was anxiety and . . . I was like, you know what, you either need to go, you need to go see about getting something to take care of this or I’m not, or we’re going to end this relationship. I was really serious and I was like I don’t deserve to get, to get treated like this. And she went in and she prescribed her something.
Similarly, Joyce described asking her wife Julie to go see a therapist because the severity of Julie’s mental health symptoms was negatively influencing their relationship: She seemed to have a little bit of an anger issue and I told her that if she, you know that I couldn’t live with that kind of anger. . . . If the vacuum hit something she’d get upset with it and you know yell or something. I think that was the most stressful thing, we just had to have a conversation about her [going to a therapist].
Julie also recounted the events leading up to her decision to seek counseling, saying: Joyce said, “We need to talk.” So, we sat down and she said she just was really not happy with how things were going because I was just in a miserable mood. I’d like try to pull it together at work but I would just be not so nice at home and not pleasant and I tried to rally but I felt like there was this big cloud. . . . So, she was wonderful and just very supportive and said “I just think we need to do something because this isn’t working.”
Joyce invoked the well-being of the couple in a plea for Julie to seek mental health care medically as this problem was not able to be adequately addressed within the home. This plea was highly effective, and Julie sought treatment.
Debbie similarly described how her wife Karen’s mental health problems affected their relationship quality and her own well-being, and thus Debbie encouraged Karen to seek professional care: The anxiety that she feels around a lot of things and the fact that she’s somewhat socially isolated has affected me. And at times I’ve said to her I can’t be like her only support. . . . This is stressing me out and part of going to therapy is taking responsibility for what’s happening.
As one of the two gay spouses that reported this strategy, Kevin was frustrated with the negative effect of his husband Joe’s mental health symptoms on their relationship: Joe also is on medication for depression and has been probably for seven years or something and does also see a therapist. That was at my insistence. It took a long time. . . . He was [so stressed]. . . . I thought, this is someone who is willing to go down with the ship in our relationship but the ship doesn’t have to go down if you’re willing to like bail some things. . . . So that was when I was really, look, I really think you need to do something here.
Joe reported that Kevin approached him about his problems, saying, “And it hadn’t really occurred to me [until Kevin said something] and I pretty quickly got on antidepressants. It definitely occurred to Kevin that I was depressed.” Couple well-being was framed as a symptom of one spouse’s mental health that must be addressed medically rather than in the home.
Finally, some regulating spouses encouraged couples’ therapy to address individual-level problems. Troy said that he attempted to persuade his husband Gerald to go to therapy: We’re reconnecting and re-communicating again after a period of not communicating and out of me trying to persuade him in couples’ therapy to go to individual therapy without actually saying go to individual therapy. . . . I don’t necessarily need to be involved in his issues and his stresses but I think somebody does. . . . I’ve told him point blank, you need to go to individual therapy and he’d always come up with excuses.
Couples in this subtheme demonstrated the ways in which a symptomatic spouse’s mental health problem required medical intervention via individual and (less commonly) couples’ therapy when the relationship well-being was affected. Because regulating spouses did not see themselves as able to remedy the individual mental health problem in the home, they saw and sought their primary solution from the medical community. This approach increased the pressure to fix the individual problem medically as it was now—a couple-level problem.
Constructing Symptoms as a Spouse’s Problem to Deal with Alone
Nearly half of heterosexual couples in our analytic sample (both men and women) but no gay or lesbian couples described failure to encourage mental health care when health symptoms arose. These nonregulating spouses conceptualized the symptomatic spouse’s mental health as a serious issue but did not promote mental health care because a spouse would not be willing to go, it was a spouse’s issue to deal with alone, or it was something the spouse was incapable of addressing. Thus, in addition to not encouraging mental health care, there was often very little encouragement or support around the mental health symptoms in these couples.
Sherri said that she believed her husband Jeremy would benefit from seeing a therapist: “I think that he probably could really benefit from going to someone like that now because I think he must be very depressed and feeling really bad about himself but he’s the type that, he’ll never do it unless I really push, push, push, push him to do it.” Sherri did not wish to push Jeremy, in part because she believed her effort would be substantial and therefore did not encourage him to seek mental health care for what she saw as a clear problem. In turn, Jeremy talked about Sherri’s mental health problems and how he did not encourage her to seek help: I am not sure if Sherri is mildly depressed. She mentioned that she takes some antidepressants but I am not quite sure if the depression was the diagnosed or if it was for something else. . . . But I don’t think she is seeing a psychotherapist and if she does I do not know about it.
In this way, Jeremy was not attuned to what was happening with Sherri’s mental health—including what medication she was taking and why. While he expressed worry about Sherri, he did not bring this up to Sherri. Similarly, Miranda’s husband Bill was having some mental health issues. She reflected on how she made note of these issues but failed to encourage him to seek help: I think the challenge always is how do you help to care for someone and not smother them or take away their sense of self. And you balance some of that with well how functional are they? Are they being self-destructive? Are they about to become self-destructive? . . . I think that his father suffered from depression and took his life. I think that in that way he’s sort of resistant to that diagnosis.
In contrast to the previous themes of encouraging mental health care, Miranda and other respondents in this theme did not frame mental health symptoms as biochemical but rather a normal part of life that should be accepted and addressed on the individual level. Respecting Bill’s independence, Miranda viewed Bill’s mental health as a problem but did not attempt to normalize or destigmatize care despite her desire to do so because she anticipated a high level of resistance. Nonregulating spouses insisted that their symptomatic spouse could handle their own health problem even though the ability of the symptomatic spouse to assess his or her personal health is sometimes questioned. Similarly, Dean, married to Cindy, said: But when she gets overwhelmed at work, I have seen her get depressed. It was for about a month and I’m like “oh my god, where did she go?” You know, even the kids noticed it. It was lousy. I’ve never seen her that bad. Usually she just, I’ve seen her get overwhelmed, cry a little bit, and get over it. She’s good like that. [Did you encourage her to seek counseling?] No, no.
This theme illustrated how both heterosexual husbands and wives readily identified mental health issues of their symptomatic spouse without an understanding of whether a spouse is currently being treated (i.e., visits with clinicians, medication use, etc.) and without intent to encourage mental health care. This stood in contrast to the majority of the gay and lesbian couples and some heterosexual couples that were aware of a spouse’s current or previous individual attempts to seek mental health care and the corresponding motivation to encourage their spouse’s care for the current issue.
Discussion
In this study, we contribute to research on mental health in marriage by considering how spouses encourage professional mental health care as part of the broader constellation of what is known as health care work (Reczek et al. 2018), as well as how these dynamics vary by the gender composition of the couple. We draw on a unique qualitative dyadic data set that allows us to consider each spouse’s perspective on mental health care and relationship dynamics within the couple and provides a comparison of men and women across gay, lesbian, and heterosexual marriages. Through this study, we demonstrate that decisions to seek mental health care are a couple-level process for some—but not all—married people. Research on mental health care utilization tends to have an individual-level focus (e.g., O’Brien, Hunt, and Hart 2005), yet our findings highlight how decisions to undertake mental health care also occur at the couple level. In particular, our findings show that many spouses intensely engage in the acquisition of mental health care via attunement to the emergence of mental health symptoms, expression of concern about those symptoms, and attempts to convince a spouse that the problems are serious enough to require professional care. This finding is in line with Horwitz’s (1982) theory of “therapeutic social control,” in which family members and professionals are expected to work to get those with mental health issues to undergo treatment (see also Perry, Frieh, and Wright 2018). Future research should explore whether these same processes occur in other family and social network ties such as parent-child relationships, siblings, and friendships.
Moreover, our study identifies unique strategies used to promote the mental health care of spouses, with variation by couple type (also see Table 2). First, findings reveal that regulating spouses reframe mental health symptoms with explicit medical language (e.g., depression, anxiety) rather than using emotional frames of sadness or worry (Dincin 2001). This language shift—a dimension of medicalization—allows for advocacy of medical intervention to “treat” a mental health concern via a psychiatrist or pharmaceuticals; this is in contrast to addressing the concern within the home or using other informal strategies such as talking to friends (Aneshensel, Phelan, and Bierman 2013; Conrad 1992). Spouses that reported this strategy framed mental health symptoms as the result of biology and chemistry, outside the individual’s locus of control, and thus requiring medical intervention. This theme varied by gender composition of a couple, taking prominence among gay men and lesbian women, although it was also discussed by heterosexual men. We theorize that spouses who enacted this approach did so by drawing on masculinity scripts avoiding informal care and relying on scientific “problem solving” via professional medicine (O’Brien et al. 2005; Trief et al. 2003).
Second, the majority of both gay men and lesbian women and some heterosexual women worked to destigmatize and normalize mental health treatment, partly in reaction to cultural norms that suggest mental health care is to be avoided due to stigma. This occurred in two specific ways that varied by gender composition of a couple. Spouses married to men (i.e., gay men and heterosexual women) worked to lessen the stigma of mental health treatment to promote men’s professional mental health care. One way this was achieved was through suggestions of couples’ counseling as spouses discuss how they could not or would not directly ask their husbands to obtain individual therapy (Oliffe and Phillips 2008). The similar processes performed by gay men and heterosexual women may reflect a particularly salient stigmatized response of men toward formal mental health care given that both groups are married to men. In contrast, but still within the broader goal of destigmatizing and normalizing formal mental health care, some lesbian women in our sample used acts of intensive and continual emotion work to get their spouses to seek care. This is consistent with prior research suggesting that women married to women are especially attuned to the emotional needs of their partners (Thomeer et al. 2015a). Taken together, this study provides new, nuanced insight into how marriage plays a key role in the acquisition of care through tactics of destigmatization in ways that vary by the gender composition of the couple (Clair, Daniel, and Lamont 2016). Heterosexual men were largely absent from discussions of destigmatizing their wife’s mental health concerns, perhaps due to the fact that this work involves intensive care and emotion work, which heterosexual men appear to engage in less often than other groups (Thomeer et al. 2013). Thus, heterosexual women do not receive the work of destigmatization, which may inhibit their utilization of mental health care.
Third, results show that lesbian spouses uniquely drew on evidence that their marriage was being harmed by a symptomatic spouse—and thus they encouraged and sometimes demanded a spouse obtain professional care. This suggests that some lesbian women in the sample viewed couple-level marital problems as the result of individual psychological, biological, and chemical problems (e.g., medicalization) rather than the result of unhealthy relationship dynamics. This finding further provides evidence that it is the gender composition of a couple, not gender alone, that influences the ways in which spouses encourage mental health care given that only women partnered to women, not women partnered to men, deployed this strategy. The combination of two women in a couple may produce a dynamic wherein both spouses create a symbiotic assessment of the importance of relationship quality and the role of individual mental health in relationship quality. This finding dovetails with a recent study showing that mental health negotiation was more emotionally intensive for lesbian women compared to gay men and that lesbian women tied intimacy more closely to sharing and monitoring emotions than gay men, heterosexual women, or heterosexual men (Thomeer et al. 2015b).
Finally, we find that a majority of heterosexual men and women who noticed spousal mental health symptoms failed to promote professional mental health care. This finding is consistent with research suggesting that heterosexual men have significant resistance to treatment because they feel that mental health issues are stigmatized to a greater degree than women (Addis and Mahalik 2003; Johnson et al. 2012; Oliffe and Phillips 2008) but inconsistent with research suggesting that heterosexual women who promote their husband’s physical health provide emotional support to men around mental health issues (Thomeer et al. 2013; Trief et al. 2003). One explanation is that heterosexual women and men who noticed mental health symptoms privilege notions of individuality and independence over spousal regulation. For example, there may be an interactive process within heterosexual couples that encourages a lack of engagement around mental health care. These gendered scripts may mean that heterosexual men may not value professional mental health care for themselves and therefore fail to encourage women to seek mental health treatment. Moreover, heterosexual men may even reproach women’s attempts to encourage men’s mental health care, and this may mean that over time, heterosexual women are less likely to encourage mental health care after initial rebukes earlier in the relationship. Therefore, this may be a particularly unique dynamic that unfolds in long-term marriages. Spouses describing this form of independence and purposeful nonregulation may be especially pronounced in the case of mental health care due to the stigmatization of mental health problems writ large (Thoits and Link 2016).
It may also be that heterosexual women (and men) experience greater stigma or less recognition of one another’s mental health issues and therefore may be more likely to pursue informal strategies to care outside of the medical domain as they do not see these issues as medical problems. While we do not have data to assess these more informal practices as our focus was on formal mental health care, we suggest that encouraging a spouse to talk to a friend rather than talk to a therapist could be occurring in heterosexual couples; spouses may also recast mental health issues as part of one’s personality and not changeable (e.g., understanding a spouse as antisocial or a homebody) and therefore not attempt to address this behavior medically. Additionally, while we worked to match respondents across union types on education, heterosexual spouses had lower levels of educational attainment, and education is associated with mental health stigma and health care utilization (Corrigan et al. 2012). Therefore, it may be that heterosexual spouses do not encourage one another to seek mental health care because heterosexual partners have less education and thus perceive higher levels of stigma than their gay and lesbian counterparts. As stigma around mental health care decreases throughout society, heterosexual spouses in particular may be more comfortable encouraging their spouses to pursue this care.
Limitations
Despite significant contributions, there are several limitations to the present study. First, there were fewer heterosexual couples where both spouses reported mental health problems relative to gay and lesbian couples, and this may explain differences in findings across groups; future work should examine heterosexual couples wherein both spouses report mental health problems to further assess these dynamics. Second, the sample presented here is of midlife adults because this is shown to be the time of highest depression and lowest happiness (Case and Deaton 2015; Galambos et al. 2015). However, regulating mental health care may take different forms later or earlier in the life course. Third, the sample in this study overwhelmingly reported depression and anxiety as their primary mental health symptoms. Very few respondents discussed more serious mental health concerns. Therefore, our findings reflect how spouses engage with what may be considered less serious mental health symptoms. Vastly different spousal dynamics may be present in relation to mental health diagnoses such as bipolar or schizophrenia, and future work should address this possibility. Fourth, this sample consists of long-term couples that have demonstrated histories of staying together over time and through periods of mental health concern. Future work should explore these dynamics in couples that are transitioning to marriage or cohabitation to see how the processes found in this study develop and change over time. Chronic mental health conditions may lead to the dissolution of a relationship, meaning that couples with the worst mental health are unlikely to be represented in our long-term sample. Fifth, this sample is socioeconomically advantaged and primarily white, with nearly all individuals reporting that they have health insurance that covers mental health care visits and have middle-class income. Spouses may engage in each other’s mental health care differently if health insurance does not cover mental health care and may operate differently by race, and future research should address these possibilities. Finally, our findings are potentially biased by the fact that all same-sex couples in this sample were legally married. For example, marriage rates among midlife sexual minority individuals show that only 24 percent are legally married, compared to 26 percent that remain partnered and unmarried and 50 percent that are single (Goldson et al. 2017). With lower rates of marriage, it is possible that same-sex individuals who select into legal marriage also carry other characteristics into the marriage that make them more likely to be invested in their partner’s mental health and that these characteristics differ from heterosexual individuals who select into marriage.
Conclusion
This study makes significant contributions to the sociology of mental health and mental health care utilization. Our main finding shows that spouses play a significant role in facilitating, promoting, and encouraging engagement with professional mental health care in ways that fit within the broader theoretical construct of “health care work” (Reczek et al. 2018); previous research has not articulated health care work dynamics regarding mental health care. Importantly, research on heterosexual men repeatedly shows that men resist seeking help for mental health conditions, yet these studies pay little attention to gender composition of couples and rarely develop theoretical models that include multiple masculinities, such as gay or lesbian masculinity (Addis and Mahalik 2003; Oliffe and Phillips 2008). Thus, gender compositional differences in strategies of mental health care facilitation suggest that there are unique, perhaps adaptive dynamics found in gay and lesbian couples that make spouses highly attuned to the mental health needs of one another. Our study confirms normative findings for heterosexual men but adds that gay men do not necessarily follow the same patterns of refusal and may be more engaged in both medicalization and destigmatizing techniques than heterosexual men. Lesbian women enact additional unique ways of supporting mental health care. Understanding how gay and lesbian adults choose to seek mental health care is important in light of higher rates of suicide ideation, suicide, and depression of gays and lesbians compared to heterosexuals (Hatzenbuehler, Hilt, and Nolen-Hoeksema 2010; Meyer 1995). This study has important implications for researchers looking to understand why some individuals seek care and others do not and provides policymakers the opportunity to promote mental health interventions via spouses or other family members.
Footnotes
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported, in part, by the following grants: The Office of the Director, National Institutes of Health and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R03HD078754 PI: Corinne Reczek, Hui Liu); The Ohio State University Institute for Population Research through a grant from the Eunice Kennedy Shriver National Institute for Child Health and Human Development of the National Institutes of Health (P2CHD058484); National Institute on Aging at the National Institutes of Health (R21AG044585, PI: Debra Umberson); Investigator in Health Policy Research Award to Debra Umberson from the Robert Wood Johnson Foundation; and the Population Research Center at The University of Texas at Austin through a grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (P2CHD042849).