
Abstract
Significance:
Wound healing in irradiated skin remains a clinical challenge, with radiation therapy (XRT) resulting in excess collagen deposition and cell death resulting in poor tissue quality. This frequently results in chronic wounds that compromise patient outcomes and quality of life.
Recent Advances:
Improved understanding of the pathophysiology behind radiation-induced soft tissue injury has led to the development of promising treatments. These include dermal substitutes, placental derivatives, fibronectin, injectable fat-derived and plasma-derived compounds, hyperbaric oxygen, and deferoxamine.
Critical Issues:
Many traditional approaches to wound healing are often limited by poor tissue quality seen following XRT. A better understanding of mechanisms by which radiation induces these pathological changes may lead to the development of more effective therapeutics.
Future Directions:
Treatments leveraging recent insights into collateral radiation injury may help to condition tissue to promote healing/regeneration of wounds. Although animal studies and human case reports have been promising, wide-scale clinical studies examining their efficacy are still needed before many of these novel strategies may be adopted to help the millions of patients worldwide suffering from radiation-related cutaneous wounds.
Derrick C. Wan, MD
SCOPE AND SIGNIFICANCE
Radiation-induced fibrosis (RIF) is a debilitating and progressive condition affecting a significant portion of patients who undergo radiation therapy (XRT) for cancer treatment. While acute manifestations of radiation-induced skin injury such as radiodermatitis are important, we refer to RIF in this review to capture the pathophysiologic effects that contribute to impaired wound healing in irradiated tissue. These changes disrupt normal healing processes and present major clinical challenges for wounds in irradiated skin. These wounds cause functional impairment and pain. With half of cancer patients receiving XRT, exploring new therapeutic approaches for wound healing in irradiated tissue is increasingly important.
TRANSLATIONAL RELEVANCE
Efforts to address RIF have led to significant advancements in preclinical models, which are now being validated in early clinical use as well. The animal studies have provided critical insight into the mechanisms of fibrosis and facilitated the exploration of these emerging therapies. Promising among these are highlighted herein and include dermal substitutes, placental derivatives, adipose- and plasma-derived injectable therapies, and topical treatments. With high-quality wound care and the addition of these treatments, nonsurgical outcomes will soon provide solace for patients with these debilitating wounds.
CLINICAL RELEVANCE
RIF profoundly affects wound healing, posing significant clinical challenges that impact both patient quality of life and potential future reconstructive efforts. Radiation injury results in an aberrant healing response characterized by persistent inflammation, excessive collagen production by fibroblasts, decreased vascularity, and dermal hypocellularity. These combined issues make for poor oxygen and nutrient delivery to the skin. Ulceration or further insult to the skin in this state frequently leads to wounds that do not heal. The showcased treatments below aim to correct RIF pathophysiology to allow the body’s natural healing response to occur.
BACKGROUND
RIF is a progressive condition that occurs as an unfortunate consequence following XRT, a staple of solid tumor cancer treatment. Its pathogenesis involves a complex interplay of many related biological processes, most notably characterized by a sustained, aberrant wound healing response leading to fibrosis and tissue/organ dysfunction. 1 As reconstructive surgeons and their patients know all too well, fibrotic tissues are clinical nightmares as they are friable and incredibly prone to wound healing issues.2,3 Patients with wounds on irradiated fields endure long-term treatments that are oftentimes painful and debilitating to keep their wounds from progressing, becoming infected, or possibly leading to further surgeries such as amputations, large debridements, or complex reconstructions that may require substantial donor tissues from elsewhere on the body. These complications affect a staggering number of patients. Half of all cancer patients undergo XRT, and it is thought that 95% of them will experience some level of radiation dermatitis. Of these patients, 10–31% experience moderate-to-severe skin reactions (e.g., wet desquamation), and 5–18% develop ulcers or chronic wounds.4–8 These figures equate to over 50,000 new patients every year in the United States who will have to deal with RIF-associated wounds. In addition, from an economic standpoint, chronic wounds and their treatments incur an estimated $28 billion in Medicare costs annually, and this is thought to be a conservative estimate (Fig. 1). 9
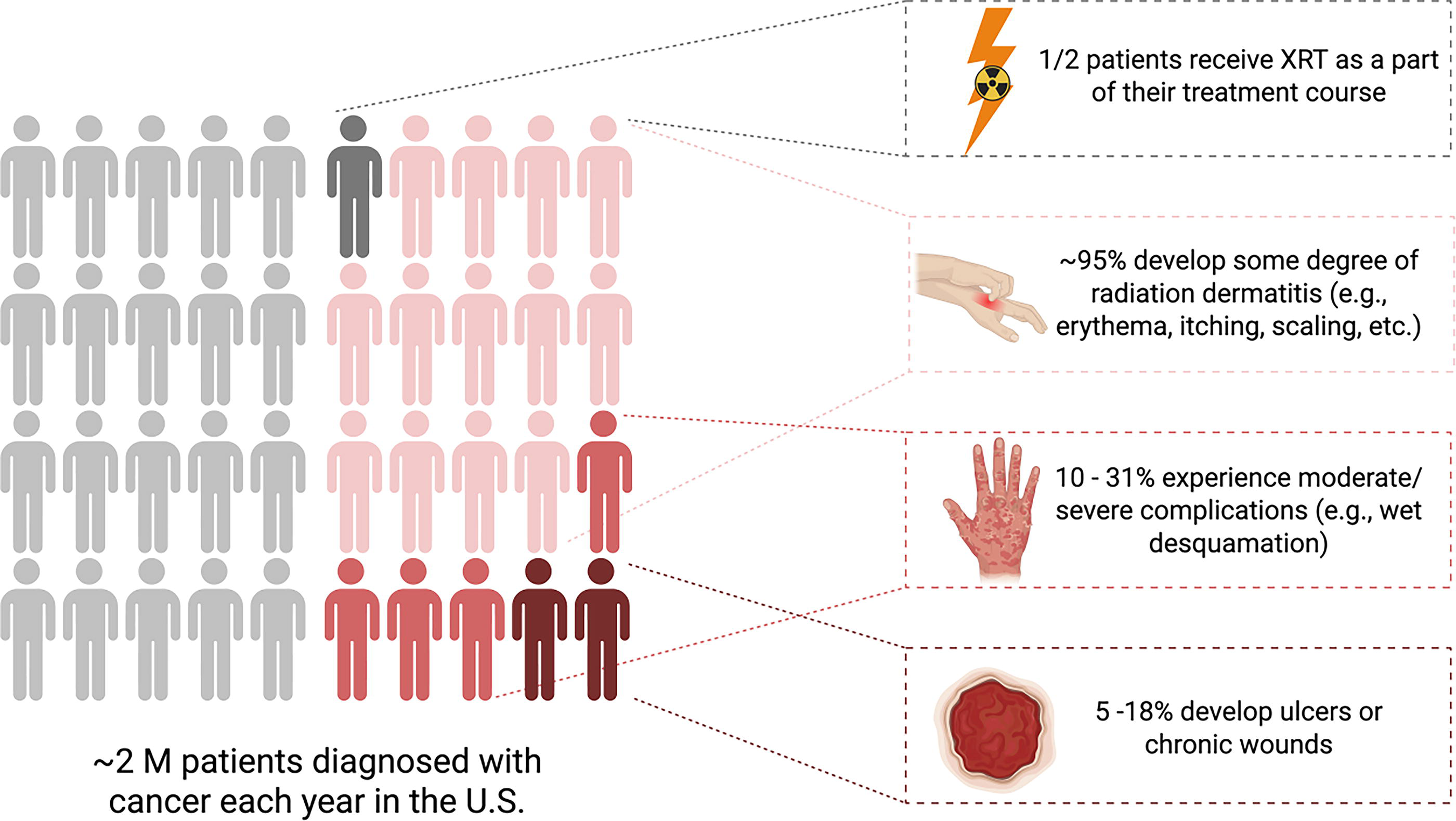
Incidence of radiation-induced skin injury. The impact of radiation-induced skin injury is staggering. Nearly two million Americans were diagnosed with cancer last year, of whom roughly half will receive radiation therapy (XRT) during their treatment course. Nearly all patients exposed to XRT experience radiation dermatitis and a significant portion experience moderate or severe cutaneous manifestations such as desquamation or ulceration.
Chronic wounds are those that do not heal within an expected time frame. This is sometimes clinically arbitrary and difficult to pinpoint experimentally since wound depth and mechanism will change expected healing rates, however, it is generally accepted that skin wounds that are open on the order of 1 month or longer can be considered chronic, as healthy tissue should have healed. As opposed to the sometimes unclear time frame for wound chronicity, chronic RIF is a defined entity characterized by specific tissue changes and typically occurs 4–12 months after radiation injury. 11 At this stage, the inflammation associated with wound healing becomes perpetually dysregulated and creates a difficult problem to circumvent as fibro-atrophic tissue changes have already set in.11,12 These changes are permanent and predispose patients to wounds in these irradiated fields for life, with many cases occurring years or decades after XRT.13,14 In addition, wounds that develop on these altered tissue beds can be incredibly difficult to heal. 15 Thus, some treatments in development target the acute phase of RIF in the hopes of avoiding problematic tissue conversion. Prevention of RIF should be the primary goal, and the field of radiation oncology has made great advances in decreasing the exposure of nearby healthy tissues with precise targeting of XRT as well as developing optimal fractionation strategies. 16 Nevertheless, there is always some level of unintended injury to the overlying soft tissue, especially in the case of oncologically necessary wider exposures. Preventative measures aside, there also exists some promise in recent wound healing therapies in reversing the fibrosis that has already set in, which will be more directly applicable to the patients who are currently dealing with chronic wounds.
Key takeaways
RIF-related wounds impact millions of patients worldwide and drive significant health care costs. Wound prevention and emerging treatments are essential to improving outcomes. Ionizing radiation kills cancer by inducing DNA damage but also harms rapidly dividing normal tissues such as skin.
Pathophysiology
Direct injury
Ionizing radiation exerts its antitumor effect by causing direct cellular injury through DNA damage. This then induces natural protective mechanisms, including cell senescence or programmed cell death processes such as mitotic catastrophe and apoptosis. 17 Rapidly dividing, highly metabolic cells such as cancer are more sensitive to this process as they spend a proportionally greater amount of time in radiosensitive phases of the cell cycle. As cells progress quickly through the cell cycle, they have less time between phases to repair damage before permanently adopting the mutation. Loss of DNA repair mechanisms in malignant cells further potentiates the accumulation of damaged DNA. It is important to keep in mind that this is a beneficial and necessary injury. Unfortunately, skin is also a highly proliferative, metabolically demanding, superficial organ that is often inadvertently harmed. 17 As skin basal layer stem cell populations and function decline, they cannot keep up with repopulating the normal shedding of superficial layers, and desquamation results. 18
Key takeaways
Ionizing radiation kills cancer by inducing DNA damage but also harms rapidly dividing normal tissues like skin.
Indirect injury
In addition to direct DNA damage, ionizing radiation produces reactive oxygen species (ROS) as a by-product of macromolecular destruction and water radiolysis. 19 These ROS cause further damage to cellular components, including DNA, lipids, and proteins, which leads to a vicious perpetuation of ROS-induced inflammation. This major component of indirect radiation injury is theorized to be even more damaging to skin than direct injury in the long term.
Damaged cells respond to injury by inducing an inflammatory response through cytokine release. This involves countless signaling molecules acting on many different cell types, but well-studied pathways reveal that a sharp upregulation of transforming growth factor-beta (TGF-β), tumor necrosis factor-alpha, and interleukin-1 occurs, which are primary drivers of the inflammatory cascade and increase ROS formation. 20 Aside from cell recruitment, these signaling molecules also play a role in catalyzing the differentiation of nearby cells into fibroblasts, and in the case of the aforementioned progressive fibrosis, myofibroblast subtypes predominate. Fibroblasts are responsible for the production of collagen, and extracellular matrix (ECM) proteins and myofibroblast subtypes serve as the contractile elements in scars and fibrotic tissues. 21 In addition to the upregulation of ECM production, the balance between matrix metalloproteinases and their inhibitor proteins is thrown into disarray. These enzymes collectively are responsible for ECM turnover and remodeling. In chronic RIF, although tissues are “woody and inflexible,” there is actually impaired ECM production and contractility by fibroblasts. 22 In addition, epidermal keratinocytes are less proliferative leading to delayed cell migration and epithelialization in the wound setting. 23 This hypocellular state and decreased rate of collagen production result in slower granulation tissue formation and weaker mechanical strength of a healing wound bed.
Key takeaways
Radiation also causes prolonged injury due to ROS propagation and inflammatory cytokine-driven pathways. This promotes fibrosis, ECM deposition/turnover imbalance, and impaired wound healing.
Endothelial damage
Concurrent injury to dermal blood vessels further complicates the picture. The same direct and indirect injuries described above are suffered by the skin’s microvasculature. The papillary dermis superficial capillary system has a remarkably large surface area, receiving >5% of total cardiac output at any given time, but can be much higher as it plays an important role in body thermal regulation. 24 Skin is metabolically demanding and epidermal turnover is rapid, so a baseline high blood flow is necessary. Widespread microvascular damage, as seen in radiation injury, causes a similar double-hit effect. The inner lining of the blood vessel, the endothelium, acts to recognize injury and drive inflammatory processes. In the event of ionizing radiation, these expected processes are instigated, but do not cease. Increased vascular permeability, that is, the loss of endothelial tight junctions, allows for capillary leak and immune cell migration. In response to an acute injury, there is a temporary increase in dermal blood flow to augment the delivery of immune cells and nutrients. This process is meant to promote a healing-centric local milieu, however, given the perpetual damage, this is not achieved. Production of nitric oxide, the key endogenous vasodilator, is increased in response to radiation injury and perpetuates oxidative stress through conversion to reactive nitrogen species such as peroxynitrite. 25 The endothelium is further damaged by the dysregulated inflammatory cascade of its own doing, eventually ending in microvascular destruction (Fig. 2). With the loss of a robust blood supply, diminished nutrient delivery and local hypoxia upregulate further pancellular destruction and inflammation. This again increases ROS production and perpetuates impairment, leading to the hypocellular, scarred chronic fibrotic state. This occurs on a spectrum that is difficult to predict. In severe cases, what is left of the skin is a wasteland of weak, disorganized ECM from the healing process gone awry. It has a low metabolic demand and no further cell death, but also no remaining healing potential if a wound were present.
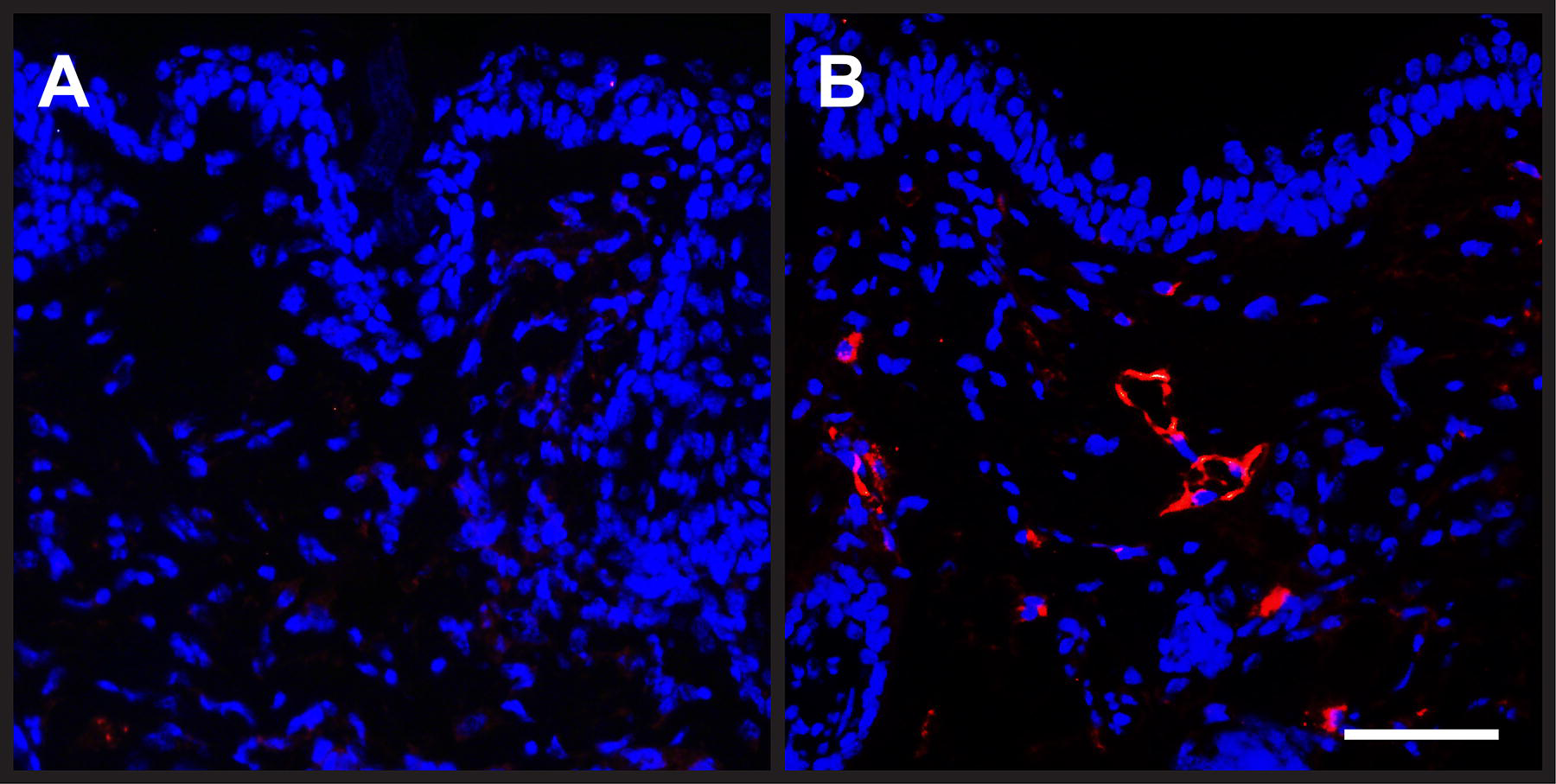
CD31 immunofluorescence demonstrating radiation-induced microvascular damage. Images of immunofluorescent staining of murine skin for endothelial marker CD31 (red) and DAPI (blue).
Histological preparations of skin in the chronic phase of RIF reveal this disheartening wound-prone landscape. 26 With epidermal thinning and a scarred, thickened underlying dermis, relatively small insults to the skin can precipitate large, difficult-to-heal wounds. Mechanical strength testing and collagen ultrastructure analysis reveal thick but weak tissues. Rather than the high tensile strength basket weave dermal collagen organization, we find thick parallel bundles of collagen in the irradiated dermis. 27 Similarly, we can visualize the impact of microcirculatory destruction. Capillary thrombosis and perivascular fibrosis contribute to significantly reduced flow and decreased oxygen tension/diffusion capacity over the blood vessels that remain. Superficial imaging of dermal blood flow, such as laser Doppler analysis, corroborates this decrease in vascularity over time.28,29
Key takeaways
Radiation damages skin microvasculature causing capillary leak, hypoxia, and further oxidative stress. Dermal collagen in the chronic RIF state is weak and disorganized, leading to vulnerability.
Ferroptosis
There has been mounting interest in the role of iron-dependent programmed cell death, termed ferroptosis, among many dermal pathologies (RIF, autoimmune, genetic, neoplastic, infectious, etc.).30,31 Studies are revealing that unique cellular morphological changes occur in ferroptotic cells that differ from classical apoptotic changes, implying that these death pathways are distinct means to a similar end. The most notable of these distinctions being mitochondrial alterations that are not seen in other programmed cell death pathways. With increased iron levels from overload or blood breakdown, iron is taken up by cells and forms labile iron pools within cell membranes. Ionizing radiation has been shown to cause an increase in local labile iron concentrations due to the disruption of normal iron metabolism, storage, transport, and direct microvascular hemorrhage.30,32
Several key players in ferroptosis have been described. First, labile free iron (Fe2+) in the tissues holds nonenzymatic redox potential and generates ROS when interacting with hydrogen peroxide (H2O2) through Fenton reactions. 33 Second, the resultant hydroxyl radicals interact with cellular phospholipids, namely polyunsaturated fatty acids, which are particularly susceptible to peroxidation reactions. The lipid radicals that are formed in this process then react with oxygen to create lipid peroxyl radicals, which abstract hydrogens from neighboring phospholipids, propagating a chain reaction. The above reactions take place without enzyme action. Endogenous enzymatic lipid peroxidation, on the contrary, is tightly controlled and occurs through lipoxygenases, which have been shown to play a regulatory role in some cancer suppression pathways, such as TP53-mediated suppression. Finally, glutathione, the endogenous antioxidant, can directly reduce these lipid peroxyl radicals, halting the free radical propagation cycle. Glutathione depletion, whether due to irradiation (IR) exposure or drug-induced, has been shown to induce cellular ferroptosis.34,35 Ultimately, therapies that target the ferroptosis pathway or hold antioxidant potential may prove themselves as powerful adjunct wound healing treatments for conditions such as chronic RIF that affect local iron concentrations.
Key takeaways
Ferroptosis is an iron-dependent cell death pathway, distinct from apoptosis. Targeting RIF’s disrupted iron metabolism and boosting antioxidant potential may offer novel treatments for radiation-related wound healing.
Clinical manifestations
When it comes to healing chronic wounds, traditional teachings emphasize reversing the underlying cause if possible. Examples include blood glucose management in diabetic patients, revascularization for peripheral arterial disease, or offloading in the case of pressure-related injuries.36,37 Unfortunately, the fibro-atrophic changes related to XRT are generally thought to be irreversible. This leaves clinicians with very few options aside from long-term, strict wound care regimens, or complex reconstructions for wound coverage.
With the aforementioned tissue changes and prolonged inflammatory response, there is a significant disruption in the expected phases of wound healing. All three stages are affected: inflammation, proliferation, and remodeling. The proliferative and remodeling phases of healing are achieved much slower and are inefficient, leaving patients with chronically open wounds.38,39
Infection
It is no wonder that wounds on irradiated fields are very susceptible to infection. First, by nature of any open wound, bacteria have an entry point. Second, with the fibro-atrophic skin changes and diminished blood/lymphatic flow, there is a reduction in immune cell transit leading to less recruitment and delays relative to bacterial invasion. 40 Third, XRT alters immune cell phenotypes. Notably, antigen presenting cells in the dermis, particularly macrophages, undergo changes in their activation states toward profibrotic niches under TGF-β signaling, which drives RIF and also diminishes their innate antimicrobial capabilities.41,42 (This switch was previously described as the M1/M2 macrophage dichotomy, which is becoming an outdated but still often-utilized term.) 43 In summary, it is not only the tissue quality but also a dysregulation of the immune cells themselves that dampens the antimicrobial response, allowing bacteria to thrive in the RIF environment. 44
Thus, when infected these areas must be debrided of dead tissue and bacteria thoroughly. Problematic organisms for wounds tend to form biofilms that will bloom into recurrent infection if not fully removed. 45 Over 90% of chronic wounds harbor bacteria and fungi living in such biofilms, which are hard to penetrate without direct debridement. Clinically, about 50% of chronic wounds would be considered infected.46,47 Treatment oftentimes means the creation of a larger wound and resetting of healing progress that may have been attained before infection. In many scenarios, these debridements can also expose deeper tissues such as tendon or bone, which may necessitate larger reconstructive surgeries to protect these structures.
Oncologic treatment delay
Among other dreaded side effects of chemotherapy are impaired wound healing and immune system suppression. 48 For many cancers, however, chemotherapy is a mainstay of treatment and cannot be avoided. Unfortunately, an open wound may preclude the initiation of chemotherapy out of fear of risking serious infections. In the setting of prior IR, surgical wound healing is impacted, and if prolonged may delay oncologic treatment timelines. In these situations, multidisciplinary discussions take place between surgeons and oncologists to decide on adjuvant chemotherapy timing, with consideration to the specific chemotherapy agents, cancer type, wound characteristics, and overall patient health.
Quality of life
RIF alone has marked impact on patient quality of life, which becomes even more significant when contributing to the development of poorly healed and/or chronic wounds. 49 In these settings, frequent debridements and dressing changes introduce daily pain for patients. Wound pain can become exceedingly difficult to manage and a significant source of suffering for patients. This pain is commonly treated with systemic opioids, particularly during dressing changes, but with wounds in irradiated fields, the need for pain control can become chronic. Dependence, addiction, and tolerance issues aside, studies have also shown that opioid medications are physiologically implicated in slower healing timelines.50,51 While alternative pain control methods are often used to mitigate these risks, the stress response associated with uncontrolled pain is also counterproductive to wound healing. 52 This does not factor in the time cost, frequent clinic visits to multiple practitioners from different disciplines, and family/caretaker help if required. Often, the wounds can preclude patient mobility and function, especially on stiff irradiated tissue, necessitating help with activities of daily living and prolonged absenteeism from work. Ultimately, these combined burdens become incredibly emotionally and financially draining for patients. 53 A validated measure of patient-reported outcomes for chronic wounds, the WOUND-Q, includes a quality-of-life section to directly measure these issues.54,55 This is done by asking patients to rate severity on psychometric scales how their wound impacts independence, relationships, emotional well-being, sleep, feelings of isolation, and much more. As a modular measure, WOUND-Q can be applied to chronic wounds of any etiology by adding other scales specific to a type of wound (e.g., lower extremity). WOUND-Q was found to be the among the highest quality wound-related patient questionnaires in terms of rigor of development and broad applicability, and interestingly, has recently been FDA-qualified as a medical device development tool. 56 In standardizing research and clinical care, it is the premiere patient-reported outcomes measure and should be prioritized.
Key takeaways
Fibro-atrophic tissue changes are largely irreversible, leaving patients reliant on strict wound care. Irradiated wounds heal poorly, are highly infection prone, and can delay critical oncologic treatments such as chemotherapy. These chronic wounds severely impact quality of life through pain, frequent procedures, limited mobility, and emotional and financial strain.
Prevention
While a detailed discussion of radiation-induced skin injury and irradiated wound prevention would be massive in scope, it is important to briefly comment on best practices given the severe risks that these complex wounds pose. These practices focus on mitigating radiation exposure to nontumor tissues, administering general skin care, and vigilantly monitoring skin and wound status to prevent progression. Exposure-mitigation methods include modifications to radiation technique (e.g., volumetric-modulated arc therapy or intensity modulated XRT), dose/frequency (e.g., hypofractionated XRT), or size of the irradiated field (e.g., partial breast IR).57–60 Each strategy has demonstrated improved side effect profiles while conserving efficacy. Patients exposed to radiation should utilize gentle washes and moisturizers, and avoid skin irritants such as friction, sunlight, perfumes, or other chemicals. Topical corticosteroids, bacterial decolonization, dressings, and ointments are additional methods with moderate evidence supporting the prevention of development of radiation-induced skin injury. 61 Given the widespread incidence of radiation-induced skin injury among patients who received XRT, the most important prophylactic measure is early detection and early treatment. Several scoring systems are available that monitor the severity of radiation-induced skin injury by incorporating both physician and patient perspectives. 60 This helps to establish each patient’s unique response to their XRT regimen. Although higher doses are associated with more severe acute and chronic symptoms, different patients can respond differently to the same dose, and skin changes do not always correspond to the degree of underlying tissue injury. 18 These scoring criteria can help monitoring over time and mitigate progression to the complex and chronic irradiated wounds that this review seeks to manage. Furthermore, as discussed below, several of the therapies included in this review have the potential to reverse or mitigate the thought-to-be permanent pathophysiologic changes that contribute to RIF, and thus may hold promise as prophylactic therapeutics as well.
DISCUSSION
The pillars of wound care remain the same for wounds in irradiated fields as they do for any difficult-to-heal wounds. Medical and nutritional optimization, restoration of blood flow, and reducing shear/mechanical forces are paramount. Assuming this optimization is already accounted for, the advances in wound treatment below are promising adjuncts.
Overview
Countless dressings and supplies are available on the market, but most of them still only fulfill the basic requirements: that is to keep a wound clean and protected while the body creates granulation tissue and eventually re-epithelializes. Selecting the appropriate dressing for wounds that are dry, exudative, or infected is imperative to create the ideal, clean environment for the body to heal. The majority of these dressings, however, do not augment the tissue’s regenerative capacity. Importantly, even with the perfect external environment, the pathophysiological changes in irradiated tissues make it very difficult for wounds to heal. Contemporary research has been focused on combating several hallmark RIF-associated tissue characteristics. Namely, self-perpetuating oxidative damage and inflammation, as well as poor oxygen and nutrient delivery following microvascular destruction. The following sections explore the mechanisms driving novel therapies that target these pathways.
Key takeaways
Regardless of wound pathophysiology, wound care best practices should still be used. Promising novel therapies directly target oxidative damage, inflammation, and poor vascularity—hallmarks of RIF that inhibit wound healing.
Dermal substitutes
Innovative biomaterial-based approaches to wound care have emerged in efforts to promote reepithelialization and revascularization, especially for large or complex wounds, when immediate skin grafting is not an option. Successful survival and integration of a skin graft require a wound bed that is clean, noninfected, and provides the nutrients and oxygen for the skin cells to survive and populate the wound. The stages of skin graft survival include initial adherence to a fibrin network that anchors the loose graft, followed by immediate nutrient supply through plasmatic imbibition for 2–3 days before inosculation occurs—the joining of already-established wound bed blood vessels to transferred skin blood vessels. True revascularization occurs around days 4–7, which allows for reliable reepithelialization. 62 During the plasmatic imbibition phase, diffusion of nutrients through plasma and interstitial fluid is limited without a blood pump mechanism, which means the graft survival depends on the timely formation of the new blood vessel network. RIF-afflicted tissues are proinflammatory, hypocellular, and hypovascular, limiting the speed at which these processes can take place. 63
This is where dermal substitutes play a role. Synthetic substitutes such as Biodegradable Temporizing Matrix (BTM), or bioengineered matrices such as Integra (derived from bovine collagen and glycosaminoglycan), are placed on wound beds to promote granulation and blood vessel growth into the matrix and allow for temporary coverage. Over several weeks, the wound is protected and once the matrix is vascularized, the top protective layer of the substitute can be peeled and a skin graft applied. While dermal substitutes are not constrained by the same survival timeline as skin grafts, as no living cells are present in the substitute, its efficacy is still limited by a compromised wound bed. If the irradiated wound cannot initiate neovascularization into the substitute matrix, the substitute itself will not be a suitable skin graft recipient either, no matter how long it has been in place. From a clinical perspective, this can be a useful test. If it fails, the cost of a dermal substitute and several trial weeks is the price, rather than the sacrifice of a skin graft donor site. However, this comparison is not to downplay the cost of these rather expensive supplies, which we discuss in detail in a subsequent section.
Both of the above dermal substitute options provide an impermeable coverage layer in addition to stimulating healing, however, these are only two of the many off-the-shelf substitute options to be utilized with cost, availability, purpose, and wound characteristics in mind. Over 75 dermal substitute options currently exist on the market, and this number is growing rapidly. 64 Acellular dermal matrices (ADMs) or other decellularized tissue products are frequently used for wound coverage, with many designed precisely for this purpose. As the name implies, these products are derived from natural ECM-rich components with their antigenic/cellular products removed in tissue processing steps during manufacturing. These promote dermal regeneration without inciting a host immune response. Fibroblasts, keratinocytes, and endothelial cells can quickly migrate along the established ECM rather than waiting for host ECM production to accelerate blood vessel and dermal growth. With their origin in large surface area burn care, they have been shown to also be useful in reconstructive surgery and wound management. 65 Some notable bovine examples include Integra’s, PriMatrix product, as well as MatriDerm, which is thinner and elastin-containing.66,67 Icelandic company, Kerecis, similarly produces decellularized intact fish skin, which has shown benefit in complicated wounds.68,69 Commonly used in breast reconstruction for implant support, human-derived ADM has also been designed for wound healing, similar to a notable example DermACELL. 70 Although the beneficial properties of these skin substitutes are well-established for chronic or complex wounds, the literature is lacking in the use for RIF-related wounds. 71 Several case reports and series reveal excellent reconstructive outcomes using dermal substitutes for enhanced skin graft take on irradiated surfaces, or nonirradiated wound beds that then go on to survive adjuvant XRT.72–74 Since more products are hitting the shelves and reconstructive surgeons are using them more frequently, we expect to see high-quality prospective studies validating their direct applicability in the near future.
Key takeaways
Dermal substitutes are off-the-shelf products that promote granulation and vascularization and can be used to temporize very large wounds. Meta-analyses of randomized controlled trials have demonstrated that dermal substitutes are effective for healing burns and chronic wounds, with Oxford Center for Evidence-Based Medicine: Evidence Level Ia. For the treatment of irradiated wounds specifically, dermal substitutes are classified as Evidence Level 4 as only case series publications are available.
Placental-derived materials
While traditional dressings or dermal substitutes serve to protect healing wounds and create a suitable environment for ingrowth of granulation tissue, they do not directly modulate the healing process. Wound care materials that are derived from placental tissues (e.g., amnion, chorion, umbilical cord), however, have proven beneficial for the treatment of chronic wounds by augmenting the healing response. Each placental-derived tissue has unique regenerative properties. For example, placental membranes function as excellent ECM scaffolds, owing to high concentrations of collagens, fibronectin, laminin, and other glycoproteins. Amniotic fluid is high in growth factors and hyaluronic acid and has utility as a near-native injectable product. Umbilical cord has high concentrations of regenerative growth factors, enabling cellular components to be highly responsive to manipulation or compression in utero. The placental disc’s high concentration of mesenchymal stem cells (MSCs), fibroblasts, and trophoblasts secretes angiogenic and antimicrobial substances. Numerous preparations of these tissues have been explored, including sheets, powders, injectables, or near-native grafts. Importantly, placental-derived tissues are immune privileged, which mitigates immunogenicity and can even eliminate the need for decellularization75,76 (Fig. 3).
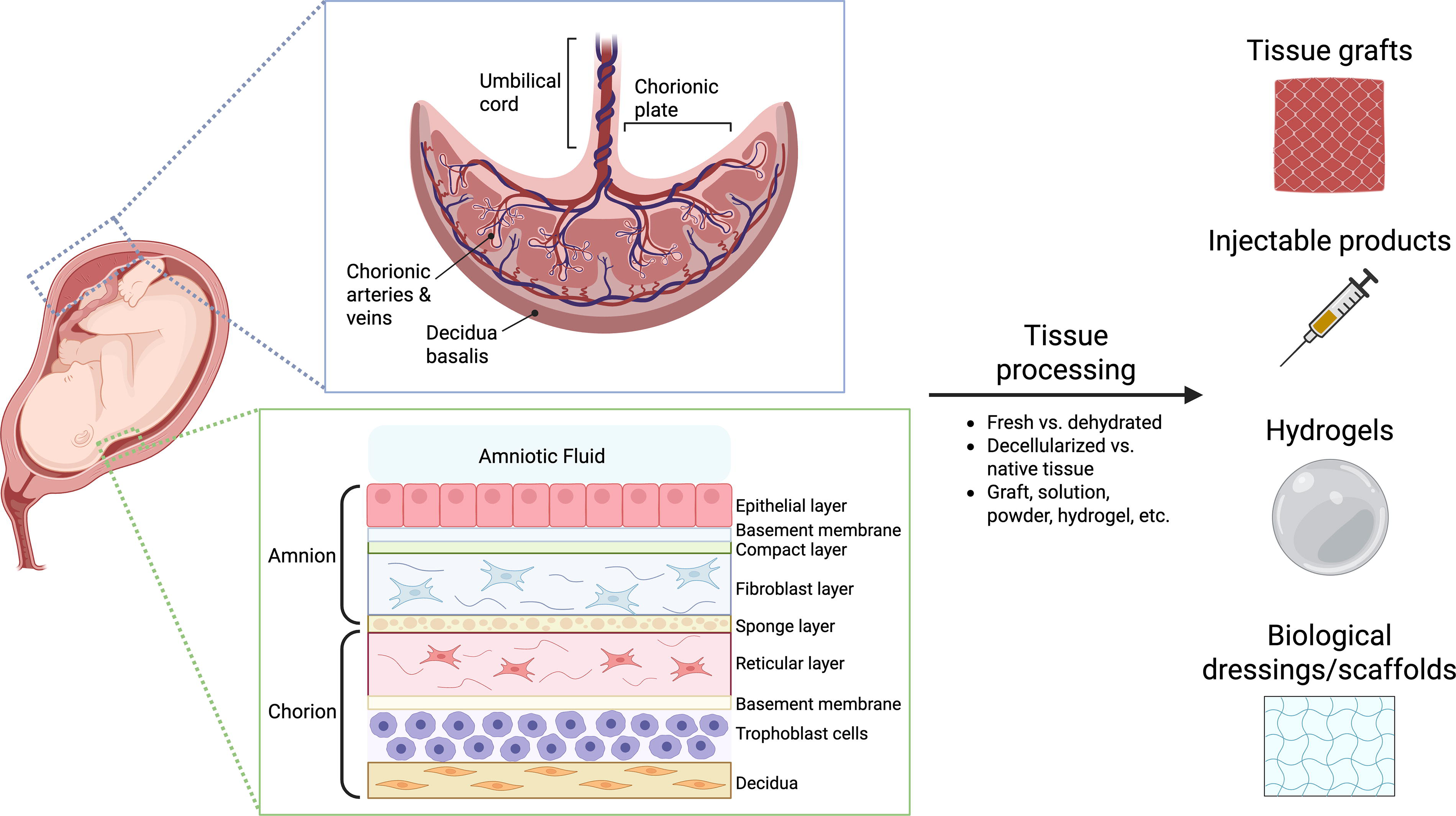
Applications of placental-derived tissues. Placental-derived tissues have growing applications in regenerative medicine, including in the setting of irradiated chronic wounds. Each tissue hosts a distinct composition of cells, extracellular matrix (ECM) components, and growth factors that offer unique regenerative potential. These tissues can be prepared in numerous configurations that enable use as grafts, dressings, injectables, etc. across several pathological states.
These versatile characteristics enable the use of placental tissues across a vast range of pathologies, including diabetic wounds, pressure ulcers, burns, and RIF-associated wounds. Well studied in complex chronic wounds, they have been shown to have a very positive safety profile. 77 In a recent review of the literature, Protzman et al. found that randomized control trials revealed an increased closure rate of complex wounds when utilizing these biomaterials compared with standard of care. Impressively, venous leg ulcer and diabetic foot ulcer studies showed between 27% and 95% wound closure along their experimental timelines (4–12 weeks), with most >50%. 77 Expectedly, there was much heterogeneity among materials and patient populations, which may limit the generalization of results. In addition, the focus was on diabetic foot ulcers and lower extremity venous stasis ulcers, which follow some similar pathogenic processes but also differ considerably from RIF-related wounds. Relating specifically to RIF, animal irradiated wound studies and human case reports reveal similar outcomes. Several rat studies have shown significantly faster closure rates with both decellularized and cell-preserved placental tissues. Brunchukov et al. found that an intradermal injection of a concentrate of placental-derived MSC-conditioned medium resulted in a 6.7-fold decrease in wound area on day 112; Kakabadze et al. developed a decellularized amniotic membrane dressing that accelerated irradiated wound healing 2.5-fold; and Sun et al. found topical Wharton’s jelly-derived MSC-conditioned medium hydrogels produced 3.38-fold smaller wounds at 6 weeks, with complete healing at 8 weeks, which none of the control animals achieved.78–80 Likewise, Regulski et al. successfully healed a human patient’s chronic ankle wound in an irradiated field using lyopreserved allograft with viable stem cells. 81 Two other case reports demonstrated that amniotic membranes promoted reepithelialization in nonhealing irradiated nasal and skull wounds.82,83 More human trials examining the efficacy of placental tissue-derived materials are required for RIF-related wounds. Given the promising preclinical results and adjacent chronic wound case-report uses in humans, this is shaping up to be a highly encouraging treatment modality.
Key takeaways
Placental-derived materials enhance healing by providing proregenerative cells, growth factors, and ECM architecture. Diverse tissue types, low immunogenicity, and adaptable formulations enable numerous applications for irradiated wounds. Multiple randomized controlled trials have demonstrated that placental-derived materials are effective for diabetic and venous ulcers, with Oxford Center for Evidence-Based Medicine: Evidence Level Ib. However, for the treatment of irradiated wounds, they are presently classified as Evidence Level V given that only case reports and preclinical data exist, emphasizing the need for more clinical trials.
Fibronectin
Fibronectin is an extracellular glycoprotein that plays a pivotal role in ECM remodeling and cell migration. These actions are of particular importance for the skin’s natural healing mechanisms, especially in the inflammatory and proliferative phases of wound healing. 84 Fibronectin secretion by fibroblasts acts as a temporary extracellular scaffold, and is a key element of granulation tissue formation and keratinocyte migration 85 (Fig. 4). These mechanisms are severely dysregulated in RIF, and several recent studies have investigated fibronectin’s role in wounds on an irradiated field. In analyzing normal and radiation-injured skin, Johnson et al. found fibronectin to be downregulated in patient samples treated with radiation. 86 Subsequent studies by the same group on irradiated mouse skin found accelerated wound healing following topical fibronectin application (wound area at 2 weeks was 45% for control mice vs. 29% for fibronectin mice, and wound area at 3 weeks was 9% for control mice vs. 3% for fibronectin mice). In an additional follow-up study by Raghuram et al., sustained fibronectin release from a hydrogel similarly improved wound healing speeds in a porcine model (wound area at 3 weeks was 21% for control pigs vs. 4% for fibronectin pigs, and wound area at 4 weeks was 6% for control pigs vs. fully healed for fibronectin pigs). 87 Fibronectin treatment in these studies downregulated SMAD3 and TGF-β, which are both known proinflammatory mediators associated with RIF. The translation of these findings into human trials may provide effective dressings for patients with these difficult-to-treat chronic wounds, by recreating the absent initial wound healing scaffold and setting the tissue on the right path. Unlike placental-derived materials or dermal substitutes, however, there has not yet been substantial study into similar wound models that may provide hints as to its clinical efficacy.
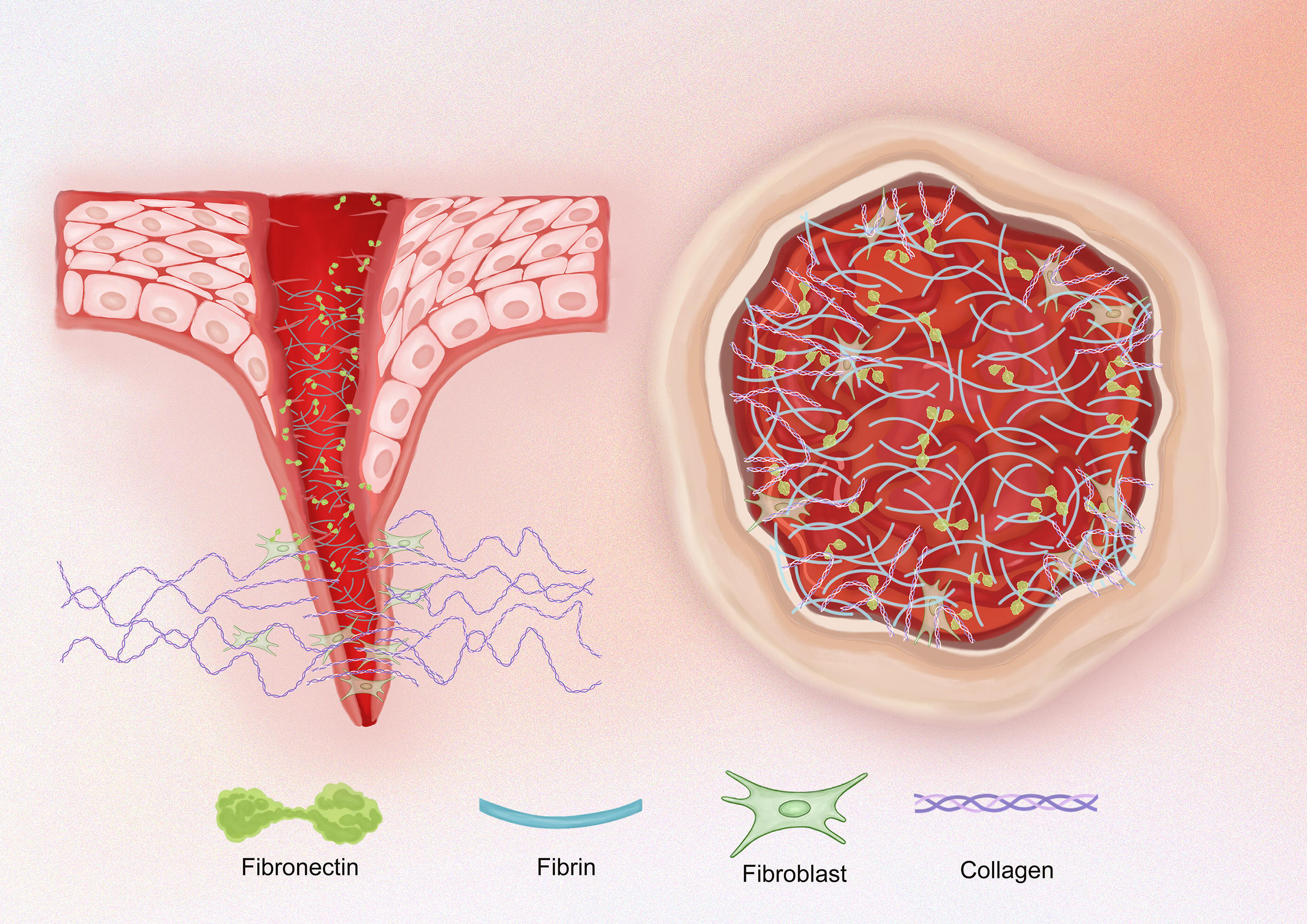
Fibronectin. In the early phases of wound healing, temporary fibrin-fibronectin scaffolds allow for integrin binding. This mediates cell migration, inducing new epithelium and fibroblasts that produce collagen and other extracellular matrix (ECM) proteins to create a more permanent scaffold for wound closure.
Key takeaways
Fibronectin, a key component of ECM scaffolding, is downregulated in RIF. Topical application shows promise by restoring this scaffold function in the early phases of wound healing. Preliminary evidence also supports anti-inflammatory effects. While numerous animal studies demonstrate promising efficacy, the lack of in-human trials characterizes fibronectin as Oxford Centre for Evidence-Based Medicine: Evidence Level V for the treatment of irradiated wounds.
Adipose- and plasma-derived injectable therapies
Autologous fat grafts have proven successful in combating RIF tissue changes and RIF-related wounds. 88 Fat transplantation into the fibrotic tissues helps to create an environment that reduces long-term inflammation and the buildup of disorganized collagen. 89 As opposed to the mature adipocytes that make up the majority of fat graft volume, adipose-derived stem/stromal cells (ADSCs) have been shown to be central players in this regenerative process. These cells play a crucial role in promoting angiogenesis and adipogenesis by secreting growth factors and their own ECM components. ADSCs support tissue repair, enhance antiapoptotic activity, alleviate anoxia, and help prevent the sequelae of RIF.90,91 Fat grafts that are augmented to contain higher levels of ADSCs have been shown to be even more efficacious. 92 The stromal vascular fraction (SVF) can be isolated when lipoaspirate is centrifuged. This SVF layer, denser than the adipocytes and aqueous layers, contains proregenerative, heterogeneous cell populations that comprised ADSCs, pericytes, fibroblasts, endothelial cells, etc. (Fig. 5). Introduction of SVF into irradiated tissue has been shown to promote angiogenesis by vascular endothelial growth factor (VEGF) expression, thereby accelerating wound healing, reducing pain, and lowering the risk of wound recurrence. 93 Yu et al. corroborated similar outcomes in human patients and also in an experimental rat model in which SVF versus saline injections were compared (SVF cell suspension injections improved semiqualitative skin injury scores [1–5] longitudinally between 12 and 60 days post-IR on their animal subjects). 94
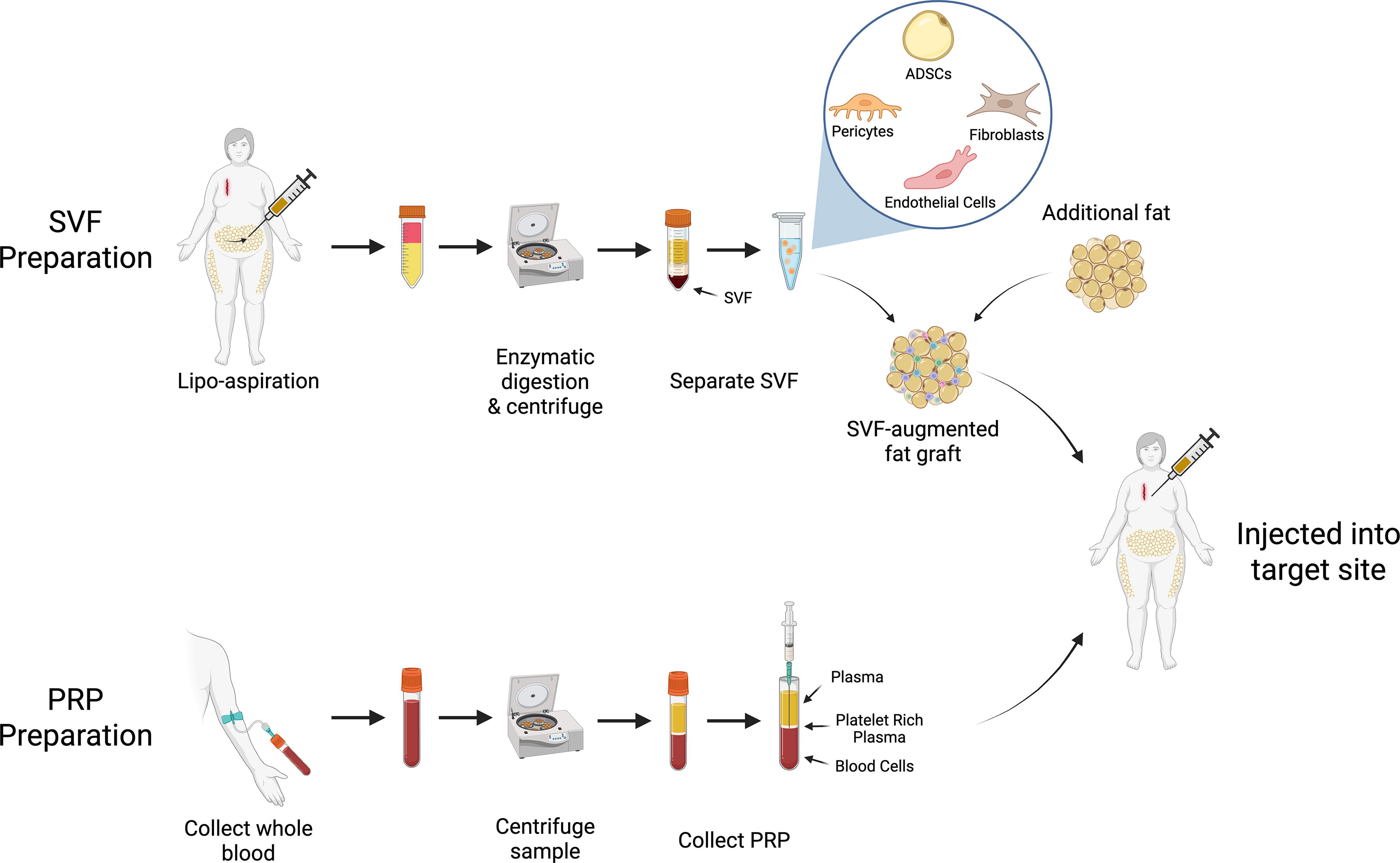
Adipose- and plasma-derived injectable therapies. The stromal vascular fraction (SVF) of lipoaspirate after centrifugation is particularly rich in adipose-derived stem/stromal cells (ADSCs) and other mesenchymal and endothelial progenitors. The augmentation of fat grafts with SVF improves the retention and local tissue conditioning properties of the grafts. Similarly, platelet-rich plasma (PRP), which is a spin-down product of whole blood, is rich in growth factors that promote tissue growth and regeneration.
Decellularized adipose matrices (DAMs), such as Renuva, offer a promising alternative for patients with irradiated skin, particularly those lacking sufficient donor fat for autologous grafting. Among cancer patients, cachexia and loss of overall body fat are common. Off-the-shelf DAMs are made from human donor fat and are readily available for use. As their name suggests, human adipose tissue is processed by techniques that decellularize the material but retains the ECM structural components as well as growth factors and signaling molecules. This is then safe for injection without provoking an immune response. Acting as scaffolds for new adipose tissue, DAMs support adipogenesis, enhance vascularity, and reduce inflammation in damaged tissue. Similar to fat grafts, they can help to mitigate RIF, although typically to a lesser degree, yet have the added advantage of not requiring donor tissue from the patient. 95
Platelet-rich plasma (PRP) is another injectable treatment for RIF-related wounds. Similar in principle to isolating the SVF in fat grafting, PRP is a spin-down product derived from the patient’s own blood. The blood is processed mechanically to concentrate platelets to levels higher than normal, then the resulting solution is injected into the affected tissue. PRP is rich in cytokines, VEGF, and platelet-derived growth factor, all of which play crucial roles in tissue repair and regeneration. 96 It has been shown to have a positive effect on chronic wounds in the clinical setting, with numerous studies reporting faster healing times and smaller wound sizes compared with traditional wound care alone. 97 Recent preclinical literature suggests that injecting PRP into irradiated wounds follows suit. Lee et al. examined PRP’s effect on an irradiated dorsal mouse skin model, finding that wound closure was accelerated, in part, due to an upregulation of the AKT signaling pathway (PRP-injected irradiated wounds were an increasingly smaller area than control irradiated wounds over the 4-week study period; ∼25% smaller at week 2, and ∼45% smaller and almost fully healed at week 4). 98 This pathway is well known as being responsible for promoting cell survival and proliferation, which is helpful in the wound environment, but also relevant as a possible inhibition target in oncologic treatment. 99
Key takeaways
ADSCs, growth factors, and ECM components found in fat grafts promote cellular proliferation and angiogenesis; these characteristics can be amplified via SVF or ADSC enhancement. Decellularized adipose matrices provide off-the-shelf benefit similar to fat grafts, albeit less potent, but without the need to harvest patient donor tissue. PRP injections deliver proregenerative cytokines that promote cell survival and cell growth pathways, resulting in more rapid wound closure. Fat grafting for the treatment of RIF associated tissue changes and irradiated wounds is supported by several prospective cohort studies, yielding an Oxford Centre for Evidence-Based Medicine: Evidence Level IIb; however, evidence supporting adipose- and plasma-derived injectable therapies are limited to case reports and preclinical studies.
Hyperbaric oxygen therapy
Hyperbaric oxygen therapy (HBOT) is a treatment in which patients enter a pressure chamber for 1–2 h several times per week, during which they are breathing 100% oxygen under 2–3× normal atmosphere pressure to improve oxygen delivery to tissues that are hypovascular (Fig. 6). HBOT has been used routinely in maxillofacial reconstruction since the 1980s to help prevent infection in the setting of osteoradionecrosis (ORN) and chronically exposed bone. With the introduction of directed XRT for the treatment of head and neck tumors, more patients were surviving long enough to experience these ORN complications, especially following reconstruction. 100 With improvements in bone healing and decreased bacterial load due to enhanced oxygen delivery to healing tissues, it was only several years later that reconstructive surgeons also began trialing HBOT for soft tissue RIF of the head and neck. Parallelling this, HBOT was also making a name for itself for diabetic wound treatment, and it was a logical application for the therapy given similar microvascular issues seen in diabetic and irradiated wounds. Initially expensive and inaccessible outside of specialty centers, HBOT is now FDA cleared for delayed radiation injury, diabetic wounds, and burns. 101 Regarding its effects on late radiation tissue injury, HBOT literature is promising, but limited. Both a 2017 systematic review and a 2023 updated Cochrane review revealed that HBOT trials show positive results for skin necrosis and prevention of complications following XRT and surgery, although the trials reviewed were small in number and deemed low-to-moderate levels of evidence.102,103 Interest is high regarding the effects of HBOT on wound healing in irradiated fields, with ongoing clinical trials in this field. 104

Hyperbaric oxygen therapy (HBOT) chamber. HBOT is FDA approved for the treatment of delayed radiation injury, diabetic wounds, and burns. Hyperbaric oxygen increases tissue oxygenation, which promotes wound healing and mitigates radiation therapy (XRT) complications. Modern pressure chambers are transparent and comfortable, as treatments or “dives” typically last 1–2 h. Author Chris can be seen enjoying a trial of what patients experience during a dive. Given the fire risk with pure oxygen gas, all metals and devices, including glasses and belts, are removed and patients wear a hospital-style gown during a real dive. Courtesy of Dr. Joshua Korman at his Los Altos, CA office.
Key takeaways
Following long-term use in the osteoradionecrosis and diabetic wound treatment, HBOT is FDA cleared for late radiation-induced soft tissue injury, including that of the skin. HBOT improves oxygenation to healing tissues and reduces hypoxia-driven inflammation. HBOT for the treatment of radiation-induced skin necrosis is characterized as Oxford Centre for Evidence-Based Medicine: Evidence Level IIb given positive cohort studies, though randomized controlled trials specific to irradiated wound healing are necessary.
Deferoxamine
Deferoxamine (DFO) is an iron chelator that was originally FDA approved in the 1960s for systemic iron overload. The human body has no efficient, direct means of excreting iron. Some loss occurs with bleeding, shedding of stored ferritin in intestinal cells, and through blood breakdown products in urine. Its regulation is centered on the rate of uptake from the gastrointestinal system, controlled by a feedback loop involving the hormone hepcidin.105,106 Iron chelation is thus necessary to prevent toxic blood iron concentrations in cases of acute ingestion or states of chronic overload such as hemochromatosis or transfusion-dependent anemias (e.g., sickle cell disease, thalassemia, myelodysplastic syndromes). DFO plays an essential role in iron clearance in these disease states. It acts to chelate plasmatic and cellular free iron, allowing it to be excreted in urine and bile. It does not exert this chelating effect on iron that is already bound to hemoglobin, cytochromes, or other essential enzymes.
Small-animal RIF and chronic wound models have evaluated DFO for local skin conditioning to promote wound healing. This was a recent advent, as DFO, similar to other bulky, hydrophilic molecules, cannot penetrate the hydrophobic outer layer of skin. Studies were possible due to an advancement in transdermal drug delivery. A reverse micelle system in which DFO is packaged with a stabilizing polymer, polyvinylpyrrolidone, within the hydrophilic center of a bipolar construct. These envelopes can penetrate through the epidermis into the dermis where they dissolve and release the DFO to enact its effects 107 (Fig. 7).
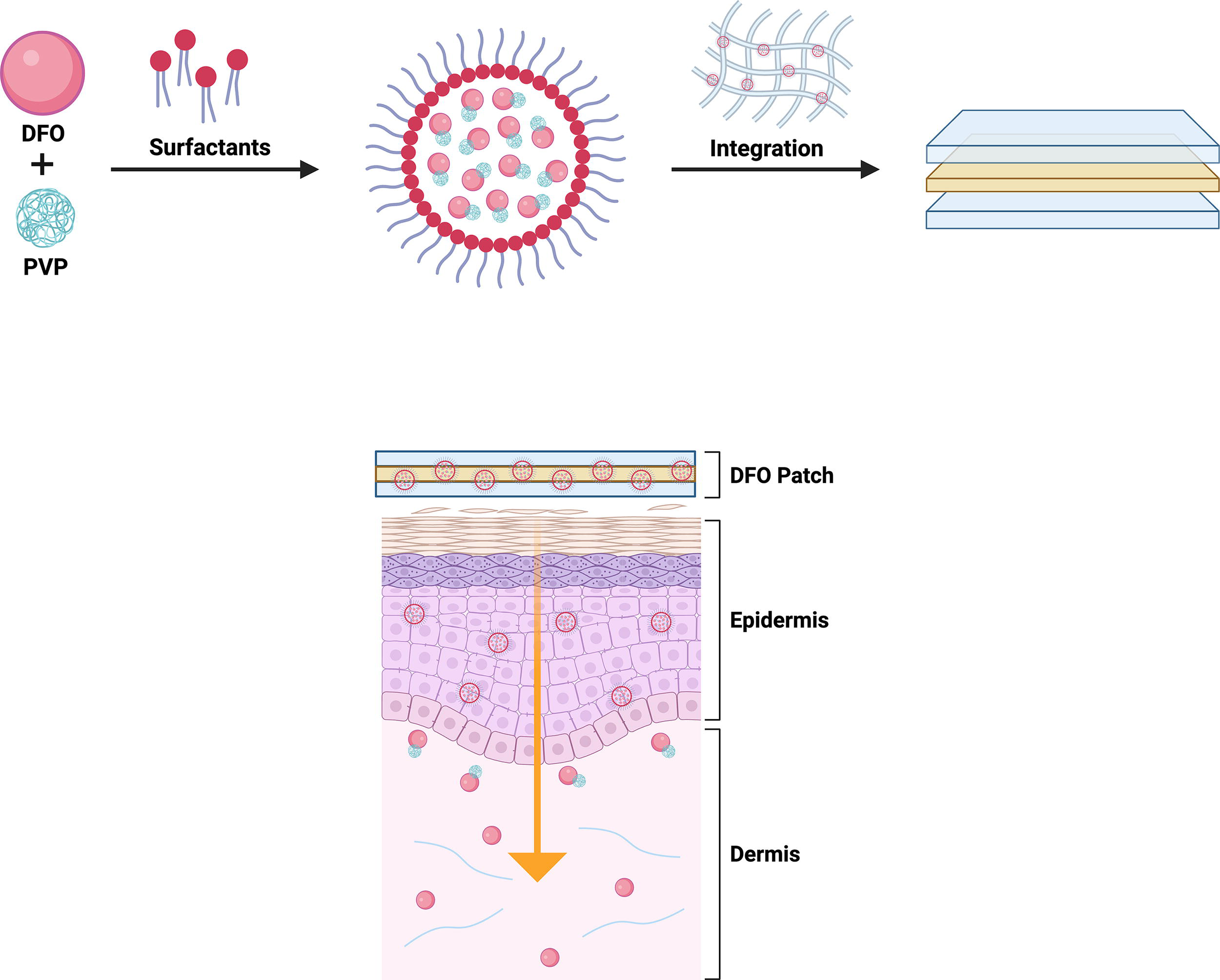
Deferoxamine (DFO) reverses micelle transdermal delivery system. DFO is a large, hydrophilic molecule. Under normal circumstances, it would not be able to penetrate the protective hydrophobic outer layer of skin, the stratum corneum. DFO forms a complex with a stabilizing polymer polyvinylpyrrolidone, which is then packaged in surfactant-based reverse micelles. This transdermal delivery system allows DFO to diffuse through the stratum corneum and enact its effects in the aqueous dermal environment. These reverse micelles are stabilized in patch or cream formulations.
Interestingly, the iron chelation action of DFO plays into several mechanisms that are beneficial for conditioning of fibrotic skin. The two most pertinent pathways are related to its direct effect on ROS mitigation and the upregulation of angiogenesis. As detailed above, ferroptosis is dependent on free labile iron in the tissues to catalyze an ROS chain reaction. Thus, DFO’s removal of the catalyst helps to decrease the vicious inflammatory cycle that contributes to chronic wound healing issues in irradiated skin. In addition, the chelation of iron induces new blood vessel growth. This occurs because iron is a necessary cofactor for prolyl hydroxylase, an enzyme that degrades hypoxia inducible factor-1ɑ (HIF-1ɑ). As HIF-1ɑ’s name implies, this transcription factor activates proangiogenic genes in response to low oxygen environments, that is, microvascular destruction and decreased oxygen delivery to the skin. 108 These upregulated gene transcripts include VEGF and other growth signaling molecules. With new blood vessel growth, increased oxygen and nutrient delivery, chronically wounded skin is shifted toward a more healing-centric milieu.
Building on prior research investigating injected and topical DFO for the mitigation of radiation dermatitis, Lintel et al. and Berry et al. tested DFO’s effects specifically on wounds in an irradiated field.26,109,110 These preclinical studies from 2022 to 2024 revealed that topical DFO accelerated the healing time of wounds on mouse skin that was in the chronic phase of RIF (Lintel et al. revealed that at 2 weeks wounds on normal mouse skin were fully healed, while irradiated skin was still 19% open and DFO-patch-treated irradiated skin was 10% open, and fewer DFO-treated mice were left with nonhealing wounds when compared with the DFO-treated irradiated control mice; Berry et al. found DFO-cream-treated irradiated wounds healed on day 17, while nontreated irradiated wounds healed on day 23).
DFO skin conditioning research has produced potent outcomes in the preclinical setting. For this specific RIF wound healing purpose, however, large-animal studies and clinical validation are necessary. 111 That being said, recent uses of DFO patch treatment on a small number of human patients have demonstrated promising results. These patches have been granted FDA orphan drug designation for Perrault et al. presented the first use of topical DFO on a human subject with transfusion-dependent anemia secondary to hereditary beta-thalassemia. 112 This patient developed a chronic, painful wound on the skin overlying the ankle’s bony prominence, which was present for an entire year before DFO application. With daily patch treatment, the wound was fully healed after 21 weeks with an improvement in local skin quality, and a notably decreased hemosiderin pigmentation. In a subsequent report using the same DFO patch on an irradiated breast wound present for 5 months, 2 weeks of DFO treatment also promoted wound healing 113 (Fig. 8). With these results and a benign safety profile, excitement is brewing for a wider scale human patient experimentation.
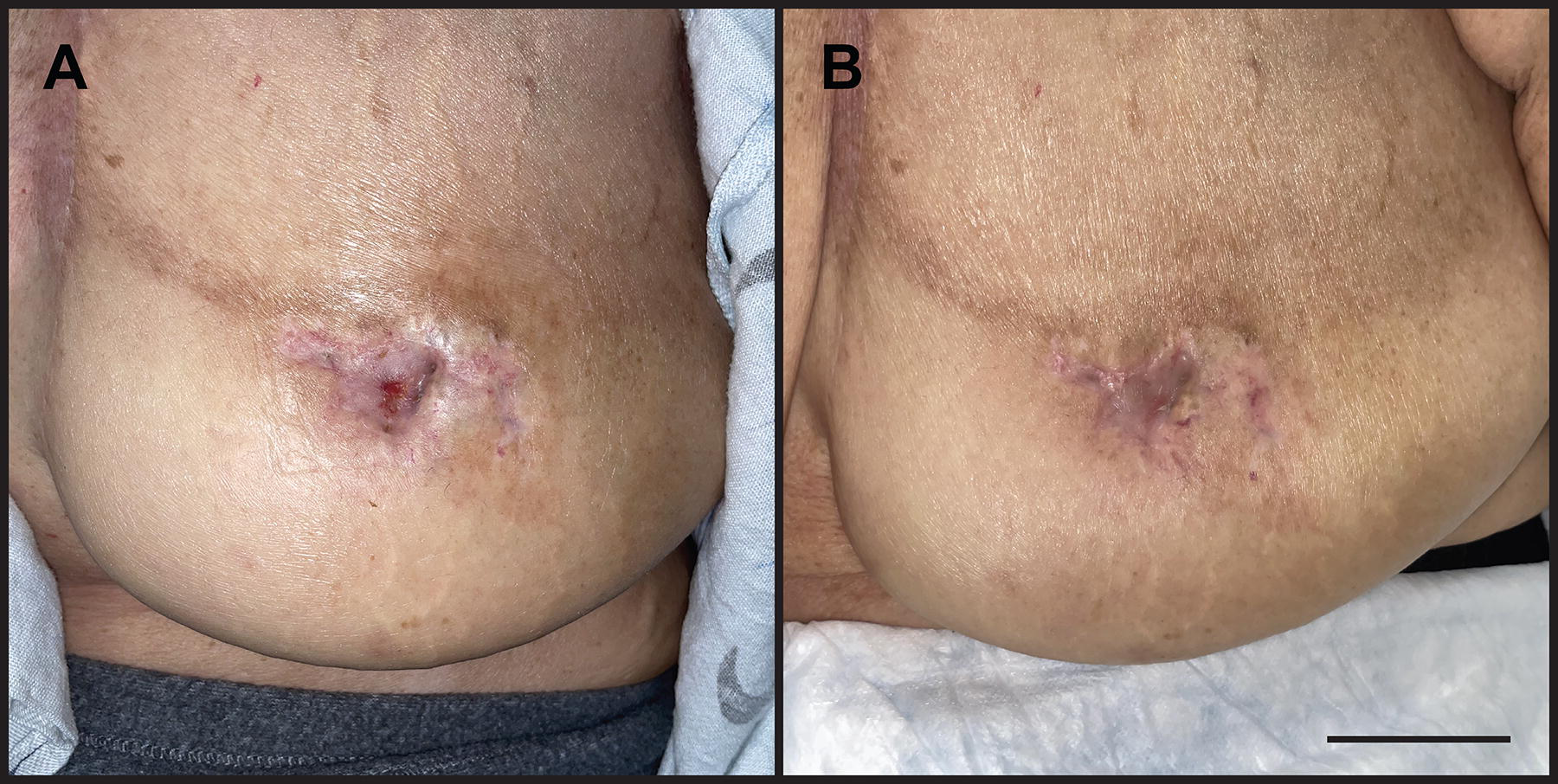
Irradiated wound healing with deferoxamine (DFO) patch. Demonstration of a chronic wound on an irradiated, reconstructed breast.
As we know, it is far easier to avoid a wound than it is to heal a wound. Prior experiments have demonstrated a difference in the efficacy of DFO skin conditioning based on the timing of administration. 29 The most effective treatment course for RIF, measured by blood flow, skin elasticity, and histology, was one that attempted to precondition skin before the chronic phase of RIF, rather than rescue an already-fibrotic skin. Therefore, prophylactic administration before XRT, and perhaps during XRT, is likely to be more beneficial in avoiding wounds. If DFO proves to be safe in these settings without influencing the XRT treatments themselves, it is reasonable to assume that earlier treatment will be better. Despite the excitement and safety profile, however, the current published literature is limited and randomized clinical trials in human patients must be performed before DFO’s efficacy is validated for wound healing in this setting.
Key takeaways
DFO targets multiple pathophysiologies of RIF including ferroptosis, microvascular injury, and persistent inflammation. Animal studies demonstrate DFO’s efficacy in both wound healing and prevention of RIF associated wounds. Despite promising results in animal studies and human case reports, widespread clinical trials are limited, thus DFO’s Oxford Centre for Evidence-Based Medicine Evidence Level is characterized as V for the management of irradiated wounds and their prophylaxis.
Tissue transfer
Plastic surgeons are familiar with the “reconstructive ladder” analogy as a way to introduce wound healing/coverage techniques (Fig. 9). Lower rungs of the ladder are simpler and well tolerated. Unfortunately, for the same reasons that a chronic wound will not heal in an irradiated field, the lower rungs of our ladder are sometimes not viable options for coverage of these wounds. Even despite best wound care practices (e.g., keeping the wound clean, selecting appropriate dressings, timely dressing changes, monitoring for infection), irradiated wounds may fail to heal by secondary intention alone as evidenced by comparative studies in the prior subsections. Furthermore, excising a wound and bringing the new skin edges together may create another nonhealing wound. Recall that the fibro-atrophic skin changes impact the elasticity and pliability of the whole area that was irradiated in addition to decreasing healing potential. This problem is particularly salient when skin closure must involve the irradiated area. Depending on body location, tumor type, and radiation regimen, postoperative dehiscence or wound complication rates following primary closure can range from 4% to 50%. Large resections and areas of high tension, pressure, and moisture are already prone to dehiscence. In examining limb sarcoma resection, O’Sullivan et al found that wound complication rates following primary closures differed, whether XRT was administered pre- or postoperatively (34% vs. 19%, respectively). 114 This range is supported by Wilke et al who observed wound complications in 47% of patients who underwent preoperative XRT versus 26% in patients who did not undergo XRT. 115 Similarly, Miyazaki et al reported preoperative XRT as a significant risk factor for midline back incision dehiscence, observing a 26% dehiscence rate in their population. 116 Fortunately, more common procedures such as breast surgery, for example, mastectomy and implant-based reconstruction, carry lower dehiscence/wound complication rates. Studies find dehiscence and implant exposure rates around 4–15% in prior irradiated tissues versus 0.2–2% in nonirradiated fields.117,118 With regard to tissue expansion, particularly for breast reconstruction, there is much debate surrounding its safety in irradiated fields as well as the timing of expansion relative to XRT. If the patient favors implant-based reconstruction over autologous reconstruction, many surgeons opt to place tissue expanders at the time of mastectomy as a placeholder for subsequent implants. The rationale behind this is to allow for gradual expansion without compromising the thin remaining breast envelope, and to allow XRT to affect the expander instead of a final implant or autologous flap. If issues such as dehiscence and extrusion are to occur, it is happening in the setting of a temporary placeholder, which needs to be swapped anyway. Interestingly and contradicting this logic, however, Nava et al found a reconstructive failure rate of 40% (prosthesis removal or conversion to autologous flap) when expanders were irradiated, versus 6.4% when permanent implants were irradiated. 119 Berry et al report an overall complication rate in tissue expander/implant reconstruction to be 45% in irradiated breasts, increased from 21% in nonirradiated breasts. 120 This showcases the need for further investigation on the safety and timing of tissue expander placement. As discussed, skin grafts also require a healthy wound bed to adhere and grow. Historically, skin grafts suffered an abysmal complication rate in irradiated fields, with studies citing partial or total graft loss rates from 40% to 100%.121,122 More recent advances, such as the wound vac, which helps to stabilize the graft and prevent mechanical shear force, have led to improved outcomes with partial or total loss rates closer to 30%. 123 Even so, this is still greater than nonirradiated wound bed graft loss rates in other traditionally difficult wound-coverage scenarios, such as burns, lower extremity wounds, or necrotizing soft tissue infection debridement coverage.124–126
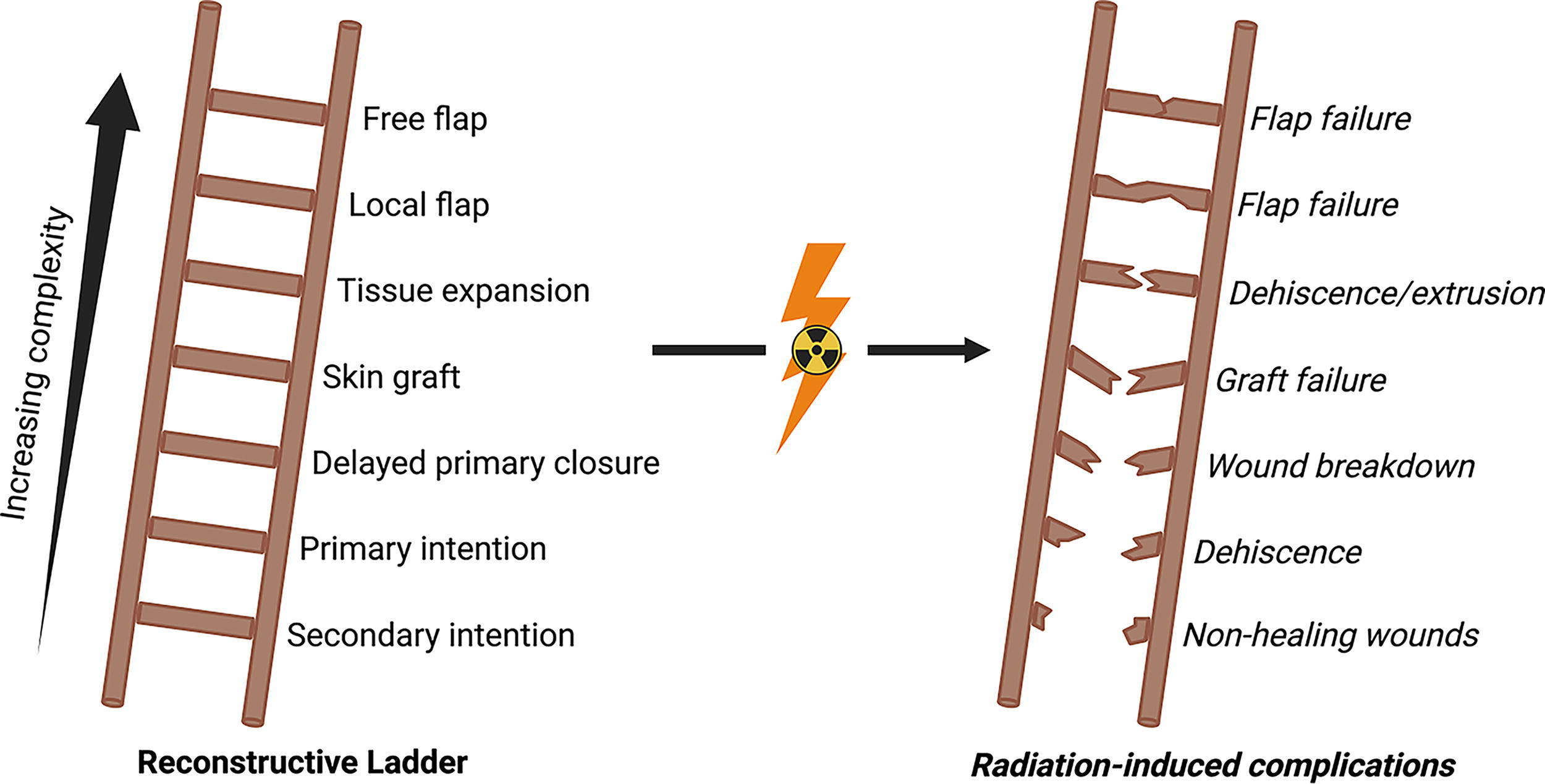
Reconstructive ladder. The reconstructive ladder is a concept in plastic and reconstructive surgery that demonstrates wound closure techniques of increasing complexity. In the case of radiation-induced fibrosis, however, tissue hypocellularity, microvascular destruction, and other fibro-atrophic changes oftentimes impact the healing potential of the tissue. This can preclude the use of simpler procedures such as skin grafting or allowing wounds to heal primarily, secondarily, or through delayed primary closure. As a result, reconstructive surgeons may choose to seek more creative options with significant donor-site morbidity. Even so, tissue expansion and flap reconstruction are more technically challenging and associated with worse outcomes when compared with the same surgeries in nonirradiated tissue. Thus, clinical decision making regarding reconstructive approach and timeline must be approached thoughtfully. All rungs of our reconstructive ladder are undoubtedly affected; however, we hope that the therapies highlighted in this review will help to restore simpler options as reasonable wound healing methods for patients who may not have been candidates for them previously.
Generally saved as final options for most wounds, surgical tissue rearrangement can be effective and quick-healing relative to prolonged wound care for chronic wounds in irradiated fields.127–129 These surgeries involve borrowing skin, fat, muscle, or even bone from other areas on the body, termed a “flap,” and using that flap to replace some or all of the fibro-atrophic tissue. Depending on the affected body part, this can be a local or regional flap, or even a “free flap” from a distant site. The common theme between these options is that they are nonirradiated healthy tissues and bring their own blood supply. Local flaps are rotated or advanced into the wound site, while free flaps are carefully dissected away from their native location with their artery and vein intact, to be joined to recipient vessels near the wound site (Fig. 10). Thus with a robust blood supply, the transferred tissue replaces the wounded area and can heal properly. Oftentimes the irradiated field is much wider than the wounded area, however. This can severely impact the quality of the surrounding tissues, which will negatively influence the healing of any new surgical wound edges unless a very wide area is excised. In addition, this irradiated area may include the blood vessels that surgeons would expect to use as their free flap recipient vessels. In these circumstances, more nuanced decision making is necessary. Local flaps from larger or less immediately adjacent donor sites may be more responsible choices. Similarly, free flap anastomosis to irradiated recipient vessels increases flap loss, as the vessels also undergo fibrotic changes if they are not already obliterated. 130 In addition, unless the recipient vessels are grossly fibrotic, calcified, or diminutive, intraoperative findings do not necessarily predict flap survival outcomes. Histo- and morphological studies have revealed that some differences, namely vessel caliber, may predict outcomes, although these would be hard to translate to the operating room since surgeons are already wary of donor–recipient vessel size mismatches and particularly large/small vessels regardless of XRT history.131,132 Thus, anastomosis to more distant healthy vessels is sometimes required, but more technically demanding. The surgeon must either achieve greater pedicle length on the flap (i.e., the length of the artery and vein harvested with the flap), or if the pedicle cannot be harvested long enough, an AV (arteriovenous) loop can be established. 133 An AV loop is performed by harvesting a long, expendable vein (usually the great saphenous vein from the medial leg) and connecting the vein to the distant nonirradiated recipient artery and vein. This creates a long loop that shunts arterial blood through the graft, directly into the recipient vein. After some maturation time, the AV loop graft itself can be divided and the first half used as the recipient “artery” and second half used as the recipient “vein” to which the flap’s artery and vein are connected. This is a creative way to provide more distant blood flow to support a free flap, avoiding the use of nearby irradiated vessels, however, doubles the number of anastomosis needed and sacrifices a vein commonly used for other procedures such as cardiac bypass. Vessel anastomosis for free flap reconstruction is on the order of millimeters, requiring significant technical ability achieved over years of microsurgical training. Additional surgical complexity is not to be taken lightly. Furthermore, XRT has been shown to increase local flap and free flap complications, including flap failure. 134 When dealing with these high-risk surgical sites, discussions with radiation oncology are warranted during preoperative planning. Full knowledge of the XRT treatment plan to understand the extent of the irradiated field, as well as the expected tissue quality if not yet in the chronic phase, is paramount to surgical planning.
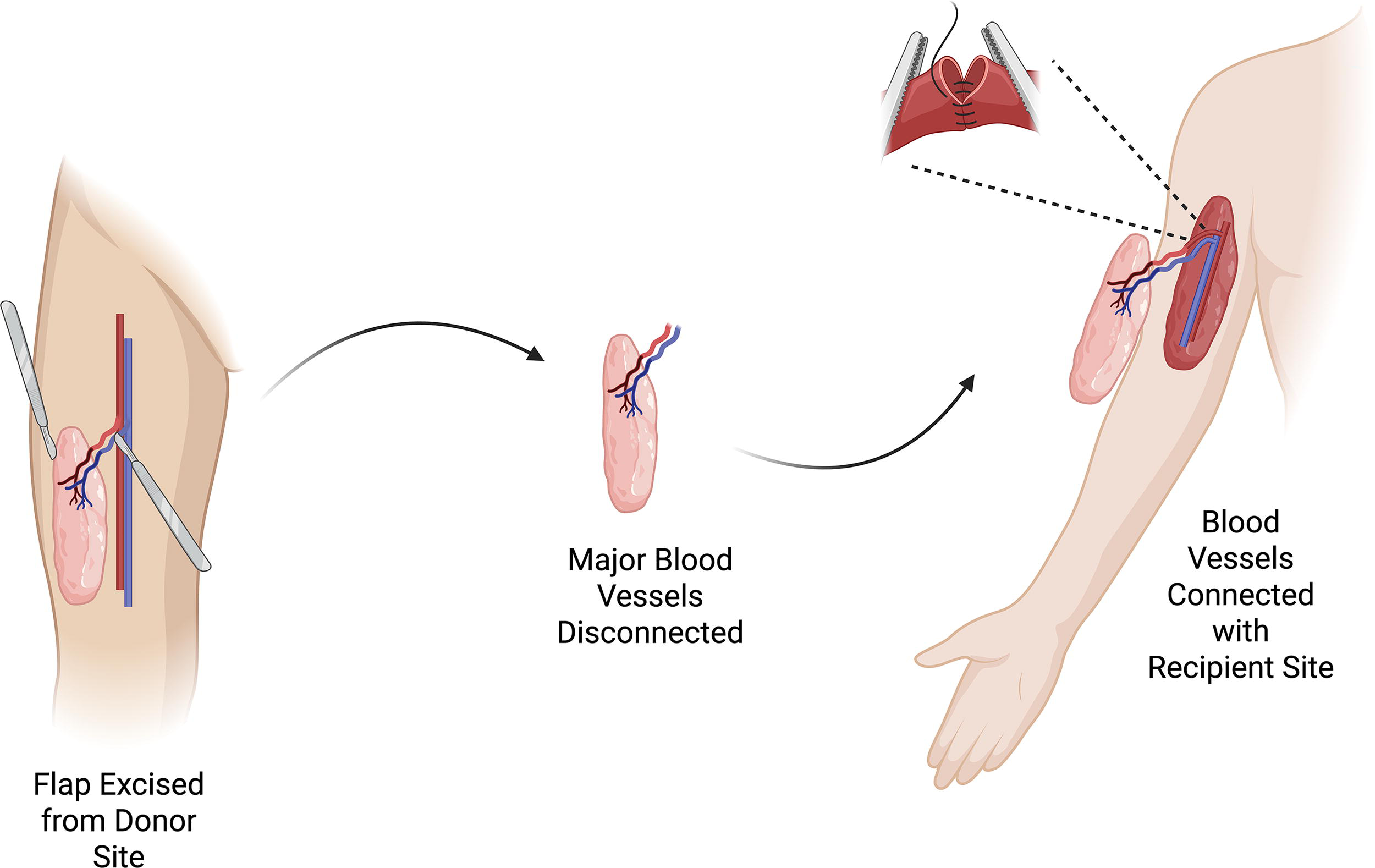
Free flap diagram. Free flaps are distant tissue transfer techniques where autologous donor tissue is excised and transplanted to repair a defect. Unlike skin grafts, free flaps carry their own vascular supply, which is then anastomosed at the recipient site. Free flaps can include any combination of tissue from the donor site (e.g., skin, fascia, muscle, fat, bone, nerve), which enables repair of large and/or complex defects.
Many flaps are described but reconstructive surgeons are tasked with choosing the most appropriate. These are classified by location, size, and tissue needs (skin, fascia, muscle, bone, or a combination). All tissues borrowed come with a price, however, and donor-site morbidity must be considered. 135 “Workhorse” flaps are those that are predictable, reliable, and have acceptable donor-site morbidity, particularly for free flaps. Some workhorse flap examples for soft tissue coverage include the anterolateral thigh, deep inferior epigastric artery perforator, or the latissimus dorsi muscle. If other tissues such as bone need to be replaced, a fibula or scapula segment can be harvested on their blood supply. 136
Unfortunately, all of the rungs on our reconstructive ladder are affected by XRT, including flaps. Even if the donor tissue is healthy, the irradiated wound bed incurs a higher failure and complication rate. 132 Herle et al reveal that preoperative XRT in head and neck reconstruction carries increased risk ratios for flap failure and overall complications, 1.8 and 1.5, respectively. Paralleling this, Miitii et al found XRT odds ratios for total and partial flap loss to be 1.8 and 1.9, respectively.137,138 Similarly, Tasch et al examined preoperative XRT in all free flaps and revealed elevated odds ratios for total and partial flap loss, citing 1.7 and 2.2, respectively. 139
Ultimately, compared with the promising wound healing treatments detailed above, surgical reconstruction is complex, expensive, and comes at a cost to the patient’s healthy donor site. Despite still carrying a relatively high complication rate in irradiated fields, many surgeons opt for more aggressive surgical options for these patients, as the bottom half of the reconstructive ladder is often ineffective for RIF-related wounds. Thus, it is imperative to continue wound healing research to pursue less invasive strategies.
Key takeaways
If RIF related wounds do not heal, last-resort surgical treatment involves the removal of unhealthy tissue and replacement with healthy tissue, commonly referred to as a “flap”. Flaps can originate from nearby tissues (local/regional flap) or be transplanted from distant sites (free flap). Nevertheless, irradiation increases surgical complexity, limits reconstructive options, and is associated with increased postoperative complications.
TRANSLATIONAL CONSIDERATIONS AND FUTURE DIRECTIONS
As approved therapies gain more widespread use in the treatment of irradiated wounds, and preclinical treatments advance into the clinical stage, several translational considerations are important to discuss. First, many treatments discussed in this review have synergistic mechanisms and should be considered for combination use. In addition, treatment expenses are discussed for approved therapies, although future coverage and cost–effectiveness of preclinical agents are difficult to predict. Lastly, as irradiated wound care continues to evolve, it is imperative to include commentary on cutting-edge advancements in the broader field of wound care that may likewise support future treatment of irradiated wounds.
Combination therapeutics
Combinations of therapies discussed in this review represent an exciting opportunity to address the multifaceted pathophysiology that underscores healing dysfunction in irradiated wounds. Notably, tissue-based treatments are inherently reliant on wound tissue integrity for survival and optimal outcomes. While dermal substitutes have less-stringent perfusion requirements compared with skin grafts or tissue transfer, their success is still dictated by wound bed vascularity. Similarly, graft survival of adipose-derived therapies is predicated on adequate blood and nutrient supply. It is therefore plausible that therapies that improve vascularity and oxygenation can promote graft survival and synergistically promote wound healing. Indeed, both HBOT and DFO have been shown to improve fat graft retention through improved perfusion.140,141 Likewise, HBOT improves dermal substitute outcomes in a diverse population of wound care patients. 142 While these methods have not yet been used in irradiated wounds, comparable efficacy is highly plausible given the hypovascularity that plagues wound healing in irradiated skin.
Interestingly, several therapies discussed in this review can function as delivery modalities in addition to their own proregenerative characteristics. Both PRP and placental-derived tissues have been used to deliver SVF to chronic or irradiated wounds. When administered as a solution, SVF experiences rapid diffusion into the surrounding extracellular spaces, limiting its efficacy at the wound site. Placental-derived biomaterials have nearly limitless applications given their numerous tissue types and formulations, including drug- or cell-delivering scaffolds. In an irradiated wound model, Oh et al. utilized amniotic membrane-derived cell-delivery scaffolds to retain SVF at the wound bed for a prolonged period. 143 Meanwhile, Yin et al. resuspended SVF in PRP to administer as a topical gel for chronic diabetic ulcers. 144 In this case, PRP acts both as a delivery vessel and brings with it supplementary proregenerative cytokines, which may support grafted ADSC survival. Similar methods can be used to deliver other cell-based therapeutics while leveraging the architecture and proregenerative substances within PRP and placental-derived tissues.
Cost–effectiveness and access
Especially when caring for chronic conditions such as many wounds on irradiated tissue, it is imperative to consider costs to patients and the health care system. Many of the procedural or tissue-derived interventions discussed in this review possess considerable expense. At present,
HBOT is the only widely covered therapy for radiation soft tissue injury by both public and commercial insurers, although typically only as an adjuvant following failure of conservative interventions.145,146 Despite common belief, accessibility of HBOT has greatly improved in the United States with an estimated 1,500 facilities, including hospitals and clinics that offer the service.
Meanwhile, insurance coverage of dermal substitutes for irradiated wounds varies significantly and often requires stringent secondary criteria when covered.147–149 Coverage for ADM and placental-derived materials is also variable. These are typically regulated by the FDA as human cell, tissue, or cellular- and tissue-based products, which means they do not need approval or clearance as long as their use aligns with the product’s intended homologous function (i.e., barrier support or inflammatory modulator). However, this has at times created ambiguous regulatory guidelines, which may impact coverage. Significant cost concerns exist for many of these products. For example, an upper extremity reconstruction cost analysis article revealed product prices as being $1,360 for BTM and $3,185 for Integra. 150 Similarly, another upper extremity study shared that 100cm2 of product costs $850 and $3,150 for BTM and Integra, respectively, at their institution. 151 Likewise, Zelen et al. found that the cost of treatment for two placental-derived products was between $1,250 and $2,500, but 73–97% of diabetic lower extremity wounds were healed within 12 weeks, compared with 51% in the standard wound care control group at 12 weeks. 152 This is in contrast to the estimated 1-year medical costs for patients with diabetic foot wounds, around $28,000. 153
Despite their upfront costs, tissue-derived biomaterials are highly cost-effective when compared with the financial burden of chronic wounds. A cost–effectiveness analysis of six analyzed human tissue-derived products—including dermal substitutes and several placental-derived materials—revealed they were more efficacious and associated with fewer overall costs than standard of care in the treatment of diabetic foot ulcers. 154 Beyond these treatments, cost analyses specific to irradiated wounds are limited. In any case, obtaining clinical data demonstrating improved wound outcomes and quality of life is the necessary first step for many of these therapies.
Cutting-edge biotechnologies
While still early in development, a number of cutting-edge biotechnologies in the wound care field represent exciting future options in the care of irradiated wounds. Temperature-, pH-, or moisture-responsive smart dressings adapt to foster the ideal wound healing environment. Other novel drug-eluting dressings can be utilized to optimally deliver DFO or tissue-based therapies, similar to how placental membrane scaffolds or PRP has been used. 155 Lastly, electrical stimulation has demonstrated promise in promoting cellular migration, vascularization, and wound closure. 156 This technology has similarly been integrated into smart bio-responsive dressings.157 These designs are on the horizon of wound care and will hopefully provide even more options for irradiated wounds.
Key takeaways
Combination therapies for the treatment of irradiated wounds employ synergistic mechanisms of action or utilize novel delivery techniques. Many treatments discussed in this review are associated with high costs, though existing data supports favorable cost effectiveness when considering the financial burden of chronic wounds. Cutting-edge technologies such as bio-responsive smart bandages will have a role to play in the evolution of irradiated wound care.
SUMMARY
RIF-associated wounds are dreadful, common sequela of external XRT for cancer treatment. They are costly to patients and health care systems from both financial and pain/emotional burden standpoints. Long-term wound care can help keep the wounds clean, but these treatments run into diminishing returns in irradiated fields as the tissue substrate cannot heal itself due to perpetual inflammation and eventual fibrotic scarring. This is where recent advancements in wound care technology play a role, by conditioning the local environment in a way that promotes healing pathways. The treatments outlined above hold great potential, and we urge the community at large to conduct further wide-scale clinical studies examining their efficacy. If successful, these treatments may provide relief for millions of patients worldwide.
CLINICAL APPLICATION GUIDE
From a treatment standpoint, it is important to identify what characteristics a patient’s RIF-associated wounds may contribute to chronicity. Identifying and documenting the patient’s local surgical and XRT exposure histories are the first step in understanding the wound environment and healing potential. Again assuming optimal nutrition, pressure offloading, and clean wound care, the risk of wound chronicity can be stratified by distinguishing favorable characteristics (well-vascularized with some bleeding on debridement, and subsequent granulation tissue formation) from concerning signs (lesser degree of the favorable characteristics) and high-risk factors such as systemic medical comorbidities or particularly large wounds. If concern exists regarding poor wound healing, or if the wound has already failed standard treatment, it would be prudent to address factors that may be limiting healing and consider supplementing conservative wound care with adjunctive treatments.
Given the diverse mechanisms and formulations of treatments discussed in this guide, the future landscape for irradiated wound care is indeed promising. While supporting evidence for several of these therapies is presently limited to preclinical studies, case reports, or clinical studies in adjacent fields, the following guide proposes a set of potential recommendations based on what is translatable. Irradiated wounds demonstrate unique manifestations, and it is our hope that new clinical trials in the field of irradiated wounds will expand these recommendations to become formal treatment stratifications.
We see unique potential in each of the discussed therapies in addressing irradiated wounds based on their size, vascularity, infection status, chronicity, and tissue quality. For example, large and complex wounds are likely to benefit from dermal substitutes for broad coverage, even if just temporizing. Hypovascular wounds, characterized by minimal bleeding during debridement, will likely benefit from proangiogenic therapies such as HBOT, DFO, or select placental-derived treatments. Fibronectin, dermal substitutes, and placental-derived products can improve the formation of healthy granulation tissue. Chronic, nonhealing wounds have seen benefit from adipose- and plasma-derived injectable therapies, DFO, placental-derived products, and HBOT. Unfortunately, infected wounds remain with limited potential treatment options outside of HBOT, as clearing the infection must come first. Lastly, for wounds that are already woody and fibrotic, DFO and adipose-derived injectables have demonstrated efficacy in preclinical studies. As these therapies gain traction with increasing evidence and physician comfort, we also see potential for earlier, prophylactic use of many of these therapies to address and prevent the pathophysiologic changes that contribute to RIF and poorly healing irradiated wounds. Already, we have seen evidence supporting prophylactic DFO use in animal experiments, and we expect that other treatments will follow suit. Regardless of which therapies are utilized, however, skin integrity and wounds of any status in irradiated fields necessitate frequent follow-up care for monitoring and potential escalation to surgical reconstruction if they remain refractory to treatments (Fig. 11, Table 1).
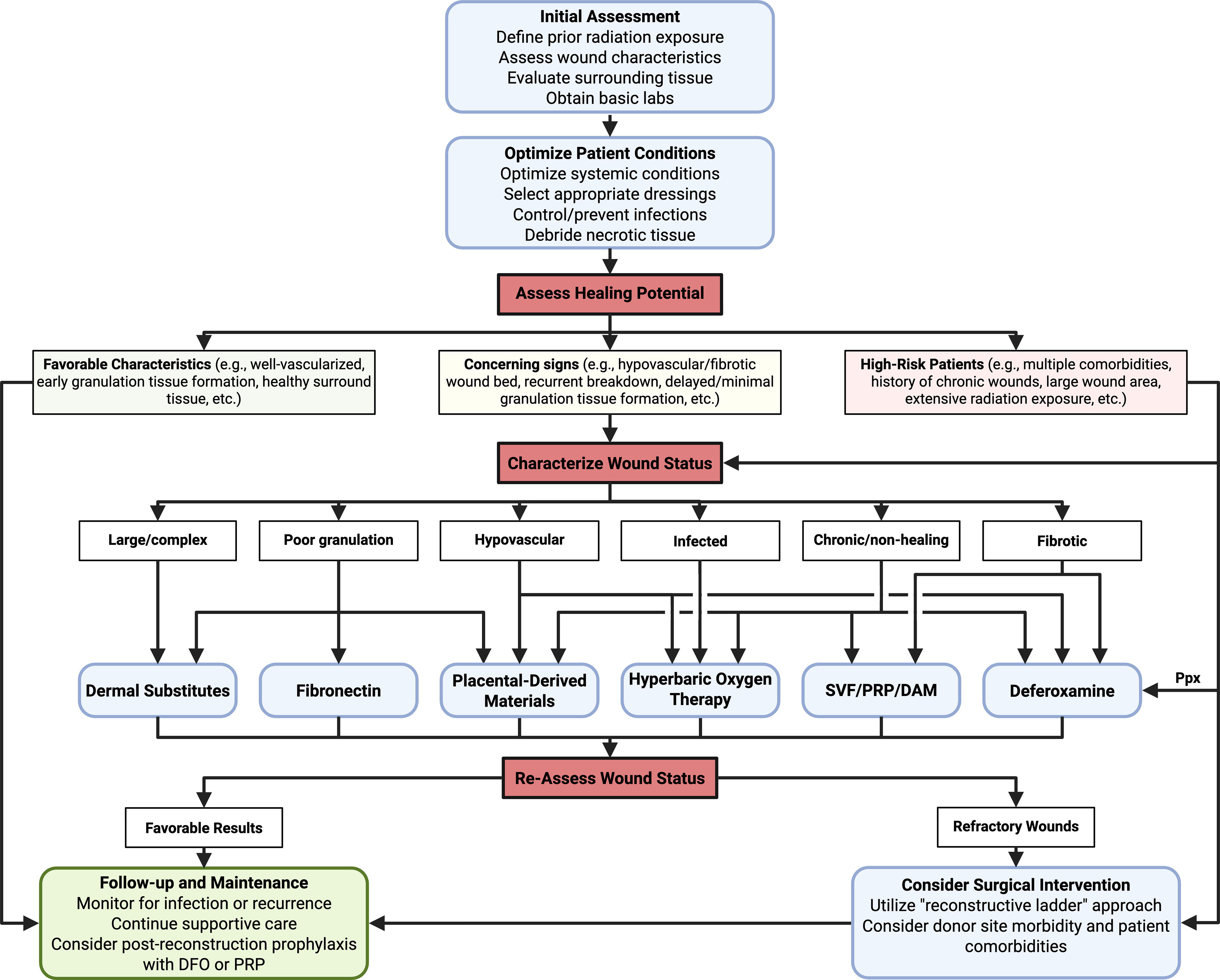
Clinical application flowchart. Flowchart demonstrating a generalizable approach to RIF-related wound management. Based on patient and wound characteristics, this graphic recommends adjunct treatments with their respective mechanisms of action in mind. Note that these recommendations are extrapolated from preclinical and limited clinical studies, and further in-human studies are required to establish formal guidelines. More specifics on each treatment are given in Table 1. SVF, stromal vascular fraction; DAM, decellularized adipose matrix; PRP, platelet-rich plasma; DFO, deferoxamine; Ppx, prophylaxis; RIF, radiation-induced fibrosis.
Adjunct treatments for radiation-induced fibrosis-related wounds
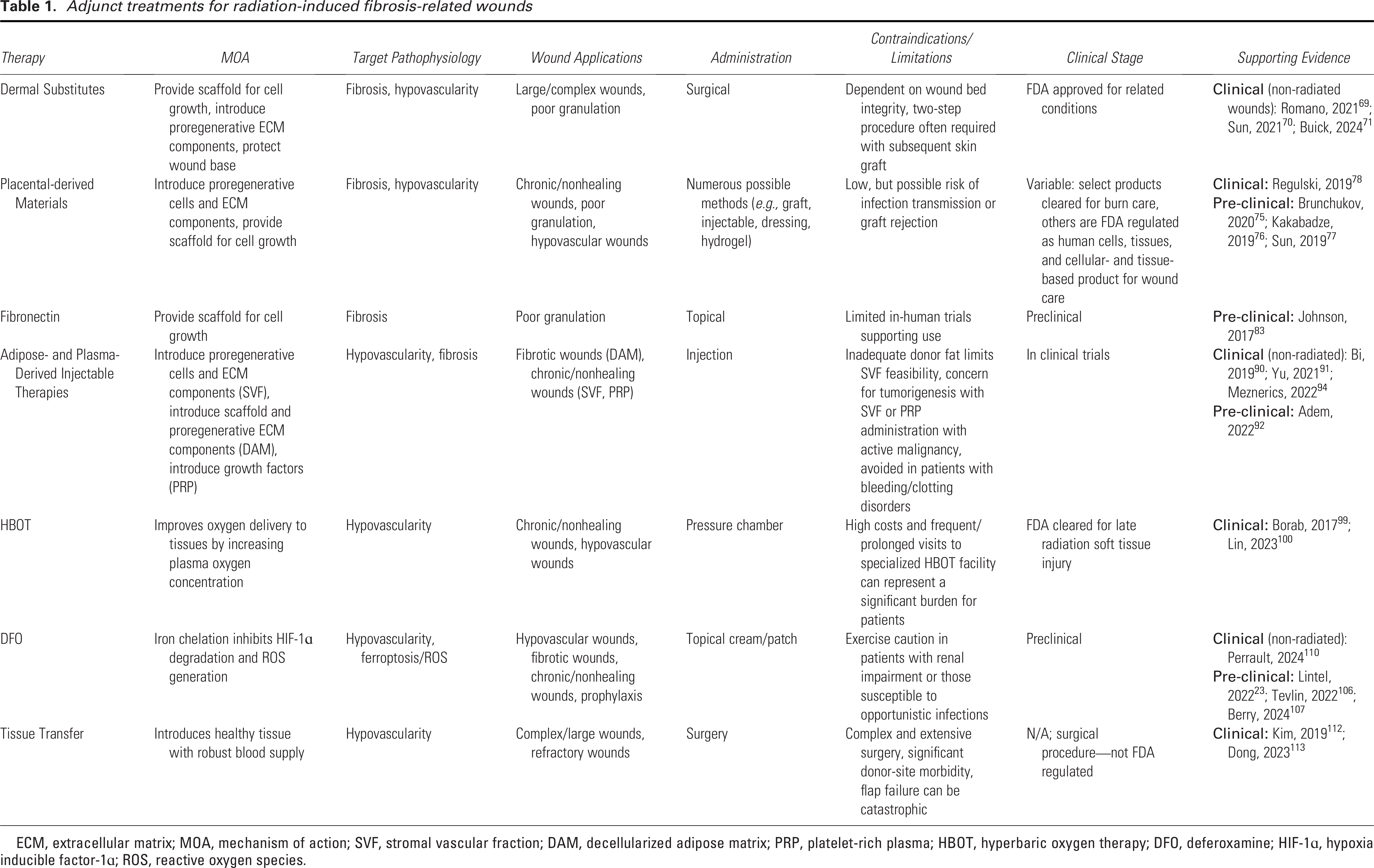
ECM, extracellular matrix; MOA, mechanism of action; SVF, stromal vascular fraction; DAM, decellularized adipose matrix; PRP, platelet-rich plasma; HBOT, hyperbaric oxygen therapy; DFO, deferoxamine; HIF-1ɑ, hypoxia inducible factor-1ɑ; ROS, reactive oxygen species.
TAKE-HOME MESSAGES
Irradiated fields are hypocellular and hypovascular. Wounds in this permanently fibro-atrophic setting are common and particularly difficult to heal.
Basic wound care is a prerequisite, but recent advancements aim to heal irradiated wounds by correcting the underlying pathophysiological problems.
Novel therapeutic strategies currently available or being studied include dermal substitutes, placental derivatives, fibronectin, injectable fat-derived and plasma-derived compounds, hyperbaric oxygen, and DFO.
As a last resort, surgical tissue transfer is used to bring healthy tissue with its own blood supply into the irradiated field.
AUTHORS’ CONTRIBUTIONS
C.V.L.: Conceptualization, methodology, investigation, and writing. C.B.K.: Conceptualization, investigation, visualization, and writing. D.K.: Investigation and writing. J.T.: Investigation and writing. H.Y.: Investigation and writing. P.S.: Investigation, visualization, and writing. P.S.S.: Investigation and writing. D.P.: Visualization. M.T.L.: Conceptualization and supervision. D.C.W.: Conceptualization and supervision.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
AUTHOR DISCLOSURE AND GHOSTWRITING
D.C.W. holds a patent for the use of DFO for conditioning irradiated tissue. All individuals who contributed to the writing of this review are credited with authorship.