
Abstract
Objective:
To evaluate wound healing with a novel bandage with hydrocolloid pad designed for daily use/replacement in a new model of laser-induced burns/wounds.
Approach:
In this randomized, controlled, single-center, 16-day study, healthy adults aged 25–55 years of age with Fitzpatrick skin type I–III and who met all eligibility criteria (N = 34) had four laser-induced wounds generated on each arm and were randomized as follows: (1) uncovered wound (control); (2) standard of care bandage (SoC); (3) petrolatum-based antibiotic ointment + SoC (petrolatum + SoC); (4) bandage with hydrocolloid pad. Primary endpoint: composite healing score (sum of scores for general wound appearance, smoothness, and epithelial confluence, minus scores for erythema, edema, and crusting/scabbing) on Days 1–7.
Results:
Mean composite healing score was significantly better with the hydrocolloid pad (Days 1–7) and petrolatum + SoC (Days 2–7) than SoC, and with either treatment than untreated controls (Days 1–7), and significantly better with the hydrocolloid pad than petrolatum + SoC (Days 1 to 2 and 7). The hydrocolloid pad and petrolatum + SoC both significantly reduced crusting/scabbing while improving epithelial confluence, smoothness, and general wound appearance, compared with untreated controls and SoC.
Innovation:
A laser-induced burn model producing consistent wounds was used to evaluate healing with a novel bandage with hydrocolloid pad versus other typical treatments.
Conclusion:
Wound healing with the novel bandage with hydrocolloid pad used daily was superior to SoC (Days 1–7), untreated wound (Days 1–7), and petrolatum + SoC (Days 1 to 2 and 7).
Jenny Du-Soriano, BSE, MBA
Keywords
INTRODUCTION
For minor acute wounds, a primary objective is to protect the wound from further damage and facilitate healing by fostering an occlusive moist wound healing environment that speeds healing and also limits infection, inflammation, and scarring.1,2 Appropriate wound dressings can facilitate the complex healing process during which the skin surface and underlying tissue undergo an intricate, highly orchestrated, multistage repair process.2,3 Furthermore, dressings can promote restoration of skin barrier function 1 and reduce inflammation and scarring 2 while providing the necessary protection. 2
When wounds are left uncovered, normal wound exudate dries up, leading to scab formation with resultant reduction in pro-healing cytokines and growth factors, diminished electrical gradient, and more difficult epithelial migration.4–8 In occluded wounds, however, the exudate facilitates the healing process by supplying moisture, allows for a variety of bioactive mediators (e.g., enzymes, growth factors, and nutrients) 8 and matrix proteins to be more readily available, facilitates electrical gradient for healing, 6 and also curbs excessive inflammation by providing various immune cells with the environment needed to eliminate debris, pathogens, and foreign bodies.4,5,7,8 As occlusion affects both the epidermis (by enhancing epithelial cell migration) 9 and the dermis (by enhancing dermal collagen synthesis and deposition),10,11 maintaining a moist environment favors restoration of epidermal barrier function and wound healing overall, while easing the dressing changes/replacements. 12 Moreover, healed occluded wounds are cosmetically more pleasing than those left uncovered, 4 hence ongoing research seeking more effective wound therapies to help optimize the healing process and fully restore tissue integrity.13,14
INNOVATION
Hydrocolloid dressings have been used since the 1960s to promote moist wound healing,15,16 yet their design has traditionally favored multiday use. However, patients prefer to change dressings daily, which can lead to unintended wound disruption during daily dressing changes.17–19 This study introduces a novel hydrocolloid pad integrated into a daily use adhesive bandage (BAND-AID® Brand Pro Heal™ Advanced Healing Bandage, Kenvue Brands LLC) that combines low adhesion with high absorbency properties of the hydrocolloid pad, enabling daily replacement of the bandage without compromising wound integrity. This innovation addresses a critical gap in consumer wound care behavior, where frequent dressing changes are common despite existing hydrocolloid products being unsuitable for such daily replacement.
A second innovation is the use of a standardized laser-induced burn/wound model to simulate minor traumatic injuries. This model produces consistent wound size and depth across subjects, allowing for within-subject comparisons of healing outcomes across multiple treatment modalities. Other models for wound generation in the study of acute wound healing in humans can involve approaches such as punch biopsy 20 or burning of skin with liquid nitrogen. 21 Unlike these known models, laser-induced burns better mimic everyday skin injuries such as scrapes and abrasions because they take longer to heal22,23 and contain cellular debris,24,25 offering a more real-world relevant evaluation of wound healing interventions.
Together, these innovations provide a clinically meaningful and consumer-relevant advancement in wound care product technology and clinical testing methodology. Clinical test results using the laser-induced burn/wound model demonstrate faster healing efficacy of the novel bandage with hydrocolloid pad (Fig. 1).
Simplified illustrative summary of main findings. SoC, standard of care.
CURRENT PROBLEM ADDRESSED
Two key challenges in wound healing research and consumer care are addressed in this study.
First is the design limitation of traditional hydrocolloid dressing. Most hydrocolloid products are designed for multiday use and feature strong adhesion, which can reinjure healing tissues when removed prematurely. 26 However, consumer behavior driven by public health guidance and product instructions often favors daily dressing changes.27,28 To address this mismatch, we developed a daily-use hydrocolloid bandage with reduced adhesive properties that maintains the moist healing environment essential for optimal recovery while allowing safe, routine replacement. This design bridges the gap between clinical efficacy and consumer usability, offering a practical solution for at-home wound care.
Second is consistency in wound modeling for clinical evaluation. Minor wounds vary in size, depth, and healing response, making it difficult to objectively compare treatment efficacy across individuals. To overcome this, we employed a laser-induced burn/wound model that reliably produces uniform wounds that best mimic real-life minor scrapes. This approach allows for controlled, reproducible comparisons of healing outcomes across treatments within the same subject, minimizing the variability due to individual health status and wound characteristics.
MATERIALS AND METHODS
Study design
This randomized, controlled, single-center, 16-day study (ClinicalTrials.gov identifier: NCT05045183; https://clinicaltrials.gov/study/NCT05045183) was conducted in the United States between September 8, 2021, and October 15, 2021, in accordance with the ethical principles of the Declaration of Helsinki, the Health Insurance Portability and Accountability Act (HIPAA), and any applicable domestic/international guidelines. The study protocol and related materials were approved by the Advarra Institutional Review Board (Columbia, MD) before enrollment started. Written informed consent was obtained from each participant before study initiation. As part of the informed consent process, the prospective subjects were given as much time as needed to read the informed consent document, which included a HIPAA disclosure and a photo release form, and had the opportunity to have any study-related questions answered to their satisfaction prior to signing the informed consent document. A Consolidated Standards of Reporting Trials (CONSORT) reporting guidelines checklist is provided in the supplementary materials (Supplementary Table S1).
Key eligibility criteria
Eligible individuals were 25- to 55-year-old men and women with Fitzpatrick skin type I–III and uniform skin color on both volar forearms who were generally in good health and able to read/write/speak/understand English. Potential participants were also required to attend all study visits and follow all study instructions, including wearing long sleeves when going outdoors during the study (to protect the test areas from exposure to sunlight) and refraining from the following for the study duration: immersing the bandages in water; showering within 2 h before each study visit; using lotions, creams, moisturizers, cosmetics, or sunscreens on their forearms (wound sites); and use of any daily cleanser/wash-off products on their forearms other than the auxiliary cleanser provided at screening (from screening to Day 16).
The key exclusion criteria were as follows: known allergies/hypersensitivity/adverse reactions to any of the products used in the study; presence of excessive hair, acne, scars, pigmentation, tattoos, or friable skin on either volar forearm that could have interfered with the study procedures or assessments; history of keloid or hypertrophic scar formation, cracked or excoriated skin, infected skin lesions, or any other skin or health conditions that could have put the subject at risk, interfered with the assessments, or confounded the study results; use of any oral/topical medications or products that could have masked an adverse event (AE), confounded the study results, or altered/compromised the bleeding/healing process, including use of vitamin A derivatives (oral or topical) within one year before the screening visit and use of topical leave-on products on the volar forearms within one week before the screening visit.
Randomization
For eligible participants, wound sites were randomly allocated to one of four treatment groups in a 1:1:1:1 ratio (one study treatment per wound site), based on a randomization scheme devised by the sponsor’s biostatistics group, using assigned treatment codes (A through D).
Study interventions and visits
Study visits were scheduled at screening (at 5–7 days prior to baseline), Day 0 (baseline), Days 1–7, and Day 16. At screening, prospective participants were reviewed for eligibility, completed the informed consent process, and were provided with the auxiliary product (Johnson’s Head-to-Toe Wash & Shampoo®, Kenvue Brands LLC) to be used on their forearms and body during the study (instead of their regular body cleanser). Demographic details, medical history, and details of concomitant medications were also collected.
At baseline (Day 0), participants returned to the clinic, and those who still met the eligibility criteria were enrolled in the study; each participant had wound sites marked on the volar forearms. After completion of the baseline evaluations (clinical grading of wound healing parameters described below), a thick layer of anhydrous numbing benzocaine-lidocaine-tetracaine cream (20%/8%/8%) was applied on each designated wound site to cover an area of ∼2 cm × 2 cm. Approximately 30 min later, the forearms of each subject were cleaned using alcohol wipes, and a certified laser specialist created four uniform minor wounds per volar forearm (at the designated wound sites) using an Erbium:Yttrium Aluminum Garnet (YAG) 2,940-nm laser (Sciton Inc, Palo Alto, CA), at an energy setting of 12.2 J/cm2 and three passes of ∼50 μm depth each.
Each created wound was circular, 6 mm in diameter, and ≥4 cm away from adjacent wounds. The wounds created by this method heal by the migration of epidermal cells from the dermal appendages located in the wound’s base (dermal islands) and/or wound borders and mimic minor wounds similar to real-life scraped skin, typically healing in less than 16 days if left untreated, based on the site’s previous experience. For each participant, wound sites were randomly assigned to one of the following treatments: (1) uncovered wound (control), (2) standard of care (SoC) (BAND-AID® Brand Adhesive Bandage® Flexible Fabric, Kenvue Brands LLC), (3) petrolatum-based antibiotic ointment (Neosporin® Plus Pain relief ointment, Kenvue Brands LLC) + SoC (petrolatum + SoC), or (4) the novel bandage with hydrocolloid pad (BAND-AID® Brand Adhesive bandage Pro Heal™ Advanced Healing Bandages, Kenvue Brands LLC). Each participant received all four treatments per arm.
On Days 1–7, the investigational products were removed, evaluations were performed, and fresh investigational products were reapplied, except on Day 7 (end of treatment reflecting typical healing time), 29 when all wound sites were left uncovered for post-healing assessments. Participants returned for a final (safety) visit on Day 16.
At the study visits, after completion of the post-wound assessments (clinical grading of wound healing parameters and digital photographs), a trained, gloved clinic staff member applied the assigned treatment on the corresponding wound site. Subjects were also provided with a unit of Cloth Tape (BAND-AID® Brand Adhesive Bandage All-Purpose Cloth Tape®, Kenvue Brands LLC) to be used at home as needed to secure the investigational products if they became loose during the study. A schematic of the sequence of events is provided (Supplementary Fig. S1).
Assessments
On Day 0 (pre- and immediately post-wounding) and Days 1–7, each wound site was graded on erythema, edema, crusting/scabbing, epithelial confluence, smoothness, and general wound appearance,4,30,31 using the 0–4 scales described in Supplementary Table S2. Briefly, for erythema and edema, 0 and 4 indicated no and severe erythema/edema, respectively. For crusting/scabbing and epithelial confluence, 0 and 4 indicated no and 91–100% crusting/scabbing or epithelial coverage, respectively. For smoothness, 0 indicated a rough, uneven wound, and 4 a completely smooth, even wound. For the general wound appearance, 0 indicated poor appearance (i.e., new or fresh wound missing the epithelium layer, with the wound bed appearing raw and possibly oozing), while 4 indicated an excellent appearance (i.e., a slight color mismatch may be present, but the wound is fully healed, with skin flush against surrounding skin). The principal investigator was blinded to the treatment groups and did not have access to the randomization schedule, and the investigational product was kept separate. Subjects were instructed not to disclose information about their assigned study treatments to the investigator or to discuss any other information that may reveal the treatment assignment. While patients were not blinded, they were not aware of the goals of the study and did not know which of the treatments were experimental. Data were collected using an electronic data capture system.
Using the same schedule, each volar forearm was separately photographed with the Canfield Twinflash system (Canfield Imaging Systems, Fairfield, NJ), which included a Nikon D7000 Digital Single Lens Reflex camera supporting intelligent-through-the-lens metering (Nikon Corp, Tokyo, Japan) and a Sigma DG 70 mm f/2.8 macro lens or equivalent (designed for a full-frame camera) under visible and cross-polarized lighting modes.
AEs were recorded at each visit per the Medical Dictionary for Regulatory Activities (MedDRA).
Outcomes and statistical analysis
The primary endpoint was the composite healing score, used as a measure of healing to compare the different treatments and reflect their overall healing benefits. The composite healing score was calculated as the sum of scores for general wound appearance, smoothness, and epithelial confluence, minus the sum of scores for erythema, edema, and crusting/scabbing. Composite wound healing scores ranged from −12 to +12; a higher composite score indicated a greater extent of wound healing. The between-treatment comparison was based on the changes from baseline at each post-baseline visit and a mixed-effect analysis of covariance (ANCOVA) model that included the treatment as a factor, the baseline value as the covariate, and the subject as random effect (to incorporate the within-subject correlation).
Secondary endpoints included erythema, edema, crusting/scabbing, general wound appearance, smoothness, and epithelial confluence, analyzed individually. The wound healing process assessment was analyzed at each post-baseline time point using logistic regression with the general estimating equations method; the model included treatment as a factor, and the within-subject covariance matrix was assumed as exchangeable. Pairwise comparisons were performed based on the adjusted means.
Analyses of the primary and secondary endpoints were based on the intent-to-treat (ITT) population (i.e., all participants who received laser-induced wounds and started the study treatments). The number (%) of participants with AEs was analyzed in the safety population (i.e., all individuals enrolled with ≥1 application of study product).
Descriptive summaries were provided for continuous variables, and frequencies were provided for categorical variables. SAS software version 9.4 was used for statistical analysis. Statistical significance was based on p ≤ 0.05.
Sample size
A sufficient number of subjects was to be screened to enroll ≤38 qualified subjects and ensure study completion by 30 subjects.
RESULTS
Patient flow, demographics, and baseline characteristics
Of 34 individuals enrolled, all (100%) completed the study and were included in the ITT and safety populations. Mean age was 44 years, 85% of participants were White, and most had a Fitzpatrick Skin Type II (Table 1).
Demographics and baseline characteristics
SD, standard deviation.
Primary endpoint
The mean composite healing score showed that wound healing was statistically significantly better with the hydrocolloid pad at Days 1–7, compared with the SoC and the untreated control (Fig. 2). In a post hoc analysis comparing the hydrocolloid pad and petrolatum + SoC, the difference between treatments statistically favored the hydrocolloid pad at Days 1, 2, and 7 and numerically favored the hydrocolloid pad at Days 3–6 (Fig. 2).
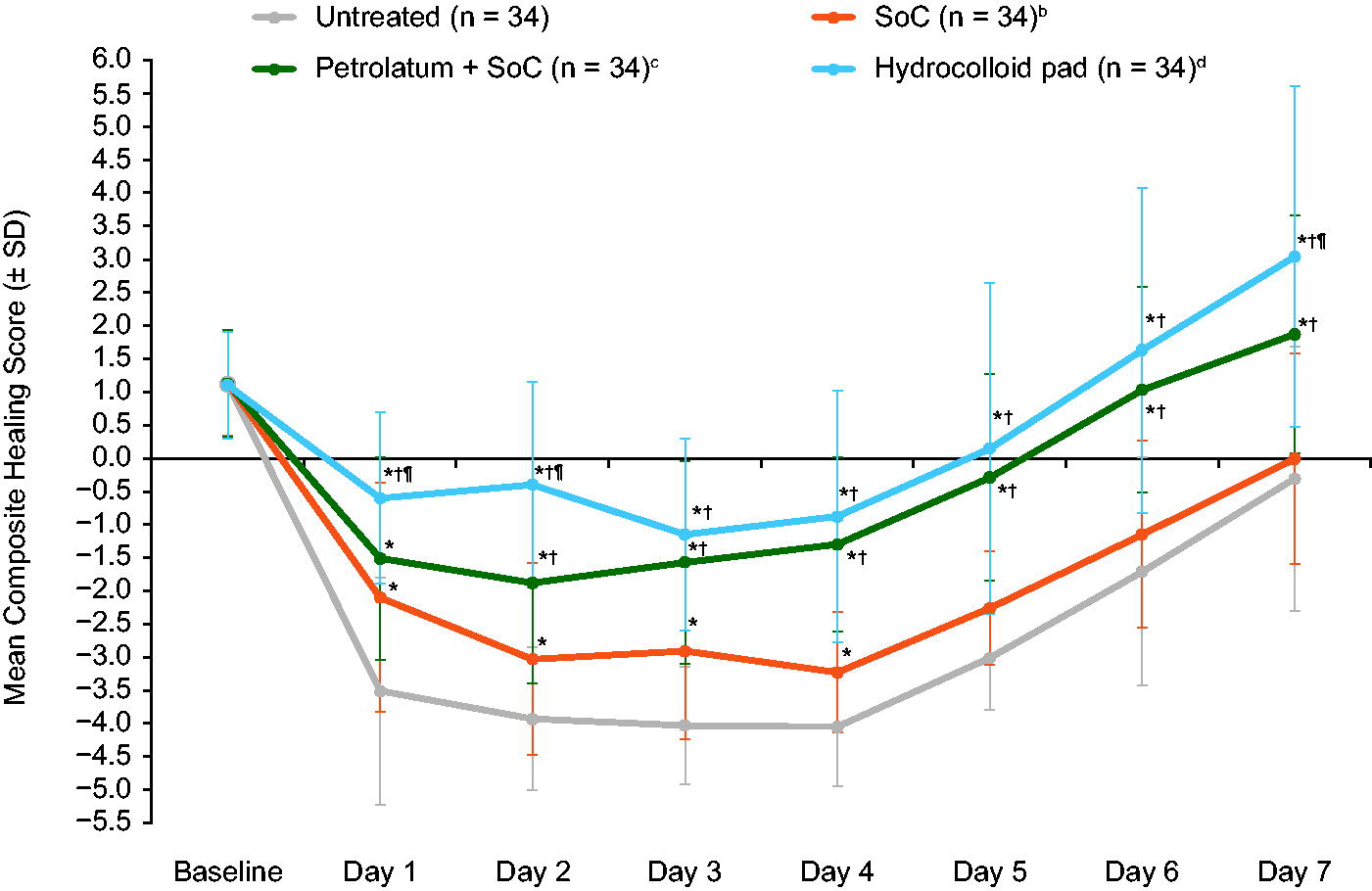
Composite healing scores at each study visita. SoC, standard of care. aComposite healing score = (General Wound Appearance + Smoothness + Epithelial Confluence) − (Erythema + Edema + Crusting/Scabbing). The total scale ranged from −12 to +12, and a higher composite score indicated a greater extent of wound healing. bBAND-AID® Brand Adhesive Bandage®; cNeosporin®; dPro Heal™ Advanced Healing Bandage; *p ≤ 0.05, change from baseline versus the untreated control; †p ≤ 0.05, change from baseline versus SoC; ¶p < 0.02, change from baseline with the hydrocolloid pad versus petrolatum + SoC.
Notably, representative images of wound healing in each treatment group support better/faster healing in the group treated with the hydrocolloid pad, compared with the other groups (Fig. 3).
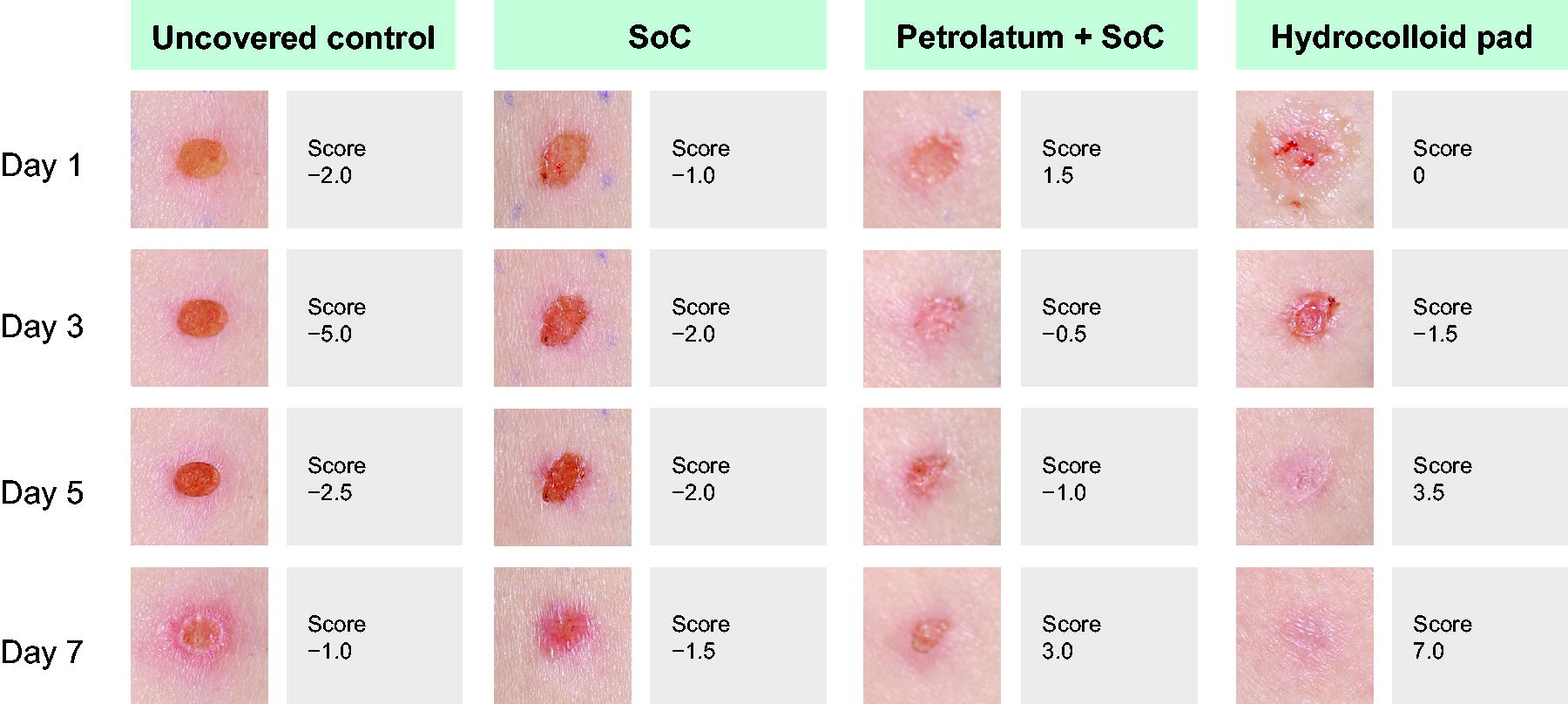
Representative photographs of laser-induced wound healing following treatment with the standard of care (SoC; BAND-AID® Brand Adhesive Bandage® Flexible Fabric), petrolatum-based antibiotic ointment (Neosporin® Plus Pain relief ointment) + SoC (petrolatum + SoC), or the novel hydrocolloid pad (Pro Heal™ Advanced Healing Bandages), compared with the uncovered control. The composite healing score of each wound was determined as described in the Methods.
Secondary endpoints
The mean scores for erythema, edema, crusting/scabbing, epithelial confluence scores, wound smoothness, and general wound appearance at baseline and Days 1–7 are presented in Tables 2 and 3. Per those tables, the most significant contributors to the composite healing score were crusting/scabbing, epithelial confluence scores, wound smoothness, and general wound appearance.
Erythema, edema, and crusting/scabbing scores, for which higher values indicate less healing. N = 34 subjects in total, each with four wounds (treatment sites) per arm
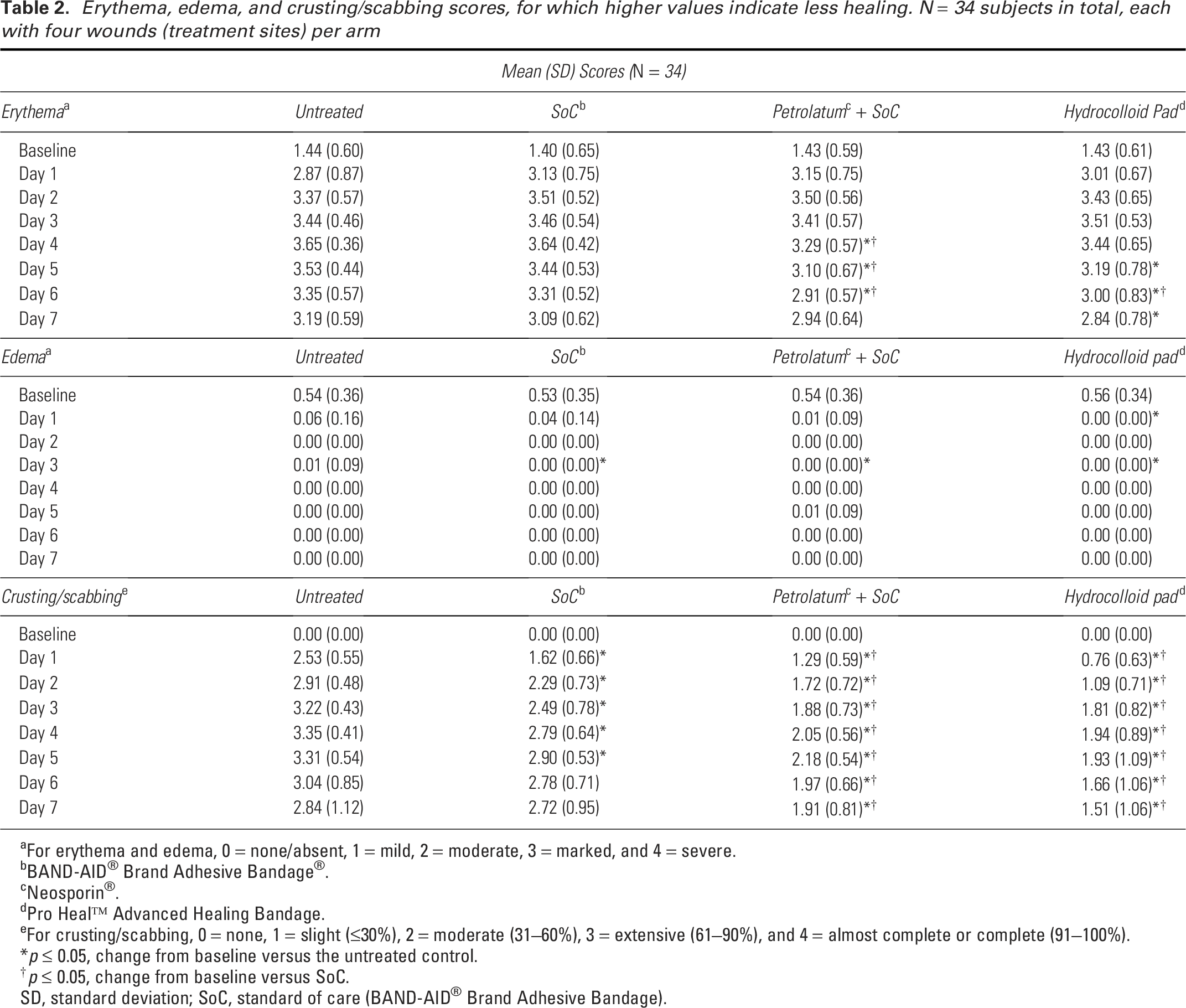
For erythema and edema, 0 = none/absent, 1 = mild, 2 = moderate, 3 = marked, and 4 = severe.
BAND-AID® Brand Adhesive Bandage®.
Neosporin®.
Pro Heal™ Advanced Healing Bandage.
For crusting/scabbing, 0 = none, 1 = slight (≤30%), 2 = moderate (31–60%), 3 = extensive (61–90%), and 4 = almost complete or complete (91–100%).
*p ≤ 0.05, change from baseline versus the untreated control.
†p ≤ 0.05, change from baseline versus SoC.
SD, standard deviation; SoC, standard of care (BAND-AID® Brand Adhesive Bandage).
Considering that less crusting/scabbing reflects better healing, the crusting/scabbing scores indicated that, on Days 1–7, both petrolatum + SoC and the hydrocolloid pad were statistically significantly more effective in reducing crusting/scabbing compared with untreated wounds and wounds treated with the SoC (Table 2).
Petrolatum + SoC and the hydrocolloid pad both statistically significantly improved the epithelial confluence scores, wound smoothness, and general wound appearance on Days 1–7, compared with untreated wounds (Tables 2 and 3). When compared with the SoC, the hydrocolloid pad and the petrolatum + SoC were both statistically significantly better in improving the wound smoothness score on Days 1–7 and general wound appearance score on Days 2–7. The hydrocolloid pad significantly improved the epithelial confluence score on Days 2–7 compared with SoC, while the petrolatum + SoC significantly improved the epithelial confluence score on Days 4–7 compared with SoC (Tables 2 and 3).
Epithelial confluence, smoothness, and general wound appearance scores, for which higher values indicate more healing. N = 34 subjects in total, each with 4 wounds (treatment sites) per arm
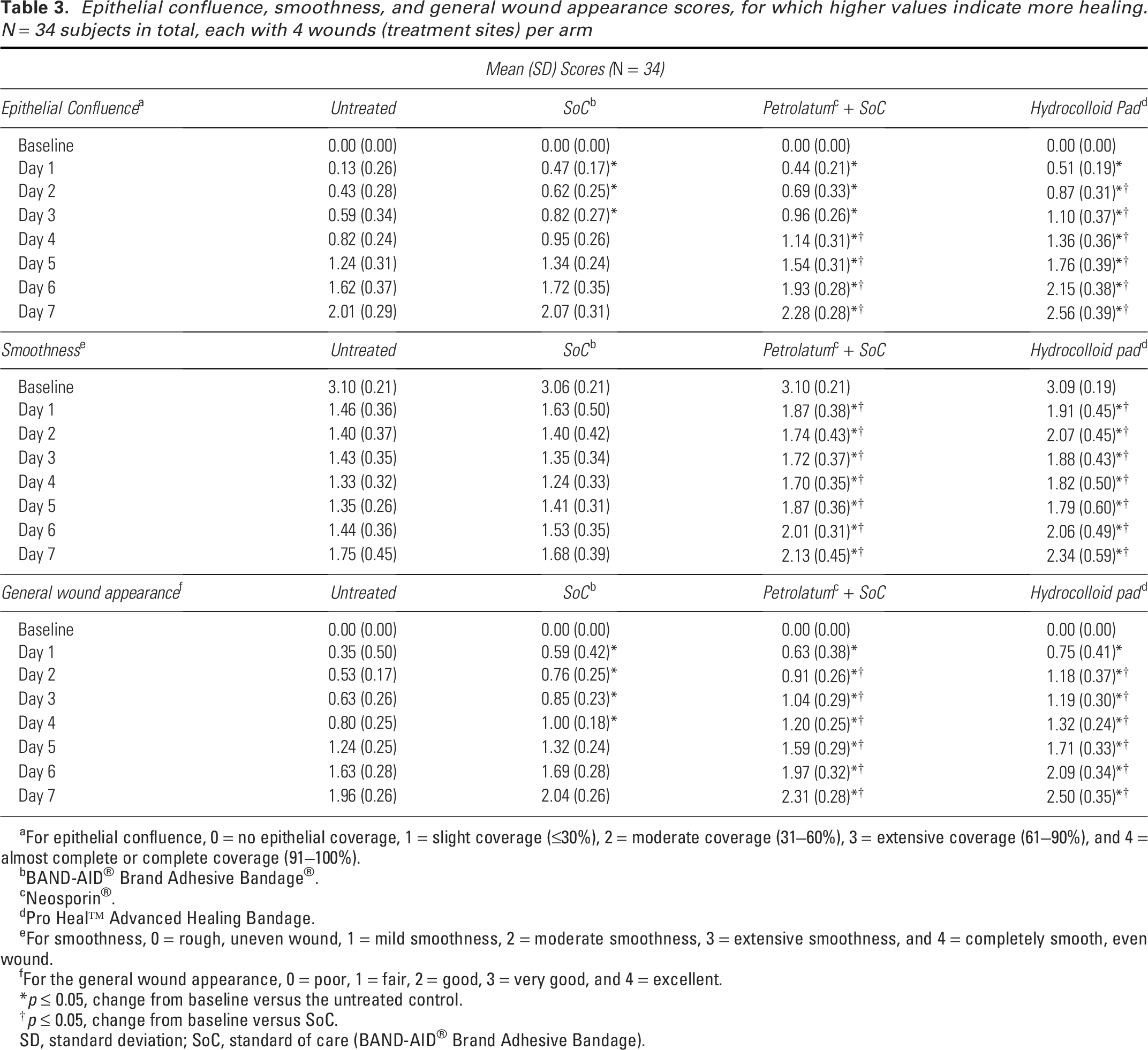
For epithelial confluence, 0 = no epithelial coverage, 1 = slight coverage (≤30%), 2 = moderate coverage (31–60%), 3 = extensive coverage (61–90%), and 4 = almost complete or complete coverage (91–100%).
BAND-AID® Brand Adhesive Bandage®.
Neosporin®.
Pro Heal™ Advanced Healing Bandage.
For smoothness, 0 = rough, uneven wound, 1 = mild smoothness, 2 = moderate smoothness, 3 = extensive smoothness, and 4 = completely smooth, even wound.
For the general wound appearance, 0 = poor, 1 = fair, 2 = good, 3 = very good, and 4 = excellent.
*p ≤ 0.05, change from baseline versus the untreated control.
†p ≤ 0.05, change from baseline versus SoC.
SD, standard deviation; SoC, standard of care (BAND-AID® Brand Adhesive Bandage).
Safety
Overall, seven (20.6%) patients reported nine treatment-related AEs during the study. All were mild skin and subcutaneous tissue disorders, consisting of dermatitis contact (n = 5, 14.7%) and dermatitis allergic (n = 4, 11.8%), and all were resolved without sequelae at study end.
DISCUSSION
Using a new model of laser-induced burn wounds, we demonstrated that the mean composite healing score was statistically significantly better with the hydrocolloid pad (Days 1–7) and petrolatum + SoC (Days 2–7) than the SoC, and statistically significantly better with either treatment (Days 1–7) than the untreated control. Notably, the mean composite healing score was also statistically significantly different with the hydrocolloid pad than with petrolatum + SoC at Days 1, 2, and 7, suggesting faster, better, and more complete healing with the hydrocolloid pad.
When analyzing the individual components of the composite healing score, the hydrocolloid pad and petrolatum + SoC both statistically significantly reduced crusting/scabbing while statistically significantly improving epithelial confluence, smoothness, and general wound appearance on most days, compared with untreated controls and the SoC. The composite healing score was significantly better with the hydrocolloid pad compared with petrolatum + SoC (Days 1 to 2 and 7) and numerically superior on Days 3–6. Dermatologists’ standard approach for minor wounds is petrolatum + SoC (bandage). Our results show that the hydrocolloid pad provided a convenient one-step treatment with better healing results than dermatologists’ SoC, supporting its use for the treatment of minor wounds encountered in everyday life.
Previous studies have evaluated wound healing of laser-induced skin burns in humans.30,32–42 However, many of those studies involved patients undergoing surgery, skin resurfacing, or other skin treatment.32,34–37,39,41 Two were preliminary studies involving ≤10 individuals,33,38 and three used a CO2 laser30,40,42 (which has been described as less precise and more invasive than the Erbium:YAG laser used herein 43 ). Of the latter three studies, only one was randomized, 30 and it was designed to compare the effects of two ointments on wound healing. Therefore, we leveraged those studies to utilize a novel, reliable laser wound model. The current study constitutes (to the best of our knowledge) the first randomized, controlled, clinical study of wound healing in a model of laser-induced burns that ensures consistency across wounds, as well as the first randomized, controlled study of the novel hydrocolloid pad designed for daily use. While it is not known, one might hypothesize it may have been even more difficult in our healthy population of subjects to observe healing differences between treatments compared with a less healthy population.
The mode of action of hydrocolloid dressings differs significantly from that of traditional bandages composed of tape and gauze. 44 Hydrocolloid dressings create a seal over the wound and the surrounding skin, providing occlusive protection while gradually and efficiently absorbing exudates. This occlusive environment maintains optimal moisture levels, which are known to accelerate wound healing. The bandage with hydrocolloid pad used in this clinical study was specifically designed to combine very low adhesion and high absorbent capacity. This design ensures ideal occlusive protection and minimizes the risk of re-injury to the wound bed during daily dressing changes. Current wound care guidelines, public health recommendations for treating minor cuts, and bandage usage instructions typically advise daily dressing replacement. As a result, most consumers tend to change their bandage daily (data on file). The hydrocolloid pad used in this study supports this behavior by enabling daily dressing changes while still promoting moist wound healing conditions. This helps improve healing outcomes and reduces the likelihood of wound bed trauma due to dressing removal.
There are a number of limitations to this study. The wounds created were 6 mm in diameter, and the findings may not translate to larger wounds. We also did not compare our hydrocolloid bandage with any currently marketed hydrocolloid bandages.
The bandage with hydrocolloid pad was generally well tolerated, without unexpected AEs during the 16-day study period. All AEs reported were mild in severity and resolved without sequelae at study end. Nonetheless, the study involved individuals with generally good health, and those with diabetes or poor circulation (for example) should consult their doctor before using the hydrocolloid pad.12,18
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The authors would like to acknowledge the contribution of Gabriella John, MSc, who was the lead of Clinical Research and Development for Kenvue Brands LLC (Summit, NJ) when the study was conducted; Paul Zhang, PhD, who was a biostatistician at Kenvue Brands LLC (Summit, NJ) when the study was conducted; and Sana Syed, PhD, of Kenvue Brands LLC (Summit, NJ), for the post hoc analyses. Medical writing support was provided by Michele Jacob, PhD, of Evidence Scientific Solutions (Philadelphia, PA), and funded by Kenvue Brands LLC (Summit, NJ).
DATA AVAILABILITY STATEMENT
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
AUTHOR CONFIRMATION
All authors met the ICMJE criteria for authorship.
AUTHOR DISCLOSURE AND GHOSTWRITING
Jenny Du-Soriano and Diana Friscia are/were employees of Kenvue Brands LLC at the time of study conduct. Robert Kirsner is a consultant for Kenvue Brands LLC.