
Abstract
Objective:
To determine whether frailty, as quantified using the Five-Item Modified Frailty Index (mFI-5), independently predicts postoperative complications in patients undergoing surgery for diabetic foot ulcers (DFUs), and to assess its utility as a clinical risk stratification tool.
Approach:
A retrospective cohort analysis was conducted using the American College of Surgeons National Surgical Quality Improvement Program database (2015–2021). Adults with type 2 diabetes and International Classification of Diseases, 10th Revision–coded DFUs (E11.621) undergoing elective surgery were identified and stratified into frail (mFI-5 >2) and prefrail (mFI-5 ≤2) groups. Preoperative variables, perioperative characteristics, and 30-day postoperative outcomes were compared using univariate tests, followed by multivariable logistic regression adjusting for clinically relevant confounders. The study design, reporting, and analysis followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for observational cohort studies.
Results:
Among 2,819 patients, 714 (25.3%) were classified as frail. Frail patients had significantly higher rates of overall complications (50.6% vs. 32.9%), mortality (4.1% vs. 1.6%), and medical complications, including reintubation and urinary tract infection. In adjusted models, frailty independently predicted any postoperative complication (odds ratio [OR] = 1.34, 95% confidence interval [CI] 1.05–1.70, p = 0.02) and medical complications (OR = 1.53, 95% CI: 1.12–2.07, p = 0.007).
Innovation:
This is the first large-scale study applying the mFI-5 to DFU surgery, demonstrating that frailty provides prognostic information beyond traditional comorbidity-based assessments and offers a rapid, objective tool for perioperative risk evaluation.
Conclusion:
Frailty, as measured by the mFI-5, independently predicts postoperative morbidity and mortality after DFU surgery. Incorporating preoperative frailty screening may improve surgical decision making, resource allocation, and enhance outcomes in this high-risk population.
Keywords
INTRODUCTION
Diabetes is a complex metabolic disorder projected to affect nearly 650 million people by 2040. 1 It significantly impairs wound healing through mechanisms such as poor circulation, neuropathy, and hyperglycemia, resulting in chronic wounds in approximately 25% of diabetic patients. 2 In addition, diabetes promotes a pro-inflammatory milieu and oxidative stress through the accumulation of advanced glycation end-products and epigenetic dysregulation, contributing to adverse perioperative outcomes.3–5 In the context of foot and ankle surgery, diabetic patients face markedly elevated infection rates, with each 1% increase in glycated hemoglobin correlating with a 5% rise in the overall risk of complications.6,7 Accordingly, preoperative health assessment in diabetic patients is crucial to mitigate surgical risks. 8
Adriana C. Panayi, MD, PhD

Diabetic foot ulcers (DFUs), in particular, are linked to high morbidity and complex comorbidities that complicate recovery. 9 These ulcers often lead to severe complications such as infections, hospitalizations, and amputations. More than half of DFUs become infected, and approximately 20% of moderate to severe infections ultimately necessitate some degree of amputation. 10
Frailty, defined as a state of increased vulnerability due to cumulative physiological decline, has emerged as a critical factor in perioperative risk assessment. This is especially pertinent in diabetic populations, where aging-related decline is often accelerated. Frailty has been shown to independently predict postoperative complications, offering a multidimensional assessment of surgical resilience.11–13 The Five-Item Modified Frailty Index (mFI-5)—comprising diabetes, hypertension, congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), and functional dependency—was developed as a concise tool to quantify frailty. 14 Its brevity and reliance on routinely available clinical data make it well-suited for integration into standard preoperative risk stratification, particularly in high-throughput or resource-constrained surgical environments.15–18 However, the specific impact of frailty on outcomes in DFU surgery remains underexplored.
Understanding the link between frailty and postoperative outcomes in diabetic patients could enable better preoperative counseling, risk stratification, and collaborative decision making between surgeons and patients. Identifying individuals at high risk of developing complications allows for targeted interventions and more efficient health care resource allocation, potentially lowering complication rates. Moreover, personalized perioperative care pathways for frail individuals—who are particularly susceptible to infections, wound dehiscence, and organ dysfunction due to diminished physiological reserves—could improve recovery and long-term outcomes.19–22
Despite extensive evidence linking frailty to adverse outcomes across a wide range of surgical disciplines, its role in DFU surgery has not yet been investigated. Patients undergoing surgery for DFUs represent a uniquely vulnerable population marked by multimorbidity, chronic infection, impaired mobility, and high risk of recurrent hospitalization. To our knowledge, no prior study has applied the mFI-5 to this surgical cohort to quantify the incremental risk attributable to frailty beyond traditional comorbidity profiles. This study, therefore, addresses a significant gap by evaluating the prognostic significance of frailty specifically in patients undergoing surgical management of DFUs. The aim is to provide clinicians with a practical and evidence-based tool for identifying high-risk patients, thereby improving preoperative planning, guiding informed consent processes, and enabling tailored interventions to support optimal recovery in this vulnerable population.
CLINICAL PROBLEM ADDRESSED
DFUs represent one of the most debilitating complications of diabetes, frequently necessitating surgical intervention and contributing substantially to morbidity, health care costs, and limb loss. Surgical management of DFUs is complicated by impaired wound healing, infection, and multiple comorbidities common in diabetic patients. Despite these risks, perioperative risk stratification in this population remains limited, as traditional scoring systems often fail to capture the cumulative physiological decline characteristic of frailty. This study addresses the critical clinical need to identify vulnerable DFU patients at heightened risk for postoperative complications by evaluating frailty—quantified using the mFI-5—as a simple, objective, and clinically applicable predictor to improve surgical decision making and outcomes.
MATERIALS AND METHODS
Data source
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) is a high-volume, risk-adjusted, outcomes-based clinical database widely utilized to assess surgical quality. It has been employed extensively to evaluate risk factors and postoperative complications across a broad range of surgical procedures.23–30 The database contains standardized clinical data on preoperative comorbidities, intraoperative variables, and 30-day postoperative outcomes, collected from more than 700 participating hospitals.
Trained Surgical Clinical Reviewers abstract data directly from the medical records of randomly selected patients, ensuring consistency and accuracy. In addition, ACS-NSQIP performs regular audits to identify and correct discrepancies, thereby maintaining high data integrity. Given the de-identified nature of the data, this study was classified as nonhuman subject research by Yale University’s Institutional Review Board (#2000036340).
Patient selection
We analyzed data from the ACS-NSQIP database for the years 2015–2021. Although earlier data are available, this time frame was selected because the International Classification of Diseases, 10th Revision (ICD-10) code E11.621 (“Type 2 diabetes mellitus with foot ulcer”)—used to identify DFU cases—was only implemented and consistently recorded starting in 2015. The ACS-NSQIP database includes only adult patients (≥18 years).
Patients were included in this analysis if their ICD-10 primary diagnosis (“PODIAG10” variable) was E11.621, “Type 2 diabetes mellitus with foot ulcer.” This ICD-10 code specifically identifies patients with type 2 diabetes; therefore, by definition, all patients included in this cohort had type 2 diabetes. The ACS-NSQIP database does not differentiate between type 1 and type 2 diabetes in its comorbidity variables; however, the use of ICD-10 code E11.621 ensures that only patients with type 2 diabetes were captured. We then screened for surgical procedures relevant to DFU management using predefined Current Procedural Terminology (CPT) codes. Only cases corresponding to one or more of the following procedural categories were retained for analysis: Amputation/Disarticulation, Debridement, Bypass, Graft, Revascularization, Gastrocnemius Recession, Flap, Decompression, Tenotomy, Negative Pressure Wound Therapy, and Thromboendarterectomy. Cases not matching any of these categories were excluded to ensure procedural relevance and clinical comparability. A comprehensive list of CPT codes and their category assignments is provided in Supplementary Table S1.
Subsequently, the following exclusion criteria were applied: (i) incomplete or inaccurate procedural coding (e.g., missing or nonspecific CPT codes); (ii) missing data required for calculation of the mFI-5; (iii) absence of 30-day postoperative follow-up data; and (iv) nonelective procedures.
Two investigators (F.J.K. and S.K.) independently reviewed the automatically extracted NSQIP cases to verify coding-based eligibility (ICD-10 E11.621 and relevant CPT codes). Any discrepancies regarding coding-based inclusion criteria were resolved by a third investigator (A.C.P.). After applying all inclusion and exclusion criteria, the final study cohort comprised 2,810 adult patients with confirmed diabetes who underwent elective surgical treatment for DFUs between 2015 and 2021 (Fig. 1).
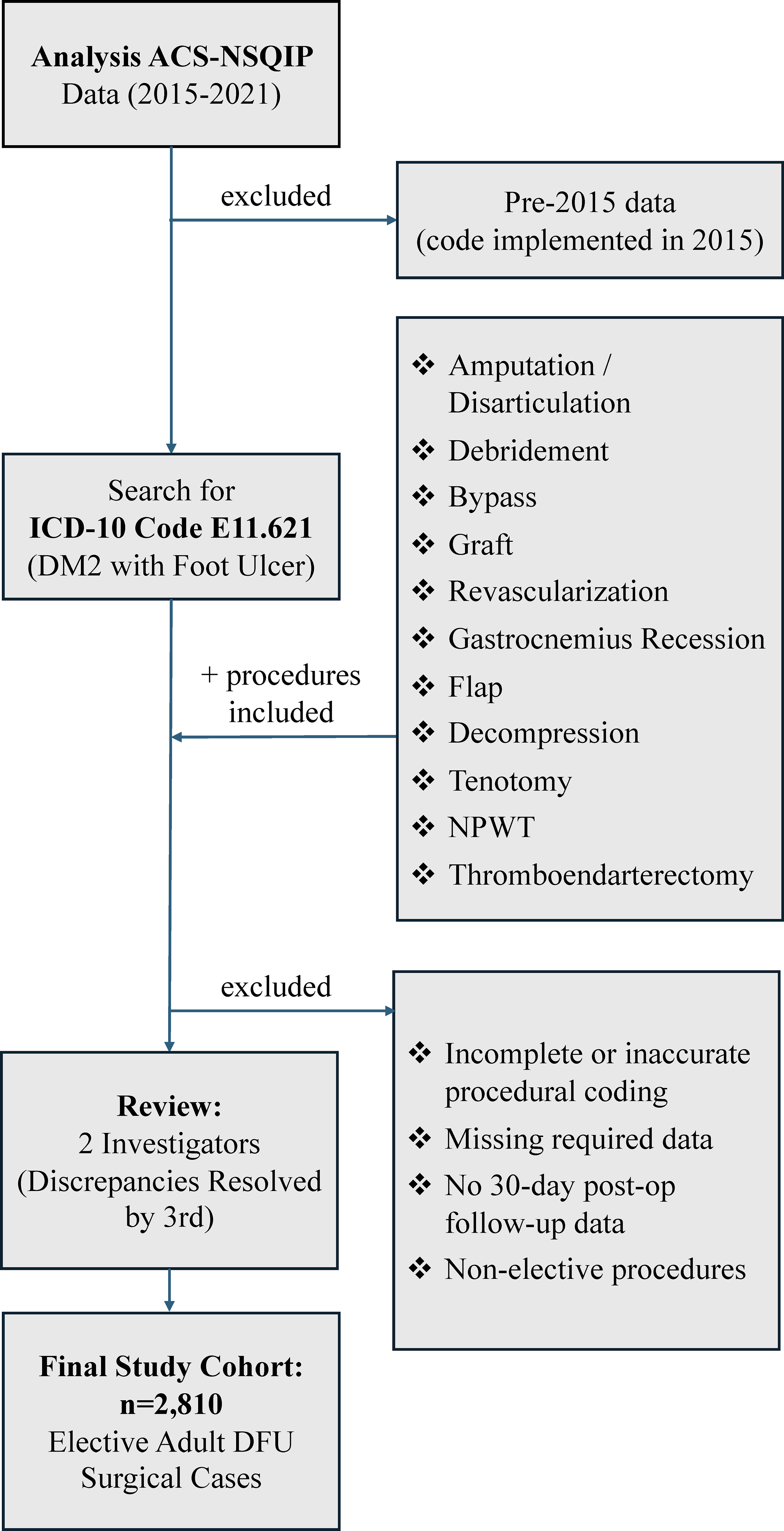
Summary graphic of study design for the analysis of patients with diabetic foot ulcers undergoing elective surgery from 2015 to 2021. Flow diagram outlining inclusion and exclusion criteria for identifying the final study cohort of patients undergoing elective surgery for diabetic foot ulcers. ACS-NSQIP, American College of Surgeons National Surgical Quality Improvement Program; DFU, diabetic foot ulcer; DM2, diabetes mellitus type 2; ICD-10, International Classification of Diseases, 10th Revision; NPWT, negative pressure wound therapy.
Variable extraction
We collected patient demographics, including age, body mass index (BMI), self-identified race (American Indian or Alaskan Native, Asian, Native Hawaiian or Pacific Islander, Black or African American, White, and other/unknown), and Hispanic ethnicity. We also extracted comorbidities, including those required to calculate the mFI-5: diabetes, hypertension, CHF, COPD, and functional dependency (Fig. 2). Based on the calculated mFI-5 value, patients were stratified into frail (mFI-5 >2) and prefrail (mFI-5 ≤2). This stratification is supported by prior evidence showing that an mFI-5 score >2 is independently associated with increased risk of postoperative complications, mortality, prolonged length of stay, nonhome discharge, and other adverse outcomes across diverse surgical cohorts.12,13,22,31,32 Of note, because diabetes is one of the five variables included in the mFI-5, all patients in this cohort had a minimum mFI-5 score of one. In addition, we assessed insulin dependence, obesity, dialysis, renal insufficiency, ascites, dyspnea, smoking status within the past year, corticosteroid use, weight loss greater than 10% in the 30 days prior to surgery, disseminated cancer, bleeding disorders, preoperative transfusion of ≥1 unit of blood within 72 h prior to surgery, wound infection, and history of sepsis. Functional health status was recorded as independent, partially or totally dependent, or unknown. We further evaluated preoperative scores, including the American Society of Anesthesiologists physical status classification (scores 1–5 and unknown) and wound classification (clean, clean/contaminated, contaminated, dirty/infected, and unknown). BMI was calculated as weight in pounds divided by height in inches squared and multiplied by 703, with values ≥30 kg/m2 indicating obesity. Perioperative data included length of hospital stay (calculated as the difference in days between admission and discharge), operative time, surgical setting (inpatient or outpatient), and the year of surgery (2015–2021). Postoperative outcomes encompassed the incidence of any complication, reoperation, and unplanned readmission within 30 days postoperatively. Any complication was defined as a composite endpoint that included mortality, reoperation, unplanned readmission, and/or the occurrence of any surgical or medical complication. Surgical complications evaluated in accordance with ACS-NSQIP definitions included deep incisional infection, organ space infection, wound dehiscence, and bleeding/blood transfusion; no superficial incisional infections were recorded in the dataset. Medical complications captured over the 7-year review period included reintubation, pulmonary embolism, ventilator dependence for more than 48 h, progressive renal insufficiency, renal failure, urinary tract infection, stroke or cerebrovascular accident, myocardial infarction, deep vein thrombosis or thrombophlebitis, and sepsis. In addition, discharge destination was recorded and categorized as home/permanent residence, nonhome facility, or other/unknown.
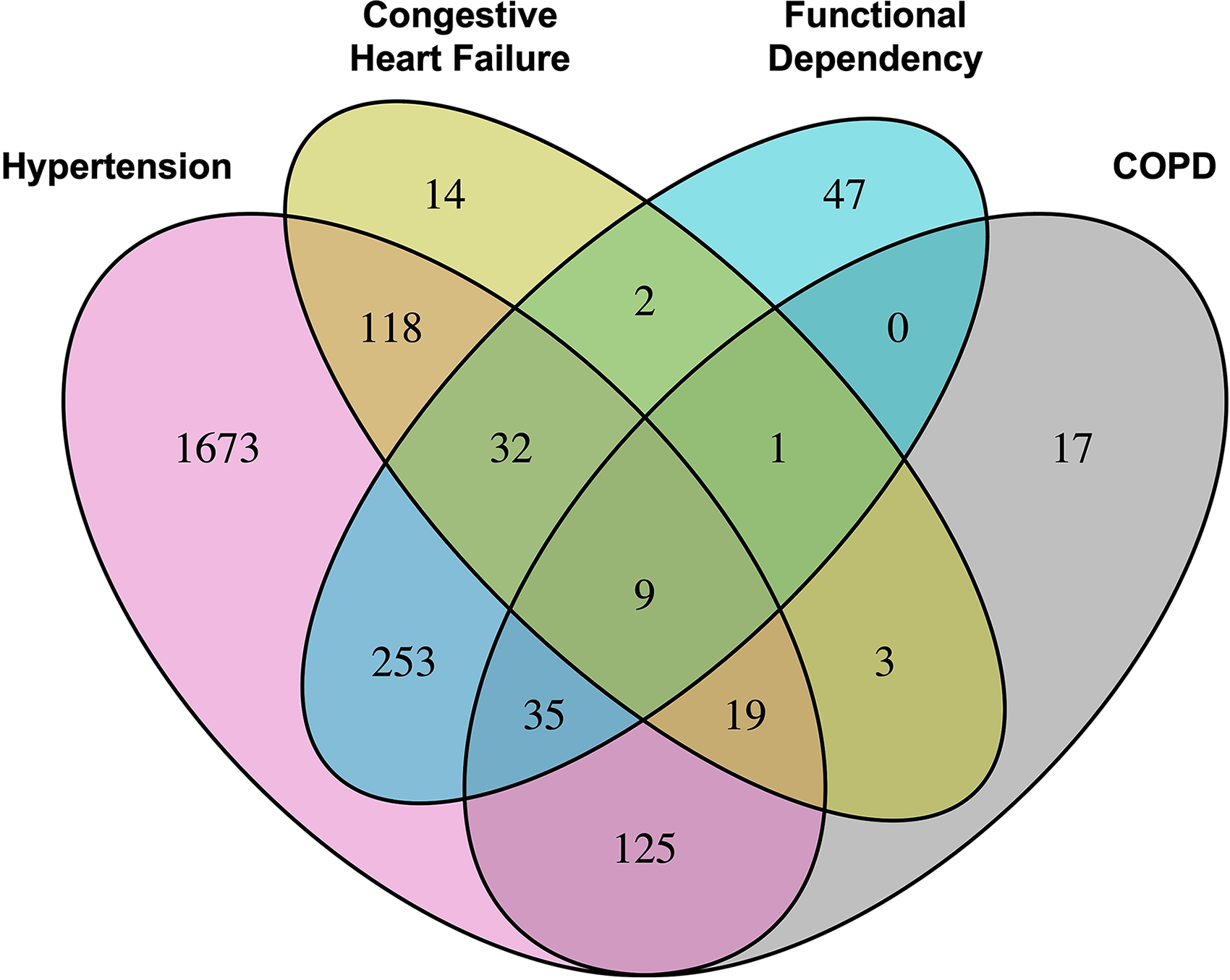
Overlap of mFI-5 frailty components in the study cohort. Venn diagram illustrating the overlap of four components of the Five-Item Modified Frailty Index (mFI-5) in patients undergoing surgery for diabetic foot ulcers. Diabetes was excluded from the diagram as all patients in the study cohort had diabetes by definition. A total of 2,819 patients were included, of whom 2,105 were classified as low frailty risk (mFI-5 ≤2) and 714 as high frailty risk (mFI-5 >2). COPD, chronic obstructive pulmonary disease.
Statistical analysis
The raw data were converted to Microsoft Excel files (V.16; Microsoft Corporation, Redmond, WA) through SPSS for Windows (V.29; IBM Corporation, Armonk, NY). The data were stored in an electronic laboratory notebook (LabArchives, LLC, San Marcos, CA) and analyzed using the R statistical software (V. 4.1.2). Categorical data are presented as absolute numbers (n) and percentages (%), and continuous variables as mean ± standard deviation for all patients, as well as those with and without obesity. Risk factors for overall, surgical, and medical complications were evaluated exploratory using two-sample t-tests for continuous variables and Fisher’s exact test or chi-square test for categorical variables as indicated. A significance level of p < 0.05 was assumed, and significance correction using the Benjamini–Hochberg procedure for multiple testing was performed when indicated. Multivariable logistic regression models were constructed using frailty (defined as mFI-5 >2) as the primary independent variable to assess the association between frailty and postoperative outcomes. Separate models were developed for the outcomes of any complication, surgical complications, and medical complications. Each model was adjusted for a predefined set of potential confounding variables based on clinical relevance and prior literature. These included age, obesity, smoking status, COPD, CHF, hypertension requiring medication, chronic steroid use, bleeding disorders, renal failure, and dialysis dependency. Odds ratios (ORs) with 95% confidence intervals (CIs) and corresponding p-values were reported. Model fit was assessed using the Hosmer–Lemeshow goodness-of-fit test, with p > 0.05 indicating adequate calibration.
RESULTS
Preoperative patient demographics and health characteristics
In our cohort of 2,819 patients undergoing DFU surgery, patients classified as frail (mFI-5 >2, n = 714) differed significantly from prefrail patients (mFI-5 ≤2, n = 2,105) across several demographic and preoperative characteristics. Analysis of the mFI-5 components revealed that, besides diabetes, which was present in all patients by definition, hypertension was the most prevalent condition, followed by COPD, functional dependency, and CHF. When comparing the two groups, frail patients were significantly older (65.2 ± 10.8 years vs. 59.4 ± 11.8 years, p < 0.001) and exhibited higher incidences of insulin-treated diabetes (82.5% vs. 74.0%, p < 0.001), COPD (29.3% vs. 0.0%, p < 0.001), CHF (27.7% vs. 0.0%, p < 0.001), dialysis (18.5% vs. 10.3%, p < 0.001), renal insufficiency (5.0% vs. 2.7%, p = 0.01), hypertension (87.1% vs. 78.0%, p < 0.001), dyspnea (19.3% vs. 6.0%, p < 0.001), significant weight loss (2.8% vs. 1.0%, p = 0.003), bleeding disorders (27.3% vs. 15.6%, p < 0.001), preoperative transfusions (7.1% vs. 4.5%, p = 0.02), and functional dependence (53.1% vs. 0.0%, p < 0.001). BMI did not differ significantly between frail and prefrail patients (32.3 ± 8.6 vs. 32.0 ± 7.8 kg/m2, p > 0.99), indicating no measurable association between BMI and frailty status in this DFU surgical cohort. Further details can be found in Table 1. Figure 3 provides a comparison of variables that were significantly different between the two groups.
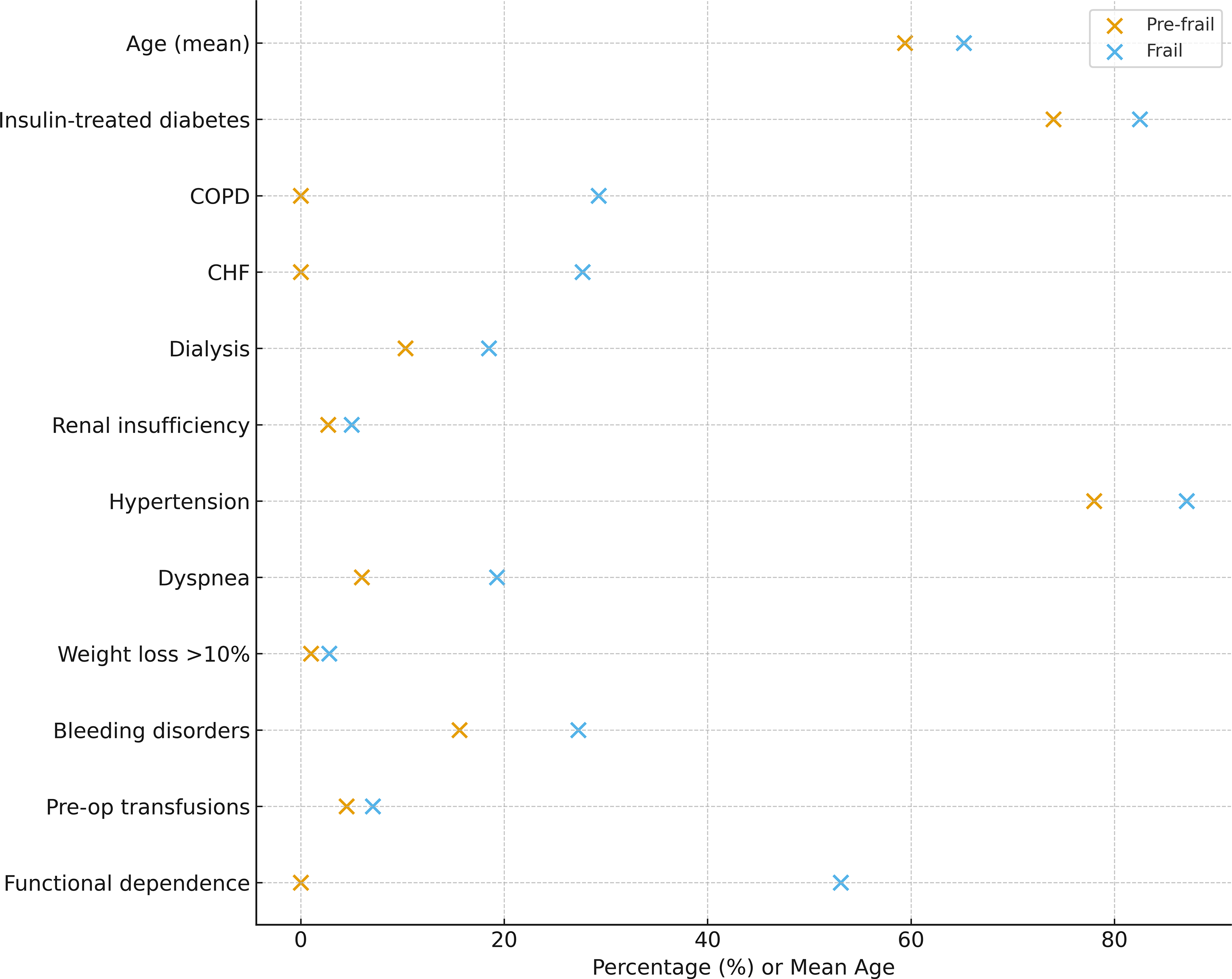
Demographic and preoperative variables differ significantly between prefrail and frail patients. Dot-plot illustrating all demographic and preoperative health variables that differed significantly between prefrail and frail patients undergoing surgery for diabetic foot ulcers (p < 0.05 after Benjamini–Hochberg correction). Each point represents the percentage of patients in each frailty group (or mean value for age). Frail patients exhibited a higher prevalence of multiple comorbidities, including insulin-treated diabetes, chronic obstructive pulmonary disease (COPD), congestive heart failure (CHF), dialysis dependence, renal insufficiency, hypertension, dyspnea, >10% unintentional weight loss, bleeding disorders, preoperative transfusions, and functional dependence. Prefrail patients demonstrated lower rates across these parameters.
Demographics and preoperative health characteristics of all patients undergoing diabetic foot ulcer surgery
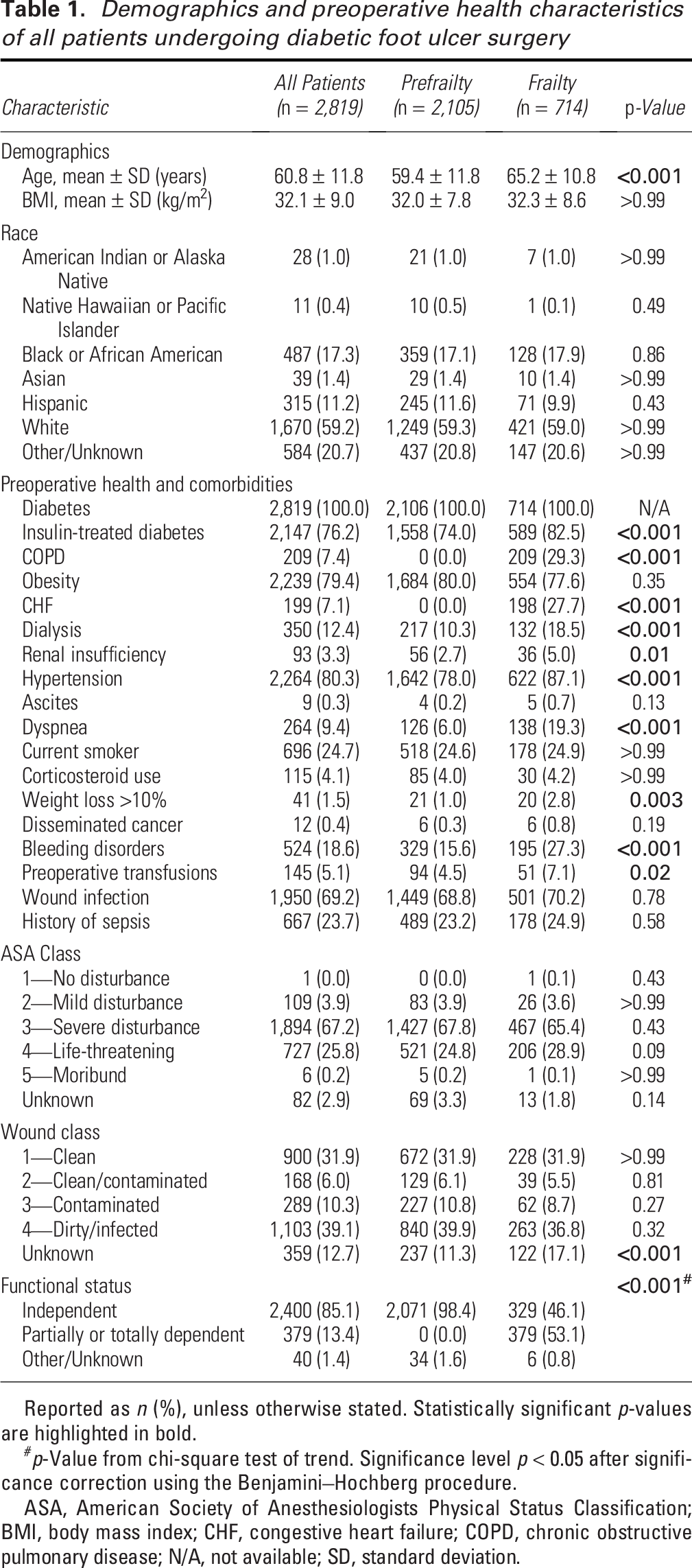
Reported as n (%), unless otherwise stated. Statistically significant p-values are highlighted in bold.
p-Value from chi-square test of trend. Significance level p < 0.05 after significance correction using the Benjamini–Hochberg procedure.
ASA, American Society of Anesthesiologists Physical Status Classification; BMI, body mass index; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; N/A, not available; SD, standard deviation.
Surgical characteristics
Analysis of perioperative characteristics (Supplementary Table S2) revealed that frail patients were significantly more likely to undergo surgery in an inpatient setting compared with those with low frailty risk (642 of 714, 89.9% vs. 1,791 of 2,105, 85.1%, p = 0.004). Furthermore, a significant difference was observed in the distribution of surgeries by year (p = 0.004), with a notably higher proportion of frail patients undergoing surgery in 2021 (122 of 714, 17.1% vs. 237 of 2,105, 11.3%). When stratified by frailty status, significant differences also emerged in the distribution of surgical procedures performed for DFU management (Table 2). Amputations or disarticulations were more frequently performed in frail patients, with 386 of 714 patients (54%) undergoing these procedures compared with 972 of 2,105 patients (46%) in the low frailty risk group (p < 0.001). Conversely, debridement procedures were more common among prefrail patients, performed in 783 of 2,105 patients (37%) versus 201 of 714 patients (28%) in the frail group (p < 0.001). Flap procedures, though infrequent overall, were significantly more common in the frail group (7 of 714, 0.98%) compared with the prefrail group (6 of 2,105, 0.29%; p = 0.04). Similarly, tenotomies were more commonly performed in prefrail patients (40 of 2,105, 1.9%) than in those with frailty (5 of 714, 0.70%; p = 0.04). Importantly, there were no significant differences in the rates of revascularization procedures between frail and prefrail groups (17% vs. 16%, p = 0.59), nor in bypass procedures (4.2% vs. 5.7%, p = 0.20), indicating that the increased complication rates among frail patients were not attributable to a higher frequency of combined vascular inflow–restoring operations.
Overview of performed surgical procedures
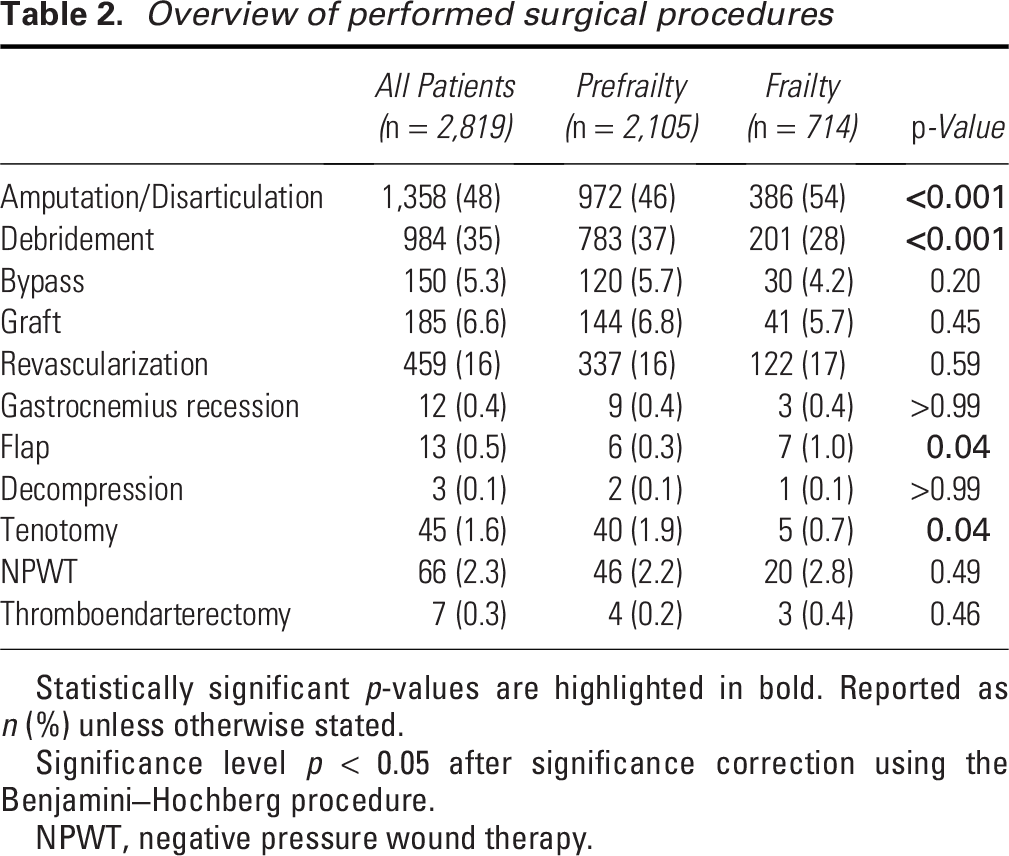
Statistically significant p-values are highlighted in bold. Reported as n (%) unless otherwise stated.
Significance level p < 0.05 after significance correction using the Benjamini–Hochberg procedure.
NPWT, negative pressure wound therapy.
Postoperative outcomes
Patients classified as frail experienced significantly higher rates of overall complications compared with those who were prefrail (50.6% vs. 32.9%, p < 0.001, Table 3). Mortality was also increased among frail patients (4.1% vs. 1.6%, p = 0.003), as were overall surgical complications (24.4% vs. 19.1%, p = 0.003). Within specific complication types, wound dehiscence occurred less frequently in frail patients (0.4% vs. 1.8%, p = 0.03), while reintubation events were more common (2.1% vs. 0.7%, p = 0.02). In addition, urinary tract infections were more frequent among frail individuals (2.1% vs. 0.9%, p = 0.049). Discharge destination differed significantly by frailty status (p = 0.02), with frail patients more often discharged to nonhome facilities (40.8% vs. 35.4%). Looking specifically at the two most common procedures, debridement and amputation, patients undergoing amputation demonstrated slightly higher complication and mortality rates than those undergoing debridement, underscoring the elevated perioperative risk associated with more extensive procedures, as shown in Supplementary Table S3.
Operative and postoperative outcomes following diabetic foot ulcer surgery
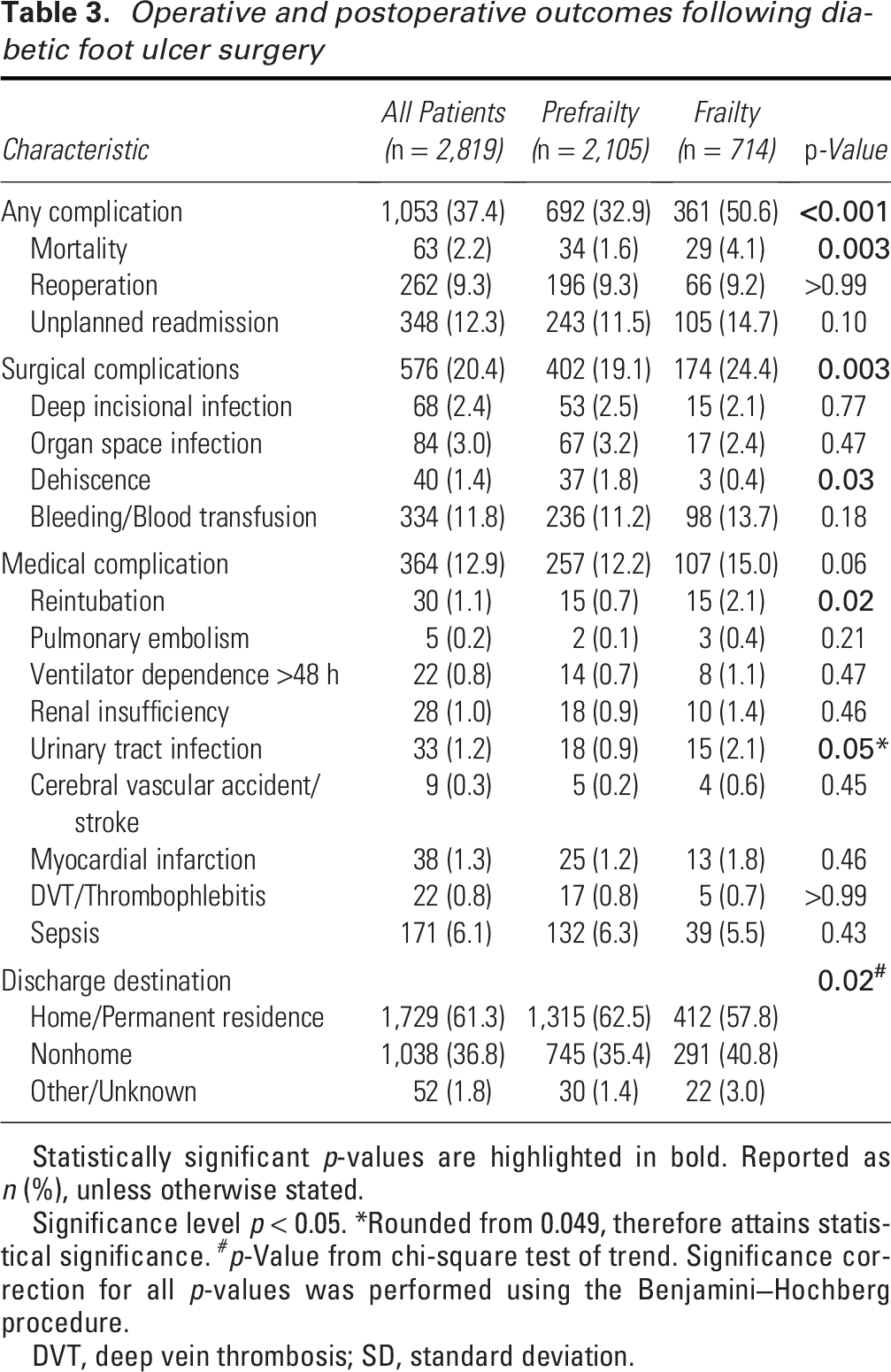
Statistically significant p-values are highlighted in bold. Reported as n (%), unless otherwise stated.
Significance level p < 0.05. *Rounded from 0.049, therefore attains statistical significance. #p-Value from chi-square test of trend. Significance correction for all p-values was performed using the Benjamini–Hochberg procedure.
DVT, deep vein thrombosis; SD, standard deviation.
Multivariate analysis
Multivariate logistic regression analysis identified frailty as a significant independent predictor of postoperative complications (Supplementary Table S4). Patients classified at high risk of frailty had a 34% higher risk of experiencing any complication compared with prefrail patients (OR = 1.34, 95% CI: 1.05–1.70, p = 0.02). While the association between frailty and surgical complications was not statistically significant (OR = 1.18, 95% CI: 0.89–1.55, p = 0.24), frailty was significantly associated with increased odds of medical complications (OR = 1.53, 95% CI: 1.12–2.07, p = 0.007). The model demonstrated a good fit to the data as assessed by the Hosmer–Lemeshow test (p = 0.95), indicating no significant discrepancy between predicted and observed outcomes.
DISCUSSION
The ACS-NSQIP database has been used in previous studies on wound care topics. Multiple studies have utilized ACS-NSQIP data to evaluate surgical site infections, wound classification, and the impact of quality improvement interventions on wound-related outcomes.33–36 For example, Ortega et al. conducted a large cross-sectional analysis of surgical site infection rates by wound classification using ACS-NSQIP data. 34 Gandaglia et al. utilized the ACS-NSQIP database to evaluate the impact of minimally invasive surgery on the risk of surgical site infections. 35 In addition, Berenguer et al. analyzed ACS-NSQIP data to assess the impact of implementing Surgical Care Improvement Project protocols on surgical site infection rates. 36 These studies demonstrate that the ACS-NSQIP database is a well-established resource for research on wound care and related surgical outcomes.
In this retrospective cohort study of more than 2,800 patients undergoing elective surgery for DFUs, we found that frail patients, defined by an mFI-5 score of >2, experienced significantly higher rates of postoperative complications, particularly medical complications, as well as higher mortality. In addition, frail patients were significantly more likely to require discharge to nonhome facilities, which has been used as a surrogate measure of impaired functional recovery and may contribute to decreased outpatient follow-up adherence. Notably, while surgical complications were more frequent in the frail cohort, the difference did not reach statistical significance. These findings underscore the importance of frailty as a clinically meaningful determinant of short-term surgical outcomes in patients with DFUs.
This study adds several novel insights to the growing literature on frailty in surgical populations. While frailty has been consistently associated with negative outcomes in general, vascular, and orthopedic surgery, its impact on patients undergoing DFU surgery has not been characterized previously. DFU surgery represents a distinct clinical phenotype, with disproportionately high rates of infection, impaired perfusion, functional dependence, and readmission. By applying the mFI-5 to this specific cohort, we demonstrate for the first time that frailty remains a strong and independent predictor of postoperative morbidity, mortality, and health care utilization in this high-risk population. These results expand the clinical relevance of frailty assessment into the domain of limb salvage and diabetic wound care, where risk stratification tools are urgently needed.37,38
Patients with DFUs represent a high-risk surgical population characterized by complex comorbidities and diminished physiological reserve—hallmarks of frailty. 39 Given this inherent vulnerability, the integration of a validated, easy-to-calculate frailty assessment tool such as the mFI-5 is of particular clinical value. While some authors have proposed more granular stratifications, distinguishing between nonfrail (mFI-5 = 0), prefrail (mFI-5 = 1–2), and frail (mFI-5 >2) individuals,40–42 this approach was not feasible in our study. Because diabetes is a required component of the mFI-5, all patients in a DFU study would have a minimum score of 1, thereby eliminating the “nonfrail” (score 0) category and compressing the score distribution toward higher frailty. This pattern reflects the well-established multimorbidity and functional impairment characteristic of DFU populations, in whom most patients accumulate multiple frailty deficits.43,44 Within this constrained score range, a binary cutoff of mFI-5 >2 versus ≤2 has been repeatedly validated in large ACS-NSQIP surgical cohorts—including gastric cancer, spine surgery, neurosurgical, and colorectal populations—as a clinically meaningful threshold associated with significantly increased morbidity and mortality.14,40,45,46 Studies in DFU and major lower-extremity amputation populations similarly demonstrate that an mFI-5 score >2 identifies patients at disproportionately elevated risk for postoperative complications, nonhealing, readmission, and mortality, even within uniformly comorbid diabetic groups.43,47 These findings underscore that the prognostic value of the mFI-5 remains robust despite the compressed score distribution inherent to DFU cohorts. Nevertheless, more granular stratification across the full score range may have added discriminatory value in surgical populations with greater baseline heterogeneity, and future prospective DFU-specific studies should evaluate whether finer categorization meaningfully improves risk prediction, clinical decision making, and individualized perioperative management. 47
Our findings align with a growing body of literature demonstrating the prognostic utility of the mFI-5 across various surgical populations. Prior studies have validated the mFI-5 in oncologic, orthopedic, and vascular procedures, consistently linking higher frailty scores with increased morbidity and mortality. In oncologic surgery, the mFI-5 has been shown to independently predict postoperative complications, mortality, and adverse outcomes in patients undergoing procedures such as mastectomy, 12 breast-conserving surgery, 30 gynecologic oncology operations, 22 and rectal and lung cancer resections. 32 Higher mFI-5 scores were found to be associated with increased rates of severe complications, nonhome discharge, and mortality in these populations. In orthopedic surgery, particularly in geriatric hip fracture patients and spine surgery, the mFI-5 has demonstrated strong predictive value for 30-day morbidity and mortality, with each point increase in the index correlating with a significant rise in risk for complications and death. 48 Regarding vascular procedures, systematic reviews and meta-analyses have confirmed frailty to be associated with increased 30-day and long-term mortality, as well as higher rates of postoperative complications. 49 However, to our knowledge, this is the first large-scale analysis to apply the mFI-5 to DFU surgery, a vulnerable population characterized by complex comorbidity profiles and impaired wound healing.
Beyond its predictive value for postoperative complications, frailty may biologically potentiate poor outcomes in DFU patients through impaired immunologic and wound healing mechanisms. Frail individuals often experience chronic inflammation, sarcopenia, and immune dysregulation—factors that are already prevalent in the diabetic population and known to impede wound healing. Chronic inflammation in frailty leads to impaired growth factor expression, increased catabolism, and attenuated immune responses, which together compromise tissue repair and increase susceptibility to infection. Sarcopenia further limits mobility and functional recovery, exacerbating the risk of nonhealing ulcers. 50 In DFU pathology, however, neuropathy and neuroischemia represent additional central determinants of disease severity, wound healing potential, and postoperative outcomes.37,38 Sensory neuropathy contributes to loss of protective sensation, recurrent trauma, and ulcer persistence, while underlying ischemia reduces perfusion and increases the risk of infection, delayed healing, and limb loss.51,52 These neurovascular impairments may interact with frailty by compounding functional limitations and reducing physiologic reserve, thereby intensifying postoperative vulnerability. Although these mechanisms are highly relevant, the ACS-NSQIP dataset does not capture measures of neuropathy, arterial perfusion, or neuroischemic ulcer severity (e.g., ABI, toe pressures, Wound, Ischemia, and foot Infection [WIfI] staging), preventing formal adjustment for these factors and representing an important limitation of the present analysis. Moreover, frailty is characterized by multisystem impairment, including undernutrition and sarcopenia, which limit the ability to maintain homeostasis under stress and are associated with poor surgical outcomes, increased risk of infection, and organ dysfunction in the perioperative setting.53,54 In the context of DFUs, frailty is highly prevalent and independently predicts nonhealing, readmission, and increased morbidity, with nutritional deficits and reduced reserve compounding these risks. 43 Recent studies also suggest that frailty is associated with delayed leukocyte recruitment and impaired angiogenesis, both of which are critical for ulcer resolution and tissue regeneration.50,55 The biology of frailty involves chronic inflammation, immune dysregulation, and mitochondrial dysfunction, which collectively impair leukocyte function and angiogenic responses, thereby hindering effective wound healing and tissue repair.56,57 In the context of DFUs, where baseline immune and vascular dysfunction are already present, the combined influence of frailty and neurovascular disease further amplifies the likelihood of postoperative complications, delayed healing, readmission, and adverse outcomes. 58
Although obesity is commonly linked to functional decline and may contribute to components of physiologic frailty in other surgical populations, 59 we did not observe a measurable association between BMI and frailty status in this cohort. BMI values were nearly identical between frail and prefrail individuals, with no statistically significant difference. This likely reflects the uniformly high prevalence of obesity among patients with DFUs, which compresses the BMI distribution and limits its discriminatory ability as a frailty-related variable. In addition, BMI alone does not capture body composition abnormalities such as sarcopenic obesity, loss of lean mass, or altered metabolic reserve—factors more directly implicated in frailty-related vulnerability.60,61 As such, while BMI is an important metabolic indicator in diabetic populations, it may be insufficient to distinguish frailty phenotypes within the context of advanced diabetic foot disease.
These findings carry significant clinical implications. First, they suggest that routine frailty assessment using the mFI-5 could improve preoperative risk stratification in patients with DFUs. Given its simplicity and reliance on readily available clinical variables, the mFI-5 is well-suited for busy surgical settings and may facilitate targeted perioperative planning. Surgeons may use this tool to engage in shared decision making, consider prehabilitation strategies, or implement enhanced postoperative monitoring for frail patients. In addition, recognition of frailty may prompt involvement of multidisciplinary teams, including endocrinology, geriatrics, and rehabilitation services, to mitigate risks and optimize recovery.
The strengths of this study include its large sample size, rigorous case selection, and use of a nationally validated, prospectively collected surgical database. Furthermore, by focusing on elective cases and adjusting for key covariates in multivariate modeling, we sought to isolate the independent contribution of frailty to adverse outcomes. The consistency of our findings with prior literature across various surgical subspecialties strengthens their external validity and highlights the robustness of the mFI-5 as a predictive instrument.12,13,22,30–32,49 This underscores the need for prospective studies to evaluate whether targeted interventions—such as nutritional supplementation, physiologic optimization, or immunomodulation—can mitigate these risks and improve both surgical and functional outcomes in frail patients undergoing DFU surgery. Furthermore, frailty represents only one component of a patient’s overall vulnerability. A comprehensive assessment of risk in individuals undergoing surgery should ideally incorporate additional quality-of-life dimensions that frequently accompany frailty, including baseline mobility, psychosocial well-being, functional independence, and patient-reported measures of daily activity and perceived health. 62
Several limitations should be considered when interpreting the findings of this study. First, the analysis relies on data from the ACS-NSQIP database, which, although robust and standardized, may not capture critical variables specific to DFU surgery, such as wound severity, presence of osteomyelitis, vascular status, or details of operative technique and surgeon expertise, which are established predictors of healing, amputation, and mortality. Prior studies incorporating these parameters—such as the WIfI classification system and other DFU-specific scoring models—have demonstrated their strong prognostic value for limb salvage and wound healing outcomes.37,38 In addition, it also lacks direct quality-of-life measures (e.g., mobility assessments, PROMIS, EQ-5D), which limits our ability to evaluate the relationship between frailty and patient-centered outcomes beyond the functional proxies available in the dataset. Second, the database includes data primarily from U.S. hospitals, which may limit the generalizability of our findings to international health care settings with differing standards of care and resource availability. Third, while our study identified associations between frailty and postoperative complications, the retrospective and observational design precludes causal inference. We attempted to mitigate confounding through multivariable logistic regression and assessed model calibration using the Hosmer–Lemeshow goodness-of-fit test; however, residual confounding and selection bias may persist. Fourth, because diabetes is a component of the mFI-5, all patients in our cohort had a minimum frailty score of 1, thereby precluding comparisons with a truly nonfrail (mFI-5 = 0) reference group. As a result, our findings reflect differences between prefrail and frail patients, which may limit generalizability to broader surgical populations. Fifth, the database lacks information on patient-centered outcomes such as functional recovery, wound healing rates, and limb salvage, which are particularly important in DFU management. Furthermore, the NSQIP only captures complications occurring within 30 days postoperatively, limiting insight into long-term outcomes such as ulcer recurrence, reoperation, or amputation beyond the immediate postoperative period. In addition, our cohort was defined using ICD-10 code E11.621 (“Type 2 diabetes mellitus with foot ulcer”), which is specific to type 2 diabetes. As a result, the study population consists exclusively of patients with type 2 diabetes, limiting the generalizability of the findings to individuals with type 1 diabetes. Last, although interaction analyses may provide additional insight into more heterogeneous surgical populations, such analyses are challenging in DFU cohorts, where frailty and its component comorbidities are highly correlated and outcome distributions are compressed; consequently, formal interaction testing may yield statistically unstable estimates without meaningfully enhancing clinical interpretability. Future studies with larger sample sizes and broader distributions of baseline health status may be better positioned to assess effect modification among frailty-related factors.
In conclusion, our findings demonstrate that frailty, as indicated by an mFI-5 score >2, is a significant independent predictor of postoperative complications in patients undergoing surgery DFUs. Frail patients experienced notably higher rates of overall and medical complications, even after controlling for relevant comorbidities. These results highlight the importance of integrating frailty assessments into preoperative risk stratification protocols, particularly in high-risk populations such as diabetics with foot ulcers. Identifying frail individuals preoperatively may allow for tailored perioperative care and optimization strategies aimed at reducing complications and improving outcomes. Future prospective studies are warranted to validate these findings and to explore whether interventions targeting frailty can mitigate surgical risk in this vulnerable group.
Innovation
Frailty has been increasingly recognized as a determinant of surgical outcomes, yet its relevance to DFU surgery has not been systematically explored. This study is the first large-scale analysis to apply the mFI-5 to DFU surgery, demonstrating that frailty independently predicts postoperative complications and mortality. By quantifying vulnerability beyond traditional comorbidities, the mFI-5 enables surgeons to identify high-risk patients using readily available clinical data. Integrating frailty screening into preoperative workflows offers an innovative, pragmatic tool to optimize perioperative care and improve surgical outcomes in diabetic wound management.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The authors declare that they have no funding sources or financial support to disclose for this study.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. All authors confirm that no ghostwriters were used in the preparation of this article. Each author contributed substantially to the study’s conception, data analysis, and article drafting and approves the final version for submission.
ETHICAL APPROVAL/INFORMED CONSENT
IRB Protocol ID: 2000035387, Yale School of Medicine, New Haven, CT.
ABOUT THE AUTHORS
Supplemental Material
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.