
Abstract
Significance:
Diabetic foot ulcers (DFUs) represent one of the most devastating complications of diabetes, leading to high rates of amputation and mortality. Their multifactorial pathogenesis—including neuropathy, ischemia, infection, and immune dysfunction—creates a chronic inflammatory microenvironment that impairs tissue repair and regeneration.
Recent Advances:
Emerging regenerative strategies using stem cells and extracellular vesicles (EVs) have demonstrated potential to restore vascularization and modulate inflammation. In particular, miRNA-enriched EVs regulate key wound-healing pathways such as angiogenesis, extracellular matrix remodeling, and oxidative stress response. Meanwhile, small-molecule drugs targeting hypoxia and inflammatory cascades are being explored to enhance re-epithelialization and fibroblast migration. Parallel advances in artificial intelligence (AI) and optical sensing—using visible, infrared, or hyperspectral imaging—enable automated wound detection, tissue classification, and healing prediction with high accuracy.
Critical Issues:
Despite these developments, translation remains limited by unstable therapeutic efficacy, variable biomarker expression, and the absence of standardized evaluation systems. AI-based wound assessment requires robust datasets and clinical validation to ensure reliability across diverse populations.
Future Directions:
Integrating molecular-targeted therapies with AI-assisted diagnostic platforms could establish a next-generation DFU management framework—combining precise molecular intervention, automated wound monitoring, and personalized treatment planning—to achieve reliable, real-time, and patient-centered wound care.
INTRODUCTION
Wound healing involves four overlapping stages—hemostasis, inflammation, proliferation, and remodeling—but chronic wounds and burn-related pathological scars often stall in the inflammatory phase, resulting in persistent inflammation, impaired healing, and disrupted extracellular matrix (ECM) function. 1 These conditions create major global health and economic burdens; in the United States alone, over 6.7 million people suffer from chronic nonhealing wounds—including diabetic ulcers, nonhealing surgical wounds, burns, and venous ulcers—imposing more than $25 billion in annual health care costs. 2 Current wound assessment relies largely on visual inspection, while infection diagnosis depends on swab-based cultures with slow turnaround times that delay clinical decision-making. Quantitative biochemical analyses remain limited to laboratory methods such as ELISA, reducing accessibility and efficiency. As a result, existing monitoring approaches are slow, lack comprehensive profiling, and provide insufficient quantitative data to reliably predict healing trajectories in clinical practice. 3 In addition, frequent manual removal of dressings for assessment further increases the risk of infection and may cause additional trauma. To overcome these limitations, wearable wound sensor patches have emerged as a noninvasive, efficient, and comprehensive monitoring tool. In parallel, researchers are integrating molecular techniques with artificial intelligence (AI) and advanced imaging to better assess diabetic foot ulcer (DFU) severity and improve management. Early detection of infected or ischemic DFUs can reduce hospitalization and lower limb amputations (LLAs). AI methods like deep learning (DL) are trained on large datasets to offer personalized treatment recommendations. Studies show that DL outperforms traditional diagnostic methods in DFU image classification, offering better results and cost-effectiveness. 4
Hsiu-Jung Liao, PhD

Yu-Feng Wu, PhD

In refining the conceptual framework of the AI section, it became essential to shift the emphasis from theoretical constructs toward clinically substantiated applications. Although advanced ideas such as multi-omic closed-loop controllers, adaptive Bayesian therapeutic modulation, and federated learning (FL) ecosystems represent exciting future directions, these models currently remain speculative within the context of DFU care and lack prospective validation. A more clinically anchored approach therefore places focus on AI systems that have demonstrated measurable performance in real-world or near-clinical settings, including RGB-based wound segmentation, thermal anomaly detection, and hyperspectral assessment of perfusion and oxygenation.
Equally important is the recognition that algorithmic sophistication alone does not determine translational success. Practical barriers—including inconsistent ground-truth annotation, device heterogeneity across imaging platforms, variability in lighting conditions, and the known limitations of RGB imaging in the presence of necrosis, biofilm, or edema—directly influence model robustness and must be explicitly considered. Ethical and medico-legal dimensions, such as data privacy, algorithmic accountability, and equitable performance across skin tones and demographic groups, further shape the viability of AI adoption in clinical workflows.
To strengthen clinical relevance, the article now emphasizes validated performance metrics—such as sensitivity, specificity, AUC, calibration behavior, and external generalizability—rather than detailing algorithmic formulations like tensor decomposition, canonical polyadic (CP) rank-R factorization, or semi-supervised regularization strategies. Evidence shows that many models achieve high internal accuracy yet exhibit performance degradation when evaluated across different institutions, underscoring the necessity of multicenter datasets, harmonized imaging protocols, and standardized benchmarking.
By reframing AI as a clinician-supervised decision-support tool—one designed to enhance trend detection, early-risk identification, and objective documentation rather than function autonomously—this refined perspective aligns computational innovation with the practical constraints of DFU management. Collectively, these adjustments provide a more balanced, evidence-driven representation of the current landscape of AI-enabled wound assessment and delineate the methodological and clinical steps required for meaningful and safe integration into regenerative and wound-care ecosystems.
Despite the expanding repertoire of regenerative modalities and AI-assisted diagnostic platforms, the field remains constrained by a significant disconnect between technological innovation and clinical applicability. Much of the existing literature provides descriptive accounts of extracellular vesicles (EVs), hydrogel matrices, siRNA nanocarriers, or hyperspectral and thermal imaging tools, yet few studies interrogate their true clinical maturity, comparative advantages, or long-term reproducibility. The therapeutic performance of many regenerative agents remains inconsistent, often limited by unstable bioavailability, batch variability, and the absence of harmonized potency metrics. Likewise, AI-driven wound stratification models have advanced rapidly in methodological sophistication but continue to depend on narrowly sourced datasets, insufficient external validation, and limited interpretability, raising concerns regarding generalizability, algorithmic bias, and translational readiness. Contradictory findings across preclinical and clinical studies further underscore the heterogeneity of the DFU microenvironment and highlight unresolved mechanistic and operational gaps. These challenges underscore the necessity of a more rigorous and critical evaluation of each technological domain—exosomes, nanodrug delivery systems (NDDSs), direct tissue reprogramming, and AI-based analytics—through systematic appraisal of evidence strength, mechanistic limitations, regulatory barriers, and unmet clinical needs. By embedding this critical lens, the present review aims to delineate not only the promise of emerging DFU technologies but also the structural limitations that must be addressed to enable their credible, scalable, and clinically impactful translation.
EXISTING TREATMENTS FOR DIABETIC WOUNDS
Diabetic wound treatment includes debridement, wound dressings, pressure off-loading, revascularization, infection management, and general care. Sharp debridement is the preferred method but may cause pain and secondary trauma. Wound dressings help maintain a moist healing environment, though bioengineered options often face challenges such as toxicity and allergic reactions. 5 Pressure off-loading, especially with nonremovable casts, effectively reduces foot pressure and promotes recovery. Revascularization, either through medication or surgical procedures, is crucial for patients with peripheral arterial disease (PAD), which affects 40% of DFU cases. Infection management follows IDSA guidelines, emphasizing targeted antibiotic use to prevent resistance. 6 Thus, nanomaterial-based antibiotic delivery is a promising innovation. General care, including blood sugar control, blood pressure management, smoking cessation, and proper nutrition, plays a key role in improving DFU outcomes. A comprehensive, multidisciplinary approach is essential to enhance healing and prevent complications.
NANODRUG DELIVERY SYSTEMS FOR ENHANCING DIABETIC WOUND HEALING
Diabetic wound healing is a highly complex and dysregulated process that requires advanced therapeutic strategies. NDDSs offer a promising approach to improve the efficacy, stability, and targeted delivery of bioactive molecules, addressing many of the limitations of conventional treatments.
The successful deployment of NDDSs and smart wound dressings extends beyond their technological performance and relies fundamentally on patient adherence, particularly among elderly individuals managing chronic diabetic ulcers. 7 Because these devices require regular maintenance, correct placement, and prompt recognition of operational failure, inadequate patient understanding can compromise therapeutic efficacy and even increase the risk of adverse events. To address this gap, patient education must become an integral component of NDDS and smart-dressing implementation. Clear, accessible guidance is essential to ensure that patients are able to maintain device hygiene, preserve sensor integrity, and identify early signs of malfunction such as adhesive detachment, abnormal temperature readings, or inconsistent sensor outputs. Incorporating simplified visual prompts, user-friendly instructional interfaces, and periodic AI-guided reminders can further strengthen patient engagement and reduce misuse. By embedding structured education within clinical and home-care workflows, adherence can be improved substantially, enabling these technologies to achieve their intended therapeutic impact and ensuring safer, more reliable wound management in real-world settings.
Growth factors
Growth factors play a crucial role in regulating cell proliferation, migration, and differentiation, all of which are essential for effective wound healing. Transforming growth factor-beta 1 (TGF-β1) is a key modulator in cutaneous tissue repair, while vascular endothelial growth factor (VEGF) promotes neovascularization by activating endothelial cells. 8 Platelet-derived growth factor (PDGF) 9 supports dermal regeneration, epidermal growth factor (EGF) 10 facilitates keratinocyte migration for re-epithelialization, and fibroblast growth factor 2 (FGF2) 11 enhances endothelial and smooth muscle cell proliferation, reducing excessive scar formation. However, DFUs and other chronic wounds are often characterized by an imbalance in growth factors, leading to impaired healing. Exogenous administration of recombinant growth factors, such as rhEGF (e.g., Heberprot-P®, Regen-D™ 150, Easyef®), has been explored as a therapeutic strategy. Yet, their clinical application remains limited due to rapid degradation, poor localization, and ineffective distribution at the wound site. NDDS-based strategies provide a viable solution to these challenges by offering controlled release and targeted delivery. Hybrid biomaterial patches, such as porous nanofiber membranes combined with GelMA hydrogels, have been developed to enhance the stability and bioavailability of growth factors, ensuring prolonged therapeutic effects. 12
miRNAs, proteins, and peptides
Gene therapy has emerged as a promising approach for correcting genetic dysfunction in diabetic wounds. MicroRNAs (miRNAs), such as miR-129 13 and miR-335, 14 play a regulatory role in gene expression by inhibiting matrix metalloproteinase-9 (MMP-9), a key enzyme involved in excessive ECM degradation. Despite their therapeutic potential, traditional gene-delivery methods, particularly viral transfection, pose significant safety concerns, including potential carcinogenicity and immune activation.
To enhance both the safety and efficiency of gene therapy, NDDS-based approaches have been developed. For instance, milk-derived exosomes engineered through electroporation have demonstrated improved cellular uptake, stability, and therapeutic efficacy in promoting angiogenesis and wound healing. Similarly, siRNA-based nanocarriers have been designed to regulate specific wound-healing pathways. One notable example is layer-by-layer assembled siRNA nanoparticles targeting prolyl hydroxylase domain-containing protein 2 (PHD-2), which stabilizes hypoxia-inducible factor-1 alpha (HIF-1α). 15 This stabilization increases the expression of pro-angiogenic factors while preventing premature degradation, thereby enhancing transfection efficiency and therapeutic outcomes.
Stem cells and exosomes
Stem cell-based therapies, particularly those using mesenchymal stem cells (MSCs), hold great potential for regenerative medicine due to their multilineage differentiation capabilities, immunomodulatory properties, and ability to promote angiogenesis. Among various MSC sources, adipose-derived stem cells (ADSCs) offer an attractive alternative to bone marrow-derived MSCs due to their ease of extraction, reduced ethical concerns, and strong VEGF secretion, which enhances vascularization and tissue repair. 16 However, MSC-based therapies face several challenges, including low survival rates, limited proliferation capacity, and logistical issues related to storage and transportation. Yadav et al. highlight the need for standardized reporting in exosome research to ensure rigor and reproducibility, emphasizing unified isolation and characterization methods, shared data platforms, and consistent quality control (QC). 17 To overcome these limitations, NDDS-based approaches incorporating hydrogels have been developed. 18 Injectable hydrogels, such as those utilizing hyperbranched PEG macromers and hypoxia-induced conductive hydrogels, have demonstrated the ability to support vascular network formation, facilitate hair follicle regeneration, and remodel collagen matrices, thereby enhancing overall wound repair. An alternative to direct stem cell transplantation is the use of exosomes, which are small EVs (40–100 nm) that carry bioactive molecules such as proteins, miRNAs, and cytokines. 19 Exosome-based therapies offer several advantages over traditional stem cell treatments, including greater stability, easier storage, and lower risks of tumorigenicity or immune rejection. These properties make exosomes an increasingly attractive cell-free approach for enhancing diabetic wound healing. Exosomes from diverse MSC sources (BMSCs, GMSCs, ADMSCs, MenSCs, hUCMSCs) and keratinocytes carry DNA, RNA, miRNAs, enzymes, and proteins that modulate regeneration and immune cell responses, such as macrophages. 20 Collectively, these reveal that keratinocyte-derived exosomes play a pivotal role in coordinating wound healing through macrophage communication. In diabetic wounds, both the abundance and molecular cargo of these exosomes are markedly impaired, leading to disrupted intercellular signaling and delayed repair. Advanced analyses, including charge-detection mass spectrometry, further demonstrate altered exosomal mass/charge profiles and dysfunctional RNA packaging under hyperglycemic conditions, underscoring the pathogenic link between exosome dysregulation and chronic nonhealing wounds.21–24 In DFUs, they attenuate vascular injury, neuropathy, hypoxia, biofilm formation, and excessive cytokine release, thereby promoting wound healing. Systemically, they enhance β-cell regeneration, improve insulin sensitivity, and restore glucose homeostasis in both type 1 diabetes (T1DM) and type 2 diabetes (T2DM), as shown in Fig. 1. Figure 1 synthesizes the principal regenerative mechanisms attributed to EV-based and nanodrug-mediated interventions, highlighting their roles in angiogenic activation, mitochondrial restoration, and inflammatory modulation. Beyond serving as a visual overview, the figure underscores a central conceptual gap in the field: although EV cargo signatures such as SIRT3/SOD2 activation and pro-angiogenic miRNAs are consistently linked with enhanced healing in preclinical models, their functional stability and potency remain highly context-dependent in clinical settings. The illustration therefore not only summarizes mechanistic pathways but also emphasizes the need to harmonize manufacturing, dosing, and biomarker evaluation to achieve reproducible therapeutic outcomes in human DFUs.
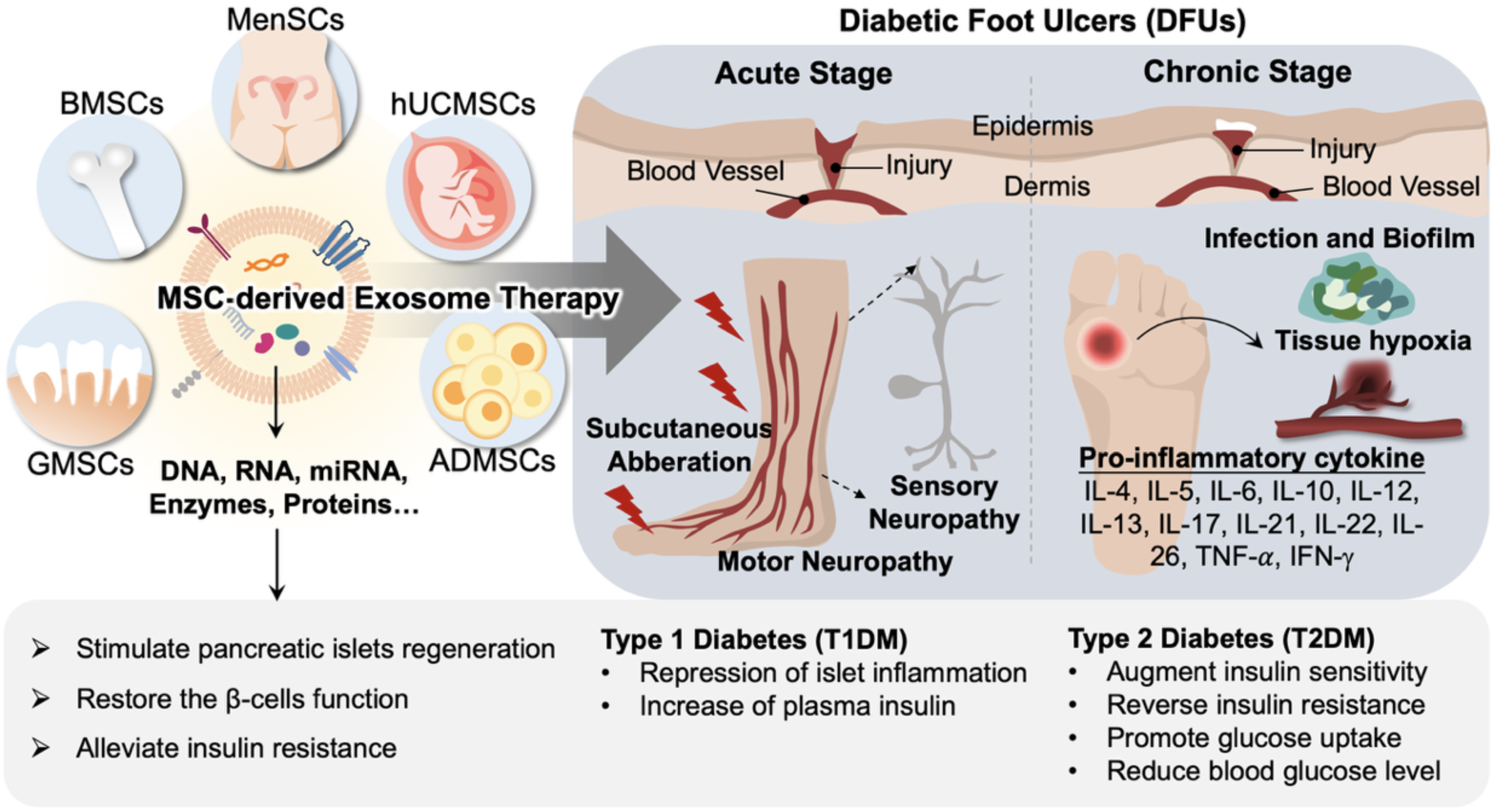
Integrated schematic of mesenchymal stem cell (MSC)-derived exosome therapy and next-generation precision systems for diabetic foot ulcers (DFUs) and diabetes mellitus. MSC-derived exosomes obtained from diverse tissue sources—including bone marrow (BMSCs), gingiva (GMSCs), adipose tissue (ADMSCs), menstrual blood (MenSCs), and human umbilical cord (hUCMSCs)—carry DNA, RNA, microRNAs, enzymes, and proteins that collectively orchestrate tissue repair, immune homeostasis, and metabolic balance. In DFUs, these vesicles intervene across both acute and chronic disease phases. Acute-phase injury involving vascular disruption and subcutaneous tissue stress precipitates motor and sensory neuropathy, whereas chronic progression is characterized by persistent vascular insufficiency, ischemic hypoxia, microbial biofilm formation, and sustained pro-inflammatory cytokine expression (IL-4, IL-5, IL-6, IL-10, IL-12, IL-13, IL-17, IL-21, IL-22, IL-26, TNF-α, IFN-γ), collectively hindering angiogenesis and tissue regeneration. MSC-derived exosomes ameliorate these pathological cascades by attenuating inflammation, stabilizing microvascular architecture, modulating immune signals, and promoting cellular repair. Beyond local wound healing, MSC exosomes regulate systemic glucose metabolism by enhancing pancreatic islet regeneration, restoring β-cell function, and mitigating insulin resistance. In type 1 diabetes, this is achieved through suppression of autoimmune islet inflammation and restoration of insulin output, whereas in type 2 diabetes, MSC exosomes potentiate insulin sensitivity, improve glucose uptake, and reduce circulating glucose levels. This therapeutic framework is embedded within a closed-loop precision-medicine ecosystem. Regenerative biologics (growth factors, stem cells, and exosomes) interface with nanodrug delivery systems (NDDSs), wearable biosensing platforms, and AI-enabled wound-monitoring technologies to achieve dynamic, data-driven clinical intervention. Real-time physiological and biochemical inputs—captured through intelligent dressings and wearable biosensors (pH, temperature, moisture, perfusion)—are integrated with multimodal imaging and biosignature analytics. These feed into AI algorithms that continuously evaluate wound status, predict healing trajectories, and guide adaptive dosing and spatial delivery of exosome-based and nanotherapeutic payloads. The mechanistic wound-healing cascade is conceptualized as a continuous progression in which chronic ulceration leads to persistent dysregulated inflammation, subsequently resulting in impaired angiogenesis and neurovascular failure. MSC exosomes, miRNA-based therapeutics, and NDDSs converge at defined intervention nodes to normalize inflammatory tone, restore angiogenic signaling, counter neuropathic degeneration, and stabilize extracellular matrix remodeling. This systems-level paradigm illustrates the emerging evolution of DFU management—from isolated regenerative interventions toward an integrated, sensor-informed, AI-augmented, closed-loop therapeutic framework that enables precision control of biological repair processes and systemic metabolic reprogramming.
Manufacturing and QC for exosome-based therapeutics and NDDSs remain fragmented, hindering comparability, scale-up, and regulatory acceptance. For EVs, field standards such as MISEV emphasize transparent reporting of source cells, isolation, and multimodal characterization; however, translation demands that these principles be embedded within current Good Manufacturing Practice (cGMP) pipelines with predefined critical quality attributes (CQAs) and in-process controls (IPCs). Practical EV CQAs should include identity (canonical and source-specific markers), purity (protein, lipid, and process-related impurities), dose metrics (particle count plus cargo or activity), potency (fit-for-purpose bioassays), safety (endotoxin, sterility, mycoplasma), and stability (storage and transport robustness). Incorporating automated, closed bioprocessing (e.g., bioreactors, TFF/SEC) with electronic batch records and process analytical technologies (PAT) can reduce operator variability and enable real-time release testing. High-throughput, automated analytics—NTA/DLS with calibrated standards, imaging flow cytometry or nFCM for single-particle phenotyping, LC–MS proteomics and lipidomics for impurity profiling, ddPCR/NGS for RNA cargos, and microfluidic assays for residuals—support batch consistency and CMC traceability.17,20–24
For nanocarriers, a similar quality-by-design (QbD) framework is required, mapping material attributes (chemistry, size/PDI, zeta potential, morphology), product attributes (encapsulation efficiency, release kinetics under physiological/stressed conditions, aggregation), and process parameters (mixing, solvent exchange, shear) to clinical performance. Automated characterization platforms that couple orthogonal measurements (e.g., asymmetrical flow-field flow fractionation–MALS, HPLC/LC–MS for free drug, microcalorimetry, and TEM/cryogenic EM) strengthen CQA–clinical outcome linkages and align with FDA/EMA risk-based expectations.
GMP-compliant production pipelines for EVs and nanocarriers should therefore (i) use closed, scalable culture and purification (single-use bioreactors; automated TFF/SEC); (ii) define harmonized release specifications (identity, purity, potency, dose, safety, stability) with reference materials and control charts; (iii) implement potency assays anchored to mechanism of action (e.g., functional biomaker induction or anti-inflammatory readouts); (iv) deploy automated, orthogonal analytics to assure batch-to-batch equivalence; and (v) maintain digital traceability from cell bank/materials through fill-finish. Collectively, these steps operationalize MISEV-aligned science within cGMP CMC dossiers and de-risk regulatory review by converting today’s descriptive EV and nanoformulation reports into quantitative, auditable manufacturing systems.
Drug-based approaches
Several pharmacological agents have demonstrated potential in promoting wound healing, but their effectiveness is often hindered by poor stability, bioavailability, and rapid clearance. 25 NDDSs provide an innovative solution to these issues by improving targeted delivery, controlled release, and enhanced drug bioactivity.
One particularly promising compound is curcumin, a natural polyphenol with strong antioxidant and anti-inflammatory properties. However, due to its hydrophobic nature and low bioavailability, its therapeutic applications have been limited. To address these challenges, curcumin nanoparticles (CNPs) have been encapsulated in gelatin microspheres (GMs) that respond to MMP-9 overexpression, enabling controlled drug release and improved stability. 26 In addition, hyaluronic acid (HA) and chitosan-based hydrogels (OHA-CMC) have been designed to further enhance curcumin’s delivery and bioactivity at wound sites. 27
Beyond curcumin, several antidiabetic drugs, including metformin (MET), 28 pioglitazone (PHR), 29 and glibenclamide (GB), 30 have demonstrated anti-inflammatory and wound-healing properties. Studies have shown that the incorporation of these drugs into nanofibrous scaffolds significantly accelerates wound healing. Interestingly, combinations of PHR and MET or PHR and GB have exhibited superior therapeutic effects compared with single-drug treatments, highlighting the potential of combinational NDDS-based approaches. By integrating NDDSs with personalized medicine, AI-driven drug optimization, and advanced biomaterial engineering, the future of diabetic wound healing may soon witness a paradigm shift toward more efficient, safe, and clinically viable treatment solutions. The current findings from both patient treatments and animal model studies are summarized in Tables 1 and 2, respectively.
Summary of current treatments in wound healing (patients)
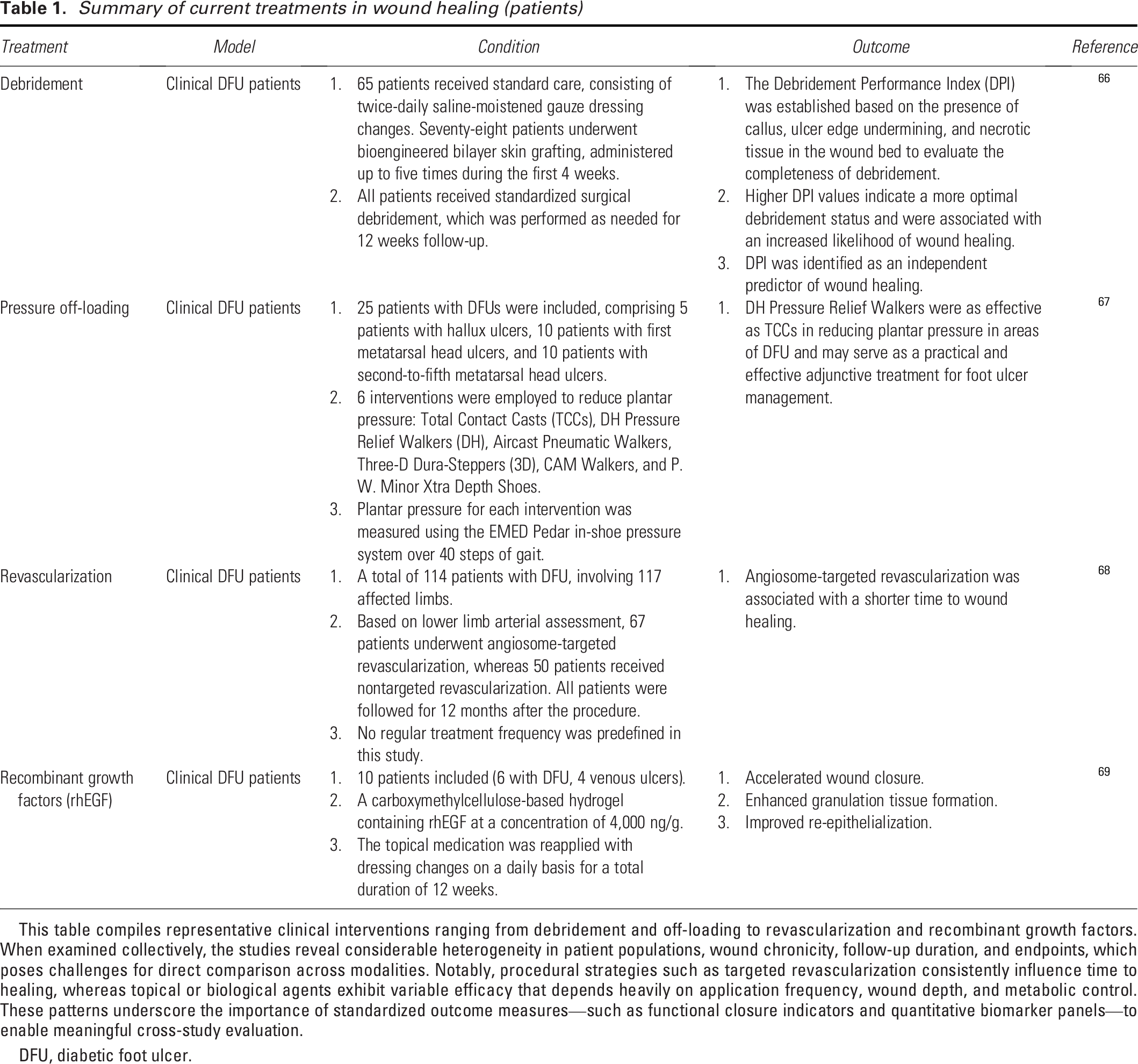
This table compiles representative clinical interventions ranging from debridement and off-loading to revascularization and recombinant growth factors. When examined collectively, the studies reveal considerable heterogeneity in patient populations, wound chronicity, follow-up duration, and endpoints, which poses challenges for direct comparison across modalities. Notably, procedural strategies such as targeted revascularization consistently influence time to healing, whereas topical or biological agents exhibit variable efficacy that depends heavily on application frequency, wound depth, and metabolic control. These patterns underscore the importance of standardized outcome measures—such as functional closure indicators and quantitative biomarker panels—to enable meaningful cross-study evaluation.
DFU, diabetic foot ulcer.
Summary of current findings in wound healing (animal models)
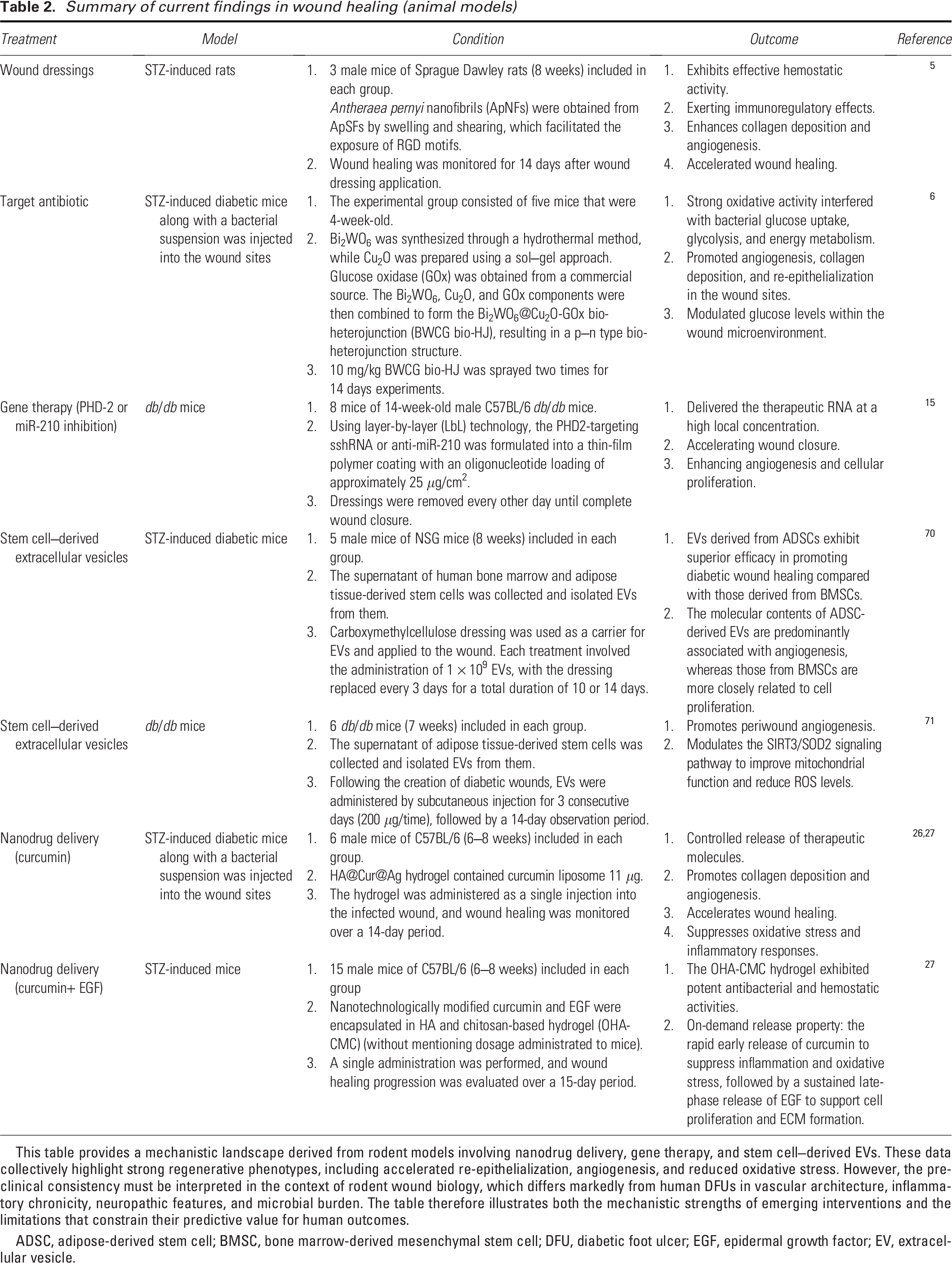
This table provides a mechanistic landscape derived from rodent models involving nanodrug delivery, gene therapy, and stem cell–derived EVs. These data collectively highlight strong regenerative phenotypes, including accelerated re-epithelialization, angiogenesis, and reduced oxidative stress. However, the preclinical consistency must be interpreted in the context of rodent wound biology, which differs markedly from human DFUs in vascular architecture, inflammatory chronicity, neuropathic features, and microbial burden. The table therefore illustrates both the mechanistic strengths of emerging interventions and the limitations that constrain their predictive value for human outcomes.
ADSC, adipose-derived stem cell; BMSC, bone marrow-derived mesenchymal stem cell; DFU, diabetic foot ulcer; EGF, epidermal growth factor; EV, extracellular vesicle.
Off-target effects, immune activation, and unpredictable gene silencing remain major challenges for nucleic acid–based NDDSs. Seed-region complementarity, passenger-strand loading, and RNAi-pathway saturation can disrupt native gene networks and cause unintended transcript repression. 31 In parallel, cationic or poorly degradable nanocarriers may trigger Toll-like receptor signaling, complement activation, or cytokine release, compromising safety and therapeutic precision. 24 Employing biocompatible, nonimmunogenic materials is essential. Biodegradable ionizable lipids, zwitterionic polymers, and PEG alternatives such as polysarcosine minimize innate immune sensing and enhance endosomal escape. Chemical modifications to RNA (e.g., 2′-O-methyl or 2′-fluoro substitutions) further reduce immune stimulation without diminishing efficacy. 31 Strict GMP control of excipients and endotoxin levels also mitigates immunotoxic risk.
Targeted delivery strategies improve specificity and reduce systemic exposure. Ligand-conjugated nanoparticles—using peptides, small-molecule ligands, or aptamers—enhance uptake in disease-relevant tissues. 32 Incorporating stimuli-responsive release mechanisms (pH, enzyme, or redox triggers) provides spatiotemporal control and limits off-site activity. 24 Integrating these design principles within a quality-by-design framework—linking material attributes to biological outcomes—can reduce off-target and immune-related risks while ensuring consistent, predictable gene silencing. Together, these strategies form the foundation for safer and more effective NDDS platforms.24,31,32
Direct tissue reprogramming for vascular, neural, and lymphatic restoration in diabetic foot ulcers
Direct tissue reprogramming has emerged as a compelling regenerative strategy capable of directly addressing the complex microenvironmental failures underlying DFU, including peripheral ischemia, neuropathy, and lymphatic dysfunction. Rather than relying solely on exogenous cell transplantation or conventional growth factor therapy, in vivo reprogramming leverages resident fibroblasts and stromal cells to generate vascular, neural, and lymphatic phenotypes within damaged tissues, thereby restoring perfusion, sensation, and fluid homeostasis in a coordinated manner.
Recent advances in endothelial lineage conversion have demonstrated that targeted delivery of transcriptional regulators or microRNA circuits can induce fibroblast-to-endothelial transdifferentiation, leading to enhanced angiogenesis and functional tissue reperfusion in ischemic limbs.33,34 Earlier foundational work similarly established the feasibility of fibroblast-to-endothelial reprogramming, with significant improvements in perfusion and tissue viability in preclinical ischemia models.35,36 Complementing vascular regeneration, direct neural reprogramming approaches have shown success in converting resident glial or fibroblastic populations into neuronal or Schwann-like cells, enhancing axonal regeneration and sensory recovery in models of peripheral neuropathy, a central pathological driver of DFU.37–39
Parallel progress in lymphatic reprogramming has highlighted the potential to reconstruct lymphatic endothelium and improve interstitial fluid clearance, thereby alleviating lymphedema and immune dysregulation in chronic wound environments.40,41 Notably, multisystem approaches that jointly enhance vascular and neural repair have yielded synergistic restoration of perfusion and sensory function, underscoring the value of combinatorial reprogramming strategies for ischemic neuropathy in diabetes. 42 Continued refinement of transient gene-delivery systems, nonviral vectors, and responsive biomaterial scaffolds has further advanced the safety and translational feasibility of reprogramming interventions. 43
Taken together, direct tissue reprogramming provides a mechanistically grounded, multifaceted approach to reversing the biological hallmarks of DFU. By actively reconstructing vascular, neural, and lymphatic networks in situ, this strategy moves beyond symptomatic wound management toward true restoration of tissue physiology. Future integration with AI-guided patient stratification, spatiotemporal control of reprogramming factor delivery, and closed-loop wound monitoring systems may accelerate clinical translation and enable precision deployment of regenerative reprogramming therapies in diabetic limb disease.
ARTIFICIAL INTELLIGENCE TECHNOLOGY FOR DETECTING WOUND CLOSURE
AI is emerging as a transformative catalyst in precision regenerative therapy for DFUs. By integrating multiomic wound and exudate profiles—encompassing miRNA cargo, inflammatory cytokines, and ECM remodeling markers—with multimodal imaging features such as RGB, hyperspectral, and thermal data, AI-driven stratification can delineate molecularly defined patient subgroups with distinct healing phenotypes. These computationally derived endotypes allow personalized prediction of therapeutic responsiveness, identifying candidates for interventions such as revascularization or exosome-based angiogenic therapy while embedding fairness and safety auditing prior to clinical application.
Beyond patient classification, adaptive AI algorithms utilizing real-time biomarker feedback from wearable biosensors and imaging analytics dynamically modulate therapeutic parameters—including nanodrug release kinetics, exosome administration frequency, or off-loading intensity—through online learning and Bayesian inference models with clinician-in-the-loop supervision. Central to this precision framework is the implementation of standardized biomarker panels integrating perfusion indices, inflammatory and infection markers, matrix remodeling enzymes, mitochondrial stress indicators (e.g., SIRT3/SOD2), glycemic control metrics (HbA1c), and exosomal molecular profiles. Such harmonized datasets provide analytical consistency across studies, enabling robust AI model training, benchmarking, and regulatory validation. However, to prevent “alarm fatigue” within the clinician-in-the-loop framework, the system applies a tiered data-filtering and thresholding algorithm rather than transmitting raw pH, temperature, and moisture streams. First, all sensor inputs undergo calibration, artifact removal, and sliding window smoothing to eliminate transient, clinically irrelevant fluctuations. Second, alerts are generated only when deviations from individualized physiological baselines exceed validated absolute and relative thresholds and persist beyond a minimum duration, preventing single-point spikes from triggering notifications. Third, the filtered parameters are integrated into a machine learning (ML)–derived composite wound-risk score; only scores surpassing the actionable threshold are escalated to clinicians, consistent with the design in which “summarized daily wound images, flagged deviations from expected trajectories, and notified clinicians only when clinically meaningful deterioration was detected.” Finally, alerts are tiered with configurable refractory periods to minimize redundant signaling. This framework ensures high-specificity, actionable alerts while avoiding information overload for the health care team.
These innovations converge into a human-centered, closed-loop therapeutic ecosystem in which standardized molecular panels continuously inform AI stratifiers and adaptive controllers, ultimately transforming DFU care from static management to dynamic, predictive, and personalized regeneration. Importantly, Sen et al. present a concise and integrative framework for implementing AI in biomedical and clinical research. The study synthesizes key pillars—data engineering, knowledge representation, and ML—into a coherent roadmap that extends to translational domains such as medical imaging and natural language processing (NLP). By introducing a standardized implementation checklist, the work underscores the importance of human-centered AI and highlights the role of clinicians and scientists as key enablers of responsible and interpretable AI adoption in precision medicine, particularly in applications such as DFUs. 44
Supervised learning methods
Supervised learning methods are commonly applied to DFU analysis, focusing on tasks such as classification, object detection, and semantic segmentation. Depending on the specific application, different training datasets are used, ensuring that a sufficient but optimal amount of data is available for model training. Given the complexity of DFU detection, research increasingly relies on DL techniques due to their ability to uncover hidden patterns and capture intricate relationships among interdependent variables. The widespread availability of sensors and spectral band data further supports DL applications, particularly in DFU monitoring through optical imaging. 45
Despite these advancements, a major challenge in medical applications remains the limited availability of labeled training data due to privacy concerns and the sensitive nature of patient information. Since supervised learning requires extensive labeled datasets, this creates a bottleneck in model development. 46 To address this issue, researchers have explored alternative approaches, such as unsupervised and semi-supervised learning, which reduce dependence on labeled data while maintaining effective model performance. These alternative methods help overcome data limitations and improve the robustness of DFU detection models.
Unsupervised learning techniques
Unsupervised learning models address the challenge of labeled data by independently identifying meaningful patterns and structures within the input data. These algorithms can extract relevant feature representations without relying on predefined labels. In health care–related research, unsupervised learning is commonly applied through clustering techniques, which uncover hidden patterns or groupings within datasets. By deriving meaningful features from raw data, unsupervised learning helps reduce the dimensionality of the feature space, ultimately improving clustering performance, which in this context refers to the enhanced separation, stability, and interpretability of latent wound phenotypes when high-dimensional sensing or imaging data are projected onto lower-dimensional manifolds. Methods such as PCA, t-SNE, UMAP, and variational autoencoders can reduce noise, mitigate collinearity, and enhance the coherence of clusters derived from heterogeneous DFU datasets. This usage does not imply reduced architectural complexity or superior predictive accuracy relative to DL models; rather, unsupervised learning serves as an exploratory analytical tool for identifying structure within raw data. It is also recognized that unsupervised approaches remain distant from clinical implementation, particularly for sensor-to-treatment workflows that require traceability, interpretability, and reproducibility. Real-world deployment necessitates supervised or rule-based systems supported by annotated datasets and regulatory-grade validation. To reflect these constraints, the discussion now emphasizes that unsupervised learning should be viewed primarily as a hypothesis-generating strategy that can guide biomarker discovery and support the development of clinically auditable supervised models. This distinction reinforces the importance of transparency and safety in AI-enabled DFU management and clarifies the limited but meaningful role of unsupervised learning within emerging closed-loop therapeutic frameworks.46,47
Semi-supervised learning techniques
Alternative approaches include tensor-based learning and semi-supervised learning. Both methods leverage feature-space projections to effectively manage high-order data and limited training sets. In the case of tensor-based learning, CP decomposition of rank-R is applied to model weights, significantly reducing the number of hyperparameters during training. Meanwhile, semi-supervised learning integrates both labeled and unlabeled data to introduce additional regularization terms, enhancing model performance. 48
Supervised learning remains the dominant paradigm for AI-based wound analysis; however, its effectiveness is constrained by the scarcity of large, well-annotated datasets. Privacy regulations, ethical concerns, and the labor-intensive nature of medical image labeling hinder data accessibility and scalability, ultimately limiting model generalizability across institutions. To address these challenges, semi-supervised and unsupervised learning frameworks are increasingly employed to reduce dependency on labeled datasets by leveraging unlabeled data for feature extraction and pattern recognition. These approaches enable models to infer latent wound characteristics and improve robustness in diverse clinical scenarios. In parallel, FL has emerged as a transformative solution for collaborative model training without the need to share raw patient data. By distributing model updates rather than sensitive information, federated architectures enable multi-institutional AI development while maintaining data privacy and regulatory compliance. The integration of privacy-preserving technologies—such as differential privacy, secure multiparty computation, and homomorphic encryption—can further strengthen data security and incentivize inter-institutional data sharing. These innovations represent a paradigm shift toward ethical, decentralized, and data-efficient AI ecosystems. By combining semi-supervised, unsupervised, and FL strategies, future wound assessment models can achieve greater scalability, transparency, and clinical reliability, fostering equitable access to precision diagnostics and personalized wound management across global health care systems.
CATEGORIZATION OF MACHINE LEARNING APPROACHES FOR DFU MONITORING
Current wound assessment frameworks remain constrained by subjective visual inspection and inconsistent biochemical readouts, limiting their prognostic accuracy and clinical reproducibility. The integration of harmonized biomarker panels—encompassing transepidermal water loss (TEWL), perfusion indices, inflammatory cytokines, ECM-degrading enzymes, and mitochondrial stress markers—offers a systematic and quantifiable approach to characterize wound status. Among these, TEWL has recently emerged as a pivotal functional indicator of barrier restoration, correlating closely with wound closure dynamics and epithelial integrity.49–54 Collectively, these studies demonstrate that TEWL reflects both epidermal recovery and microcirculatory function, establishing its clinical relevance as a dynamic, noninvasive biomarker of wound-healing progression.
The concept of TEWL-based Functional Wound Closure represents a paradigm shift from morphology-based healing endpoints toward physiology-driven evaluation, capturing both structural and metabolic recovery.49,51,52 For example, recent work53,54 has shown that integrating TEWL measurements with cytokine and ECM enzyme profiles enhances discrimination between healing and nonhealing phenotypes, while studies employing advanced imaging modalities49,50 have validated TEWL as a surrogate marker for epithelial barrier restoration across diverse wound etiologies. To operationalize this framework, standardization of measurement techniques and biomarker thresholds is essential. Variability in device calibration, sampling time, and the local wound microenvironment can confound inter-study comparisons, underscoring the need for consensus-driven protocols.51,52 Importantly, integrating standardized biomarker panels with AI-driven stratification enables predictive analytics that distinguish healing phenotypes, forecast chronicity risk, and guide individualized interventions. ML models trained on multimodal datasets—such as TEWL dynamics, inflammatory markers, and ECM remodeling—could generate personalized predictions of healing outcomes. This approach shifts wound assessment from descriptive observation to quantitative, predictive medicine, advancing precision-guided management and therapeutic optimization.
Noninvasive sensors have significantly advanced diabetic foot monitoring, and recent datasets from these sensors have fueled ML applications in this field. This section categorizes studies based on the sensor type and electromagnetic spectrum range used for data acquisition, dividing them into four main groups: visible spectrum, hyperspectral imaging (HSI), thermal imaging, and mid-infrared (mid-IR) data. Each subsection presents relevant research in a structured table, detailing the study identifier, data collection equipment and conditions, clinical study participants, ML approach, and key findings. This structured review provides a clear overview of ML techniques in DFU monitoring, emphasizing how different spectral ranges contribute to improved detection and assessment. Table 3 presents the detection of wounds using AI.
Detection of wounds using AI
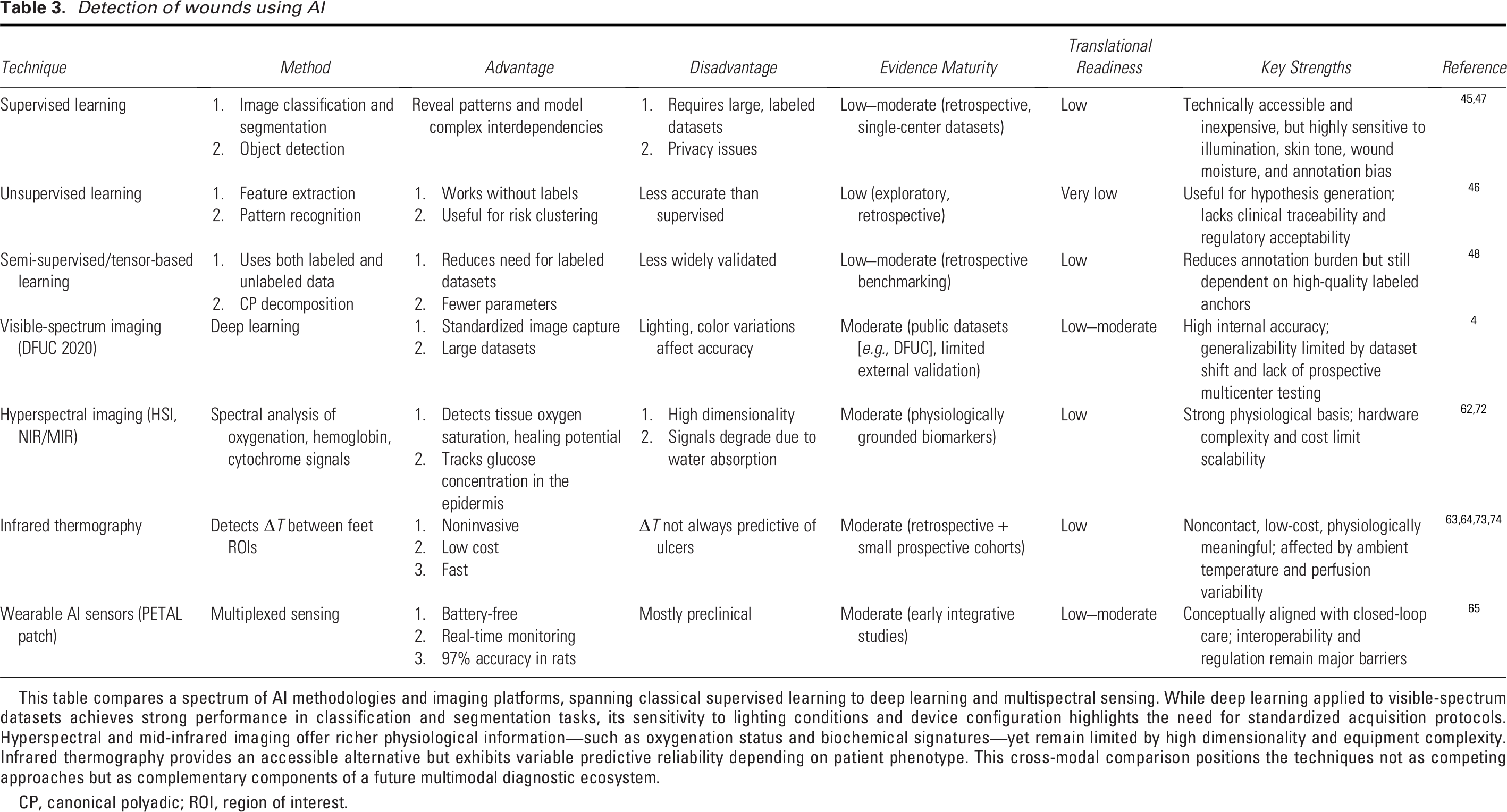
This table compares a spectrum of AI methodologies and imaging platforms, spanning classical supervised learning to deep learning and multispectral sensing. While deep learning applied to visible-spectrum datasets achieves strong performance in classification and segmentation tasks, its sensitivity to lighting conditions and device configuration highlights the need for standardized acquisition protocols. Hyperspectral and mid-infrared imaging offer richer physiological information—such as oxygenation status and biochemical signatures—yet remain limited by high dimensionality and equipment complexity. Infrared thermography provides an accessible alternative but exhibits variable predictive reliability depending on patient phenotype. This cross-modal comparison positions the techniques not as competing approaches but as complementary components of a future multimodal diagnostic ecosystem.
CP, canonical polyadic; ROI, region of interest.
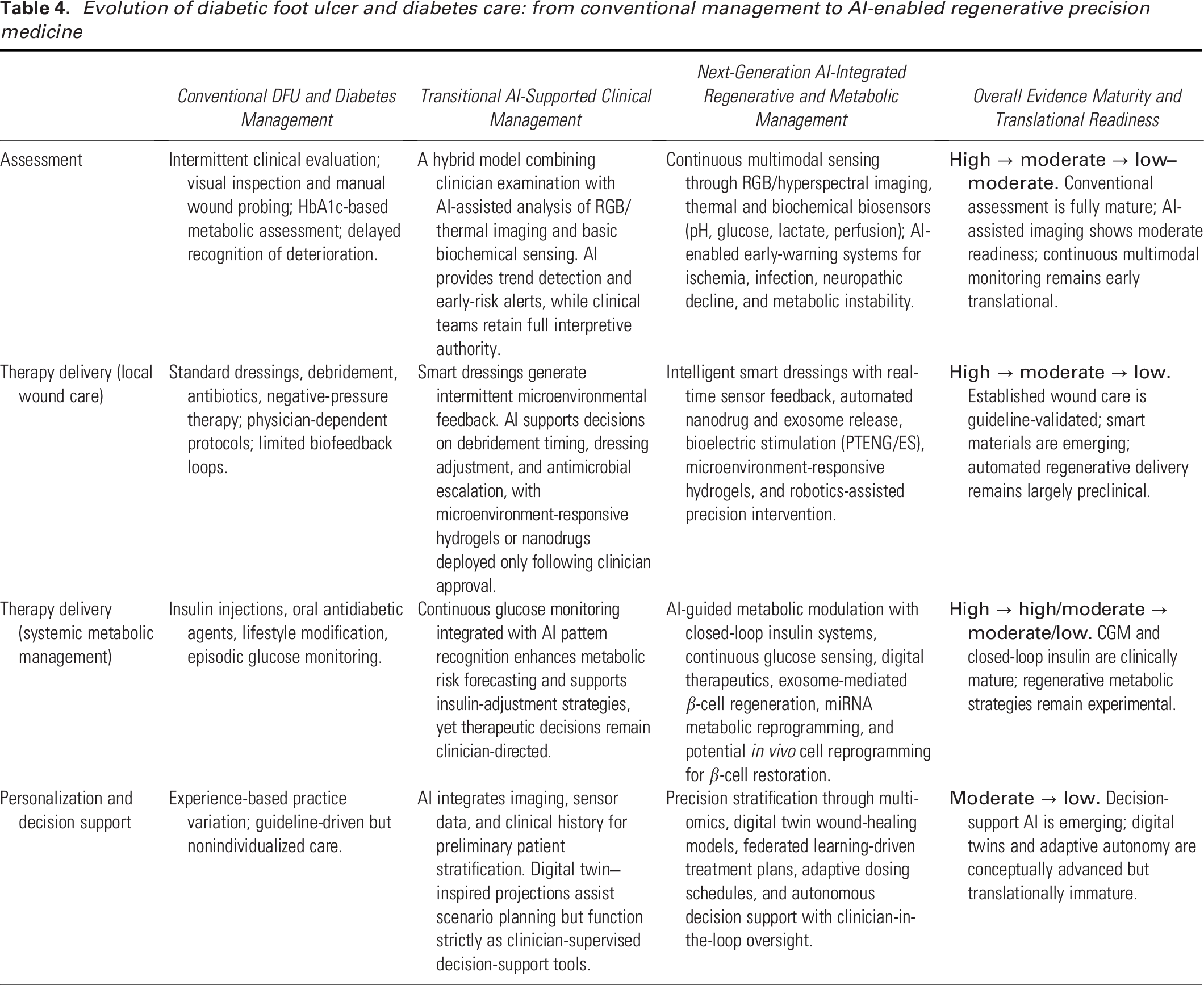
Evolution of diabetic foot ulcer and diabetes care: from conventional management to AI-enabled regenerative precision medicine
AI techniques and imagery data in the visible spectrum
This subsection reviews studies that process imagery data in the visible spectrum (RGB), particularly for DFU detection, a growing research area due to the increasing prevalence of diabetes. Early applications of ML showed promising results. This study utilized four support vector machines (SVMs) to identify wound areas in images, 55 while another research group assessed an application for standardizing DFU image capture. 56 Nanda et al. explored shallow learning techniques, including random forests (RF), SVM, naive bayes (NB), and K-nearest neighbor (KNN), for identifying DFU risk factors. 57
The release of the DFUC 2020 dataset, containing labeled images, has spurred interest in ML applications for DFU monitoring. This dataset includes 2,496 training images and 2,097 testing images, enabling the development of DL approaches. With labeled datasets, DL techniques have gained traction. For classification, Preiya et al. used a DL autoencoder for feature extraction and trained multiple models to classify healthy and DFU-affected skin. Xie et al. introduced feature fusion techniques combining low- and high-level information to enhance DFU classification. 58
For semantic segmentation, Ohura et al. compared SVMs with two convolutional neural networks (CNNs)—U-Net and a patch-based CNN—finding U-Net superior. 59 Ohura et al. supported these results, demonstrating U-Net’s sensitivity of 85.8% and specificity of 98.8%. Recent advancements utilize object detection models such as Faster R-CNN, YOLOv3, YOLOv5, and EfficientDet. 60 In addition, ensemble methods and cascade attention networks have been explored to further improve DFU detection accuracy.
AI techniques and hyperspectral/mid-infrared imagery for DFU analysis
HSI leverages near-infrared (NIR) and mid-IR spectra for biomedical applications, including DFU assessment. NIR radiation penetrates tissue without being absorbed by water or hemoglobin, allowing for the identification of biochemical changes. The distinct absorption spectra of oxygenated and deoxygenated hemoglobin, cytochrome c oxidase, and myoglobin in the NIR region have been widely studied for disease diagnostics, including diabetes complications. 61
HSI has been applied to estimate tissue oxygen saturation (SpO2) and detect ulcer healing potential based on oxygenation levels. However, the high dimensionality of hyperspectral data can reduce classification efficiency. Techniques such as SVMs, neural networks (NNs), and CNNs have been applied to classify DFUs as healing or nonhealing. 45
Mid-IR photoacoustic spectroscopy has also been explored for DFU monitoring, particularly for glucose concentration tracking in the epidermis. While mid-IR signals degrade due to water absorption, Kounas et al. proposed a hybrid approach combining a photoacoustic device with a tunable quantum cascade laser (QCL) to enhance penetration depth and improve glucose monitoring accuracy. 62 These advancements highlight the potential of hyperspectral and mid-IR imaging in DFU assessment and prognosis.
Infrared thermal sensing for DFU detection
Infrared thermography (IRT) is a fast, noninvasive technique that detects subtle temperature variations using long-wavelength infrared (LWIR) cameras. Its ease of use and cost-effectiveness make it valuable for medical applications, including DFU monitoring. A thermal imaging system consists of an optical system, a detector, an amplifier, a signal processor, and a display. The generated thermal images provide physiological insights into tissue conditions. DFU detection often involves dividing images into regions of interest (ROIs) and analyzing temperature differences between corresponding points on both feet. 63
The mean temperature difference (ΔT) between homologous ROIs serves as a key diagnostic metric. ML models enhance detection by comparing temperatures within a patient’s feet or against healthy individuals. Unsupervised learning techniques have also been explored for DFU severity risk clustering. These advancements underscore the potential of IRT in early DFU diagnosis and assessment. 64
Zheng et al. report a paper-like, battery-free, AI-enabled multiplexed sensor platform (PETAL) for holistic wound assessment by leveraging DL algorithms. The PETAL sensor consists of a wax-printed paper panel with five colorimetric sensors designed to measure temperature, pH, trimethylamine, uric acid, and moisture. Sensor images captured through a mobile phone are analyzed using NN-based ML algorithms to determine the healing status of wounds. For ex situ detection, the PETAL sensor demonstrated the ability to classify healing versus nonhealing status with an accuracy as high as 97% when analyzing exudates collected from rat perturbed wounds and burn wounds. In situ monitoring of wound progression or severity was successfully demonstrated by attaching the sensor patches to rat burn wound models. This platform facilitates early warning of adverse events, enabling timely clinical intervention to improve wound-care management. The PETAL sensor offers simultaneous detection of five wound markers or condition indicators using an adaptable wax-printed sensor layout, intricate sensor functionalization techniques, and a deep neural network–based image analysis algorithm. Its efficacy has been demonstrated for benchtop analysis of perturbed wound exudates and for monitoring wound healing in burn wounds, both ex situ and in situ, highlighting its potential as a transformative tool in wound management. 65 A schematic illustration of integrated wearable technologies and AI-driven analytics, combining smart wound dressings, multifunctional hydrogels, and PTENG-based bioelectrical stimulation with DL-based wound assessment to enhance DFU management and accelerate wound-healing outcomes, is presented in Fig. 2. Figure 2 outlines an emerging ecosystem integrating smart wound dressings, multimodal imaging, biochemical sensing, and deep learning analytics. The figure demonstrates how these technologies collectively enable continuous microenvironmental monitoring and early detection of deterioration—an advantage unattainable through visual inspection alone. At the same time, the schematized workflow highlights key translational constraints, including sensor variability, risks of skin injury in elderly patients, and limited cross-institutional validation of AI models. As such, the figure functions not merely as a conceptual diagram but as a framework that delineates technological potential alongside practical considerations for real-world implementation.

Schematic overview of emerging wearable biosensing technologies and AI-enabled analytics for precision management of diabetic foot ulcers (DFUs). DFUs, driven by persistent inflammation, ischemia, and impaired tissue repair, remain a critical and costly complication of diabetes (left). To address this challenge, next-generation wearable systems are illustrated across three representative platforms: (1) battery-free, wireless smart wound dressings integrating microelectronic biosensors for continuous physiological monitoring and on-demand therapeutic delivery; (2) multifunctional amphiphilic ion hydrogels capable of sensing wound-specific biochemical cues (e.g., pH, glucose, reactive oxygen species), transmitting signals, and modulating therapeutic responses to the wound microenvironment; and (3) piezoelectric triboelectric nanogenerator (PTENG)–based dressings that generate localized bioelectrical stimulation to enhance angiogenesis, fibroblast migration, and epithelial repair (top middle to right). In parallel, the AI component highlights a multimodal data-fusion pipeline in which RGB and hyperspectral wound images, together with continuous biosensor readouts (pH, temperature, moisture, perfusion), are streamed to deep learning models such as AlexNet, GoogLeNet, and DFUNet for wound classification, feature extraction, and decision support (bottom middle). Data processed through these models are relayed to an interactive predictive-healing dashboard, enabling clinicians and patients to visualize tissue oxygenation, infection risk, healing trajectories, and response to therapy in real time. In addition, the wearable sensor ecosystem is emphasized, featuring a smart dressing embedded with biochemical and biophysical sensors coupled to a mobile application interface. This platform supports autonomous data logging, remote clinician oversight, and adaptive drug-release logic triggered by threshold-based fluctuations in wound biomarkers or microenvironmental deterioration. Together, this integrated architecture illustrates the convergence of advanced bioresponsive materials, continuous sensing, and AI-driven analytics to enable closed-loop, personalized DFU care. By combining real-time wound surveillance, predictive modeling, and precision therapeutic intervention, wearable-AI ecosystems hold the potential to dramatically accelerate healing, reduce amputation risk, and transform chronic diabetic wound management into a proactive, data-informed discipline.
Enhanced integrative explanation for closed-loop DFU management framework
This section provides a clearer conceptualization of closed-loop architectures for DFU management, outlining how regenerative therapeutics and AI-enabled diagnostics may be integrated within a unified clinical workflow. A meaningful closed-loop system requires explicit definition of the data streams that trigger therapeutic decisions, the feedback signals that guide adaptive modulation, and the translational steps needed to progress from current practice toward semi-autonomous or autonomous wound-care models.
In this framework, multimodal sensing—including RGB and HSI, thermal profiling, TEWL-derived barrier metrics, and biochemical markers such as pH, lactate, and inflammatory cytokines—forms the diagnostic layer. These inputs are processed by supervised AI models that classify wound status, predict deterioration, and estimate healing trajectories. Model outputs then inform a therapeutic response layer in which microenvironment-responsive hydrogels, nanodrug reservoirs, or exosome-loaded dressings adjust release kinetics or dosing frequency according to predicted biological needs. As conditions evolve, updated sensor readings are reanalyzed, generating iterative feedback cycles that approximate a functional closed-loop system.
Advancing toward this integrated architecture requires sequential translational steps. Independent validation of imaging algorithms, biochemical sensors, AI-based stratification tools, and responsive delivery platforms is essential. Early feasibility studies assess accuracy, safety, and usability, followed by integration trials evaluating interoperability among sensors, computational models, and therapeutic materials. Ultimately, multicenter clinical studies are needed to confirm performance under DFU-relevant conditions, including necrosis, biofilm formation, ischemia, and neuropathy.
To consolidate these concepts, Fig. 3 presents an integrated schematic demonstrating how automated wound monitoring can interface with targeted molecular interventions. The framework highlights patient subgroups—such as those with unstable microenvironmental profiles, ischemic vulnerability, or high inflammatory burden—that may particularly benefit from adaptive, feedback-driven therapeutic modulation. Through this synthesis, a clinically grounded pathway is outlined for combining regenerative technologies, sensing modalities, and AI-driven analytics into future closed-loop systems for DFU management.
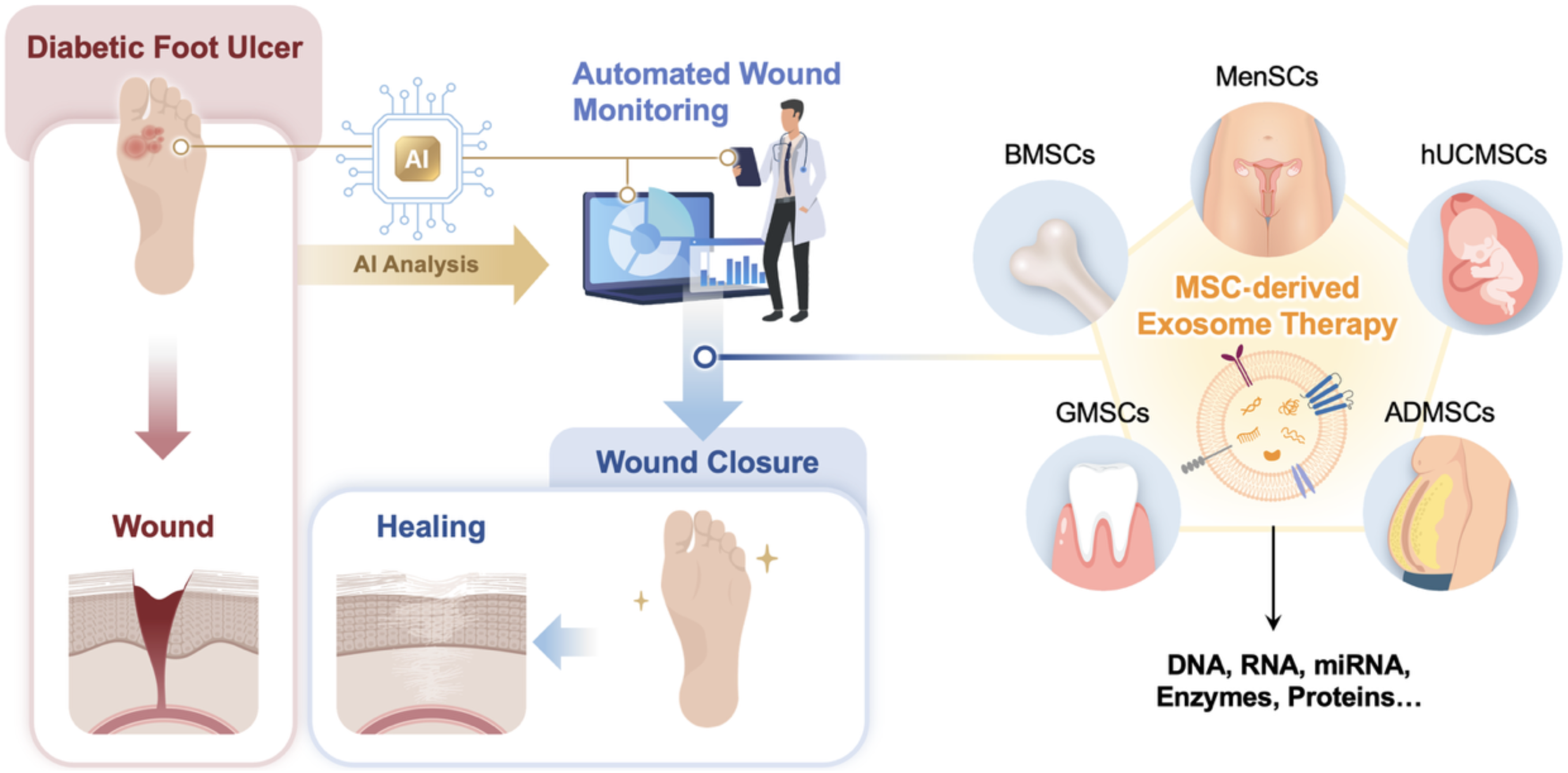
An integrative and next-generation therapeutic paradigm combining AI-guided wound monitoring with mesenchymal stem cell (MSC)-derived exosome therapy for diabetic foot ulcer (DFU) management. This figure depicts a novel integrative treatment strategy that unites digital health technology with advanced regenerative medicine to address the unmet clinical needs of DFUs. Automated, AI-driven wound monitoring enables continuous, objective evaluation of wound progression, providing real-time feedback on tissue status and healing trajectories. Guided by this digital assessment, a next-generation biological therapy based on MSC-derived exosomes is applied. Exosomes derived from multiple MSC sources, including bone marrow MSCs (BMSCs), menstrual blood MSCs (MenSCs), human umbilical cord MSCs (hUCMSCs), adipose-derived MSCs (ADMSCs), and gingiva-derived MSCs (GMSCs), function as cell-free regenerative therapeutics, delivering a rich cargo of DNA, RNA, microRNAs, enzymes, and proteins. This multifunctional molecular payload orchestrates immunomodulation, angiogenesis, re-epithelialization, and extracellular matrix remodeling. Importantly, this integrative and adaptive approach represents a shift from conventional passive wound care toward a precision, feedback-driven, and biologically active therapeutic model, establishing a new paradigm for DFU treatment that accelerates wound closure and improves tissue regeneration outcomes.
Future direction
The integration of NDDSs into diabetic wound healing represents a transformative advancement, offering precise, sustained, and localized delivery of therapeutic agents. By overcoming many of the limitations associated with conventional treatment methods, NDDSs have the potential to significantly improve clinical outcomes. However, despite these promising developments, several challenges must be addressed to fully realize their therapeutic potential.
One of the primary challenges lies in optimizing delivery systems to ensure proper spatial and temporal control over growth factors and gene therapies. The healing process of diabetic wounds is highly dynamic, requiring finely tuned therapeutic interventions at different stages. Uncontrolled release of bioactive molecules may lead to suboptimal effects or even adverse outcomes. Therefore, innovative delivery platforms capable of stimuli-responsive or sustained release mechanisms are crucial for maximizing the benefits of NDDSs in wound healing. Another critical aspect is the stability and bioavailability of therapeutic agents. Many bioactive compounds, such as curcumin, EGF, and exosomes, suffer from rapid degradation, poor solubility, or inefficient cellular uptake, which limits their therapeutic impact. Advanced nanocarrier designs, including polymeric nanoparticles, lipid-based vesicles, and hydrogel-based matrices, have been explored to enhance drug stability and pharmacokinetics. However, further research is needed to refine these strategies and ensure consistent bioactivity throughout the healing process.
The variable outcomes observed in regenerative therapies involving growth factors, exosomes, and NDDSs largely stem from inconsistent bioavailability, premature degradation, and poor spatiotemporal control of therapeutic release. These limitations underscore the urgent need for the development of stimuli-responsive nanocarriers capable of precise and sustained delivery in response to specific biological cues—such as pH, redox potential, or enzymatic activity—within the regenerative microenvironment. Such smart delivery systems can dynamically regulate the bioactivity of therapeutic molecules, minimize off-target effects, and enhance retention at the defect site, thereby improving overall therapeutic efficacy. Equally important is the standardization of hydrogel and nanoparticle formulations to ensure reproducibility and comparability across studies. Variations in polymer composition, cross-linking density, particle size distribution, and encapsulation efficiency significantly influence the pharmacokinetics and mechanobiological behavior of the delivery system. Establishing consensus on characterization metrics, QC parameters, and reporting standards will be essential to advance the clinical translation of these regenerative modalities. Harmonized protocols supported by regulatory-compliant analytical frameworks will not only enhance interlaboratory reproducibility but also facilitate regulatory approval processes. Ultimately, integrating stimuli-responsive nanocarriers with standardized hydrogel scaffolds represents a promising convergence of materials science and regenerative biology. This approach enables controlled therapeutic release, supports tissue-specific regeneration, and bridges the translational gap between bench-scale innovations and clinically viable regenerative therapies.
Balancing safety and efficacy is also a major concern, particularly in the context of siRNA and miRNA therapies. While these genetic interventions offer precise regulatory control over wound-healing pathways, the risk of off-target effects, immune activation, and unpredictable gene silencing poses significant hurdles to their clinical application. To mitigate these risks, NDDS formulations must incorporate biocompatible, nonimmunogenic materials while leveraging targeting strategies to improve specificity and minimize unintended consequences. Moreover, the clinical translation of NDDS-based therapies, particularly exosome-based treatments, faces significant scalability challenges. The efficient manufacturing, storage, and QC of nanoparticle formulations, hydrogel-based carriers, and engineered exosomes remain key bottlenecks in large-scale production. Ensuring batch-to-batch consistency and cost-effective production methods will be crucial for bringing these therapies from the laboratory to clinical practice.
In this review, clinical investigations provide the most translationally relevant evidence for DFU management, showing that recombinant growth factors, exosome-based therapeutics, and targeted revascularization effectively promote granulation, angiogenesis, and epithelialization. Nonetheless, heterogeneity in wound etiology, metabolic control, and patient comorbidities continues to limit reproducibility and therapeutic predictability. Establishing multicenter clinical trials and standardized biomarker panels is therefore essential to confirm efficacy and long-term safety. In contrast, preclinical studies have elucidated key regenerative mechanisms—such as SIRT3/SOD2-dependent mitochondrial restoration and macrophage–keratinocyte exosomal signaling—that underpin tissue repair. However, the structural and physiological disparities between rodent and human skin, particularly in immune regulation and chronicity of inflammation, constrain translational fidelity. To bridge this gap, future animal models should incorporate ischemic, neuropathic, and infectious elements reflective of the clinical DFU microenvironment.
The integration of AI-based patient stratification, semi-supervised learning, and federated data frameworks offers a pathway to harmonize mechanistic and clinical insights, enhancing predictive accuracy and therapeutic personalization. Collectively, while animal models remain vital for mechanistic exploration, human studies provide the cornerstone for clinical translation, steering DFU treatment toward intelligent, precision-guided regenerative medicine.
AI-based wound-assessment tools have advanced rapidly in recent years; however, their clinical integration remains constrained by the absence of unified benchmarks and validation frameworks across heterogeneous datasets. Most existing models are trained on limited, single-institution datasets that lack demographic diversity, standardized image capture protocols, and consistent annotation schemes, resulting in reduced generalizability and biased diagnostic outcomes. To overcome these barriers, the establishment of open-access, multi-institutional, and expertly annotated datasets encompassing DFU imaging (RGB, hyperspectral, thermal) and sensor-derived data is essential. These datasets should capture variations in ethnicity, skin tone, wound stage, and comorbidity to ensure equitable model performance across populations.
Furthermore, standardized performance metrics—such as sensitivity, specificity, accuracy, precision, recall, and F1 score—must be universally adopted to enable objective benchmarking and transparent comparison among studies. Implementing such uniform evaluation criteria would facilitate the reproducibility of algorithmic results and accelerate regulatory review. In parallel, the development of formal regulatory frameworks under agencies such as the U.S. Food and Drug Administration (FDA) and the European Conformity (CE) pathways is imperative to guide ethical approval, post-market surveillance, and clinical reliability of AI-based wound care systems. In summary, open-access data resources, harmonized performance metrics, and regulatory oversight will foster robust, interoperable, and trustworthy AI tools capable of delivering clinically validated, real-world impact in DFU management.
The absence of unified benchmarks and formal approval pathways for AI-based wound care systems impedes clinical adoption, comparability, and regulatory trust. A rigorous evaluation framework should mandate standardized performance metrics reported with confidence intervals and predefined clinical thresholds. At minimum, studies should disclose accuracy, sensitivity, specificity, and F1 score, alongside area under the ROC/PR curves for imbalanced datasets; calibration indices (e.g., Brier score, calibration slope/intercept); decision-curve analysis for net clinical benefit; and failure analysis stratified by wound etiology, Fitzpatrick skin type, comorbidities, and imaging conditions. External, multisite validation and prospective testing must be required to demonstrate transportability and mitigate dataset shift.
Regulatory engagement should follow established Software as a Medical Device (SaMD) paradigms. In the United States, developers should institute an ISO 13485-compliant quality management system with documented risk management (ISO 14971), software lifecycle controls (IEC 62304), cybersecurity (e.g., SBOMs, vulnerability handling), and human-factors engineering (IEC 62366). Early interaction with FDA through Q-Submission can clarify benefit–risk claims, reference standards, and clinical evidence needs, including whether a 510(k), de novo, or PMA route is appropriate. For adaptive models, sponsors should predefine change protocols (e.g., data governance, monitoring triggers, retraining boundaries, and verification/validation gates) and align them with Good Machine Learning Practice and real-world performance plans.
For CE marking under the EU MDR, manufacturers should establish a conformity strategy with a notified body: device classification and intended use, state-of-the-art comparison, clinical evaluation per MEDDEV/MDR, and post-market clinical follow-up. Harmonized standards (ISO 13485, ISO 14971, IEC 62304, IEC 82304-1) and transparent technical documentation (intended purpose, datasets, metrics, bias and fairness analyses, human oversight) should be integral.
Post-market, both FDA and CE pathways require active surveillance: continuous real-world performance monitoring, drift and bias detection, periodic safety update reports, complaint/incident handling, cybersecurity patching, and prespecified action limits for model rollback or retraining. Together, standardized metrics, proactive regulatory dialogue, and lifecycle safety oversight can convert promising prototypes into clinically reliable, ethically governed wound-care AI.
Despite rapid progress, AI has not yet been fully integrated into therapeutic decision-making or drug delivery systems. Future developments should focus on AI-guided, stimuli-responsive drug-release platforms that dynamically adjust therapeutic delivery according to wound microenvironmental cues—such as pH, temperature, oxygenation, or inflammatory biomarkers. These intelligent nanoplatforms could autonomously modulate the release kinetics of growth factors, peptides, or exosomes in response to real-time physiological changes, thereby maintaining an optimal healing niche.
Moreover, the convergence of wearable biosensors and AI analytics offers a powerful framework for real-time therapeutic feedback and precision control. By continuously monitoring biochemical and biophysical parameters—such as moisture, cytokine levels, or perfusion indices—wearable systems can feed data into adaptive AI algorithms capable of recalibrating dosing, frequency, and modality of treatment in situ. This closed-loop, patient-specific management system transforms wound care from a reactive to a predictive paradigm.
Finally, digital twin technologies represent the next frontier in AI-assisted regenerative medicine. By generating virtual patient replicas based on multiomic, imaging, and physiological datasets, digital twins can simulate individualized wound-healing trajectories, predict therapeutic outcomes, and optimize intervention timing. The integration of such AI-empowered simulation models with biosensor-guided drug delivery will accelerate the realization of intelligent, self-regulating, and precision-oriented wound-regeneration systems—marking a decisive step toward data-driven, adaptive therapeutics in clinical practice.
To strengthen the Digital Twin section, it is essential to explicitly address the ethical foundations governing data ownership, privacy, and informed consent when generating virtual patient replicas. Digital Twin models rely on continuous multimodal data streams—including imaging, biosensor outputs, and molecular biomarkers—to simulate individualized wound-healing trajectories. However, the creation and operation of such high-fidelity virtual replicas introduce substantial ethical risks that remain insufficiently discussed. We therefore recommend incorporating a dedicated subsection outlining the governance mechanisms required to safeguard patient data rights.
First, data ownership must be defined within a legal–ethical framework specifying who controls, accesses, and benefits from the Digital Twin. Patients should retain clear ownership of their raw physiological and imaging data, while processed data and model derivatives must be governed by transparent custodial agreements. Second, informed consent should be reconceptualized as a dynamic, ongoing process rather than a one-time authorization. Because digital twins continuously evolve as new biosensor and clinical data are ingested, patients must be able to modify or withdraw consent as model functions expand. Third, strong data-protection measures—including FL, differential privacy, and secure multiparty computation—should be implemented to minimize re-identification risk during model development and cross-institutional collaboration. These safeguards align with the responsible AI principles highlighted elsewhere in this work, in which patient-generated data are filtered, summarized, and escalated only when clinically meaningful deviations occur. Finally, Digital Twin deployment must incorporate auditable oversight mechanisms with clinician-in-the-loop governance to ensure that predictive outputs do not override human clinical judgment. Embedding these ethical, legal, and regulatory protections will ensure that Digital Twin technologies advance precision wound care while upholding patient autonomy, privacy, and data sovereignty.
A major limitation in current AI-driven wound assessment and prediction models lies in their reliance on small, single-institution datasets, which inherently restrict model generalizability and clinical applicability across diverse patient populations. Models trained on homogeneous datasets often fail to account for variations in ethnicity, age, comorbidities, imaging modalities, and clinical workflows—factors that profoundly influence wound morphology and healing dynamics. Consequently, these models may exhibit strong internal validity but limited external robustness when applied in real-world, multicenter clinical settings.
To address this issue, the development of open-access, multi-institutional datasets with broad demographic representation and standardized imaging protocols is imperative. Harmonization of image capture parameters—such as lighting, resolution, angle, and calibration—alongside uniform metadata annotation (e.g., wound type, stage, infection status, and treatment history) can significantly enhance interoperability and cross-study comparability. Such large-scale, well-curated datasets would enable the benchmarking of algorithmic performance and promote reproducibility across research groups, thereby accelerating the regulatory readiness of AI tools for clinical deployment. Furthermore, emerging FL frameworks and privacy-preserving computation paradigms (e.g., differential privacy, homomorphic encryption, and secure multiparty computation) provide a transformative pathway for collaborative model development without the need to exchange raw patient data. By allowing institutions to train models locally while sharing only model parameters or gradients, FL enables the integration of distributed datasets into robust, generalizable AI systems that respect patient confidentiality and comply with ethical and legal standards such as GDPR and HIPAA.
Integrating these federated and privacy-aware infrastructures with standardized, demographically diverse wound image repositories could revolutionize predictive modeling in wound care. This approach promotes data equity, enhances model transparency, and ensures that AI systems are trained under clinically realistic, globally inclusive conditions. Ultimately, such a strategy will bridge the translational gap between algorithmic innovation and clinical reliability, paving the way for scalable, ethical, and precision-driven AI applications in regenerative and wound medicine.
As wearable biosensors and smart dressings (e.g., PETAL platforms) become increasingly integrated into AI-enabled wound monitoring, future research must systematically address a critical yet underexamined barrier to clinical translation: biocompatibility and the high incidence of Medical Adhesive–Related Skin Injury (MARSI) in elderly diabetic patients. Age-related dermal thinning, impaired microcirculation, neuropathy, and delayed inflammatory resolution substantially elevate the risk of epidermal stripping, skin tears, and irritant dermatitis during repetitive device application and removal. These vulnerabilities are especially pronounced in DFU populations, who often require long-term, continuous monitoring in home-care settings.
To ensure safe adoption of wearable diagnostics, next-generation smart dressings must incorporate low-trauma adhesion technologies, including silicone-based, hydrocolloid, or hybrid atraumatic adhesives with controlled peel force and moisture-balanced interfaces. Equally essential are standardized protocols for device placement, removal, and rotation, supported by barrier-film conditioning, gentle-angle detachment procedures, and routine periwound skin assessments to detect early erythema, maceration, or shear-related microinjury. Embedding microtextured, breathable adhesive matrices may further reduce shear stress and humidity accumulation—two major contributors to MARSI. AI-driven platforms should be designed not only to interpret biochemical and biophysical wound markers but also to monitor adhesive–skin interactions. By analyzing temporal patterns of localized redness, temperature elevation, or moisture retention beneath the dressing, adaptive algorithms could autonomously flag early MARSI risk and recommend repositioning schedules, switching adhesive types, or reducing wear time. In addition, interoperability between patient-facing mobile applications and clinician dashboards can facilitate remote supervision, enabling timely intervention before clinically significant skin injury develops.
Ultimately, incorporating MARSI-aware biodesign principles, evidence-based home-care protocols, and AI-supported safety monitoring will be essential for the responsible, equitable translation of wearable wound technologies. Addressing these biocompatibility challenges will significantly enhance patient adherence, reduce complications, and strengthen the clinical value of AI-enabled, multimodal sensing ecosystems in DFU management.
As DL-based wound assessment models continue to advance, a critical next step for clinical translation is the integration of robust explainable AI (XAI) frameworks that enhance interpretability for frontline health care providers. While DL architectures can achieve high accuracy in distinguishing nonhealing versus infected wounds, their “black-box” nature limits clinical trust and hinders adoption in routine wound-care workflows, particularly among nursing staff who are responsible for daily wound evaluation and escalation of care.
Future development should prioritize XAI mechanisms capable of producing clear, human-interpretable visualizations that map the model’s decision-making process onto clinically meaningful wound features. Techniques such as class activation maps, Grad-CAM, saliency heatmaps, and feature-attribution overlays can highlight regions of concern—such as increased exudate, erythema borders, slough accumulation, or necrotic patches—and allow nursing staff to verify whether AI predictions align with visual cues observed at the bedside. These visualization tools not only support diagnostic transparency but also provide actionable insights, enabling nurses to more confidently triage wounds that require debridement, antimicrobial therapy, or specialist consultation. In addition, integrating XAI outputs into user-friendly dashboards within remote monitoring platforms can facilitate seamless communication between AI systems and clinical practitioners. For instance, heatmap-guided alerts could be paired with standardized wound-assessment terminology, allowing nursing personnel to rapidly interpret model outputs in home-care or telehealth settings. Future work should also evaluate the usability of these XAI interfaces across varying levels of digital literacy among health care providers, ensuring equitable and safe deployment.
By embedding interpretable, evidence-aligned visualization methods into DL-based wound classification systems, AI technologies can transition from being high-performance research tools to clinically trustworthy decision-support systems, ultimately strengthening their integration into nursing workflows and improving outcomes in diabetic wound management.
Integrative framework linking regenerative biology and AI-driven precision monitoring
A unified framework that tightly integrates regenerative biology with AI-driven analytics is essential for translating DFU management from parallel technological efforts into a coherent precision-medicine ecosystem. Regenerative interventions—such as NDDS-mediated cytokine regulation and exosome-based delivery of pro-healing nucleic acids—produce quantifiable biomarker trajectories that can be transformed into predictive AI signatures. These include dynamic changes in TEWL, cytokine gradients, ECM remodeling indicators, and transcriptomic states that collectively reflect the biological responsiveness of the wound microenvironment. When encoded as temporal feature vectors, such multimodal biomarkers provide a mechanistically meaningful substrate for ML models capable of forecasting healing probability, stratifying patients by expected therapeutic response, and identifying early deviations suggestive of treatment failure.
AI systems further enable objective validation of regenerative therapy by integrating molecular signals with serial imaging assessments. High-frequency wound imaging—capturing granulation patterning, perfusion asymmetry, and tissue optical characteristics—can be correlated with molecular and transcriptomic shifts to construct composite response curves. These cross-modal correlations allow AI to confirm whether biological effects induced by NDDS or exosome therapies are translating into measurable structural improvement, thereby overcoming the limitations of purely clinical inspection. Such integration naturally establishes a biologically informed feedback loop, in which continuous monitoring feeds real-time data into adaptive inference models. These models can recommend adjustments in regenerative treatment intensity, timing, or modality based on predicted healing trajectories and emerging biomarker patterns. By merging TEWL measurements, cytokine panels, imaging features, and transcriptomic signatures into a standardized inference pathway, the resulting analytics pipeline functions as a clinically usable predictive tool—one capable of supporting precision dosing, early intervention, and personalized therapy planning. Collectively, this integrative perspective delineates a robust translational pathway in which regenerative therapeutics and AI-enabled monitoring operate synergistically, enabling DFU management to evolve toward a data-rich, adaptive, and biologically grounded precision-care paradigm.
An integrative framework that couples regenerative biology with AI-driven precision monitoring offers a compelling conceptual pathway toward next-generation management of chronic DFUs. However, a rigorous translational perspective requires clear differentiation between mechanistic efficacy demonstrated in preclinical systems and therapeutic benefit substantiated by human clinical evidence, particularly for advanced regenerative modalities such as EVs and direct tissue reprogramming.
EV-based therapies have generated substantial enthusiasm due to their capacity to deliver miRNAs, proteins, and metabolic regulators that modulate angiogenesis, inflammation, mitochondrial function, and ECM remodeling. In rodent and in vitro models, EVs derived from mesenchymal or epithelial lineages consistently accelerate re-epithelialization, enhance vascular density, and attenuate oxidative stress. Nevertheless, these effects remain context-dependent and highly variable, influenced by EV source, isolation method, cargo heterogeneity, dosing metrics, and delivery route. Importantly, robust clinical evidence demonstrating durable superiority over standard DFU care is still lacking. To date, most human studies remain exploratory or early phase, with limited sample sizes, heterogeneous endpoints, and insufficient longitudinal follow-up to establish reproducibility, dose–response relationships, or long-term safety. Thus, while EVs represent a biologically elegant and potentially scalable cell-free modality, their current status should be regarded as translationally immature rather than clinically established.
A similar distinction applies to direct tissue reprogramming strategies, which aim to convert resident fibroblasts or stromal cells into endothelial, neural, or lymphatic lineages in situ. These approaches address fundamental DFU pathologies—ischemia, neuropathy, and impaired immune drainage—at a mechanistic level that conventional wound dressings cannot reach. Preclinical studies demonstrate impressive restoration of perfusion, axonal regeneration, and microenvironmental homeostasis. However, clinical translation remains speculative, constrained by unresolved challenges in delivery efficiency, spatial control, off-target lineage conversion, and long-term genomic or epigenomic safety. At present, no large-scale human trials have validated the safety or efficacy of in vivo reprogramming for DFUs, underscoring the gap between conceptual innovation and regulatory readiness.
Within this context, AI-driven precision monitoring should not be framed as a validation shortcut for regenerative therapies, but rather as an objective adjudication layer that can expose the discrepancy between molecular activation and true clinical benefit. By integrating longitudinal imaging, functional biomarkers (e.g., TEWL, perfusion asymmetry), and molecular readouts into unified inference models, AI systems can distinguish transient biological signals from sustained tissue recovery. Crucially, such platforms enable comparative effectiveness assessment, benchmarking regenerative interventions against established standards of care—including debridement, off-loading, revascularization, and infection control—rather than evaluating them in isolation.
Therefore, the value of this integrative framework lies not in amplifying optimism, but in enforcing evidence stratification. Regenerative therapies should be positioned along a continuum of translational maturity, with AI serving as a rigor-enhancing tool to (i) identify responder phenotypes, (ii) quantify real-world durability of biological effects, and (iii) define failure modes early in development. Only through this critical, data-anchored integration can regenerative biology advance from mechanistic promise toward reproducible, clinically actionable therapy within DFU care.
Translational barriers: clinical, regulatory, and manufacturing considerations
Although emerging NDDS platforms, exosome therapeutics, and AI-enabled wound-assessment tools show substantial mechanistic promise, their clinical translation remains constrained by several structural limitations. Most regenerative biologics for DFU are supported only by early-phase or preclinical studies, with a lack of Phase II/III trials to establish dose–response relationships, long-term safety, and superiority over standard interventions such as debridement, off-loading, revascularization, and infection control. Regulatory pathways add significant complexity: exosome and gene-modulating nanocarriers frequently fall under ATMP, MDR, or FDA CBER frameworks requiring rigorous CMC documentation, validated potency assays, and robust sterility and stability data, while AI-based systems must fulfill SaMD requirements for external validation, drift monitoring, and human-factors engineering. Manufacturing bottlenecks further hinder clinical feasibility, as EV production suffers from batch variability, inconsistent cargo potency, and high costs due to labor-intensive purification processes and immature GMP pipelines; similarly, NDDS formulations struggle with the reproducibility of nanoparticle attributes essential for quality-by-design compliance. At the digital front, AI wound-analysis models—often trained on single-center, demographically narrow datasets—frequently fail to generalize across populations, imaging devices, and workflows, leading to algorithmic bias and poor external validity. These translational gaps collectively underscore the need for harmonized clinical endpoints, multicenter datasets, scalable and automated bioprocessing, standardized EV and NDDS quality attributes, and regulatory-ready AI validation frameworks to enable safe, reliable, and economically viable integration of next-generation regenerative and digital technologies into real-world DFU care. As summarized in Table 4, the management of diabetic foot ulcers and diabetes care has undergone a progressive paradigm shift, evolving from conventional clinical approaches to AI-enabled regenerative precision medicine.
Concluding remarks
This article presents a structured approach to science communication, transforming complex biomedical AI concepts into an accessible, narrative-based format. Set in Taiwan in 2035, it follows Mr. Da-Ming Wang, an elderly diabetic patient in a semi-rural area who experiences next-generation AI-assisted wound care. Through his journey, advanced computational systems are portrayed as integrated, human-centered tools in clinical decision-making. The framework is organized into three tiers: foundations, core techniques, and applications. The foundations tier covers Data Engineering and Preprocessing (DEP), Knowledge Representation and Reasoning (KRR), and Symbolic AI, which establish the interpretive base of biomedical intelligence. The core techniques tier includes expert systems, ML, DL, and XAI, enabling prediction and transparent reasoning. The applications tier brings these into clinical reality through NLP, computer vision (CV), robotics, and distributed AI multi-agent systems (DAI-MAS), under ethical and regulatory guidance. By embedding this framework in Mr. Da-Ming Wang’s story, the article bridges computation and compassion, illustrating how AI can enhance precision and safety while preserving the human essence of care (Box 1). 44
Box 1. AI-Enabled Decision Support in Diabetic Foot Ulcer Care: A Streamlined Clinical Scenario
Mr. Da-Ming Wang, a 72-year-old patient with long-standing diabetes and recurrent foot ulcers, used an AI-integrated smart dressing at home. The system continuously monitored pH, temperature, and moisture, transmitting data through a validated preprocessing pipeline. When the dressing detected rising temperature and abnormal pH, the AI assistant generated a clear risk alert suggesting early infection and recommended medical evaluation. Upon visiting the hospital, clinicians accessed Mr. Wang’s wound data through his electronic health record. The AI decision-support module analyzed these inputs alongside reference datasets and provided evidence-based guidance, including estimated infection severity and recommended diagnostic imaging. Deep learning–assisted wound assessment highlighted areas suspicious for necrosis, while explainable AI tools visualized the key parameters contributing to the risk score. These outputs supported clinical judgment rather than replacing it.
During treatment planning, the multidisciplinary team used the AI interface to compare therapeutic options and projected outcomes based on established clinical evidence and regional datasets. After debridement and antimicrobial therapy, Mr. Wang continued rehabilitation with remote monitoring. The AI system summarized daily wound images, flagged deviations from expected healing trajectories, and notified clinicians only when clinically meaningful deterioration was detected. This scenario illustrates how AI can support a practical, closed-loop wound-care workflow—linking patient-generated data, clinician assessment, and interpretable algorithmic insights—to enhance timely decision-making and individualized DFU management.
Translating such a scenario into routine clinical practice requires a staged development pathway. First, each AI module—image-based wound classifiers, risk-prediction algorithms, and sensor anomaly detectors—must undergo independent analytical and clinical validation with predefined performance metrics and external, multicenter testing. Second, smart dressings, biosensors, and decision-support software need feasibility and safety trials in DFU populations to establish reliability, usability, and patient adherence. Third, integrative studies are necessary to verify interoperability among sensing hardware, electronic health records, and AI platforms, ensuring robust data flow and effective human–machine interaction at the bedside. Finally, pragmatic multicenter clinical trials should compare this closed-loop, AI-assisted workflow against optimized standard care, evaluating healing outcomes, infection and amputation rates, clinician workload, and cost-effectiveness. Only through this sequential validation and integration process can real-time AI-assisted wound care of the type depicted here be credibly and safely implemented at scale.
The present review underscores that, although DFU research now spans diverse scientific frontiers—including molecular wound biology, nanotechnology, stem cell and EV therapeutics, GMP manufacturing, gene editing, multispectral imaging, thermal sensing, and advanced AI analytics—the resulting conceptual breadth risks diluting clinical depth. By synthesizing these scattered domains through a more clinically anchored lens, several unifying principles emerge. First, when benchmarked against standard DFU care, regenerative nanotherapies and AI-driven diagnostic systems demonstrate clear mechanistic promise but remain unevenly validated in human populations. Most efficacy data for NDDSs, growth factors, or exosome-based interventions originate from rodent models whose inflammatory dynamics, vascular architecture, and chronicity do not fully recapitulate human DFUs, thereby limiting translational predictability. Likewise, AI platforms trained on institution-specific datasets lack the external validation, workflow integration, and interpretability required for dependable clinical deployment.
A refined synthesis therefore highlights the need to transition from mechanistic enumeration toward clinically meaningful evaluation—specifically, how emerging technologies improve healing trajectories, diagnostic sensitivity, or decision-making compared with current standards such as sharp debridement, pressure off-loading, infection control, and revascularization. NDDSs and exosome-based therapeutics must be assessed through harmonized potency metrics, dose–response relationships, and reproducible human trial endpoints. Similarly, AI systems should be positioned not as standalone solutions but as clinician-supervised tools embedded within real-world workflows, providing actionable trend detection, early deterioration alerts, and objective comparison against established DFU management guidelines.
Looking forward, true innovation lies in bridging existing evidence gaps. This requires (i) multicenter clinical trials that align mechanistic advances with patient-centered outcomes; (ii) translational animal models that more accurately mirror ischemic, neuropathic, and infectious dimensions of human DFUs; (iii) standardized datasets and validation protocols for AI-driven wound assessment; and (iv) comparative studies quantifying the added value of regenerative or AI-assisted platforms relative to conventional care. By consolidating mechanistic insights into clinically grounded frameworks, next-generation NDDSs, exosome therapeutics, and AI-enabled sensing can evolve from fragmented technological innovations into coherent, evidence-based strategies. Ultimately, such integration will accelerate the development of precision, scalable, and clinically actionable solutions capable of transforming DFU management in real-world practice.
Innovation
This study introduces a transformative paradigm integrating NDDSs, stem cell–derived EVs, and AI-enabled sensing for precision diabetic wound management. By uniting regenerative nanotherapeutics with DL-driven image analytics and wearable biosensors, it enables real-time wound profiling, adaptive drug release, and predictive healing assessment. This closed-loop platform transcends conventional treatment boundaries, establishing an intelligent regenerative ecosystem that bridges molecular therapeutics and digital diagnostics—advancing DFU care toward proactive, personalized, and data-guided regeneration.
KEY FINDINGS
Nanodrug delivery systems enable precise, sustained delivery of growth factors and miRNAs, restoring angiogenesis and suppressing inflammation in diabetic wounds. Stem cell–derived extracellular vesicles act as stable cell-free therapeutics, enhancing vascular repair and metabolic regulation through paracrine signaling. AI-driven imaging and biosensors provide real-time, high-accuracy wound assessment and predictive healing analytics. Integrating regenerative nanotherapy with AI establishes a closed-loop, personalized platform for intelligent diabetic foot ulcer management.
AUTHORS’ CONTRIBUTIONS
Conceptualization: H.-J.L. and Y.-F.W.; investigation: H.-J.L. and T.-C.L.; writing—original draft preparation: H-J.L. and T-C.L.; writing—review and editing: H.-J.L. and Y.-F.W.; supervision: H.-J.L. and Y.-F.W.; project administration: H-J.L. and Y-F.W.; and funding acquisition: H.-J.L. and Y.-F.W. All authors have read and agreed to the published version of the article.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The authors thank the Institute of Biopharmaceutical Sciences, National Yang Ming Chiao Tung University, for their support of this project. This research was funded by the Ministry of Science and Technology (MOST 111-2314-B-418-004, MOST 111-2321-B-418-002-, MOST 111-2314-B-418-003-, NSTC 112-2321-B-418-004-, and NSTC 112-2314-B-418-010-MY3), Far Eastern Memorial Hospital (FEMH; 2022-C-042, 2022-C-123, 2023-C-124, 2024-C-105, 2025-C-093, and 2025-C-010), and National Taiwan University Hospital–FEMH Cooperation (114-FTN0001).
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors declare no conflicts of interest.