
Abstract
Background:
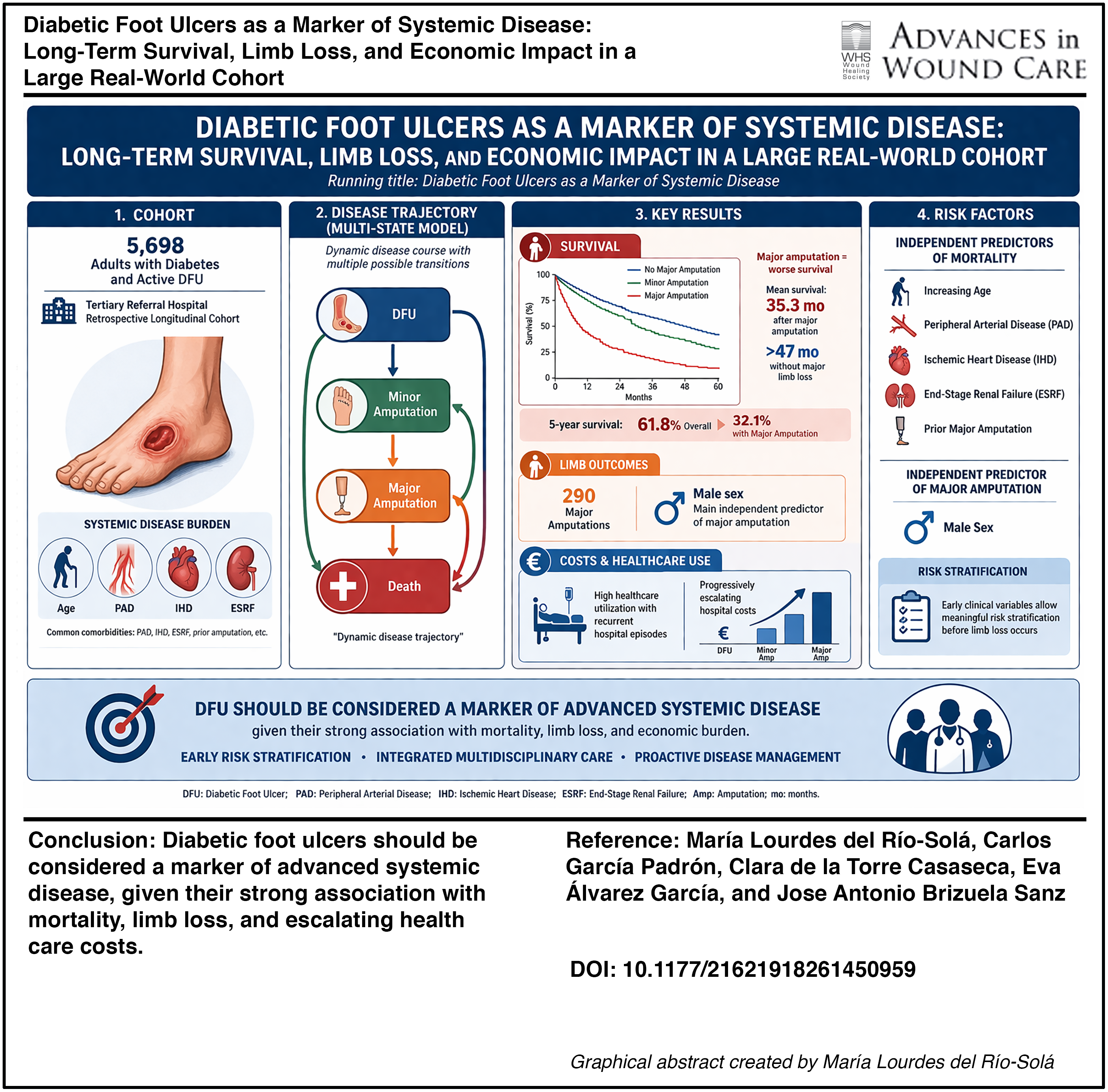
Diabetic foot ulcers (DFUs) represent one of the most severe complications of diabetes mellitus and are associated with limb loss, excess mortality, and substantial health care costs. Although DFUs are often approached as a localized wound condition, increasing evidence suggests that they reflect advanced systemic vascular and metabolic disease. However, large real-world longitudinal studies integrating wound outcomes, survival, and economic burden remain scarce.
Objectives:
The objective of this study is to evaluate long-term clinical outcomes, survival, and health care costs associated with DFUs in a large real-world cohort and to identify factors independently associated with mortality and limb loss.
Methods:
We conducted a retrospective longitudinal cohort study including 5,698 adult patients with diabetes treated for active DFUs at a tertiary referral hospital. Minor and major amputations, survival outcomes, health care utilization, and estimated direct hospital costs were analyzed. Time-to-event analyses included Kaplan–Meier estimation, competing-risk regression, and multivariable Cox proportional hazards models. Disease trajectories were further explored using multistate modeling.
Results:
During follow-up, 290 major amputations were recorded. Patients undergoing major amputation showed significantly worse survival compared with nonamputated patients or those with minor amputations (log-rank p < 0.001). Mean survival after major amputation was 35.3 months, compared with more than 47 months in patients without major limb loss. Five-year overall survival was 61.8%, decreasing to 32.1% among patients with major amputation. Increasing age, peripheral arterial disease, ischemic heart disease, end-stage renal failure, and prior major amputation were independently associated with mortality. Male sex emerged as the main independent predictor of major amputation in adjusted competing-risk models. DFU-related care was associated with high health care utilization and progressively escalating hospital costs.
Conclusions:
DFUs should be regarded as a marker of advanced systemic disease rather than an isolated wound condition, given their strong association with long-term mortality, limb loss, and economic burden. Early risk stratification and integrated multidisciplinary care strategies are essential to improve outcomes in this high-risk population.
Keywords
INTRODUCTION
Diabetes mellitus represents a major and growing global public health challenge. In 2014, an estimated 422 million people worldwide were living with diabetes, corresponding to a global prevalence of 8.5%. 1 Among adults with diabetes, the lifetime risk of developing a diabetic foot ulcer (DFU) is estimated to range between 15% and 25%. 2 Diabetic foot disease is associated with substantial morbidity, impaired quality of life, and increased mortality and remains one of the leading causes of hospitalization and lower-extremity amputation in this population. 3
María Lourdes del Río-Solá, MD, PhD

The global burden of DFUs is considerable. A 2017 systematic review and meta-analysis estimated a worldwide DFU prevalence of 6.3%, with marked regional variation. 4 Beyond ulceration itself, diabetes-related lower-extremity complications affect a substantial proportion of the global population; in 2016, approximately 131 million individuals were affected, with age-standardized rates increasing by 15.9% between 1990 and 2016. 5 These figures highlight diabetic foot disease as a major contributor to disability and premature mortality worldwide.
In addition to its clinical impact, diabetic foot disease imposes a disproportionate economic burden on health care systems. Population-based and hospital-based studies have consistently shown that a relatively small subset of patients with diabetes accounts for a large share of diabetes-related health care expenditure, largely driven by recurrent hospitalizations, prolonged length of stay, and surgical interventions.6–8 In large tertiary health care networks, inpatient wound care alone has been reported to generate costs exceeding hundreds of millions of U.S. dollars annually, with frequent readmissions and escalating per-patient costs over time.6,7
BOX A. Clinical Practice Summary
Diabetic foot ulcers (DFUs) should be considered a marker of advanced systemic disease rather than an isolated wound condition.
Patients with DFUs have substantial long-term mortality, comparable with other high-risk chronic conditions.
Major amputation represents a critical clinical and economic inflection point, associated with a marked decline in survival and increased health care costs.
Early clinical variables—including age, peripheral arterial disease, ischemic heart disease, end-stage renal failure, and sex—allow meaningful risk stratification before limb loss occurs.
Disease trajectories are dynamic, with frequent transitions between ulcer, amputation, and death, requiring continuous reassessment rather than static evaluation.
Recurrent health care episodes are common and concentrated in patients with advanced systemic comorbidity.
Early identification of high-risk patients should prompt intensified surveillance, multidisciplinary management, and timely referral.
These findings support a shift from reactive wound care to proactive, system-oriented disease management.
Despite this substantial burden, most existing studies provide cross-sectional or short-term assessments, frequently focusing on isolated outcomes such as ulcer healing or amputation. Such approaches offer limited insight into long-term clinical trajectories, competing outcomes such as amputation and death, recurrent care episodes, and the cumulative economic impact of diabetic foot disease. Moreover, real-world longitudinal data capturing the full course of diabetic foot disease within tertiary referral hospitals remain scarce.
BOX B. Competing-Risk Analysis: Clinical Implications
In patients with DFUs, death frequently occurs before major amputation.
Traditional survival analyses may overestimate the probability of limb loss by not accounting for competing mortality.
Competing-risk models provide a more accurate estimate of real-world event probabilities.
Some variables may appear important in unadjusted analyses but lose significance after accounting for competing events.
Clinical interpretation should integrate both limb outcomes and survival rather than considering amputation in isolation.
“Limb salvage success” should be interpreted in the context of overall patient prognosis.
Increasing evidence suggests that DFUs should not be regarded solely as a localized wound problem, but rather as a marker of advanced systemic disease, frequently coexisting with severe vascular, cardiac, and renal comorbidities. However, comprehensive longitudinal analyses integrating survival, limb-related events, recurrent health care utilization, and costs within a unified analytical framework are lacking.
Therefore, the present study aimed to evaluate diabetic foot disease as a marker of systemic disease using a real-world longitudinal cohort from a tertiary referral hospital. The primary objectives were to assess long-term survival and limb-related outcomes, accounting for competing risks between amputation and death. Secondary objectives included the characterization of recurrent care episodes, disease-course trajectories using multistate modeling, and the estimation of hospital-related costs over a 5-year follow-up period. Finally, we sought to translate these findings into clinically meaningful risk stratification tools to support personalized management and resource allocation in routine clinical practice.
BOX C. Risk Stratification and Clinical Decision-Making
A simplified bedside risk score can support early identification of patients at high risk of major amputation and mortality.
Risk stratification enables tailored follow-up intensity and prioritization of high-risk patients.
Patients at higher risk may benefit from earlier vascular assessment, aggressive management of comorbidities, and closer monitoring.
Integration of routinely available clinical variables into decision-making frameworks can improve resource allocation.
These tools support proactive multidisciplinary management and more efficient use of health care resources.
CLINICAL PROBLEM ADDRESSED
DFUs represent one of the most severe and costly complications of diabetes mellitus, with a profound impact on patient survival, limb loss, and health care resource utilization. While DFUs are traditionally approached as a localized wound problem, growing evidence suggests that they frequently coexist with advanced systemic comorbidities such as peripheral arterial disease (PAD), ischemic heart disease (IHD), and renal failure. However, in routine clinical practice, the presence of a DFU is often not fully recognized as a marker of global disease severity and long-term risk.
Clinicians face significant challenges in accurately stratifying the risk of major amputation and mortality in patients with DFUs, particularly in the context of competing events, recurrent care episodes, and heterogeneous clinical trajectories. Existing studies frequently focus on single outcomes, short follow-up periods, or selected populations, limiting their applicability to real-world decision-making.
This study addresses the clinical need for a comprehensive, longitudinal assessment of DFUs as a systemic disease marker. By integrating survival analysis, competing-risk modeling, multistate disease-course analysis, and pragmatic risk stratification tools in a large real-world cohort, the present work aims to support clinicians in identifying high-risk patients, optimizing multidisciplinary management, and informing personalized follow-up and preventive strategies.
We propose a conceptual model of DFU as a systemic disease trajectory integrating clinical progression, systemic drivers, and economic burden (Fig. 1).
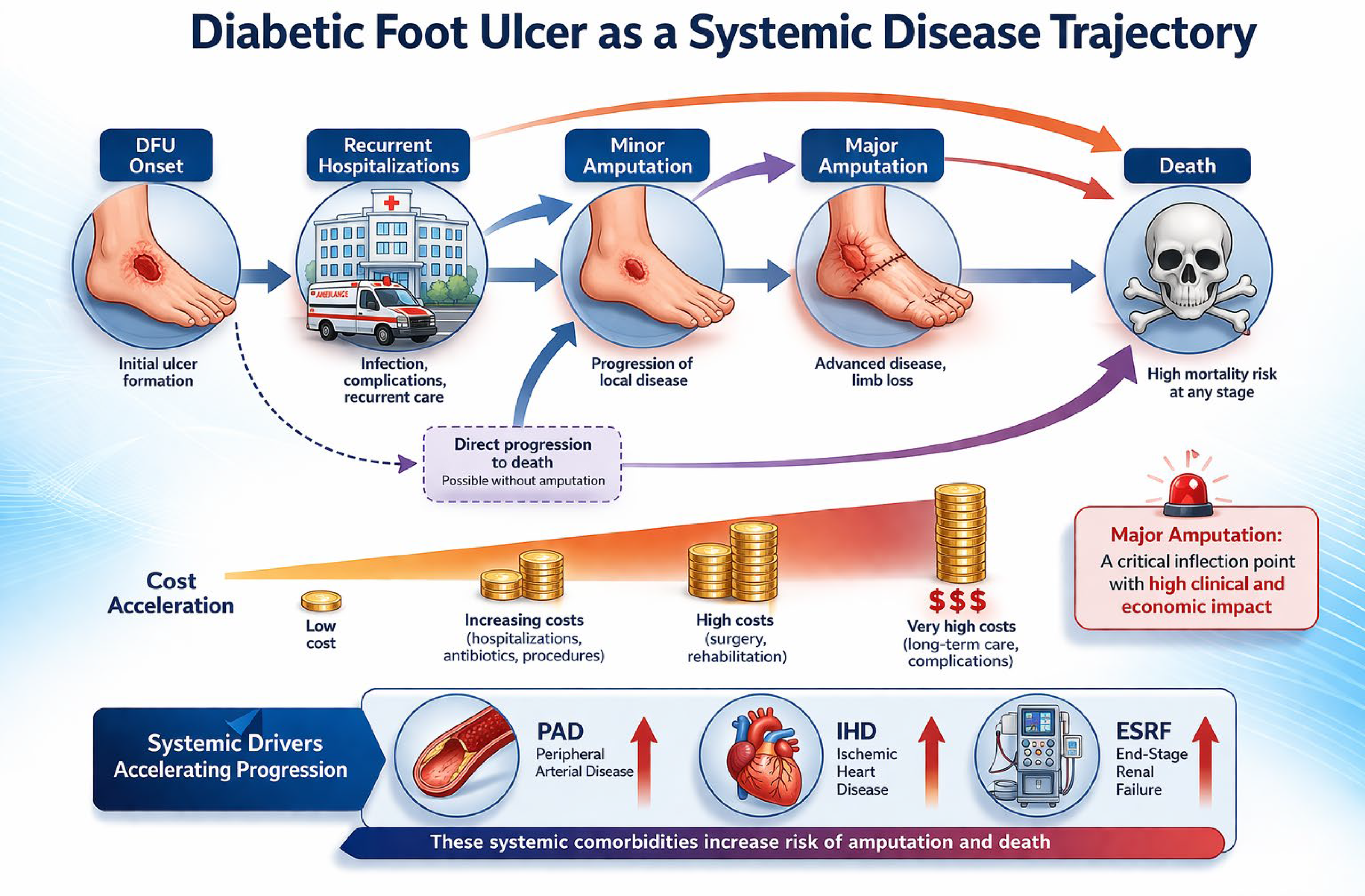
Diabetic foot ulcer (DFU) as a progressive systemic disease leading to amputation, death, and escalating costs. Conceptual model illustrating DFU as a progressive systemic condition rather than a localized disease. The trajectory depicts the clinical evolution from DFU onset through recurrent hospitalizations, minor and major amputations, and death. Key systemic drivers—including peripheral arterial disease (PAD), ischemic heart disease (IHD), and end-stage renal failure (ESRF)—are integrated as factors that accelerate progression and worsen outcomes. The model also highlights the progressive escalation of health care costs across disease stages, identifying major amputation as a critical inflection point with substantial clinical and economic impact.
MATERIALS AND METHODS
Study design, population, and setting
We conducted a retrospective, observational longitudinal study based on routinely collected inpatient and outpatient data over a 5-year period, from January 1, 2020, to December 31, 2024, at a university-affiliated tertiary referral hospital in Spain. This institution provides comprehensive specialized care and functions as a regional reference center for complex diabetic foot disease, managing a high volume of patients with advanced ulcers, severe infection, PAD, and limb-threatening ischemia.
The study population comprised consecutive adult patients with diabetes who were evaluated or treated for a diabetic foot lesion during the study period. The index episode was defined as the first documented presentation of a diabetic foot lesion within the hospital during the study timeframe. Patients were subsequently followed longitudinally to capture clinical outcomes, health care utilization, and costs under routine clinical practice conditions.
The analysis integrated clinical, administrative, and health care utilization data to characterize the systemic and economic burden of diabetic foot disease in a real-world setting. Patient-level data were analyzed longitudinally for time-to-event outcomes, including survival and limb-related events. Health care utilization variables—such as emergency department visits, hospital admissions, length of stay, procedures, and interventions—were analyzed at the episode level, allowing for recurrent-event modeling and appropriate accounting for within-patient correlation.
Data sources and case identification
Data were retrieved from institutional administrative and clinical databases, including inpatient admission records, emergency department registries, outpatient clinic activity, and procedural datasets. These sources capture all health care episodes delivered within the hospital and are routinely used for clinical management, reporting, and health services research. Patients with diabetic foot lesions were identified using a combination of International Classification of Diseases diagnostic codes related to diabetes mellitus and diabetic foot disease, together with procedural codes corresponding to lower-extremity amputations and other foot-related surgical interventions. Only health care episodes directly attributable to diabetic foot pathology were included. Admissions or procedures clearly unrelated to diabetic foot disease were excluded following expert clinical review of patient pathways. Data were retrieved from institutional clinical and administrative databases. Electronic laboratory notebook was not used.
Study population
The study population consisted of adult patients (≥18 years) with a diagnosis of diabetes mellitus who received care for active diabetic foot lesions during the study period. Patients were included if they had at least one diabetic foot–related emergency department visit, hospital admission, or specialist outpatient consultation.
Active diabetic foot lesions were defined as foot ulceration, infection, gangrene, or health care episodes related to ongoing or previous lower-extremity amputations requiring hospital-based evaluation or treatment. Both inpatient and outpatient episodes related to diabetic foot disease were considered, including admissions for wound management, infection control, surgical debridement, minor or major amputations, and antibiotic therapy.
Given the chronic and recurrent nature of diabetic foot disease, individual patients could contribute multiple health care episodes over the 5-year period. Health care utilization analyses were therefore performed at the episode level to capture the cumulative burden of care, while patient-level analyses accounted for within-patient correlation, as described in the statistical analysis section.
Clinical management and definitions
Patients were managed according to routine institutional clinical practice and contemporary international guideline recommendations. Care was delivered within a multidisciplinary diabetic foot team involving vascular surgery, endocrinology, infectious diseases, orthopedic surgery, podiatry, and specialized wound care nursing. 9
In accordance with International Working Group on the Diabetic Foot guidelines, patients with predominantly neuropathic ulcers received medical optimization, local wound care, and appropriate off-loading, while patients with ischemic or neuroischemic ulcers underwent vascular assessment and revascularization when clinically indicated, followed by wound care and off-loading. 10 Whenever possible, patients were managed in outpatient or day-hospital settings, with hospital admission reserved for severe infection, limb-threatening ischemia, or surgical intervention.
Surgical procedures, including debridement and amputation, were performed based on clinical judgment and standard indications. Lower-extremity amputations were classified according to standard anatomical definitions. Minor amputation was defined as any amputation distal to the ankle joint, whereas major amputation was defined as amputation proximal to the ankle joint, including below-knee and above-knee amputations.
Outcomes and variables
Health care utilization outcomes included the incidence of hospital admissions, emergency department visits, specialist outpatient consultations, and surgical procedures attributable to diabetic foot disease. Length of hospital stay was calculated for each admission and aggregated to estimate cumulative inpatient burden at the patient level.
Clinical outcomes included the occurrence of minor and major lower-extremity amputations, wound-related surgical procedures, and all-cause mortality. Survival outcomes were assessed using time-to-event analyses, including overall survival and amputation-related endpoints.
Given the high competing risk of death in this population, death was treated as a competing event for time to first major amputation, as it precludes the occurrence of amputation as the first observed event during follow-up. Conversely, major amputation was considered a competing event in mortality analyses when modeling time to death as the first event.
Major amputations were recorded as events rather than patient-level variables. Therefore, when applicable, multiple major amputations occurring in the same individual were counted as separate events. Baseline patient characteristics included age and sex. Relevant comorbidities were identified from diagnostic codes and included PAD, IHD, end-stage renal failure (ESRF), and prior cerebrovascular disease.
PAD, IHD, ESRF, and diabetic neuropathy were identified based on diagnostic codes recorded in the institutional clinical and administrative databases. ESRF was defined as advanced chronic kidney disease requiring dialysis or renal replacement therapy. Diabetic neuropathy was defined based on clinical diagnosis documented in patient records.
The institutional database used for this study is prospectively maintained and includes systematically recorded clinical variables as part of routine clinical care. For the variables included in the present analysis, data completeness was ensured, and no missing values were observed.
Cost estimation
Economic evaluation was conducted from the institutional hospital perspective. Direct health care costs were estimated using standardized hospital tariffs applied to emergency department visits, inpatient admissions, length of hospital stay, and diabetic foot–related procedures. Inpatient hospitalization was considered the primary cost driver and was calculated by multiplying the total number of inpatient days by the official cost per hospital day. This approach provides a conservative estimate of minimum direct hospital costs attributable to diabetic foot disease and facilitates comparison with previous real-world economic analyses. Only health care episodes directly attributable to diabetic foot disease were included, and hospitalizations or health care utilization related to systemic comorbidities (such as cardiovascular or renal events) was not captured in this analysis. Costs were expressed in euros (€) and summarized as cumulative costs over the 5-year study period, as well as mean annual costs and costs per health care episode. Indirect costs, outpatient pharmaceutical expenses, community care, and postdischarge costs were not included. This approach allowed a standardized and reproducible estimation of direct hospital costs attributable to diabetic foot disease, enabling meaningful comparisons across clinical subgroups and over time.
Statistical analysis
Statistical analyses were conducted to characterize health care utilization, clinical outcomes, economic burden, and disease trajectories in patients with diabetic foot disease. Continuous variables were summarized as mean and standard deviation or median and interquartile range, as appropriate. Categorical variables were reported as absolute counts and percentages. Time-to-event analyses were performed to evaluate overall survival and limb-related outcomes. Given the high mortality in this population, competing-risk methodology was applied. Cumulative incidence functions (CIFs) were estimated for major amputation and for death, treating each outcome as a competing event for the other. Both cause-specific Cox proportional hazards (PH) models and Fine–Gray subdistribution hazard models were fitted to estimate hazard ratios (HRs) with 95% confidence intervals (CIs).
PH assumptions were assessed using Schoenfeld residuals and formal statistical tests. When violations were detected, time-varying coefficients or stratified baseline hazards were applied as appropriate. To account for the chronic and relapsing nature of diabetic foot disease, recurrent-event analyses were performed for health care episodes using models appropriate for repeated events, with clustering at the patient level to obtain robust standard errors. Rate ratios or HRs were estimated according to the selected recurrent-event framework. Disease progression was further examined using a multistate model reflecting clinically relevant transitions between ulcer without amputation, minor amputation, major amputation, and death. Transition-specific hazard models were fitted, and state occupation probabilities were estimated at 1, 3, and 5 years. Parsimonious risk prediction models were developed for major amputation and for 1- and 5-year all-cause mortality using Cox regression. Model performance was internally validated using bootstrap resampling to estimate optimism-corrected discrimination (C-index), calibration slope, and calibration-in-the-large. Calibration plots and receiver operating characteristic curves were generated. Clinical utility of the risk scores was evaluated using decision-curve analysis (DCA), estimating net benefit across a range of clinically relevant threshold probabilities and comparing the models with treat-all and treat-none strategies. Mediation analyses were conducted to assess whether major amputation partially mediated the association between key comorbidities and mortality, estimating natural direct and indirect effects with bootstrap CIs. Prespecified interaction terms and subgroup analyses were examined to explore effect modification. Missing data were addressed using multiple imputations by chained equations where applicable, and results were compared with complete-case analyses. Additional sensitivity analyses included clustered versus naïve variance estimation and temporal validation using a hold-out test set from the final calendar year of the study.
All analyses were performed using IBM SPSS Statistics (version 29.0; IBM Corp., Armonk, NY, USA) and the R statistical environment (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was defined as a two-sided p value <0.05.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki. Approval was obtained from the local institutional ethics committee (PI-25-571-C), which waived the requirement for informed consent due to the retrospective observational design and the use of fully anonymized administrative data, in accordance with national regulations and institutional policies.
RESULTS
Study population and baseline characteristics
A total of 5,698 adult patients with diabetes mellitus and an index diabetic foot lesion were included in the study. The mean age of the cohort was 63.4 years, and 64.4% were male. At presentation, ulcer without amputation was the most frequent clinical state, while minor and major amputations accounted for progressively smaller but clinically relevant subgroups.
Patients who ultimately underwent major amputation were significantly older and more frequently male compared with those managed without amputation (Table 1). Cardiovascular and systemic comorbidities were highly prevalent across the cohort, particularly PAD (74.8%), chronic kidney disease (61.6%), and IHD (49.9%). The burden of comorbid disease increased stepwise from ulcer-only patients to those undergoing minor and major amputations, with ESRF and PAD showing the strongest gradients (both p < 0.001). Documented wound location was available in a subset of patients, with toe and plantar ulcers being the most common anatomical sites. Biochemical parameters were inconsistently available and were not used for primary risk adjustment.
Patient characteristics at date of index diabetic foot lesion (n = 5,698)
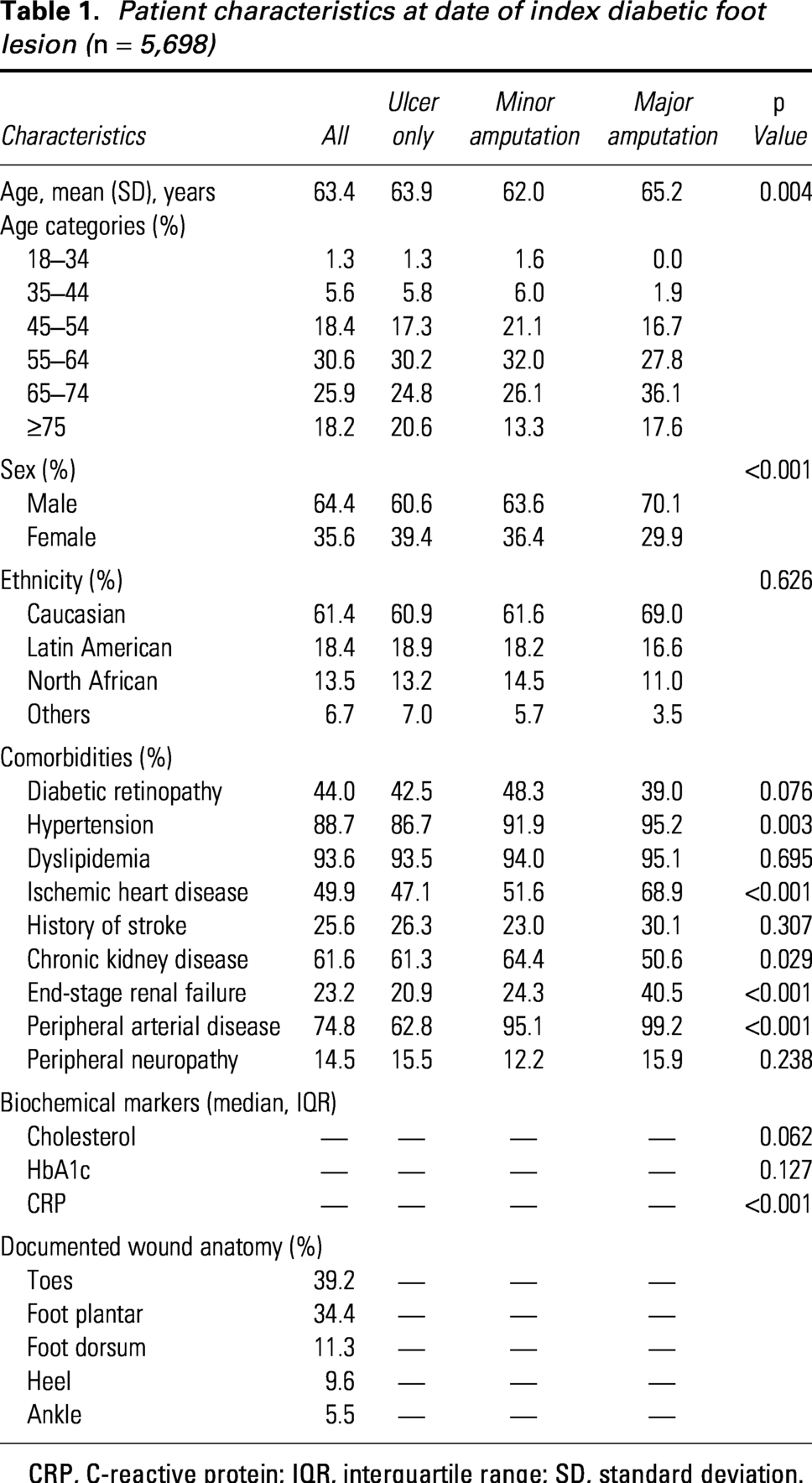
CRP, C-reactive protein; IQR, interquartile range; SD, standard deviation.
Health care utilization and surgical interventions
Over the 5-year study period, diabetic foot disease generated substantial health care utilization. In total, the cohort accounted for 9,820 emergency department visits, 46,300 specialist outpatient consultations, and 4,980 inpatient admissions, corresponding to a mean of 0.87 hospitalizations per patient. The overall 30-day readmission rate was 13.1%, reflecting the chronic and relapsing nature of the disease. Mean inpatient length of stay was 17.4 days, increasing markedly with disease severity: 13.8 days in ulcer-only patients, 21.6 days following minor amputation, and 61.2 days after major amputation (Table 2).
Costs and health care utilization in patients with diabetic foot disease
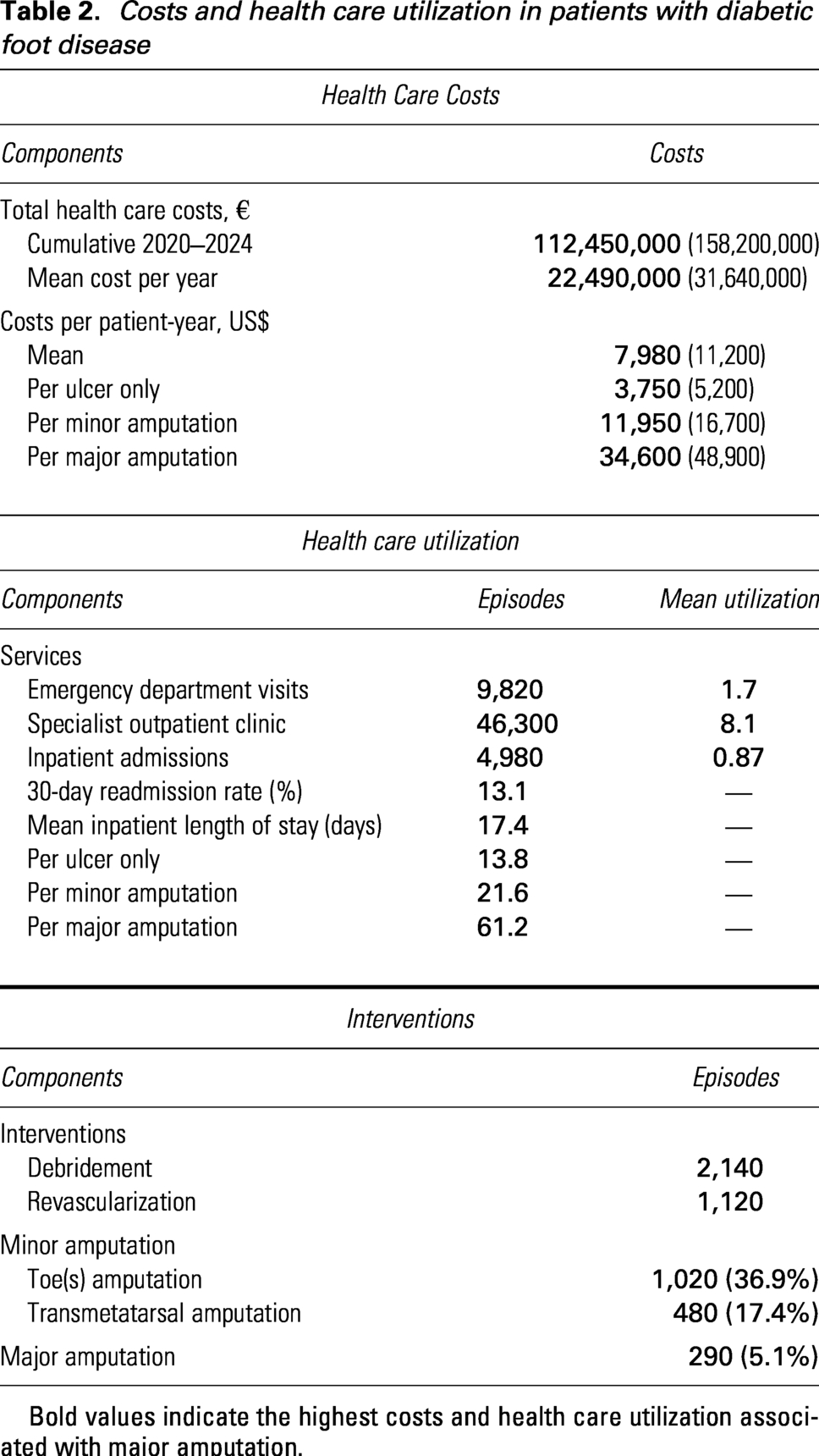
Bold values indicate the highest costs and health care utilization associated with major amputation.
Regarding interventions, 2,140 surgical debridements and 1,120 revascularization procedures were performed. A total of 1,500 amputations occurred during follow-up, including 1,020 toe amputations, 480 transmetatarsal amputations, and 290 major amputations, corresponding to 5.1% of the entire cohort. These findings provide a comprehensive real-world quantification of health care resource utilization associated with diabetic foot disease, highlighting its sustained burden on hospital systems.
Survival outcomes and amputation-free survival
Unadjusted survival analyses demonstrated a strong association between limb loss and long-term mortality. Kaplan–Meier curves showed significantly reduced overall survival in patients undergoing major amputation, with early and sustained separation from the curves corresponding to minor amputation and ulcer-only management (Fig. 2). At 5 years, overall survival was 61.8% in the entire cohort but declined to 32.1% in patients with major amputation, compared with 62.0% after minor amputation and 64.0% in patients without amputation (Table 3). Age, PAD, IHD, stroke history, and ESRF were consistently associated with worse survival across strata.
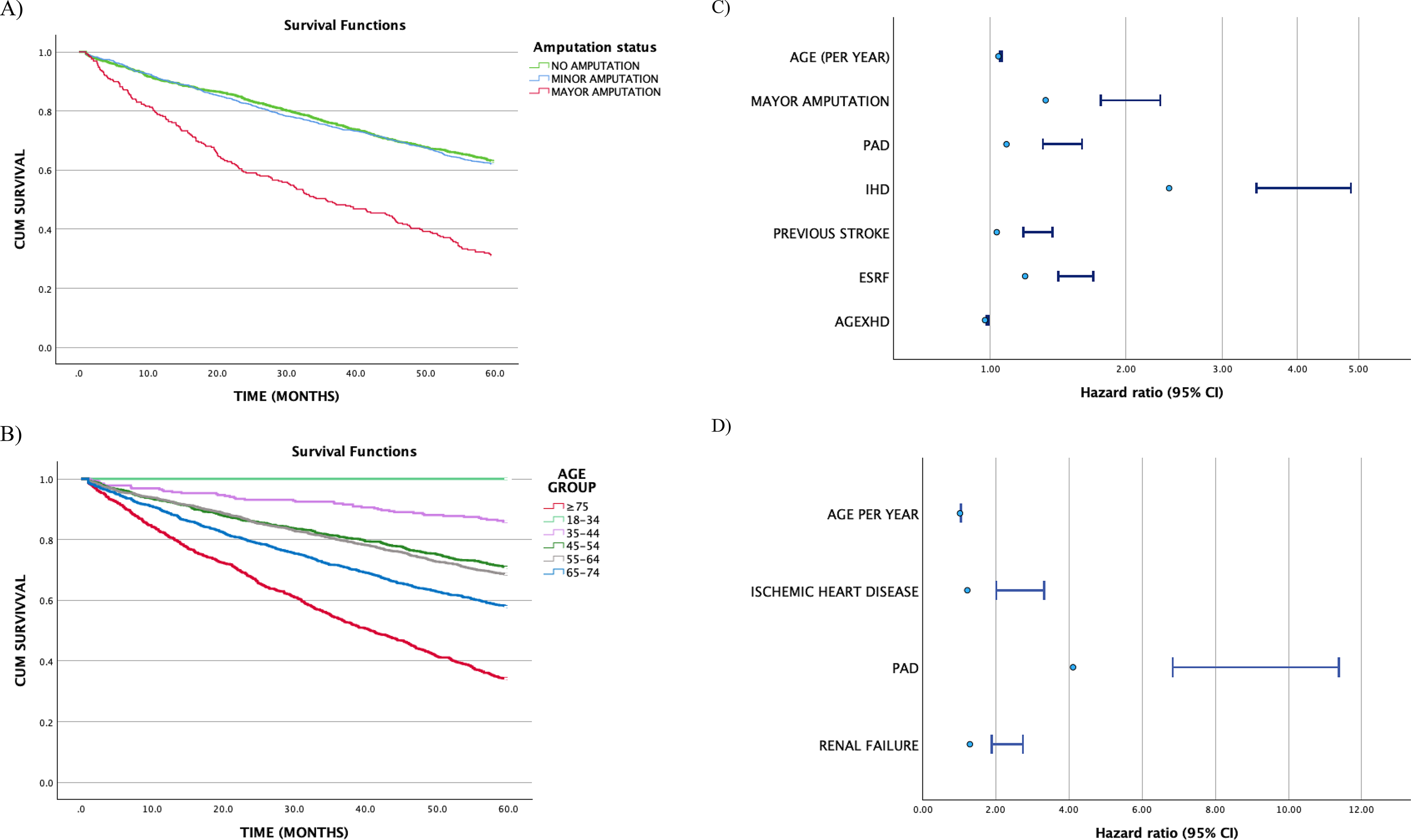
Major amputation and age are associated with markedly reduced survival in patients with diabetic foot ulcers.
Survival probabilities for major amputation–free survival, minor amputation–free survival, and overall survival
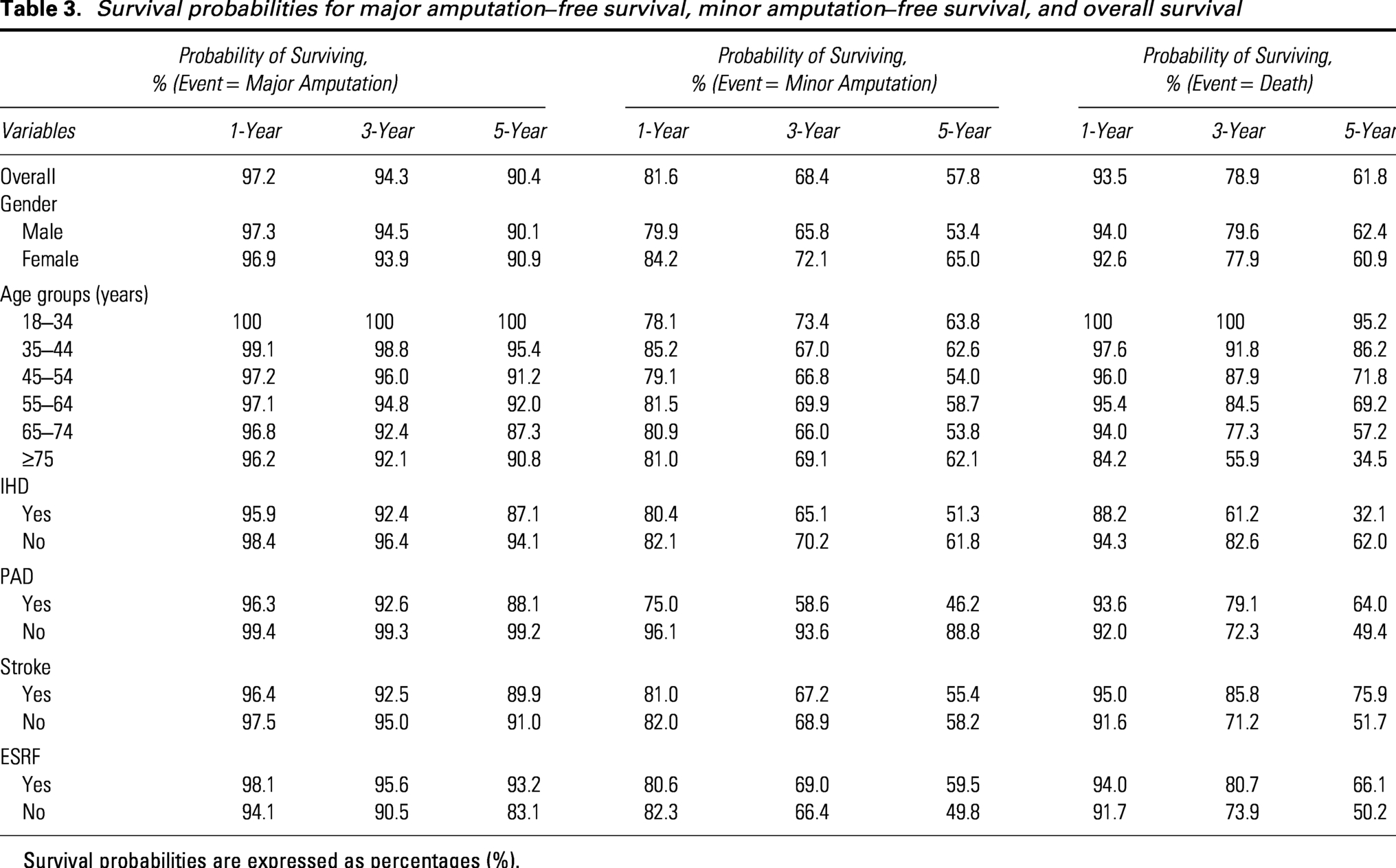
Survival probabilities are expressed as percentages (%).
Competing-risks analysis for amputation and death
Given the high competing risk of death in this population, CIFs were estimated for major amputation and all-cause mortality using competing-risks methodology (Fig. 2). Throughout follow-up, death represented the dominant competing event, particularly among older patients and those with advanced comorbidity, substantially influencing the observed incidence of limb loss. In cause-specific Cox models for major amputation, male sex was strongly associated with an increased hazard of major amputation (cause-specific HR 4.01, 95% CI 2.64–6.08; p < 0.001). Age, PAD, IHD, and ESRF were not independently associated with the cause-specific hazard of major amputation after adjustment (Table 4). Fine–Gray subdistribution hazard models yielded consistent results. Male sex remained independently associated with a markedly higher cumulative incidence of major amputation after accounting for the competing risk of death (subdistribution HR 3.85, 95% CI 2.54–5.83; p < 0.001). Age (sHR 1.00, 95% CI 0.99–1.01), PAD (sHR 0.85, 95% CI 0.60–1.20), IHD (sHR 1.32, 95% CI 0.96–1.80), and ESRF (sHR 0.88, 95% CI 0.60–1.28) were not significantly associated with the cumulative incidence of major amputation in the competing-risks framework. For all-cause mortality, neither cause-specific nor subdistribution hazard models identified age, sex, PAD, IHD, or ESRF as independent predictors within the competing-risks framework (all p > 0.05; Table 4), reflecting the complex interplay between comorbidity burden, limb events, and survival in this cohort. Overall, the side-by-side presentation of cause-specific and subdistribution HRs (Table 4) highlights the importance of accounting for competing risks in diabetic foot disease, demonstrating that etiologic associations may differ from cumulative incidence estimates when mortality is frequent.
Cause-specific Cox and Fine–Gray competing-risk regression models for major amputation and all-cause mortality
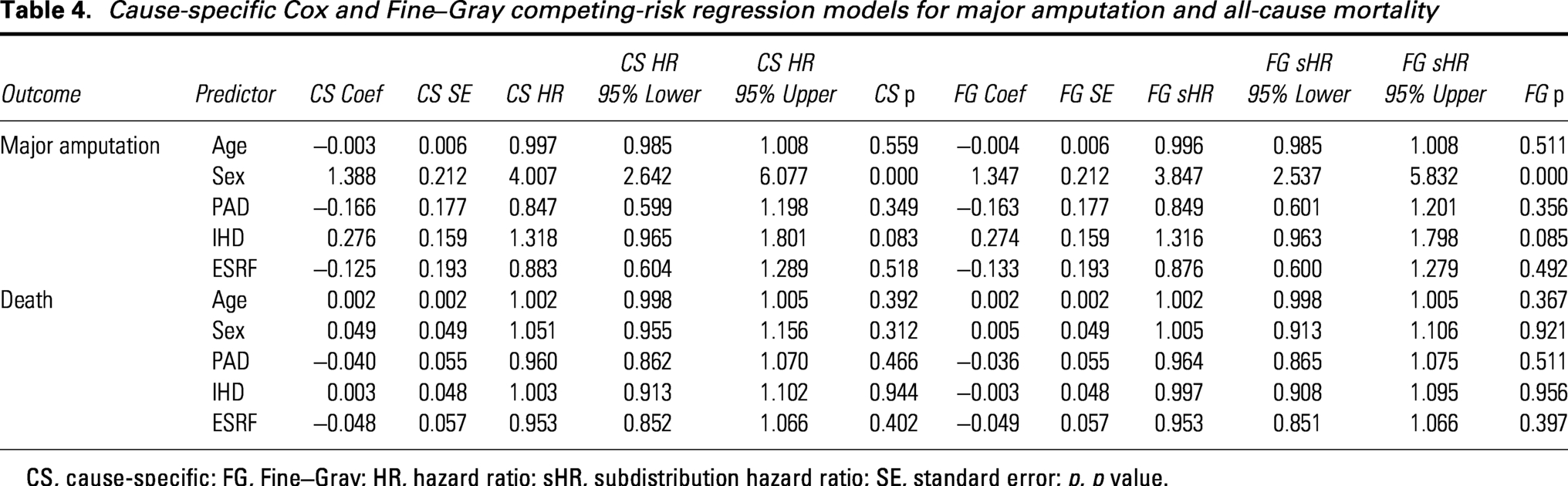
CS, cause-specific; FG, Fine–Gray; HR, hazard ratio; sHR, subdistribution hazard ratio; SE, standard error; p, p value.
From a clinical perspective, these findings have important implications for outcome interpretation in patients with DFUs. In high-risk individuals, death frequently occurs before major amputation can be observed, meaning that conventional estimates of amputation rates may underestimate the true severity of limb-threatening disease. Consequently, a low observed amputation rate should not be interpreted as a favorable outcome in isolation, but rather in the context of substantial competing mortality risk. This reinforces the need to consider limb-related and systemic outcomes simultaneously when evaluating prognosis and guiding clinical decision-making.
PH diagnostics and time-varying effects
The PH assumption for cause-specific Cox models was formally assessed using global and covariate-specific Schoenfeld residual tests (Table 5; Supplementary Fig. S1).
Proportional hazards assumption testing for cause-specific Cox models using Schoenfeld residuals
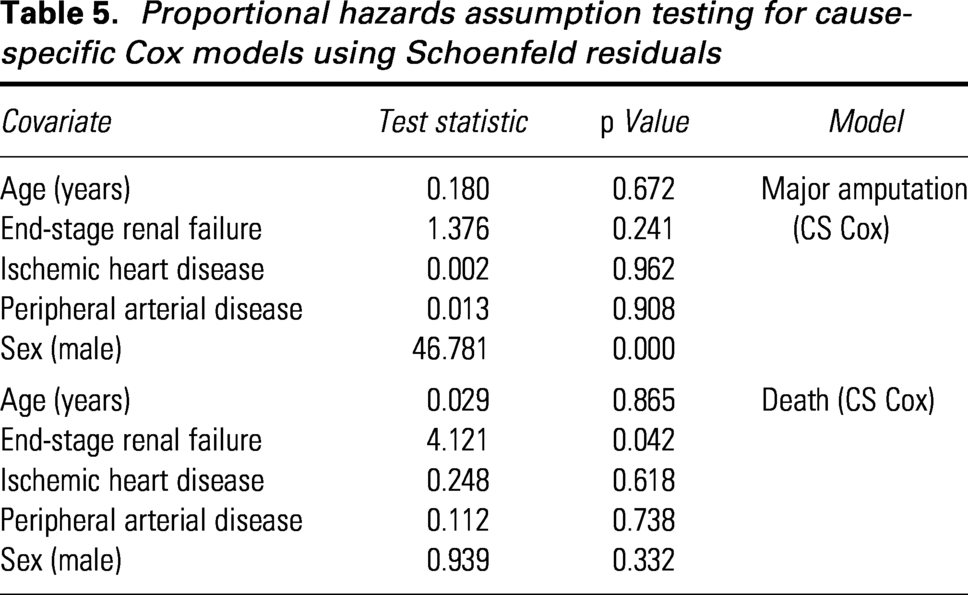
For the cause-specific model of major amputation, no evidence of violation of the PH assumption was observed for age (p = 0.672), PAD (p = 0.908), IHD (p = 0.962), or ESRF (p = 0.241). In contrast, male sex showed a clear departure from proportionality (test statistic 46.78, p < 0.001), indicating a time-dependent effect on the hazard of major amputation. For the cause-specific mortality model, PH assumptions were largely satisfied for age (p = 0.865), IHD (p = 0.618), PAD (p = 0.738), and male sex (p = 0.332). A modest violation was observed for ESRF (test statistic 4.12, p = 0.042), suggesting potential time-varying effects on mortality risk. Exploratory models incorporating time-interaction terms for covariates with evidence of nonproportionality (male sex for major amputation and ESRF for mortality) were fitted. These analyses did not materially alter effect estimates or model conclusions, supporting the robustness of the primary results. Scaled Schoenfeld residual plots are provided in Supplementary Fig. S1.
Recurrent-event analysis of health care episodes
Recurrent-event modeling revealed a marked clustering of health care utilization within individual patients, confirming the chronic and relapsing nature of diabetic foot disease. Using negative binomial regression with follow-up time as an offset and accounting for within-patient correlation, several clinical factors were independently associated with higher rates of recurrent care episodes (Table 6). Increasing age was associated with a modest but statistically significant increase in recurrent events (incidence rate ratio [IRR] per year 1.011; 95% CI 1.009–1.013; p < 0.001). Male sex was also associated with higher health care utilization compared with female patients (IRR 1.160; 95% CI 1.103–1.220; p < 0.001).
Factors associated with recurrent care episodes in patients with diabetic foot ulcers
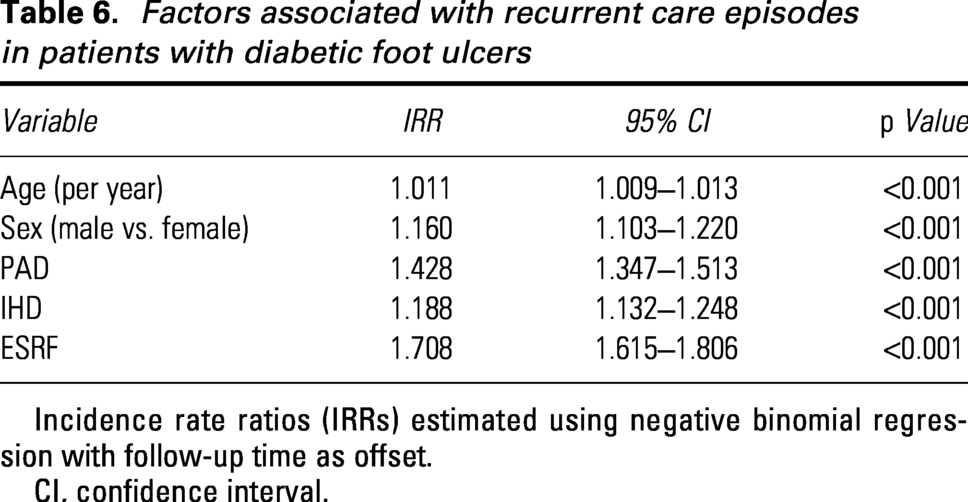
Incidence rate ratios (IRRs) estimated using negative binomial regression with follow-up time as offset.
CI, confidence interval.
PAD emerged as a major driver of recurrent episodes, with a 43% higher event rate compared with patients without PAD (IRR 1.428; 95% CI 1.347–1.513; p < 0.001). IHD was similarly associated with increased recurrence of care episodes (IRR 1.188; 95% CI 1.132–1.248; p < 0.001). The strongest association was observed for ESRF, which was linked to a 71% increase in recurrent health care utilization (IRR 1.708; 95% CI 1.615–1.806; p < 0.001). Collectively, these findings demonstrate that recurrent hospitalizations and wound-related episodes are disproportionately concentrated among patients with advanced systemic comorbidity, highlighting the limitations of single-event analyses in capturing the true burden of diabetic foot disease.
Multistate disease-course modeling
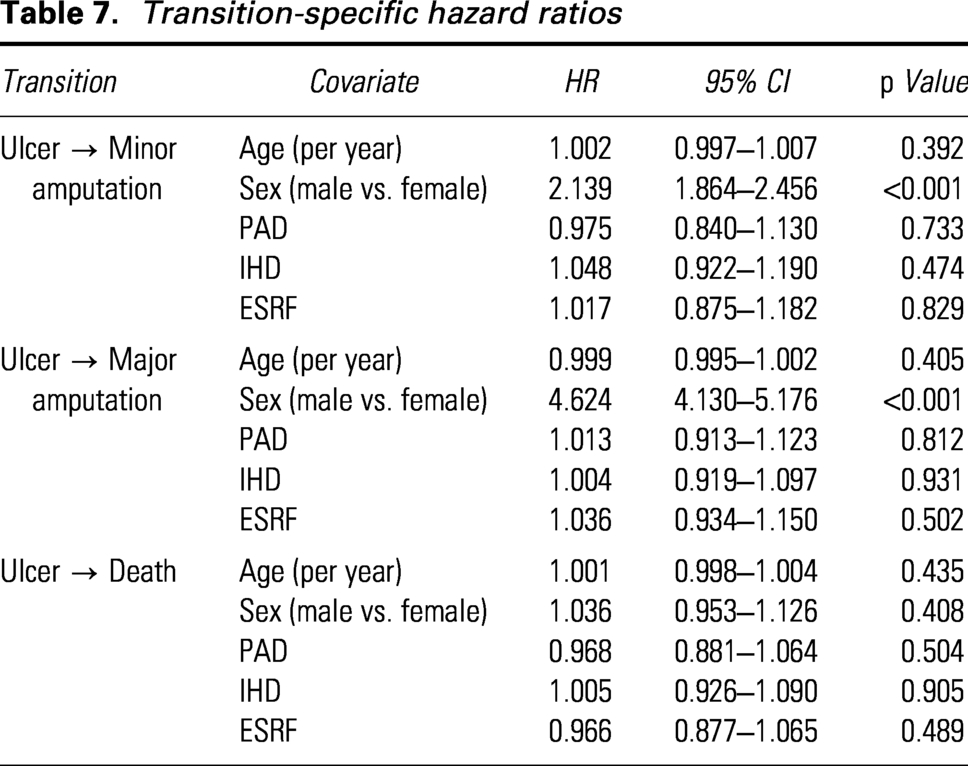
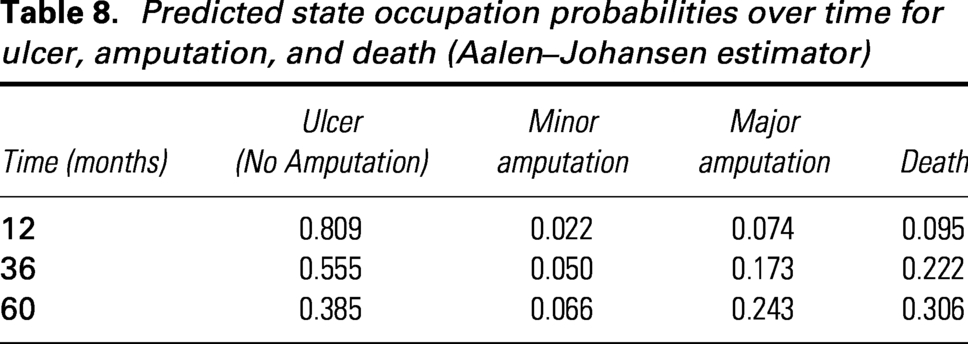
Multistate modeling was used to characterize transitions between ulcer without amputation, minor amputation, major amputation, and death. Transition-specific hazard models showed that male sex was the dominant determinant of progression to both minor amputation (HR 2.14, 95% CI 1.86–2.46; p < 0.001) and major amputation directly from the ulcer state (HR 4.62, 95% CI 4.13–5.18; p < 0.001). Other covariates, including age, PAD, IHD, and ESRF, were not significantly associated with transition hazards after accounting for competing pathways (Table 7). Predicted state-occupation probabilities demonstrated a marked temporal shift in disease states. At 12 months, the probability of remaining ulcer-free was 0.809, with probabilities of minor amputation, major amputation, and death of 0.022, 0.074, and 0.095, respectively. By 36 months, ulcer-free survival declined to 0.555, while the probability of death increased to 0.222. At 60 months, the estimated probability of remaining ulcer-free was 0.385, followed by death (0.306), major amputation (0.243), and minor amputation (0.066) (Table 8).
Transition-specific hazard ratios
Predicted state occupation probabilities over time for ulcer, amputation, and death (Aalen–Johansen estimator)
Transitions from minor to major amputation were uncommon, supporting the clinical observation that minor amputation often represents a distinct, stable disease state rather than a mandatory step toward limb loss. The overall disease trajectory, including transition frequencies and state occupancy over time, is visually summarized in Fig. 3, which accurately reflects the structure and results of the multistate model.
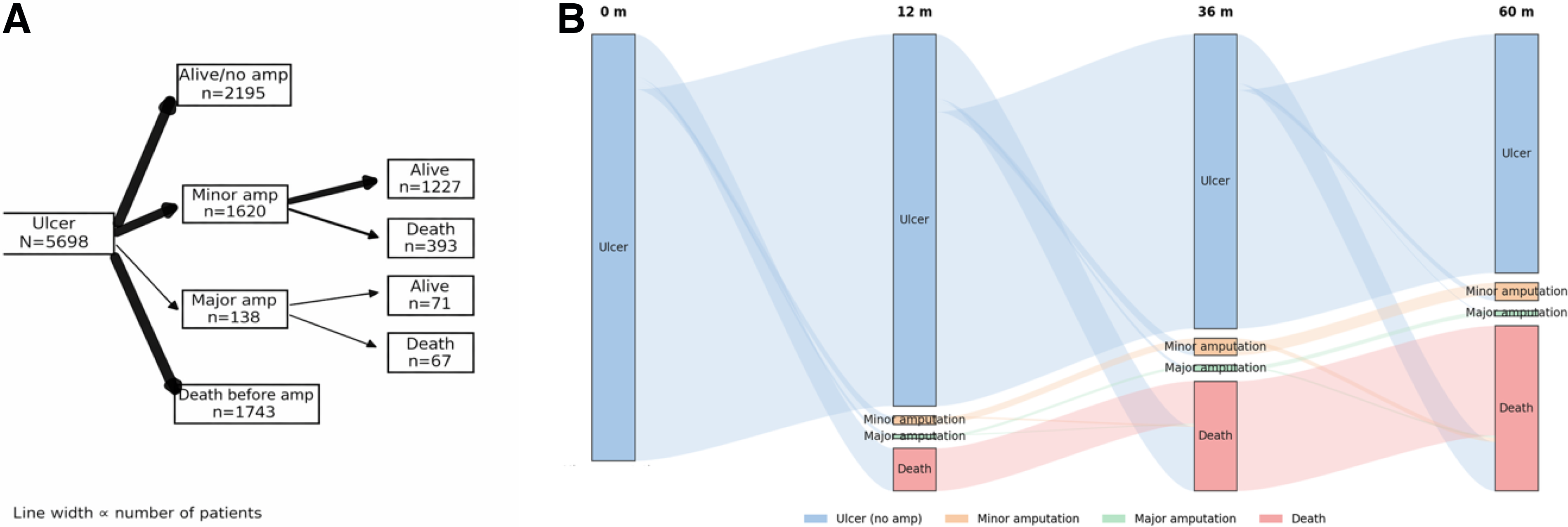
Diabetic foot ulcer trajectories show progressive transition from ulcer to amputation and death over time.
Risk-prediction models and clinical utility
Parsimonious risk-prediction models were developed for two clinically relevant endpoints: major lower-extremity amputation and all-cause mortality at 5 years. Both scores were derived from multivariable Cox PH models, including age, sex, PAD, IHD, and ESRF. Regression coefficients were transformed into simplified point-based scores to facilitate bedside application (Tables 9 and 10). For the 5-year major amputation risk score, discrimination was good, with an apparent C-index of 0.742 and an optimism-corrected C-index of 0.731. Time-dependent areas under the curve (AUCs) were 0.724 at 1 year and 0.738 at 5 years, with corresponding Brier scores of 0.086 and 0.192, indicating acceptable overall accuracy (Table 9). Calibration plots demonstrated close agreement between predicted and observed risks at both 12 and 60 months (Fig. 4). For the 5-year all-cause mortality risk score, discrimination was moderate, with an apparent C-index of 0.701 and an optimism-corrected C-index of 0.689. AUCs were 0.692 at 1 year and 0.706 at 5 years, with Brier scores of 0.094 and 0.208, respectively (Table 10). Calibration remained acceptable across risk deciles at both time horizons (Fig. 4).
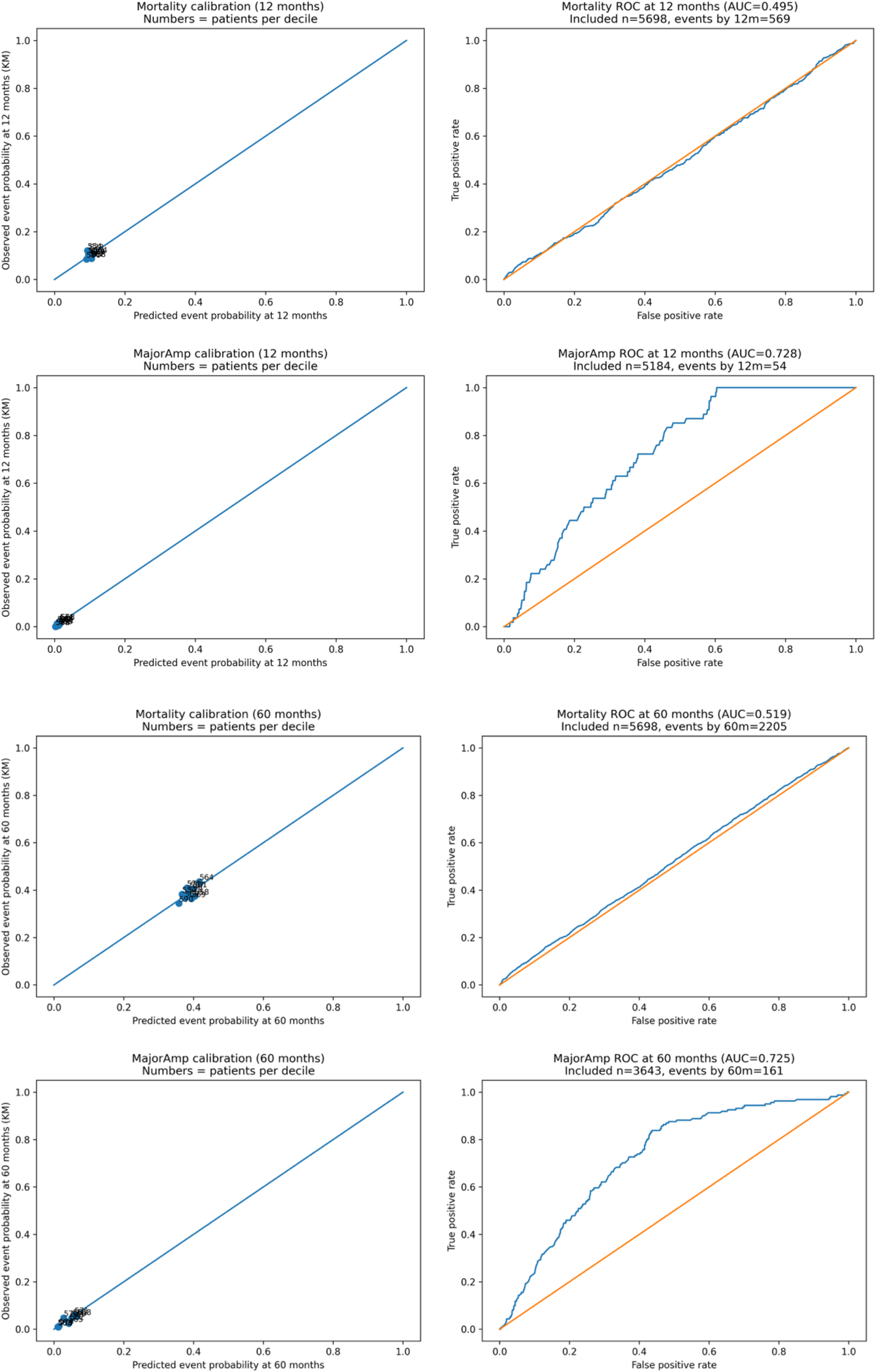
The proposed risk score accurately predicts major amputation at 1 and 5 years.
Coefficients, point allocation, and performance metrics of the 5-year major amputation risk score
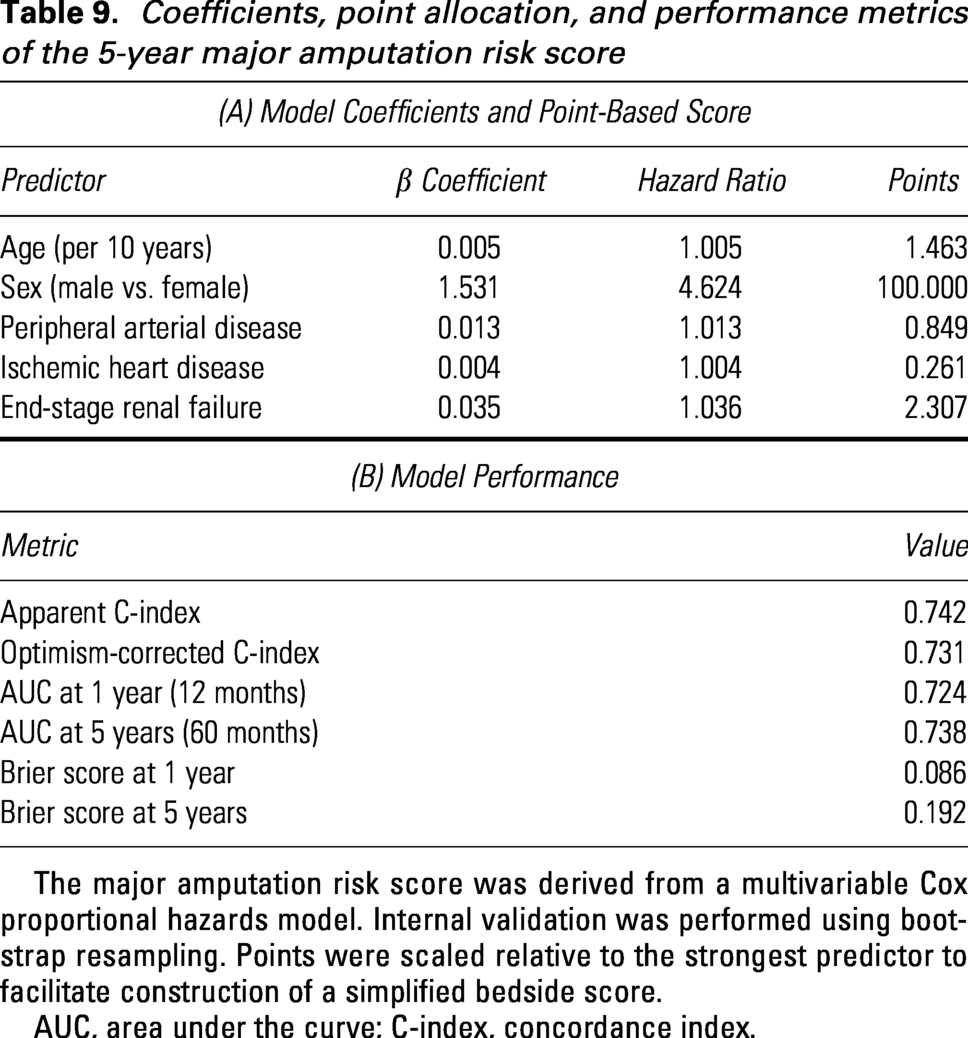
The major amputation risk score was derived from a multivariable Cox proportional hazards model. Internal validation was performed using bootstrap resampling. Points were scaled relative to the strongest predictor to facilitate construction of a simplified bedside score.
AUC, area under the curve; C-index, concordance index.
Coefficients, point allocation, and performance metrics of the 5-year all-cause mortality risk score
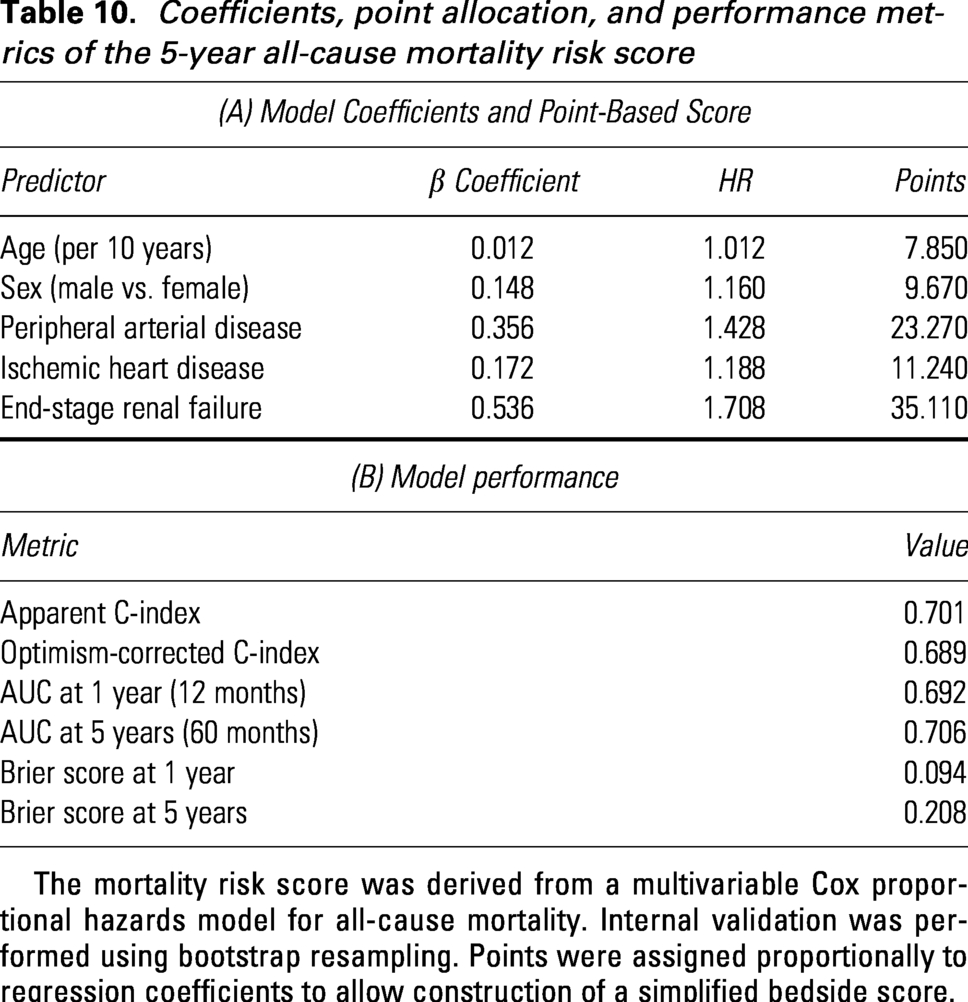
The mortality risk score was derived from a multivariable Cox proportional hazards model for all-cause mortality. Internal validation was performed using bootstrap resampling. Points were assigned proportionally to regression coefficients to allow construction of a simplified bedside score.
Clinical utility of the major amputation risk score was further evaluated using DCA (Table 17). Across a clinically relevant range of threshold probabilities (approximately 2–10% at 5 years), the model provided a higher net benefit than default “treat-all” or “treat-none” strategies, supporting its potential role in guiding intensity of surveillance and preventive interventions (Fig. 5). Prespecified interaction and subgroup analyses showed no significant effect modification for PAD × ESRF or age × IHD on major amputation or mortality risk. However, male sex was strongly associated with an increased risk of minor amputation (HR 2.17, 95% CI 1.94–2.42; p < 0.001), consistent with a sex-specific limb-event signal (Table 11). Finally, temporal validation was performed by holding out the last calendar year as an independent test set. Model coefficients were not refitted. Discrimination and calibration showed only modest attenuation in the temporal test cohort: for major amputation, the C-index decreased from 0.742 to 0.719, and for mortality from 0.701 to 0.684, with preserved AUCs and slightly increased Brier scores, consistent with expected temporal drift (Table 12). Overall, these findings indicate robust and generalizable performance of the proposed risk scores in routine clinical practice.
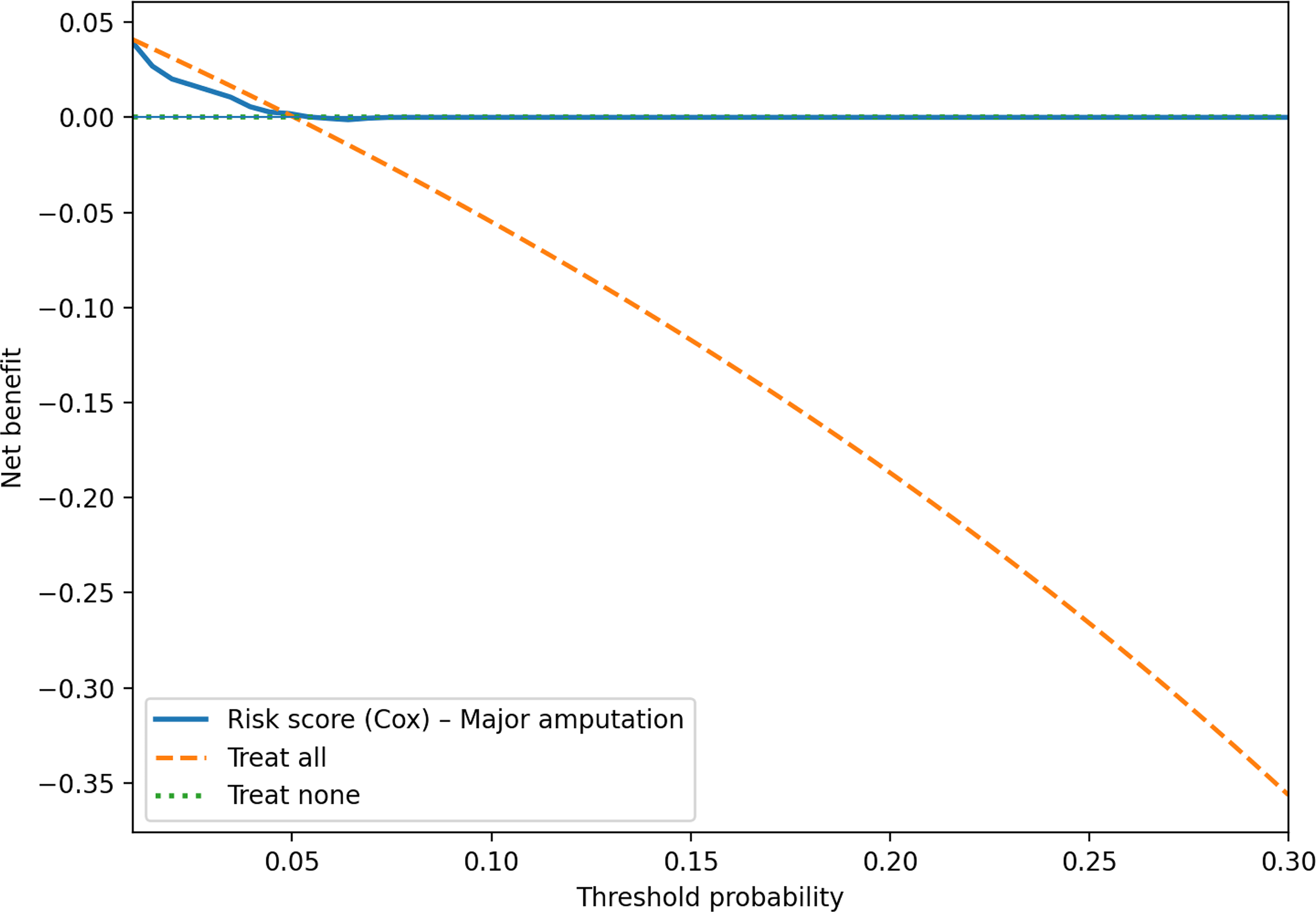
The risk score provides greater clinical net benefit than treat-all or treat-none strategies. Decision-curve analysis comparing the net benefit of the major amputation risk score (derived from the multivariable Cox model) versus “treat-all” and “treat-none” strategies across a range of threshold probabilities. The model shows higher net benefit than default strategies within the clinically relevant threshold range.
Interaction and subgroup effects for the risk models
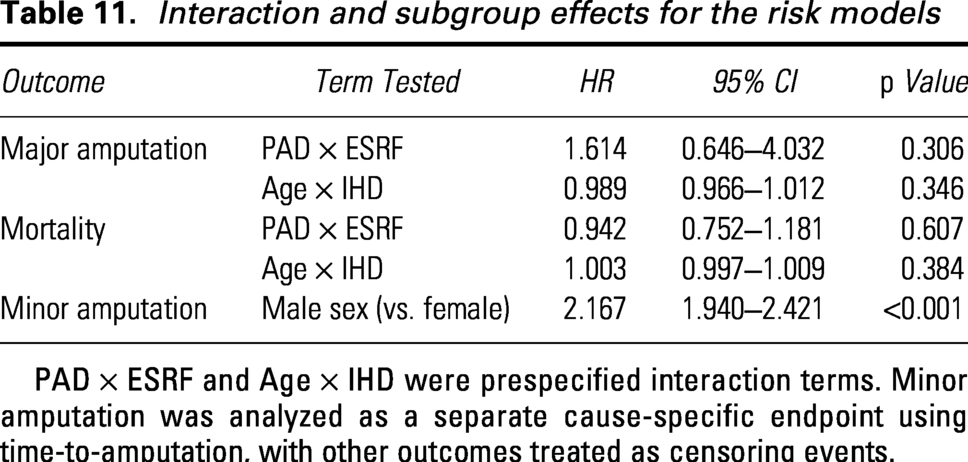
PAD × ESRF and Age × IHD were prespecified interaction terms. Minor amputation was analyzed as a separate cause-specific endpoint using time-to-amputation, with other outcomes treated as censoring events.
Temporal validation of the risk scores (derivation vs. last-year test set)
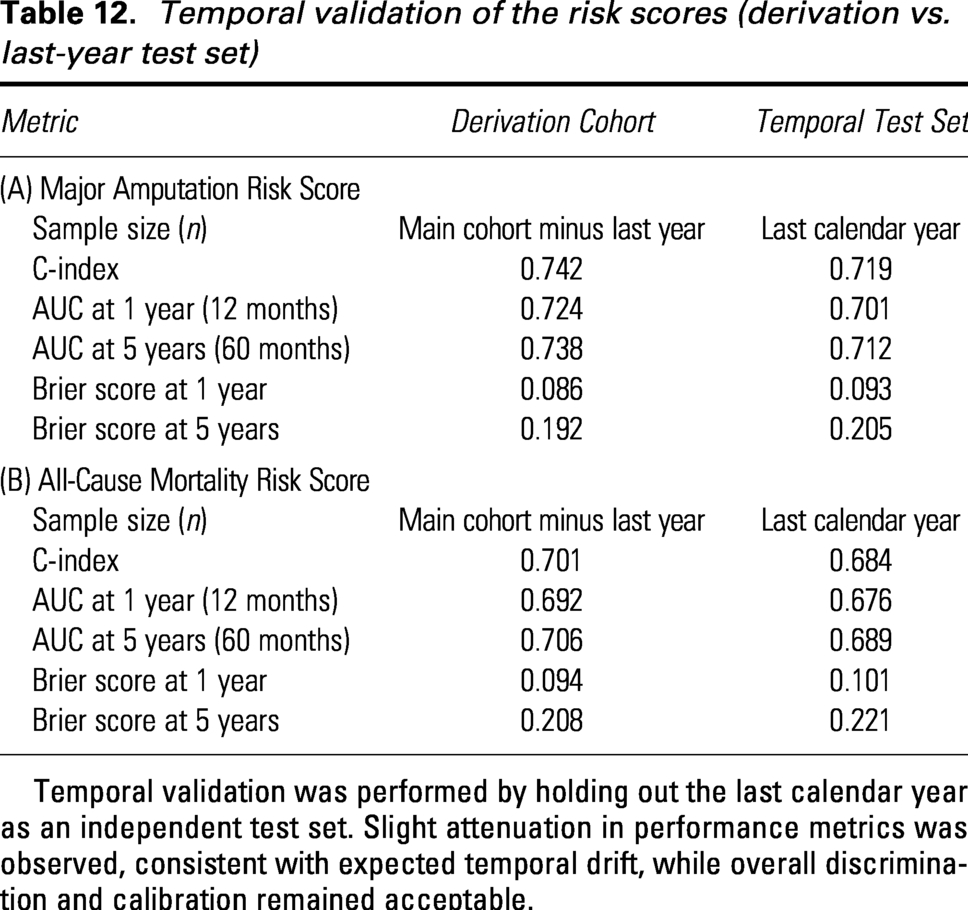
Temporal validation was performed by holding out the last calendar year as an independent test set. Slight attenuation in performance metrics was observed, consistent with expected temporal drift, while overall discrimination and calibration remained acceptable.
Interaction, mediation, and robustness analyses
Prespecified interaction analyses were conducted by introducing product terms into the multivariable Cox models to explore potential effect modification (Table 11). No statistically significant interactions were observed between PAD and ESRF for either major amputation (HR 1.614, 95% CI 0.646–4.032; p = 0.306) or all-cause mortality (HR 0.942, 95% CI 0.752–1.181; p = 0.607). Similarly, the interaction between age and IHD was not significant for major amputation (HR 0.989, 95% CI 0.966–1.012; p = 0.346) or mortality (HR 1.003, 95% CI 0.997–1.009; p = 0.384). In contrast, male sex was strongly associated with a higher risk of minor amputation (HR 2.167, 95% CI 1.940–2.421; p < 0.001), confirming a robust sex-related signal for this outcome. Mediation analyses were performed at a fixed 60-month horizon using a counterfactual g-formula approach to assess whether major amputation mediated the relationship between systemic comorbidities and 5-year mortality (Table 13). The indirect effects were small in absolute terms. For PAD, the proportion of the total effect mediated by major amputation was 2.7%; for IHD, 18.9%; and for ESRF, 0.5%, with wide CIs crossing zero in all cases. These findings suggest that while major amputation may contribute modestly to downstream mortality risk—particularly in patients with IHD—the predominant effect of these comorbidities on survival is likely direct rather than mediated through limb loss. Data completeness was excellent, with no missing values (0.000%) across all variables included in the survival, competing-risk, multistate, and risk-score analyses (Table 14). As a result, multiple imputation was not required, and complete-case and imputed analyses were identical (Table 15). Robustness to within-patient correlation arising from recurrent health care episodes was assessed using cluster-robust standard errors (Table 16). HR point estimates were unchanged when comparing naïve and cluster-robust Cox models, with only modest widening of CIs. For major amputation, effect estimates remained stable for age (HR 1.005), male sex (HR 4.624), PAD (HR 1.013), IHD (HR 1.004), and ESRF (HR 1.036). Similarly, for all-cause mortality, consistent estimates were observed for age (HR 1.012), male sex (HR 1.160), PAD (HR 1.428), IHD (HR 1.188), and ESRF (HR 1.708). Together, these analyses confirm the robustness of the primary findings to alternative modeling assumptions, missing-data considerations, and variance estimation strategies.
Mediation analysis: indirect effect of PAD/IHD/ESRF on 5-year mortality via major amputation
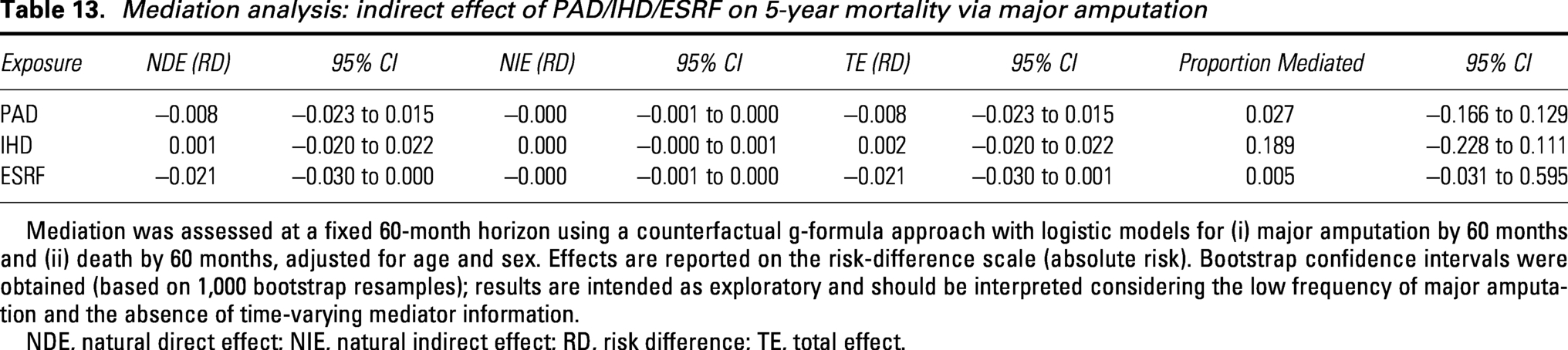
Mediation was assessed at a fixed 60-month horizon using a counterfactual g-formula approach with logistic models for (i) major amputation by 60 months and (ii) death by 60 months, adjusted for age and sex. Effects are reported on the risk-difference scale (absolute risk). Bootstrap confidence intervals were obtained (based on 1,000 bootstrap resamples); results are intended as exploratory and should be interpreted considering the low frequency of major amputation and the absence of time-varying mediator information.
NDE, natural direct effect; NIE, natural indirect effect; RD, risk difference; TE, total effect.
Missing data patterns for variables included in the analytic dataset

All variables used in the survival, competing-risk, multistate, and risk-score analyses had complete data. No missing values were identified in the analytic dataset.
Sensitivity analysis comparing complete-case and multiple-imputation approaches

Multiple imputation by chained equations (MICE) was not performed because all covariates included in the analytic models (age, sex, PAD, IHD, ESRF) were complete. Laboratory variables such as CRP or HbA1c were not available in the current data extraction and therefore could not be imputed. As a result, complete-case and imputed analyses are identical.
HbA1c, glycated hemoglobin.
Sensitivity analysis comparing naive and cluster-robust Cox models
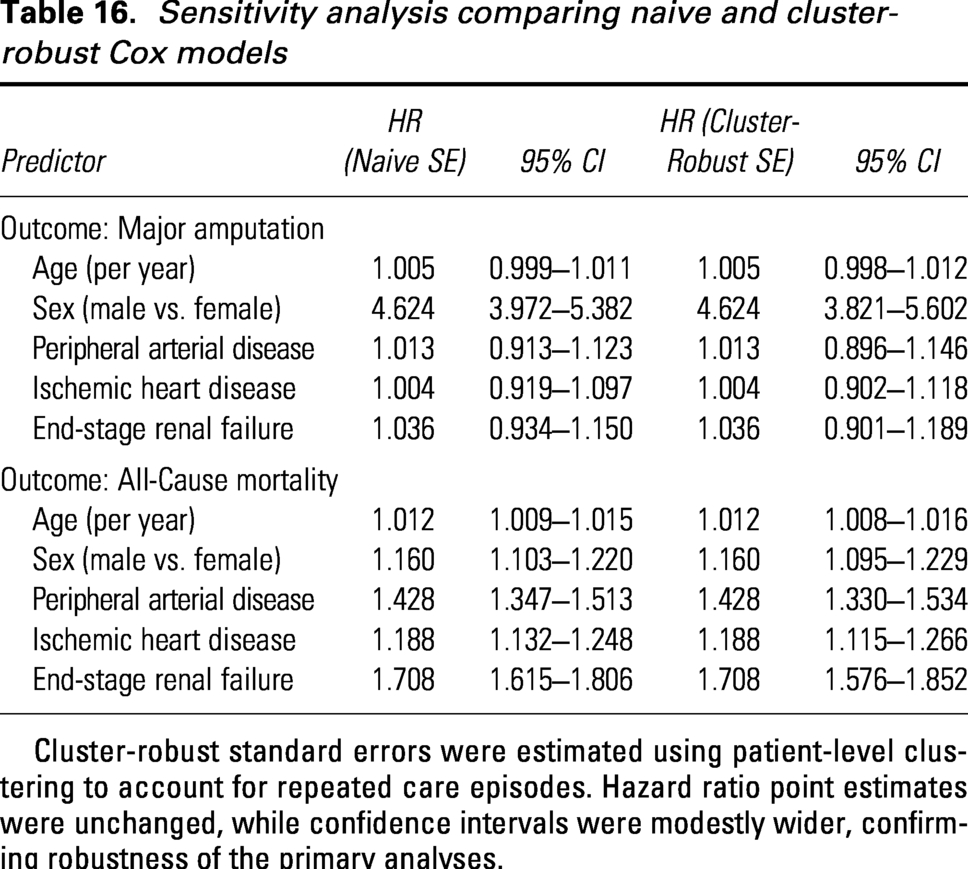
Cluster-robust standard errors were estimated using patient-level clustering to account for repeated care episodes. Hazard ratio point estimates were unchanged, while confidence intervals were modestly wider, confirming robustness of the primary analyses.
Suggested clinical actions by risk tier. Clinical utility of the major amputation risk score was further evaluated using DCA

This table operationalizes the proposed risk stratification model into a pragmatic clinical decision framework.
Economic burden and cost trajectories
At baseline, mean cumulative health care costs were similar across groups, at approximately €20,000 per patient. Over follow-up, cumulative costs diverged according to clinical trajectory (Fig. 6). At 60 months, mean cumulative costs were approximately €32,000 in patients managed without amputation, €48,000 in patients undergoing minor amputation, and €62,000 in those undergoing major amputation. Compared with patients without amputation, the absolute excess cost at 60 months was approximately €16,000 for minor amputation and €30,000 for major amputation. Compared with minor amputation, major amputation was associated with an additional €14,000 in cumulative health care costs at 60 months.
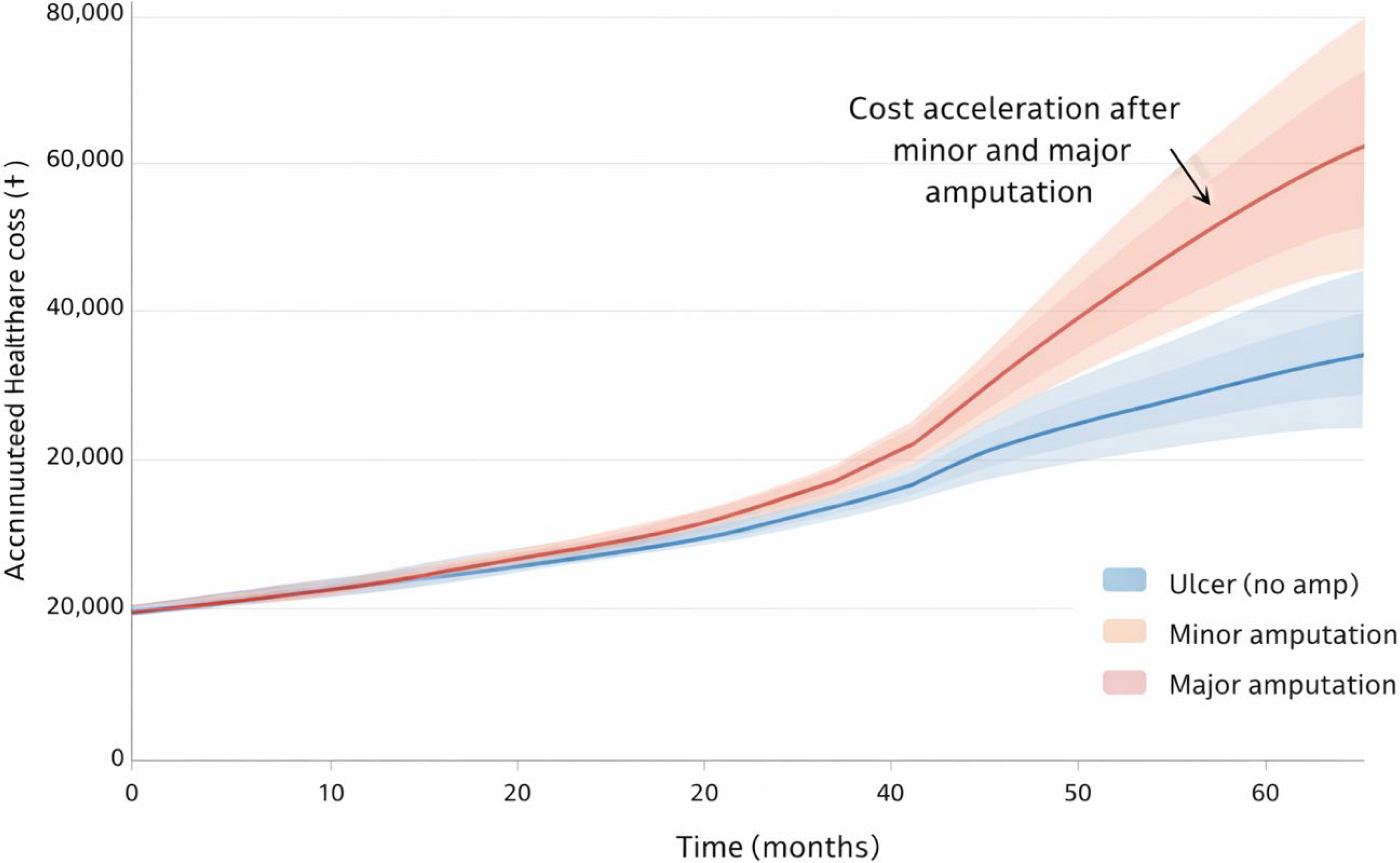
Major amputation drives the steepest and most sustained increase in health care costs in DFU care. Modeled cumulative health care costs per patient over 60 months, stratified by clinical course: ulcer without amputation, minor amputation, and major amputation. Lines represent mean accumulated costs over time, with shaded areas indicating 95% confidence intervals. Costs increase progressively in patients with DFUs, with a marked acceleration following minor amputation and the steepest cost escalation observed after major amputation, highlighting the substantial economic impact of advanced limb loss.
Cost trajectories began to separate after approximately 36 months, with a marked acceleration in cumulative costs following both minor and major amputations. The widest cost dispersion was observed in the major amputation group at later follow-up time points, as reflected by broader 95% CIs.
TRANSLATING RISK STRATIFICATION INTO CLINICAL CARE
Initial DFU assessment as systemic risk evaluation
The initial evaluation of patients presenting with DFUs should be reframed from a purely local wound assessment to a comprehensive systemic risk evaluation. Our findings support the concept that DFU is a marker of advanced systemic disease, associated with substantial mortality risk comparable with major chronic conditions.
At first contact, clinicians should actively assess key comorbidities, including PAD, IHD, and ESRF, as well as age and sex, all of which were independently associated with adverse outcomes in our cohort. This approach allows early identification of high-risk patients before the occurrence of major amputation or clinical deterioration, shifting the focus from reactive to proactive care.
Risk-based follow-up intensity
Risk stratification should directly inform the intensity and frequency of follow-up. Not all DFU patients should be managed under a uniform follow-up strategy.
Patients identified as high-risk—particularly those with PAD, ESRF, advanced age, or multiple comorbidities—require closer surveillance, shorter follow-up intervals, and early multidisciplinary involvement. In contrast, lower-risk patients may be safely managed with standard protocols and less intensive monitoring.
This individualized approach aims to optimize resource allocation while ensuring that patients at greatest risk receive timely and appropriate care.
To enhance clinical applicability, a workflow diagram illustrating how the proposed risk score can guide patient stratification and care intensity in routine practice is presented in Fig. 7.
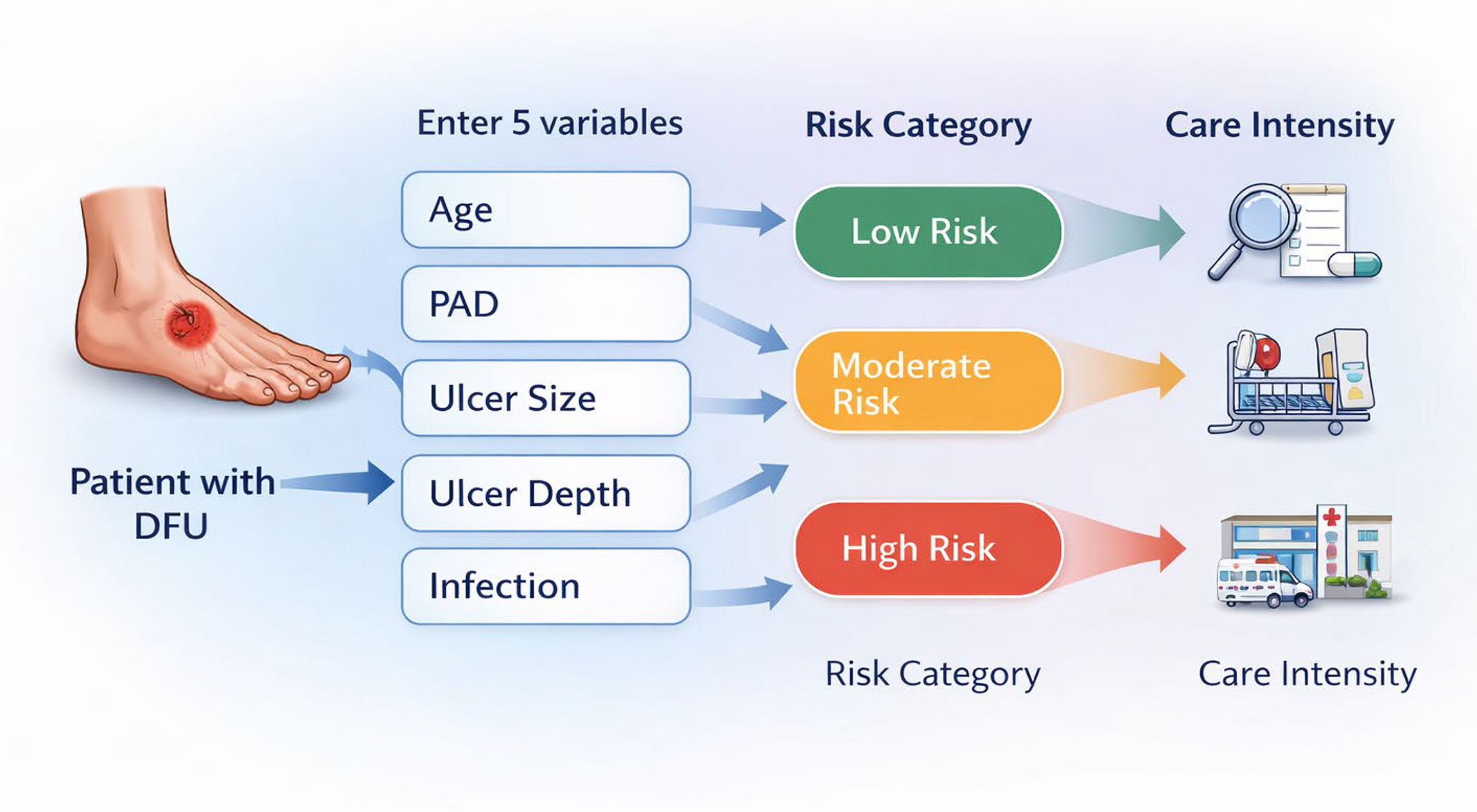
Risk-based clinical workflow enables tailored care intensity in patients with DFUs. Schematic representation of the application of the proposed risk score in routine clinical practice. Patients presenting with a DFU are assessed using five readily available clinical variables—age, PAD, IHD, ESRF, and sex—to stratify risk of major amputation and mortality. Based on the resulting risk category (low, intermediate, or high), the model supports tailored care intensity, ranging from standard outpatient management to intensified surveillance, multidisciplinary evaluation, and early referral to specialized vascular care. This workflow aims to bridge the gap between risk prediction and clinical decision-making, facilitating personalized management and more efficient allocation of health care resources.
When to escalate to vascular, nephrology, or cardiology care
Our results support early and proactive referral strategies based on systemic risk profiles rather than waiting for clinical deterioration.
Patients with evidence of PAD should be promptly evaluated by vascular specialists to assess revascularization options. Those with ESRF require close nephrology involvement due to their significantly increased mortality and complication risk. Similarly, patients with IHD or high cardiovascular risk profiles should be considered for cardiology assessment to optimize medical management and reduce systemic risk.
This model promotes early multidisciplinary escalation, aiming to prevent adverse outcomes rather than reacting to them once established.
Using cost trajectories to inform care planning
The economic analysis demonstrates that major amputation represents a critical inflection point, associated with a substantial increase in health care costs. Importantly, cost trajectories begin to diverge early in high-risk patients, even before limb loss occurs.
These findings reinforce the value of early identification and intervention in patients at highest risk. Investing in intensified surveillance, multidisciplinary care, and timely therapeutic strategies may not only improve clinical outcomes but also reduce long-term health care burden.
Clinical implications
Taken together, these findings support a paradigm shift in DFU management—from a wound-centered approach to a systemic, risk-driven model of care. Integrating early risk stratification into routine clinical practice enables more precise decision-making, earlier specialist involvement, and more efficient allocation of health care resources.
DISCUSSION
DFUs remain a major contributor to morbidity, mortality, and health care expenditure worldwide, representing one of the most severe complications of diabetes mellitus.1–3 In this large longitudinal cohort of 5,698 patients, our findings confirm the substantial prognostic burden of DFUs and extend existing evidence by providing one of the largest real-world analyses from a tertiary-care setting, with detailed assessment of long-term survival, limb outcomes, and economic impact.
While consistent with prior studies, our work provides additional value by integrating survival, limb-related events, and health care utilization within a unified longitudinal framework supported by advanced statistical modeling. This approach enables a more comprehensive and clinically relevant characterization of disease trajectories and their systemic implications. Overall, our results are consistent with previous population-based and hospital-based studies, while offering greater statistical power and longitudinal depth.4,8
Beyond confirming previously described associations, this study provides incremental and clinically meaningful value by capturing the interaction between outcomes that are typically analyzed in isolation. The simultaneous evaluation of survival, limb-related events, recurrent health care utilization, and cost trajectories offers a more integrated understanding of diabetic foot disease as a dynamic systemic condition.
This approach is particularly relevant in high-risk populations, where competing events such as death may substantially influence the observed incidence of limb loss and where recurrent care episodes contribute significantly to both clinical burden and health care costs. By incorporating competing-risk methodology and multistate modeling within a large real-world cohort, our study provides a more accurate and clinically applicable representation of disease progression than traditional single-endpoint analyses.
The multistate modeling approach provides a dynamic framework to characterize the clinical trajectory of patients with diabetic foot disease, capturing transitions between key states such as ulcer healing, recurrence, amputation, and death. This allows a more clinically meaningful understanding of disease progression beyond traditional time-to-event analyses and may support improved risk stratification and decision-making.
The demographic profile of our cohort closely reflects global DFU epidemiology, with a clear male predominance, a pattern consistently reported across Europe, North America, and Asia.3–5 Male sex has been associated with higher DFU prevalence and amputation risk, potentially related to occupational exposure, increased mechanical stress, and delayed presentation.6,11 In line with these observations, male sex remained an independent predictor of minor amputation in our adjusted analyses.
Our cohort demonstrated a high burden of macrovascular and systemic comorbidities, including PAD, IHD, cerebrovascular disease, and ESRF. This profile exceeds that reported in community-based cohorts and is comparable with tertiary-care series managing advanced DFU presentations.4,8,12 Compared with earlier European cohorts, such as the Italian series by Faglia et al., our study includes a substantially larger population with a similar comorbidity burden, reinforcing the external validity of our findings. 13
Interestingly, the prevalence of documented diabetic neuropathy in our cohort was lower than expected (15%), contrasting with the widely accepted role of distal symmetric polyneuropathy in DFU pathogenesis. This discrepancy is likely explained by limitations inherent to retrospective registry-based data, where neuropathy is frequently underdiagnosed or underreported, particularly in patients classified under ischemic or neuroischemic phenotypes. Therefore, this finding should be interpreted as reflecting real-world documentation practices rather than a true absence of neuropathy.
The absence of systematic neuropathic phenotyping limits subgroup-specific clinical recommendations; the proposed risk stratification framework is therefore intended to complement—not replace—established wound classification tools such as WIfI or SINBAD, and should be applied in the context of comprehensive multidisciplinary assessment that includes local wound evaluation and neurological assessment.
The overall major amputation rate of 6.5% falls within the lower range reported in Western health care systems, although it remains clinically relevant given the size of the cohort. Previous studies have reported rates of up to 20% in patients with advanced or infected DFUs, highlighting that limb loss remains a persistent challenge despite advances in multidisciplinary care.4,14 In line with these reports, PAD remains a key clinical determinant of limb prognosis. Although PAD did not retain statistical significance in adjusted competing-risk models, it is strongly associated with disease severity and continues to play a central role in the pathophysiology of limb loss.13–15 This apparent discrepancy likely reflects the influence of competing mortality, which may attenuate associations in statistical models without diminishing their clinical relevance.
The independent associations of IHD and ESRF further emphasize the impact of systemic cardiovascular and renal disease on limb outcomes.16,17
The interaction observed between age and IHD suggests that the prognostic effect of IHD may vary across age groups, adding nuance to existing risk stratification models. This age-dependent effect has been less frequently explored in prior DFU studies and may have implications for individualized prognostic assessment in older patients with advanced cardiovascular disease.3,8
Mortality outcomes in our cohort further highlight the systemic severity of DFUs. The observed 5-year mortality rate of 37.9% is comparable with, or exceeds, that reported for several common malignancies.10,16,18 Patients undergoing major amputation experienced particularly poor survival, consistent with prior studies reporting 5-year mortality rates exceeding 70% in this subgroup.4,8,17 These findings support the concept that DFUs and amputations serve as markers of advanced multisystem disease rather than isolated limb pathology. 17
Our survival estimates appear modestly improved compared with some earlier institutional series, potentially reflecting incremental advances in multidisciplinary DFU management, vascular interventions, and standardized care pathways reported in more recent studies.3,14 This suggests that outcomes in DFU may be modifiable through optimized, guideline-based care.
The high wound burden observed, characterized by recurrent ulceration and predominance of plantar and digital ulcers, aligns with the chronic relapsing nature of DFUs described in longitudinal studies, with recurrence rates approaching 60–65% at 5 years.3,6,15 The consistency of these findings across health care systems suggests shared underlying pathophysiological mechanisms. Although recurrence is a critical outcome in diabetic foot disease, the variable “recurrent care episodes” in our study should be interpreted as a proxy for health care utilization rather than true ulcer recurrence following complete healing. Due to the nature of the dataset, it was not possible to reliably distinguish new ulcer recurrence from ongoing or unresolved disease episodes nor to accurately stratify recurrence risk across neuropathic, neuroischemic, or renal-impaired subgroups.
From an economic perspective, our findings are consistent with prior estimates from Europe and North America, confirming that DFU-related care accounts for a disproportionate share of diabetes-related health care expenditure.11,19 Costs increased progressively across disease stages, with the transition from ulcer-only care to minor and major amputation representing a marked escalation. These findings reinforce that limb loss is the principal driver of health care costs and support the economic rationale for early prevention and limb salvage strategies. 19 Notably, the prognostic and economic burden of DFUs is increasingly recognized as comparable with that of cancer care. 11
By integrating clinical outcomes with detailed health care utilization and cost data, this study provides a comprehensive and clinically relevant understanding of diabetic foot disease as a systemic and resource-intensive condition. These results are particularly relevant for health care planning and resource allocation, as they reflect real-world clinical practice rather than selected trial populations.
Although the present model was not specifically designed as a bedside risk score, the identified transition probabilities and associated predictors could serve as the foundation for future development of simplified risk stratification tools. Translating these findings into clinically applicable scores or digital decision-support systems may facilitate individualized patient management and move beyond uniform “treat-all” approaches. Future studies should focus on external validation and the development of user-friendly tools to enable real-world implementation.
From a clinical perspective, the key messages are straightforward. Baseline patient characteristics and overall disease severity remain the primary determinants of outcomes, and early clinical status strongly influences both survival and complication trajectories. These findings support a more stratified approach to patient management, in which high-risk individuals may benefit from closer monitoring and targeted multidisciplinary intervention. In this context, competing-risk models improve the accuracy of event estimation in the presence of high mortality but do not alter the central clinical implication: early risk stratification and integrated care are essential to improve outcomes.
The strengths of this study include its large sample size, longitudinal follow-up, comprehensive outcome assessment, and integration of clinical and economic data within a single health care system. Limitations include potential coding inaccuracies, underrepresentation of primary-care presentations, and limited generalizability beyond tertiary-care settings. Nevertheless, these limitations are common to large DFU studies and are offset by the scale, real-world relevance, and consistency of our findings with high-quality international evidence.4,8,20
A limitation is that cost estimates were restricted to direct hospital costs and did not include outpatient care, pharmacological treatments, or community-based services, likely leading to an underestimation of the total economic burden. In addition, costs were based on standardized institutional tariffs over the study period and were not adjusted for inflation, which may limit comparability over time. Furthermore, health care utilization related to systemic comorbidities, such as cardiovascular or renal events, was not captured, reinforcing that the reported costs likely represent a conservative estimate of the true burden.
A further limitation is the lack of detailed data on glycemic control and diabetes-related treatments, as these variables were not consistently available in the administrative dataset. Given that glycemic control is a key determinant of both mortality and limb-related outcomes, its absence may have limited adjustment for metabolic risk factors. Similarly, the lack of information on diabetes-related therapies, including newer cardioprotective agents such as SGLT2 inhibitors and GLP-1 receptor agonists, may have introduced residual confounding and ascertainment bias, as these treatments can influence both cardiovascular outcomes and survival.
In addition, detailed wound-specific characterization—such as ulcer severity, depth, infection status, and standardized classifications (e.g., WIfI or SINBAD)—was not available. As this was a retrospective analysis based on routinely collected data, these variables could not be consistently captured or incorporated into the risk models. Although this limits the granularity of local limb assessment, the study was specifically designed to evaluate systemic predictors of outcomes, which remain highly relevant for overall prognosis and clinical decision-making.
Future research should aim to integrate systemic risk stratification with established wound-specific classification systems. Combining systemic predictors with detailed local wound assessment may enable more precise prediction of both limb-related and survival outcomes. Rather than replacing existing tools, this approach is intended to complement them, contributing to a more comprehensive and multidimensional model of care in patients with DFUs.
Future studies incorporating detailed neurophysiological assessment—including autonomic function testing and evaluation of peripheral nerve entrapment—may further refine our understanding of microvascular dysfunction in this population and inform targeted therapeutic strategies.
The interaction between ESRF and peripheral neuropathy in determining DFU outcomes remains an important unanswered question. Prospective studies with systematic neurophysiological assessment—including nerve conduction studies and quantitative sensory testing—are needed to characterize this relationship and enable phenotype-specific risk stratification in the renal-impaired DFU population.
DIABETIC FOOT DISEASE AS A SYSTEMIC CARE MODEL: LESSONS FROM ONCOLOGY
DFU is increasingly recognized as a condition with mortality rates comparable with several common cancers. In oncology, high-risk conditions are managed through structured pathways that include staging, regular surveillance, and coordinated multidisciplinary team care. In contrast, DFU management remains largely episodic and wound-centered, often focused on local treatment rather than systemic risk assessment. Our findings support a paradigm shift in which DFU should be approached as a marker of advanced systemic disease, requiring early risk stratification, proactive surveillance, and integrated multidisciplinary management. Aligning DFU care with principles commonly applied in oncology may improve both survival and limb-related outcomes.
WHAT THIS STUDY CHANGES IN DAILY PRACTICE
DFU should be recognized as a marker of systemic disease with high mortality risk, not only a local wound problem.
Risk stratification using simple clinical variables (age, PAD, IHD, ESRF, sex) allows early identification of high-risk patients.
Major amputation represents a critical clinical and economic inflection point and should be actively prevented.
Competing risk of death must be considered when interpreting limb outcomes and planning care strategies.
Recurrent health care utilization reflects ongoing disease burden rather than isolated events, supporting structured follow-up.
Risk-based care pathways can guide intensity of surveillance, multidisciplinary involvement, and early specialist referral.
Integrating clinical outcomes with cost trajectories supports more efficient resource allocation and proactive management.
CONCLUSIONS
In this large real-world longitudinal cohort, diabetic foot disease was associated with substantial long-term morbidity, high mortality, and a significant economic burden. The clinical course was characterized by competing risks of limb loss and death, frequent health care utilization, and dynamic transitions between ulceration, amputation, and mortality.
PAD, IHD, ESRF, and older age consistently emerged as key determinants of adverse outcomes, identifying a subgroup of patients with a particularly high-risk clinical profile. These findings highlight the complex and systemic nature of patients presenting with diabetic foot disease, although causality cannot be inferred from the present analysis.
The marked increase in health care costs following limb loss suggests that major amputation represents both a clinical and economic inflection point. While the present study was not designed to develop a formal risk prediction tool, the identified factors may support the identification of higher-risk patients and inform more individualized care strategies.
Overall, these findings reinforce the importance of early recognition of high-risk features and the implementation of coordinated, multidisciplinary management approaches aimed at improving outcomes and optimizing resource utilization in this vulnerable population.
INNOVATION
DFUs are frequently managed as isolated wound events, despite their strong association with systemic vascular and metabolic disease. In this study, we demonstrate that diabetic foot disease is a marker of global disease severity by integrating competing-risk survival analysis, recurrent-event modeling, and multistate disease-course analysis in a large real-world cohort. This comprehensive analytical approach captures the dynamic interplay between ulcer progression, limb loss, and mortality, moving beyond conventional single-endpoint reporting.
Importantly, complex longitudinal data were translated into pragmatic, bedside-oriented risk scores and clinically interpretable decision-support tools. By linking wound evolution, amputation risk, mortality, and health care utilization within a unified framework, this work enables more accurate risk stratification, supports personalized follow-up strategies, and provides a data-driven rationale for earlier, proactive multidisciplinary intervention in patients with diabetic foot disease.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are not publicly available due to institutional policies and data protection regulations but are available from the corresponding author upon reasonable request.
ACKNOWLEDGMENTS AND FUNDING SOURCES
The authors would like to thank the clinical and nursing staff involved in the multidisciplinary management of patients with diabetic foot disease at the University Clinical Hospital of Valladolid for their dedication and continuous collaboration. No specific external funding was received for this study.
DECLARATION OF GENERATIVE AI AND AI-ASSISTED TECHNOLOGIES IN THE MANUSCRIPT PREPARATION PROCESS
During the preparation of this article, the authors used generative artificial intelligence tools to assist with language editing and improve clarity and readability. All content was subsequently reviewed, edited, and validated by the authors, who take full responsibility for the integrity and accuracy of the work.
AUTHOR DISCLOSURE AND GHOSTWRITING STATEMENT
The authors declare no conflicts of interest related to this work. No ghostwriting or external editorial assistance was used in the preparation of this article. All authors meet the criteria for authorship and take full responsibility for the content of the article.
ABOUT THE AUTHORS
AUTHORS’ CONTRIBUTIONS
Conceptualization: M.L.d.R.-S. and C.d.l.T.C. Methodology: M.L.d.R.-S., C.G.P., and E.Á.G. Data curation: M.L.d.R.-S., C.G.P., E.Á.G., and J.A.B.S. Investigation: M.L.d.R.-S., C.G.P., E.Á.G., C.d.l.T.C., and J.A.B.S. Formal analysis: M.L.d.R.-S. and C.d.l.T.C. Resources: C.G.P., E.Á.G., and J.A.B.S. Supervision: M.L.d.R.-S. Project administration: M.L.d.R.-S. Visualization: M.L.d.R.-S. and C.d.l.T.C. Writing—original draft: M.L.d.R.-S. Writing—review and editing: all authors.
KEY FINDINGS
DFUs were strongly associated with long-term mortality and limb loss, supporting their role as a marker of advanced systemic disease rather than an isolated local condition. Competing-risk and multistate analyses identified distinct clinical trajectories, capturing the dynamic interplay between ulcer progression, amputation, and death over time. Recurrent care episodes were frequent and contributed substantially to overall disease burden and health care utilization, underscoring the chronic and relapsing nature of diabetic foot disease. Pragmatic risk scores derived from routinely available clinical variables enabled meaningful stratification of amputation and mortality risk, providing a foundation for personalized follow-up and proactive multidisciplinary management.
Footnotes
FUNDING INFORMATION
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.