
Abstract
Adults with intellectual disabilities (ID) struggle to gain access to sexual knowledge and experiences. Sexual knowledge increases opportunities for intimacy and positive sexual identities as well as decreases the risk of victimization. This review evaluated the extant literature on sexual education programs for adults with ID. Six studies met inclusion criteria. Findings suggest that sexual education programs can be effective in increasing sexual knowledge, decision-making capabilities, and interpersonal skills for adults with ID. Despite positive results, this synthesis revealed the need for further methodological rigor in this area to identify and/or develop specific instructional curriculum to meet the diverse needs and preferences of adults with ID. Researchers discuss findings and implications for practice at the secondary and postsecondary levels.
Humans are sexual beings. Many adults learn about sex through family, friends, community initiatives, online resources, and lived experiences (Bleakley, Hennessy, Fishbein, & Jordan, 2009). Sexual knowledge and awareness requires self-initiative and agency to gain access to information and connect with potential sexual partners. These opportunities for access are often not afforded or available to adults with disabilities (Blanchett & Wolfe, 2002). Adults with intellectual disabilities (ID) are routinely desexualized in society, refused opportunities for sexual education and romantic partnership, and excluded from sexual education courses (Schaafsma, Kok, Stoffelen, & Curfs, 2015; Shakespeare, 2000). The increased risk of victimization adults with ID face generates even greater concern (Byrne, 2017). During 2011–2015, persons with ID experienced the highest victimization rate of all disability types (Harrell et al., 2017). While it is impossible to ignore how intellectual and physical limitations may affect decision making and ability to engage in sexual activity, neither of these factors should deny access to knowledge (Pownall, Jahoda, & Hastings, 2012).
Previous research demonstrates individuals with disabilities are sexually curious and want to know about sex and engage in sexual experiences (Löfgren-Mårtenson, 2012). Kelly, Crowley, and Hamilton (2009) conducted a preliminary analysis into the sexual education experiences of 15 adults with disabilities (seven women and eight men). The authors conducted focus groups on the experience of participants in sexual education, how they received sexual knowledge, and their experiences and aspirations for sexual experiences. Results found that only three individuals had participated in formal sexual education courses. The majority of participants reported receiving information through observations of others, television, and magazines. This study revealed a shocking lack of sexual knowledge by participants, potentially due to their lack of training. In response to a researcher’s question on where babies come from, some of the participants responded “In hospitals” and “Tummies” (Kelly et al., 2009, p. 311). The researchers found that participants strived to fill the gaps in their knowledge through secondary sources like TV but still lacked foundational information on sex and sexual experiences.
Similarly, Löfgren-Mårtenson (2012) conducted 16 qualitative interviews with individuals with ID aged 16 to 21 years old to understand their sexual experiences, knowledge, and perceptions of sexual education. Results from this investigation found that most participants did not remember ever receiving sexual education or found the education they did have too little or too difficult to understand. Many participants described not being able to remember content of sexual education courses. Participants recommended that courses should include videos, role-playing, and books to facilitate learning rather than discussing only formats. The final theme generated from this study centered on loneliness and the need for young adults to have someone to talk to about sex and sexual experiences that they can trust. This finding suggests that someone who takes adequate time to develop mutual trust and understanding with participants should teach sexual education courses. Furthermore, results of this study indicate young adults with ID need to have recurrent sexual education courses to ensure comprehension of material and acquisition of skills as adults mature and gain more experience. Finally, the author discovered that sexual education provided to informants whether through structured curriculum or otherwise focused on heterosexual experiences, abstinence, contraception, and overall sexual avoidance. Results from this study indicate that sexual education coursework typically emphasizes restrictive lessons of “waiting” and “learning how to say no” rather than helping participants explore and craft a positive view of their own sexuality (Löfgren-Mårtenson, 2012, p. 222).
Sex education provides not only sexual awareness but may prevent adults with ID from becoming victims of sexual violence (Byrne, 2017). Recent statistics show that the rate of serious violent crimes against persons with disabilities was more than 3 times the rate for persons without disabilities (Harrell et al., 2017). Prior research also reveals that individuals with ID are the victims of violent crimes, including rape and sexual assault, at higher rates than other types of disabilities (Fisher, Baird, Currey, & Hodapp, 2016). Contributing factors include a lack of sexual education across the life span and social isolation in adulthood (Byrne, 2017). Providing appropriate sexual education may decrease these problematic variables and increase the ability of adults with ID to avoid and advocate against assault.
Given the startlingly high rates of sexual crimes committed against individuals with ID, sexual education is essential for both safety and quality of life (Rand & Harrell, 2009). Previous literature reviews evaluated sexual education across populations and research methodologies (e.g., Schaafsma et al., 2015) or compared different sexual education curricula (e.g., Blanchett & Wolfe, 2002). The present review differs in that it examined experimental and quasi-experimental research in sexual education for adults with ID. An analysis of sexual education interventions serves to identify if and/or how programs affect sexual knowledge and related skills. By concentrating on adults alone, the authors sought to identify how the research community has addressed building sexual knowledge for this population and potential considerations yielded from this literature for practice and future research. The authors asked the following research questions of the literature:
Method
The authors initially located articles through a search of electronic databases (ERIC and PsycInfo) using the following search terms and truncations: sex*, educat*, adults, and disabilit*. This search resulted in 1,070 studies. An ancestral search of relevant literature reviews followed the computerized search (Blanchett & Wolfe, 2002; Schaafsma et al., 2015). Articles met inclusion criteria if they (a) were published in a peer-reviewed journal; (b) implemented a single-subject, experimental, or quasi-experimental research design; (c) evaluated the effects of a sexual education program that explicitly included content related to sexual behavior such as sexual reproduction and sexual safety; and (d) evaluated the effects of a sexual education program through a demonstration of sexual knowledge (examples include a posttest, structured interview, etc.). If studies met inclusion criteria but contained additional dependent variables (e.g., impact of sexual education program on hygiene), the review included these studies but restricted analysis to the impact of the education program on knowledge of sexual education content. As the present study sought to examine the effects of interventions in sexual education, only experimental research with quantitative data was considered for review. Exclusion criteria included qualitative research studies (e.g., Robinson, 1984), studies that investigated the effects of sexual education on sexual offenders with disabilities (e.g., Reyes, Vollmer, & Hall, 2011), and studies that evaluated the effects of sexual abuse and reporting programs (e.g., Brown-Lavoie, Viecili, & Weiss, 2014). The authors placed no restrictions on country of research because sexual identity and intimacy represent universal concepts. This search yielded six studies from six journals (see Table 1; Casper & Glidden, 2001; Dukes & McGuire, 2009; Hayashi, Arakida, & Ohashi, 2011; Mueser, Valenti-Hein, & Yarnold, 1987; Valenti-Hein, Yarnold & Mueser, 1994; Zylla & Demetral, 1981).
Summary of Sexual Education Programs.
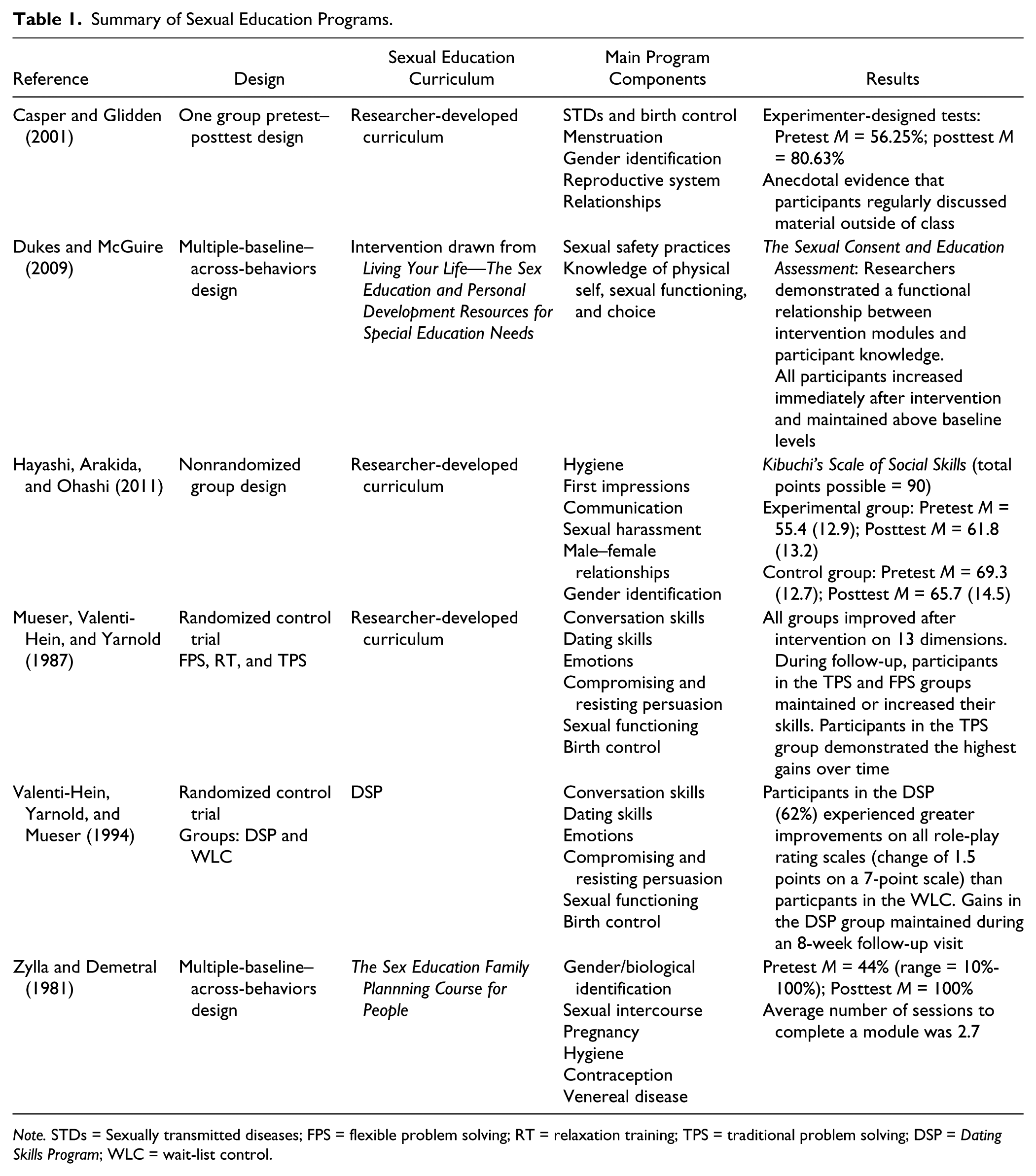
Note. STDs = Sexually transmitted diseases; FPS = flexible problem solving; RT = relaxation training; TPS = traditional problem solving; DSP = Dating Skills Program; WLC = wait-list control.
Results
Participants
Participants included 102 adults (age range = 19–45 years old) with 47 females and 55 males. Four of the six studies included specific diagnoses for participants (Casper & Glidden, 2001; Dukes & Mcguire, 2009: Hayashi et al., 2011; Zylla & Demetral, 1981). From these four studies, approximately 17 adults were diagnosed with mild ID, 18 with moderate ID, and one with severe ID. Mueser et al. (1987) and Valenti-Hein et al. (1994) included adults with mild to moderate ID but did not specify the number of individuals with these diagnoses or the ages of participants. Two of the six studies included sufficient information to confirm the presence of ID using IQ scores (Dukes & Mcguire, 2009; Zylla & Demetral, 1981).
Within Casper and Glidden (2001), 10 of the 12 participants had a diagnosis of a serious mental illness. In addition, eight of the 12 participants engaged in what the residential agency described as “sexually inappropriate incidences” (Casper & Glidden, 2001, p. 174). Five studies described the living arrangements of participants, which included 47 participants living in residential facilities and community group homes, eight participants living with their families, and seven participants living independently (Casper & Glidden, 2001; Dukes & Mcguire, 2009: Hayashi et al., 2011; Valenti-Hein et al., 1994; Zylla & Demetral, 1981). No studies included additional demographic information of participants.
Research Design
The reported research designs included two single-subject designs (Dukes & Mcguire, 2009; Zylla & Demetral, 1981) and four group designs (Casper & Glidden, 2001; Hayashi et al., 2011; Mueser et al., 1987; Valenti-Hein et al., 1994). Of the four group designs, two studies reported using randomized control trials (RCTs) each with a sample size of 26 participants (Mueser et al., 1987; Valenti-Hein et al., 1994). The remaining two group designs were quasi-experimental. Hayashi et al. (2011) conducted a nonrandomized group study (n = 17). The authors did not demonstrate equivalency between control and treatment groups prior to intervention. Casper and Glidden (2001) conducted their intervention with a single group (n= 12).
Both single-subject studies implemented a multiple-baseline design across participants or behaviors (Dukes & Mcguire, 2009; Zylla & Demetral, 1981). In Dukes and Mcguire (2009), the introduction of the intervention across participants occurred only one session apart. Similarly, Zylla and Demetral (1981) staggered intervention across behaviors by either one or two sessions.
Dependent Variables
All studies investigated the effects of sexual education programs on sexual knowledge. Two studies did not further operationalize sexual knowledge (Casper & Glidden, 2001; Zylla & Demetral, 1981), whereas the rest of the included articles specified target areas and/or skills within sexual knowledge (Dukes & Mcguire, 2009; Hayashi et al., 2011; Mueser et al., 1987; Valenti-Hein et al., 1994). These subskills were not further defined into observable and measurable responses. Dukes and McGuire (2009) measured participant knowledge of sexual safety practices, physical self, sexual functioning, and choices and consequences of sexual matters. The authors related this knowledge to the ability to consent to sexual activities. Hayashi et al. (2011) built social skills training into their sexual education program to teach participants how to form and maintain relationships. The outcomes of this program included demonstrations of sociosexual skills such as dating skills in addition to measures of sexual knowledge. Mueser et al. (1987) and Valenti-Hein et al. (1994) investigated the development of heterosexual dating skills and heterosocial interactions within their sexual education program. The authors defined heterosocial interactions as interactions between members of the opposite sex. Neither study further defined dating skills.
Only one study used tests from the sexual education curriculum to collect participant data (Zylla & Demetral, 1981). The program used by Zylla and Demetral (1981) contained seven modules each with its own pretest and posttest. Three studies developed their own tests to assess sexual knowledge (Casper & Glidden, 2001; Mueser et al., 1987; Valenti-Hein et al., 1994). Casper and Glidden (2001) constructed two forms of a pretest and posttest based off of the curriculum that included true or false questions, multiple-choice, and subjective responses. Mueser et al. (1987) developed a nonvalidated 20-item pretest and posttest. The authors did not explicitly state how questions were created or the relationship of assessment questions to course material. Valenti-Hein et al. (1994) measured sociosexual knowledge by implementing Stacking the Deck Baseline Procedures (STDs; Foxx, McMorrow, Storey, & Rodgers, 1984). Participants were presented with a series of social/sexual questions in the context of playing a board game, and researchers recorded participant responses. Researchers conducted this procedure throughout each phase of the study, but it was unclear whether participants received the same questions during each replication.
The remaining two studies used rating scales to assess acquisition of sexual knowledge (Dukes & Mcguire, 2009; Hayashi et al., 2011). Hayashi et al. (2011) applied a published instrument titled Kikuchi’s Scale of Social Skills (KiSS-18) to measure the effects of intervention on interpersonal skills and ability to problem solve social and sexual situations. The KiSS-18 has demonstrated satisfactory reliability and validity but had never been used for people with ID until this study. Dukes and McGuire (2009) incorporated the Sexual Consent and Education Assessment (SCEA) to assess sexual knowledge and capacity to make sexual-related decisions. The SCEA is composed of the following scales: Knowledge of Human Sexuality (K-Scale), Safety Practices (S-Scale), and Inappropriate Sexual Behavior Scale. The authors reported the high internal stability, interrater reliability, and the satisfactory test–retest reliability of this scale. In addition, Dukes and McGuire (2009) described how previous research used the SCEA to assess decision-making capacity with adults with ID; however, the authors gave no further detail on the outcomes of this research.
Two studies included naturalistic observations and role-plays in addition to information tests to assess the effects of intervention (Mueser et al., 1987; Valenti-Hein et al., 1994). Mueser et al. (1987) rated clients during six role-plays on 13 skills related to social and sexual knowledge with higher ratings associated with more appropriate responses. Valenti-Hein and colleagues (1994) also rated participants during role-plays using a consolidated version of these skills. Skills incorporated in role-play scales included demonstrations of general skills, appropriate content, appropriate style, comprehension, positive emotions, and physical attractiveness.
Independent Variables
Curriculum
The level of detail in the description of the curriculum and how participants received content during intervention sessions varied across studies, making curricular comparisons difficult. Two of the six studies included commercial sexual education curricula: Living Your Life—The Sex Education and Personal Development Resource for Special Education Needs–Revised Edition (Dukes & McGuire, 2009) and The Sexual Education Planning Course for People (Zylla & Demetral, 1981). Two studies reported developing their own curriculum (Hayashi et al., 2011; Valenti-Hein et al., 1994). Hayashi et al. (2011) developed a sexual education curriculum that focused on interpersonal relationships and social skills. Following their initial study in dating skills and heterosocial interactions (Mueser et al., 1987), Valenti-Hein and Mueser (1990) developed and standardized a program called the Dating Skills Program (DSP) that was used in their later study (Valenti-Hein et al., 1994). Casper and Glidden (2001) and Mueser et al. (1987) did not state whether their curriculum was commercially available or developed by the authors.
Content
All studies implemented sexual education curriculum that included content on sexual intercourse, functioning, and birth control. Four of the articles shared the following content in their curriculum: biological identification, gender identification, pregnancy and pregnancy prevention, hygiene, and safe sex (Casper & Glidden, 2001; Dukes & Mcguire, 2009; Hayashi et al., 2011; Zylla & Demetral, 1981). Three articles also included information on protective behaviors and choice (Casper & Glidden, 2001; Dukes & Mcguire, 2009; Hayashi et al., 2011). Hayashi et al. (2011) included training on manners in public spaces, self-assertiveness, communication, first impressions, and domestic violence. Similarly, Mueser et al. (1987) and Valenti-Hein et al. (1994) focused their curriculum on social interactions and dating skills by including the following topics: initiating, maintaining, and ending conversations; listening skills; identifying and recognizing emotions; identifying similarities between oneself and others; compliments; places to go on a date; asking for a date; compromising; and resisting persuasion. Across studies, the sexual education curriculum focused solely on heterosexual relationships.
Presentation
All six studies varied in the presentation of course content. Four studies provided brief, generic descriptions on how trainers presented content to participants (Dukes & Mcguire, 2009; Hayashi et al., 2011; Mueser et al., 1987; Valenti-Hein et al., 1994), and the remaining two studies provided few details on how researchers conducted sessions (Casper & Glidden, 2001; Zylla & Demetral, 1981). Hayashi et al. (2011) integrated games, demonstrations, group conversations, and lectures during their intervention sessions. Mueser et al. (1987) and Valenti-Hein et al. (1994) described using role-plays and group discussions as the primary presentation of skills. Mueser et al. compared the efficacy of three different strategies for teaching dating skills: traditional problem-solving (TPS) training, flexible problem-solving (FPS) training, and relaxation training (RT). In each training, therapists presented a topic and scenario associated with that topic (e.g., “Let us pretend you are about to go on a date”). All groups received the same course content but different problem-solving approaches. In their follow-up study, Valenti-Hein and colleagues further examined the TPS approach in isolation.
Materials
Two of the six articles discussed the inclusion of handouts and worksheets, although the authors did not describe the level of detail on these materials or the frequency of their use (Casper & Glidden, 2001; Dukes & Mcguire, 2009). Dukes and McGuire (2009) and Zylla and Demetral (1981) included two anatomically detailed dolls but did not describe how, when, and how often the researchers incorporated these dolls within sessions. Both Dukes and McGuire (2009) and Casper and Glidden (2001) included line drawings in their curriculum, but did not disclose how, when, or what was depicted using line drawings. Two studies discussed incorporating supplementary materials into their curriculum including a feminine hygiene kit, contraceptive samples, films, and overhead slides but did not provide details on how often trainers employed these materials and with what sexual content (Hayashi et al., 2011; Zylla and Demetral, 1981).
Instructional duration and format
The programs varied in duration (range = 6 weeks–3 months) and format. Two studies conducted individual training sessions (Dukes & Mcguire, 2009; Zylla & Demetral, 1981) and four implemented group sessions (Casper & Glidden, 2001; Hayashi et al., 2011; Mueser et al., 1987; Valenti-Hein et al., 1994).
Fidelity, Validity, and Reliability
Treatment fidelity
None of the studies reported collecting treatment fidelity data or any protocols in place to assess the fidelity with which instructors implemented the intervention. Similarly, none of the studies provided information on training procedures or qualifications of persons leading the sexual education sessions.
Social validity
None of the studies explicitly described investigating the social validity of their intervention; however, Hayashi et al. (2011) and Casper and Glidden (2001) collected some information on participant perceptions. Hayashi et al. gathered data at the end of every session on participant perceptions of enjoyment, difficulty, and usefulness of the information discussed. Participants answered these three questions for each session, and the authors reported the mean of participant responses in the final results. Casper and Glidden collected information on participants’ values, opinions, attitudes, and perception of their own sexuality on their pretest and posttest assessment, but did not include questions on participants’ opinions of the program. The authors also briefly reported and discussed anecdotal data. For example, program staff from four participants’ homes reported that participants “regularly discussed class material with their peers and staff outside the class, and increased requests for information and assistance with sexuality issues” (Casper & Glidden, 2001, p. 175). The results did not include quotes or interactions with participants as support of the social relevancy of the sexual education program.
Reliability
Four studies collected interobserver agreement (IOA) on at least one of their measures (range = 91%-100%; Dukes & Mcguire, 2009; Mueser et al., 1987; Valenti-Hein et al.,1994; Zylla & Demetral, 1981). Zylla and Demetral (1981) calculated point-by-point IOA at the end of each training session and reported 100% IOA. Dukes and Mcguire (2009) reported that a second rater reviewed a sample of 12.5% of data collected which resulted in an interrater reliability score of 91%. The authors did not provide the formula for how they calculated agreement. Furthermore, two studies collected IOA on only one outcome measure rather than all measures included within their research (Mueser et al., 1987; Valenti-Hein et al., 1994). Mueser et al. (1987) reported that two raters simultaneously observed during behavioral observations only and the percentage of agreement was 92%. The authors did not disclose the formula used to calculate reliability or the percentage of observations authors collected IOA. Valenti-Hein et al. (1994) also reported IOA for behavioral observations alone and calculated IOA using the Cohen kappa statistic (κ = 0.96). The authors did not report the percentage of total observations observers collected IOA.
Effects
Outcomes across studies demonstrated participants successfully learned sexual content regardless of the curriculum or treatment participants received (e.g., TPS, FPS, and RT). Hayashi et al. (2011), Mueser et al. (1987), and Valenti-Hein et al. (1994) focused on building sociosexual knowledge through structured role-plays and large group discussions. Each of these studies varied slightly in its analytic procedures, but the collective result indicates a positive change in participant understanding and responses to sociosexual situations (Hayashi et al., 2011; Mueser et al., 1987; Valenti-Hein et al., 1994). Mueser et al. conducted two repeated-measures MANOVAs, one from pretreatment to posttreatment and one from pretreatment to follow-up using the means of the 13 skill dimensions from the role-play rating scale as dependent variables. Valenti-Hein et al. also analyzed differences between groups on rating scales from pretreatment and posttreatment by conducting separate ANOVAs for each scale. Mueser et al. reported that the TPS group alone consistently increased their skills across time. Results from Valenti-Hein et al. replicate the effects of Mueser et al.’s research by demonstrating that participants applying TPS methods to sociosexual situations increased their skills and knowledge from pretreatment to follow-up.
Similar to Mueser et al. (1987) and Valenti-Hein et al. (1994), Hayashi and colleagues (2011) focused their intervention on building interpersonal skills within sexual education. Findings from this study demonstrate that the intervention group went from approximately 55.4 (SD = 12.9) to 61.8 (SD = 13.2) posttreatment on the KiSS-18 (out of 90 possible points) versus the control group whose average score decreased across the study from 69.3 (SD = 12.7) to 65.7 (SD = 14.5). Results of the Wilcoxon signed-rank test (an alternative to a t-test) found a meaningful difference between pretest and posttest (p < .05). The authors provided results for the group average but did not publish results for individual participants.
Unlike the previous studies, Casper and Glidden (2001) targeted sexual knowledge directly rather than through sociosexual skills. The authors reported participants, on average, increased from 9.0 points on a pretest to 12.9 on the posttest and all but one participant demonstrated improvement from pre- to posttest measures. Casper and Glidden conducted a 2 × 2 ANOVA with repeated measures on the pretest versus posttest factor on the paired data and identified a significant difference between scores, F(1, 10) = 20.80, p = .001. The authors also included subjective pretest and posttest scores to determine attitudinal changes due to intervention. Only 50% of the adults demonstrated a change from pretest to posttest. A paired-samples t-test indicated that the increase for these participants was significant, t(11) = 3.02, p < .05.
Both single-subject studies demonstrated the characteristics of a functional relationship (Dukes & Mcguire, 2009; Zylla & Demetral, 1981). Zylla and Demetral (1981) reported that all participants went from an average of 44% on pretests to an average of 100% on posttests. Results from Dukes and McGuire (2009) found that all participants increased their knowledge on each SCEA scale to approximately 100%. Participants maintained at or slightly below intervention levels at a 6-month follow-up.
Limitations of the Literature
Primary limitations within this literature include the broad definition of sexual knowledge and a lack of clarity on the sexual education program itself. Although four of the articles explicitly explored subskills or content areas within sexual knowledge, the objectives generated from these studies are still relatively general. Without sexual knowledge operationalized into a measurable, well-defined goal or divided into quantifiable components, it is difficult to analyze how the various data collection and procedural systems aligned with the dependent variable. A similar lack of detail occurred with how researchers described sexual education curriculum and content presentation. The current descriptions of the sexual education programs did not provide evidence toward the quality of program, particularly for researcher-created curriculum. Precise descriptions of curriculum content would facilitate comparisons across studies and examinations of how content and instructional delivery affected diverse populations across settings. Explicit data collected on instructional techniques such as role-plays corresponding with the type of format (e.g., individual vs. group) and population (e.g., adults with mild ID) may provide practical information on how various populations of adults respond to diverse formats and presentations.
Research designs and data analysis
This review identified issues with the appropriateness of the study designs being implemented and the methods researchers used to conduct data analysis. The two studies that implemented a multiple-baseline design introduced the intervention condition one to two sessions apart per participant. The temporal distance of the introduction of the intervention across participants does not allow for adequate data collection or analysis to determine whether a functional relationship exists and fails to follow the standards of multiple-baseline designs (Horner, Carr, Halle, McGee, Odom, & Wolery, 2005).
Similar methodological problems exist in the two studies that implemented quasi-experimental pretest–posttest designs (Casper & Glidden, 2001; Hayashi et al., 2011). The lack of randomization and an inadequate demonstration of comparability between experimental groups and participants generate some wariness of the reported outcomes (Gersten et al., 2005). Both Hayashi et al. (2011) and Casper and Glidden (2001) demonstrated significant differences between pretest and posttest scores using methods of analysis traditionally utilized for larger, homogeneous comparison groups (Kar & Ramalingam, 2013). Neither study addressed the choice of data-analytic method or discussed how they addressed the potential heterogeneity between participants and how this may have influenced their findings.
Even though Mueser et al. (1987) and Valenti-Hein et al. (1994) implemented stronger designs and analyses, their methods require further discussion. Difficulties exist when researchers attempt to use statistical tests that may not be sensitive to small samples (n = 26). Both authors conducted ANOVA and detected significant results, but a potentially more useful analysis would be to compare individual responding across time. Adults with disabilities vary significantly; therefore, research using smaller sample sizes may benefit from an analysis of individual responding versus reporting changes in the group as a whole. Data collected and analyzed individually may provide necessary guidance on future trainings with a similar population.
Of greater concern to this review is the lack of treatment fidelity across studies, as there is no data to confirm that these studies implemented program content as intended. This recurring methodological flaw affects the validity of findings included in this synthesis.
Strengths of the Literature
Despite concerns with study methodology and comprehensiveness of procedures, this review extends research in sexual education in several ways. Each study explored a sensitive topic and encouraged the continued access to knowledge and age-appropriate experiences for adults with varying degrees of ID. The positive findings indicate the potential for sexual education programs to increase participant knowledge regardless of the level of cognitive impairment. Furthermore, the diversity between independent variables signifies the robustness of sexual education to affect adults with ID irrespective of format, context, duration, or curriculum content. As each study reached the collective objective to increase sexual knowledge, the use of differing approaches suggests the potential scaffolding or matching of sexual material depending on the needs and interests of participants.
Discussion
Sexual education is a challenging but essential content area for adults to have. Sexual knowledge provides adults with disabilities opportunities for exploration in negotiating their own sexuality, increases awareness of sexual safety, and may facilitate the formation of intimate relationships with others. This review examined previous experimental and quasi-experimental literature in sexual education training for adults with disabilities to provide an updated comparison of program components and effects. A systematic search of the literature produced only a small number of experimental studies that investigated the effects of sexual education in adulthood. Participants across studies demonstrated gains from baseline assessments to post-intervention measures despite differences in sexual education curriculum and procedures. Although the positive findings are encouraging, this synthesis exposed the need for additional research in sexual education that attends to the quality indicators for experimental designs.
The questions guiding this review attempted to identify the effects of sexual education programs on adults with ID and the curricula components of these programs. As a whole, the components included in the sexual education interventions appeared to stem from a more traditional approach of sexual prevention and restraint. None of the studies outlined the theoretical perspectives influencing their approaches, and all researchers focused on heteronormative content. This synthesis supports previous research findings that suggest individuals with disabilities often receive a restrictive sexual education (Löfgren-Mårtenson, 2012; Stoffelen, Kok, Hospers, & Curfs, 2013). While all studies in this review yielded positive results, a more comprehensive program may have provided participants opportunities for exploration in sexuality and sexual intimacy. In addition, the values of the researchers and sociocultural expectations for individuals with disabilities may have influenced the components of each intervention (Barak & Fisher, 2001).
Limitations
This synthesis has several limitations. One limitation is due to the quantity and quality of studies reviewed. A majority of articles identified were published over a decade ago. While the identified articles represent the intervention literature available in sexual education for adults, the age of the literature may not reflect current standards of research or practice. Given the paucity of research on this topic, future reviews should consider expanding the inclusion criteria (e.g., age range, study design, diagnosis) to potentially identify additional articles. In addition, this review included articles from three different countries (Japan, the United States, and Canada). Sexual expression and education may reflect the national policies and cultural norms of these countries; therefore, the results of this analysis should be interpreted with caution. There is the potential that differences between countries and cultures resulted in variability between seemingly similar participants. This may have influenced how researchers presented and discussed similar content. Future reviews may consider grouping articles by country and/or culture to further examine differences in intervention components and effects.
Implications for Practice
Sexual education is necessary for adults with ID to be fully included in our society (Shakespeare, 2000). Practitioners and disability organizations that work with adults with ID should use these encouraging findings to evaluate their current sexual education curriculum, and consider methods to assess existing sexual knowledge of adults with ID and how adults with ID can be involved in sexual education opportunities. A majority of participants included in this synthesis lacked basic knowledge of reproductive functioning and gender identification; therefore, gaining foundational sexual knowledge in secondary school may promote safer practices among secondary students and young adults with ID. A critical evaluation of program content at the secondary level may streamline content from school age to adulthood and permit postsecondary settings to provide more complicated aspects of romantic relationships, sexual safety, and physical intimacy. Given the large number of participants from the included studies who lived in group housing (n = 47), residential settings may provide the primary pathway to identify adults interested or in need of sexual education programs (Casper & Glidden, 2001: Dukes & Mcguire, 2009; Hayashi et al., 2011; Valenti-Hein et al., 1994; Zylla & Demetral, 1981).
Implications for Research
This review revealed the need for additional studies in sexual education for adults with ID that include detailed descriptions of materials, methods, and procedures to allow for systematic replication and an enhanced understanding of how instructional programs influence diverse participants. Researchers should consider implementing more rigorous experimental designs and quantitative measures to promote greater confidence in study findings. The articles included in this synthesis primarily used rating scales and quizzes as outcome measures. The information gleaned from these measures solely indicates a change in knowledge, not behavior. To address this issue, future research should include data on behavioral outcomes such as burgeoning or ongoing romantic relationships, sexual safety, and sexual health. The addition of these outcomes would demonstrate the durability and generalizability of sexual education to not only increase sexual knowledge but positively affect sexual behavior over time.
Further development of comprehensive curriculum that reflects coupling beyond heterosexual pairings should also be investigated. Researchers should not assume all participants respond to the same sexual stimuli nor should information be restricted to the dominant sexual paradigm. It is necessary for future research to create and disseminate resources to involve participants who may not engage in heterosexual relationships.
Final Thoughts
The present review served to examine the current state of the field of sexual education research for adults with ID. Findings support the potential efficacy of sexual education programs and extends literature on sexual education for adults with ID. Despite evidence suggesting the possible effectiveness of interventions and an established need for sexual education within adulthood, the results of this review suggest experimental research on sexual education for adults remains low. The field of special education has an obligation to further explore sexual education programs for adults with ID and other disability categories. Sexual education programs provide opportunities for adults to gain sexual knowledge, reduce sexual vulnerability, and increase capacity for making sexually related decisions. Using the extant literature as a guide, researchers and practitioners must continue to examine and identify effective frameworks for sexual education interventions that promote sexual knowledge and safety within adulthood. It is the hope that this review may serve as a call to action and initiate the resurgence of experimental literature investigating sexual education opportunities for all adults with disabilities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.