
Abstract
Many people surgically alter their physical appearance with the intent of boosting their social and psychological well-being; however, the long-term effectiveness of aesthetic surgery on improving well-being is unconfirmed. The present comparison-controlled study examines outcomes in a sample of 544 patients who underwent aesthetic surgery (surgery group) and 264 participants who were interested in aesthetic surgery but did not undergo it (comparison group). Participants were followed 3, 6, and 12 months after aesthetic surgery or after contacting the clinic (comparisons). Overall, the results reveal positive outcomes of receiving aesthetic surgery across areas, including anxiety, social phobia, depression, body dysmorphia, goal attainment, quality of life, life satisfaction, attractiveness, mental and physical health, well-being, self-efficacy and self-esteem. Among those dissatisfied with a particular physical feature and considering aesthetic surgery, undergoing surgery appears to result in positive self-reported psychological changes.
Modern advances in surgical technology, combined with increased monetary means and media messages about beauty, have seen an explosion in aesthetic surgery procedures since its modern emergence at the turn of the 20th century (Haiken, 1997). An estimated 8.5 million aesthetic surgeries are performed worldwide each year (International Society of Aesthetic Plastic Surgery, 2011), including approximately 1.5 million in the United States (American Society of Plastic Surgeons, 2011) and more than 200,000 in Germany (International Society of Aesthetic Plastic Surgery, 2011). Despite its popularity, aesthetic surgery is also controversial, as scientists, scholars, and members of society express ambivalence between a view of aesthetic surgery as an empowering procedure with the potential to enhance life satisfaction and one emblematic and reinforcing of oppressive, idealized, unattainable, and primarily Caucasian societal beauty norms, in effect pathologizing and homogenizing normal human variation, including racial and age-related differences (Heyes & Jones, 2009). Scholars have described aesthetic surgery not as a mere beauty-enhancing procedure but as an embodied identity intervention that has the potential to assist people in “passing” for, or having more features of, a different ethnic group (typically Caucasian), age, or norm group (typically one with more status), thus addressing the suffering that follows from internalizing a sense of “otherness” or difference (Davis, 2003). Societal implications aside and despite limited research indicating that individuals are generally satisfied with the procedures they undergo (Honigman, Phillips, & Castle, 2004), little is known about the real psychological outcomes for those who undergo aesthetic surgery procedures.
The features of beauty, such as facial averageness and proportion, appear to be universally recognized (Kościński, 2007; Rubenstein, Langlois, & Roggman, 2002) and confer advantage in that attractive people are judged more positively, treated more positively, and display more positive behaviors than their less attractive peers (Langlois et al., 2000) across a variety of domains (Eagly, Ashmore, Makhijani, & Longo, 1991). But do all of these advantages result in greater happiness and well-being? More attractive people (both self-rated and other rated) do report greater subjective well-being, but the correlation is small (Diener, Wolsic, & Fujita, 1995) and research limited.
The pressure for beauty has traditionally been felt more strongly by women than men, and although aesthetic surgery patients hail from both genders, the majority of patients are female, with women undergoing 87% of aesthetic surgery procedures and 92% of increasingly popular “minimally invasive” cosmetic procedures (injections, laser resurfacing, etc.; American Society of Plastic Surgeons, 2011). Thus, it is typically feminist scholars who raise concerns about aesthetic surgery, arguing that it places the responsibility for the beauty advantage on women (and their surgeons), rather than placing blame on the discriminatory societal and systemic constraints that compel people to bodily dissatisfaction and subsequent surgery. Furthermore, they compare the implicit acceptance of discrimination against “ugliness” (or even normal “imperfection”) that is inherent in aesthetic surgery to saying that racism is an individual problem to be overcome, rather than a societal ill (Bordo, 2009). Conversely, the reality of the beauty advantage being what it is, other scholars suggest that aesthetic surgery is an agentic personal choice with the potential to enhance happiness, well-being, and success in life (i.e., Heyes & Jones, 2009). Indeed, both aesthetic surgery patients (Kinnunen, 2010) and researchers (Grossbart & Sarwer, 1999) tend to frame the ultimate goals of aesthetic surgery in psychosocial terms, despite the fact that in reality, major life events do not tend to have a long-lasting effect on set levels of life satisfaction or general subjective well-being (i.e., the hedonic treadmill effect; Brickman & Campbell, 1971; Diener, Lucas, & Scollon, 2006). Is embodied change via aesthetic surgery an exception?
Whereas perioperative psychological distress in the form of anxiety and depression tends to be more common than physical complications in aesthetic surgery patients and more common in those with preoperative psychological symptoms (Borah, Rankin, & Wey, 1999; Rankin & Borah, 2009), recipients of aesthetic surgery generally tend to report high satisfaction with the aesthetic procedures (Honigman et al., 2004). A recent review in the medical literature reported postsurgery improvements in self-esteem, confidence, happiness, and anxiety, although, as the authors themselves concede, most of the studies reported were over a decade old, with some from the 1960s and with psychological benefits not well elaborated (Shridharani, Magarakis, Manson, & Rodriguez, 2010). A review from a psychological perspective, written to address the question of the justifiability of elective aesthetic surgery to third-party payers as a “psychotherapeutic” treatment, summarized 22 prospective studies of the psychological outcomes of plastic surgery. This review reported improvements in quality of life after breast surgeries (Cook, Rosser, & Salmon, 2006), although this contrasts other research indicating increased mortality by suicide in breast augmentation patients (Sarwer, Brown, & Evans, 2007; Shridharani et al., 2010). The patterns of cause and effect for the latter phenomenon are not yet clear (Rohrich, Adams, & Potter, 2007). Cook et al. (2006) indicated that the studies they reviewed were often plagued by weak methodological standards (i.e., lack of adequate comparison groups, short follow-up periods, and loss to follow-up), leaving the evidence for enduring quality of life for nonbreast surgeries unsupported. Evidence for improvements in mental health (i.e., general mental health and depression, anxiety, and body dysmorphic disorder) and self-esteem for any type of cosmetic surgery were inconsistent, and methodological concerns hampered the ability to draw firm conclusions. As indicated in Honigman et al. (2004), some patients can even experience negative psychological outcomes, especially when they are younger, are male, have unrealistic expectations for the procedure, are motivated to surgery by a relationship, or have a history of anxiety, depression, a personality disorder, or body dysmorphic disorder.
In a more recent comparison-controlled prospective study, 51 aesthetic surgery patients (receiving surgery on the nose, breasts, or upper limbs) were compared with 105 nonaesthetic, nonappearance-altering surgery patients (general, ear-nose-throat, and maxillofacial surgeries) in the United Kingdom on psychological outcomes, with results indicating postoperative improvements in anxiety and depression in both groups, with greater reductions in anxiety and improvements in appearance-related emotions and behaviors related to the specific body part for the plastic surgery patients, and with gains maintained for both groups at 12 months postoperative (Moss & Harris, 2009). In another prospective study of facial surgery patients, patients generally reported decreased appearance-related distress at 3 months postsurgery (Litner, Rotenberg, Dennis, & Adamson, 2008). In one 2-year prospective study of 100 patients, results indicated improvements in overall appearance and body image, satisfaction with the altered feature, and decreased negative body image emotions in social situations 3 months postoperatively, with gains maintained at the 2-year follow-up and effects on self-esteem and depression not statistically significant (Sarwer et al., 2008). In another study of 155 female cosmetic surgery patients, improvements in body image were found, with small improvements in self-esteem and no change in psychological problems at 6 months postsurgery (von Soest, Kvalem, Roald, & Skolleborg, 2009).
The goal of the present study was to provide a large-scale, comparison-controlled, comprehensive investigation of a broad array of psychological outcomes of cosmetic surgery, assessed at presurgery and at follow-ups at 3, 6, and 12 months in a previously understudied population of adults in Germany. The present study offers the following strengths: a large, inclusive patient sample with high participation rates; a systematic comparison with people who are interested in, but do not undergo, surgery; comparisons with a representative sample; a high follow-up rate; an analytical strategy to improve comparability of the patients to the interested group; and assessment with a comprehensive psychological battery. Outcomes included in this battery include goal attainment expectations and actual goal attainment, feelings of attractiveness, self-esteem, quality of life, well-being, and psychopathology. Postsurgical increases in feelings of attractiveness were expected. Given mixed findings in past research and the hedonic treadmill effect, whereby levels of life satisfaction typically begin returning to trait levels within a year of a major life event (Brickman & Campbell, 1971; Diener et al., 2006), long-term (1-year) changes in self-esteem, quality of life, well-being, and psychopathology were expected to be small. Finally, patients’ perception of attaining their primary personal goal was expected both short-term and at 1-year follow-up, consistent with literature indicating that patients are generally satisfied with the outcomes of cosmetic surgery. The interested but nonoperated comparison group served the purpose of excluding alternative explanations that the observed effects were due not to the surgery but to other factors, such as spontaneous remission, repeated measures, hope for success, social acceptance, seasonal mood changes, and so on.
Method
Study procedure
The study was evaluated and approved by the Ethics Committee of the German Society for Psychology (Deutsche Gesellschaft für Psychologie; letter dated March 4, 2007; Registration No. JM20022007DGPS), and it was conducted between March 2007 and September 2009. For ethical reasons, patients could not be assigned randomly to surgery or comparison conditions; thus, the study is quasi-experimental. Data were collected at four time points: before surgery and 3, 6, and 12 months after surgery (treatment condition) or after the initial assessment (comparison condition). Data were collected at each participating hospital with standardized questionnaires, which were typically completed online via SSL encryption and for some patients, upon request, on paper and returned by post. Participation took less than an hour at each time point. All responses were stored under pseudonyms and were not connected to patients’ names or data. At each hospital, the database with name, age, date of birth, gender, address (postal or e-mail), occupation, income, date of surgery, and hospital name was kept separate from the questionnaire responses. The two sets of data were connected by a code for each participant. Data were sent to the authors with participant names, dates of birth, addresses, and e-mail addresses removed. Personally identifying data were deleted after completion of the last data collection, and participants could request to be removed from the study and have all data deleted with no penalty.
No additional physical exams, drug tests, or other invasive measures were performed, and no surgery or other invasive or risky measures were carried out for the purpose of the study. Rather, patients sought out and elected to have surgery of their own volition and were additionally asked about their goals, mental states, and the psychological effects of surgery. The study was therefore purely a survey study based on standardized questionnaires and rating scales. The examinees were thus neither physically nor mentally stressed. The comparison group completed assessments with the same measurement methods and at the same time points as the surgery group.
Participants
Participants were informed in detail about the aims and methods of investigation before the start of the study, and participants signed an informed consent form detailing data protection measures, the voluntary nature of participation, and the right to revoke the agreement at any time, without notice and for any reason. Participation and all generated data were confidential, and no individually identifiable data were provided to the clinics. Participants in the clinical group received compensation for their time, whereas the participants in the comparison group received a small gift and were entered into a drawing for one of three prizes, including a weekend for two at a hotel as an incentive for participation. There were no other stated benefits offered or given for participation. A summary of the sociodemographic characteristics of the sample is given in Table 1. The age range was 18 to 65 years. Persons with missing values on age, income, or gender were not included in the table (listwise deletion).
Full Sample: Predicted Means of Sociodemographic Characteristics
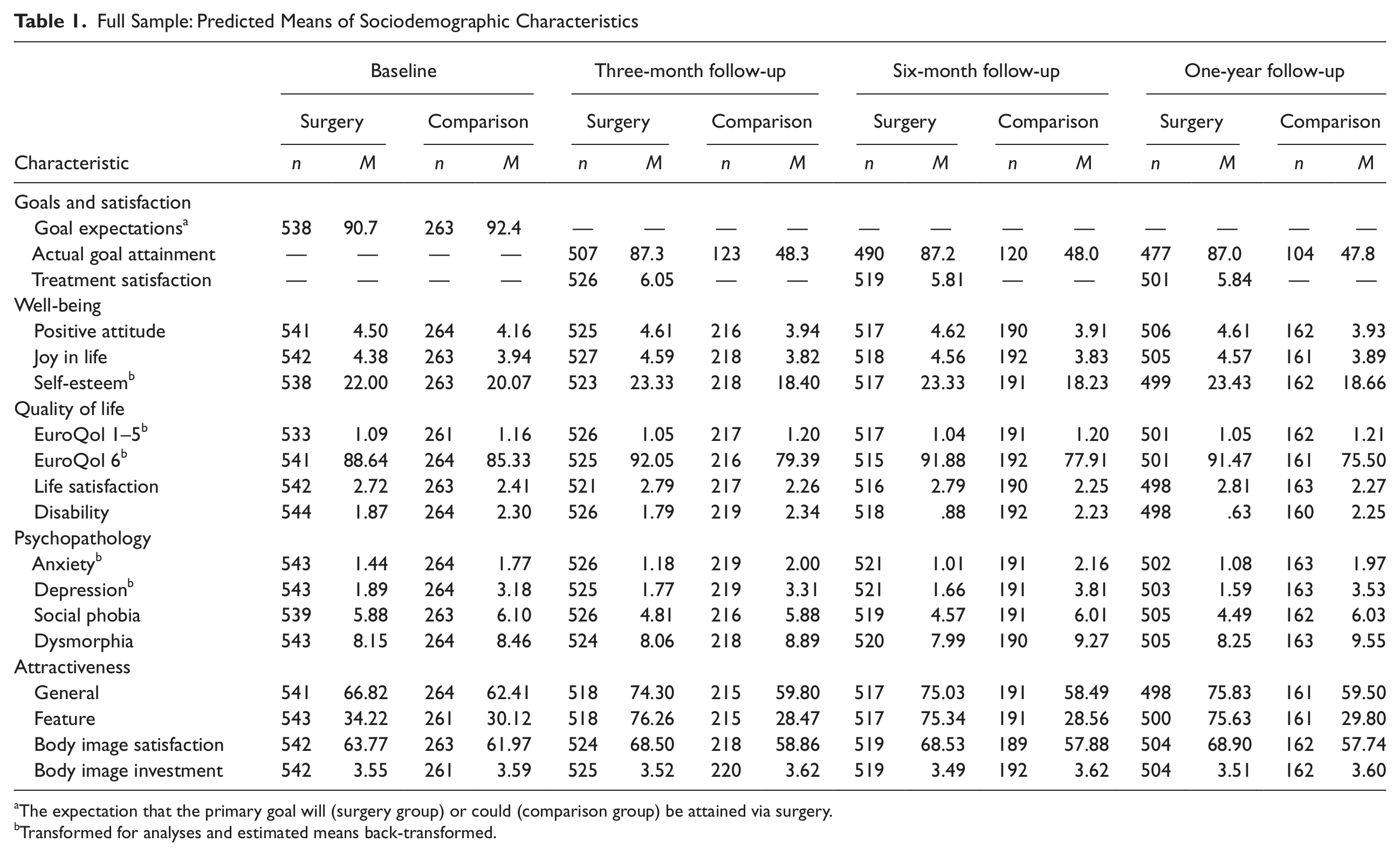
The expectation that the primary goal will (surgery group) or could (comparison group) be attained via surgery.
Transformed for analyses and estimated means back-transformed.
Surgery group
The surgery group consisted of patients who elected to undergo aesthetic surgery and had already been judged to be eligible for surgery, recruited through advertisements and the website of the Mang Medical One AG and during consultations in the clinics. All eligible surgery patients during the time of the study were invited to participate. Exclusion criteria for the study included previous plastic/aesthetic surgery, age younger than 18 years, nonsurgical intervention (i.e., wrinkle injections), and hair transplantation (owing to the different time course of this surgery). Furthermore, prospective patients with body dysmorphic disorder were excluded from surgery via a screening at the clinic, as is standard ethical practice by cosmetic surgeons, and were therefore not included in this sample. Inclusion criteria were informed consent and operation between March 2007 and April 2008 at one of the participating clinics of Mang Medical One AG. A total of 676 patients were initially invited to participate, of whom 564 agreed and 112 declined (see Fig. 1 for participation flowchart). This represents a participation rate of 83.4%. The grounds for refusal were lack of interest (n = 67), lack of time (n = 19), too much effort (n = 14), language problems (n = 9), confidentiality concerns (n = 6), and other (n = 3; multiple entries possible). Of the 564 patients who declared themselves willing to participate, 20 did not meet the inclusion criteria (they were below the age cutoff) so that the final clinical sample comprised 544 patients. The number of people who were not invited to participate owing to a diagnosis of body dysmorphic disorder was not tracked by the clinic and is therefore not known. Data on surgical complications were not available for participants.
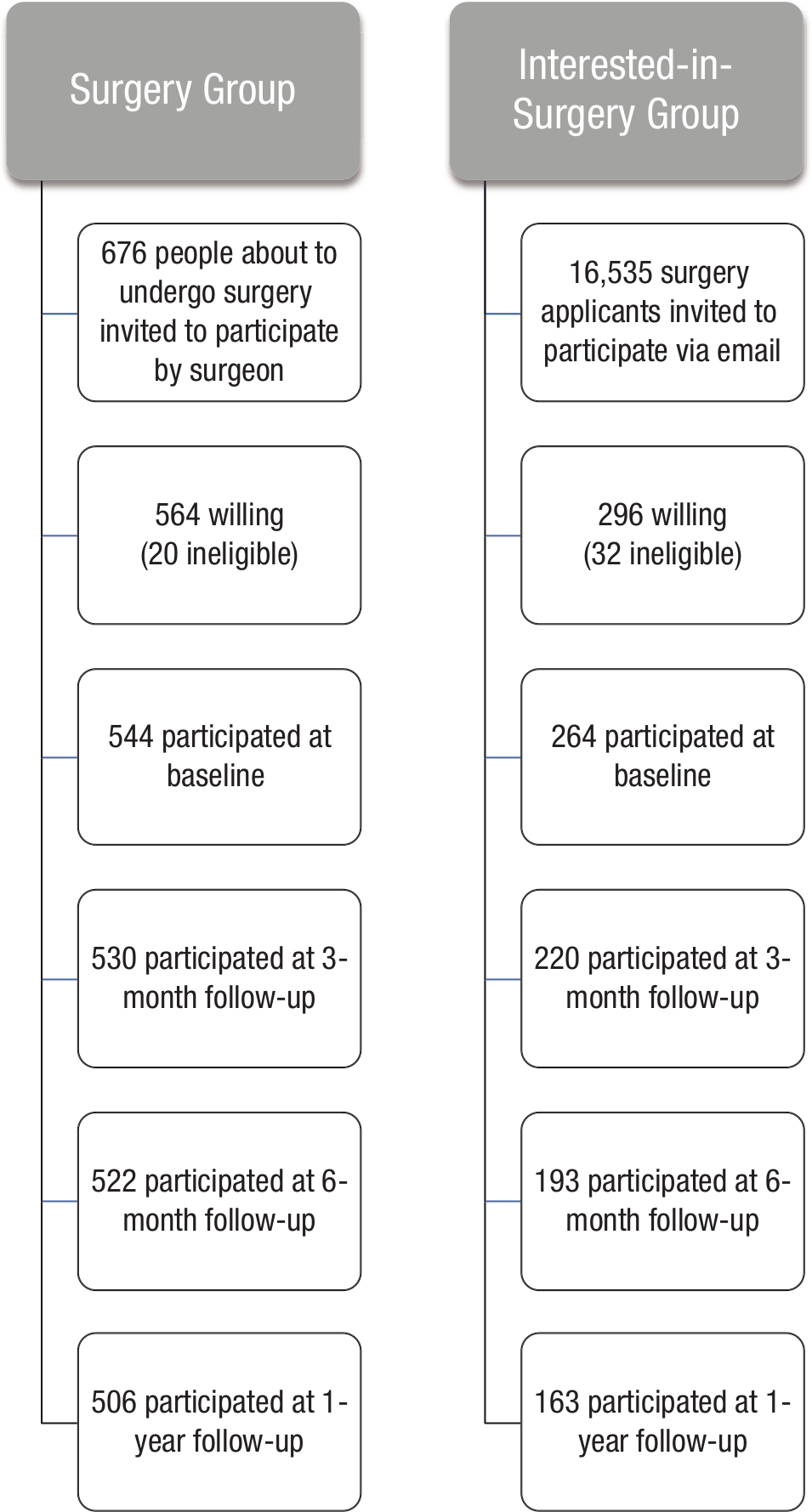
Participation flowchart.
Comparison group
The comparison group consisted of applicants for aesthetic surgery who had not yet undergone surgery. The comparison group was recruited from the Mang Medical One AG address pool of interested but not operated-on people. They were contacted by e-mail with an invitation to participate. The exclusion criteria in the comparison group were the same as in the clinical group and included former aesthetic plastic surgery, age below 18 years, body dysmorphic disorder, and interest in nonsurgical treatments (wrinkle injections) and hair transplantation. Inclusion criteria included informed consent and initial intent to participate for the duration of the study period. A total of 16,535 addresses were contacted via e-mail. Because it was not possible to determine whether all e-mails reached their addressees, we cannot calculate a participation rate for the comparison group. Of the total 296 persons who declared themselves willing to participate, 32 did not meet the inclusion criteria so that the final comparison group comprised 264 persons. The members of the comparison group gave the following information on the reasons for which no operation had yet been performed: financial reasons (61.1%), anxiety (12.2%), and other reasons (e.g., lack of time, lack of information; together 17.5%).
Measures
Global
General assessment of surgical success
Global satisfaction with the operated feature postsurgery was assessed using a single-item bipolar rating scale ranging from 1 (very much more dissatisfied) to 7 (very much more satisfied) to indicate the degree of general deterioration or improvement postsurgery. This provides a direct measurement of change, using the patient’s personal frame of reference.
Goals
Goal attainment scaling
Goal expectations and achievement were assessed on the basis of the classic Kiresuk and Sherman (1968) method for scaling individual treatment goals, which is well suited for measuring change and evaluating courses of therapy. Patients were asked to briefly describe the personal goals they want to accomplish with the planned operation and define up to five different targets in order of personal importance. For each target, patients also specified the extent to which they expected to reach the target with the operation and the extent to which they did reach the target postsurgery. All estimates were made on a scale of 0% (no expectation of meeting the goal/no attainment) to 100% (full expectation/full attainment). The open-ended responses were coded and categorized after all data were collected. The use of open questions minimizes examiner influence and enables the detection of the most salient themes. At the same time, answers can be subject to social desirability
Therefore, in a second step, participants were asked to respond to 10 standard items assessing various realistic targets (i.e., “to feel better,” “to eliminate a blemish”) and some potential unrealistic expectations (i.e., “to be a new man/woman,” “all my problems will be solved”) by checking off which items represented additional goals they had. These combine the advantage of better standardization and easy evaluation with the possibility to obtain information that is not currently salient in the memory structure of the respondents and possibly subject to a lesser degree of social desirability but also perhaps influenced by the constraints of the question formulations. By combining the two methods, an optimal detection of targets is ensured. An index measuring the degree of unrealistic expectations with respect to the success of the cosmetic surgery was calculated according to the ratings from five independent raters, all from the Department of Clinical Psychology and all having a PhD in clinical psychology, who were asked to indicate to what degree they believe that each of the 10 standard questions is realistic on a scale from 1 (completely realistic) to 4 (completely unrealistic). The index was then obtained by computing a weighted average of the 10 questions, with each question getting the weight from the mean across the five raters and used to match groups in the propensity score analysis. For the evaluation of therapeutic response, participants were asked at the postoperative time point to indicate whether they achieved each of the goals they reported in both in the open-ended and closed questions.
Well-being
Positive attitude toward life and joy in life
Positive attitude toward life (eight items; e.g., “My future looks good”) and joy in life (five items; e.g., “In the past few weeks have you felt completely happy?”) were assessed via the respective two subscales of the German-language Berner Fragebogen zum Wohlbefinden (Bern Questionnaire on Subjective Well-Being; Grob, 1995), on a scale ranging from 1 (completely false) to 6 (completely correct) for positive attitude toward life and 1 (never) to 6 (often) for joy in life. Scores across items for each subscale were averaged. Cronbach’s alpha in the present sample was .90 for positive attitude toward life and .77 for joy in life.
Self-esteem
Patient self-esteem was assessed with the German version of the Rosenberg Self-Esteem Scale (original: Rosenberg, 1965; German translation: Ferring & Filipp 1996; German revision: von Collani & Herzberg 2003), consisting of 10 items rated on a scale ranging from 1 (strongly disagree) to 4 (strongly agree), with 5 items reverse coded. The scale yields a total value that can range from 0 (minimal self-worth) to 30 (maximum self-worth). Cronbach’s alpha in the present sample was .87.
Quality of life
Quality of health
Quality of health was assessed with five items across five domains from the EuroQol 5D questionnaire (Brooks, 1996; EuroQol Group, 2007), rated on a scale ranging from 1 (no problems) to 3 (extreme problems). These five items yield an overall summary score and can also be examined separately as indices for the areas of health and quality of life that they assess (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression). In the present study, the alpha for the full scale was .41. Finally, an additional item assesses overall current health status on the current day, on a scale ranging from 0 (worst imaginable health) to 100 (best imaginable health).
Life satisfaction
Life satisfaction was assessed with 13 Likert scale ratings (Trumpf et al., 2010), each ranging from 0 (very unsatisfied) to 4 (very satisfied), assessing satisfaction with 13 areas of life (health, money, looks, marriage, friendships, etc.). The mean across the 13 ratings yields a total score for which Cronbach’s alpha in the present sample was .83.
Disability
Perceptions of the impairment caused by the operated feature was assessed with responses to a German-translated single item from the Sheehan Disability Rating Scale (Sheehan, 1983), rated on a scale ranging from 0 (not at all impaired) to 4 (seriously impaired).
Psychopathology
Screenings for anxiety, depression, and social phobia
German versions of short screening questionnaires designed for rapid detection of the presence of clinically relevant mood disorder symptomatology in routine medical practice (Margraf, 1994, 1998) were used to assess anxiety disorders, depression, and social phobia. The Anxiety Scale consists of 6 items from the 21-item German version of the Beck Anxiety Inventory (Beck, Tiftein, Brown, & Steer, 1988; German version: Margraf & Ehlers, 2007; alpha = .81); the Depression Scale consists of 6 items from the SCL-90-R Depression Scale (Derogatis, 1994; alpha = .85); and the Social Phobia Scale contains 6 items from the Liebowitz Social Anxiety Rating Scale (Liebowitz, 1987; alpha = .82). All items were rated on a scale ranging from 0 (not at all) to 3 (strong). The ratings across items and within each scale were then summed for a score between 0 and 18 points. Clinical cutoffs values were ≥ 7 points for anxiety and depression and ≥ 10 points for social phobia.
Body dysmorphia
Body dysmorphia was assessed with the Dysmorphic Concerns Questionnaire (Oosthuizen, Lambert, & Castle, 1998), a screening instrument designed to detect distorted body image symptoms (i.e., excessive worries about bodily appearances) across seven items rated on a scale ranging from 0 (not at all) to 3 (much more than other people). Summing across items yields a total score ranging from 0 to 21 points, with a clinical cutoff of ≥ 14 points (Oosthuizen et al. 1998). Research indicates that the questionnaire is a sensitive and specific screening tool for routine clinical practice (Jorgensen, Castle, Roberts, & Groth-Marnat, 2001). Cronbach’s alpha in the present sample was .73.
Attractiveness
Attractiveness compared with others
Perceptions of relative appearance as compared with others was assessed using a global single item in the format of a visual analog scale. Using a scale, patients are asked to indicate how good or poor they consider their appearance to be in comparison to the appearance of other people, with 100 representing perfectly beautiful people and 0 indicating completely ugly. This scale is administered in conjunction with that assessing overall health from the EuroQol. Patients were asked to estimate both their general attractiveness and the attractiveness of specific bodily features to be operated on (e.g., chest, abdomen) in comparison with other people.
Body image satisfaction
Feelings of satisfaction with body image were assessed with the Body Image Inventory (Berscheid, Walster, & Bohrnstedt, 1973; Özgür, Tuncali, & Gürsu, 1998), a survey assessing satisfaction with 25 physical traits on a scale ranging from 0 (very dissatisfied) to 4 (very satisfied). Summing the individual items yields a total score ranging from 0 (minimum) to 100 (maximum). Cronbach’s alpha in the present sample was .86.
Body image investment
Investment in bodily appearance was assessed with the Appearance Schema Inventory–Revised (Cash, 2003; Cash, Melnyk, & Hrabosky, 2004; German version: Grocholewski, Heinrichs, & Lingnau, 2007; Grocholewski, Tuschen-Caffier, Margraf, & Heinrichs, 2011), which consists of 20 items rated on a scale ranging from 1 (strongly disagree) to 5 (strongly agree). The inventory contains two subscales assessing self-evaluative salience (i.e., the extent to which people define themselves by and base their self-worth on their physical appearance) and motivational salience (i.e., the extent to which people attend to their appearance and take various measures to uphold it). A total score is derived from the mean across items and indicates the general investment in body image, ranging from 1 (minimal importance) to 5 (maximum importance). Cronbach’s alpha in the present sample for the full scale was .86.
Data analysis
Fifteen outcome measures were longitudinally analyzed. Analyses were performed for each outcome individually and in a combined model of perceived operation success that included 14 outcomes (i.e., all outcomes measured longitudinally except for body image investment, which was not considered a perceived measure of surgery success). We used a random intercept model, a type of linear mixed model (Pinheiro & Bates, 2002), assuming a first-order autoregressive error covariance matrix. Note that mixed models have been shown to provide more efficient and less biased results compared with complete case analyses or analyses in which missing values are imputed using the “last observation carried forward” method (Lane, 2008). Furthermore, mixed models do not require the omission of participants with missing data from the analyses, thereby minimizing data loss, increasing power, and allowing for participants who dropped out of the study to be included in the analyses.
Two analyses were performed. In the first, we used the complete sample (N = 808) and included in the model time (baseline, 3-, 6-, and 12-month follow-up) as the within-subjects factor and group (surgery vs. comparison) as the between-subjects factor. In the second, we used the matched sample (n = 358) and added to the two predictors the propensity scores variable (Gelman & Hill, 2007). Outcomes were transformed if necessary and outliers (standardized residuals with values > 3.0) removed for the final analyses. All analyses were done with R 2.13 (R Development Core Team, 2011), including the packages nonrandom (Stampf, 2011) for propensity scores analysis and nlme (Pinheiro, Bates, DebRoy, Sarkar, & the R Development Core Team, 2011) and lme4 (Bates, Mächler, & Bolker, 2011) for random intercept models.
Propensity score analysis
Propensity scores were used to match pairs on baseline characteristics for a matched analysis of treatment outcomes. Twenty-six baseline characteristics, containing sociodemographics as well as outcomes, were selected for use in propensity score analysis: clinic, occupation, treatment type sought, gender, age, body mass index, income, unrealistic goals, joy in life, positive attitude toward life, social phobia, body image, body image investment, dysmorphia, goal expectations/attainment, quality of health, current health status, self-esteem, anxiety, depression, disability, general attractiveness, operated feature attractiveness, expected general attractiveness after surgery, and expected operated feature attractiveness after surgery. These were thought to be potentially related to both the treatment and the outcome.
Prior to the analysis, missing values were imputed using chained equations as implemented in the R package mice (van Buuren & Groothuis-Oudshoorn, 2011). Owing to the low percentage of missing values (the highest percentage was 5.7% for the body mass index; all other variables had percentages between 0% and 1.9%), we refrained from using multiple imputation models, which would have complicated further analyses, and used single imputation instead. This procedure seemed sufficiently accurate because subjects with missing body mass indices did not significantly differ from those with available indices on the baseline characteristics when adjusting for group membership, based on an alpha of .05, even if not correcting for multiple tests using the Bonferroni error correction method.
We first ran a multiple regression logistic model with group membership as outcome and the 26 baseline characteristics as predictors. We then included two-way interaction terms and quadratic polynomials in turn. The final model contained 24 main effects (all baseline characteristics), one quadratic polynomial (for joy in life), and 21 two-way interactions, χ2(68) = 396.3, p < .001, McFadden’s R2 = .39. Propensity scores were the predicted values from the logistic regression model. Propensity scores were then used to find pairs of participants in each sample with comparable values. To ensure similarity within matched pairs, we used caliper matching; that is, the difference between participants within pairs had to be less than or equal to .25 standard deviations of the logit of the estimated propensity scores (Stampf, 2011). This resulted in 179 matched pairs, the remaining participants being excluded from the analysis of this matched sample.
Results
Missing values analysis
Completers were defined as having available data at all four time points, as opposed to dropouts who did not. The comparison group contained more dropouts than the surgery group (comparison: 38%; surgery: 7.0%; odds ratio = 8.3, χ2 = 122.0, p < .001). The percentage of available cases at time points 0, 3, 6, and 12 months after study start was 100, 97.4, 96.0, and 93.0 in the surgery group and 100, 83.3, 73.1, and 61.7 in the comparison group, respectively. Completers did not differ from dropouts with respect to any analyzed outcome variable at baseline, 3-, and 6-month follow-up and neither with respect to the following eight time-invariant features at baseline: clinic, occupation, treatment type, gender, age, body mass index, income, degree of unrealistic goal setting (p > .05 in each case, adjusted for surgery group versus comparison group membership and corrected for multiple testing using the Bonferroni correction method).
Demographics, surgery type, and participation
The surgery group consisted of 88% females, as compared with the 90% females in the comparison group. Participants fell into four age groups: 18–24 years (27% of surgery, 22% of comparison group), 25–34 (36% surgery, 37% comparison), 35–44 (22% surgery, 26% comparison), and 45–65 (14% surgery, 15% comparison). Sixty percent of the surgery group (64% of the comparison group) had a net monthly income of 1,500 euros or more. The remainder had an income greater than 1,500 euros. The distribution of age groups (p = .44), females (p = .50), a net monthly income higher than 1,500 euros (p = .37), and the prevalence for social phobia (p = .27) were all comparable between surgery and comparison groups, based on chi-square tests. Furthermore, the majority of the surgery and comparison groups was within the normal range in psychopathology. The proportion of people with clinical values was between 8.3% and 17.7% on measures of anxiety, depression, social phobia, and body dysmorphia for patients in the clinical group, depending on the variable, and between 13.3% and 28.8% in the comparison group, with more psychopathology in the comparison group. The groups differed in the probability of a clinically significant value for anxiety (p = .038), depression (p < .001), and body dysmorphia (p = .016; all tests based on chi-square tests). Sought treatment type included the following: liposuction (25% surgery, 24% comparison), breast enlargement (32% surgery, 20% comparison), breast reduction (5% of each group), breast lift (5% surgery, 9% comparison), abdominoplasty (4% surgery, 8% comparison), eyelid surgery (8% surgery, 11% comparison), rhinoplasty (10% surgery, 12% comparison), and other (11% surgery, 12% comparison). Surgery and comparison groups significantly differed at baseline in their distributions of treatment types (p < .001; based on chi-square tests). Ethnicity was not assessed; therefore, exact data on ethnicity are not available, though the demographic was primarily Caucasian.
Goal attainment forecasts
Means for goal attainment forecasts for participants’ top goal are presented in Tables 1 and 2. Goal attainment expectations before treatment were similar between groups, in both the full sample, t(506) = −1.92, p = .055, and the matched sample, t(350) = 0.79, p = .433 (based on Welch two-sample t tests).
Matched Sample: Predicted Means of Sociodemographic Characteristics
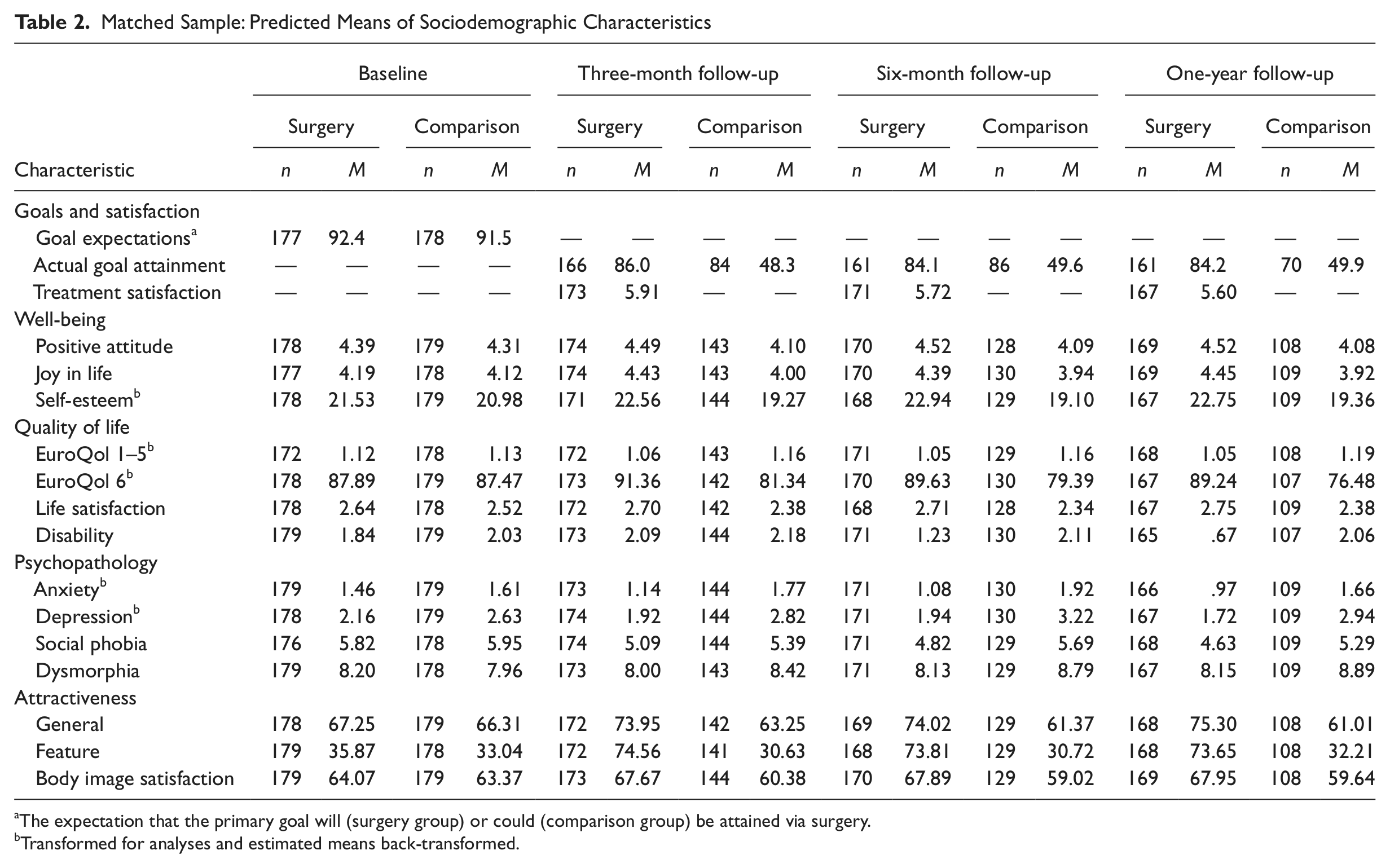
The expectation that the primary goal will (surgery group) or could (comparison group) be attained via surgery.
Transformed for analyses and estimated means back-transformed.
Treatment satisfaction and goal attainment
Means for postsurgical treatment satisfaction and goal attainment for participants’ top goal are presented in Tables 1 and 2. Surgery patients in the full sample indicated a goal attainment of about 87% that was stable across time, whereas the comparison group reported much lower goal attainment at 3-month, t(1,807) = 17.8, p < .001, 6-month, t(1,807) = 17.7, p < .001, and 12-month follow-up, t(1,807) = 17.1, p < .001. Percentages in the matched sample were slightly lower in the surgery group but slightly higher in the comparison group. Differences between groups, however, remained very high for all three time points: 3 months, t(718) = 12.0, p < .001; 6 months, t(718) = 11.0, p < .001; 12 months, t(718) = 10.5, p < .001.
Postsurgery, recipients reported success in terms of satisfaction, with an average in the full sample between 5.81 and 6.05 (much more satisfied). Values at 6 months, t(1,015) = 2.96, p = .003, and 1 year, t(1,015) = 2.56, p = .011, were both significantly lower than those at 3 months. Values for the matched sample were slightly lower in general, and only those at 1-year follow-up were significantly lower than those for 3-month follow-up, t(334) = 2.09, p = .037, whereas those at 6-month follow-up were not, t(334) = 1.30, p = .194.
Baseline comparison of longitudinal outcomes
Predicted means for longitudinal outcomes measures based on the mixed model are presented in Table 1 for the full sample and in Table 2 for the matched sample. Differences between groups at baseline and 1-year follow-up are presented in Table 3 for both samples. In the full sample, the surgery group reported better baseline results than the comparison group in well-being (positive attitude, joy in life, self-esteem), quality of life (health status on the two EuroQol measures, life satisfaction, and disability), psychopathology (anxiety, depression), and self-rated attractiveness (general and feature). There were no significant group differences in social phobia, dysmorphia, body image satisfaction, or body image investment. In the matched sample, no significant differences were found between groups for any outcome at baseline. This basically underlines the successful matching of subjects based on propensity scores and supports the comparability of the two groups.
Between-Group Point Differences and Group × Time Interactions
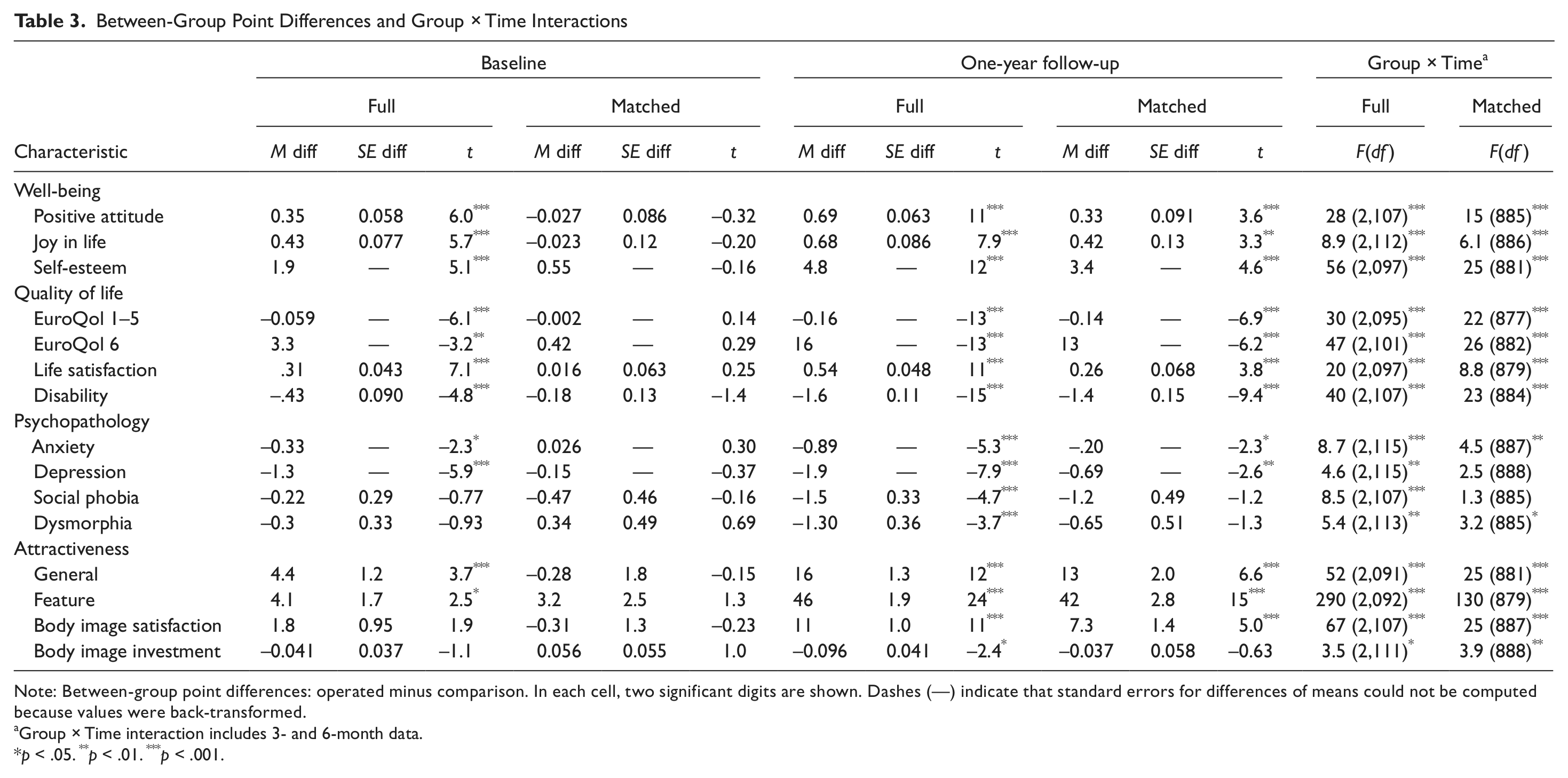
Note: Between-group point differences: operated minus comparison. In each cell, two significant digits are shown. Dashes (—) indicate that standard errors for differences of means could not be computed because values were back-transformed.
Group × Time interaction includes 3- and 6-month data.
p < .05. **p < .01. ***p < .001.
Longitudinal trend
The combined model including 14 outcomes indicated positive effects for the surgery group over the comparison group. An examination of the temporal trend indicates that in both the full sample and the matched sample, psychological outcomes generally improved between baseline and 3-month follow-up and then remained more or less constant in the surgery group, but they slightly declined for the comparison group between baseline and 6-month follow-up. This resulted in a highly significant Group × Time interaction: full sample: F(3, 29,501) = 35.2, p < .001; matched sample: F(3, 10,928) = 21.8, p < .001. Also, values at 1-year follow-up were higher in the surgery group compared to the comparison group: full sample, t(40,805) = 8.32, p < .001; matched sample: t(15,879) = 2.45, p = .014. An examination of effects on individual outcomes in the full sample indicated significant Group × Time interaction effects and highly significant group differences at 1-year follow-up in favor of surgery relative to comparisons for all 15 outcomes (see Table 3). In the matched sample, these effects were in general much smaller than in the full sample, yet they were still highly significant in most cases. Exceptions concerned the psychopathology outcomes social phobia and dysmorphia, as well as body image investment, which no longer differed between groups and the nonsignificant Group × Time interaction effects for social phobia and dysmorphia in the matched sample. Temporal trajectories in the full sample improved (i.e., increased for positive outcomes and decreased for disability and pathology outcomes) in the surgery group more than the comparison group on the following variables: well-being (positive attitude, joy in life, self-esteem), quality of life (EuroQol 1–5, EuroQol 6, life satisfaction, disability), psychopathology (anxiety, depression, social phobia, and dysmorphia), and attractiveness (general, feature, and body image satisfaction). The outcome body image investment decreased for the surgery group as compared with the comparison group, which experienced a slight increase at 3 and 6 months and then a decrease back to baseline at 1 year. Temporal trends in the matched sample were comparable to those observed in the full sample.
Discussion
Results from the present study indicate that among people who are dissatisfied with a physical feature and interested in obtaining aesthetic surgery to correct the feature, those who actually undergo surgery experience more positive outcomes than those who are interested in surgery but do not undergo it, lasting at least 1 year postsurgery. People undergoing aesthetic surgery were generally “somewhat more satisfied” with the operated feature than they were before surgery (reported post hoc) and reported that their primary personal goal had been 80% achieved postsurgery. Furthermore, in comparison to those who were interested but did not obtain surgery, trajectories improved across almost all measures (i.e., increased for positive outcomes and decreased for disability and pathology outcomes) in the following domains: well-being (i.e., positive attitude, joy in life, and self-esteem), quality of life (i.e., general health status, life satisfaction, and disability), some measures of psychopathology (i.e., anxiety and dysmorphia), and attractiveness (i.e., perceptions of general attractiveness, attractiveness of the operated feature, and body image satisfaction), even when matching the two groups on baseline characteristics to comparison for selection effects. Positive effects (i.e., improvements) on depression and social phobia for the surgery group were also found in the full sample but were not robust, becoming nonsignificant in the matched sample. In addition, the surgery group as a whole did not experience any negative psychological effects in the assessed areas postsurgery. In a more exploratory analysis, body image investment decreased for the surgery group versus the comparison group, perhaps indicating that once the unsatisfying feature became more satisfying for the surgery group, patients were less preoccupied with their looks and thus experienced a decrease in body image investment or salience.
Overall, it appears that aesthetic surgery does not generally result in negative psychological outcomes and can indeed have positive effects in multiple domains, helping patients to feel better about a specific feature and meet their goals regarding that feature, more generally increasing feelings of general well-being, life quality, and attractiveness and decreasing anxiety and dysmorphia while having a smaller impact on less directly related psychopathology, such as depression and social phobia. Perhaps surprising, given the hedonic treadmill effect in other domains, whereby major life events tend to have relatively short-term effects on happiness, the positive outcomes for aesthetic surgery appear to be stable, at least over the course of 1 year. Although research has shown that many to most major life changes produce effects than can be powerful but ultimately do not last, because set-level well-being tends to return to an individual’s norm within a year (Brickman & Campbell, 1971; Diener et al., 2006), it may be that embodied changes via aesthetic surgery can produce more permanent psychological change than more temporary or malleable life events, such as relationship changes, relocations, and so on.
First, whereas the current longitudinal study provided extended follow-up data at 1-year postsurgery, the stability of effects after the first year is not addressed. An even longer-term study following surgery patients and comparisons at 2, 3, and more years postsurgery would be helpful in understanding more permanent effects.
Second, the present study included a limited population of surgery patients who were undergoing a first surgery. It would be beneficial to assess outcomes in people who undergo minimally invasive procedures (i.e., injections) or multiple surgeries to determine whether effects may be additive or capped at a certain level or whether the pattern of effects may be different in people seeking multiple surgeries or minimally invasive surgeries.
Third, the present study did not address causation. For this, a true experiment would be required. Random assignment was not done in the present study for obvious ethical reasons; however, it may be that a future study could assign surgery seekers to immediate treatment and wait-list conditions. This may also decrease the dropout rate in the comparison condition that was experienced in the present study.
Fourth, the present study did not differentiate among types of surgeries. It may be that satisfaction with surgery and the psychosocial effects of surgery are dependent upon surgery type and the risks and success rates associated with each surgery type. Future studies should investigate this further.
Fifth, the present study excluded patients with body dysmorphic disorder, as is standard practice at the clinics participating in the study. It could be that initial baseline characteristics of the two groups may have differed or that outcomes for people with body dysmorphic disorder would not have been as positive as those found in the present study, had they been included. Unfortunately, the clinics did not have available data on how many people were determined to be ineligible for surgery owing to body dysmorphic disorder.
Sixth, the present study did not address meditational pathways. It would be interesting to evaluate whether effects on attractiveness (including other-rated attractiveness) mediated the effects of surgery on psychological outcomes, perhaps via more positive treatment by members of society, one’s family, romantic partners, and so on. Other potential mediators of the effects could include self-efficacy or a sense of control or mastery. In taking action, surgery patients may have increased their self-efficacy relative to those in the comparison group, who wanted to make a change but did not.
Seventh, the question of what constitutes true satisfaction in life should be acknowledged. Certainly, life satisfaction comes in different forms for different people. However, it is quite possible that were other factors in surgery seekers’ lives improved or focused on—such as connection to accepting partners and family members, spirituality, a quest for meaning, or self-acceptance—life satisfaction would improve just as much as or more than what was experienced by surgery patients. Indeed, despite the multitude of studies in support of the beauty advantage, some research indicates that less attractive people with less symmetrical faces are more generous (Sanchez-Pages & Turiegano, 2010) than their prettier, more symmetrical peers. Other advantages of being less physically attractive should be further clarified. Future studies should also seek to more fully understand the characteristics of people who opt for aesthetic surgery in comparison to the general population to determine other potential areas for positive changes that could increase well-being.
Finally, future studies should compare the effects of surgery with the effects of a well-established psychotherapy or with interventions to increase, for example, self-acceptance, meaning, spirituality, and connection for improving self-esteem, well-being, feelings of attractiveness, and so on. For instance, although research is limited, cognitive-behavioral therapy is considered a generally efficacious therapy for body dysmorphic disorder (Veale, 2010). Thus, it could be that therapeutic intervention would have positive effects in subclinical cases of bodily dissatisfaction as well. Comparisons between therapy and actual physical changes via aesthetic surgery should be undertaken.
Results from the present study indicated overall positive effects on appearance satisfaction, goal attainment, well-being, life quality, self-perceived attractiveness, and decreased anxiety and dysmorphia, whereas no group-level negative psychological effects were observed. Instead, there were also small decreases in depression and social phobia. Among people who are dissatisfied with a particular physical feature and who are considering aesthetic surgery, undergoing aesthetic surgery appears to be more psychologically beneficial on the outcomes measured than not undergoing surgery, in the absence of any other type of intervention, such as psychotherapy and increased acceptance by loved ones.
Footnotes
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This study was supported by Mang Medical One AG, a large provider of plastic surgery in Germany, under the direction of the first author while at the Department of Psychology at the University of Basel. The study directors were scientifically independent and not bound by the directives on any important issues such as design, analysis, and presentation. We appreciate the participants in this study and the research assistants on the project for their assistance in data collection and management.