
Abstract
Although it is well established that bipolar I disorder (BD) is characterized by excessive positive emotionality, the cognitive and neural processes that underlie such responses are unclear. We addressed this issue by examining the role that an emotion regulatory process called self-distancing plays in two potentially different BD phenotypes—BD with versus without a history of psychosis—and healthy individuals. Participants reflected on a positive autobiographical memory and then rated their level of spontaneous self-distancing. Neurophysiological activity was continuously monitored using electroencephalogram. As predicted, participants with BD who have a history of psychosis spontaneously self-distanced less and displayed stronger neurophysiological signs of positive emotional reactivity compared with the other two groups. These findings shed light on the cognitive and neural mechanisms underlying excessive positive emotionality in BD. They also suggest that individuals with BD who have a history of psychosis may represent a distinct clinical phenotype characterized by dysfunctional emotion regulation.
The core clinical features of bipolar I disorder (BD) involve difficulties regulating positive emotions, including periods of mania characterized by persistent and abnormally elevated positive mood associated with significant impairment (American Psychiatric Association, 2013; Angst, Stassen, Clayton, & Angst, 2002). Empirical models of BD suggest that the inability to effectively regulate positive emotions may play a critical role in the onset and maintenance of BD (Gruber, Eidelman, Johnson, Smith, & Harvey, 2011; Johnson, 2005). Yet surprisingly few researchers have examined the cognitive and neurophysiological mechanisms associated with positive emotion regulation in BD using carefully controlled laboratory paradigms.
In the current research, we explored this issue in two ways. First, using a combination of self-report and neural measures, we examined whether individuals with BD differ from healthy individuals in their tendency to spontaneously engage in a widely studied emotion regulatory process, referred to as self-distancing (Ayduk & Kross, 2010a; Kross, 2009; Kross & Ayduk, 2011), when they reflect on positive autobiographical memories. Second, we examined whether a history of psychosis influences the ability of people with BD to regulate positive emotions spontaneously—in particular, their ability to spontaneously self-distance while reflecting on positive autobiographical memories.
Self-Distancing as an Emotion Regulatory Process
Converging evidence has indicated that people can reflect on emotional memories from different vantage points, which directly influence the type of information that becomes accessible and the degree of emotional reactivity people display (Kross, Ayduk, & Mischel, 2005; Nigro & Neisser, 1983; Robinson & Swanson, 1993). For example, when individuals reflect on emotional memories, they typically adopt a self-immersed perspective in which they visualize their experience happening all over again through their own eyes. However, it is also possible for people to analyze their experiences by adopting a self-distanced perspective in which they see themselves in the event from afar, akin to a “fly on the wall” peering down on the scene.
A number of recent studies performed with healthy children (Kross, Duckworth, Ayduk, Tsukayama, & Mischel, 2011), adult (Kross, 2009; Kross & Ayduk, 2011), subclinical (Kross & Ayduk, 2009; Wisco & Nolen-Hoeksema, 2011), and clinical (Kross, Gard, Deldin, Clifton, & Ayduk, 2012) populations have indicated that people who adopt a self-distanced (vs. self-immersed) perspective—either because they are instructed to do so in the context of an experiment or because they spontaneously engage in this process—are buffered against the harmful consequences of analyzing negative experiences. That is, they display lower levels of negative emotional and physiological reactivity and engage less in maladaptive rumination (for reviews, see Ayduk & Kross, 2010a; Kross, 2009; Kross & Ayduk, 2011).
Recent work has extended these findings by focusing on the role that self-distancing plays in positive emotion regulation. In one line of work, Verduyn, Van Mechelen, Kross, Chezzi, and Van Bever (2012) used experience-sampling methods with an unselected sample of young adults to examine the relationship between spontaneous self-distancing and daily positive mood intensity and duration. Complementing prior research on self-distancing and negative emotion regulation, their results showed that reflecting on daily positive events from a self-distanced perspective led to shorter and less intense positive mood episodes. More germane to the present study, Gruber, Harvey, and Johnson (2009) found that individuals with BD were capable of reflecting on positive emotional experiences from a self-distanced perspective when they were instructed to do so. Moreover, they demonstrated that doing so led to reductions in both self-report and physiological positive emotional reactivity. It is important to note that in the Gruber et al. study, the self-distancing manipulation led to equivalent reductions in positive emotional reactivity for both people with BD and healthy individuals, which suggests that self-distancing may play an equally effective role of facilitating positive emotion regulation in both groups.
Taken together, these studies highlight the role that self-distancing plays in allowing normal healthy and clinical populations to reflect adaptively on intense positive and negative emotional experiences in ways that minimize emotional reactivity and duration. However, they leave open an important question concerning whether people with BD display heightened positive emotional reactivity because they do not spontaneously self-distance sufficiently when they reflect on positive memories. The first goal of the present research was to address this issue.
Psychosis and Emotion Regulation in BD
Our second goal in the current work was to examine whether a history of psychosis influences the tendency of individuals with BD to spontaneously self-distance. Researchers have increasingly begun to examine the role that psychosis history plays in BD to enhance understanding of the heterogeneity of this disorder in terms of symptom severity, clinical course, and other illness characteristics, such as age of onset and comorbidity (Aminoff et al., 2013; Delgado & Chaves, 2013; Mazzarini et al., 2010; Ryu, Song, Hab, Ha, & Cho, 2012).
Approximately 50% to 70% of people with BD experience psychotic symptoms at some point during their lifetime (Goodwin & Jamison, 1990; Keck et al., 2003). Recent work has suggested that those with (vs. without) psychotic symptoms are genetically distinguishable (Pearlson et al., 1995; Potash et al., 2003) and are characterized by more severe illness courses, including earlier illness onset (Bellivier, Golmard, Henry, Leboyer, & Schurhoff, 2001), higher lifetime frequency of manic episodes (Tohen et al., 2003), and slower illness recovery times (Brockington, Hiller, Francis, Helzer, & Wainwright, 1983).
Emerging evidence has also suggested that a history of psychosis in BD is linked to a range of neuropsychological deficits that are related to BD, including impaired executive functioning (Glahn et al., 2007), learning (Martinez-Aran et al., 2008), visual processing (Albus et al., 1996), and memory recall (Simonsen et al., 2011; see Bora, Yücel, & Pantelis, 2010, for a meta-analysis on this topic). With respect to emotion regulation in BD, this is especially important, given that known deficits in cognitive functioning (especially executive functioning) affect emotion regulation (Gyurak et al., 2009; Gyurak, Goodkind, Kramer, Miller, & Levenson, 2012).
Despite these findings, relatively little is known about how a history of psychosis influences emotional processing in BD. One recent study (Anticevic et al., 2013) demonstrated that individuals with BD showed fronto-limbic dysfunction, indexed by reduced connectivity within medial prefrontal cortex (mPFC) and its connectivity abnormalities with limbic structures, which is likely to be responsible for emotion dysregulation in BD (Phillips, Ladouceur, & Drevets, 2008). It is important that this effect was driven by those individuals with a history of psychosis, which suggests that these individuals may be more vulnerable to emotion dysregulation than those without a history of psychosis. Yet no research that we are aware of has directly compared these two BD subgroups in their capacity to regulate positive emotion or examined the psychological mechanisms that underlie differences in the way the subgroups process emotional information.
Our second goal was to address these issues by exploring whether a history of psychosis influences people’s ability to regulate positive emotions via self-distancing. In particular, we explored whether a history of psychosis impairs the capacity of individuals with BD to spontaneously self-distance while reflecting on positive memories, compared with those without a history of psychosis and with healthy individuals.
Research Overview
We addressed these issues by recruiting individuals with BD, both with (n = 25) and without (n = 16) a history of psychosis, and healthy control participants (n = 20). To induce positive emotions, we asked participants to reflect on a positive autobiographical memory. We used idiosyncratic memories because the imagery component of emotional memories tends to amplify manic responses in people with BD (Holmes, Geddes, Colom, & Goodwin, 2008; Holmes & Mathews, 2010). We thus expected that asking participants to reflect on positive emotional memories would simulate more closely the types of emotional experiences that are associated with BD in everyday life. While participants reflected on their positive memories, we continuously monitored their brain activity via electroencephalogram (EEG). At the end of the study, we asked participants to rate (a) the extent to which they spontaneously self-distanced while reflecting on their positive memories and (b) their current level of positive emotions.
Emerging evidence has suggested that increased EEG activity in frontal regions of the left (vs. the right) hemisphere indicates both a trait- and a state-level propensity to engage a stimulus, including heightened positive emotional reactivity (for a review, see Coan & Allen, 2004). Importantly, Harmon-Jones et al. (2008) found that individuals with BD, compared with healthy control participants, exhibited increased relative left frontal cortical activation to positive challenges (i.e., performing a challenging task to obtain reward vs. performing the same task to avoid punishment), thereby demonstrating their stronger approach motivation to positive stimuli. Thus, we focused on relative left frontal activity in this study as a neurophysiological index of positive emotional reactivity.
Method
Participants
Forty-one individuals diagnosed with BD (24 females, 17 males; mean age = 41.49, SD = 10.23) and 20 healthy control participants (10 females, 10 males; mean age = 37.10, SD = 13.23) with no lifetime Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM–IV; American Psychiatric Association, 1994) Axis I diagnosis participated in this study in exchange for compensation of $15 per hr. All participants were right-handed and had normal or corrected-normal vision.
Participants were a subset of those who were recruited for a larger longitudinal study and had provided written consent to participate in future studies. They were recruited through an outpatient specialty psychiatry clinic, an inpatient psychiatric unit, and community advertisements on the Web, in the newspaper, on the radio, and on billboards. The Diagnostic Interview for Genetic Studies (DIGS; Nurnberger et al., 1994) was administered to confirm BD diagnosis and no current or past DSM–IV Axis I psychiatric diagnosis of healthy control participants. Final diagnoses were determined through a best-estimate process, which two psychiatrists and clinical psychologists performed using clinical interviews and, when available, medical-record data. 1
To evaluate mood state at the time of participation, we assessed depressive and manic symptoms with the Beck Depression Inventory (BDI; Beck, Ward, Mendelson, Mock, & Erbaugh, 1961) and the Altman Self-Rating Mania Scale (ASRM; Altman, Davis, Hedekar, & Peterson, 1997), respectively. For the BD group, 18 (43.9%) were euthymic (BDI < 14; ASRM < 6), 9 (22.0%) were hypomanic/manic (BDI < 14; ASRM ≥ 6), 8 (19.5%) were depressed (BDI ≥ 14; ASRM < 6), and 2 (4.9%) were mixed (BDI ≥ 14; ASRM ≥ 6). The mood state of 4 BD participants (9.8%) was unknown because 2 did not complete both scales and 2 additional participants did not complete the ASRM. All healthy control participants scored below the clinical cutoffs on both the BDI (< 14; M = 0.55, SD = 1.23) and the ASRM (< 6; M = 1.20, SD = 1.96).
The average age at onset of BD was 17.63 years (SD = 7.50); the average illness duration was 23.85 years (SD = 12.47). Thirty-seven BD participants (90.2%) were taking at least one psychotropic medication (M = 1.98, SD = 1.11), including mood stabilizer (63.4%), antidepressants (61.0%), antipsychotics (39.0%), and lithium (34.1%). As is common among individuals with BD, 14 (34.1%) had at least one additional current comorbid Axis I disorder (M = 0.41, SD = 0.59), including panic disorder (12.2%), agoraphobia (2.4%), social phobia (9.8%), specific phobia (4.9%), obsessive-compulsive disorder (4.9%), posttraumatic stress disorder (2.4%), and attention-deficit/hyperactivity disorder (2.4%), but for these participants, the primary diagnosis was confirmed as BD (Di Nardo, Moras, Barlow, Rapee, & Brown, 1993).
Among the BD group, 24 (58.5%) had at least one current and past diagnosis of substance abuse or dependence (M = 1.28, SD = 1.56), including abuse of or dependence on alcohol (39.0%), cannabis (36.6%), cocaine (9.7%), opiate (9.7%), sedative (7.3%), stimulant (2.4%), and others (17.1%). One healthy control participant (5%) had a past diagnosis of nicotine dependence. Five BD participants (12.2%) and 1 healthy control participant (5%) were current smokers.
The BD group was further categorized into participants with (i.e., psychotic BD; n = 25, 61.0%) or without (i.e., nonpsychotic BD; n = 16, 39.0%) a history of psychosis on the basis of the criterion used in the vast majority of the current literature on BD (e.g., Bora et al., 2010; Glahn et al., 2007; Savitz, van der Merwe, Stein, Solms, & Ramesar, 2009). Specifically, the lifetime history of experiencing psychosis, such as hallucinations, delusions, or grossly disorganized thoughts or behaviors, was assessed through the structured diagnostic interview (DIGS) and review of medical records when available and was confirmed through the best-estimate process by two doctoral-level clinicians. When the best estimators were not certain about the presence of psychosis history, we categorized participants on the basis of their self-reported experience of psychotic symptoms assessed during the DIGS interview. There were 3 such BD participants who endorsed experiencing psychotic symptoms. These participants were included in the psychotic BD group for further analyses. 2 Among the 25 BD participants with a history of psychosis, 14 (56.0%) experienced hallucinations, 19 (76.0%) experienced delusions, and 2 (8.0%) experienced grossly disorganized thoughts and behaviors. None of the BD participants had chronic psychosis or psychosis outside of 2 weeks of each mood episode.
BD participants with and without a history of psychosis did not differ in any of their clinical and health characteristics, including their age at onset of BD, illness duration, number of medications, comorbidity, past or current diagnoses of substance abuse/dependence, and smoking status (ps > .28), except that those individuals with a history of psychosis were less depressed (BDI = 7.71) than were those without a history of psychosis (BDI = 13.47), F(1, 37) = 7.16, p < .05, η p 2 = .16. The subgroups did not differ in their manic symptoms (psychotic BD: ASRM = 4.41; nonpsychotic BD: ASRM = 2.93), F(1, 35) = 1.58, p = .22. Table 1 illustrates demographic variables and clinical and health characteristics of the study participants.
Demographic Variables, Current Mood State, and Clinical and Health Characteristics of Study Participants
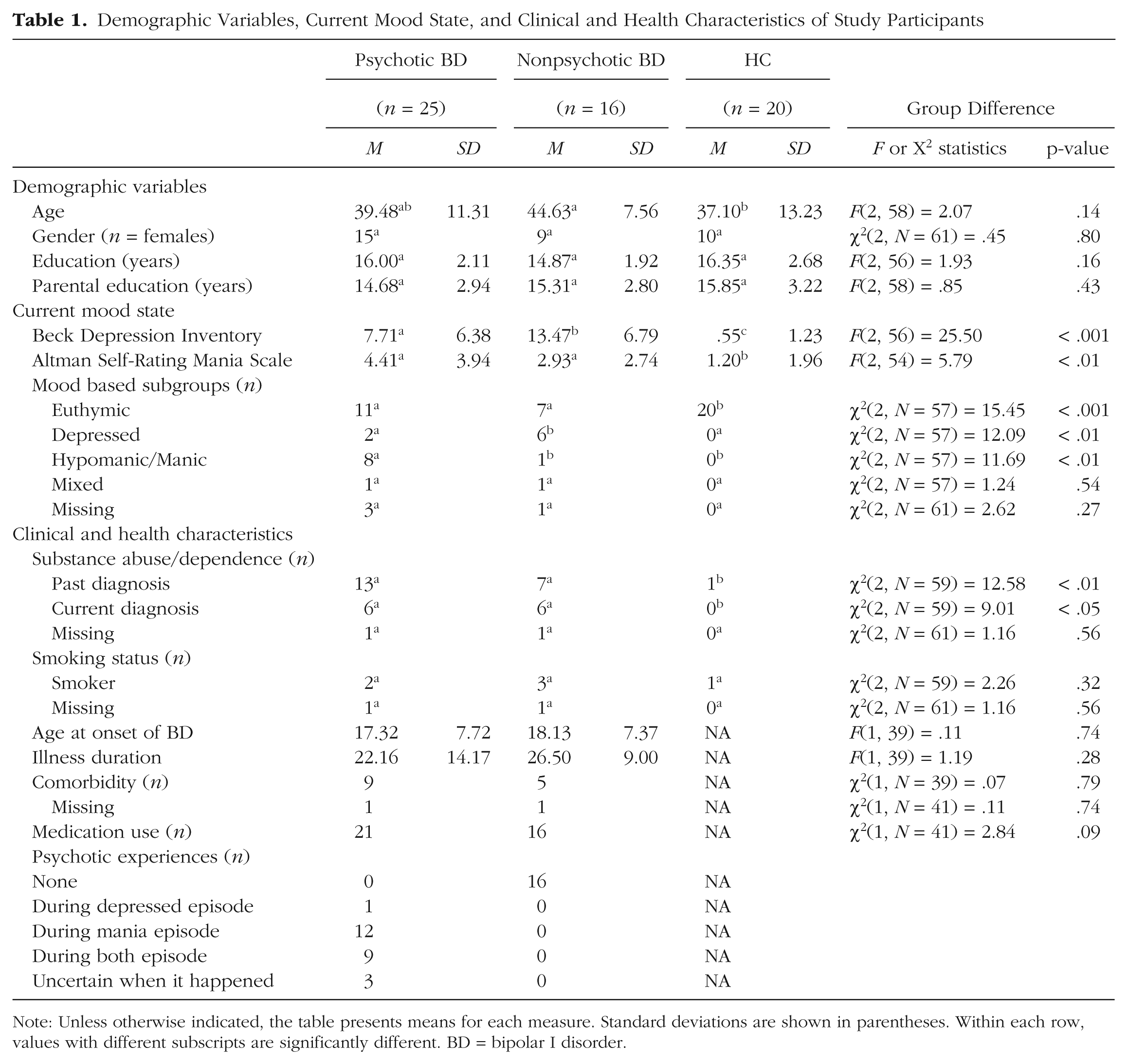
Note: Unless otherwise indicated, the table presents means for each measure. Standard deviations are shown in parentheses. Within each row, values with different subscripts are significantly different. BD = bipolar I disorder.
Procedure
The study proceeded in seven phases.
Phase 1: Baseline affect
First, participants rated how happy they felt “right now” using the Valence subscale of the Self-Assessment Manikin (Bradley & Lang, 1995). Participants responded to the item using a scale from 1 (very unhappy) to 9 (very happy; M = 6.36, SD = 1.34).
Phase 2: Baseline EEG
Next, participants were told that their brain activity would be noninvasively monitored using EEG. After the attachment of the electrodes, baseline EEG was recorded during both an eyes-open and an eyes-closed resting period for 3 min each, with the order of the two counterbalanced across participants (see Physiological Recording and Processing section for more details on EEG recording).
Phase 3: Positive memory reflection task
After the baseline EEG recording was obtained, participants completed a positive-memory-reflection task while we continuously monitored their EEG activity. Following a modified version of established procedures (Ayduk & Kross, 2010b; Grossmann & Kross, 2010), we asked participants to recall an experience from their past in which they felt extreme joy and happiness (recall time: M = 34.22 s, SD = 68.72). Next, they were asked to reflect on the emotions they experienced during the event for 90 s (Reflection 1). To allow a wider window of brain responses during the reflection period, we extended the standard reflection period duration by another 90 s. During the second reflection phase (Reflection 2), participants were asked to continue to focus on the causes and reasons underlying their feelings surrounding the event for another 90 s (see Appendix A for the task instructions).
Phase 4: Spontaneous self-distancing
Following prior research (Kross et al., 2014; Mischowski, Kross, & Bushman, 2012), we used two items to assess spontaneous self-distancing. First, we had participants rate the extent to which they adopted the perspective of an immersed participant (i.e., “saw the event replay through my own eyes, as if I were right there . . .”) versus a distanced observer (i.e., “watched the event unfold from the perspective of an observer, in which I could see myself from afar . . .”) as they pondered their deepest thoughts and feelings during the task. Responses were made on a scale from 1 (predominantly immersed participant) to 7 (predominantly distanced observer). Next, we had participants rate how far they were from the scene in their mind’s eye during the task; responses were made on a scale from 1 (very close, saw it through my own eyes) to 7 (very far, saw it as if an observer). These ratings were averaged to create a single self-distancing index (α = .90; M = 3.00, SD = 1.52). Because self-distancing scores were significantly nonnormal, D(61) = .17, p < .001, Kolmogorov-Smirnov test, they were log-transformed.
Phase 5: Self-reported positive emotion
Subsequently, participants completed three measures of positive emotion. First, participants again rated how happy they felt “right now” using the Self-Assessment Manikin (1 = very unhappy, 9 = very happy; M = 6.85, SD = 1.38). Second, participants’ global positive affect was assessed with the Positive Affect subscale of the Positive and Negative Affect Schedule (PANAS; Watson, Clark, & Tellegen, 1988). Using a 5-point scale ranging from 1 (very slightly or not at all) to 5 (extremely), participants rated the extent to which they felt 10 positive emotions (e.g., excited, active; α = .85; M = 3.02, SD = 0.77). Third, following prior work (Ayduk & Kross, 2010b; Grossmann & Kross, 2010), we directly examined emotional reactivity surrounding participants’ recalled experiences by averaging their agreement with the following two items to create an index of event-specific emotional reactivity: “I re-experienced the emotions I originally felt during the event when I thought about it now,” and “As I think about this event now, my emotions and physical reactions are still intense.” Participants responded using scales from 1 (strongly disagree) to 7 (strongly agree; α = .90; M = 4.77, SD = 1.35).
Phase 6: Stream of thoughts
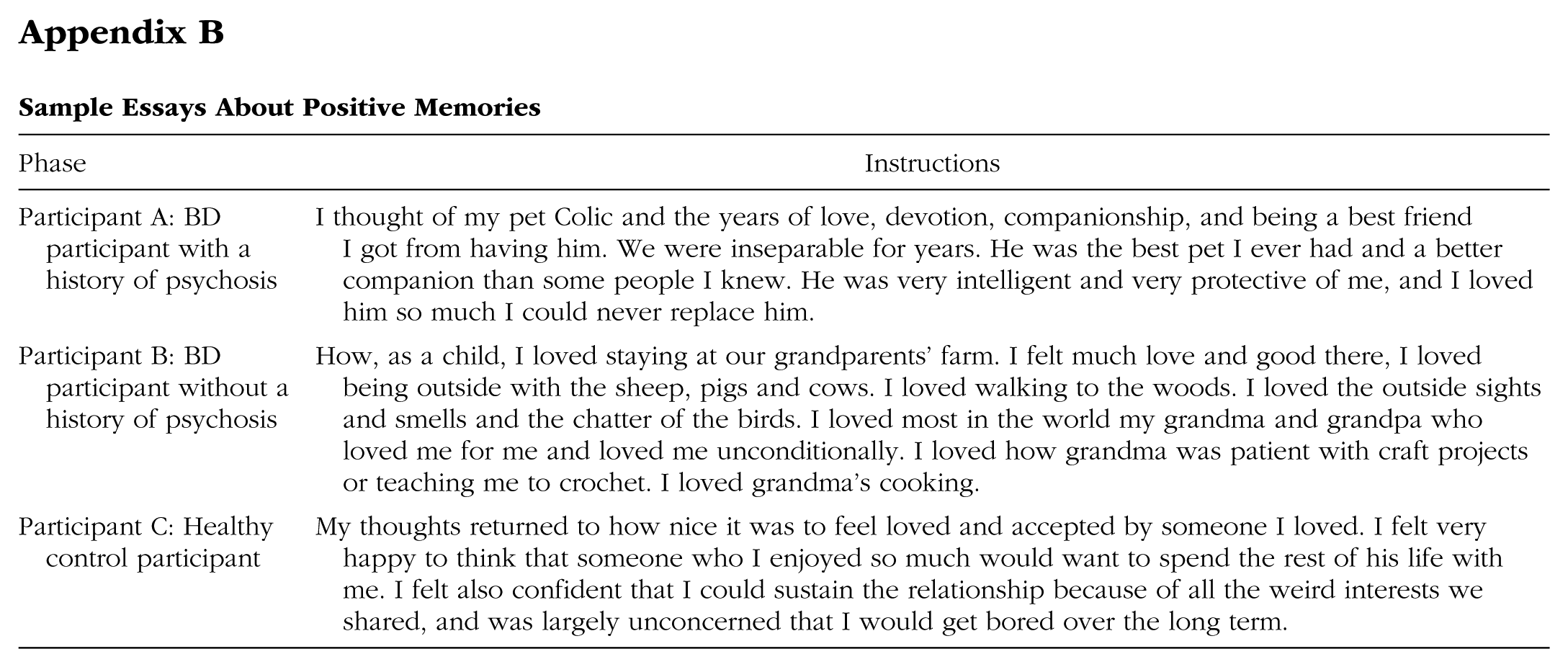
Next, participants were asked to describe in writing the thoughts and feelings that flowed through their mind as they thought about their positive experience during the memory-reflection task. These essays were used to examine whether participants recalled qualitatively different types of positive memories or memories that varied in their degree of positive emotional content. Sample essays are presented in Appendix B. We analyzed the essays in two ways. First, following a modified version of established procedures (Ayduk & Kross, 2010b; Grossmann & Kross, 2010; Kross et al., 2005), we had the essays rated by two independent coders, who were blind to each participant’s diagnosis, in terms of the extent to which positive emotions were described in each essay (0 = not at all, 3 = a great deal). The two coders’ ratings were averaged to create a single index of emotionality (intraclass correlation = .77; M = 2.19, SD = 1.00). Second, the essays were analyzed with the Linguistic Inquiry and Word Count (Pennebaker, Booth, & Francis, 2007), which yielded the percentage of positive emotion words written by participants (e.g., happy, excited; M = 10.82, SD = 15.24).
Phase 7: Positive memory characteristics
Previous research has indicated that the farther in the past a memory occurred, the more people self-distance and the less emotion they display when they think about the memory (Nigro & Neisser, 1983; Robinson & Swanson, 1993). Therefore, following prior work (Ayduk & Kross, 2010b; Park, Ayduk, & Kross, 2013), we asked participants to indicate when their experience occurred (memory age: M = 3,699.03 days, SD = 4,384.83) and controlled for this variable in all analyses. Because the distribution of memory age did not follow normal distribution, D(61) = .23, p < .001, Kolmogorov-Smirnov test, these data were log-transformed before analyses.
Physiological recording and processing
EEG was recorded with 32 electrodes placed in a nylon cap according to the International 10/20-System with FCz as a common ground reference. The electrooculogram was recorded from 2 additional channels placed beneath the left eye and at Fp1, respectively. EEG and electrooculogram signals were amplified with a band pass of 0.01 to 30 Hz by BrainCap MR-32 system (Brain Products GmbH, Gilching, Germany) and sampled with 512 Hz. Impedance for all electrodes was kept below 5kΩ. All data were rereferenced to the averaged M1 and M2 off-line and resampled at 250 Hz. The data were corrected for ocular artifacts (Gratton, Coles, & Donchin, 1983) and visually inspected to remove artifacts. When artifacts occurred in one channel, data from all channels were removed. All artifact-free epochs 1 s in duration were extracted through a Hamming window with 50% overlap to minimize data loss. The data were then subjected to a fast Fourier transform algorithm to calculate the power spectra. These power values were averaged across the 1-s epochs.
Recent findings have indicated that approach-related tendencies (e.g., enhanced positive emotional reactivity) captured via relative left frontal activity are greater for the alpha2 (10–13 Hz) band (e.g., Pizzagalli, Sherwood, Henriques, & Davidson, 2005). Therefore, we obtained total power within the alpha2 band. The power values (µV2/Hz) were log-transformed to normalize the distributions.
In the baseline EEG recording, we obtained two 3-min trials of resting EEG (eyes open and eyes closed). The log-transformed power values were averaged across the two trials using the weighted average following Tomarken, Davidson, Wheeler, and Kinney (1992). Specifically, the power value in each trial was multiplied by the number of artifact-free epochs for that trial (eyes open: M = 343.15, SD = 22.27; eyes closed: M = 324.86, SD = 90.00). These values were summed and divided by the total number of artifact-free epochs across trials. The epochs that belong to each phase of the reflection task were averaged to yield a mean power density value for each electrode site (recall: M = 58.80, SD = 137.41; Reflection 1: M = 169.31, SD = 15.06; Reflection 2: M = 168.55, SD = 16.50).
Finally, asymmetry indices were computed for each phase (baseline, recall, Reflection 1, and Reflection 2) by subtracting the log-transformed alpha power on the left site from the log-transformed alpha power on the right site. Given that alpha power is inversely related to brain activity (e.g., Davidson, Chapman, Chapman, & Henriques, 1990), higher numbers in these indices indicate stronger left (vs. right) cortical activity. On the basis of past research showing stronger effects at F7/F8 (e.g., Harmon-Jones & Sigelman, 2001), we focused our primary analysis on this region, with C3/C4 and P3/P4 as comparison sites.
Results
Attrition
Six participants’ EEG data were not analyzable because of an experimenter error (3 participants with psychotic BD and 3 healthy control participants). All other analyses used the total sample.
Analyses overview
We first examined whether the entire BD group, regardless of their psychosis history, differed from the healthy control group on any of the outcome variables we assessed. We found no group differences (Fs < 1.91, ps > .15). Therefore, we subsequently split participants with BD into two subgroups—psychotic BD and nonpsychotic BD—and compared both of these subgroups with each other and the healthy control group using a combination of omnibus analyses of covariance (ANCOVAs) and follow-up planned comparisons. This analytic strategy allowed us to test our a priori predictions concerning the role that a history of psychosis plays in BD.
Preliminary analyses
We conducted a series of preliminary analyses to address potential confounding factors. First, the types of positive memories participants recalled included pleasant memories with friends or family (37.7%), experiences in which participants felt loved by a romantic partner (19.7%), achievement of life goals (9.8%), and others (32.8%; e.g., giving birth, a religious experience). This variable did not differ across the groups, χ2(6, N = 61) = 5.33, p = .50. Content analyses of participants’ essays on the basis of both the coding data and the linguistic analysis index also confirmed that participants recalled memories that did not vary in their degree of positive emotional content (Fs < 1.88, ps > .16).
Next, we analyzed whether baseline affect, task order, or participants’ gender influenced any of the outcome variables. Participants did not differ in their baseline affect across the groups (F < 1, n.s.), and neither this variable nor the order of the baseline EEG trials (eyes open first vs. eyes closed first) interacted with group to predict any outcome variable (Fs < 2.21, ps > .12). However, we found a trend toward a gender effect on self-distancing, with females distancing more than males (females: 3.32; males: 2.59), F(1, 59) = 3.61, p = .06, η p 2 = .06. Therefore, gender was included as an additional covariate in the analysis involving self-distancing. There was no effect of gender on the rest of the outcome variables (Fs < 2.15, ps > .14).
We also examined whether mood symptoms influenced the BD subgroup differences we observed. The two subgroups did not differ on their manic symptoms (psychotic BD: ASRM = 4.41; nonpsychotic BD: ASRM = 2.93), F(1, 35) = 1.58, p = .22, but BD participants with a history of psychosis were less depressed than those without a history of psychosis (psychotic BD: BDI = 7.71; nonpsychotic BD: BDI = 13.47), F(1, 37) = 7.16, p < .05, η p 2 = .16. Neither depressive symptoms nor manic symptoms predicted any of our dependent variables (rs < −.21, ps > .10). In addition, controlling for depressive or manic symptoms did not substantively alter any of the results we report.
Finally, the two BD subgroups did not differ on any of their clinical and health characteristics, including the number of medications (psychotic BD: 1.84; nonpsychotic BD: 2.19), F(1, 39) < 1, n.s., comorbidity, past or current diagnoses of substance abuse or dependence, or smoking status, χ2s(1, N = 39) < 1.12, ps > .28, and controlling for these variables did not influence any subgroup differences we report later. Thus, we do not discuss these variables further.
Spontaneous self-distancing
We predicted that BD participants would spontaneously self-distance less than healthy control participants when they reflected on their positive memories. We further predicted that this group difference would be more pronounced among BD participants with a history of psychosis. To test these predictions, we compared the three groups (psychotic BD vs. nonpsychotic BD vs. healthy control) using ANCOVA with group as a between-subjects factor and memory age and gender as covariates.
The effect of group was significant, F(2, 56) = 3.86, p < .05, η p 2 = .12. As Figure 1 illustrates, BD participants with a history of psychosis self-distanced less (0.33) than did both those without a history of psychosis (0.53), F(1, 56) = 7.37, p < .01, η p 2 = .12, and healthy control participants (0.44), F(1, 56) = 2.70, p = .10, η p 2 = .05, although the latter effect fell short of conventional standards of statistical significance. The latter two groups did not differ (F = 1.24, p = .27).
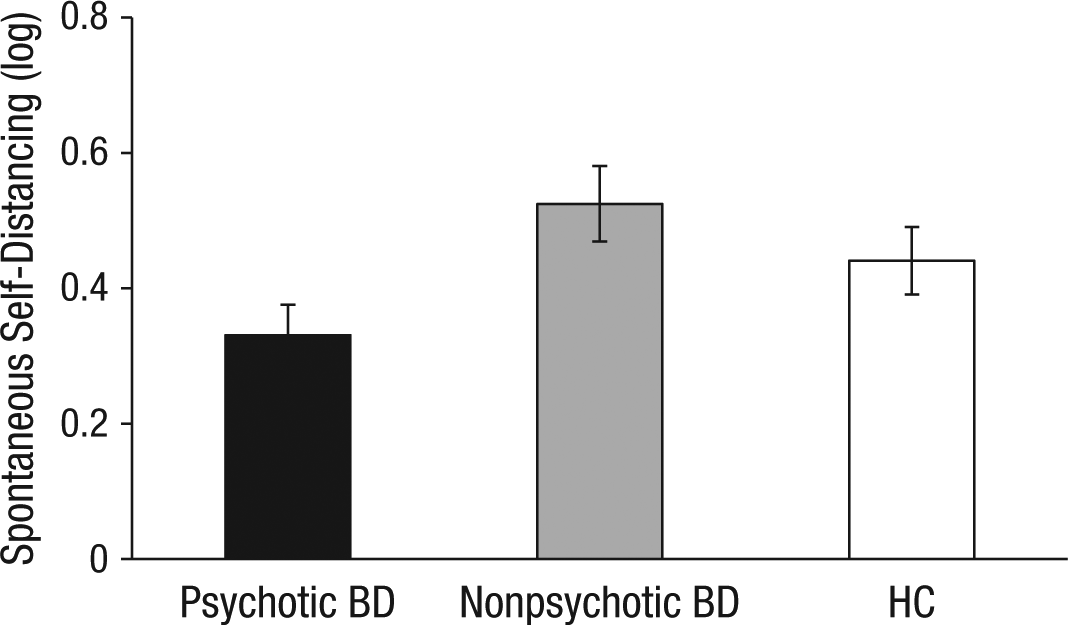
Group differences in spontaneous self-distancing. Memory age and gender were controlled. Error bars represent standard errors. BD = bipolar I disorder. HC = healthy control participants.
Neural signals of emotional reactivity
Next, we examined whether the pattern of results we observed for spontaneous self-distancing across the three groups was mirrored in the neurophysiological signals of emotional reactivity that we assessed.
To examine group differences in neurophysiological reactivity, we conducted a 3 (Group) × 4 (Phase: baseline vs. recall vs. Reflection 1 vs. Reflection 2) repeated measures ANCOVA on the asymmetry index on F7/F8 with group as a between-subjects factor, phase as a within-subjects factor, and memory age as a covariate. There was no main effect of group, F(2, 51) = 1.30, p = .28. But the Group × Phase interaction was significant, F(6, 153) = 2.49, p < .05, η p 2 = .09. As Figure 2a illustrates, this interaction shows that the three groups displayed distinct profiles of brain responses across the task. 3

Group differences in relative left (vs. right) cortical activity (F7/F8) in the four task phases (a) and the two reflection phases (b). Memory age was controlled for in the four task phases, and memory age and baseline EEG were controlled for in the two reflection phases. Error bars represent standard errors. BD = bipolar I disorder. HC = healthy control participants.
Specifically, BD participants with a history of psychosis showed a steady increase in their relative left frontal activity during the task. When they reached the second reflection period, their activity was significantly higher than at baseline (0.36 vs. 0.08), t(20) = 2.05, p = .05, r = .42. In contrast, BD participants without a history of psychosis showed a similar profile of increasing relative left frontal activity until they peaked at the first reflection period (0.37), but they then displayed a significant drop during the second reflection period (−0.19), t(14) = 3.49, p < .01, r = .68, which resulted in a significant quadratic effect for the Group × Phase interaction, F(2, 51) = 3.15, p = .05, η p 2 = .11. Although healthy control participants showed a tendency to decrease their relative left frontal activity from recall (−0.04) to the first reflection period (−0.12), this effect, as well as the changes in other phases, was not significant, ts(15) < 1.63, ps > .12.
Given that the group differences in the relative left frontal activities were evident during the two reflection phases, Reflection 1: F(2, 51) = 3.07, p = .05, η p 2 = .11; Reflection 2: F(2, 51) = 4.21, p < .05, η p 2 = .14, but not during baseline and recall, Fs < 1, n.s., we next conducted a 3 (Group) × 2 (Phase: Reflection 1 vs. Reflection 2) ANCOVA with baseline EEG and memory age as covariates to better understand the group differences during reflection—the critical phase of the experiment.
This analysis revealed a significant Group × Phase interaction, F(2, 50) = 5.52, p < .01, η p 2 = .18 (see Fig. 2b). This interaction indicated that BD participants without a history of psychosis showed a significant reduction in their activity from the first reflection period (0.37) to the second reflection period (−0.19), t(13) = 3.38, p < .01, r = .68, whereas those with a history of psychosis maintained elevated activity and displayed no change from the first reflection period (0.28) to the second reflection period (0.36), t(19) < 1, n.s. During the reflection period overall, healthy control participants remained consistently low in their activity (−0.02) compared with BD participants with a history of psychosis (0.33), F(1, 50) = 4.89, p < .05, η p 2 = .09. BD participants without a history of psychosis fell in between the two groups (0.08), but they did not significantly differ from the other two (Fs < 2.40, ps > .12).
Additional analyses confirmed that the group differences were evident in frontal sites (F7/F8), consistent with results from prior work (e.g., Harmon-Jones & Sigelman, 2001). 4 There was no comparable effect of Group × Phase interaction in the comparison regions C3/C4 and P3/P4, Fs < 1.50, ps > .18, which resulted in a significant Group × Phase × Region three-way interaction effect, F(12, 306) = 1.88, p < .05, η p 2 = .07.
Subjective indices of emotional reactivity
We then examined the effect of group on three measures of emotion. First, we performed a 3 (Group) × 2 (Time: baseline vs. after reflection task) repeated measures ANCOVA on happiness with group as a between-subjects factor, time of happiness measurement as a within-subjects factor, and memory age as a covariate. This analysis revealed a significant main effect of time, F(1, 57) = 4.59, p < .05, η p 2 = .07. Participants felt happier after recalling their positive memories (6.80) compared with at baseline (6.32), which indicated that our affective manipulation was successful. However, contrasting sharply with the neural data, results showed that there was no significant effect of group or its interaction with time (Fs < 1.39, ps > .25). Similarly, global positive affect and event-specific emotional reactivity did not differ across the groups (Fs < 1, n.s.).
Spontaneous self-distancing and emotional reactivity
Finally, we conducted a series of regression analyses to examine the relationship between self-distancing and our neural and self-report measures of emotional reactivity. 5 As predicted, self-distancing correlated negatively with all three self-report measures of emotion—happiness: b = −0.36, t(56) = −2.14, p < .05; global positive affect: b = −0.66, t(56) = −2.80, p < .01; event-specific emotional reactivity: b = −0.48, t(55) = −3.58, p < .001. Self-distancing was also negatively related to the relative left frontal activity during the first reflection period, b = −0.53, t(50) = −1.77, p = .08, although this relationship fell just short of conventional levels of statistical significance. These findings suggest that the more participants reported spontaneously self-distancing while reflecting on positive memories, the less emotional reactivity they displayed on both neural and self-report measures. There was no significant relationship between self-distancing and the relative left frontal activity during other task phases (ts < 1, n.s.).
Discussion
In the current research, we examined the role that spontaneous self-distancing plays in healthy individuals and two potentially different types of BD groups—those who have a history of psychosis and those who do not—to shed light on the cognitive and neural processes that underlie positive emotion regulation in BD. Our research generated two key findings.
First, we found that a history of psychosis modulated the way people with BD process idiosyncratic positive information at both the cognitive and the neural levels. Specifically, BD participants with a history of psychosis, compared with both healthy control participants and individuals with BD who were not characterized by a history of psychosis, displayed heightened neurophysiological signs of emotional engagement (i.e., relative left frontal activity) as they reflected on their positive memories. Our analyses of the essays participants wrote to describe their thoughts and feelings regarding their positive memories confirmed that the three groups recalled positive memories that did not vary in their degree of positive emotional content, thereby suggesting that BD participants with a history of psychosis, compared with the other two groups of participants, magnified their emotional response to the same type of emotional stimuli. These findings are also consistent with previous evidence that has indicated that people with BD, compared with healthy individuals, show increased approach motivation toward positive stimuli, such as reward, indexed by enhanced relative left frontal activity (Harmon-Jones et al., 2008). Our work extends this study by suggesting that such a tendency is primarily shown among those individuals with a history of psychosis when they respond to highly idiosyncratic positive emotional memories.
It is important to note that the differences between the two subgroups of BD were not explained by any clinical characteristics or mood symptoms. These findings suggest that a history of psychosis may modulate the way people with BD process not only cognitive information, which has been the focus of prior work, but also emotional information. More generally, they suggest that the psychotic and nonpsychotic forms of BD may represent distinct clinical phenotypes that are distinguishable on the basis of neurobiological and genetic factors (Pearlson et al., 1995; Potash et al., 2003; Strasser et al., 2005). Future research is needed to further examine this issue and is important for refining our understanding of BD.
Second, we found that BD participants without a history of psychosis resembled healthy control participants on their spontaneous self-distancing scores but differed from both healthy control individuals and people with BD who have a history of psychosis in terms of their neurophysiological reactivity. Specifically, BD participants without a history of psychosis showed a steady increase in their relative left frontal activity during the first phase of the reflection period, which indicated their high levels of emotional engagement (similar to participants with a history of psychosis). However, whereas participants with a history of psychosis continued to show high emotional engagement during the second reflection phase of the task, those without a history of psychosis displayed a sharp reduction in their relative left frontal activity during this phase of the task. It is not clear why participants without a history of psychosis showed such a disengagement tendency. 6 One interpretation of this finding is that this disengagement tendency indicates the attempt of participants in this group to regulate their positive emotions. This interpretation is consistent with recent evidence that has suggested that compared with people with BD who have a history of psychosis, those with BD who do not have a history of psychosis are characterized by less severe illness course, including lower lifetime frequency of manic episodes (Tohen et al., 2003) and faster illness recovery (Brockington et al., 1983). If true, this would explain why the self-distancing scores of BD participants without a history of psychosis—which were assessed immediately after the second reflection phase—resembled that of healthy control participants. This is, of course, a post hoc speculation; future research is needed to test this idea by assessing self-distancing repeatedly throughout the different phases of the reflection task.
It is important to emphasize that had we not used a methodology that allowed us to examine the temporal dynamics of neural responses, we would not have observed many of the differences detected among the three groups examined. This underscores the importance of using continuous measures of psychological and biological activities in BD research as well as clinical psychopathology research more generally.
Given prior research that has documented that healthy individuals show increased relative left frontal activity in response to positive stimuli, it seems puzzling that we did not observe any such responses among our healthy control participants. We speculate that the discrepancy between previous studies and our finding is likely due to the type of positive mood induction we used. We used emotional memories to induce positive emotions because they facilitate mental imagery of emotional scenes (Arntz, de Groot, & Kindt, 2005), which, in turn, is likely to amplify emotional responses in people with BD (Holmes et al., 2008; Holmes & Mathews, 2010). Conversely, previous studies that have revealed increased relative left frontal activity in healthy individuals typically used emotionally evocative stimuli, such as films (Davidson, Ekman, Saron, Senulis, & Friesen, 1990; Ekman, Davidson, & Friesen, 1990; Jones & Fox, 1992; Wheeler, Davidson, & Tomarken, 1993) or images (Davidson, Schaffer, & Saron, 1985; Hagemann, Naumann, Becker, Maier, & Bartussek, 1998), to induce positive emotions, which may have had a stronger effect compared with asking participants to reflect on past emotional memories. Future research should explore this issue further by comparing emotional reactivity in response to different positive mood induction procedures among people with BD (both with and without a history of psychosis) and healthy control individuals.
Several limitations of the current work should be noted. First, although we observed a consistent pattern of results on the neurophysiological and self-distancing measures we administered, we did not detect a similar set of significant results for self-report emotional reactivity. Although unexpected, the asymmetry we observed between participants’ responses on our physiological and self-report emotional-reactivity measures is consistent with research indicating that self-report measures of emotion often do not cohere with physiological responses (e.g., Lang, Bradley, & Cuthbert, 1998; Lang, Greenwald, Bradley, & Hamm, 1993). Further research is needed to more fully understand the dissociation between different types of emotional-reactivity measures.
Another issue that was left unaddressed is the cognitive mechanism that differentiates the two BD subgroups, especially during the second reflection phase when they displayed distinct neurophysiological signals. Future research should directly assess self-distancing as well as other potential emotion regulatory processes (e.g., reappraisal or suppression; Gruber, Hay, & Gross, 2013) that BD participants without a history of psychosis may have engaged in during this later stage of emotional processing.
Finally, the current work focused on regulation of positive emotion in BD. Thus, it remains unclear whether the failure to spontaneously self-distance when reflecting on negative emotional experiences also plays a role in BD (both with and without a history of psychosis). Although prior research has indicated that self-distancing allows people to reflect adaptively over both positive and negative emotional experiences in a variety of samples, including healthy children (Kross et al., 2011), adult (Kross, 2009; Kross & Ayduk, 2011; Verduyn et al., 2012), subclinical (Kross & Ayduk, 2009; Wisco & Nolen-Hoeksema, 2011), and clinical (Gruber et al., 2009; Kross et al., 2012) populations, future research is needed to directly test whether people with BD, particularly those who have a history of psychosis, exhibit similar difficulties in engaging in this process while reflecting on negative experiences.
Concluding remarks
The current findings suggest that individuals with BD who have a history of psychosis may represent a distinct clinical phenotype that is characterized by dysfunctional positive emotion regulation—in particular, the inability to spontaneously self-distance while reflecting on positive emotional memories. Although future research is needed to more fully characterize the cognitive and neural mechanisms that distinguish such individuals from people with BD who do not have a history of psychosis, the current findings suggest that taking the next steps to address this issue is important from both a basic science and a clinical perspective.
Footnotes
Appendix
Sample Essays About Positive Memories
| Phase | Instructions |
|---|---|
| Participant A: BD participant with a history of psychosis | I thought of my pet Colic and the years of love, devotion, companionship, and being a best friend I got from having him. We were inseparable for years. He was the best pet I ever had and a better companion than some people I knew. He was very intelligent and very protective of me, and I loved him so much I could never replace him. |
| Participant B: BD participant without a history of psychosis | How, as a child, I loved staying at our grandparents’ farm. I felt much love and good there, I loved being outside with the sheep, pigs and cows. I loved walking to the woods. I loved the outside sights and smells and the chatter of the birds. I loved most in the world my grandma and grandpa who loved me for me and loved me unconditionally. I loved how grandma was patient with craft projects or teaching me to crochet. I loved grandma’s cooking. |
| Participant C: Healthy control participant | My thoughts returned to how nice it was to feel loved and accepted by someone I loved. I felt very happy to think that someone who I enjoyed so much would want to spend the rest of his life with me. I felt also confident that I could sustain the relationship because of all the weird interests we shared, and was largely unconcerned that I would get bored over the long term. |
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This study was supported by a grant from the Heinz C. Prechter Bipolar Research Fund at the University of Michigan Depression Center to M. G. McInnis, National Center for Research Resources Grant UL1RR024986 (now the National Center for Advancing Translational Sciences Grant 2UL1TR000433) to M. Kamali, and American Foundation for Suicide Prevention Young Investigator Grant YIG-xxxx-00176-1209 to M. Kamali.