
Abstract
Persistent fear and avoidance in patients with social anxiety disorder (SAD) has been associated with reduced testosterone levels. Because threat avoidance is a major maintaining factor in SAD, and because testosterone administration promotes social approach, we tested whether testosterone administration can directly facilitate threat approach behavior in SAD. In a double-blind, placebo-controlled study, 17 female participants with SAD received a single dose of testosterone before performing a well-established social Approach-Avoidance Task. This objective implicit measure of social motivational action tendencies requires participants to approach or avoid visually presented emotional faces. After testosterone administration, the patients showed increased approach tendencies to angry facial expressions. These results suggest that testosterone can counteract persistent automatic social avoidance tendencies in SAD. This finding advances our understanding of steroid involvement in the regulation of social motivational action in general and in SAD in particular, and may have important clinical implications, promoting testosterone’s candidacy for pharmacological treatment-enhancement studies.
Keywords
Social anxiety disorder (SAD) is the most common anxiety disorder, characterized by an intense fear of social situations in which the individual may be scrutinized by others (American Psychiatric Association, 2013). Avoidance behavior is one of the core characteristics of SAD and plays a crucial role in its persistence as it hinders extinction of fear in social situations (Clark & Wells, 1995). Previous work showed that women with SAD have reduced endogenous testosterone levels, which were also related to the severity of social phobia symptoms (Giltay et al., 2012). Despite mounting evidence for the social approach facilitating properties of testosterone administration (Enter, Spinhoven, & Roelofs, 2014; Terburg, Aarts, & van Honk, 2012), to date no studies have tested whether testosterone administration can alleviate actual social avoidance behavior in SAD.
Testosterone is important in the regulation of social motivational behavior, and enhances social approach motivation while reducing social fear in a socially challenging environment (Archer, 2006; Bos, Panksepp, Bluthe, & van Honk, 2012; Radke et al., 2015; Terburg & van Honk, 2013). Also in socially anxious individuals it can increase fixations to the eyes of emotional faces (Enter, Terburg, Harrewijn, Spinhoven, & Roelofs, 2016). Recently, we have shown that testosterone promotes actual social approach behavior in healthy women (Enter et al., 2014). After a single dose testosterone administration, the participants showed reduced automatic avoidance of social threat (i.e., angry facial expressions) and relative increased threat approach tendencies. Such effects would be of particular interest for SAD, as social avoidance is a major characteristic and an important factor in the persistence of the disorder. Therefore, testing whether testosterone can alleviate social avoidance tendencies in SAD would be of theoretical and clinical importance.
We set out to test whether testosterone administration promotes threat approach in SAD by using a well-established objective and implicit measure of social motivational behavior: the Approach-Avoidance Task (AAT; Heuer, Rinck, & Becker, 2007; Roelofs et al., 2010; Roelofs, Minelli, Mars, van Peer, & Toni, 2009; Roelofs, van Peer, et al., 2009; Volman, Roelofs, Koch, Verhagen, & Toni, 2011; Volman, Toni, Verhagen, & Roelofs, 2011). This reaction time task requires participants to approach and avoid socially aversive and appetitive visually presented stimuli (angry and happy faces, respectively) by pulling a joystick toward themselves (approach) or pushing the joystick away from themselves (avoidance). Angry faces with direct gaze constitute a potent threat stimulus that elicits avoidance responses, particularly in socially anxious individuals (Adams, Gordon, Baird, Ambady, & Kleck, 2003; Öhman, 1986; Roelofs et al., 2010).
Based on the approach-enhancing and social-anxiolytic role of testosterone in social motivational behavior, we predict that administration of testosterone to SAD participants would reduce threat avoidance and increase threat approach tendencies to angry faces on the AAT.
Method and Materials
Participants
Participants with SAD were recruited from outpatient anxiety departments of mental health centers and through advertisements on the Internet and in local newspapers. The inclusion criterion was a total score of 60 or higher on the Liebowitz Social Anxiety Scale (LSAS; Liebowitz, 1987), representing the cutoff score for the presence of SAD (Rytwinski et al., 2009). 1 In addition, participants were screened with the Mini International Neuropsychiatric Interview script (Lecubier et al., 1997) to determine the presence of a Diagnostic and Statistical Manual for Mental Disorders (4th ed.; DSM-IV) diagnosis of generalized SAD. Only female participants were included because there are as yet no known parameters (e.g., dose and time course) for inducing neurophysiological effects in men after administration of a single dose of testosterone cyclodextrin (Tuiten et al., 2000). Both women using single-phase contraceptives and normally cycling women participated in the study (Hermans et al., 2010). Exclusion criteria were younger than 18 and older than 50 years old, use of (psychotropic) medication, somatic illnesses, neurological conditions, psychotic disorder, current comorbid diagnosis of mood or anxiety disorders other than SAD, history of head injury, left-handedness, peri- or postmenopause, and pregnancy or breast feeding. After initial screening of 24 socially anxious participants, 17 participants fulfilled all DSM-IV criteria for generalized SAD at the time of testing and were selected for this study. This group had a mean age of 22.8 years (SD = 5.0) and a LSAS total score of 78.6 (SD = 14.3; see Table S1 in the Supplemental Material available online for additional participant characteristics). All participants had completed or were following higher education, had normal or corrected-to-normal vision, were unaware of the aim of the study, provided written informed consent, and received a financial compensation of €80 and a travel allowance. Data on ethnicity were not recorded. The study was approved by the Medical Ethics Committee of the Leiden University Medical Centre and was in accordance with the Declaration of Helsinki.
Testosterone administration
In a double-blind, randomized, placebo-controlled, crossover design, participants received a single dose of 0.5 mg testosterone suspended in a clear solution (0.5 ml) with 0.5 mg hydroxypropyl-beta-cyclodextrin, 0.005 ml ethanol 96%, and distilled water. The matched placebo contained the same ingredients, except testosterone. Participants were asked to hold the liquid under their tongue for 60 s. During sublingual administration of 0.5 mg testosterone with cyclodextrin as carrier, testosterone is directly absorbed into the bloodstream. In females, such a dose yields a sharp increase of 20 to 25 nmol/l in plasma testosterone levels within 15 min, which declines to baseline levels within the next 90 min (van Rooij et al., 2012). Pharmacodynamic effects are measurable approximately 4 to 6 hr after testosterone intake (Bos et al., 2012; Tuiten et al., 2000).
Approach-Avoidance Task
During this reaction time (RT) task, participants responded to happy, angry, and neutral facial expressions presented on a computer screen by pulling a joystick either toward their body (approach movement) or pushing it away from their body (avoidance movement). Pulling or pushing the joystick increased or decreased the size of the picture, respectively, giving the impression of moving toward or moving away from the participant. Usually, response latencies are shorter for affect-congruent (e.g., happy-approach; angry-avoid) as compared with affect-incongruent response conditions (e.g., angry-approach; happy-avoid). This task has previously been used by Enter and colleagues (2014). A detailed description is available in the Supplemental Material available online.
Procedure
Participants were tested individually at two identical testing sessions with 2 days in between. Testing sessions started at either 9:30 a.m. or 1:30 p.m., and participants were tested at the same time of day on both sessions. Participants performed the AAT in a dimly lit and sound attenuated room 4.5 hr after administration of testosterone or placebo. After completion of the two sessions, participants had to indicate in which session they thought to have had testosterone or placebo. Responses of 6 of the 17 participants were correct, which is at chance level, Binomial P(X = 6) = 0.094, confirming that participants were unaware of the condition. Before the first testing day the participants completed additional questionnaires, including the Dutch versions of the Beck Depression Inventory (Beck, Rush, Hollon, & Emery, 1979) and the Social Phobia and Anxiety Inventory (SPAI; Turner, Beidel, Dancu, & Stanley, 1989; see Table S1).
Statistical analyses
RT outliers were filtered using a less than 150 and greater than 1,500 ms cutoff. A cutoff of three standard deviations from the mean was used for defining outliers in the remaining RTs. Error rates were calculated after removal of outliers. For each participant, the median of the remaining RTs (91%) for the correct responses (RT1) was calculated per cell (defined by Emotion and Movement). Following Enter and colleagues (2014) AAT effect scores were computed for each participant and for each emotion separately by subtracting median pull RTs from corresponding median push RTs (e.g., RT angry push – RT angry pull; RT happy push – RT happy pull; RT neutral push – RT neutral pull). As a result, more negative AAT effect scores (push is faster than pull) reflect a relative avoidance tendency.
To test effects of testosterone administration on approach-avoidance tendencies to emotional faces, AAT effect scores were entered in a two-way repeated measures analysis of variance (rmANOVA) with condition (testosterone, placebo) and emotion (angry, happy, neutral) as within-subject factors. Greenhouse–Geisser correction was used when appropriate (uncorrected degrees of freedom are reported together with the correction factor epsilon [ε]). In addition, we tested whether AAT effect scores were significant in certain conditions (i.e., differed from zero) using one-sample t tests. Alpha was set at .05, and effect sizes are reported as partial eta-squared (η p 2). Finally, we checked whether avoidance behavior to angry faces in the placebo condition was associated with severity of social anxiety symptomatology by computing Spearman’s correlation coefficient between baseline corrected AAT effect scores and SPAI total scores.
Results
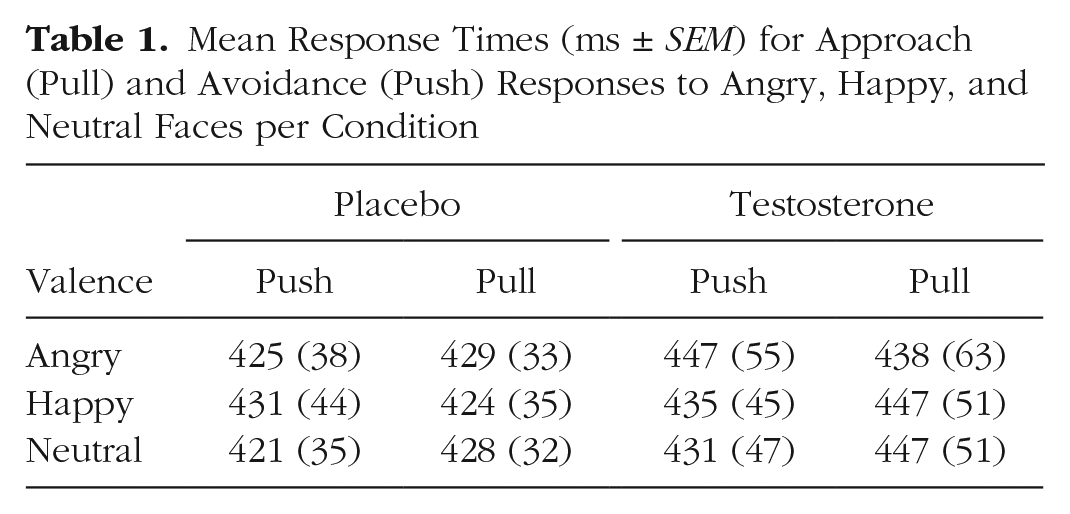
Table 1 provides an overview of the outcomes for RTs. The task was well performed, as indicated by low error rates (9%).
Mean Response Times (ms ± SEM) for Approach (Pull) and Avoidance (Push) Responses to Angry, Happy, and Neutral Faces per Condition
In line with our hypotheses, the two-way rmANOVA for the AAT effect scores, with Condition (Placebo, Testosterone) and Emotion (angry, happy, neutral) as within-subject factors, revealed a significant Condition × Emotion interaction, F(1.22, 19.5) = 4.95, p = .032, ε = .608, η p 2 = .236, and a significant effect of Emotion, F(1, 16) = 6.25, p = .024, η p 2 = .281. There were no significant Condition effects for each Emotion separately (all Fs < 2.6, ps > .13), but separate two-way rmANOVAs for each pair of emotions demonstrated a significant Condition × Emotion interaction for angry versus happy faces, F(1, 16) = 6.25, p = .024, η p 2 = .281, and for angry versus neutral faces, F(1, 16) = 4.61, p = .047, η p 2 = .224, but not for happy versus neutral faces, F(1, 16) = 0.561, p = .465, η p 2 = .034. As expected, these findings pointed toward a specific effect of testosterone on the AAT effect scores for angry faces, compared with happy and neutral faces. Indeed, when looking into each condition separately, one-way rmANOVAs for Emotion (angry, happy, neutral) revealed a significant effect for Emotion in the testosterone condition, F(1.43, 22.95) = 4.90, p = .026, ε = .717, η p 2 = .234, but not in the placebo condition, F(1.44, 23.0) = 1.22, p = .300, ε = .718, η p 2 = .071. Separate follow-up analyses for each pair of emotions showed that the AAT effect scores in the testosterone condition were markedly higher for angry faces compared with happy and neutral faces, by revealing a significant main effect of Emotion for angry versus happy, F(1, 16) = 6.94, p = .018, η p 2 = .303, and angry versus neutral, F(1, 16) = 16.14, p = .001, η p 2 = .502, but not for happy versus neutral faces, F(1, 16) = 0.098, p = .759, η p 2 = .006. Taken together, these results suggest a significant increase of approach tendencies toward angry faces by testosterone in SAD participants (see Fig. 1).
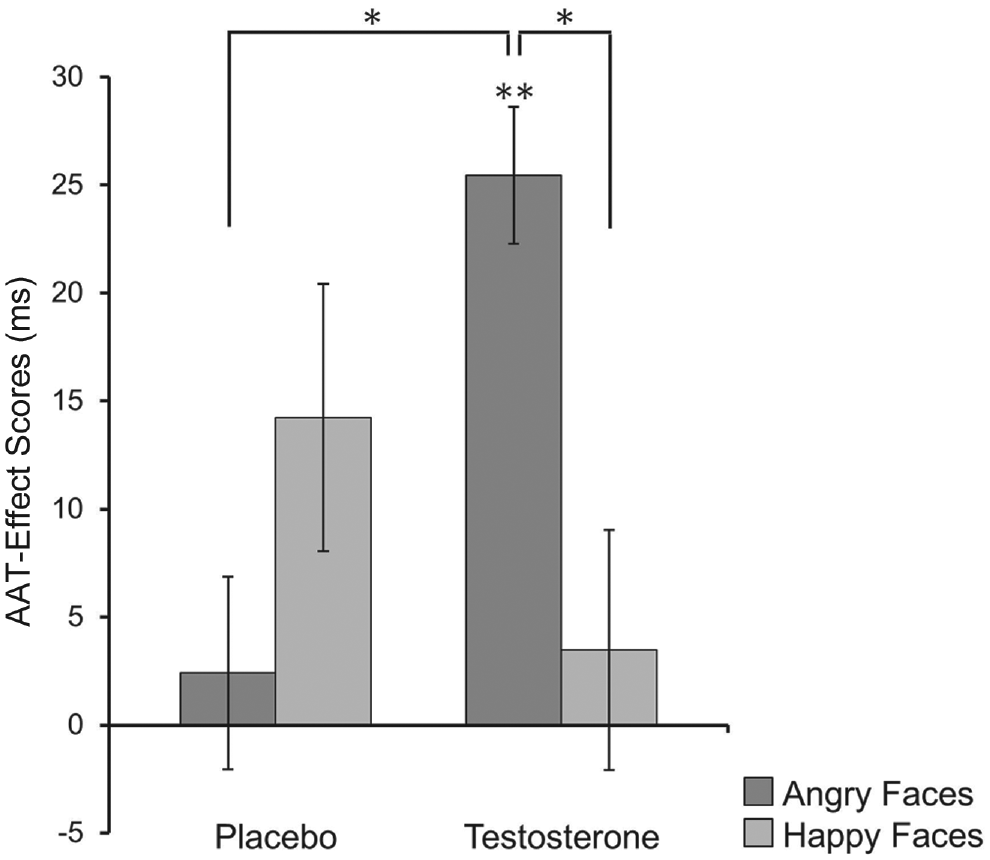
Mean Approach-Avoidance Task (AAT) effect scores (ms) for approach and avoidance movements to angry and happy faces in the placebo and testosterone condition. Participants show significant approach tendencies toward angry faces after testosterone administration, compared with happy faces. For display purposes, mean scores are baseline corrected (i.e., AAT effect scores for neutral faces subtracted from the AAT effect scores of angry and happy faces, respectively). Of note, baseline corrected AAT effect scores for angry faces showed a significant treatment effect, F(1, 16) = 4.61, p = .047, η p 2 = .224, and differed significantly from zero in the testosterone condition, t(16) = 4.02, p = .001, indicating threat approach. *p < .05. **p < .01.
Next we checked whether avoidance behavior to angry faces in the placebo condition was associated with social anxiety symptomatology. A significant negative correlation between the baseline corrected AAT effect scores and the SPAI scores, r = –.660, p = .004, indicated that those patients who had stronger avoidance tendencies also had more severe social anxiety symptoms. Social anxiety scores did not modulate the testosterone effects (SPAI: all Fs < 1.81, ps > .199). There were also no such effects when taking LSAS as symptom severity measure (all Fs < 0.757, ps > .398).
To test whether this threat-approach enhancing effect of testosterone is comparable to the effect previously observed in healthy participants, we added the AAT effect scores based on the RTs (operationalized as movement initiation times at 7° displacement instead of 30°) of the previously published group of healthy participants (Enter et al., 2014) as a control group (HC). 2 We conducted a three-way rmANOVA, with Condition (placebo, testosterone) and Emotion (angry, happy, neutral) as within-subject factors, and Group (SAD, HC) as between-subjects factor. Age was added as a standardized covariate because the HC-group has a higher age-range. Similar to the previous analyses in both groups separately, this analysis revealed a significant Condition × Emotion interaction, F(2, 76) = 4.61, p = .013, η p 2 = .108. There were no significant effects of Age (all ps > .37, η p 2 ≤ .02) or Group (all ps > .33, η p 2 < .03), the latter indicating that SAD participants benefitted to a similar extent from testosterone as the nonanxious group. Separate follow-up analyses for each pair of Emotions showed that the AAT effect scores in the testosterone condition tended to be higher for angry faces compared with happy and neutral faces, by revealing a significant main effect of Emotion for angry versus neutral, F(1, 38) = 9.52, p = .043, η p 2 = .200, a trend-level significant effect of Emotion for angry versus happy, F(1, 38) = 3.19, p = .082, η p 2 = .077, but a nonsignificant effect of Emotion for happy versus neutral faces, F(1, 38) = 0.284, p = .597, η p 2 = .007. There were no effects of Group (all ps > .17, η p 2 < .04), nor age (all ps > .27, η p 2 < .03). Therefore, these results indicate that testosterone promotes similar threat approach tendencies in nonanxious healthy participants and participants suffering from generalized SAD.
The effects of testosterone on AAT effect scores were not affected by administration order, time of testing, or use of contraceptives (see the Supplemental Material available online).
Discussion
The present findings show that single dose testosterone administration can lead to increased approach of social threat cues in women with SAD. This is the first study in SAD showing that testosterone directly influences automatic approach-avoidance actions and promotes approach behavior that directly affects the perceived distance of the social threat (Rinck & Becker, 2007).
Angry faces play an important role in social communication as they convey social dominance and are being perceived as a threat, especially by socially anxious individuals (Adams et al., 2003; Öhman, 1986). In our study, testosterone administration leads to a significant increase in approach of angry faces, relative to happy and neutral facial expressions. This finding is in agreement with literature that shows that testosterone reduces fear and sensitivity to threat, and enhances social dominance related behavior (Archer, 2006; Bos et al., 2012; Enter et al., 2016; Terburg & van Honk, 2013). Our previous study showed that testosterone promotes actual threat approach behavior in healthy participants (Enter et al., 2014), and the current study extends these findings by showing that testosterone also promotes social threat approach in participants with generalized SAD. Socio-neuroendocrine models of SAD propose that individuals with SAD display exaggerated socially submissive behavior, which is associated with social avoidance and low endogenous testosterone levels (Gilbert, 2001; Giltay et al., 2012; Hermans & van Honk, 2006; Öhman, & Wiens, 2003; Sapolsky, 1991; Weisman, Aderka, Marom, Hermesh, & Gilboa-Schechtman, 2011). An increase in threat approach behavior after administration of testosterone would be the result of an enhanced motivational tendency toward social dominance in this socially submissive group (Archer, 2006; Bos et al., 2012; Enter et al., 2014; Terburg & van Honk, 2013). This interpretation fits recent findings that testosterone can promote gaze behavior toward the eye regions in healthy and socially anxious individuals (Enter et al., 2016; Terburg et al., 2012).
Performance on the AAT depends on the coordinating role of the anterior prefrontal cortex and its connection with the amygdala and other brain regions (Volman et al., 2013; Volman, Roelofs, et al., 2011). This neural circuit is important for the regulation of social emotional behavior, and frontal-amygdala crosstalk during operation of the AAT is influenced by endogenous testosterone levels (Volman, Toni, et al., 2011). Studies featuring testosterone administration showed that testosterone affects neural responsiveness of brain areas involved in social approach such as amygdala and striatum toward socially salient stimuli (Hermans, Ramsey, & van Honk, 2008; van Wingen, Mattern, Verkes, Buitelaar, & Fernandez, 2010). Moreover, the way testosterone affects the amygdala depends on motivational context and it specifically promotes threat approach during performance of the AAT (Radke et al., 2015). Typically, these neural circuits show altered functioning in SAD. Neuroimaging studies in SAD have consistently shown increased activation of the amygdala and connected frontal-striatal circuits when participants were exposed to threatening facial expressions (Fouche, van Der Wee, Roelofs, & Stein, 2013), and it has been proposed that the amygdala is not properly regulated by cortical areas during social threat in SAD (Cremers et al., 2015; Freitas-Ferrari et al., 2010). Future neuroimaging research should elucidate whether testosterone administration also promotes threat approach in SAD by influencing activity in these neural circuits underlying social motivational behavior.
A few methodological issues are relevant to consider with regard to this study. First, following previous hormone administration studies featuring clinical participants on the AAT (van Peer, Spinhoven, van Dijk, & Roelofs, 2009), we selected the movement initiation time (7° joystick rotation) and not the full movement time (30° joystick rotation) as an outcome measure. It has been proposed that the initiation time reflects the time necessary for neural processes involved in stimulus evaluation, response selection, and programming the execution of motor movements, whereas the movement time includes the neuromuscular response (Rotteveel & Phaf, 2004). The latter usually shows a general slowing in patient samples with affective disorders, such as anxiety and depression, compared with HC (Sabbe, Hulstijn, van Hoof, Tuynman-Qua, & Zitman, 1999; Volman et al., 2013). Because we aimed to test effects on the cognitive affective processes reflected in the initiation time, we selected this measure for our analyses instead of the actual movement execution which may be confounded by general slowing in SAD. Second, previous studies featuring the AAT found that socially anxious participants show typical social avoidance behavior in response to angry faces (Heuer et al., 2007; Roelofs et al., 2010; van Peer et al., 2009; but see Roelofs, van Peer, et al., 2009). Although our results seem to point toward a relatively stronger tendency to avoid angry compared with happy faces in the placebo condition (see Fig. 1), this effect did not reach significance in the present study. Despite this absence of avoidance of angry faces on a group level, we found that avoidance of angry faces was stronger for more severely affected patients, as indicated by a significant correlation between baseline corrected AAT effect scores for angry faces and SPAI scores. In addition, it should be noted that testosterone can evoke strong placebo responses (Handelsman, 2011); therefore, we cannot exclude the possibility that placebo effects have contributed to decreased avoidance of angry faces in the placebo condition. Third, our sample size is small, even though it falls within a range that is common for SAD studies, and is employed in a powerful within subjects design. Future studies including a larger number of participants should replicate these findings and would also have the power to investigate the role of individual differences in endogenous testosterone levels. Finally, as a consequence of the testosterone administration method, only female participants were tested in this study (Tuiten et al., 2000). Future research should investigate whether testosterone administration to men has similar effects as suggested by similarities in social behavior related to endogenous and exogenous testosterone across sexes (Goetz et al., 2014; Hermans et al., 2008).
The finding that testosterone promotes social approach motivation in SAD may have clinical implications. A large proportion of SAD patients (up to 50%) does not recover after current evidence based psychological and pharmacological treatments (Hofmann & Bögels, 2006; Stein & Stein, 2008), and there is a need for new treatment strategies that enhance remission rates. A novel line of research has shown that treatment effects are augmented by pairing exposure therapy with a pharmacological agent (Hofmann, Fang, & Gutner, 2014; Singewald, Schmuckermair, Whittle, Holmes, & Ressler, 2015). Given our promising findings showing that testosterone promotes actual social approach behavior in SAD during a social challenge, and because exposure therapy is aimed at reduction of social avoidance behavior, it would be interesting for future investigations to explore whether adding testosterone as a pharmacological enhancer in the first few therapy sessions can boost efficacy of exposure therapy in SAD. In addition, future studies should test for dose-response relationships before administering testosterone in clinical practice.
In conclusion, this is the first study in SAD that shows that testosterone counteracts automatic avoidance behavior by promoting social approach tendencies that have a direct effect on the perceived distance of the social threat. These findings support theories on the role of testosterone in the regulation of social motivational behavior and concur with the predictions of socio-neuroendocrine models of SAD. These findings also may have clinical implications as social avoidance plays a crucial role in the persistence of SAD. The finding that this core characteristic can directly be influenced by single dose testosterone administration may encourage exploration of testosterone administration as a means to enhance therapy efficacy.
Supplemental Material
Enter_CPS_Supplemental_Material_Accepted_edits – Supplemental material for Dare to Approach
Supplemental material, Enter_CPS_Supplemental_Material_Accepted_edits for Dare to Approach by Dorien Enter, Philip Spinhoven and Karin Roelofs in Clinical Psychological Science
Footnotes
Acknowledgements
We acknowledge Frank Leonhard and Mike Rinck as authors of the AAT software. In addition, we are grateful to the women who participated in this study.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This work was supported by research grants from the Netherlands Organization for Scientific Research (NWO) awarded to K.R. (VIDI Grant 452-07-008; also supporting D.E.; VICI Grant 453-12-001) and a starting grant from the European Research Council (ERC_StG2012_313749).
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.