
Abstract
We previously reported on a 16-week, double-blind, randomized placebo-controlled trial (RCT) using 3 grams per day of N-acetyl cysteine (NAC) (1.5 grams twice per day) in 44 participants (aged 18–70) with DSM-5-diagnosed obsessive-compulsive disorder (OCD). We now report on an analysis of age, severity and duration of illness, OCD presentation type, baseline anxiety and depression scores, as well as the use of antidepressant medications as potentially modifying factors. Results revealed a significant effect (p = .037) for younger participants (under mean age of 34) responding to NAC. This remained significant using OCD severity as a covariate (p = .044). For those under 34 years of age with less than 17 years of OCD duration, this was also significant (p = .037). Regression analysis within the NAC treatment group also revealed that duration of OCD presentation was a significant predictor of Yale-Brown Obsessive Compulsive Scale (YBOCS) change at study endpoint (p = .019), whereas baseline Montgomery–Asberg Depression Rating Scale scores were also a trend-level predictor (p = .060) of YBOCS change in the NAC group.
Obsessive-compulsive disorder (OCD) is a frequently debilitating neuropsychiatric disorder, and often presents in a chronic waxing and waning nature (Franklin & Foa, 2011). Selective serotonin reuptake inhibitors (SSRIs), as well as clomipramine (an older tricyclic antidepressant) are considered to be the first-line pharmacological interventions for OCD (Franklin & Foa, 2011; Slade, Johnston, Oakley Browne, Andrews, & Whiteford, 2009). Despite demonstrating positive effects in several instances (Bloch, McGuire, Landeros-Weisenberger, Leckman, & Pittenger, 2010), it is estimated that 40% of patients do not achieve a clinical response from these medications, nor other augmentation strategies (Pallanti, Grassi, & Cantisani, 2014). In addition, SSRIs are often required at significantly higher doses than those used for the treatment of depression to obtain clinical benefits in OCD, which may result in a greater degree of adverse side effects including sedation, insomnia, and sexual dysfunction, and complete functional recovery is rare (Bandelow, 2008). Due to these reasons, other adjunctive treatments are often of necessity; one such potential treatment is the amino-acid-based agent N-acetyl cysteine (NAC).
NAC is a pharmaceutically prepared amino acid agent that acts as a “pro-drug” for cysteine, which then normalizes glutamate transmission in corticostriatal brain circuitry (Choy, Dean, Berk, Bush, & van den Buuse, 2010). NAC exerts glutamate-modulating effects through its interaction with the glutamate/cystine antiporter system (XC-), and is also a key precursor in the synthesis of the endogenous antioxidant glutathione. Cystine, the oxidized form of cysteine, has the ability to activate XC-, which are primarily located on glial cells in the brain and responsible for the clearance of glutamate in the synapse (Han et al., 1997). Once activated by cystine, intracellular glutamate is exchanged and released into the extracellular space, whereas cystine taken up by the glial cell is used to form glutathione. Extracellular glutamate has the ability to bind to group II metabotropic receptors (mGluR2/3), located on neighboring presynaptic glutamatergic neurons. This results in the inhibition of further glutamate release from presynaptic neurons and thus regulates its neurotransmission (Moran, McFarland, Melendez, Kalivas, & Seamans, 2005). By modulating excess levels of synaptic glutamate, excitoxicity and neuronal damage is also reduced, and thus provides an additional mechanism by which NAC may improve brain health (Miyamoto, Murphy, Schnaar, & Coyle, 1989). Furthermore, low levels of glutathione and excessive levels of glutamate have both been shown to contribute to hypofunction of the N-methyl-D-aspartate receptor (Steullet, Neijt, Cuenod, & Do, 2006). NAC’s ability to replenish glutathione levels and regulate excessive levels of glutamate provides an additional effect on modulating glutamate activity by restoring the function of this receptor.
Several clinical trials have been conducted using NAC for a range of psychiatric disorders (Berk, Malhi, Gray, & Dean, 2013; Deepmala et al., 2015), and it has been demonstrated to be well tolerated in doses up to 8 grams per day (De Rosa et al., 2000). Although NAC has evidence of efficacy in bipolar depression, schizophrenia, trichotillomania, and other compulsive behaviors, to our knowledge there is limited evidence to date assessing its efficacy in treating OCD. Recent data exist from a double-blind randomized controlled trial (RCT) of adjunctive NAC in the treatment of OCD (Afshar et al., 2012). This 12-week study conducted in Iran involved 48 participants with OCD diagnosed according to criteria of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994), using 2.4 grams per day of NAC or matching placebo tablets and found that the NAC treatment group demonstrated a significant reduction in OCD symptoms as measured by the Yale-Brown Obsessive Compulsive Scale (YBOCS; p = .003). Due to results appearing in the study to be more pronounced only after Week 8, we conducted a longer 16-week double-blind RCT (Sarris et al., 2015) using a higher dose of NAC (3 grams per day) to potentially elicit a stronger effect. In brief, our RCT involved 44 participants (aged 18–70) with DSM-5-diagnosed OCD, recruited between 2013 and 2015 in Melbourne, Australia. The primary outcome measure was the YBOCS, conducted every 4 weeks. Results of the main analysis of the full sample with repeated-measures mixed linear modeling revealed a nonsignificant Time × Treatment interaction for the YBOCS scale total score (p = .39; cf. Sarris et al., 2015). Although like the 12-week Iranian study an apparent effect was emerging by Week 12 on a per protocol analysis removing protocol violators, at Week 16 this study failed to show a significant Time × Treatment interaction for YBOCS total score (p = .15). It is unclear why the effect dissipated from Week 12; this is potentially due to a ceasing of efficacy, or the active group having worsening of OCD due to potential concern over the study ending. However, a significant Time × Treatment interaction was observed for the YBOCS Compulsions subscale in favor of NAC (p = .013), with a significant reduction observed at Week 12 (dissipating at Week 16). At 16 weeks only four (20%) of the participants in the NAC group were considered “responders” (YBOCS ≥ 35% reduction at endpoint) versus four (27%) in the placebo group.
In the recent systematic review of NAC for the treatment of OCD and related disorders (Oliver et al., 2014), a number of factors were identified that may moderate the efficacy of NAC for patients with OCD. First, it was argued that patients with a more chronic and severe presentation of OCD may be less responsive to NAC treatment in comparison to patients with moderate presentations of OCD. Second, when NAC is used as an augmentation strategy it was identified that there may be a differential response to NAC on the basis of which class of antidepressant that the patient was also concurrently receiving. However, in addition to these elements, there is potential that other differential factors such as age and OCD presentation (i.e., the nature of the obsessions and compulsions) may also influence whether a significant response to NAC is observed. For example, a moderator analysis of an RCT (Magalhaes et al., 2012) testing NAC in bipolar disorder found that participants with systemic illness had a greater response on functional outcomes, indicating an advantage for those with medical comorbidity. Furthermore, in an analysis of an OCD RCT (Wheaton, Rosenfield, Foa, & Simpson, 2015) comparing the effects of augmenting psychotropic medications versus exposure and ritual prevention and placebo, pretreatment OCD severity, age, baseline depression, and hoarding moderated outcome after acute treatment, whereas baseline level of functioning predicted outcome and rate of change across all of the augmentation strategies. For these reasons, in this article we explored the data further to determine any participant characteristics or modifying factors that may elucidate whether NAC is more effective in certain presentations of OCD.
Method
Overview
The overarching study was a 16-week double-blind RCT using 3 grams per day of NAC (1.5 grams twice per day) or matching placebo in 44 randomized adult participants with DSM-5-diagnosed OCD. The study was conducted according to Good Clinical Practice at the Melbourne Clinic (where participants were primarily recruited) during June 2013 to April 2015. The study was registered on the Australia New Zealand Clinical Trials Registry, and had ethical approval from The Melbourne Clinic Ethics Committee (TMC_HREC no. 219). The NAC was provided in opaque capsule form, produced by Lipa Pharmaceuticals PTY Ltd., and supplied by BioCeuticals PTY Ltd., in strict compliance with pharmaceutical Good Manufacturing Procedure. The certificate of analysis confirmed the NAC to have a 99.97% purity. The placebo group was administered the same dosing regimen of matching opaque capsules containing cellulose.
Participants were required to meet the following criteria: age 18 to 70, capacity to consent to the study and follow its procedures, fulfill the DSM-IV-TR diagnostic criteria (based on the Mini International Neuropsychiatric Interview–Plus; MINI-Plus) for obsessive-compulsive spectrum disorder (OCSD; and diagnosed OCD with the insight specifier from the DSM-5, via clinician assessment), score 16 (moderate) or over on the YBOCS at the time of study entry, and on either no treatment or a stable treatment regimen for a minimum of 4 weeks of current treatment and a minimum of 12 weeks if it was their first OCD treatment. Self-reported OCD was assessed and confirmed by physician diagnosis; female participants were required to use effective contraception if of childbearing age and sexually active. Participants were ineligible to enter the trial if they had any of the following conditions: currently engaged in a psychological program (e.g., a 2-week OCD behavioral modification program or an intensive cognitive behavioral therapy course; ongoing psychological or medical care was accepted); known or suspected clinically unstable serious medical disorder; bipolar I disorder, schizophrenia, epilepsy, asthma, or recent gastrointestinal ulcers; pregnancy or breastfeeding; consumption per day of over 250 mg of NAC, 100 mcg of selenium, or 500 IU of vitamin E; or history of hypersensitivity or intolerance to NAC or any component of the preparation. The primary outcome assessment was the YBOCS (Goodman, 1989). Secondary outcome assessments were the Clinical Global Impression Scales–Severity and Improvement (CGI; Guy & Bonato, 1970), the Hamilton Anxiety Rating Scale (HAMA; Hamilton, 1959), the Montgomery–Asberg Depression Rating Scale (MADRS; Montgomery & Asberg, 1979), the General Health Questionnaire-28 (Goldberg, 1978), and purpose-designed demographics/medical history/drug/alcohol use forms.
Moderator analysis
Details of the primary efficacy analysis are included in Sarris et al. (2015). The effects of five moderator variables (both separately and in combination where significance or trend for significance was found) were assessed in the current analysis: age (years), OCD severity (YBOCS total at baseline), duration of illness (years), gender, medication status, and OCD symptom presentation. A median split was conducted on age to calculate a dichotomous age group variable (young, old). Similarly, an OCD severity variable (moderate, severe) was calculated by conducting a median split on baseline YBOCS total scores, and OCD duration was similarly determined by median split on OCD illness duration. Analyses were also conducted stratifying participants who were taking antidepressant medication versus those who were not. The data were also stratified and analyzed based on participants’ OCD domains: aggressive, contamination, sexual/religious, symmetry/order. Separate repeated measures ANOVAs were then conducted using the stratified samples, with study visit (Baseline, Week 4, Week 8, Week 12, and Week 16) as the within-subject variable and treatment group (placebo, NAC) as the between-subject variable. The continuous variable characteristics were also used as covariates in a repeated measures ANCOVA model. Regression analysis was also conducted on YBOCS change scores, from baseline to study endpoint (16 weeks), using continuous predictors which were found to correlate (p < .10) with YBOCS change in the NAC treatment group. All variables were centered on zero by subtracting the mean from each case, then entered into a single-step linear regression. All tests of treatment effects were conducted using a two-tailed alpha level of .05 (.10 considered a trend for significance) and 95% confidence intervals. Data were analyzed via SPSS 22.0.
Results
Participant characteristics
After 189 enquiries, a total of 44 participants were randomized into the study, demonstrating a recruitment conversion rate of 23% and achieving 88% of the calculated projected sample size required (n = 50) to detect a clinically significant result. Seven participants withdrew from the study with no between-group differences. The sample consisted of slightly more males (n = 24; 54.5%), whereas the median age of the sample was 34 years (range 18 to 68 years; interquartile range 15). All participants met the DSM-5 criteria for OCD at the time of entry into the study. The chronicity of OCD ranged from 2 years to over 45 years in duration (M = 16.36 years, SD = 9.5 years). Five participants (11.4%) reported a family history of OCD, and more than half the participants (56.8%; n = 25) had a DSM-IV-diagnosed comorbid psychiatric disorder (as per the MINI-Plus Version 6). A majority of the participants (79.5%) were taking psychotropic medication, namely SSRIs (56.8%), and 13 participants (29.5%) were utilizing adjunctive therapies such as antipsychotics. Examples of the intrusive thoughts and compulsions experienced by the participants can be seen in Table 1. These consisted primarily of aggressive, contamination, sexual/religious, or symmetry/order domains.
Obsessive Thoughts and Compulsions Experienced by Participants

Note: Domains extracted from the Dimensional Yale-Brown Obsessive Compulsive Scale (DYBOCS).
Moderator analysis outcomes
A significant effect was revealed for younger participants (< 34 years; f = 2.70, p = .037; Fig. 1). This remained significant using OCD severity as a covariate (f = 2.98, p = .044). Further analysis revealed a trend (f = 2.38, p = .089) for those with duration of OCD illness under 17 years (mean duration), and for younger participants with less than 17 years of duration this was also significant (f = 3.19, p = .037). A nonsignificant effect was revealed when the sample was stratified for severity (p = .61 < 26 YBOCS, p = .59 > 26 YBOCS), and also for female gender (p = .42). Investigations into whether NAC was effective for differing presentations of OCD (e.g., aggression, sexual/religious, symmetry/ordering obsessions), revealed a trend in favor of the NAC group for the “aggression” subtype (f = 3.15, p = .059), whereas a subanalysis of participants taking medication (70.5%; primarily selective serotonin reuptake inhibitors) revealed no effect (p = .19). A trend in favor of the NAC group was revealed for those who were younger and taking antidepressants (f = 2.38, p = .098).
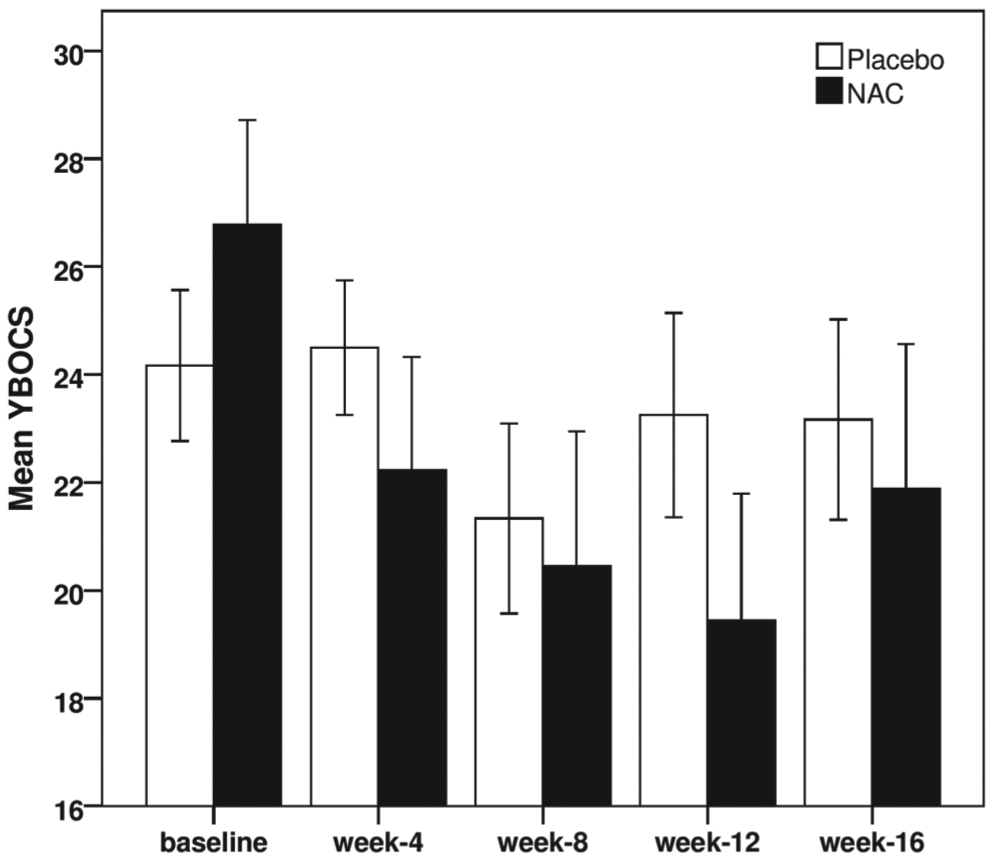
Change in Yale-Brown Obsessive Compulsive Scale (YBOCS) scores (<34 years of age). Group × Time interaction, p = .034. Bars represent standard errors.
Regression analysis outcomes
The following continuous predictors were found to correlate (p < .10) with YBOCS change in the NAC treatment group: baseline MADRS total (r = .441, p = .04), baseline HAMA total (r = .391, p = .072), baseline CGI severity (r = .456, p = .033), and duration of OCD presentation (r = .389, p = .073). These variables were not found to correlate significantly with YBOCS change in the placebo group. The only variable that was found to correlate at the p = .10 level with YBOCS change in the placebo group was age (r = −.387, p = .075).
The linear regression analysis in the NAC treatment group demonstrated that the duration of OCD presentation was a significant predictor of YBOCS change at study endpoint (β = .629, t = 2.598, p = .019), and that baseline MADRS total score was also approaching significance as a predictor of YBOCS change (β = .799, t = 2.018, p = .060). The overall model, with the four predictors, was found to explain 46.5% (adjusted R2 = 33.9%) of the variance in YBOCS change scores at study endpoint. The variance explained by the four predictors was found to be significant, R2 = .465, F(4, 21) = 3.694, p = .024. A summary of the regression output is displayed in Table 2.
Linear Regression Model for YBOCS Change as Predicted by OCD Duration, Baseline HAMA, Baseline MADRS, and Baseline CGI Severity

Note: CGI = Clinical Global Impression Scales–Severity and Improvement; HAMA = Hamilton Anxiety Rating Scale; MADRS = Montgomery–Asberg Depression Rating Scale; YBOCS = Yale-Brown Obsessive Compulsive Scale. All variables were centered on zero, by subtracting raw scores from the mean.
These findings demonstrate that in the current sample receiving NAC for 16 weeks, a longer duration of OCD presentation was associated with a reduction in the amount of YBOCS improvement observed, that is, for every additional 10 years of OCD illness, there was on average a 3.88 point YBOCS decrease in treatment response. Similarly, participants who presented with a higher level of depression symptoms at baseline, were also found to display less of a response to NAC treatment, that is, for every additional 10-point increase on the MADRS at baseline there was on average a 4.51 point YBOCS decrease in treatment response at study endpoint. Partial regression plots for duration of OCD presentation and baseline MADRS versus YBOCS changes are displayed in Figure 2.
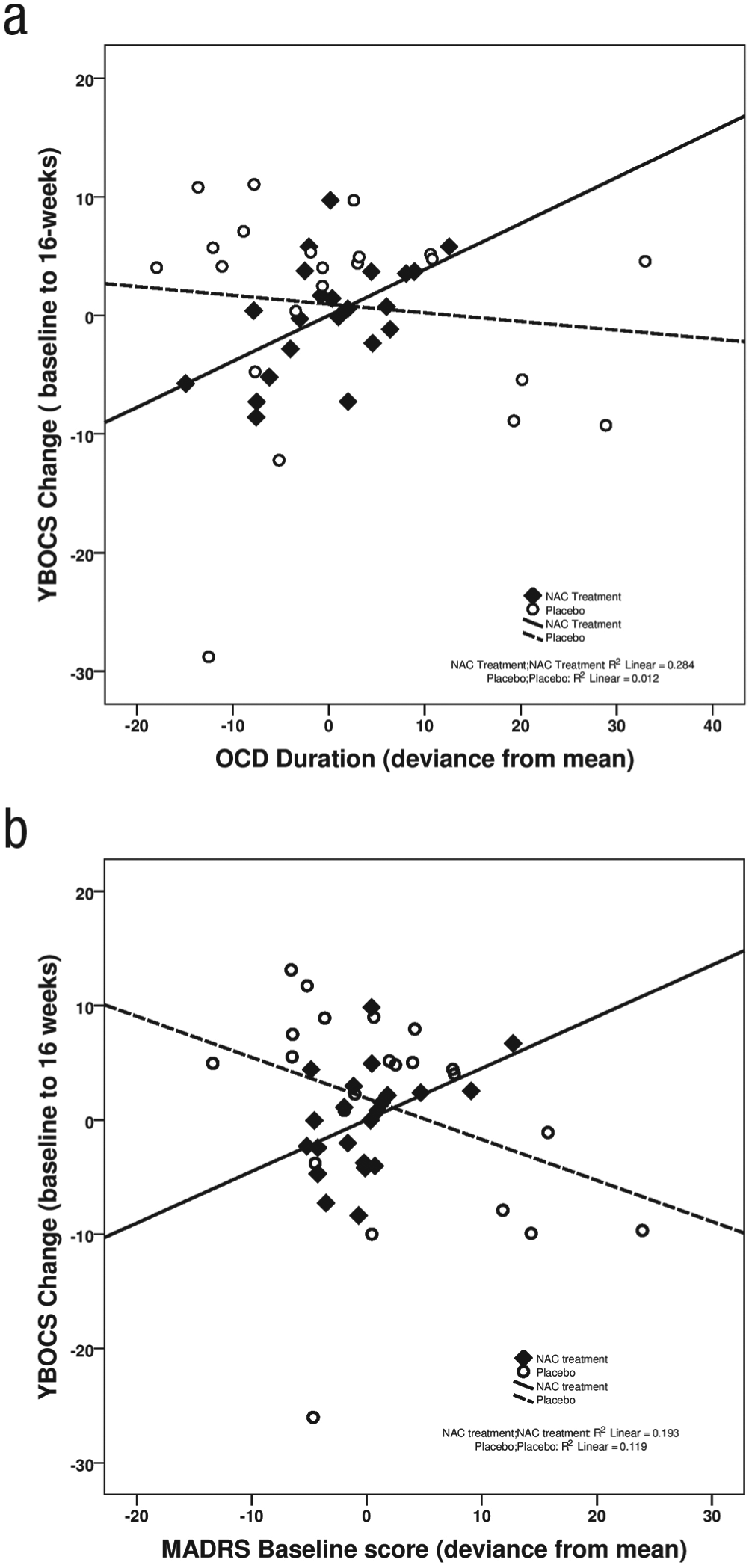
Partial regression plots with linear regression lines for Yale-Brown Obsessive Compulsive Scale (YBOCS) change versus (a) OCD duration and (b) Montgomery–Asberg Depression Rating Scale (MADRS) baseline score. Note that negative YBOCS change indicates an improvement in symptoms (baseline to endpoint).
Discussion
As we have previously reported, 3 grams of NAC supplemented for 16 weeks did not to exert a statistically significant effect over placebo for reducing the severity of OCD symptoms as measured by the YBOCS (time by treatment interaction). However, when stratified for a range of characteristics, it was revealed that those who were younger, and had a lesser duration of OCD diagnosis may respond more favorably to NAC. This latter finding was also corroborated by the regression analysis in the NAC treatment group, whereby less of a treatment response to NAC was found in participants with a longer duration of OCD presentation. There is also the potential that NAC may work more effectively in younger people or in those who may have the ‘aggressive’ subtype of OCD. It stands to reason that NAC is more effective in younger people with a lesser duration of the illness, could be due to “intractable” treatment-resistant OCD presentations being harder to treat. It is interesting to note that more cases of placebo response were found in the older participants (aged > 34); this may be due to reporting error from potential cognitive decline. NAC may also potentially work synergistically with medications. A recent animal model exploring the effects of NAC adjunctively with various antidepressants highlighted its beneficial activity on the tricyclic antidepressant imipramine and the SSRI escitalopram (Costa-Campos et al., 2013). A dose of 5 mg/kg escitalopram and 1 mg/kg of NAC, used adjunctively to the antidepressants respectively, resulted in the reduction of the minimum effective doses required of each, as determined by a reduction in immobility in the tail suspension test. These effects were, however, not seen with NAC adjunctive to fluoxetine, or with increased doses of NAC with escitalopram and imipramine. It is also interesting to note that regression analysis revealed that those with higher levels of depression (MADRS baseline scores) may also be less responsive to NAC treatment. Although this predictor was found to be significant only at a trend level (p = .060), it is worthy of further investigation regarding whether comorbid depression may reduce the efficacy of NAC treatment.
It should be noted that this cohort’s OCD was extremely chronic, with a long duration of the disorder, majority taking multiple medications (SSRIs, tricyclic antidepressants, anticonvulsants, or antipsychotics) and OCD severity ranging from moderate to extreme (YBOCS range 25–34 at baseline). Participants who did not demonstrate a full clinical response to NAC in the current study share similarities those in the Van Ameringen cohort (Van Ameringen, Patterson, Simpson, & Turna, 2013) in respect to OCD severity and dose of NAC used. This suggests that NAC at the 3 gram dose may not be satisfactory to elicit a clinical effect. However, larger scale clinical trials are required to confirm this, given that the subanalysis in the current study to explore these variables resulted in small sample sizes. Thus, the insignificant findings could be the result of a Type II error.
This study was not without its limitations. Final recruitment resulted in 44 participants, and thus the targeted sample size of 50 to power the study was not achieved. Recruitment itself proved difficult, with many people ineligible due to comorbidities or not inclined to participate. The inability to obtain large sample sizes appears consistent with other OCD clinical trials exploring NAC, given the termination of the proposed study by Pittenger and colleagues at Yale University in the last few years. Investigations into the benefits of NAC for differing presentations of OCD (e.g., taboo thoughts vs. perfectionistic vs. contamination), chronicity, gender, severity, effects of comorbidities, adjunctive to medication, monotherapy, and so on were also limited, given that stratifying for these variables yielded even smaller sample sizes. In addition, a proportion (n = 5, 14.3%) of the final group did not complete the full 16 weeks of the study, and four of these participants completed only until Week 4. Although ITT principles were employed in the statistical analysis, detecting a clinically relevant result may have been hindered further given that NAC has been repeatedly shown to produce therapeutic effects after 8 to 12 weeks (Afshar, et al., 2012; Berk et al., 2008; Grant, Odlaug, & Kim, 2009). A further limitation acknowledged is in regard to one of the methods of analysis used (i.e., dichotomizing the continuous data); however, other OCD studies have also assessed outcomes based on score cutoffs (see A. M. Garcia et al., 2010). We accept that applying continuous data into groups should ideally be done in quartiles or quintiles; however, this could not be undertaken due to the small sample size. However, it is reassuring that regression analysis using continuous predictors within the NAC group corroborated one of the primary findings of the stratified analysis. Finally, we did not control for multiple testing, and the results would not have held statistical significance after being corrected.
It is important to consider that the effects of NAC in OCD may differ depending on the neurobiologies between specialized subdisorders and provide additional evidence for the heterogeneous nature of OCD. For example, although disturbed glutamate activity is becoming an increasingly regarded feature of OCD, it may be limited to a subset of people with polymorphisms in glutamate genes (Pauls, Abramovitch, Rauch, & Geller, 2014). Thus, NAC may be more suitable in these cases, only a handful of which may have been randomized into the current study. Furthermore, the form of NAC used may be poorly metabolized and thus its therapeutic effects limited. A preclinical study has demonstrated significantly greater glutathione levels in the brain after the administration of N-acetyl cysteine ethyl ester (NACET) compared with NAC alone (Giustarini, Milzani, Dalle-Donne, Tsikas, & Rossi, 2012). NACET is a form of NAC with esterification at its carboxyl group, which enhances its solubility in lipids and other nonpolar substances and thus improves its pharmacokinetics (Giustarini et al., 2012). Although NACETs use in clinical studies is currently lacking, this preclinical study raises questions as to NAC’s ability to induce the production of GSH in the brain and outlines the need for imaging studies to explore the bioavailability and activity of both NAC and NACET.
Although a clinical signal of effect for NAC in OCD is potentially evident (especially for addressing compulsions), a larger sample size study is now crucial to avoid the potential occurrence of Type II errors and allow for sizable subanalyses to explore the effects of chronicity, comorbidity, medication use, gender, as well as OCD symptom domains. The diverse clinical presentations and complexities of treatment response in OCD calls for the integration of genetic and neurobiological investigations alongside psychological and pharmaceutical or nutraceutical interventions. Ideally a trial to encompass all these elements and employing advanced spectroscopic imaging techniques (to better assess glutamate neurotransmitter activity and explore glutathione production in the brain) will assist in ascertaining if NAC exerts clinical benefits in modulating activity in the regions most heavily implicated in the pathogenesis of the disorder. Furthermore, a longer study period, with poststudy observational periods, is still warranted to ascertain if the implied 12-week effects of NAC continue to dissipate or improve with time. Given that higher doses of NAC appear to be well tolerated and elicit improved effects in other conditions such as ADHD (R. J. Garcia et al., 2013), there still remains scope to explore higher doses (> 3 grams) in OCD, particularly in more chronic presentations.
Footnotes
Acknowledgements
The NAC was kindly donated and supplied by BioCeuticals®. Trial registry: ACTRN 12613000310763.
Declaration of Conflicting Interests
The authors declared that they had no direct conflicts of interest with respect to their authorship or the publication of this article.
Funding
J.S. is funded by a CR Roper Fellowship.