
Abstract
The study was designed to test the hypothesis that indirect inhibition of the insula via cathodal transcranial direct current stimulation (tDCS) would decrease disgust and moral rigidity in 36 healthy individuals undergoing 15 min of tDCS over the temporal lobe. To obtain a comprehensive assessment of disgust, we used subjective (affect rating), physiological (heart rate variability [HRV]), and implicit measures (word-fragment completion), and moral judgment was assessed by asking participants to rate the deontological and altruistic moral wrongness of a revised version of the moral foundations vignettes. We found anodal and cathodal stimulations to, respectively, enhance and decrease self-reported disgust, deontological morality, and HRV. Note that these effects were stronger in individuals with higher levels of obsessive compulsive (OC) traits. Because disgust and sensitivity to deontological guilt are among the most impairing features in OC disorder, it is auspicious that cathodal tDCS could be implemented to reduce such symptoms.
In the literary canon, Shakespeare’s Lady Macbeth washing her hands to clean the guilt away has symbolized the human tendency to treat moral impurity as a physical grime. Empirical studies have emphasized that—when faced with both physical contaminants and moral transgressions—people subjectively feel and express disgust (Chapman et al., 2009; Haidt, 2003; Haidt et al., 1997; Miller, 1997; Rozin et al., 2010), with a notable overlapping in terms of behavioral response (Rozin et al., 1993) and neural activation (Basile et al., 2011; Borg et al., 2008; Ottaviani et al., 2018).
At a cognitive-behavioral level, physical and moral disgust share fear of contamination, which arises when people contact an object or a person perceived as dirty (Rachman, 2004). This fear acts as a motivational trigger to avoid or withdraw from the contaminant entity, and such motivation is often coupled with the urge to wash and purify oneself (Rozin et al., 1993). Contamination also occurs with no physical contact (Herba & Rachman, 2007); in this case, the dirty site is not accessible or removable (Radomsky et al., 2018), and people affected feel themselves as bad persons, worthless or immoral. Not surprisingly, mental contamination is a prominent characteristic of obsessive compulsive disorder (OCD). Some individuals with OCD express great frustration about the inability to remove their persistent feeling of dirtiness even after a number of washing sessions (Rachman, 1994).
Zhong and Liljenquist (2006) called the “Lady Macbeth effect” the urge to undertake washing behavior as a result of perceived threats to moral purity. These authors showed that without wiping their hands, participants felt guilty about their past transgressions, whereas participants who wiped their hands experienced a decrease in guilty feelings. Because a dirty moral conscience leads to a sense of disgust that one wants to clean out, empirical studies have demonstrated that the reverse pattern is also true, that the induction of physical disgust by exposure can exacerbate the severity of moral judgments (Eskine et al., 2011; Schnall, Benton, & Harvey, 2008; Schnall, Haidt, et al., 2008). In the same vein, Tobia (2015) reported that the sensation of dirtiness elicits a stronger tendency to judge oneself more negatively from a moral point of view.
Several studies have replicated the Lady Macbeth effect (D’Olimpio & Mancini, 2014; Elliott & Radomsky, 2009; Fairbrother & Rachman, 2004), whereas others have failed to obtain the same results (Earp et al., 2014). A possible explanation for this incongruence relies on the fact that participants were asked to recall an ethical or unethical deed without considering the distinction between altruistic and deontological guilt (Gangemi & Mancini, 2017; Ottaviani et al., 2019). Whereas the former is due to the violation of empathic/altruistic principles, in which not standing by the victim’s side is enough for feeling guilty, deontological guilt emerges from the assumption of having violated one’s own moral rules (Mancini & Gangemi, 2015). D’Olimpio and Mancini (2014) and Ottaviani et al. (2019) induced altruistic guilt in a group of participants and deontological guilt in another group. In both studies, the Lady Macbeth effect was found in the second group but not in the first one, pointing to a more plausible implication of deontological guilt in the Lady Macbeth effect. Deontological guilt has been suggested to play a pivotal role in the genesis and maintenance of OCD (Basile et al., 2014; Gangemi & Mancini, 2017; Mancini, 2018). In line with this claim, studies have shown that the obsessive concern over a harmful event (e.g., a gas explosion) is dramatically reduced in individuals with OCD when they do not have a direct responsibility for such an event. Patients’ worries are not for the victims of an explosion but rather for being responsible for it (Lopatka & Rachman, 1995). Likewise, OCD-related concerns often imply religious or sexual sins even if the behavior is not harmful toward anyone. Furthermore, patients with OCD were found to choose deontological options in the trolley dilemma (e.g., letting five people die instead of just three but without taking the responsibility of changing the natural course, thereby respecting the “do not play God” moral rule) more frequently than individuals with anxiety and mood disorders, who opted for more consequentialist choices (Mancini & Gangemi, 2015).
At a brain level, the association between physical and moral disgust has been recently studied. It is well known that the insular cortex is involved in processing disgust, an observation first suggested by studies on Huntington’s disease. These patients are severely impaired in the perception and experience of disgust (Hayes et al., 2007; Mitchell et al., 2005; Sprengelmeyer et al., 1996), a defect associated with reduced functional responses in the insular cortex (Hennenlotter et al., 2004; S. A. Johnson et al., 2007). An abnormal insula functioning also plays a role in the enhanced disgust sensitivity found in individuals with OCD (George, 2013). The insula and other disgust-relevant brain regions are in fact more easily activated in persons with OCD than in other persons (Berle & Phillips, 2006; Schienle et al., 2005). For instance, in patients with contamination concerns, the disgust-inducing stimuli are associated with a greater activation in several regions, most notably the insula, compared with nonclinical individuals (Shapira et al., 2003). Note that Phillips et al. (2000) showed that patients with washing compulsions rated disgust pictures as provoking more disgust, fear, and anxiety than did patients with checking compulsions; moreover, specific washing-relevant pictures activated both visual regions and the insula only in the group with washing compulsions.
Imaging studies with healthy participants have corroborated the aforementioned findings (Phillips et al., 1997; Pujol et al., 2018; Wicker et al., 2003; Wright et al., 2004). Nonetheless, whether the insula selectively processes disgust remains an area of contention (Berle & Phillips, 2006) because this region was also found to be involved during perception of facial expressions of pain, fear, and happiness (George, 2013). Given its role in a range of functions, from the representation of internal bodily state, visceral and gustatory processing, and autonomic regulation to self-generated affective experiences (Coghill et al., 1994), Wright et al. (2004) deemed both the general affective and the disgust-specific role for the insula as plausible.
Neuroimaging studies have also attempted to identify the role of the insula during reactions to moral concerns (Borg et al., 2008; Moll et al., 2005). Greene et al. (2004) found that resolving moral dilemmas requiring “personal” moral violations (e.g., smothering a crying baby to save oneself and one’s townspeople from enemy soldiers) activated both brain regions associated with cognitive control (e.g., dorsolateral prefrontal cortex) and the anterior insula. Activation of the insula has also been linked to a tendency to reject unfair offers in the ultimatum game (Sanfey et al., 2003). Because the insula seemingly subserves negative affective states that bear on decision-making, as Greene et al. (2004) speculated, the involvement of the insula in difficult personal moral judgment may reside on dealing with actions that would otherwise be considered morally repugnant. Using an event-related functional MRI (fMRI) paradigm, Basile et al. (2011) investigated the neural substrate of altruistic and deontological guilt. The authors found the former to activate the medial prefrontal brain areas, involved in the representation of others’ intentions and empathy, whereas the experience of deontological guilt selectively activated the insula. To overcome the limitations of correlational fMRI studies in investigating the relationship between morality and disgust, Ottaviani et al. (2018) used transcranial direct-current stimulation (tDCS) to indirectly stimulate the insula and showed that anodal tDCS stimulation over the temporal lobe (which comprises the region of the insula) elicited disgust as indicated by implicit (word completion task) and physiological measures (heart rate variability [HRV]) and by self-reports (momentary affect assessment) and triggered more severe moral judgments compared with sham condition in the deontological domain but not in the altruistic domain.
The Present Study
The tDCS is increasingly used for therapeutic purposes, and there have been promising initial results in pain treatment, motor rehabilitation after stroke, epilepsy therapy (Fregni, Boggio, et al., 2006; Fregni et al., 2005; Fregni, Gimenes, et al., 2006; Fregni, Otachi, et al., 2006; Hummel et al., 2005), and also in psychiatric disorders, mainly major depression (Nitsche et al., 2009; Rigonatti et al., 2008). Given that Ottaviani et al. (2018) successfully used anodal tDCS to enhance feelings of disgust and deontological rigidity, in the current investigation, we aimed at evaluating whether the opposite pattern of results could be achieved by inhibitory cathodal tDCS in psychiatrically healthy individuals, with the ultimate aim of advancing clinical science in finding ways to alleviate such difficult to address symptoms of OCD.
Although such inhibitory effects have not always been replicated (Jacobson et al., 2012), cathodal tDCS is still considered to have the potential to decrease excitability (Nitsche et al., 2003; Nitsche & Paulus, 2000, 2001), and incongruent results depend mainly on the protocol used (Monte-Silva et al., 2010).
With these premises, the present study was guided by the hypothesis that a decrease in cortical excitability in the insula via cathodal tDCS would dampen both disgust and moral rigidity in a sample of nonclinical individuals. Moreover, we expected to replicate findings by Ottaviani et al. (2018) of increased disgust sensitivity and moral rigidity following anodal tDCS. Finally, we expected these effects to be stronger in individuals with higher levels of OC traits.
Method
Participants
Most of the participants were undergraduate students recruited by advertisement on the Internet or by word of mouth. Forty individuals initially agreed to participate in the present study and completed the prescreening online questionnaires. Criteria of exclusion were current diagnosis of neurological, psychiatric, or heart disease; self-reported history of head injury; cognitive impairment; history of substance or alcohol abuse or addiction; and pregnancy. After the exclusion of four participants who dropped out before starting the study, the final sample consisted of 36 healthy individuals (18 women) with a mean age of 22.44 years (SD = 3.3; range = 19–38 years). All participants were White and participated in the study after providing signed informed consent. The present study was carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans and was approved by the Bioethical Committee of Santa Lucia Foundation of Rome, Italy.
Procedure
A series of online questionnaires were first administered to assess eligibility and obtain information on demographics and lifestyle as well as dispositional psychological characteristics. Participants were required to abstain from drinking coffee or smoking cigarettes for at least 2 hr before the experiment. The design used for the study was randomized, sham controlled, and within subjects. Each participant underwent three different sessions, in a counterbalanced random order, in which either anodal, sham, or cathodal tDCS were used on different days with at least a 48-hr interval between sessions. During the entire experimental protocol, a heart rate (HR) device was attached using a standard electrode configuration to derive HRV while participants sat in front of a 15-in. color monitor. Stimulus presentation (i.e., instructions, experimental tasks) and response collection were computerized and run with the E-Prime software (Version 2.0; Psychology Software Tools, 2017).
First, participants underwent a 3-min vanilla baseline assessment during which they browsed a neutral magazine (Jennings et al., 1992). At baseline and at the end of each experimental session (i.e., after tDCS stimulation), participants rated their momentary emotional state on a series of 5-point Likert scales. Then, participants underwent either a 15-min sham, anodal, or cathodal tDCS stimulation during which they were asked to color a mandala for the first 10 min (to avoid the complete focus on the physical sensations provoked by the stimulation) and to complete the computerized tasks (i.e., a moral task and a word-stem completion task) for the remaining 5 min.
Measures of psychological traits
Prescreening online questionnaires
Along with questionnaires assessing sociodemographic (age and level of education) and lifestyle information (nicotine, alcohol, caffeine consumption; medication; and physical activity), a set of questionnaires evaluating psychological traits and symptoms (e.g., anxiety, depression, disgust sensitivity, obsessive compulsive [OC] tendencies, scrupulosity, altruistic conduct) were administered online before the first experimental session.
Relatively stable aspects of anxiety proneness were assessed by using the trait version of the State-Trait Anxiety Inventory (Spielberger et al., 1970; Italian translation by Pedrabissi & Santinello, 1989). This is a 20-item scale that also includes general states of calmness, confidence, and security (e.g., “I am a steady person”). Cronbach’s α in the present study was .82.
The Center for Epidemiologic Studies Depression Scale (Radloff, 1977; Italian validation by Fava, 1983) is a 20-item scale whereby participants reported the occurrence of depressive symptoms during the previous week (e.g., “I felt that everything I did was an effort”). Total score ranges from 0 to 60. Standard cutoffs are 16 for mild depression and 23 for clinical depression. Cronbach’s α in the present study was .80.
The Obsessive–Compulsive Inventory–Revised (OCI-R; Foa et al., 2002) was administered to measure the presence and severity of obsessions and compulsions. Participants rated 18 items on a 5-point scale (0 = not at all, 4 = very much) according to the degree of disturbance caused by a series of behaviors (e.g., “I check things more often than necessary”). Cronbach’s α in the present study was .88.
Individual differences in sensitivity to disgust were measured by the Disgust Scale–Revised (Olatunji, Abramowitz, et al., 2007; Olatunji, Williams, et al., 2007), which consists of 27 items divided in two parts: (a) 14 items rated on a 5-point scale (0 = totally disagree, 4 = totally agree) depending on the level of agreement with a sentence (e.g., “I never let any part of my body touch the toilet seat in public restrooms”) and (b) 13 items rated on a 5-point scale (0 = not at all disgusting, 4 = extremely disgusting) indicating the repugnance caused by a situation (e.g., “While you are walking through a tunnel under a railroad track, you smell urine”). Cronbach’s α in the present study was .73.
Through the 15 items of the Pennsylvania Inventory of Scrupulosity-Revised (PIOS-R; Olatunji, Abramowitz, et al., 2007; Olatunji, Williams, et al., 2007), participants reported their degree of scrupulosity on a 5-point scale (0 = never, 4 = constantly) according to the frequency of subjective experiences (e.g., “I worry that I might have dishonest thoughts”). Cronbach’s α in the present study was .79.
The Self-Report Altruism Scale (Rushton et al., 1981) is a 20-item scale whereby participants rated how often they engaged in a series of altruistic conducts (e.g., “I have donated blood”) on a 5-point scale (0 = never, 4 = very often). Cronbach’s α in the present study was .76.
tDCS
For each session, the overall duration of the current flow was 15 min, including both a ramp-up and a ramp-down period for 30 s each. The tDCS was delivered at 2 mA by a battery-driven (9V) constant current stimulator (BrainSTIM; EMS s.r.l., Italy), presenting a maximal output of 10 mA. Conductive rubber electrodes (7 × 5 cm), covered by sponges soaked in isotonic saline solution (0.9% [wt/vol] NaCl), were used and held in place by an elastic bandage material. The appropriate amount of saline (6 mL per sponge) was obtained by using a syringe to avoid oversaturation of the sponge. Moreover, an electroconductive gel was applied under the sponges before the montage to reduce skin impedance (< 5 kΩ; DaSilva et al., 2011).
The montage and stimulation parameters used were chosen to widely target the left insular cortex (see Lang et al., 2005; Montenegro et al., 2011; Okano et al., 2015; Petrocchi et al., 2017; Piccirillo et al., 2016). Participants underwent head measurements at each session, using the 10-20 International EEG System (Klem et al., 1999), to accurately locate electrode placement: (a) In the anodal condition, the anode electrode was placed at scalp coordinate T3 and the cathode electrode over brain region Fp2; (b) in the cathodal condition, the cathode was placed at coordinate T3 and the anode over Fp2 area; and (c) for the sham condition, to ensure a sham control effect, the electrodes placement was identical to cathodic or anodic configuration, but the stimulation lasted only 30 s before ramping down to zero. In this way, the participants had an initial itch on the portion of skin under the electrode, but they did not receive any further electrical current, and this made them unaware of the type of stimulation received (Gandiga et al., 2006). All tDCS sessions were administered by a trained experimenter.
Measures of disgust and morality
To obtain a comprehensive assessment of disgust, we used subjective self-report (affect rating), physiological (HRV), and implicit measures (word-fragment-completion task; Landy & Goodwin, 2015). The assessment of moral judgment in deontological and altruistic domains was conducted by using a revised version of the moral foundations vignettes developed by Clifford et al. (2015).
Affect rating
At the beginning (i.e., after the 3-min baseline assessment) and at the end of the experimental protocol, participants were asked to rate their momentary levels of shame, sadness, fear, disgust, anger, pity, altruistic guilt, deontological guilt, and happiness on a 5-point Likert scale from 1 (not at all) to 5 (very much; adapted from D’Olimpio & Mancini, 2014). Given the within-subjects design and the need to perform the three tDCS sessions in different days, a change score was computed for each session by subtracting the baseline for that specific session from the affect rating after stimulation or sham tDCS. Positive scores reflect higher levels of the perceived emotional state from baseline to post-tDCS.
Physiological data
HRV has been used as a valuable index to examine the autonomic correlates of disgust (Cisler et al., 2009; Davey, 2011). As opposed to fear, which is associated with a heightened sympathetic activity linked to increased HR (Rohrmann & Hopp, 2008) and phasic HRV suppression (e.g., Park et al., 2014), disgust is characterized by parasympathetic dominance, decreased HR, and heightened HRV (Ekman et al., 1983; Levenson et al., 1990; Rohrmann & Hopp, 2008; Rozin et al., 1999; Schlegel et al., 2001; Woody & Teachman, 2000), mainly because disgust-related functions (e.g., processing of tastes, rejection of toxic foods) are achieved by activation of the parasympathetic drive to the heart via brain-stem nuclei (Babic & Browning, 2014).
In the present study, HR was recorded as beat-to-beat intervals in milliseconds by using the Bodyguard 2 device (Firstbeat Technologies Oy, Jyväskylä, Finland). Vagally mediated HRV (vmHRV) was assessed by computing the root mean square of successive beat-to-beat interval differences, which reflects the vagal regulation of HR (Task Force of the European Society of Cardiology, 1996). Outlier and artifact detection as well as vmHRV analysis were performed using Kubios HRV software (Tarvainen et al., 2014). Given the within-subjects design and thus the need to perform each of the three tDCS sessions in different days, a change score was computed for each session by subtracting the baseline values for that specific session from the vmHRV values during stimulation or sham tDCS. Positive values reflect an increase from baseline to post-tDCS.
Word-fragment-completion task
The word-fragment-completion task has been previously used in studies on mental accessibility (e.g., Schimel et al., 2003; Zhong & Liljenquist, 2006). Thirty-five participants took part in a pilot study aimed at validating the stimuli used in the current version of the task. During this pilot task, 30 incomplete words, including those previously used in Ottaviani et al. (2018), appeared in random order in the center of the computer screen and remained visible until participants completed it. Words were chosen in a way that they could be completed either with a disgust-related word (with a cleaning/dirtiness meaning) or a nondisgust alternative (with a neutral meaning). Examples of stimuli include “S_ _ _NE” (sapone, “soap”; salone, “saloon”) and “DO_ _ _A” (doccia, “shower”; doppia, “double”). Respondents were simply asked to complete each item without any further instruction other than to do it as quickly as they could to avoid conscious deliberation.
From the pilot study, six diverse words were used in each session (anodic, cathodic, and sham; for a total of 18 different words); attention was given to the fact that the words chosen for the different sessions did not differ in terms of accessibility of the disgust-related meaning (the same number of participants needed to have completed them with a cleaning/dirtiness meaning in the pilot study). For each of the six words presented in random order, subjects had to write three letters in the consecutive empty spaces to complete the fragmented word. As in Ottaviani et al. (2018), to account for potential contamination as a result of cognitive ability, the ratio of target words the participants filled in as disgust-related to that of the total words completed was used in the analysis (R. E. Johnson & Steinman, 2009). Response latency was not assessed.
Moral task
After the first 10 min of tDCS, sentences describing immoral situations were shown in random order on the computer screen. Subjects were asked to rate the level of immorality of a selection of vignettes adapted from the validated set of moral foundations vignettes (Clifford et al., 2015; for details on the adaptation, see Ottaviani et al., 2018). Foundations concern dislike for others’ pain and suffering (care/harm), proportional fairness (fairness/cheating), group loyalty (loyalty/betrayal), deference to authority and tradition (authority/subversion), purity and contamination (sanctity/degradation), and domination and coercion (liberty/oppression; Haidt, 2013; Iyer et al., 2012).
One hundred eighty-eight participants took part in a preliminary study aimed at validating the set of vignettes in an Italian sample. A link to an online questionnaire was sent via institutional mailing lists and social media. Following the methodology of Clifford et al. (2015), participants were asked to evaluate the moral wrongness of each of the 92 vignettes on a Likert scale from 1 (not at all) to 5 (very much). Twenty-one vignettes per each experimental condition (anodal, cathodal, and sham) were selected so that the 63 vignettes with the highest scores were chosen for the final selection. On the basis of the score obtained during the preliminary study, the vignettes presented in the three experimental sessions were matched within each domain.
Within each group of 21 vignettes, there were three vignettes for each specific moral foundation that had been violated: physical animal care (n = 3; e.g., “You see a boy setting a series of traps to kill stray cats in his neighborhood”), emotional care (n = 3; e.g., “You see a man snickering as he passes by a cancer patient with a bald head”), physical human care (n = 3; e.g., “You see a girl throwing her hot coffee on a woman who is dating her ex-boyfriend”), authority (n = 3; e.g., “You see a boss who obligates his employees to eat at his brother’s fast food”), fairness (n = 3; e.g., “You see a referee favoring the team he supports”), liberty (n = 3; e.g., “You see a mother who forces her daughter to enroll in the faculty of medicine”), and sacrality (n = 3; e.g., “You see a man in a bar offering sex to anyone he meets”). Categories of “animal,” “emotional,” and “physical human care” are attributable to the altruistic domain, whereas “authority,” “fairness,” “liberty,” and “sacrality” belong to the deontological domain. Each vignette depicts a behavior violating a particular moral foundation and not others.
The task started with the following instructions appearing on the computer screen: Please rate how much, in your opinion, each of the following behaviors is morally wrong. To answer, please press the number on the computer keyboard that corresponds to the level of immorality from 1 = not at all to 5 = very much.
Each sentence appeared on the top of the computer screen followed by the rating scale to remind participants of the possible answers, and they remained visible until a response was given.
The score in each category (e.g., animal care) was computed as the sum of the scores obtained on three items belonging to the same moral category (range = 3–15). Then, the total score for each of the two domains (altruistic and deontological) was calculated as the average of the scores obtained in the categories belonging to that domain (e.g., in the case of altruistic domain, because it is composed of three categories, the sum of the animal care, emotional care, and physical human care scores was computed and then divided by three; differently, the total score for the deontological domain was divided by four because it is composed of four categories).
Data analysis
The analyses were carried out using IBM SPSS (Version 21). Differences of p < .05 were regarded as significant. Data were first checked for outliers, normality of variables, and violations of statistical assumptions of general linear models (GLMs). Moreover, given the implications of the current study for individuals with OCD, the variability and distribution of OC symptoms (i.e., scores on the OCI-R) in the sample was thoroughly investigated.
First, given that sex differences have been previously acknowledged in moral judgments (e.g., Fumagalli et al., 2010), vmHRV (Koenig & Thayer, 2016), and neural responses to disgust (Caseras et al., 2007), differences between men and women in the main variables of the study were examined by t test.
Second, to identify potential confounders, differences based on physical exercise and nicotine, alcohol, and medication intake on physiological variables were assessed by t tests. In the case of significant differences, these variables were included as covariates in the GLMs having physiological measures as outcome.
Third, to evaluate the effects of anodal, cathodal, and sham tDCS on disgust and morality, a series of GLMs with stimulation type as within-subjects factor were performed on the following variables: (a) change in affect rating for each of the examined items (explicit measure of disgust); (b) the ratio of disgust-related words over total recognized words to test for the accessibility of disgust-related information from memory (implicit measure of disgust); (c) change in HR and change in vmHRV (physiological indicators of disgust); (d) the average of scores attributed to altruistic vignettes (i.e., animal, emotional, and physical human care); and (e) the average of scores attributed to vignettes in the deontological domain (i.e., authority, fairness, liberty, and sacrality).
Finally, to investigate whether changes in levels of physiological and self-reported disgust and deontological morality after a specific stimulation would be intercorrelated and particularly present in participants with higher OC dispositional tendencies, Pearson correlations were performed between scores on the OCI-R, Fear of God, and Fear of Sin subscales of the PIOS-R, change in self-reported disgust, change in vmHRV, and moral judgment to the deontological vignettes in the anodal and cathodal conditions, separately.
Results
No adverse tDCS effects occurred with the exception of commonly reported side effects such as tingling and itching on the skin portion under the electrode. None of the participants were able to distinguish between stimulation conditions.
As to the variability of OC symptoms in the current sample, scores on the OCI-R were nonnormally distributed, with skewness of 0.81 (SE = 0.39) and kurtosis of 0.16 (SE = 0.77; see Table S1 and Fig. S1 in the Supplemental Material available online).
Sex differences and range values for baseline and dispositional variables are depicted in Table S2 in the Supplemental Material. Women were characterized by higher levels of depressive symptoms, t(34) = 2.62, p = .013, and trait anxiety, t(34) = 2.54, p = .016, compared with men. No other sex differences emerged.
No differences emerged in physiological variables based on age, smoking status, physical exercise, or alcohol or medication intake; therefore, the GLMs were performed without controlling for these potential confounders. With the exception of HR, all physiological variables were log transformed because of skewed distributions.
As illustrated in Table 1, the repeated measure GLMs yielded a significant effect of condition (sham, anodic, cathodic) in the models having dependent variables change in self-reported disgust, F(2, 70) = 5.38, p = .007, η p 2 = .13; change in vmHRV, F(2, 62) = 3.91, p = .02; η p 2 = .11; and morality judgments in the deontological domain, F(2, 70) = 4.37, p = .016, η p 2 = .11, and a marginally significant effect in the model having changes in self-reported deontological guilt as dependent variable, F(2, 70) = 2.63, p = .07, η p 2 = .07. No significant differences emerged in the models having changes in self-reported altruistic guilt and the ratio of disgust-related words over total recognized words as dependent variables. The minimum number of words completed with a cleaning/dirtiness meaning was zero in all conditions, and the maximum was five in the sham and cathodal conditions and six in the anodal condition.
Self-Reported, Physiological, Implicit, and Morality-Judgment Measures in the Three tCDS-Stimulation Conditions

Note: Values in parentheses are standard deviations. For self-reported measures, change was calculated by subtracting values recorded (on a 5-point scale) at baseline from values recorded after transcranial direct-current stimulation (tCDS). For physiological measures, change was calculated by subtracting values recorded at baseline from values recorded during tCDS. For morality judgments, averages were calculated (from values recorded on a 5-point scale) across the categories belonging to the indicated domain. HRV = heart rate variability.
Values for degrees of freedom are 2,70 (except for the physiological measures, for which they are 2,62).
p = .07. *p < .01.
As shown in Figure 1, self-reported levels of disgust increased in the anodal condition and decreased in the cathodal condition. Post hoc comparisons showed that the difference between the change in self-reported levels of disgust after anodal stimulation compared with sham stimulation was significant but small in size (d = 0.18), whereas the difference between cathodal and sham was of medium size (d = 0.54). Particularly, cathodal stimulation had stronger effects on self-reported levels of disgust compared with anodal stimulation (d = 0.67).
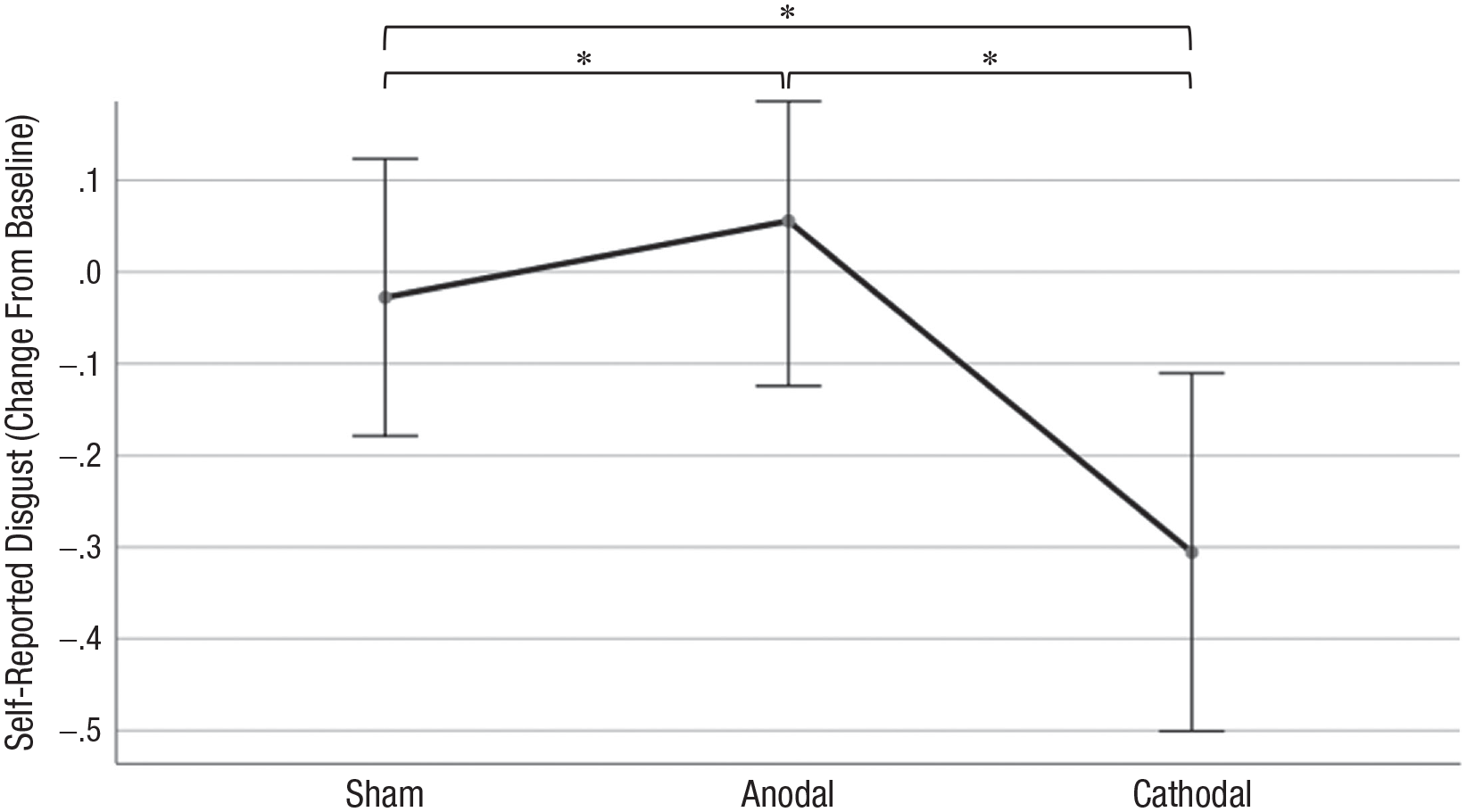
Effects of sham, anodal, and cathodal transcranial direct current stimulation on self-reported levels of disgust. Asterisks represent significant difference between conditions (p < 0.5).
Figure 2 illustrates differences in vmHRV change scores across the three conditions. Sham stimulation yielded different effects on vmHRV compared with both anodal (d = 0.24) and cathodal stimulations (d = 0.30), and the difference between the two types of active stimulation was of medium size (d = 0.65).
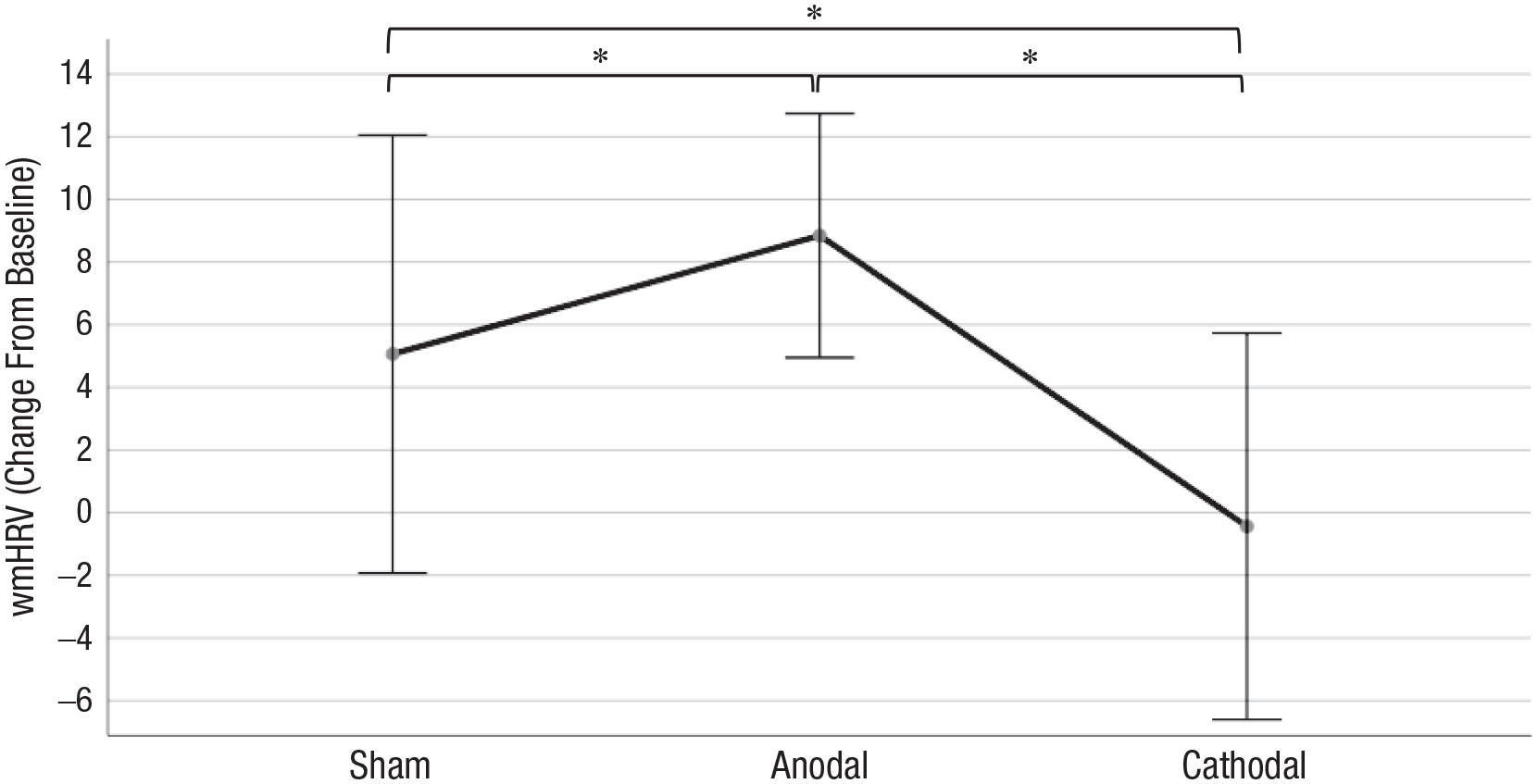
Effects of sham, anodal, and cathodal transcranial direct current stimulation on the physiological correlate of disgust (i.e., vagally mediated heart rate variability [vmHRV]). Asterisks represent significant difference between conditions (p < 0.5).
As to judgment about the deontological vignettes, a difference of small size emerged in the anodal and cathodal conditions compared with the sham condition (d = 0.09 and d = 0.26, respectively), whereas the difference between the two active conditions was of small to medium size (d = 0.36; see Fig. 3).

Effects of sham, anodal, and cathodal transcranial direct current stimulation on moral judgment in the deontological domain. The total score for “how much is it morally wrong” in this domain represents the average score. Asterisks represent significant difference between conditions (p < 0.5).
Note that during cathodal stimulation, change in vmHRV was positively correlated with judgments in the deontological domain during cathodal stimulation (r = .34, p = .04); change in self-reported disgust after cathodal stimulation was inversely correlated with washing (r = −.49, p = .002), obsessing (r = −.35; p = .037), and Fear of Sin subscales (r = −.48, p = .003). After anodal stimulation, change in self-reported disgust was positively correlated with scores on the OCI-R (r = .38, p = .022), as was change in self-reported deontological guilt with the checking (r = .41, p = .013), obsessing (r = .39, p = .018), and Fear of Sin (r = .49; p = .002) subscales. Moreover, judgment in the deontological domain during anodal stimulation was positively correlated with disgust sensitivity (r = .43, p = .010). No other significant associations emerged. Correlational results did not change when potential outliers were removed from the analyses.
Discussion
Given that the aforementioned results indicate that enhanced excitability in the insular cortex leads to increased feelings of disgust and moral rigidity (Ottaviani et al., 2018), in the present study, we hypothesized that reduction of insula excitability would lead to an opposite pattern of results. Indeed, a decrease of both disgust and moral severity by cathodal (inhibitory) tDCS over T3 was found. Particularly, self-reported and physiological measures provided convergent results with decreases in levels of disgust of small to medium effect size. This was accompanied by reductions in levels of moral rigidity only in the deontological domain and not in the altruistic one, as indicated by moral judgments about the vignettes. Note that the decrease in physiological levels of disgust (indexed by vmHRV) was significantly associated with the decrease in moral rigidity in the deontological domain. Current results also partially replicated those of Ottaviani et al. (2018): Anodal tDCS stimulation over T3 increased the severity of moral judgments in the deontological domain and elicited disgust as indicated by physiological and self-report measures but not by implicit measures.
Although the current study was conducted—for clear ethical reasons—on a sample of nonpathological individuals, results have potential implications for the treatment of OCD. As described previously, evidence suggests that disgust and deontological morality play a pivotal role in the genesis and maintenance of OCD and points to the role of the insula as one of the putative neural substrates underlying these constructs (e.g., for deontological guilt, see Basile et al., 2014; for disgust, see Viol et al., 2019). In light of this, Buyukturkoglu and colleagues (2015) conducted a promising pilot study using real-time fMRI feedback with the aim of training patients with contamination obsessions and washing compulsions to volitionally down-regulate blood-oxygen-level dependent (BOLD) activity in their anterior insula. At the end of the training, all patients were able to successfully decrease the BOLD signal in the insula in the presence of disgust-inducing stimuli. Furthermore, two out of the three participants improved their capability to bear the physical proximity of a real-world, disgusting, symptom-provoking object by employing the same successful cognitive strategies used during the down-regulation training. Although making straightforward conclusions from a study with such a limited number of participants is not advisable, this is a remarkable example of how down-regulation of a brain region represents a clinical method for promising treatments. Thus, noninvasive brain stimulation is increasingly used in psychiatry with therapeutic purposes (Brunoni et al., 2019).
Although our sample was composed of healthy individuals, given our aim to translate current results to a clinical population, we have looked at whether the effects were stronger in people with the dispositional traits typically associated with OCD, such as the tendency to engage in obsessions and compulsions, disgust sensitivity, deontological guilt, and scrupulosity (Ottaviani et al., 2013). In the anodal condition, the increase in self-reported levels of disgust was stronger for participants with higher scores on the OCI-R. Likewise, moral rigidity to deontological vignettes increased more in people having higher scores on the Fear of Sin subscale of the PIOS and on the checking and obsessing subscales of the OCI-R. In the cathodal condition, self-reported levels of disgust decreased more in participants with higher scores on the Fear of Sin subscale of the PIOS and on the washing and obsessing subscales of the OCI-R. In looking at these results, one has to consider that the distribution of scores on these questionnaires was skewed toward lower scores. However, correlational results did not change when potential outliers were removed from the analyses. Even given this potential limitation, these associations suggest that the effects of tDCS on disgust and deontological guilt were stronger in individuals with higher OC tendencies, which has promising clinical implications (Mancini, 2018; Power & Dalgleish, 2008). In fact, although it is known that tDCS has only short-lasting effects, long-term retention of the benefits can be achieved with multiple sessions (Boggio et al., 2008; Fregni, Boggio, et al., 2006). In case of successful replication, feasibility studies should be performed to establish the number and frequency of sessions needed to achieve stable results in individuals with OCD.
Further limitations need to be acknowledged. First, the elicitation of disgust was not confirmed by implicit measures (i.e., word completion task). Nonetheless, at a descriptive level, results went in the expected direction with fewer disgust-related words reported in the cathodal condition compared with the anodal and sham conditions. The absence of a significant effect for the implicit measure of disgust may be because the presence of three sessions required a higher number of incomplete words compared with those in Ottaviani et al. (2018). Despite our best attempt to match the words in the three conditions by running a small pilot study, it is still possible that disgust-related words of varied frequency of use were selected, and this confounder has been shown to affect performance on the word-fragment-completion test (Macleod & Kampe, 1996). A proper validation study for the stimuli to be used in the word completion task is warranted for future replication studies. A second major limitation concerns the lack of topographical selectivity in tDCS effect, which may label the observed findings as nonspecific. Another limitation is the characteristics of the sample. Although we attempted to extend advertisement among the general population via the use of social networks, the recruitment was carried out mainly within the university, thus the majority of the sample consisted of graduate and postgraduate students, which may weaken the generalization of the results. Furthermore, during the recruitment, there was no control on specific parameters (e.g., religious or political preferences). For this reason, the results of some scales and the judgment about some vignettes (e.g., the dominion of sanctity) may be questionable. For future studies, it would be of interest to use additional measurements of disgust that have been demonstrated to be reliable (i.e., electromyography to measure facial motor activity; Chapman et al., 2009). Because facial expression of disgust emotion is universal (Ekman & Friesen, 2003), this technique would be a more selective indicator of disgust (Gardhouse & Anderson, 2013) than vmHRV and word-fragment completion.
In conclusion, although the findings of the present study are promising in a therapeutic perspective, they need replication in a clinical sample. More importantly, mapping the brain correlates of deontological morality in OCD has to be further investigated before testing the feasibility of noninvasive brain stimulation techniques in a randomized controlled trial on patients with OCD. Overall, current experimental results support the intrinsic link between disgust and morality in the deontological domain and point to the insula as a crucial shared region for these two processes. If replicated, the present study suggests that it would be possible to enhance and dampen disgust sensitivity and rigidity in deontological morality by, respectively, increasing and decreasing cortical excitability in the insular region.
Supplemental Material
sj-pdf-1-cpx-10.1177_21677026211009508 – Supplemental material for Filthiness of Immorality: Manipulating Disgust and Moral Rigidity Through Noninvasive Brain Stimulation as a Promising Therapeutic Tool for Obsessive Compulsive Disorder
Supplemental material, sj-pdf-1-cpx-10.1177_21677026211009508 for Filthiness of Immorality: Manipulating Disgust and Moral Rigidity Through Noninvasive Brain Stimulation as a Promising Therapeutic Tool for Obsessive Compulsive Disorder by Giuseppe Salvo, Samantha Provenzano, Maria Di Bello, Francesca D’Olimpio, Cristina Ottaviani and Francesco Mancini in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Erin B. Tone
Editor: Kenneth J. Sher
Author Contributions
C. Ottaviani and F. Mancini developed the study concept and coordinated the project. F. D’Olimpio contributed to the study design. Testing and data collection were performed by G. Salvo, S. Provenzano, and M. Di Bello. Data analysis was performed by C. Ottaviani. G. Salvo drafted the manuscript, which all authors reviewed. All of the authors approved the final manuscript for submission.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.