
Abstract
Research suggests that individuals who are more depressed are prone to behaviors that reinforce their depressive symptoms. We performed a novel test of the self-verification perspective of this phenomenon. In two experiments, nonclinical participants completed a sham color-gazing task in which depressed people ostensibly see colors become less intense (less-intense condition) or more intense (more-intense condition) while gazing at them. Depression related to perceiving colors as turning less intense in the less-intense condition and more intense in the more-intense condition. These effects of depression (a) persisted after controlling for proneness for nondepressive negative affect or gender, (b) likely occurred without awareness, and (c) were not attributable to accuracy goals or opportunistic self-presentation goals. Depression also related to self-reported increased likelihood of possessing depression characteristics and rating them as more tolerable, and mediation evidence suggested that responses on the color-gazing task partly drove these reports.
Depression encompasses various symptoms that generally involve depressed mood, a loss of pleasure, lethargy, hopelessness, agitation, and difficulty concentrating (American Psychological Association, 2013). Hence, depression can be studied dimensionally to account for the severity of depression symptoms in nonclinical populations (e.g., depression severity or depression levels; Angst et al., 2000; Beck et al., 1996; Enns et al., 2001; Lewinsohn et al., 2000; Pilkonis et al., 2011) rather than studied as a categorical label. Although research on this matter is still ongoing, Haslam et al. (2012; also see Hankin et al., 2005) performed a quantitative review of taxometric research involving psychopathological constructs and concluded that mood disorders are best conceptualized as dimensional rather than categorical. In fact, most people in nonclinical samples experience at least some depression symptoms over an extended period, and the extent of these symptoms (indexed by validated dimensional depression measures) is associated with various important outcomes, including an increased risk of being diagnosed with major depression (Cuijpers et al., 2004; Cuijpers & Smit, 2008), reduced happiness (Cheng & Furnham, 2003), hindered job performance (Martin et al., 1996), and suicidal ideation (Cukrowicz et al., 2011). Along these lines, in the present research, we focused on depression as a dimensional construct that can influence the lives of nonclinical individuals.
Unfortunately, research on the interpersonal features of depression presents a rather bleak picture: People who are high in depression engage in behaviors that tend to reinforce depressive symptoms (Reinhard et al., 2020). Broadly, this reality can be contextualized in stress-generation and stress-exposure perspectives on depression (Hammen, 2016; Liu & Alloy, 2010). For example, people high in depression are prone to engage in various socially undesirable behaviors during interactions (e.g., reduced eye contact, inappropriate levels of self-disclosure, hostile voice, negative body gestures) that generate sources of dependent stress, such as rejection from audiences (Coyne, 1976a, 1976b; Hammen, 2016; Liu & Alloy, 2010). In turn, this stress can promote and reinforce features of depression such as negative self-views, pessimism, and depressed mood (Liu & Alloy, 2010; Reinhard et al., 2020). Essentially, people high in depression are seemingly trapped in an unfortunate feedback loop (Liu & Alloy, 2010). Depression inspires behavior that maintains and strengthens its unfortunate symptoms via the generation of dependent stress. To understand depression, psychological science must seek to understand this feedback loop (Giesler et al., 1996; Liu & Alloy, 2010).
To this point, Giesler et al. (1996) noted that psychology offers two broad and competing perspectives on why people high in depression might engage in some stress-generating behavior. On the one hand, the “ironic perspective”—which is considered the most widely endorsed explanatory perspective (Giesler et al., 1996)—says that this behavior is, ironically, intended to project an often positive identity and attain desired treatment (e.g., social acceptance). Unfortunately, because of an apparent lack of social skills and/or choosing inappropriate strategies to project a positive identity (e.g., defensive self-protection; M. G. Hill et al., 1986; Weary & Williams, 1990), their well-intentioned behavior backfires, and they receive negative social feedback from audiences. For example, according to one conception (Coyne, 1976a, 1976b; see also M. G. Hill et al., 1986), people high in depression may be trying too hard to make a good impression, so they can seem to possess a number of unattractive characteristics (e.g., insecure, defensive, and demanding) that cause them to be disliked and rejected.
On the other hand, the “self-verification perspective” claims that people high in depression are prone to engage in some stress-generating behavior to validate their depressed identity (Swann et al., 1987; Swann, Hixon, & De La Ronde, 1992; Swann & Read, 1981; Swann, Wenzlaff, et al., 1992). Self-verification theory (Swann, 2012) suggests that all people—even people with negative identities—are driven by a human motive to validate their identities. The theory is based in the undeniable reality that a coherent identity is necessary for basic human functioning (Swann, 2012). Identity grounds the physical body into the social matrix, so a coherent identity allows people to participate in social exchanges with feelings of predictability and control (Schlenker, 1980). To this perspective, being depressed is an identity that, like any identity, must be created and maintained, which entails monitoring and controlling symbolic expressions relevant to depression. Indeed, Swann, Wenzlaff, et al. (1992) proposed that depressed individuals’ reliance on negative thinking styles and their creation of stressful life events are part of a broader tendency to verify a depressed identity.
In sum, the ironic perspective and the self-verification perspective are opposing explanations for the same troubling phenomenon: People high in depression engage in behaviors that ultimately reinforce their depressive symptoms. Adjudicating between these perspectives is complicated but necessary to help clarify the foundations of depression. Unfortunately, these perspectives have been difficult to parse in research.
Consider some evidence that is offered to support the self-verification perspective and challenge the ironic perspective: People higher (vs. lower) in depression or features of depression (e.g., lower self-esteem) (a) seek more negative feedback about the self from others (Giesler et al., 1996; Joiner, 1995; Joiner et al., 1997), (b) show a greater preference for interacting with someone who evaluated them rather negatively (e.g., as unhappy and socially insecure) compared with positively (e.g., happy and socially secure; Swann, Wenzlaff, et al., 1992; Swann, Wenzlaff, & Tafarodi, 1992), (c) prefer their dating partners and friends to have a more tempered (vs. highly positive) view of them (Swann, Wenzlaff, & Tafarodi, 1992), (d) show a reduced preference for reading questions that probed others for positive versus negative self-relevant information (Swann, Wenzlaff, & Tafarodi, 1992), and (e) evaluate negative (vs. positive) self-relevant information as more accurate and also evaluate its author as more competent (Seih et al., 2013; Swann et al., 1987; Swann, Wenzlaff, et al., 1992; Swann, Wenzlaff, & Tafarodi, 1992).
But does this evidence necessarily support the self-verification perspective and challenge the ironic perspective? Perhaps the answer is no. In line with the ironic perspective, the depression-validating behavior in these studies can achieve various alternative goals that inadvertently (or ironically) produce rejecting social worlds. For example, people high in depression might avoid people that think they are happy and well adjusted because they fear letting these people down (M. G. Hill et al., 1986; Tortoriello & Hart, 2019; Weary & Williams, 1990); by contrast, people high in depression might seek out people that think they are unhappy and troubled because they believe they can ultimately impress these people (M. G. Hill et al., 1986; Tortoriello & Hart, 2019). Alternatively, perhaps people high in depression wish to avoid social interactions in the lab and assume that people who view them negatively will leave them alone (M. G. Hill et al., 1986). In addition, people high in depression might engage in self-effacing self-presentations (e.g., asking others for negative self-relevant information) in hopes of obtaining contrarian information (i.e., “fishing for compliments”; Coyne, 1976b; Schlenker, 1980) or sympathy from others (Fontana & Klein, 1968; M. G. Hill et al., 1986; Schlenker, 1980). Finally, people high in depression may tend to seek, process, and recall predominantly negative self-relevant information partly because they want accurate self-relevant information for accurate self-assessment (not necessarily self-verifying information; e.g., Trope, 1986). Unfortunately, accurate and self-verifying information are confounded in the aforementioned studies, so a self-verification process is obscured.
Nonetheless, prior studies have provided some strong evidence that depression-validating behaviors could reflect a self-verification process. For example, people high in depression showed a stronger preference for negative self-relevant information after they received identity-inconsistent information (i.e., positive feedback; Swann, Wenzlaff, & Tafarodi, 1992). This evidence is consistent with presuming the operation of a self-verification goal. Presumably, the self-verification goal was blocked by positive feedback and somewhat satisfied by negative feedback; hence, people high in depression were more motivated to achieve a self-verification goal under positive-feedback conditions compared with negative-feedback conditions. Moreover, when considering whether to interact with someone who evaluated them negatively compared with positively, a think-aloud protocol revealed that people high in depression mainly considered that the negative evaluator would be an attractive choice because this person would confirm their self-views (Swann, Stein-Seroussi, & Giesler, 1992).
In that light, in the present work, we provided novel tests that help to further differentiate between the self-verification and certain ironic-perspective explanations. Specifically, for theory-testing purposes, we relied on artificial experimental methods to ensure that self-verifying behavior is unlikely to shield the self from realizing negative information about the self, to manipulate an external audience in some desired way (e.g., get sympathy), or to obtain an unbiased and accurate perspective on the self’s realities.
Experiment 1
Nonclinical participants completed dimensional depression indices among various other measures of personality to distract from the study’s purpose. Participants were then misled into believing that the study on personality was over. At that point, under the guise of a mandate by an Institutional Review Board (IRB), participants were told that the research team had to provide them with an opportunity to complete a diagnostic measure for their own edification. The measure in question was framed as measuring their propensity to suffer from depression. In reality, the measure was bogus. It had participants gaze at colors and indicate how the colors’ intensity appeared to change. Color intensity actually did not change. As a between-subjects manipulation of symptom expression, participants were told that possessing a “depressed brain” is diagnosable from seeing colors turn less intense (less-intense condition) or more intense (more-intense condition). In this task, changes in intensity percepts merely symbolize depression propensity and can be used to verify or refute a depressed identity.
Note that by design, we did not study any real symptom of depression. Our methods were intended to be artificial because, as we have described, real-world situations naturally confound some features that are relevant to distinguishing between the self-verification perspective and ironic-perspective explanations, and we aimed to maximize internal validity for the sake of stronger theory testing; moreover, the depression-signaling behavior was intentionally benign (color perception) because, for ethical reasons, we did not see any need to compel changes in a consequential behavior (e.g., actual depression symptoms) when a benign behavior could be used to test the theory.
If people high in depression seek to confirm their depressed identity, they should adopt depression-consistent behaviors in private (Swann, 2012). According to the self-verification perspective, these identity-consistent behaviors are emitted to symbolize their depressed identity. If these ideas have merit, then people should privately change their behavior to express the bogus depression symptoms. Hence, self-verification theory anticipates an interaction between depression levels and the symptom-expression manipulation (i.e., condition, for short) on intensity ratings. In the less-intense condition, depression should relate negatively to intensity ratings; in the more-intense condition, depression should relate positively to intensity ratings. These effects of depression on intensity ratings should have downstream effects on people’s belief that they actually possess a depressed brain (Swann, 2012). Specifically, depression should relate positively to believing one possesses the depressed brain via self-reported changes in intensity ratings. Indeed, a critical assumption underlying the self-verification conception of depression is that depressed people can remain unaware of their role in creating their own symptoms and therefore trust this behavior as diagnostic for self-judgment (Swann, Wenzlaff, et al., 1992). Hence, we examined people’s belief that they actually possessed the depressed brain and also their conscious awareness of self-verifying behavior.
Critically, these data patterns anticipated by the self-verification perspective could not also be understood as straightforward attempts to (a) manipulate an external audience into providing favorable feedback (e.g., no audience is present), (b) self-protect against receiving negative information (e.g., the information being sought is delivered as such), or (c) acquire accurate information for objective self-assessment (e.g., people are distorting rather than accepting objective reality). If anything, in the context of this study, a version of the ironic perspective might suggest people high in depression would be less likely to adopt the artificial depression characteristics; if people high in depression are highly motivated to claim a positive identity (Coyne, 1976a) or are highly concerned about losing self-esteem (M. G. Hill et al., 1986), then they should be particularly likely to project a positive self-image in the context of this study. In this study, disclaiming a depression propensity requires no skill or aptitude and can be done with ease, if so desired. Hence, the present study offers a test that should help differentiate the self-verification perspective from some explanations that cohere with the ironic perspective.
Method
Sample characteristics, power analysis, and data quality
Our sample comprised U.S. undergraduate students enrolled in an introductory psychology course; students participated for partial fulfillment of a course requirement. Enrollment for the experiment was solicited on the psychology department’s participant pool website that informed participants the experiment would last about 30 min and involved completing self-report and cognitive measures.
Our choice of sample size was multiply determined. First, although interactions are usually small in psychological research and require large sample sizes to be detected, we were interested in testing for a “crossover” interaction and therefore assumed the interaction effect would be rather robust (f2 = .08; see Kwang & Swann, 2010). A power analysis suggested that 101 participants would provide .80 power (at α = .05) to detect such an effect size. Second, we ran a Monte Carlo power analysis for mediation effects and learned that a sample of 164 would provide .80 power (α = .05) to detect, in either study condition of this experiment, a mediation effect if the a, b, and c paths were about moderate in size (r = .30; Schoemann et al., 2017). Nonetheless, we recruited 371 participants to ensure more reliable and stable estimates. Participants completed attention checks (Oppenheimer et al., 2009) and bot checks to verify responders were not artificial. We excluded 20 cases for failing two of two additional attention checks in personality questionnaires that asked participants to indicate their attentiveness by selecting a specific scale response. One failed attention check could indicate an accidental response but otherwise careful responding, but two failed attention checks most likely indicate careless responding. We excluded one case for invariable responding and one case for being incomplete, resulting in a final sample of 349 (age: M = 18.53, SD = 0.95; 292 women; 81% White). The studies reported herein were approved by the University of Alabama IRB.
Procedure and materials
See Table 1 for descriptive statistics and correlations for all Experiment 1 variables. The experiment was completed online. Participants first read an informed consent document on the screen and consented to participate in the experiment by advancing. To mask our focus on depression, participants first completed a battery of randomly presented questionnaires that also included two depression measures: (a) the Beck Depression Inventory–II (BDI-II; Beck et al., 1996) comprising cognitive and somatic depression symptoms (Whisman et al., 2000) and (b) a computerized form of the Patient-Reported Outcomes Measurement Information System−Depression−Short Form (PROMIS-D-SF; Pilkonis et al., 2011). We are aware of some concern that depression severity inventories may be unreliable in college student samples when they are used to create discrete depression categories (Kendall et al., 1987; Zimmerman, 1986). When dimensional scores are collapsed into categories, people with scores close to category cutoff points can show minor deviations in their scores over time and change categories. But this does not necessarily mean that dimensional depression measures are unreliable. Indeed, Wang and Gorenstein (2013) reviewed test-retest reliability of (dimensional) BDI-II depression scores in student samples and found reliabilities ranging from good (r = .73) to excellent (r = .96) with a mean period of about 2 weeks between measurement periods. As a point of comparison, these test-retest reliability estimates are similar to what has been obtained with Big Five traits over similar test-retest measurement periods (Gnambs, 2014). In the battery of randomly presented questionnaires, participants also completed a Five Factor Model measure (IPIP-NEO-60; Maples-Keller et al., 2017), which included an index of Neuroticism (facets include anxiety, anger, depression, self-consciousness, vulnerability, and immoderation/impulsivity). We averaged IPIP-NEO-60 Neuroticism items for anger, anxiety, self-consciousness, vulnerability, and immoderation. We will refer to this composite as negative affect for brevity. Technically, negative affect measures dispositional, nondepressive negative affects.
Descriptive Statistics and Correlations Among Experiment 1 Variables

Note: BDI-II = Beck Depression Inventory–II (Beck et al., 1996); PROMIS-D-SF = Patient-Reported Outcomes Measurement Information System−Depression−Short Form (Pilkonis et al., 2011); depression = standardized average of the two depression indicators; intensity = average intensity ratings; AB1-brain possession = self-reported possession of an AB1-brain.
p ≤ .01.
Task 2 involved the self-verification task in which participants could self-signal possession or nonpossession of a depressed identity. Before beginning the task, participants were informed that the study was formally over and that the next task was for their own edification. As part of an ostensible IRB initiative, participants were told that researchers have been mandated to include short tasks at the end of their studies that allow for self-discovery. We provided this framing to ensure that participants would not view the task as a means for conveying their identity to the experimenter. It also reduced the possibility that participants would connect the task to the personality questionnaires. Next, participants were told that the task could diagnose people who possess an “AB1-brain,” which, unbeknownst to the participants, was a fictitious brain type we created for the study. Participants read that possessing an AB1-brain links to features of major depressive disorder (American Psychological Association, 2013) such as feeling like nothing you do really matters, experiencing less pleasure, having pessimistic outlooks on life and the future, and feeling persistently sad and empty. After receiving this description, participants were required to pass a manipulation-check item confirming they understood the attributes associated with possessing an AB1-brain.
Next, as a between-subjects manipulation, participants were randomly assigned to learn that possession of an AB1-brain is diagnosable by perceiving colors to become either less intense (less-intense condition) or more intense (more-intense condition) while gazing at them. All participants were then required to pass another manipulation-check item confirming they understood this information.
Finally, participants were told they would complete five trials of a color-gazing task in which they would gaze at a colored square presented on their screen for several seconds (each trial lasted 15 s) and then indicate whether the color seemed to become more or less intense during that time. The task was adapted from the task used by Hart et al. (2020), which assessed self-verification tendencies as a function of identifying as “authentic” (rather than depressed). As in this prior work, we presented participants with the ostensible average color-intensity ratings from past participants who did and did not have AB1-brains (i.e., cutoff norms). These ostensible ratings served as anchors from which participants could adjust their own intensity ratings. For example, the ostensible average color-intensity ratings of people with an AB1-brain in the less-intense condition indicated smaller values on a scale from −5 (much less intense) to 5 (much more intense) than people in the more-intense condition. Participants were not allowed to select 0 (no change) to cohere with the cover story that people should experience even minor changes in intensity. This methodological choice also reduced the possibility of satisficing. Indeed, “no-opinion” options in questionnaires encourage apathetic responding and discourage the expression of meaningful opinions (Krosnick et al., 2005).
We collapsed ratings across the five trials to create an overall intensity rating index. After five trials, participants reported the extent to which they believed they possessed an AB1-brain (AB1-brain possession; 1 = extremely unlikely to have an “AB1-brain”, 7 = extremely likely to have an “AB1-brain”) and the extent to which they felt like they were intentionally altering their intensity ratings (intentional alteration; 1 = not at all, 5 = extremely). Participants then provided demographics and were debriefed. As part of the debriefing, participants were informed that the AB1-brain and the color-gazing task were bogus and designed to assess a theory; they had to indicate understanding of this information via selecting a correct multiple-choice response on a subsequent screen. A subsequently presented debriefing sheet explained that we had to hide information from them to provide a strong theory test.
Analytic technique
We first contextualized the main analyses by examining descriptives for the depression scores and AB1-brain-possession scores. To avoid redundant analyses, we z scored and averaged the two highly related (r = .81) depression inventories.1,2 This composite depression measure (called depression) was used in the primary multiple regression analyses. Multiple regression techniques rely on several assumptions regarding data properties (e.g., linearity, normality of residuals, heteroscedasticity). In line with recommendations in Darlington and Hayes (2017), these assumptions were tested as a set: If the Bonferroni-corrected p value of the largest t residual in a regression model is less than .05, then an assumption has been violated. We present this information in the Notes section for the primary analyses to assure the reader that assumptions were met. These primary regression analyses investigated whether condition (less-intense vs. more-intense condition) moderated the effect of depression on intensity ratings. In the presence of moderation, we reported simple effects of depression at each level of condition and simple effects of condition at relatively high (+1 SD) and low levels (−1 SD) of depression along with Johnson-Neyman significance regions (Darlington & Hayes, 2017). Next, we tested whether depression related to reports of AB1-brain possession via how intensity was reported as a function of condition. We tested this mediation idea using PROCESS (Model 4, Hayes, 2013; for this approach to testing moderated mediation, see Hart et al., 2020). Direct and indirect effects were estimated with 5,000 resamples and with 95% confidence intervals (CIs) indicating the likely values of the indirect effect across bootstrapped resamples.
To the extent the main analyses supported the self-verification perspective, we performed multiple follow-up tests. Two tests examined whether the results were dependent on conscious awareness. For one of these tests, we examined the relation between depression and reports of conscious alteration. If self-verification effects are dependent on conscious awareness, we should find a positive quadratic relation between depression and reports of conscious alteration; that is, people low in depression and people high in depression should indicate altering their scores the most. For the other test, we reran the main analyses with only participants that indicated providing completely authentic responses (i.e., no conscious alteration) on the color-gazing task. If we were able to replicate the main findings with this subsample of participants, we would conclude that conscious awareness is not necessary to produce the effects.
Two additional tests accounted for some confounds of depression. The first of these tests accounted for what we termed negative affect (i.e., dispositional, nondepressive negative affect). Recall that the self-verification perspective presumes that people who are more depressed seek to verify their identity as more depressed on the color-gazing task. Yet if depression is confounded with a general proneness for negative affect, the effects of depression might be attributed to this general proneness rather than depression per se. This alternative interpretation can be tentatively ruled out if the anticipated effects of depression on intensity ratings remain after controlling for negative affect. The second of these tests accounted for the complicating effects of gender, which can be confounded with depression severity (Finan et al., 2009) and associated with some forms of stress-generating behavior (Liu & Alloy, 2010). If the effects of depression on intensity ratings remain after controlling for gender, we may tentatively rule out that effects of depression on intensity ratings merely reflect gender differences in claiming depressed identities. Moreover, because self-verification processes would presumably extend across genders (Swann, 2012), gender should fail to moderate the effects of depression on intensity ratings.
Results
Preliminary analyses: depression in the sample and AB1-brain possession
Note that although our sample means (see Table 1) and modes indicate generally low depression as indexed by both the BDI-II (mode = 7; scores ranging from 1 to 16 are considered low) and the PROMIS-D-SF (mode = 8; scores ranging from 8 to 16 are considered low), it would be incorrect to believe that maladaptive depression levels were not being represented. In fact, 74 participants (21% of the sample) had scores above 20 on the BDI-II, which qualify as at least moderately depressed (Beck et al., 1996). By the same token, 75 participants (21% of the sample) scored above 22 on the PROMIS-D-SF and therefore could be considered at least moderately depressed (Pilkonis et al., 2011). But as noted in the Analytic Technique section above, we ultimately collapsed the two depression measures to use in the primary analyses because of their extremely high correlation.
According to a one-sample t test, the mean AB1-brain-possession score (see Table 1) was significantly below the scale midpoint of 4, t(348) = 8.98, p < .001, suggesting participants generally did not believe they possessed the depressed brain. This is not surprising because the sample was nonclinical. But as shown in Table 1, depression related moderately to AB1-brain possession such that people with relatively lower depression scores (−1 SD) indicated an AB1-brain-possession scores that were well below 4 (M = 2.64), t(348) = −11.69, p < .001, but people with relatively higher depression scores (+1 SD) indicated AB1-brain-possession scores that were approximately equal to 4 (M = 3.82), t(348) = −1.50, p = .133.
Primary analyses
Intensity was submitted to a hierarchical regression with an interaction term. Condition (0 = less-intense condition, 1 = more-intense condition) and depression (continuous, z scored) were entered at Step 1; the interaction was entered at Step 2. 3 Step 1 (R2 = .04) revealed a main effect of condition (β = −0.21, p < .001), suggesting lower intensity in the more-intense condition. Depression had no main effect on intensity (β = −0.04, p = .475). The interaction at Step 2 was significant and about large in size (β = 0.47, p = .002, R2 = .12). As shown in Figure 1, depression related negatively to intensity in the less-intense condition (β = −0.35, p < .001) and positively to intensity in the more-intense condition (β = 0.36, p < .001).
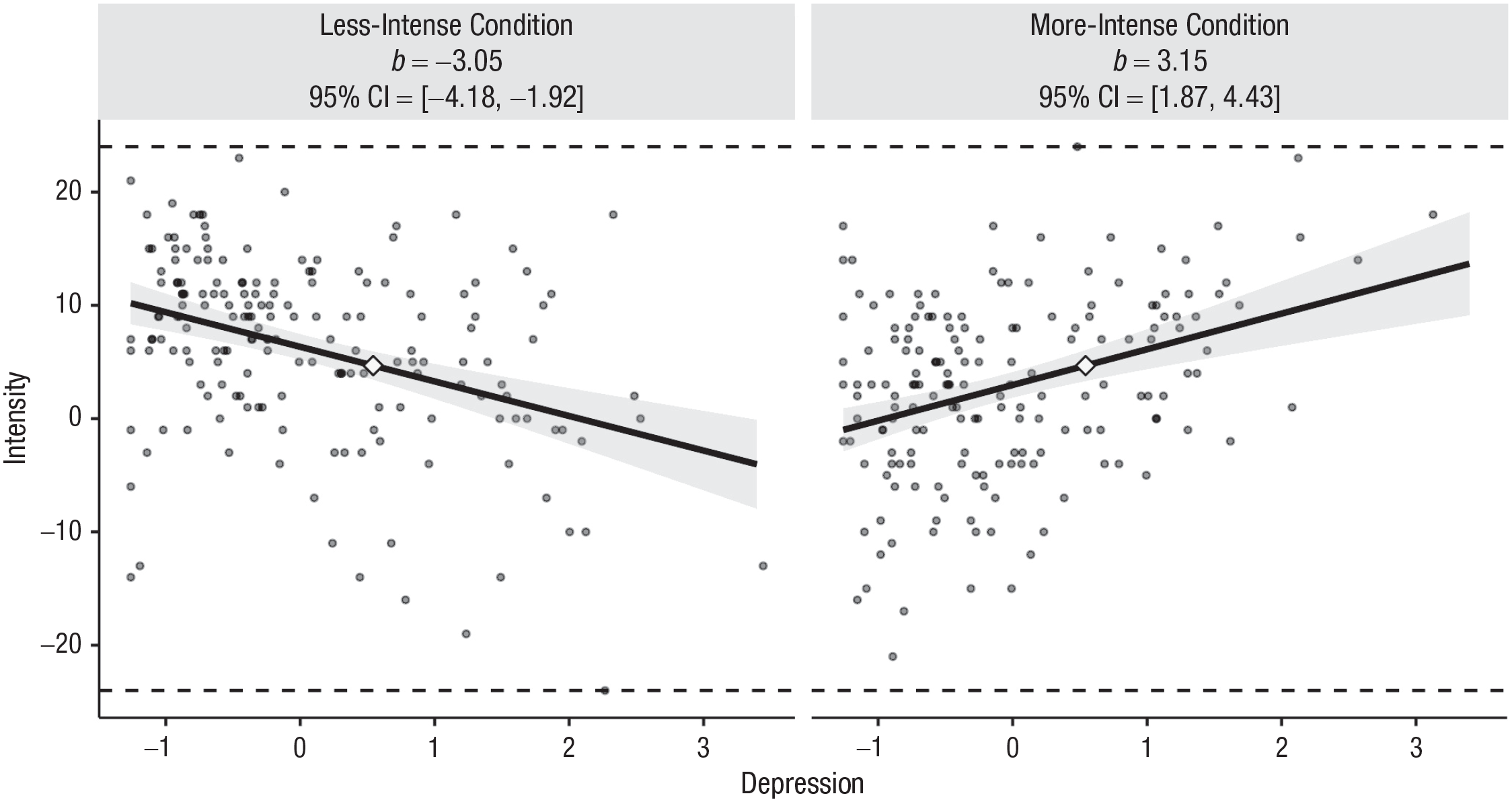
Scatterplots (with best-fitting regression lines) illustrating the Depression × Condition interaction in Experiment 1. Simple slopes for the effect of depression in each condition are displayed; b = unstandardized regression coefficient. Each graph displays the minimum/maximum values of the outcome (horizontal dashed lines), observed data points (gray circles), the crossover point (diamond), and the 95% confidence band (shaded area). The x-axes represent observed depression scores in standard deviation units. Illustrations generated by interActive (McCabe et al., 2018).
To further understand the nature of this interaction, we examined the simple effect of condition at relatively high (+ 1 SD) and low (−1 SD) levels of depression. At relatively high depression, the simple effect of condition was positive (β = 0.15, p = .030), which indicates the reporting of intensity in a way that would make a person seem depressed; by contrast, at relatively low depression, the simple effect of condition was negative (β = −0.56, p < .0001), which indicates the reporting of intensity in a way that would make a person seem nondepressed. Relatedly, we ran the Johnson-Neyman test of significance regions and found that the effects of condition on intensity first became significantly positive for depression scores at the 80th percentile of depression in our sample and first became significantly negative for scores at the 67th percentile of depression in our sample. These tests, together, show that effects of condition diverged across participants with relatively high and low depression and, in turn, suggest that effects of condition are relevant to both participants with relatively high depression and low depression in our sample.
Finally, we isolated the 74 participants that scored above 20 on the BDI-II and therefore qualified as at least moderately depressed (Beck et al., 1996). For these participants, we found higher intensity in the more-intense condition (M = 8.51, SD = 6.22; n = 33) than in the less-intense condition (M = 2.02, SD = 9.26; n = 41), F(1, 72) = 11.88, p = .001, d = 0.82. Similar effects were obtained when we isolated the 75 participants that scored above 22 on PROMIS-D-SF (i.e., could be considered moderately depressed; Pilkonis et al., 2011); we found higher intensity in the more-intense condition (M = 7.31, SD = 6.92; n = 35) than in the less-intense condition (M = 1.15, SD = 10.31; n = 40), F(1, 73) = 8.96, p = .004, d = 0.70. This suggests that people who can be categorized as at least moderately depressed showed approximately large tendencies to engage in responses that would suggest a depressed identity. Despite potential problems with categorizing participants according to dimensional depression measures collected at a single time point (Zimmerman, 1986), these data are consistent with the simple effect estimates from the full regression that relied on dimensional depression scores. To assuage concerns further, we attempted to replicate these patterns in Experiment 2.
Next, to evaluate mediation, we examined whether depression related to reports of AB1-brain possession via how intensity was reported differently as a function of condition. Specifically, AB1-brain possession was the outcome, depression was the exogenous predictor, the Intensity × Condition interaction was the mediator, and condition and intensity ratings were covariates. Indirect effects were estimated with 5,000 resamples and with 95% CIs indicating the likely values of the effect across bootstrapped resamples. The model, overall, accounted for a significant and large amount of variance in AB1-brain-possession scores, F(4, 344) = 47.45, p < .001, R2 = .36. The 95% CI for the indirect effect did not contain zero, suggesting significant mediation (indirect effect = 0.29, SE = 0.05, 95% CI = [0.19, 0.39]). This mediation evidence is consistent with, but does not prove, that people with higher depression scores reported higher AB1-brain-possession scores because they altered their intensity ratings in a way that symbolized a greater chance of having an AB1-brain compared with not having an AB1-brain. Mediation aside, there was still a direct effect of depression on AB1-brain-possession score (b = 0.33, SE = 0.08, p < .0001). Regardless of how people completed the task, people higher in depression reported a greater likelihood of having an AB1-brain.
Intentional alteration
The grand mean for intentional alteration was 1.79 (SD = 1.00); 53% of the sample (184 participants) indicated a 1 (completely authentic responders). Hence, for the most part, participants did not feel they were altering their responses. This finding is important because although we did compel people to indicate some change in intensity, people did not generally indicate feeling as if they were being compelled. We used regression to examine whether depression showed a positive quadratic relation to intentional alteration. The linear effect was nonsignificant (β = 0.02, p = .789, R2 = .000), but the quadratic effect was significant but negative (β = −0.16, p = .016, R2 = .02). This means that participants with the highest and lowest scores in depression—that is, participants who changed their intensity ratings the most as a function of symptom-expression condition—showed the strongest tendencies to deny altering their responses. This pattern is of course inconsistent with assuming that the self-verification behavior associated with depression was accompanied by conscious awareness.
A strong test of whether intentional alteration is necessary to explain the interactive effect of depression and condition on intensity ratings involves analyzing the data with the completely authentic responders (53% of the sample). We reran the primary regression analyses with this subsample again. The findings from the subsample were replicated in the findings from the full sample. Specifically, condition significantly moderated effects of depression on intensity (β = 0.50, p < .001, R2 = .14). Moreover, we were able to replicate the mediation evidence. There was still a significant indirect effect of depression on AB1-brain possession via how intensity was reported differently as a function of condition (indirect effect = 0.28, SE = 0.08, 95% CI = [0.14, 0.43]). Finally, there was still a direct effect of depression on AB1-brain possession (b = 0.31, SE = 0.11, p = .004).
Complicating effects of negative affect and gender
Negative affect
Are effects of depression on intensity ratings distinct from negative affect? Analyses pertaining to this question involve the full sample. Negative affect about strongly related to depression, r = .49. To address this confounding, we used linear regression with interaction terms to predict intensity. Condition, negative affect, and depression were entered at Step 1; the three two-way interactions were entered at Step 2. The three-way interaction was not examined because we had no theoretical grounds for testing it. Critically, the Depression × Condition interaction effect remained significant at Step 2 (β = 0.45, p < .001); no effects involving negative affect approached significance in the model (all ps > .37). Hence, negative affect cannot account for the effects of depression on intensity.
Gender
Analyses pertaining to gender effects involved the full sample. A one-way analysis of variance (ANOVA) showed that men (M = −.39, SD = .75) had lower depression scores than women (M = .08, SD = .97), F(1, 347) = 11.63, p = .001, R2 = .032. To address the confounding of gender and depression, we used linear regression with interaction terms to predict intensity. Condition, gender, and depression were entered at Step 1; all two-way interactions were entered at Step 2; and the three-way interaction was entered at Step 3. Critically, the Depression × Condition interaction effect remained significant at Step 2 (β = 0.48, p < .001); no effects of gender approached significance in the model (all ps > .28). Hence, gender cannot account for the effects of depression on intensity ratings, nor did gender moderate effects of depression on intensity ratings. Nonetheless, because of the low number of men in the sample, these null effects of gender should be considered tentative and require replication.
Discussion
Experiment 1 confirmed predictions from the self-verification perspective. People higher in depression altered their reports of intensity to claim a depressed brain, whereas people lower in depression altered their reports of intensity to disclaim a depressed brain. Hence, after the bogus test, people high in depression were more likely to feel like they had a depressed brain. These effects of depression could not be attributed to depression’s confounding with nondepressive negative affect or gender. Generally, participants seemed unaware they were altering their intensity ratings, and self-verification effects were present even among people who indicated providing completely authentic responses. If people’s self-reports of intentional alteration can be trusted and participants had no strong incentive to lie about them, then the findings suggest that the self-verification behavior occurred without awareness. Experiment 2 continued to probe this idea, but we changed the phrasing of the intentional alteration item to convey a more specific meaning. Rather than ask participants whether they altered their responses, we asked them whether they altered their responses to seem as if they had an AB1-brain.
A demand interpretation of the data stipulates that participants knew our hypotheses and intentionally engaged in behavior to confirm them. This interpretation is unlikely for at least four reasons. First, the present study took various steps to reduce demand. We measured various individual differences in addition to depression (e.g., agreeableness) to mask any interest in studying a correspondence between depression and behavior on the color-gazing task. Moreover, the color-gazing task was framed as irrelevant to our ostensible goal to catalog personality and was framed as a reaction to an IRB mandate to allow students to learn about themselves. Second, it is entirely unclear that our hypotheses would be apparent to participants so that they could confirm them: How would participants know to confirm a self-verification hypothesis over an ironic-perspective hypothesis? Third, if participants in the study felt generally compelled by demand to provide inauthentic responses on the color-gazing task, then participants should have indicated high levels of inauthentic responding to accommodate demand. Of course, they did not. Fourth, in reality, demand effects dictating results is more lore than empirical fact (McCambridge et al., 2012). In computerized studies like this one without a researcher physically present, even very strong demand effects are probably inconsequential. For example, without a researcher in sight, when participants were explicitly told a researcher’s hypothesis compared with not being told this hypothesis, results of the study went unchanged (Mummolo & Peterson, 2019).
In Experiment 2, we sought to conceptually replicate the main findings from Experiment 1 and advance them in two ways. First, because participants completed two depression measures before performing the self-verification (color-gazing) task, the self-verification effects might be contextualized to specific situations that entail first acknowledging a depressed or nondepressed identity. Although this limitation is not troubling for theory testing, it would suggest that our findings are limited to situations that make a depressed or nondepressed identity salient. To check on this matter, participants completed the color-gazing task before completing depression measures.
Second, we addressed the role of a “tolerance process” that may occur as a function of self-verification behavior. The self-verification of a depressed identity runs counter to self-enhancement motivation (Swann, Wenzlaff, Krull, & Pelham, 1992; Swann, Wenzlaff, & Tafarodi, 1992), and it has been suggested that self-enhancement strivings are muted but still present among people high in depression (Giesler et al., 1996; Pelham, 1991). When self-verification and self-enhancement motives clash, self-verification is usually fulfilled via overt behavior, and self-enhancement is usually fulfilled via trivializing the implications of that overt behavior (Giesler et al., 1996). So, in the current study, people high in depression can both (a) self-verify possession of a depressed brain via their behavior and (b) be less disturbed by this behavior if they trivialize the downsides of possessing this brain. Hence, we asked participants the extent to which a depressed brain is likely to benefit them. It is possible that depression will relate to heightened benefit ratings of the brain via behavior that claims the brain (i.e., altered intensity ratings as a function of condition).
Experiment 2
Method
Sample characteristics, power analysis, and data quality
We used the same recruitment procedure described in Experiment 1 to obtain our sample for Experiment 2. The large interaction effect in Experiment 1 (f2 = .13) informed our power analysis. A power analysis suggested that a sample size of 63 would provide .80 power (α = .05) to detect such an effect size. This sample size might be appropriate for power but was unlikely to support stable estimates of effects or be appropriate for testing mediation, which we estimated could require a sample of 164 (see Experiment 1). So, we recruited 220 participants to obtain at least 200 participants for the final analysis after exclusions. Participants completed the same preliminary attention checks and bot checks from Experiment 1. Ten cases were excluded for failing two of two attention checks nested in the personality questionnaires (see Experiment 1). Six cases were excluded as incomplete. The final sample was 204 (age: M = 18.87, SD = 1.29; 136 women; 84.8% White).
Procedure and materials
See Table 2 for descriptives and correlations for all Experiment 2 variables. Participants provided their informed consent as described in Experiment 1. Next, participants completed the color-gazing task from Experiment 1. The task was once again framed as part of the IRB mandate, but to justify its placement at the beginning of the experiment, we explained that the mandate dictated researchers include these tasks at the start of the session so that people that do not finish the experiment can still benefit. As in Experiment 1, participants were required to pass the two manipulation-check items indicating their understanding of the characteristics of the AB1-brain and how it can be diagnosed from the task. In addition, participants completed a question regarding their authentic responding (−5 = very much tried to change my responses to seem as if I did not have an “AB1-brain,” 5 = very much tried to change my responses to seem as if I did have an “AB1-brain”) and a question regarding the extent to which they perceive benefits to possessing an AB1-brain (1 = not at all, 7 = very much), which assessed AB1-brain benefit. Next, as in Experiment 1, participants completed a randomized battery of personality questionnaires that included the BDI-II (Beck et al., 1996) and the PROMIS-D-SF (Pilkonis et al., 2011) to index depression as well as the IPIP-NEO-60 (Maples-Keller et al., 2017) that included the items we used to create negative affect. Finally, participants completed demographics and were thoroughly debriefed following the same procedure as in Experiment 1.
Descriptive Statistics and Correlations Among Experiment 2 Variables

Note: BDI-II = Beck Depression Inventory–II (Beck et al., 1996); PROMIS-D-SF = Patient-Reported Outcomes Measurement Information System−Depression−Short Form (Pilkonis et al., 2011); depression = standardized average of two depression indicators; intensity = average intensity ratings; AB1-brain possession = self-reported possession of an AB1-brain; AB1-brain benefit = self-reported benefit of possessing an AB1-brain.
p ≤ .05. **p ≤ .01.
Analytic technique
We relied on the same analytic technique as in Experiment 1.
Results
Preliminary analyses: depression in the sample, AB1-brain possession, and AB1-brain benefit
Although our sample means (see Table 2) and modes indicated generally low depression as indexed by both the BDI-II (mode = 11) and the PROMIS-D-SF (mode = 8), maladaptive depression levels were still represented. In fact, 55 participants (27% of the sample) had scores above 20 on the BDI-II, which qualify as at least moderately depressed (Beck et al., 1996). By the same token, 61 participants (30% of the sample) scored above 22 on the PROMIS-D-SF, which qualify as at least moderately depressed (Pilkonis et al., 2011). As in Experiment 1, we z scored and averaged the highly related (r = .80; see Table 2) BDI-II and PROMIS-D-SF into a composite depression measure, which we used in analyses.
According to a one-sample t test, the mean AB1-brain-possession score (see Table 2) was significantly below the scale midpoint of 4, t(203) = −5.28, p < .001, suggesting that participants did not generally believe they possessed the depressed brain. But as shown in Table 2, depression was moderately related to AB1-brain possession, such that people with relatively lower depression (−1 SD) indicated AB1-brain-possession scores that were below 4 (M = 3.03, SE = 0.14), t(202) = −6.76, p < .001, but people with relatively higher depression (+1 SD) indicated AB1-brain-possession scores approximately equal to 4 (M = 3.89, SE = 0.14), t(202) = −0.77, p = .444.
According to a one-sample t-test, the mean AB1-brain-benefit rating (see Table 2) was significantly below the scale midpoint of 4, t(203) = −17.76, p < .001, suggesting that participants did not generally believe the depressed brain was beneficial. As shown in Table 2, depression was rather weakly (albeit significantly) related to AB1-brain-benefit ratings, such that people with relatively lower depression (−1 SD; M = 2.16, SE = 0.13) and higher depression (+1 SD; M = 2.59, SE = 0.13) indicated AB1-brain-benefit ratings below 4, t(202) = −13.96, p < .001 and t(202) = −10.69, p < .001, respectively.
Primary analyses
Intensity was submitted to a regression with depression (z scored, continuous) and the symptom-expression condition (condition: 0 = less-intense condition, 1 = more-intense condition) at Step 1 and their interaction at Step 2. 4 Step 1 (R2 = .01) revealed a null effect of condition (β = −0.09, p = .204) and depression (β = −0.01, p = .868). The interaction at Step 2 was significant and about moderate in size (β = 0.35, p = .001, R2 = .06). As shown in Figure 2, depression related negatively to intensity in the less-intense condition (β = −0.27, p = .008) and positively to intensity in the more-intense condition (β = 0.21, p = .024).
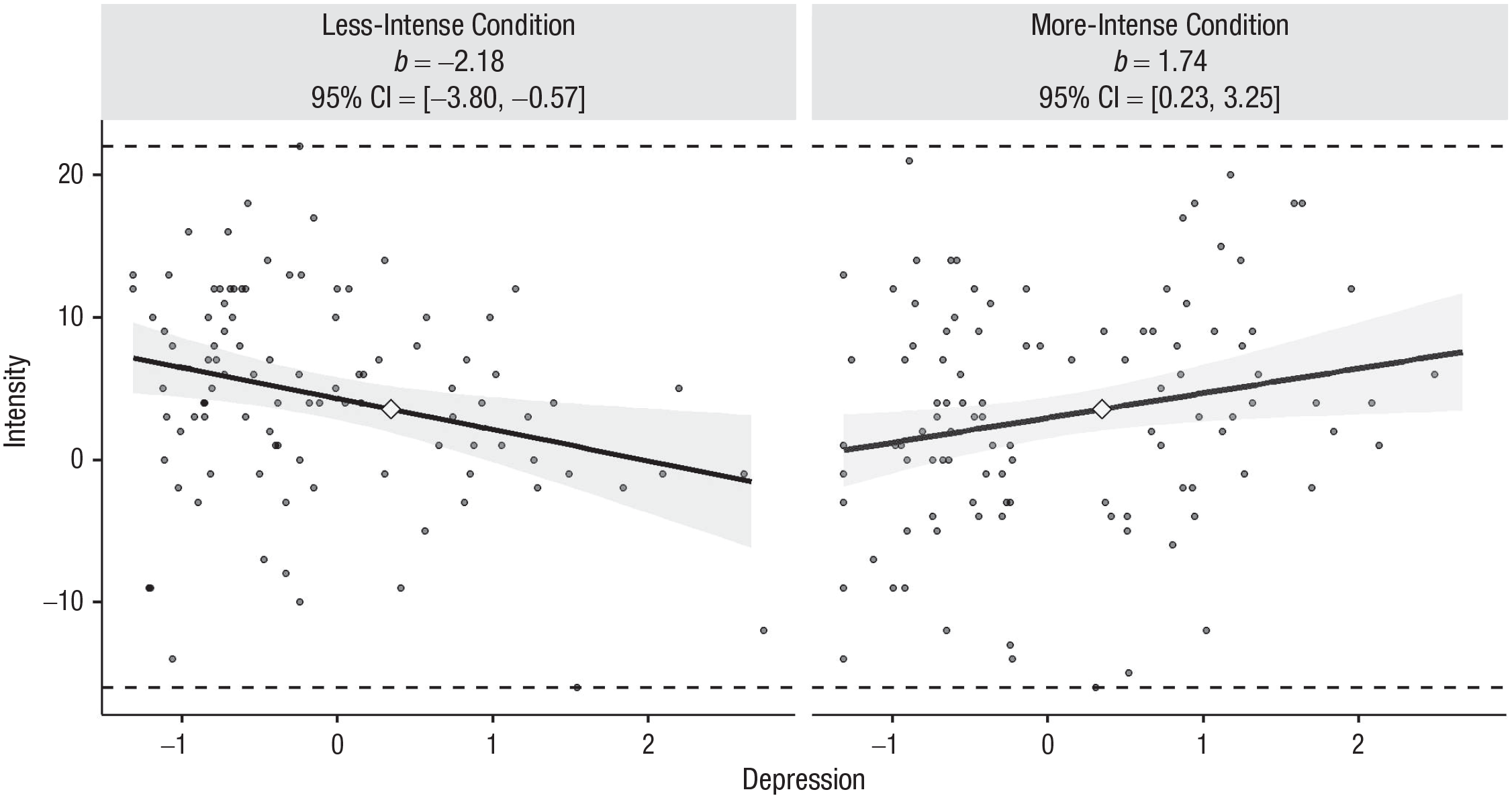
Scatterplots (with best-fitting regression lines) illustrating the Depression × Condition interaction in Experiment 2. Simple slopes for the effect of depression in each condition are displayed; b = unstandardized b coefficient. Each graph displays the minimum/maximum values of the outcome (horizontal dashed lines), observed data points (gray circles), the crossover point (diamond), and the 95% confidence band (shaded area). The x-axes represent observed depression scores in standard deviation units. Illustrations generated by interActive (McCabe et al., 2018).
As in Experiment 1, the simple effect of condition for participants at +1 SD from the mean on depression was positive (albeit nonsignificant; β = 0.15, p = .118), which reflects the reporting of intensity in a way that would make a person seem depressed; by contrast, the simple effect of condition for participants at −1 SD from the mean on depression was negative (β = −0.33, p = .001), which indicates the reporting of intensity in a way that would make a person seem nondepressed. Furthermore, a Johnson-Neyman test of significance regions revealed that the effects of condition on intensity first became significantly positive for depression scores at the 87th percentile (i.e., +1.2 SD from the mean) and first became significantly negative for depression scores at the 55th percentile. These findings are similar to those in Experiment 1.
Finally, we isolated the 55 participants that scored above 20 on the BDI-II. This subsample revealed nonsignificantly higher intensity in the more-intense condition (M = 5.03, SD = 8.46; n = 33) than in the less-intense condition (M = 1.27, SD = 6.52; n = 22), F(1, 53) = 3.10, p = .084, d = 0.62. We found similar but significant effects when we isolated the 61 participants that scored above 22 on PROMIS-D-SF; that is, we found higher intensity in the more-intense condition (M = 6.06, SD = 7.87; n = 35) than in the less-intense condition (M = 1.23, SD = 6.14; n = 26), F(1, 59) = 6.73, p = .012, d = 0.68. As in Experiment 1, these effects were nontrivial and were moderate to large in size. In sum, as in Experiment 1, the data were consistent with the idea that participants with relatively elevated levels of depression in our sample or participants who can be categorized as at least moderately depressed exhibited tendencies to engage in responses that would symbolize a depression propensity.
Next, as in Experiment 1, we examined whether depression related to reports of AB1-brain possession via how intensity was reported differently as a function of condition. The mediation model was identical to the mediation model described in Experiment 1. As in Experiment 1, the model accounted for a significant and large amount of variance in AB1-brain possession, F(4, 199) = 22.96, p < .001, R2 = .32. The 95% CI for the indirect effect did not contain zero, suggesting significant mediation (indirect effect = 0.17, SE = 0.06, 95% CI = [0.07, 0.29]). The data are therefore consistent with the idea that people higher in depression reported higher AB1-brain possession because they altered their intensity ratings to symbolize a greater chance of having an AB1-brain compared with not having an AB1-brain. Note that there was still a direct effect of depression on AB1-brain possession in the model (b = 0.24, SE = 0.09, p = .010).
Next, we examined whether depression related to reports of AB1-brain benefit via how intensity was reported differently as a function of condition. The mediation model was the same as the one used above except AB1-brain benefit was inserted as the lone outcome. Overall, the model accounted for a significant and moderate amount of variance in AB1-brain-benefit ratings, F(4, 199) = 7.13, p < .001, R2 = .13. The 95% CI for the indirect effect did not contain zero, suggesting significant mediation (indirect effect = 0.11, SE = 0.04, 95% CI = [0.04, 0.19]). The data are therefore consistent with the idea that people higher in depression reported higher AB1-brain-benefit ratings because they altered their intensity ratings in a way that symbolized a greater chance of having compared an AB1-brain with not having an AB1-brain. Depression had no direct effect on AB1-brain-benefit ratings (b = 0.11, SE = 0.09, p = .264).
Intentional alteration: analyses with only authentic responders
The grand mean for intentional alteration was 0.05 (SD = 1.10); 67% of the sample (137 participants) indicated a 0 (completely authentic responders). As in Experiment 1, although we compelled participants to indicate some change in intensity, participants did not report feeling as if they were giving inauthentic responses. Depression was unrelated to intentional alteration (see bivariate correlation in Table 2), suggesting self-verification effects attributed to depression were not accompanied by conscious awareness. This also speaks against an experimenter-demand interpretation.
We reran the primary analyses with only participants who indicated 0 on intentional alteration. In analyses with this subsample, we were able to replicate the main findings discussed from the full sample. Specifically, condition significantly moderated effects of depression on intensity (β = 0.32, p = .006, R2 = .05). Moreover, the mediation models revealed a significant indirect effect of depression on AB1-brain possession (indirect effect = 0.17, SE = 0.07, 95% CI = [0.05, 0.32]) and on AB1-brain benefit (indirect effect = 0.10, SE = 0.05, 95% CI = [0.02, 0.21]) via how intensity was reported differently as a function of condition.
Complicating effects of negative affect and gender
Negative affect
Analyses pertaining to negative affect involve the full sample. As in Experiment 1, negative affect about strongly related to depression, r = .47. To address this confounding, as in Experiment 1, we used linear regression with interaction terms to predict intensity. Condition, negative affect, and depression were entered at Step 1, and the three two-way interactions were entered at Step 2. As in Experiment 1, the three-way interaction was not tested. Critically, the Depression × Condition interaction effect remained significant at Step 2 (β = 0.39, p = .001); no effects involving negative affect approached significance (all ps > .39). Hence, as in Experiment 1, negative affect cannot account for the effects of depression on intensity.
Gender
Analyses pertaining to gender effects involve the full sample. A one-way ANOVA showed that men (M = −.16, SD = .83) had nonsignificantly lower depression scores than women (M = .08, SD = .99), F(1, 202) = 2.89, p = .091, R2 = .014. We addressed gender’s role as a confounder and moderator for effects of depression on intensity, as in Experiment 1. Condition, gender, and depression were entered at Step 1; all two-way interactions were entered at Step 2; and the three-way interaction was entered at Step 3. Critically, the Depression × Condition interaction effect remained significant at Step 2 (β = 0.36, p < .001); no effects of gender approached significance (all ps > .13). Hence, as in Experiment 1, gender cannot account for the effects of depression on intensity, nor did it moderate effects of depression on intensity. But because this sample underrepresented men, the data are not entirely conclusive on the matter.
Discussion
In Experiment 2, we were able to conceptually replicate the evidence of self-verification of a depressed identity. Participants higher (vs. lower) in depression reported perceiving color as less intense when they were told a depressed brain makes colors appear less intense but reported perceiving color as more intense when they were told a depressed brain makes colors appear more intense. As in Experiment 1, these effects of depression could not be attributed to gender or negative affect. Moreover, as in Experiment 1, this self-verification behavior had implications for convincing people higher in depression that they had a greater likelihood of possessing a depressed brain. Building on Experiment 1, Experiment 2 also showed that self-verification behavior had implications for tolerating a depressed brain. Specifically, as anticipated, the self-verification of possessing a depressed brain coincided with trivializing the dysfunction of having such a brain. Presumably, this trivialization helped minimize threats to self-enhancement striving, which are thought to be present, albeit diminished, at high depression levels (Giesler et al., 1996; Pelham, 1991). Once again, the vast majority of participants indicated not altering their behavior on the color-gazing task, and analyses with completely authentic responders failed to change any patterns in the data or any of the main statistical conclusions. Hence, conscious awareness does not seem necessary to produce the present effects.
General Discussion
People with elevated levels of depression tend to engage in behaviors that reinforce depressive symptoms. Although this phenomenon is complicated (Liu & Alloy, 2010), in the present article, we examined it in the context of an identity-maintenance process specified by a self-verification perspective. Across two experiments, people high in depression engaged in strategic behavior that entailed adopting faux symptoms of depression. Moreover, this strategic behavior felt genuine and contributed to the belief that one possessed characteristics of depression and that these characteristics were more tolerable. It is unlikely that the observed self-verification effects are manifestations of people’s opportunistic self-presentation (e.g., behavior was conveyed in private and information conveyed via computer rather than a human), people’s search for the truth, realism on behalf of people high in depression (e.g., altering reality was present), self-protection (no fear of failure on the task could possibly exist), or any organic defect of depression per se. Instead, it is likely that the observed self-verification behavior is being appropriately labeled as such: The strategic behavior appears to be a manifestation of people’s tendencies to confirm their self-beliefs about their own depression levels. Presumably, people sought to validate these self-beliefs because they wished to believe in a predictable and coherent self, which is necessary to anticipate control over one’s social endeavors and engage in culture (Baumeister, 2005; Swann, 2012).
But to what extent were people with high levels of depression prone to adopt faux depression symptoms in our experiments? In both Experiments 1 and 2, the simple effect of condition on intensity ratings for people relatively high in depression (defined as +1 SD from the mean in our sample) was β = 0.15 (i.e., ds = 0.33, 0.31 for Experiments 1 and 2, respectively), which indicates a small to medium effect (Cohen, 1988). But our depression index was a composite of BDI-II and PROMIS-D-SF, and—as can be gleaned from Tables 1 and 2—scores that are +1 SD from the mean on either BDI-II or PROMIS-D-SF are only slightly beyond cutoffs for moderate depression. So, we examined the simple effect of condition on intensity ratings for people with depression scores that were +2 SD from the mean in our samples; consider that scores that were +2 SD from the mean on either BDI-II or PROMIS-D-SF in Experiments 1 and 2 would be toward the low end of severe depression. In these analyses, the simple effect of condition on intensity was estimated to be at least large in both Experiment 1 (β = 0.51, d = 1.11) and Experiment 2 (β = 0.40, d = 0.81). Although these estimates are illustrative, note that scores at or above +2 SD on depression were quite rare in Experiment 1 (n = 15) and Experiment 2 (n = 8), so these estimates could be unstable across replications. Furthermore, recall that analyses with participants that fell beyond cutoffs for moderate depression showed moderate to strong (d = 0.62) to strong effects (d = 0.80) of condition on intensity ratings across both experiments.
When evaluating the potential practical significance of our main findings, it might be prudent to consider that the effects we studied pertain to one instance of a behavior category that, in theory, extends over time and situations (Swann, 2012). So if, for example, people with at least moderate depression show moderate to strong tendencies to adopt depression symptoms at one time point, these tendencies might accumulate over time to shape people’s self-concept and life history in potentially more dramatic ways (Funder & Ozer, 2019). Nonetheless, because our experiments did not address longitudinal effects, this idea requires empirical support.
Behavior that verifies a depressed identity is likely to have multiple consequences, and we exposed some of those consequences. For one, such behavior is likely to influence beliefs about the self. In these experiments, participants were strategically altering their responses to confirm their views on their own depression and appeared unaware of doing so. Thus, participants were prone to trust the authenticity of their strategic behavior and use it to judge the self. Hence, people higher in depression were more likely to trust that they had a depressed brain than people lower in depression, and this belief was based in part on the way they completed the color-gazing task. Second, self-verifying behavior is likely to change attitudes toward those characteristics that are claimed (or disclaimed). For example, people high in depression probably experienced some tension between validating high levels of depression and satisfying goals for self-esteem (Kwang & Swann, 2010; Swann, Wenzlaff, Krull, & Pelham, 1992; Swann, Wenzlaff, & Tafarodi, 1992), but they seemingly managed to cope with this struggle somewhat by trivializing the depression characteristics they were claiming. In Experiment 2, people higher in depression rated the depressed brain as more tolerable than people lower in depression based in the way they completed the color-gazing task. These two consequences, together, can potentially cause the maintenance and enhancement of high levels of depression and reduce motivation to change (Swann, 2012).
The present findings are consistent with the rather controversial idea that mental illness can be socially constructed (Horwitz, 2012; Scheff, 1966; Schlenker, 1980; Szasz, 1960). Scheff (1966), for example, suggested that people accept the mentally ill identities forced on them by society and, in turn, consciously or unconsciously feel compelled to express the socially defined symptoms of their apparent “illness.” In Scheff’s view, mental illness symptoms are identity symbols that people adopt rather than necessarily direct or organic consequences of an actual medical condition or psychological turmoil. In fact, institutionalized patients with schizophrenia who have lengthy stays have been shown to strategically produce symptoms of schizophrenia, presumably to remain institutionalized (Braginsky et al., 1969). As we highlighted, Scheff’s views can be contextualized in self-verification theory, and the present findings suggest they are viable. Indeed, we created bogus symptoms of depression in a short lab session. Nonetheless, it is important to recognize that the present findings do not disconfirm the possibility that depression can also arise as a direct consequence of other processes, and of course, no one laboratory study will definitively prove Scheff’s ideas.
Although we think our findings can offer a contribution to an important topic, the present experiments are not without shortcomings. First, note that we relied on self-reports of depression severity collected at one point in time. Although the self-report measures we used have been shown to be valid and reliable (Beck et al., 1996; Teresi et al., 2016), they rely on people’s recall and are unlikely to be perfect reflections of symptom severity (Finan et al., 2009). To help address these matters, future research might include experience sampling methods to assess depression severity along with observer reports of depression severity. Furthermore, future research might seek to replicate our findings using a categorical conceptualization of depression. Indeed, since at least its fourth edition, the Diagnostic and Statistical Manual of Mental Disorders has acknowledged the presence of continuums in psychopathology but retains the categorical approach to diagnosis for pragmatic reasons (Klein et al., 2005). Replicating our results with categorically depressed individuals could be a useful increment.
Second, it is important to understand that our mediation analyses, given their correlational nature, cannot provide unambiguous support for any causal processes. Experimental work is needed to flesh out causal processes that are implied by the mediation modeling. Third, the samples included mostly female college students, which limits the ability to securely apply the findings to other samples. For example, it remains unclear whether the present findings would apply to a clinical sample. Although depression may appear to operate similarly in clinical and nonclinical samples (e.g., college student samples; Cox et al., 1999; Enns et al., 2001; A. B. Hill et al., 1987; Vredenburg et al., 1993), it remains unclear whether the underlying causes and correlates of depression are always similar in these samples. Hence, we encourage scholars to replicate the present study using more diverse sample frames (e.g., clinical samples). Regardless of whether the findings can be easily applied to clinical samples, the present research can still be important; indeed, the self-verification of mental illness identities can have adverse effects on mental health in nonclinical young adult populations and perhaps promote negative consequences in these populations (Joiner, 1995).
In sum, our experiments provide evidence that people emit behaviors that are likely to validate their depression levels and these behaviors feel authentic. Hence, we think that self-verification theory probably provides an accurate way to understand how some psychological (e.g., self-motives and beliefs about the self) and sociocultural variables (e.g., culturally accepted symbols of depression) can shape how depression, as a dimensional feature, manifests in people.
Footnotes
Transparency
Action Editor: Christopher G. Beevers
Editor: Kenneth J. Sher
Author Contributions
W. Hart contributed to the study design and manuscript writing. C. J. Breeden contributed to data collection, analyses, and manuscript writing. K. Richardson contributed to analyses and manuscript writing. C. Kinrade contributed to manuscript writing. All of the authors approved the final manuscript for submission.