
Abstract
Given robust support for internalizing psychopathology as a broad construct, the field has shifted focus from its specific subcomponents to studying internalizing overall, leaving it unclear whether its components provide additional information. We investigated whether internalizing syndromes have incremental validity beyond each other in their associations with 22 external criteria (e.g., health, functioning) using the National Epidemiological Survey on Alcohol and Related Conditions data, a representative adult sample (Wave 1: N = 43,093). We extracted a five-factor model for five lower-order internalizing syndromes (generalized anxiety, major depression, social anxiety, specific phobia, panic). All were moderately correlated with each other and associated with external criteria. Adjusting for other internalizing syndromes, generalized anxiety, major depression, and panic syndromes demonstrated incremental validity, or unique associations with external criteria. Our findings suggest internalizing syndromes exhibit shared and unique features. Investigating both the internalizing spectrum and its more specific syndromes can offer deeper insights into psychopathology.
The Hierarchical Taxonomy of Psychopathology (HiTOP) consortium was formed to improve the nosology and measurement of psychopathology to better inform research and practice (Kotov et al., 2017, 2018). Using empirically derived models, researchers have extracted broad higher-order dimensions of psychopathology that reflect the shared variance in their constituent disorders (Achenbach, 1966). Featured prominently in HiTOP’s hierarchical arrangement of psychopathology are spectra, or higher-order dimensions (e.g., externalizing, internalizing, psychosis). The internalizing spectrum, which includes conditions of negative affect broadly construed, contains subfactors for fear and distress that are, in turn, composed of numerous lower-order syndromes (Conway et al., 2022; Kotov et al., 2021). Internalizing’s fear subfactor includes syndromes characterized by fearful and/or avoidant responses to specific contexts (e.g., panic disorder [PD], social anxiety disorder [SAD], specific phobia [SP]); distress includes syndromes characterized by pervasive negative affect (e.g., generalized anxiety disorder [GAD], major depressive disorder [MDD]; Watson et al., 2022). The structural validity of lower-order internalizing syndromes is well established (Kotov et al., 2021). However, the incremental clinical utility of distinguishing between these syndromes has not been as rigorously tested.
Hierarchical models of psychopathology posit that lower-order clinical syndromes are characterized by both shared features captured in the higher-order spectra and unique features, both of which can be related to clinically relevant variables (Conway et al., 2022). However, most research validating HiTOP has focused on higher-order spectra (Leucht et al., 2024). The literature supporting the internalizing spectrum’s validity often overlooks unique characteristics of phenomena within internalizing given that researchers have increasingly prioritized the broader spectrum over its narrower, more specific syndromes. This shift is illustrated by a review on the validity of the emotional-dysfunction superspectrum in the HiTOP model, in which 54% of the cited empirical studies assessing the internalizing spectrum’s validity in relation to environmental risk factors, cognitive/affective difficulties, neuroimaging, and childhood temperament focused exclusively on correlations between higher-order factors and these variables (Watson et al., 2022). This focus on higher-order dimensions limits understanding of whether lower-order internalizing syndromes relate to clinically relevant variables. In addition, 15% of the studies of interest from the same review examined associations between specific lower-order internalizing syndromes and external criteria without adjusting for other internalizing syndromes (Watson et al., 2022), precluding the possibility of assessing whether any observed associations with external criteria reflect features that are unique to a given internalizing syndrome or if they are shared across syndromes.
Questions remain regarding whether lower-order internalizing syndromes demonstrate incremental validity in their relations with clinically relevant variables, which would suggest they contain unique information beyond what is offered by the spectra. To evaluate the utility of lower-order syndromes in research and clinical practice (Kotov et al., 2021), it is ideal to test whether lower-order syndromes are differentiable from each other, with such distinctions being evident in their differential nomological networks.
Present Study
One way to assess whether a lower-order syndrome is informative beyond other internalizing syndromes is to examine the relation between individual internalizing syndromes and clinically meaningful variables. Here, we consider a broad swath of internalizing syndromes to examine whether they have incremental validity above and beyond each other in the statistical prediction of various external criteria (e.g., physical health, emotional interference, pain, substance use) that have been linked to internalizing (Barry et al., 2013; Blanco et al., 2014; Eaton et al., 2013; D. L. Hoffman et al., 2008; Slade, 2007). If lower-order internalizing syndromes demonstrate unique associations with clinically relevant variables, this would suggest differentiating between syndromes offers clinical utility, whereas the absence of such incremental associations would suggest the link between internalizing symptoms and the external criteria are better explained by variance shared across internalizing syndromes.
Transparency and Openness
Preregistration
This secondary data analysis was not preregistered.
Data, materials, code, and online resources
In the present analysis, we relied on epidemiological data from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC; Grant, Moore, et al., 2003). Detailed NESARC study procedures have been documented elsewhere (Grant & Dawson, 2006). The sample size and recruitment criteria were determined by the broader study. NESARC data are available on request from the National Institute on Alcohol Abuse and Alcoholism. For code to facilitate reproducible findings, see the Supplemental Material available online.
Reporting
We used a subset of study variables; we report on the measures that are relevant to the current study.
Ethical approval
In the present analysis, we used de-identified, preexisting data and did not involve new data collection. The data cannot be reidentified; thus, the current analysis is not considered human-subjects research and is not subject to Institutional Review Board approval.
Method
Sample
We used Wave 1 (2001–2002) data from the NESARC (Grant, Moore, et al., 2003), a representative sample of the adult, civilian U.S. population (N = 43,093; 57.0% female; 57% White, 19% Black or African American, 2% American Indian/Native American, 3% Asian, 19% Hispanic or Latino). The sample’s personal income reflected the U.S. population at the time the data were collected ($0–$19,999: 48.9%; $20,000–$34,999: 23.2%; $35,000–$69,999: 21.0%; $70,000+: 6.9%).
Symptom assessment
The Alcohol Use Disorder and Associated Disability Interview Schedule–DSM-IV version (AUDADIS-IV; Grant, Dawson, et al., 2003), a structured interview, assessed diagnoses and lower-order symptoms according to the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994). The AUDADIS-IV has fair to good test-retest reliability (κs = .40–.65) and convergent validity for past-year mood and anxiety diagnoses (Grant, Dawson, et al., 2003; Grant et al., 2005; Hasin et al., 2005). We examined past-year symptoms for five internalizing syndromes: GAD, MDD, SAD, SP, and PD.
NESARC investigators employed “gating” rules, or branching logic based on participants’ responses. If a participant endorsed any gating item(s) for a disorder, the diagnostic module was completed. If no gating items were endorsed, the diagnostic module for that disorder was skipped under the assumption that the participant did not have the disorder. There is no consensus regarding handling data that are missing not at random because of skip-out rules; each approach has advantages and disadvantages (M. Hoffman et al., 2019; McBride et al., 2023). We imputed missing values from skip-outs with zeros (Huisman, 2009).
External criteria
We considered 22 external criteria linked to internalizing: general self-rated health; accomplished less in the past 4 weeks because of emotional problems; completed work or activities less carefully than usual because of emotional problems; pain interference with work in previous 4 weeks; social interference because of physical- and emotional-health problems; past-year job loss; past-year unemployment; past-year trouble with boss or coworker; past-year separation, divorce, end of steady relationship; past-year major financial crisis; past-year trouble with police; past-year chronic illness; nine forms of past-year substance abuse or dependence (i.e., alcohol, nicotine, stimulant, opioid, sedative, tranquilizer, cocaine, hallucinogen, cannabis); and average daily volume of ethanol consumed in the past year. For further information on how each external criterion was measured and scored, see the Supplemental Material.
Analytic approach
We conducted analyses using Mplus (Version 8.5; Muthén & Muthén, 2019). To account for the complex survey design, we used NESARC’s stratum and primary sampling units as stratum and cluster variables, respectively. To account for the large sample size and multiple comparisons, we employed a conservative significance level of α = .001. For scripts for the analyses, see the Supplemental Material.
Structural validity
Using confirmatory factor analysis, we extracted a five-correlated-factors (representing GAD, MDD, SAD, SP, and PD) model on dichotomous diagnostic-module items (i.e., excluding gating items). Each diagnostic-module item represented an individual symptom for a given syndrome (e.g., difficulty controlling worry, restlessness for GAD; depressed mood, loss of interest for MDD). The model was estimated using the weighted least squares mean and variance (WLSMV) adjusted estimator and fixed latent factor means and variances to 0 and 1, respectively. WLSMV is the recommended estimator for dichotomous indicators because it does not assume normality of observed variables and produces less biased factor-loading estimates than maximum-likelihood estimators when used with ordinal data (Flora & Curran, 2004). Although WLSMV may overestimate interfactor correlations in nonnormal latent distributions, this effect is mitigated by large sample sizes (Li, 2016). We assessed model fit using the comparative fit index, Tucker-Lewis index, and root mean square error of approximation using established guidelines (Browne & Cudeck, 1993; Hu & Bentler, 1999; MacCallum et al., 1996). Although we report the χ2 value, p value, and degrees of freedom, we did not rely on them to determine the adequacy of model fit; χ2 significance tests are sensitive to large sample sizes (Brown, 2015).
Partialled associations between internalizing syndromes and external criteria, adjusting for age and sex
Next, we specified five separate latent-variable models, one for each internalizing syndrome (i.e., GAD, MDD, SAD, SP, PD). We entered the diagnostic-module items for a given syndrome into the appropriate model to define the latent syndrome factor, and each external criterion was regressed onto the latent syndrome factor to examine the partialled associations of each latent internalizing-syndrome factor with each external criterion, adjusting for age and sex only (i.e., “partialled associations”).
Partialled (unique) associations between internalizing syndromes and external criteria, adjusting for age, sex, and other syndromes
Finally, to investigate the unique associations between the latent syndrome factors and external criteria, we entered the diagnostic-module items for all latent syndrome factors into a single model simultaneously, and each external criterion was regressed onto all of the latent syndrome factors simultaneously to determine the association between the syndromes and external criteria, adjusting for age, sex, and other internalizing syndromes (i.e., “partialled [unique] associations”). 1
Results
Structural validity of internalizing
The five-factor correlated-factors model of internalizing was well supported and had strong model fit and loadings (> .40) onto all factors (Table 1). Factors were moderately correlated (range = .38 [MDD-SP]–.63 [GAD-MDD]), suggesting that internalizing syndromes are overlapping but not isomorphic.
Structural Validity
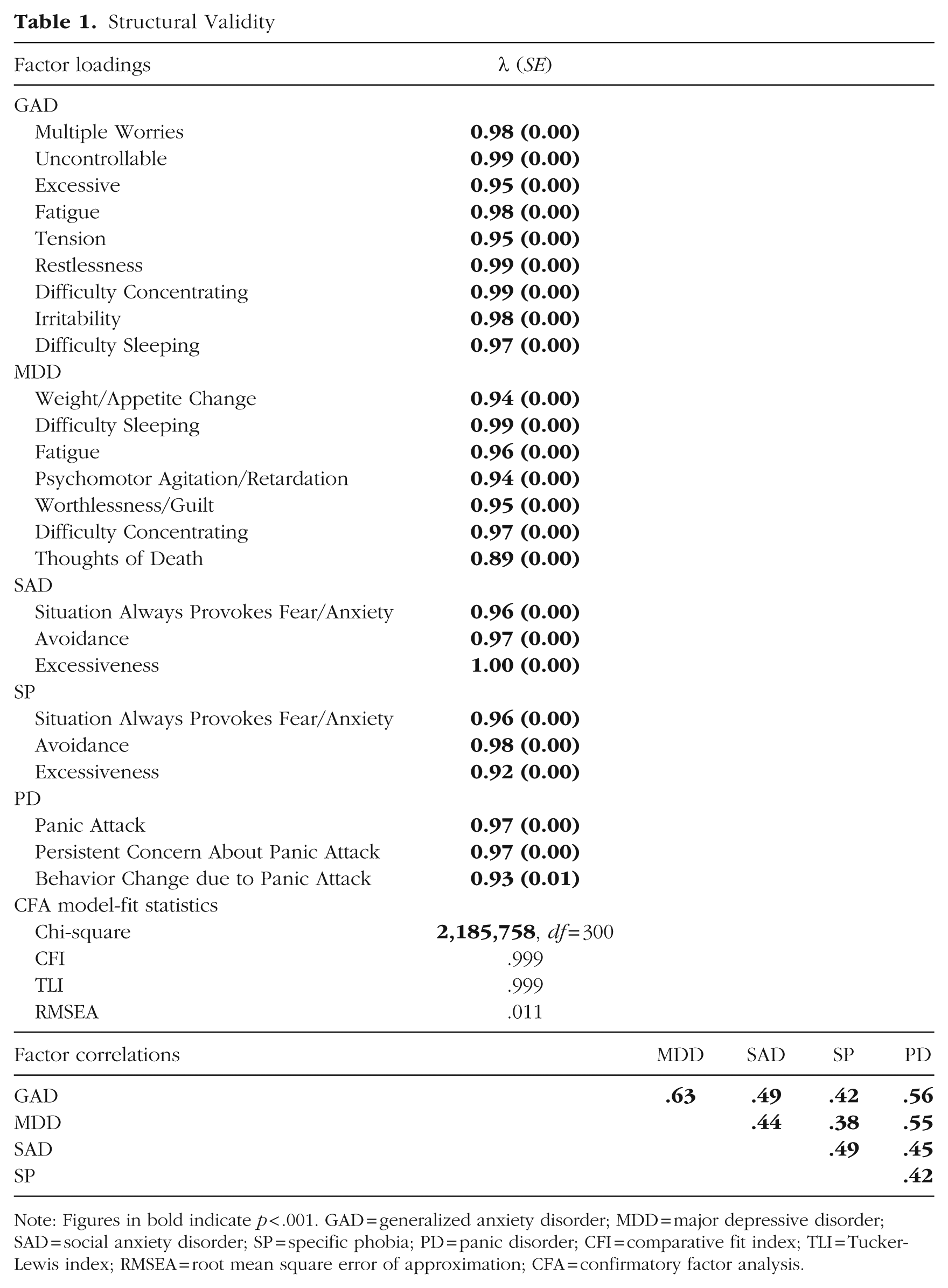
Note: Figures in bold indicate p < .001. GAD = generalized anxiety disorder; MDD = major depressive disorder; SAD = social anxiety disorder; SP = specific phobia; PD = panic disorder; CFI = comparative fit index; TLI = Tucker-Lewis index; RMSEA = root mean square error of approximation; CFA = confirmatory factor analysis.
Partialled associations between internalizing syndromes and external criteria, adjusting for age and sex
When each internalizing factor was entered into the model separately, the partialled associations (adjusting for age and sex) between each latent internalizing condition and each external criterion ranged from small (GAD-Alcohol Volume = 0.07) to large (SAD-Social Interference = 0.62; Table 2).
Partialled Associations, Adjusted for Age and Sex
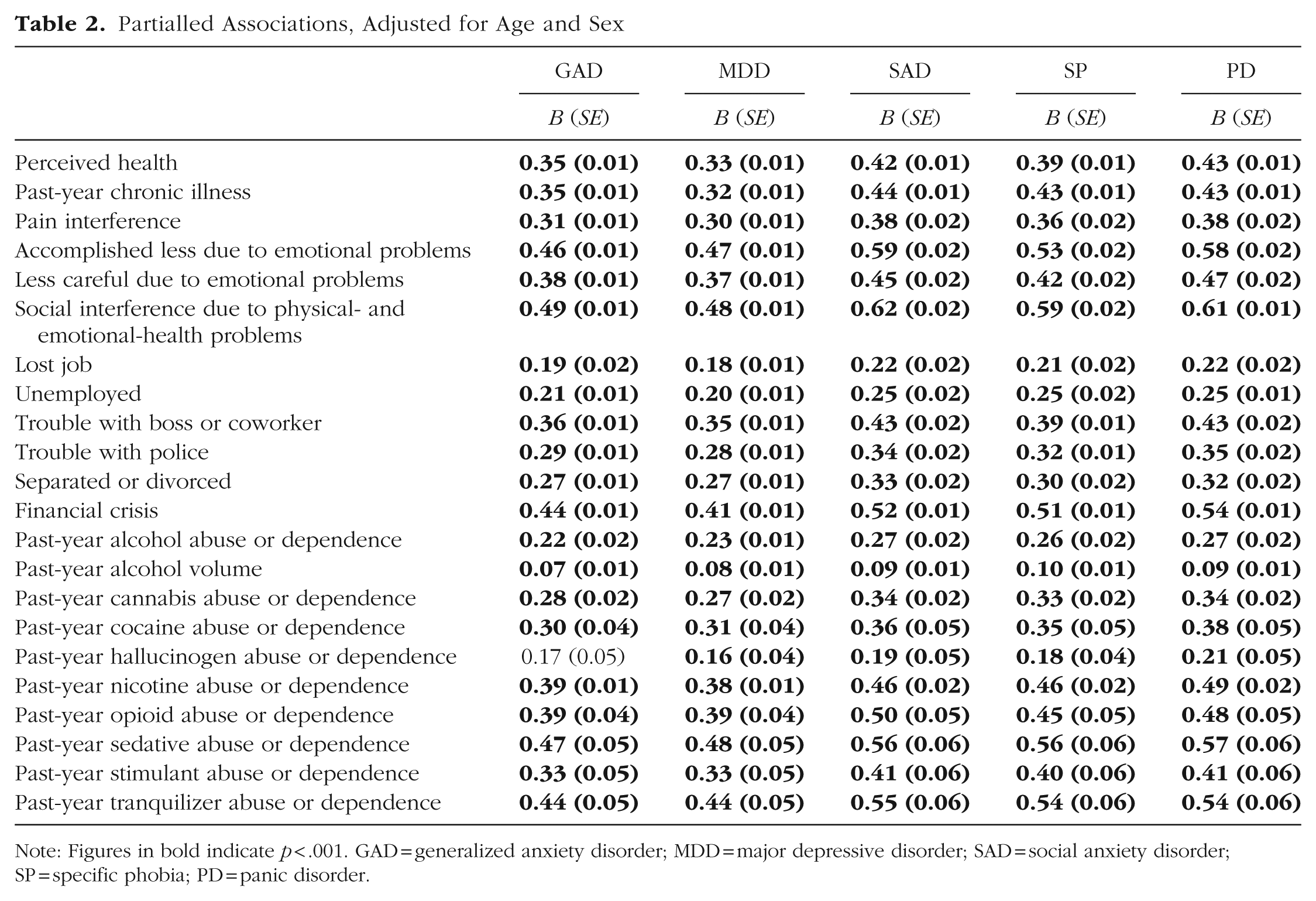
Note: Figures in bold indicate p < .001. GAD = generalized anxiety disorder; MDD = major depressive disorder; SAD = social anxiety disorder; SP = specific phobia; PD = panic disorder.
There were moderate to large associations between internalizing syndromes and accomplishing less because of emotional problems (range = 0.46 [GAD]–0.59 [SAD]); completing work or activities less carefully because of emotional problems (range = 0.37 [MDD]–0.47 [PD]); interference in social activities because of physical or emotional problems (range = 0.48 [MDD]–0.62 [SAD]); experiencing a financial crisis, bankruptcy, or inability to pay bills in the past year (range = 0.41 [MDD]–0.54 [PD]); past-year opioid abuse or dependence (range = 0.39 [GAD, MDD]–0.50 [SAD]); past-year sedative abuse or dependence (range = 0.47 [GAD]–0.57 [PD]); and past-year tranquilizer abuse or dependence (range = 0.44 [GAD, MDD]–0.55 [SAD]).
There were moderate associations between internalizing syndromes and perceived health (range = 0.33 [MDD]–0.43 [PD]), past-year chronic illness (range = 0.32 [MDD]–0.44 [SAD]), pain interference with work (range = 0.30 [MDD]–0.38 [PD]), past-year issues with a boss or coworker (range = 0.36 [GAD]–0.43 [SAD]), past-year issues with police (range = 0.28 [MDD]–0.35 [PD]), past-year separation or divorce (range = 0.27 [GAD]–0.33 [SAD]), past-year cannabis abuse or dependence (range = 0.27 [MDD]–0.34 [PD]), past-year cocaine abuse or dependence (range = 0.30 [GAD]–0.38 [PD], past-year nicotine abuse or dependence (range= 0.38 [MDD]–0.49 [PD]), and past-year stimulant abuse or dependence (range = 0.33 [GAD, MDD]–0.41 [SAD, PD]).
There were small associations between internalizing syndromes and past-year job loss (range = 0.18 [MDD]–0.22 [PD]), past-year unemployment (range = 0.20 [MDD]–0.25 [SP, PD]), past-year alcohol abuse or dependence (range = 0.22 [GAD]–0.27 [PD]), past-year daily average of ethanol consumed (range = 0.07 [GAD]–0.10 [SP]), and past-year hallucinogen abuse or dependence (range = 0.16 [MDD]–0.21 [PD]).
Partialled (unique) associations between internalizing syndromes and external criteria, adjusting for age, sex, and other syndromes
When all internalizing factors were entered into the model simultaneously (i.e., partialled [unique] associations), we found that MDD was consistently incrementally associated with external criteria beyond other internalizing syndromes. GAD and PD were also incrementally associated with some external criteria (Table 3, Fig. 1). SAD did not show incremental associations with the external criteria.
Partialled (Unique) Associations: Standardized Path Coefficients When Adjusting for Other Internalizing Conditions
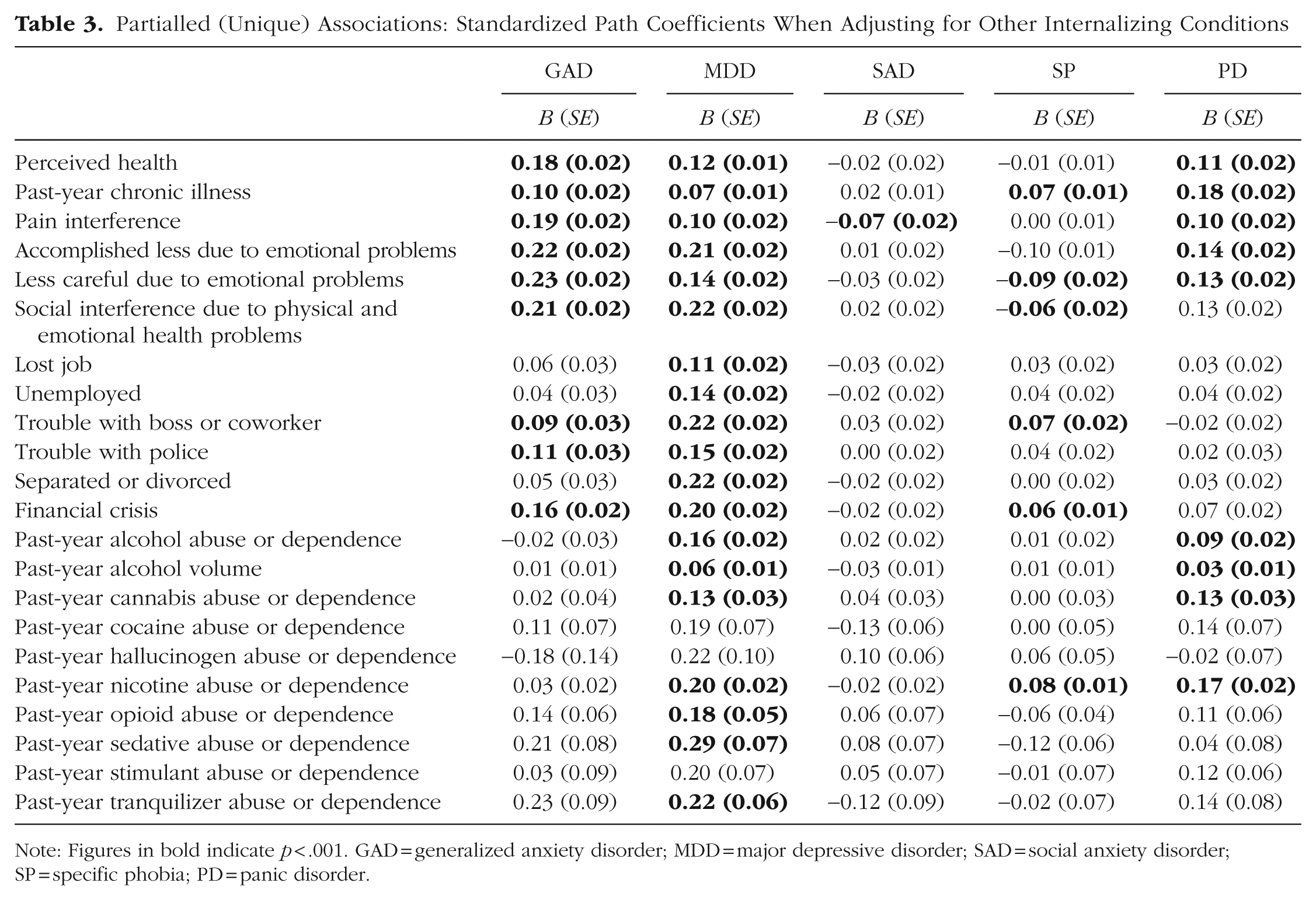
Note: Figures in bold indicate p < .001. GAD = generalized anxiety disorder; MDD = major depressive disorder; SAD = social anxiety disorder; SP = specific phobia; PD = panic disorder.
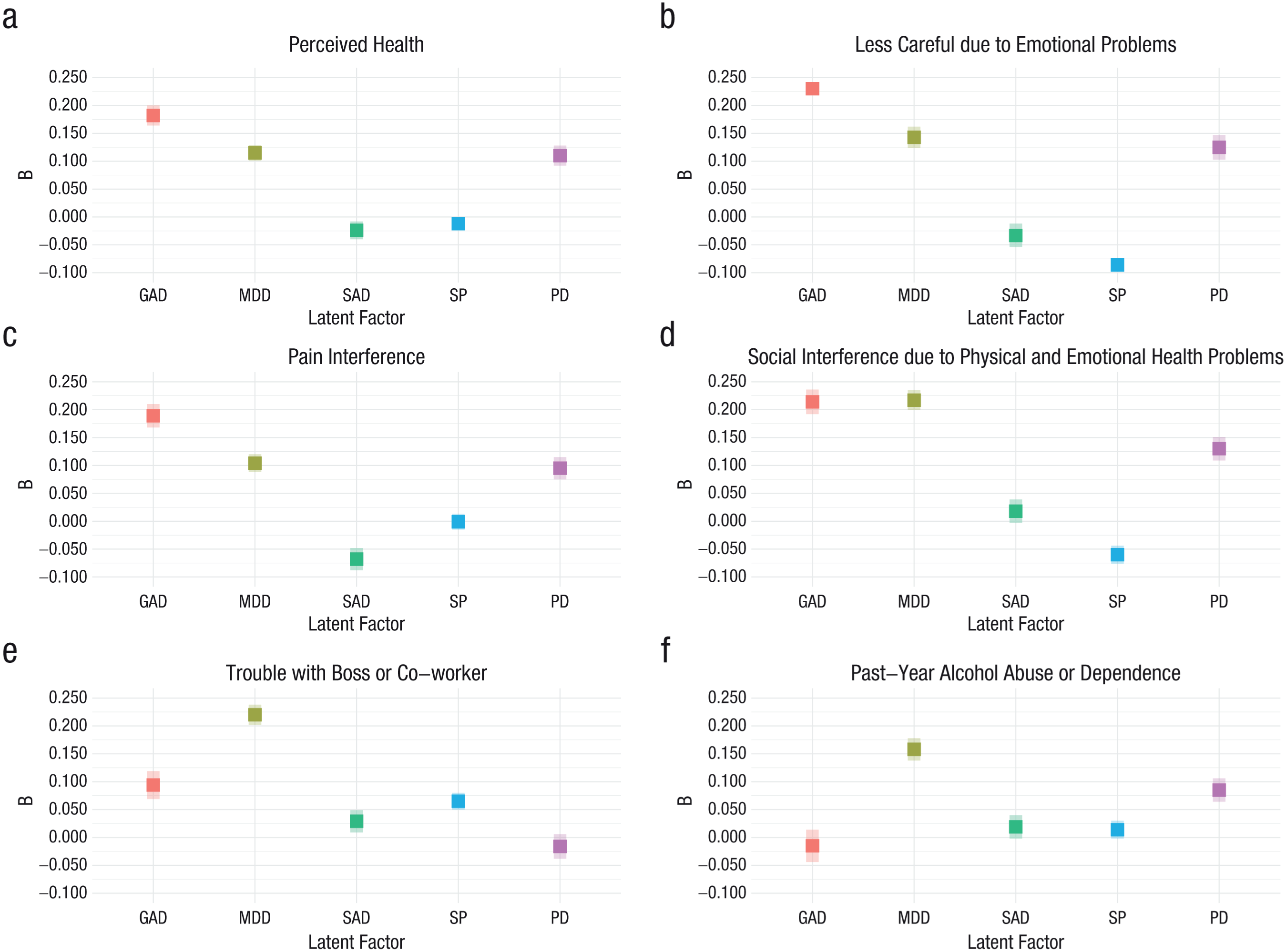
Standardized partialled (unique) path coefficients and 95% confidence intervals of each latent syndrome factor, controlling for age, sex, and other internalizing syndromes. (a) Perceived health. (b) Being less careful due to emotional problems. (c) Interference due to pain. (d) Social interference due to physical- and emotional-health problems. (e) Trouble with boss or coworker. (f) Past-year alcohol abuse or dependence.
GAD, MDD, and PD were the conditions most incrementally associated with health-related variables, having small but clinically meaningful effects. Specifically, these conditions demonstrated incremental associations with perceived health (GAD: B = 0.18; MDD: B = 0.12; PD: B = 0.11), past-year chronic illness (GAD: B = 0.10; MDD: B = 0.07; PD: B = 0.18), and pain interference (GAD: B = 0.19; MDD: B = 0.10; PD: B = 0.10). SAD and SP did not demonstrate consistent incremental associations with health-related external criteria, although SP had a small incremental association with past-year chronic illness (B = 0.07), and SAD had a small, negative incremental association with pain interference (B = −0.07).
MDD consistently demonstrated small incremental associations with functioning across life domains, whereas GAD showed small incremental associations with select areas of life functioning. Specifically, MDD was associated with past-year job loss (B = 0.11), past-year unemployment (B = 0.14), and past-year separation or divorce (B = 0.22), but GAD was not. Both GAD and MDD were associated with accomplishing less because of emotional problems (GAD: B = 0.22; MDD: B = 0.21), completing tasks less carefully because of emotional problems (GAD: B = 0.23; MDD: B = 0.14), social interference because of physical/emotional-health problems (GAD: B = 0.21; MDD: B = 0.22), past-year trouble with boss or coworker (GAD: B = 0.09; MDD: B = 0.22), past-year trouble with police (GAD: B = 0.11; MDD: B = 0.15), and past-year financial crisis (GAD: B = 0.16; MDD: B = 0.20).
MDD also demonstrated small to moderate incremental associations with most forms of substance abuse and dependence, including alcohol (B = 0.16), cannabis (B = 0.13), nicotine (B = 0.20), opioid (B = 0.18), sedative (B = 0.29), and tranquilizer (B = 0.22) abuse or dependence. PD demonstrated small incremental associations with alcohol (B = 0.09), cannabis (B = 0.13), and nicotine (B = 0.17) abuse or dependence.
Discussion
We extended prior research by investigating whether lower-order internalizing syndromes have incremental validity beyond each other. Our findings suggest that lower-order internalizing syndromes exhibit shared features captured by the internalizing spectrum and unique features. All internalizing syndromes demonstrated associations with external criteria when adjusting for age and sex only, and there were small to large associations with health, life functioning, and substance abuse and dependence. These findings highlight the pervasive impact of internalizing syndromes across multiple life domains, which may be driven by shared underlying mechanisms, such as negative affect/neuroticism and cognitive deficits (Bloemen et al., 2018; Griffith et al., 2010; Jacobson et al., 2018). This pattern aligns with treatments targeting broad, shared mechanisms (García-Escalera et al., 2016; Newby et al., 2015).
Nevertheless, when adjusting for all other internalizing syndromes, age, and sex, we observed that certain internalizing syndromes had incremental validity above all other internalizing syndromes. Although the incremental associations were relatively modest in magnitude, they remain clinically relevant because they suggest some internalizing syndromes had unique variance that is not well captured by the higher-order internalizing construct. When all syndromes were entered into the model simultaneously, MDD was consistently incrementally associated with external criteria. GAD and PD were incrementally associated with some external criteria. However, SAD did not show incremental validity with the criteria considered in the present study.
GAD, MDD, and PD were the conditions most incrementally associated with health-related variables, including perceived health, past-year chronic illness, and pain interference. GAD exhibited a stronger incremental association with perceived health and pain interference than the other syndromes, extending findings on its link to poor perceived health and increased risk of pain symptoms and pain disorder (Beesdo et al., 2009, 2010; García-Campayo et al., 2012; Gureje, 2008; Means-Christensen et al., 2008). GAD, MDD, and PD also showed incremental associations with past-year chronic illness beyond other internalizing syndromes, consistent with research showing that these conditions commonly co-occur with physical illnesses, and their comorbidity is associated with adverse outcomes such as poorer perceived health (Ferro, 2016; Scott et al., 2023; Whitehead et al., 2002). Our results highlight GAD, MDD, and PD as unique predictors of physical-health characteristics beyond other internalizing syndromes.
Consistent with our findings, individuals diagnosed with GAD, MDD, and PD show higher rates of health-care use than individuals without these diagnoses (Horenstein & Heimberg, 2020; Luber et al., 2000; Olfson & Gameroff, 2007). This observation is thought to be driven by several factors, including difficulty recognizing the link between somatic symptoms and anxiety or depression, reassurance-seeking behaviors, and a putative reciprocal relationship between GAD, MDD, PD, and physical health (Horenstein & Heimberg, 2020). Targeting the mechanisms underlying the connection between GAD (e.g., excessive worry, reduced heart rate variability), MDD (e.g., reduced treatment adherence), PD (e.g., elevated anxiety sensitivity, decreased physical activity), and chronic illness may result in reduced health-care costs and improved mental- and physical-health outcomes (Horenstein & Heimberg, 2020; Tully et al., 2013; Ziegelstein et al., 2000).
GAD and MDD demonstrated incremental associations with several functional deficits when adjusting for other internalizing syndromes, age, and sex, including completing tasks less carefully, accomplishing less, social interference, financial crisis, and trouble with law enforcement. GAD and MDD fall under the distress subfactor of the internalizing spectrum and are characterized by pervasive negative affect rather than context-dependent fear and avoidance (Kotov et al., 2021; Watson et al., 2022). By definition, GAD and MDD symptoms persist at least more days than not (American Psychiatric Association, 2022). Moreover, GAD and MDD are characterized by worry and rumination, respectively, which are styles of repetitive negative thinking that are relatively uncontrollable, focused on negative content, and largely context-independent (McEvoy et al., 2018). In contrast, the negative affect experienced in fear-based disorders may be more circumscribed to specific contexts (American Psychiatric Association, 2022). Individuals with a fear-based condition may use avoidance or escape/flight behavior to prevent or reduce stress responses more effectively, but such behaviors may not be as feasible or as effective at reducing stress responses in GAD and MDD given that the distress in those conditions is not typically linked to one specific trigger (Ohi et al., 2025). Compared with the context-dependent negative affect in other internalizing conditions, the pervasive distress experienced in GAD and MDD may exert greater influence on broad dimensions of well-being (Gorrell et al., 2026; Henning et al., 2007; Stein & Heimberg, 2004). Importantly, our results support prior findings that GAD and MDD are related but distinct constructs (Beesdo et al., 2010; Blanco et al., 2014; Stein & Heimberg, 2004; Wittchen et al., 2000).
MDD showed the strongest incremental association with past-year trouble with a boss or coworker, and it was the only condition that was associated with being fired/laid off from a job and being unemployed for more than a month during the past year when adjusting for other internalizing syndromes, age, and sex, suggesting a unique association between MDD and occupational functioning. Indeed, research suggests there is a bidirectional relationship between depression and job loss (Riumallo-Herl et al., 2014; Whooley et al., 2002). One proposed mechanism linking MDD to job loss is MDD’s association with impairments in cognitive domains such as executive functioning and processing speed, which may lead to impaired occupational functioning (Buist-Bouwman et al., 2008; Snyder, 2013). It is possible that treatments that aim to reduce neurocognitively based workplace deficits or help individuals adapt to them could improve functioning for individuals diagnosed with MDD (Blumberg et al., 2020). Conversely, longitudinal research has linked job loss to subsequent increases in depression, which has, in turn, been linked to lower rates of reemployment (Riumallo-Herl et al., 2014; Stolove et al., 2017).
MDD showed the strongest incremental association with past-year alcohol abuse or dependence and past-year average daily volume of ethanol consumed when adjusting for other internalizing syndromes, age, and sex. Moreover, when adjusting for other internalizing syndromes, age, and sex, MDD was the only syndrome that was significantly associated with past-year opioid, sedative, and tranquilizer abuse or dependence, whereas MDD and PD were similarly associated with past-year cannabis and nicotine abuse or dependence. It is possible that syndrome-specific processes are involved in the maintenance of substance use disorders. For example, the misuse of alcohol and other substances may result in impaired functioning and neurobiological changes, which can increase risk of depression (Semenkovich et al., 2014; Swendsen & Merikangas, 2000). Likewise, social isolation or attempts to reduce mood symptoms related to depression by using alcohol and other substances may exacerbate substance use disorders (Crum et al., 2013; Grodin et al., 2024; Ingram et al., 2020). Regular use of cannabis or nicotine may increase risk for elevated anxiety sensitivity (i.e., fear of anxiety-related physiological symptoms), which can predispose someone to the development of PD (Zvolensky et al., 2006). In PD, it is possible that heightened responses to physiological cues may lead to substance use to reduce anxiety and may also interfere with quit attempts for individuals with substance use disorders (Zvolensky et al., 2006). An integrated model for understanding and treating MDD, PD, and substance-use-disorder symptoms may improve patient outcomes.
In contrast to other internalizing syndromes, SAD showed no evidence of incremental associations with external criteria when adjusting for other internalizing syndromes, age, and sex despite showing strong associations when adjusting for age and sex only. One possible explanation is that the associations between SAD and external criteria are better explained by comorbid conditions. SAD commonly co-occurs with depression, and both disorders are characterized by both heightened negative affect and deficits in positive affect (Kashdan et al., 2011). However, the SAD diagnostic criteria do not include positive affect deficits, but depression symptom criteria do (American Psychiatric Association, 2022). Thus, future research should investigate the unique role of positive-affect deficits in physical health, life functioning, and substance abuse and dependence. SAD also frequently co-occurs with other internalizing conditions, and the majority of individuals with comorbid conditions do not view social anxiety as their primary complaint, suggesting they view the co-occurring condition(s) as the primary driver of their physical- and mental-health concerns (Koyuncu et al., 2019).
Limitations and future directions
Our findings should be interpreted in the context of several limitations. First, we used dichotomous DSM-IV (American Psychiatric Association, 1994) symptoms, which are less reliable than dimensional measures (Narrow et al., 2013). Future studies should examine the relations between dimensional symptom profiles and clinically relevant criteria. Second, we examined the relationship between specific lower-order syndromes and relatively nonspecific external criteria. More pronounced differences among lower-order internalizing syndromes may emerge with more specific criteria, such as specific chronic illnesses linked to particular conditions (e.g., coronary heart disease and GAD; asthma and PD; Katon et al., 2004; Tully et al., 2013). Differences may also emerge when focusing on biomarkers underlying subtypes of internalizing disorders. For example, the late positive potential, a neural marker of emotional reactivity, may be attenuated in distress/misery syndromes but enhanced in fear-based syndromes (Granros et al., 2022). Future studies should examine these relationships to shed light on the shared and unique etiologies of specific internalizing phenomena. Third, in this study, we did not account for the temporal relationships between internalizing syndromes. For example, anxiety disorders are associated with increased risk of subsequent MDD (Klein et al., 2013). Future research should consider temporal dynamics in the development of internalizing psychopathology. Fourth, NESARC investigators relied on gating questions, which are common in large-scale epidemiologic studies. Gating criteria may skip questions that could be important for understanding an individual’s symptom profile, reducing variability in item endorsement and inflating the correlations between symptoms within a disorder (McBride et al., 2023). We elected to impute missing values that were due to skip-outs with zeros, which can inflate the within-syndromes factor loadings and underestimate between-syndromes correlations (M. Hoffman et al., 2019). Thus, the syndromes may appear to be more distinct than they truly are. Future research should consider alternative approaches, such as the split-questionnaire survey design, to mitigate issues with missing data (McBride et al., 2023; Raghunathan & Grizzle, 1995).
Conclusion
Overall, our findings suggest that internalizing disorders are closely related but distinct constructs. These findings have important implications for clinical practice, but longitudinal research is required to understand the relation between specific disorders and clinical correlates. For example, targeting disorder-specific mechanisms, such as chronic worry in GAD, may be important in improving certain clinical characteristics, such as perceived health, but further research on the mechanisms linking specific disorders to clinically relevant characteristics is needed. Finally, our findings suggest the common practice of examining only higher-order internalizing is misguided because it leads to missed opportunities for deeper insights and reinforces the misconception that all relevant variance lies within the internalizing spectrum, hindering the identification of unique features within lower-order internalizing syndromes.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026261443518 – Supplemental material for Do Internalizing Syndromes Have Incremental Validity for External Criteria Above and Beyond Each Other?
Supplemental material, sj-docx-1-cpx-10.1177_21677026261443518 for Do Internalizing Syndromes Have Incremental Validity for External Criteria Above and Beyond Each Other? by Kerry L. Kinney, Matthew C. Morris, Katja Beesdo-Baum and Ashley L. Watts in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Kelsie T. Forbush
Editor: Jennifer L. Tackett
Author Contributions
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.