
Abstract
Design
Retrospective study.
Objective
To evaluate the predictive performance of a simplified, MRI-derived vertebral bone quality score (VBQ) using measurements at L1/2 (VBQL1/2) for opportunistic bone quality screening, compared to the established VBQL1-4.
Methods
In patients undergoing lumbar surgery for degenerative spondylolisthesis, VBQL1/2 was assessed using circular regions of interest on sagittal T1-weighted sequences in L1 and L2, while VBQL1-4 included measurements from L1 through L4. Measurements were normalized to cerebrospinal fluid intensity at L2/3. Bone mineral density (BMD) was measured by opportunistic qCT, with osteoporosis defined as BMD < 80 mg/cm3 and impaired bone quality (osteoporosis or osteopenia) as BMD < 120 mg/cm3. Agreement between VBQL1/2 and VBQL1-4 was determined using the intraclass correlation coefficient (ICC), and predictive performance was evaluated using receiver operating characteristic analysis with Youden’s index optimization.
Results
Among 144 patients included ((39% male, n = 56) the median age was 69 years (interquartile range 64-67). Osteopenia was present in 47% and osteoporosis in 22%, yielding 69% impaired bone quality. VBQL1/2 and VBQL1-4 showed excellent agreement (ICC: 0.988, 95% CI: 0.982–0.991). Predictive performance was comparable for osteoporosis (AUC: VBQL1/2 0.71 vs. VBQL1-4 0.69) and impaired bone quality (AUC: 0.68 vs. 0.67). For osteoporosis detection, VBQL1/2 showed a higher sensitivity (94% vs 71%) but a lower specificity (45% vs 64%), as well as for detecting impaired bone quality (sensitivity 77% vs. 47%, 56%, vs 82%).
Conclusions
VBQL1/2 offers a simplified alternative to VBQL1-4 for MRI-based bone quality assessment. Further validation and threshold refinement are warranted.
Introduction
Patients with low bone mineral density have an increased risk for complications when undergoing lumbar fusion surgery, including adjacent level fractures, non-union, implant loosening, leading to increased healthcare costs and ongoing disability.1,2,3,4 Despite osteoporosis screening guidelines for the general population,5–7 about 10% of lumbar surgery patients are undiagnosed with osteoporosis,8–10 highlighting the need for improved preoperative detection strategies. While spine specific guidelines need more evidence, 11 they propose employing opportunistic screening to evaluate bone quality in patients scheduled for lumbar surgery, utilizing existing imaging without the need for additional radiation or resources. 12 If a preoperative CT scan is performed, the opportunistic measurement of vertebral Hounsfield units (HU) or an asynchronous quantitative CT (qCT) is feasible. qCT provides reliable volumetric BMD at L1 and L2, aligning with WHO definitions of osteopenia (BMD 80–120 mg/cm3) and osteoporosis (BMD <80 mg/cm3),13,14 but it necessitates asynchronous calibration and additional software. HU measurements are constrained by their dependence on scanning conditions. 15
The MRI-based vertebral bone quality (VBQ) score has been proposed as an alternative without the need for a preoperative CT by Ehresman et al 1 16 The described approach involves measuring the intensities within a circular region of interest (ROI) on sagittal T1 MRI scans of the lumbar vertebrae L1 through L4 and normalizing the median value to the intensity of the cerebrospinal fluid (CSF).16–18 In patients with prior fusion or higher-grade segmental degeneration leading to local MRI alterations such as Modic changes in degenerative spondylolisthesis or metal artifacts in the lower lumbar spine, the application of this L1-L4 VBQ may be limited. Furthermore, the process of measuring several ROIs, determining the median and normalizing it to the CSF is time consuming, potentially hindering broader application. A simplified VBQ measurement at L1/L2, similar to the ACR-recommended qCT sites, could improve feasibility while maintaining diagnostic accuracy.
Therefore, we conducted this study to compare the predictive accuracy of VBQL1/2 with VBQ L1-L4 for detecting impaired bone quality (osteopenia and osteoporosis) and specifically osteoporosis in a cohort of patients undergoing lumbar surgery for degenerative lumbar spondylolisthesis.
Methods
Study Design
A secondary analysis was conducted on a study involving patients who underwent surgical treatment for DLS at the L4/5 level at an academic tertiary spine care center between 2016 and 2018, which has been previously described.19–21 The study complies with the guidelines established by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) initiative. 22 Institutional Review Board (IRB) approval was obtained before the commencement of the study (IRB# 2015-237). The patients underwent a preoperative CT scan and a lumbar MRI as part of their preoperative planning for lumbar surgery. Patients whose MRI scans were unsuitable for VBQ measurements, specifically those without a sagittal, non-contrast, T1 sequence, were excluded. Patient demographic and surgical data included age, sex, BMI and pre-existing conditions.
qCT Bone Density Measurements
BMD measurements were performed using Mindways QCT Pro Software (Mindways Software, Inc., Austin, TX) as previously described 23 and in accordance with the ACR recommendations. 13 The trabecular BMD of L1 and L2 was measured by placing an elliptical volume in the anterior trabecular area of the vertebral body and the L1/L2 BMD average calculated. Patients were then categorized based on their qCT derived BMD. Osteopenia was defined as BMD <120 mg/cm3 and ≥ 80 mg/cm3, osteoporosis as BMD < 80 mg/cm3 13. Impaired bone quality was defined as the presence of either osteoporosis or osteopenia.
VBQ Measurements
VBQ measurements were conducted using ITK-SNAP (Version 3.8.0, University of Pennsylvania, Philadelphia, USA) on sagittal MRIs. For the VBQL1-4, as described by Ehresman et al,
16
the signal intensity of the medullary portion of the L1–L4 vertebral bodies on mid-sagittal T1-weighted MR images was used (Figure 1). To exclude focal lesions and the posterior venous plexus from the vertebral ROI, parasagittal images were selected if necessary. The CSF ROI was placed posterior to L2/3, ensuring avoidance of nerve roots. If spinal stenosis prevented CSF ROI selection at this level, the adjacent level was used. The VBQL1-4 score was calculated by dividing the median signal intensity of L1–L4 by the CSF signal intensity at L2/3. The VBQL1/2 score was calculated by dividing the median (equaling the mean) signal intensity of L1–L2 by the CSF signal intensity at L2/3. Only T1-weighted images without STIR or postcontrast sequences were included to prevent signal alterations. Inter-rater reliability for the VBQ score has been reported as good to excellent, with an interclass correlation coefficient (ICC) between 0.800 and 0.910.24,25 Measurement of the signal intensities of T1 weighted sagittal MRI sequences for the calculation of VBQL1/2 and VBQL1-4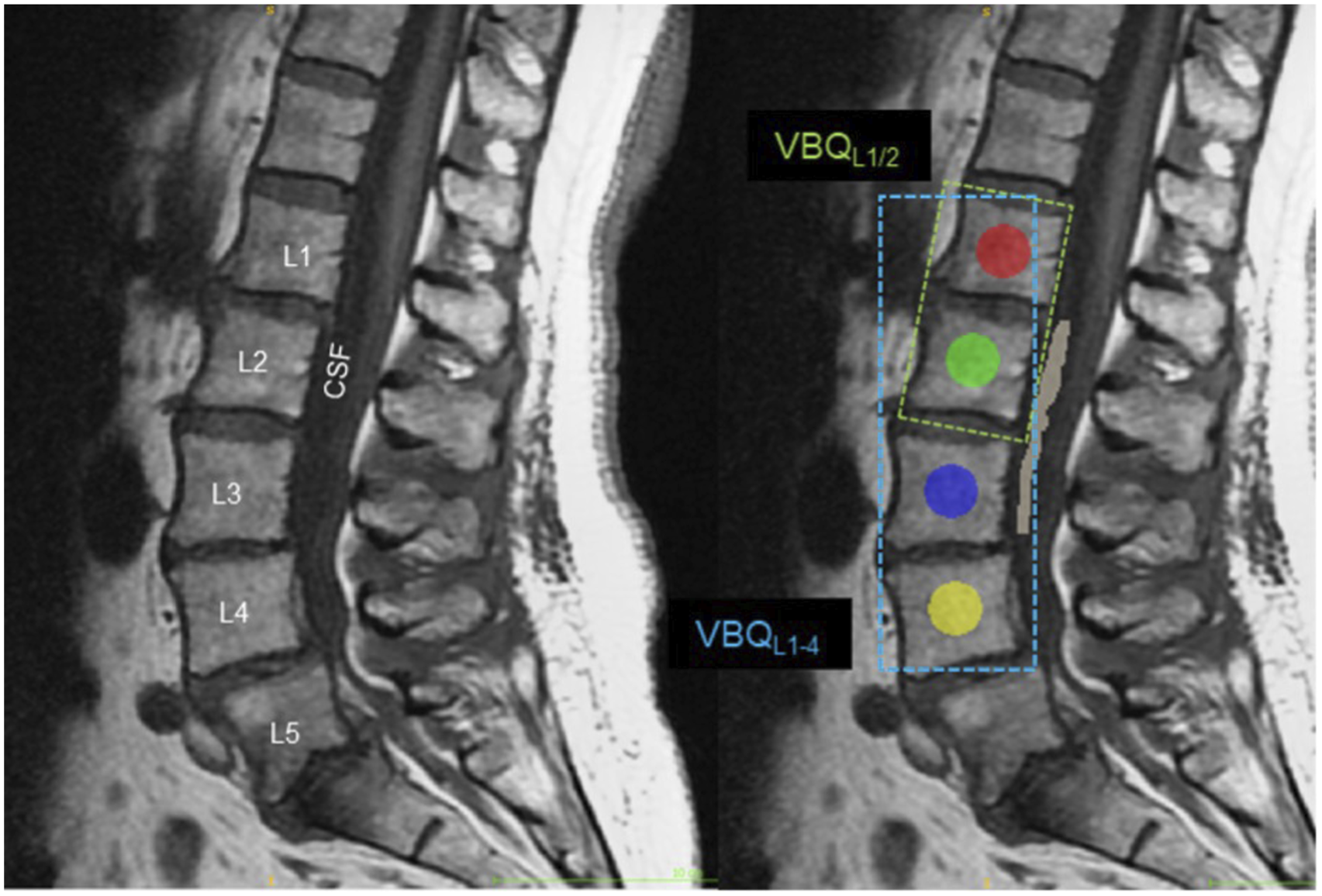
Statistical Analysis
The distribution of data for normality was assessed by both visual inspection and the Shapiro-Wilk test. For consistency, data was analyzed as medians with interquartile ranges (IQRs) and treated as non-normally distributed. Categorical data is presented as percentages and frequencies. The Fisher’s exact test or Pearson’s chi-squared test, as appropriate, was applied to assess differences between categorical variables. The Wilcoxon rank-sum test (Man-Whitney-U Test) was employed for unpaired ordinal and continuous variables, while the Wilcoxon signed rank test was applied for paired analysis, respectively. For comparison of more than two unpaired groups, the Kruskal-Wallis test with post-hoc Wilcoxon Rank Sum (Mann-Whitney U) test with Holm correction for multiple testing was performed. Two-way single score Intraclass Correlation (ICC) analysis for agreement between the VBQL1/2 and the VBQL1-4 was performed. Spearman correlation analysis was performed to investigate the association between both VBQ versions and BMD. To analyze the utility of VBQL1/2 and the VBQL1-4 to detect osteoporosis (BMD < 80 mg/cm3) or impaired bone quality (osteopenia or osteoporosis, BMD < 120 mg/cm3), receiver operator curve (ROC) analysis with Youden’s index optimization was applied. Statistical analysis was performed with R Studio (Version 2023.06.2, Posit Software, Boston, Massachusetts, USA). Statistical significance was set at P < 0.05.
Results
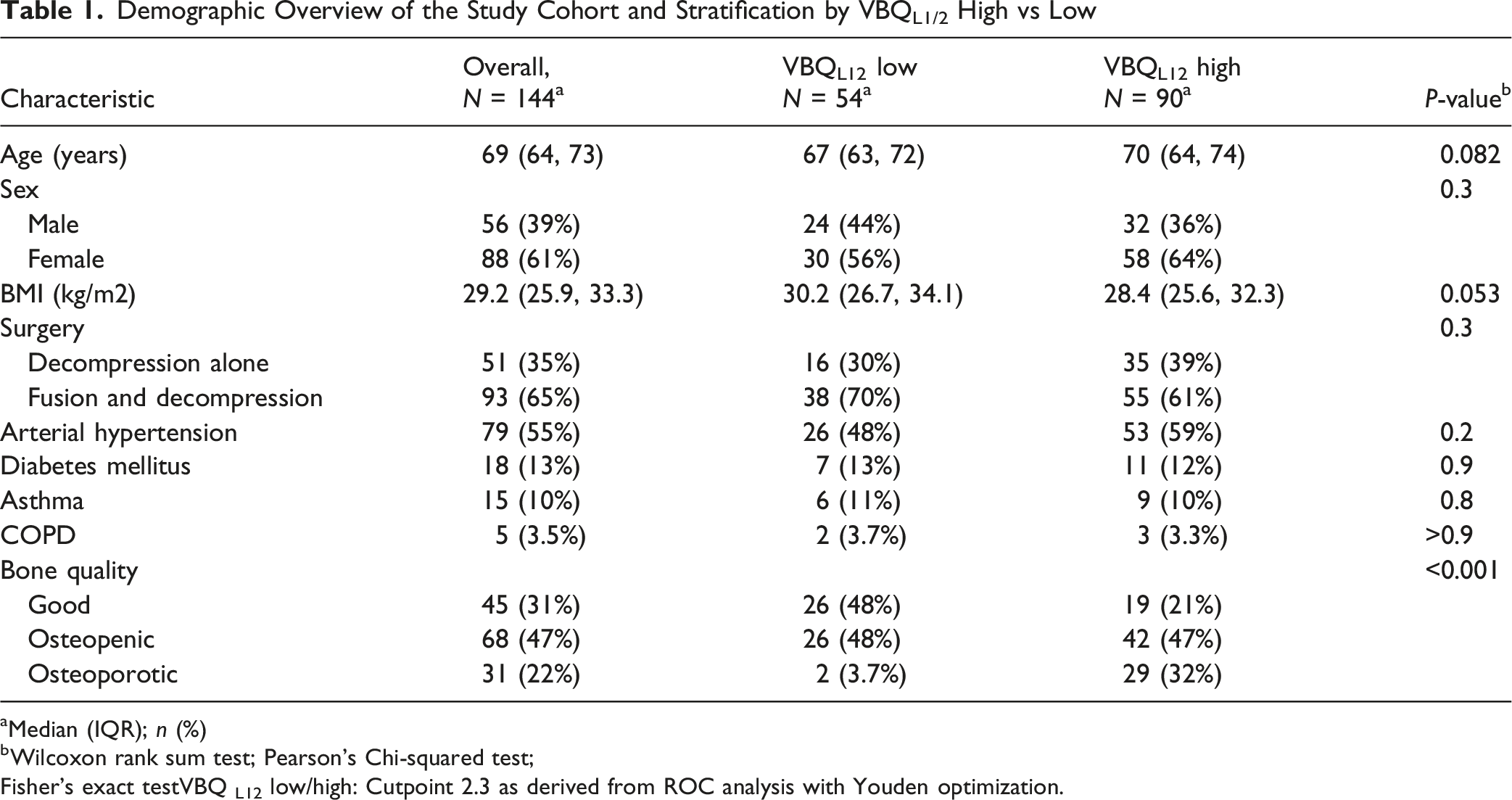
Out of 202 patients, 58 were excluded due to the inability to perform VBQ measurements (Figure 2). The demographic data is summarized in Table 1. The median age was 69 years (inter quartile range 64-67), 56 (39%) were male and the median BMI was overweight (29.2 kg/m2, IQR 25.9-33.3). The most prevalent chronic conditions were arterial hypertension (n= 79, 55%), diabetes mellitus (n= 18, 13%), and asthma or COPD (combined n= 20, 14%). The median BMD of the cohort was 105 mg/cm3 (IQR 84-126), 31 (22%, median BMD 70 mg/cm3 (IQR 64-75)) patients had osteoporosis, 68 (47%, median BMD 102 mg/cm3 (IQR 90-11)) osteopenia, resulting in 99 cases (69%) with impaired bone quality. Patients with a high VBQL1/2 (>2.3, as derived from ROC analysis to detect osteoporosis), were not significantly different from those with a low VBQL1/2 regarding their demographic data or pre-existing conditions, but a non-significant trend towards older age (P = 0.082) and lower BMI (P = 0.053) was observed. Bone quality was significantly different (P < 0.001) between the group with low VBQL1/2, where two patients (4%) had osteoporosis compared to 29 (32%) in the group with a high VBQL1/2. BMD was significantly lower in the high VBQL1/2 group, while both VBQL1/2 and VBQL1-4 were significantly higher. Strobe diagram for the study Demographic Overview of the Study Cohort and Stratification by VBQL1/2 High vs Low aMedian (IQR); n (%) bWilcoxon rank sum test; Pearson’s Chi-squared test; Fisher’s exact testVBQ L12 low/high: Cutpoint 2.3 as derived from ROC analysis with Youden optimization.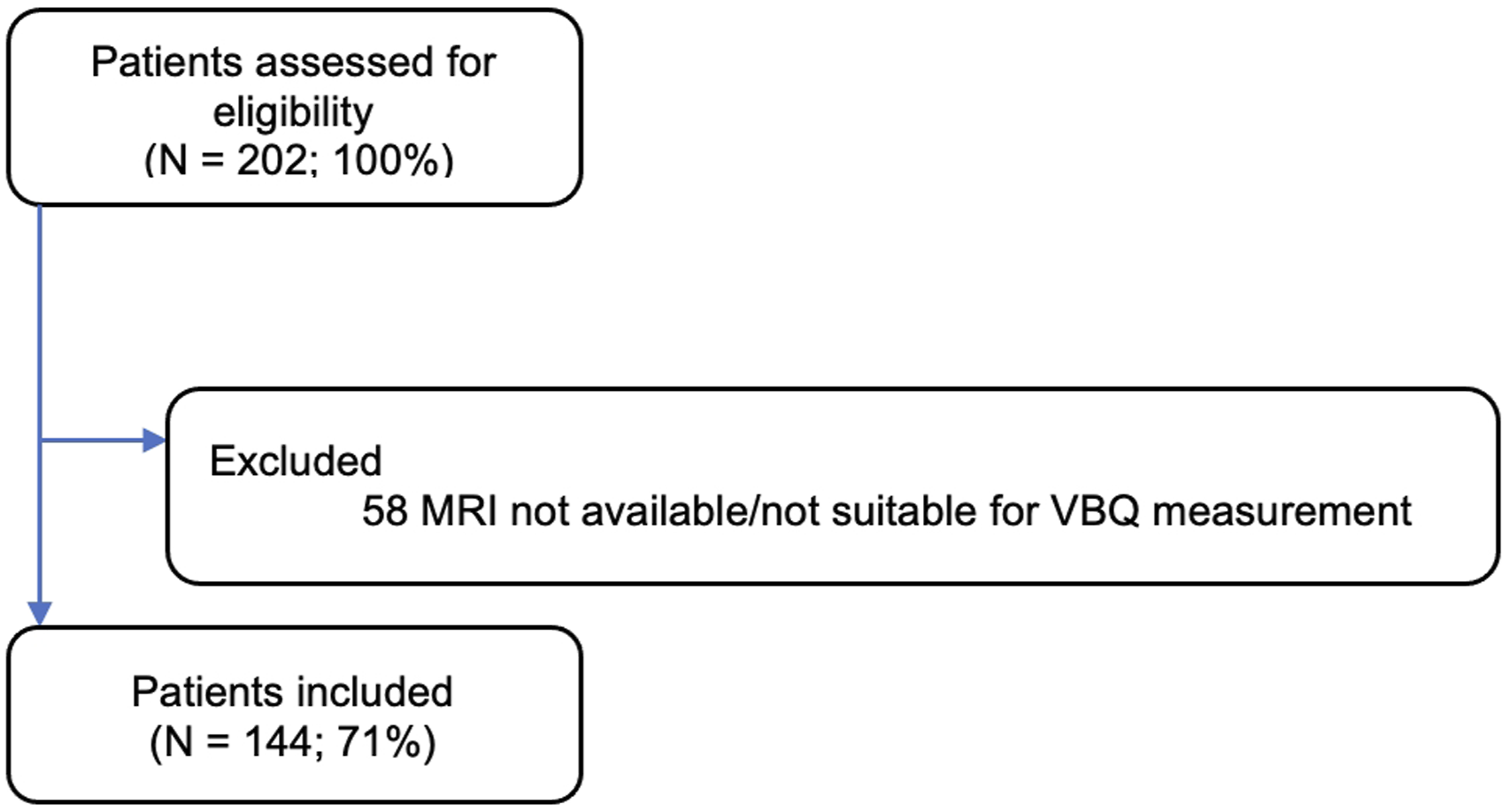
VBQ Score Values Stratified by Bone Quality as Defined by qCT Derived BMD
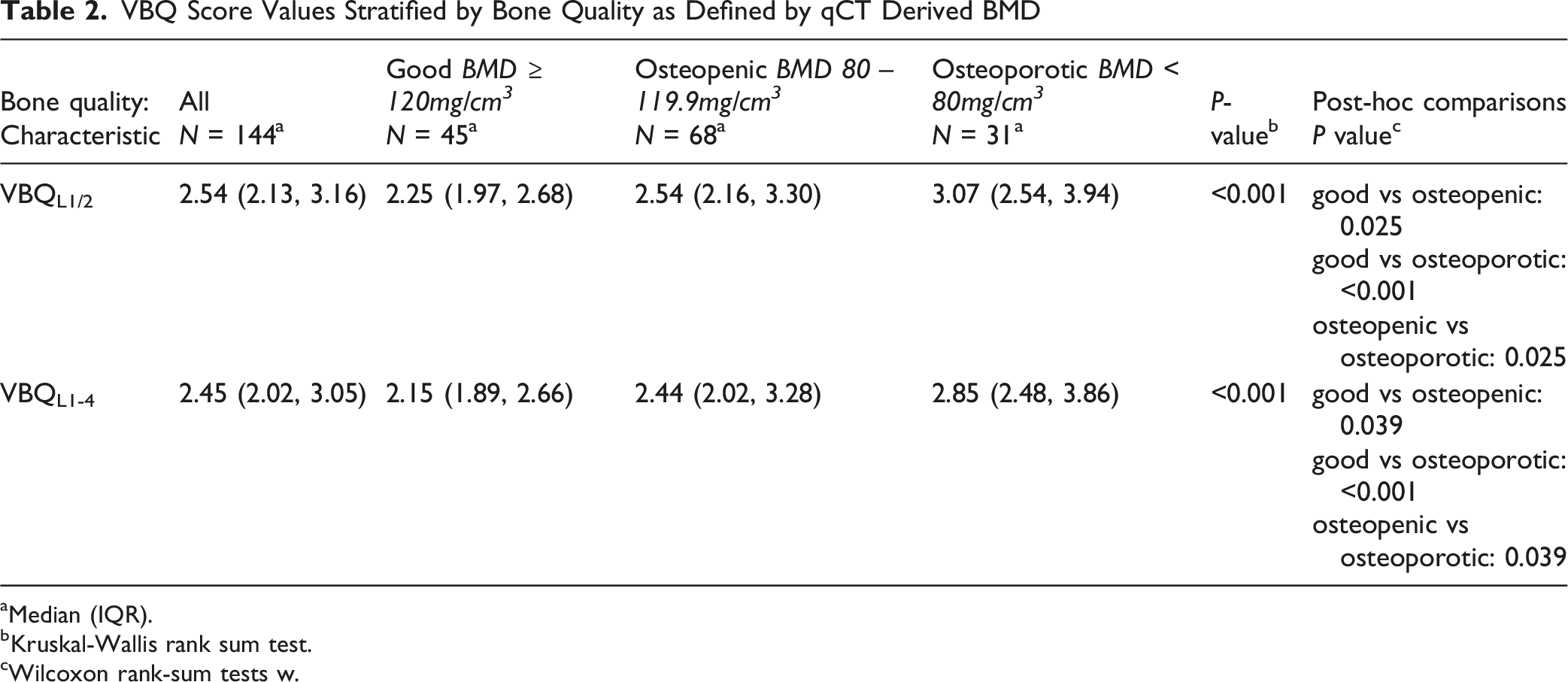
aMedian (IQR).
bKruskal-Wallis rank sum test.
cWilcoxon rank-sum tests w.
The ICC for agreement between VBQL1/2 and VBQL1-4 was 0.988 (95% CI: 0.982–0.991). Both VBQ variants showed a moderate negative correlation with BMD (VBQL1/2 rho = −0.41, P < 0.001; VBQL1-4 rho = -0.37, P < 0.001). For detecting osteoporosis with VBQL1/2, the ROC analysis derived an AUC of 0.71 (95% CI: 0.607-0.809) (cut-off: 2.30 (95% CI: 2.30-3.44), sensitivity: 94%, specificity: 45%, Figure 3A), while VBQL1-4 had an AUC of 0.69 (95% CI: 0.589-0.790) (cut-off: 2.63 (95% CI: 2.01-2.95, sensitivity: 71%, specificity: 64%, Figure 3B). For detecting impaired bone quality, VBQL1/2 had an AUC of 0.68 (95% CI: 0.593-0.774) (cut-off: 2.26 (95% CI: 2.25-3.00), sensitivity: 77%, specificity: 56%, Figure 3C), and VBQL1-4 had an AUC of 0.67 (95% CI: 0.582-0.765)(cut-off: 2.69 (95% CI: 2.08-3.02), sensitivity: 47%, specificity: 82%, Figure 3D). Receiver operator curve (ROC) analysis of the VBQL1/2 and VBQL1-4 to detect patients with osteoporosis (BMD < 80 mg/cm3) or impaired bone quality (osteoporosis or osteopenia, BMD < 120 mg/cm3). (A and B) ROC curves for detecting osteoporosis using VBQL1/2 and VBQL1-4, respectively, with Youden index optimization used to establish the cut-points of 2.30 (95% CI: 2.30-3.44) for VBQL1/2 and 2.63 (95% CI: 2.01-2.95) for VBQL1-4. (C and D) ROC curves for detecting impaired bone quality (osteopenia or osteoporosis) using VBQL1/2 and VBQL1-4, respectively, with optimized cut-points of 2.26 (95% CI: 2.25-3.00), for VBQL1/2 and 2.69 (95% CI: 2.08-3.02) for VBQL1-4. Sensitivity, specificity, and area under the curve (AUC) values are displayed within each panel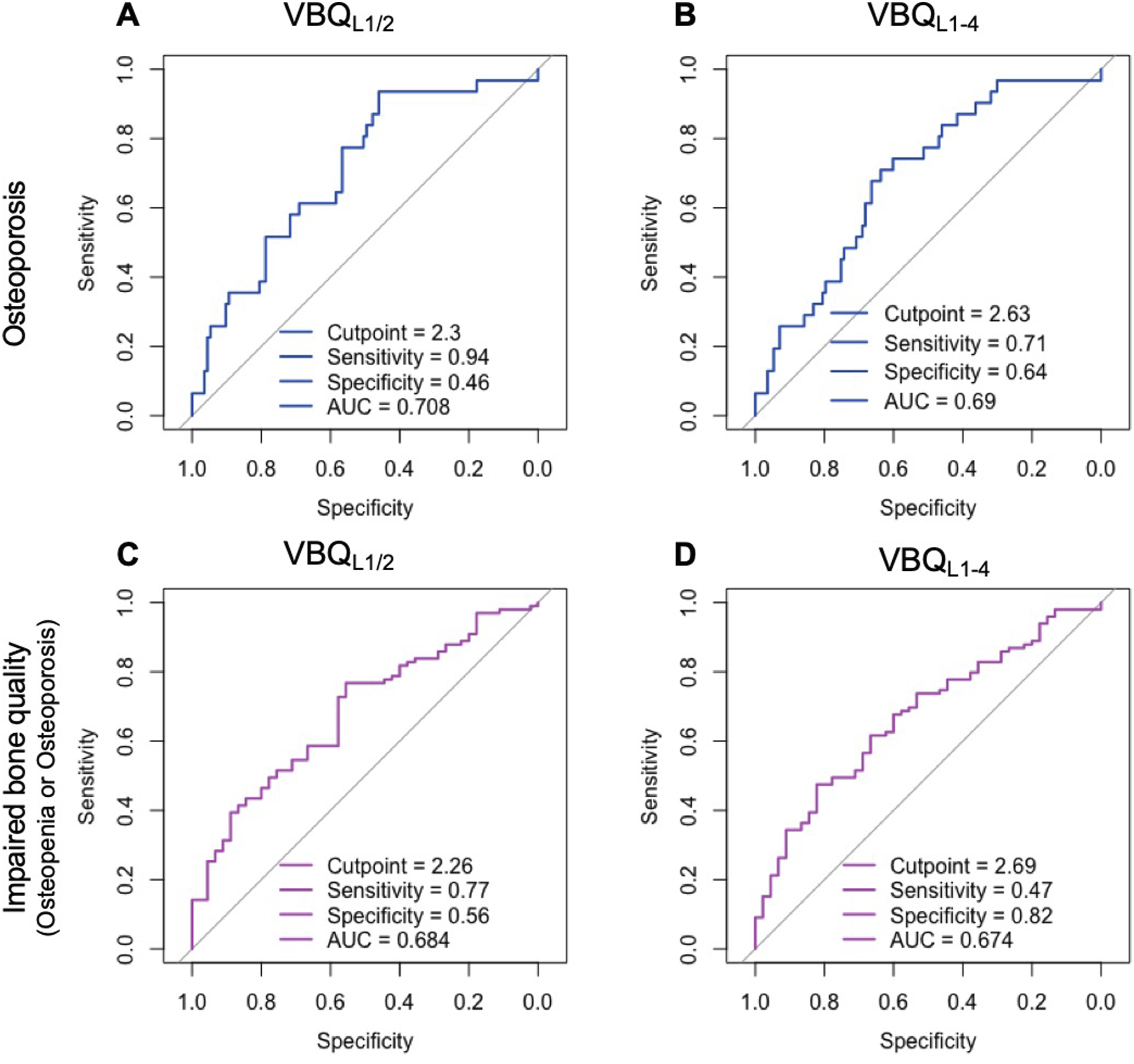
Discussion
This study analyzed patients undergoing surgery for DLS at the L4/5 level, comparing the modified VBQL1/2 to the VBQL1-4 methodology described by Ehresman et al, 16 as a potential method more streamlined use in MRI-based bone quality screening.
We observed the following key findings: • The VBQL1/2 and VBQL1-4 showed an excellent agreement (ICC 0.988; 95% CI: 0.982–0.991) despite minor differences in magnitude. • VBQL1/2 and VBQL1-4 were negatively correlated to BMD. • The VBQL1/2 had comparable performance in detecting osteoporosis (AUC 0.71 vs 0.68) or impaired bone quality (AUC 0.68 vs AUC 0.67), compared to the VBQL1-4. • A cut-off of 2.3 for VBQL1/2 resulted in a high sensitivity of 94% for detecting osteoporosis, with a moderate specificity of 45%, with no significant differences regarding demographic data, suggesting its potential diagnostic utility as a pre-screening tool for osteoporosis.
Impaired bone quality and osteoporosis are frequent among spinal surgery patients. In a recent meta-analysis,78% of spinal fusion patients aged 50 years or older were found to have osteopenia or osteoporosis, and 34% osteoporosis. 26 These rates are even higher than those observed in this cohort, potentially due to the inclusion of patients undergoing decompression alone for DLS in this study, or a location-based selection-bias. Impaired bone quality is linked to adverse outcomes after lumbar fusion surgery, 27 and perioperative anti-osteoporotic treatment can reduce these risks.3,28,29 However, the bone quality’s impact on lumbar decompression without fusion remains unclear. Preoperative screening could inform decision-making between decompression alone versus decompression with fusion in DLS, 19 and facilitate timely anti-osteoporotic treatment, reducing the risk of osteoporotic vertebral fractures (OVFs).7,29 OVF risk rises with paraspinal muscle degeneration,30,31 which correlates with reduced spinal BMD32,33 and altered bone microstructure. 34 As the surgical approach damages the paraspinal muscles, leading to their degeneration, 35 decompression surgery could further enhance the risk for OVF as it damages the paraspinal musculature, a topic that warrants further study. Incorporating opportunistic osteoporosis screening into preoperative assessments could optimize surgical planning and reduce OVF risk, reinforcing the clinical value of tools like VBQ.
In this study, VBQL1/2 demonstrated excellent agreement with VBQL1-4, and the AUCs to detect osteoporosis or impaired bone quality were comparable, indicating that the performance of VBQL1/2 is at least equal to that of the VBQL1-4. The slightly stronger correlation observed between VBQL1/2 and qCT-derived BMD may partly reflect anatomical concordance, as both measurements are obtained from the L1–L2 levels. Ehresman et al used L1-4 for the initial VBQ score based on its common application in BMD assessments (e.g., DXA) due to its representative sampling of lumbar bone quality. 16 However, this approach potentially limits its broader application in patients with advanced lumbar degeneration or previous fusion at lower segments. The L4/5 level is most commonly affected by degeneration and is the most frequently involved in lumbar fusion surgery, 36 which could distort the VBQL1-4 signal. Since degeneration and surgery are less prevalent in more cranial segments, qCT-derived BMD measurements are recommended for the upper lumbar spine. The VBQL1/2 offers additional advantages, including simpler measurement with only two segmentations and a straightforward calculation where the median equals the mean. This method may also be more applicable to a wider range of patients, particularly those with prior fusions or advanced lumbar degeneration.
For the detection of osteoporosis using VBQ, we observed that both VBQL1/2 and VBQL1-4 had lower performance than the initial study by Ehresman et al that used DXA-based osteoporosis definitions and reported an AUC of 0.81 in 68 spine surgery patients. 16 Early follow-up studies by Salzmann et al involving 296 patients using qCT for BMD measurements reported an AUC of 0.7118, aligning more closely with our results (0.68–0.71). Chen et al found a weaker VBQ-BMD correlation in patients with severe degeneration, which may explain our findings in our exclusively degenerative cohort. 37 Notably, VBQL1/2 demonstrated a high sensitivity of 94% for detecting osteoporosis. Prioritizing sensitivity over specificity could theoretically push sensitivity close to 100%, suggesting VBQL1/2 as a promising osteoporosis screening tool before lumbar fusion surgery. However, further studies are needed to validate its clinical utility, establish optimal cut-offs, and assess broader applicability.
The Congress of Neurological Surgeons mandates preoperative osteoporosis assessment for spinal surgery candidates, although specific guidelines are lacking. 11 Evidence-based screening algorithms tailored for LFS patients are therefore essential, as many may have undiagnosed osteopenia or osteoporosis. While VBQ is not a current diagnostic tool, it could be an additional risk indicator, encouraging the use of FDA-approved BMD assessment methods such as DXA or qCT, which are more accurate for detecting osteoporosis, even in patients with spinal degeneration. Integrating VBQL1/2 into clinical practice could streamline preoperative screening by using existing MRI scans to identify patients at risk for poor bone quality, potentially prompting further assessment with FDA-approved BMD methods like DXA or qCT. This approach allows efficient prioritization for additional testing, and with automated tools, could help tailor perioperative care plans to improve outcomes and reduce complications, such as osteoporotic fractures.
With VBQL1/2, we propose a tool with potentially broader applicability for patients with prior fusions or advanced spinal degeneration at the lower levels. This method demonstrated a slightly higher correlation with BMD than the conventional VBQL1-4, with improved sensitivity and reduced time for measurement and calculation. We hope this sparks further investigations that ultimately lead to optimized screening practices in lumbar fusion surgery patients.
Limitations
This study’s cross-sectional design and exclusion of non-degenerative spine cohorts limit conclusions on causality between low BMD and spinal degeneration. The absence of detailed data on osteoporosis screening prevented direct comparisons between DXA and qCT accuracy. The available medical history information restricted our ability to perform FRAX score comparisons as essential parameters were missing. Since osteoporosis treatment status was not analyzed, it remains unclear whether non-osteoporotic BMD readings in osteoporotic patients reflect varying treatment regimens. VBQ was not measured at intended instrumentation levels, therefore limiting conclusions on level-specific fixation or fusion outcomes. Finally, as this study focused on lumbar BMD, findings may not be generalizable to other skeletal sites, such as the femoral neck.
Conclusions
The VBQL1/2 demonstrated excellent agreement with the traditional VBQL1-4, with comparable performance in detecting osteoporosis and impaired bone quality. The higher sensitivity of VBQL1/2 suggests potential as an efficient pre-screening tool to identify patients at risk for osteoporosis, guiding further evaluation with FDA-approved BMD methods like DXA or qCT. Particularly in patients with prior fusions or advanced lumbar degeneration, VBQL1/2 provides a practical alternative without compromising diagnostic accuracy. Further research is needed to refine cutoff values and validate its clinical utility across broader populations, ultimately improving preoperative bone health screening and surgical outcomes.
Footnotes
Author Note
The Work Was Performed at Hospital for Special Surgery, New York City, NY, USA. The institutional review board of the Hospital for Special Surgery approved this study.
Acknowledgments
P.K. is a participant in the BIH-Charité Junior Clinician Scientist Program funded by the Charité–Universitätsmedizin Berlin and the Berlin Institute of Health.
ORCID iDs
Ethical Considerations
The study was approved by the HSS’ Institutional Review Board (IRB), under the approval number (IRB# 2015-237).
Consent to Participate
Informed consent was obtained.
Author Contributions
Conception and design: Paul Köhli Acquisition of data: Ali E. Güven, Paul Köhli, Erika Chiapparelli, Lukas Schönnagel, Gisberto Evangelisti, Roland Duculan Analysis and Interpretation of data: Paul Köhli, Alexander P. Hughes Drafting the article: Paul Köhli. Critically revising the article: all authors. Preparation of Graphical Content: Paul Köhli. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Alexander P. Hughes. Statistical analysis: Paul Köhli, Daniel M. Alschuler, Ranqing Lan. Administrative/technical/material support: Jennifer Shue, Study supervision: Alexander P. Hughes.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declare that they have no competing interests related to the materials or methods used in this study or the results reported in this article.
Data Availability Statement
The underlying data is available on reasonable request to the corresponding author.
Disclosure
Dr. Sama reports royalties from Ortho Development, Corp. DePuy Spine Products/Medical Device Business Services, Clariance, Inc.; private investments for Vestia Ventures MiRUS Investment, LLC, ISPH II, LLC, ISPH 3, LLC, and Centinel Spine (Vbros Venture Partners V); consulting fees from DePuy Spine Products/Medical Device Business Services, Clariance, Inc., Kuros Biosciences AG; speaking and/or teaching arrangements for DePuy Spine Products/Medical Device Business Services; membership of scientific advisory board of DePuy Spine Products/Medical Device Business Services, Kuros Biosciences AG, Clariance, Inc., and research support from Spinal Kinetics, Inc./Orthofix, Inc., outside the submitted work. Dr. Cammisa reports royalties from Accelus; ownership interest for 4WEB Medical/4WEB, Inc.; Healthpoint Capital Partners, LP; ISPH II, LLC; ISPH 3 Holdings, LLC; Ivy Healthcare Capital Partners, LLC; Medical Device Partners II, LLC; Medical Device Partners III, LLC; Orthobond Corporation; Spine Biopharma, LLC; Tissue Differentiation Intelligence, LLC; Tissue Connect Systems, Inc.; VBVP VI, LLC; VBVP X, LLC; Woven Orthopedics Technologies; consulting fees from Spine Biopharma, LLC, and Accelus; membership of scientific advisory board/other office of Healthpoint Capital Partners, Medical Device Partners II, LLC, Orthobond Corporation, Spine Biopharma, LLC, and Woven Orthopedic Technologies; and research support from 4WEB Medical/4WEB, Inc., Camber Spine, Choice Spine, DePuy Synthes, Centinel Spine, and Royal Biologics outside the submitted work. Dr. Girardi reports royalties from Lanx, Inc. and Ortho Development Corp.; ownership interest in Centinel Spine, BICMD; consulting fees from Lanx, Inc., Ortho Development Corp, and Sea Spine; stock ownership in Centinel Spine, Healthpoint Capital Partners, LP; membership of scientific advisory board/other office of Healthpoint Capital Partners, outside the submitted work. Dr. Hughes reports research support from Kuros Biosciences AG and Expanding Innovations, Inc.; private investments in Tissue Connect Systems, Inc.; and fellowship support from NuVasive, Inc. outside the submitted work.