
Abstract
Background
Spinal muscular atrophy (SMA) is caused by loss-of-function of the survival motor neuron 1 (SMN1) gene and deficiency of the ubiquitously expressed SMN protein. Genetic therapies can partially rescue motor units and improve prognosis of SMA, but effects of SMN shortage in other tissues has not been studied in detail.
Methods
We longitudinally assessed renal function in a cohort of patients with SMA before and after the start of genetic therapies.
Results
We enrolled 263 patients with SMA types 1c-4. Median age was 33 years (IQR: 22–49). Fifty (19%) patients had serum cystatin C based eGFR rates <90 ml/min/1.73m2, indicating increased risk of developing chronic kidney failure, 9 (3.5%) patients had eGFR compatible with chronic kidney failure (eGFR <60 ml/min/1.73m2) and 2 patients showed end-stage renal failure based on eGFR <15 ml/min/1.73m2. Symptoms of tubular dysfunction (abnormal low serum potassium levels (<3.8 mmol/L) and proteinuria) were present in 134 (51.7%) and 53 patients (22%), respectively. Forty-two (16%) patients had a history of kidney stones or nephrocalcinosis. Treatment with nusinersen or risdiplam resulted in reduction of the number of patients with hypokalaemia, but not of those with proteinuria. Cystatin C eGFR continued to decline during treatment.
Conclusions
Patients with SMA are at risk of impaired renal clearance, which does not improve after treatment with SMN2-splicing modifying therapies. Tubular function may improve partially following the start of treatment. These data indicate that SMN protein deficiency affects kidneys and that this will probably cause health problems in later life.
Introduction
Hereditary proximal spinal muscular atrophy (SMA) is characterized by motor neuron degeneration, muscle atrophy and weakness of proximal, axial and respiratory muscles. 1 Before gene-targeting treatments were available, SMA was the most important genetic cause of childhood mortality and childhood disability. SMA is caused by the loss of function of the SMN1 gene and the resulting deficiency of the survival motor neuron (SMN) protein. Adequate SMN protein levels are critical for many generic cellular functions including mRNA splicing, ubiquitination, endocytosis, ribosomal assembly and function and translation of specific mRNA. 2 In the absence of SMN1, the highly homologous human SMN2 gene that critically differs in a single nucleotide, ensures the production of residual levels of functional SMN protein. Variation in the number of SMN2 copies is the most important modifier of SMA severity, with higher copy number associated with milder disease, probably through a gene-dose mechanism that ensures higher SMN protein expression in motor neurons with increasing copy numbers.3,4
Alpha-motor neurons are obviously the most affected tissue in SMA, but the ubiquitous presence, generic functions and high expression levels of SMN protein in many tissues, suggest that other tissues and cell types may also be affected by its depletion. SMA animal models and post mortem studies of patients with severe SMA have indeed shown that SMA pathology may not be limited to motor neurons and that SMA has characteristics of a multi-system disorder, with abnormalities described in brain, heart, bones, kidney, pancreas and liver.5,6 The relevance of documenting systemic abnormalities has clearly increased since the introduction of genetic therapies for SMA that have been mostly developed to improve survival and motor function by targeting motor neurons. Meanwhile, the effects of such treatments on other tissues with high SMN expression are largely unknown.
Kidney tissue expresses high levels of SMN protein comparable to brain and spinal cord and with a similar distribution across nuclear, cytoplasmic and ribosomal compartments. 7 This may suggest that the kidney is particularly vulnerable to low SMN protein concentrations. The Taiwanese mouse model of severe SMA showed extensive pathological abnormalities in kidneys, including reduced nephron numbers and ultrastructural changes to the filtration layers of the remaining nephrons. 8 Moreover, impaired renal function with histopathological changes such as loss of brush border, flattened epithelium with detachment and sporadic protein casts, compatible with tubular dysfunction was found in a post-mortem study in a small cohort of infants with SMA type 1. 9
Taken together, these observations suggest that patients with SMA may be at increased risk of kidney disease. Because this has not yet been studied in detail, the aim of our study was to perform biochemical and clinical assessments of renal function in a large cohort of (young) adults with SMA.
Materials and methods
Subjects
The participants in this study take part in an ongoing observational cohort study on SMA in the Netherlands. The study was approved by the local Medical Ethics Committee (METC No. 09307/NL29692.041.09). Inclusion criteria for the ongoing cohort study are a genetic confirmation of SMA and residence in the Netherlands. We used multiplex ligation-dependent probe amplification (SALSA MLPA kit P021–B1–01 (MRC-Holland)) for genetic confirmation and SMN2 copy number determination based on exon 7 of the SMN2 gene.
All patients or their legal representatives gave written informed consent. Data for this study were collected during visits to the outpatient clinic of the UMC Utrecht that aimed to determine eligibility for reimbursed treatment with nusinersen (as of 1st February 2020) or for participation in a compassionate use program for risdiplam that started in February 2021 (Supplementary Fig. 1). We routinely performed renal function assessments every 8 months, with a maximum follow-up duration of 18 months in patients treated with risdiplam and 30 months in patients treated with nusinersen. We included serum samples of disease and healthy controls, gathered as part of an ongoing biobank study at the UMC Utrecht (METC No. 19190). All disease controls were diagnosed with ALS and had no history of renal comorbidities.
We determined SMA type according to the SMA classification system, i.e., based on the highest achieved motor milestone and age at onset of symptoms.10,11 We classified patients as non-ambulatory when they were wheelchair-bound or when they are only able to stand and move a few steps for the purpose of transfers.
Measurement of renal function
We assessed renal function, i.e., estimated glomerular filtration rate (eGFR) and tubular function, using serum (creatinine, cystatin C and potassium levels), urine samples (protein and β2-microglobulin concentrations) and 24 h urine collection (proteinuria, sodium, potassium, phosphate, uric acid, oxalic acid, citrate and calcium). 12 Treatment and follow-up protocols were different between patients treated with nusinersen and risdiplam. The central diagnostics laboratory analyzed serum samples approximately every 8 months in both treatment groups and in addition urine samples from patients treated with nusinersen and 24-h urine collections from patients treated with risdiplam (Supplementary Table 1). Hypokalemia was defined as potassium < 3.8 mmol/L in serum, i.e., the lower limit of the normal range from the central reference center. Creatinine levels are numerically expressed, with levels of < 9 defined as unmeasurable low. Proteinuria was defined as >0.14 g/L and β2-microglobulin was increased when >0.2 mg/L. Renal clearance expressed as eGFR (i.e., the flow rate of filtered fluids through the kidneys) was calculated based on serum cystatin C, using the CKD-EPI cystatin C formula. 13 Renal clearance was categorized as normal (eGFR >90 ml/min/1.73m2), mild renal failure (eGFR between 60 and 90/ml/min/1.73m2), moderate renal failure (eGFR <60 ml/min/1.73m2), severe <30 ml/min/1.73m2 or end-stage renal failure (eGFR <15 ml/min/1.73m2). 14 Kidney stones were identified by studying medical history and examine routine spinal CT scans (obtained to assess feasibility of intrathecal injections required for nusinersen) for calcifications (deposition of calcium in the kidney parenchyma and tubules).
Data analysis
Descriptive statistics were used to describe baseline characteristics. We present data in numbers with percentages for categorical variables. Continuous data is presented with mean (SD) when normally distributed and with median and interquartile range (IQR) when not normally distributed. Spearman's rank correlation coefficient (Spearman's rho) was used to measure the strength and direction of the associations between eGFR. Linear Regression analysis was performed to test whether the association between age and eGFR differed between groups. An independent samples t-test was conducted to compare mean eGFR between two groups. Friedman's test to analyze repeated measures data. A p-value <0.05 was considered as statistically significant. We used IBM/SPSS Statistics (version 27.0) for statistical analyses.
Sensitivity analysis
To compare creatinine and cystatin C-based eGFR, we included 100 healthy controls and 100 patients with ALS, both age-matched to our SMA cohort.
Results
Demographics
We included 266 patients. Clinical characteristics are summarized in Table 1. Three patients had a history of renal disease other than nephrocalcinosis. One patient had one functional kidney due to uretero-pelvic junction (UPJ) stenosis of the other kidney and another patient underwent a nephrectomy of the right kidney because of kidney stones. The third patient had a history of IgA glomerulonephritis and had undergone a kidney transplantation. We therefore excluded those patients from our final analysis (i.e., total 263 patients).
Baseline characteristics of 263 patients with spinal muscular atrophy.
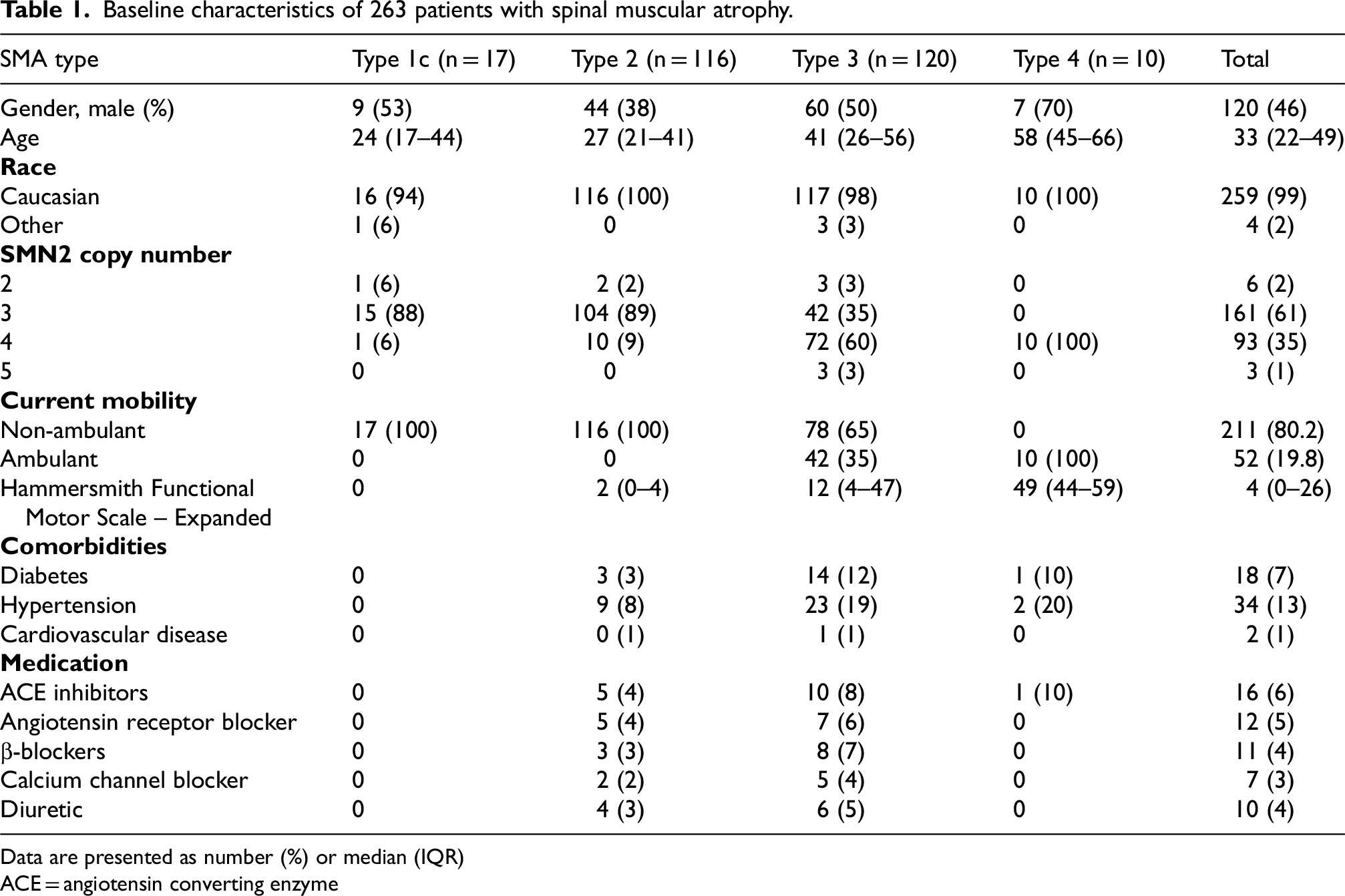
Data are presented as number (%) or median (IQR)
ACE = angiotensin converting enzyme
Cystatin C is reliable to assess renal clearance in patients with SMA
Creatinine levels in 257 patients varied from <9 μmol/L – 149 μmol/L, with a median value of 15 μmol/L (IQR: 11–28) in the 138 (53.7%) patients in which a creatinine level could be determined. In 119 patients (46.3%) creatinine was unmeasurable low due to their low muscle mass. We used cystatin C as an alternative to calculate eGFR (Figure 1). Median eGFR was 111 ml/min/1.73m2 (IQR: 93–123). 206 Patients (80.5%) had a normal renal clearance, 41 patients (16%) had mild renal failure. Moderate renal failure was measured in 6 patients (2.3%), severe renal failure in 1 patient (0.4%) and end-stage renal failure in 2 patients (0.8). Renal failure in general was not detected by creatinine eGFR and could have gone unnoticed. Moderate to severe renal failure was seen in two patients with SMA type 2 and seven with SMA type 3. Patients who suffered from diabetes mellitus or hypertension had a slightly impaired renal function, which was significantly (p < 0.001) lower than in the group of patients without diabetes mellitus or hypertension. Patients with either diabetes, hypertension or both were also significantly older (p < 0.001). Regression analysis showed a significant difference (p = 0.013) in slope for eGFR in time between both groups. Among patients without diabetes or hypertension the eGFR showed an average decline of 0.89 ml/min/1.73m2; in patients with diabetes and/or hypertension the average annual decline was 1.45 ml/min/1.73m2. (Supplementary table 2, supplementary table figure 2)
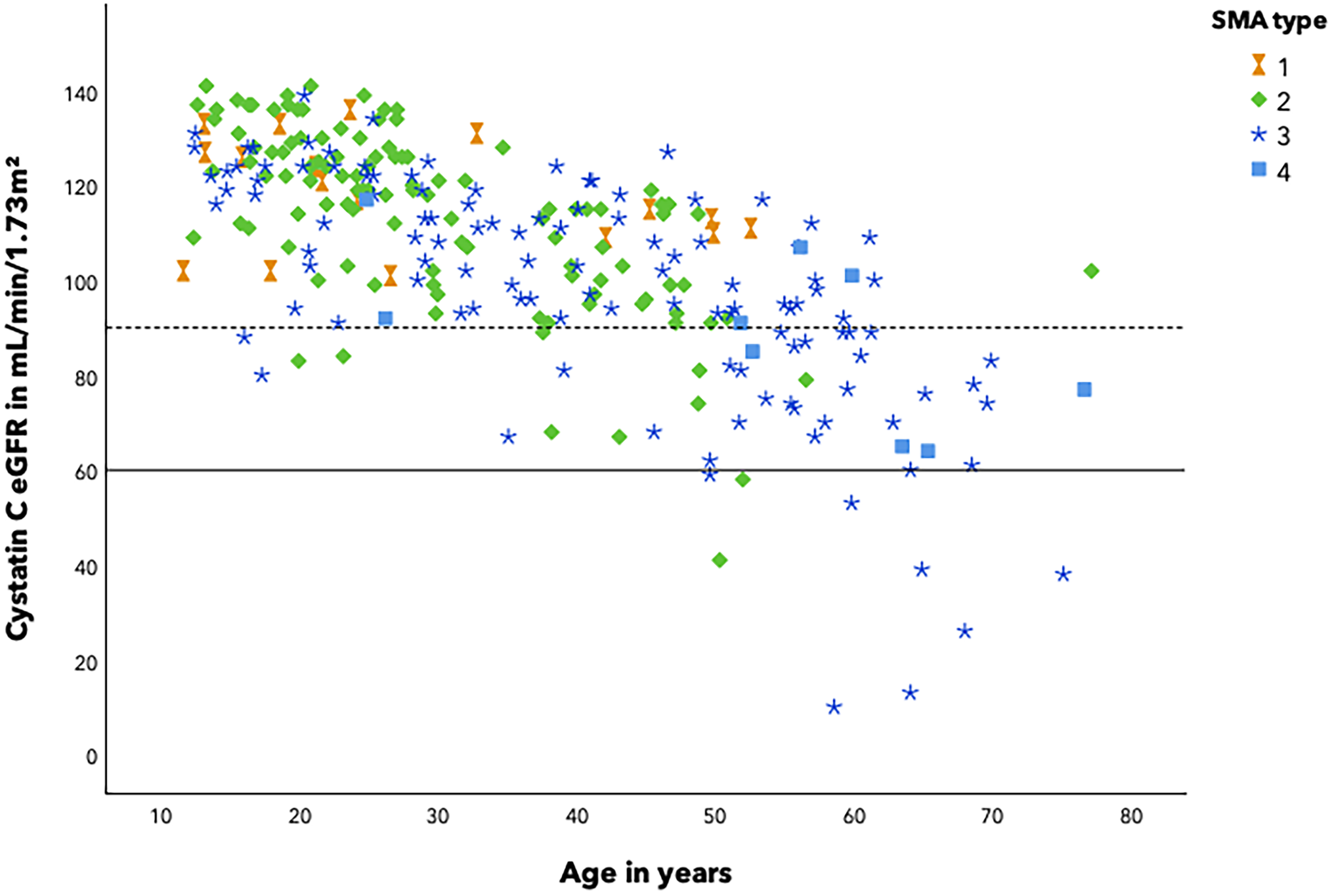
Impaired renal function in SMA patients. Renal clearance is impaired in patients with SMA. Cystatin C was used to estimate the global filtration rate (eGFR) in 259 patients with SMA (CKD-EPI formula, in mL/min/1.73m2 ) and plotted against age. There was a significant relationship between cystatin C eGFR and age, with an r2 = 0.357, p < 0.001 with a 1.011 mL/min/1.73m2 decrease in cystatin C eGFR for every year. SMA type is indicated with symbols.
Sensitivity analysis
Creatinine concentrations were lower in the ALS group than in the healthy control group but higher than in patients with SMA. This indicates that although eGFR based on creatinine concentrations is flawed in both SMA and ALS, the effect is much higher in patients with SMA. Baseline characteristics of healthy controls and disease controls and results are summarized in the supplemental file. (Supplementary Table 3,4).
Tubular dysfunction is common in SMA
We assessed protein levels in urine portions of 241 SMA patients. Samples from 53 patients (22%) showed elevated urine protein levels with a range of 0.15–1.09 g/L and 52 patients (21.6%) had elevated β2-microglobulin concentrations with a range of 0.21–29 mg/L. Additional 24-h urine collection of 85 patients confirmed protein loss of > 0.3 g/24h in six patients (7.1%) and β2-microglobulin >0.20 mg/L in 13 patients (16.5%). Proteinuria, in particular with significant elevated β2-microglobulin, indicates tubular dysfunction. To further investigate tubular function, we analyzed potassium levels in serum of 259 patients and found hypokalemia (potassium < 3.8 mmol/L) in 134 patients (51.7%). Five patients (1.9%) had potassium levels lower than 3.0 mmol/L without clinical symptoms of hypokalemia (Table 2). The kidney retains potassium and avoids excretion of potassium in the urine in case of hypokalemia. In 24-h urine collection samples of 80 patients we nevertheless observed an abnormal median potassium urine secretion of 42 mmol/24 h (IQR 32.4–54.6). There was no clear difference between urine potassium levels of 61 patients with serum hypokalemia (median potassium level 41.8 mmol/24 h (IQR 31.8–57.3) and 19 patients with normal serum potassium levels (median urine potassium of 44.5 mmol/24 h (IQR 34.2- 49.2). Comorbidities were equally distributed between the group of patients with and without hypokalemia. Patients with diabetes mellitus had increased levels of proteinuria. (Supplementary table 2).
Tubular dysfunction in patients with SMA.
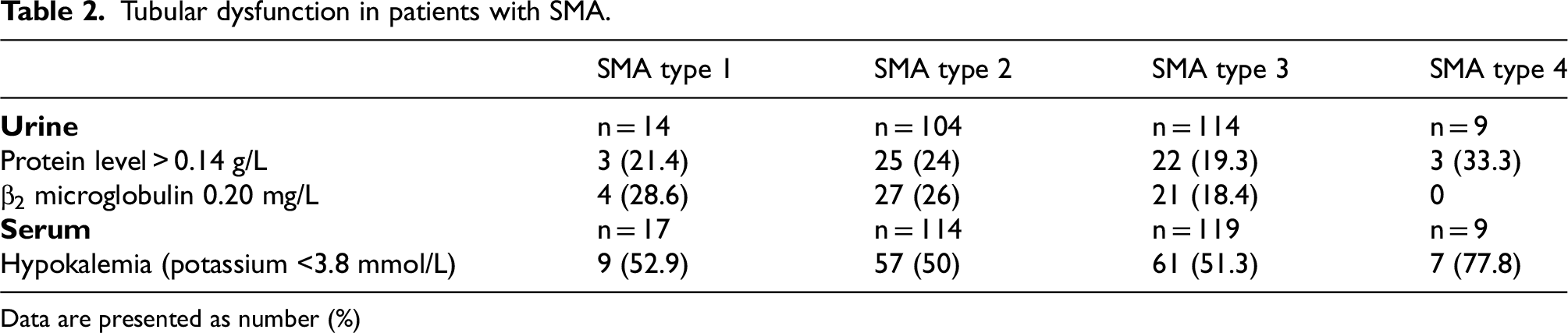
Data are presented as number (%)
Kidney stones and nephrocalcinosis
Twenty-nine patients (11%) had a documented history of kidney stones. By examination of routine spinal CT scans of 111 patients we found calcifications in (at least one of the) kidneys of 19 patients (17.1%). Thirteen of these patients (68.4%) had no medical history of kidney stones, totaling 42 patients (16%) with confirmed nephrocalcinosis. Urine samples of 88 patients did not show any abnormal values for calcium, citrate, oxalic acid and uric acid, which can be the cause of crystal formation when supersaturated. Serum calcium and urine pH levels were within the normal range (Supplementary Table 5). Protein levels were slightly increased in the group of patients with confirmed nephrocalcinosis (28.6%) compared to the group of patients without documented history (22%). No differences were observed between the groups in β2-microglobulin and potassium levels. A slight, but statistically significant difference in renal function was found between the group of patients without nephrocalcinosis (mean eGFR 108 ml/min/1.73m2) and the group with nephrocalcinosis (mean eGFR 94 ml/min/1.73m2) (p = <0.001).
Course of renal function during SMA-therapies (nusinersen and risdiplam)
A total of 231 patients (87%) started treatment with SMN2 splicing modifiers (nusinersen: 153 patients (67%); and risdiplam: 75 patients (33%)). Thirty-five patients could not be treated due to spondylodesis (with nusinersen) or decided against treatment. eGFR decreased during follow-up (Figure 2), irrespective of treatment (p < 0.0001). We documented a median cystatin C eGFR decrease of 14 ml/min/1.73m² during the 30-month follow-up in patients treated with nusinersen and 6 ml/min/1.73m² during the 18-month follow-up in patients treated with risdiplam. Urine protein levels did not change during follow-up. We observed a reduction in the number of patients with hypokalemia (55.1% to 26.1% in the group treated with Nusinersen and 56% to 42.4% in the group treated with Risdiplam) (Table 3).
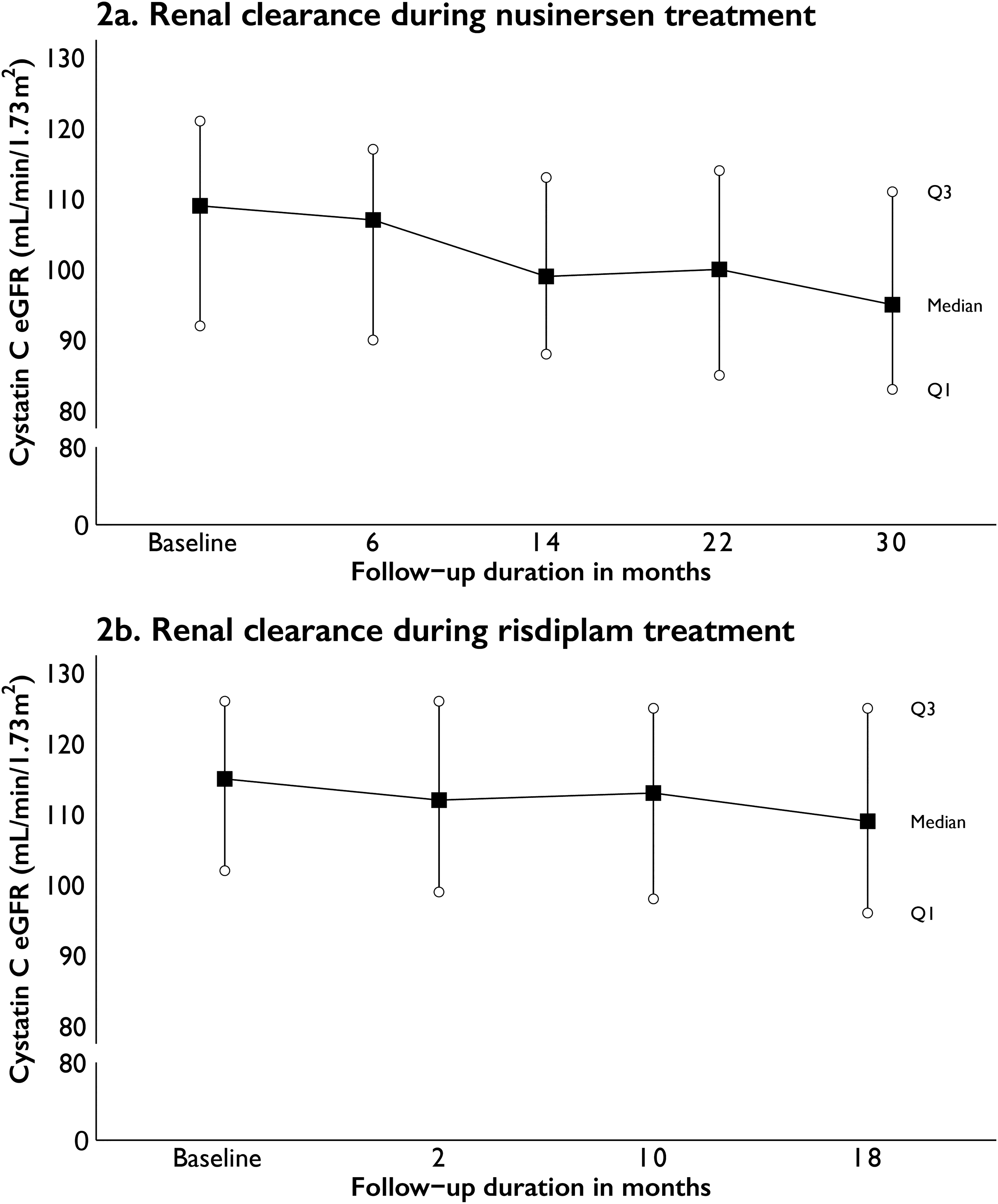
Median serum cystatin C eGFR during follow-up. (A) renal clearance during nusinersen treatment, median decrease of 14 mL/min/1.73m2 cystatin C eGFR between baseline and 30 months follow-up (B) renal clearance during risdiplam treatment, median decrease of 6 mL/min/1.73m2 cystatin C eGFR between baseline and 18 months follow-up.
Tubular (dys)function in treated patients.
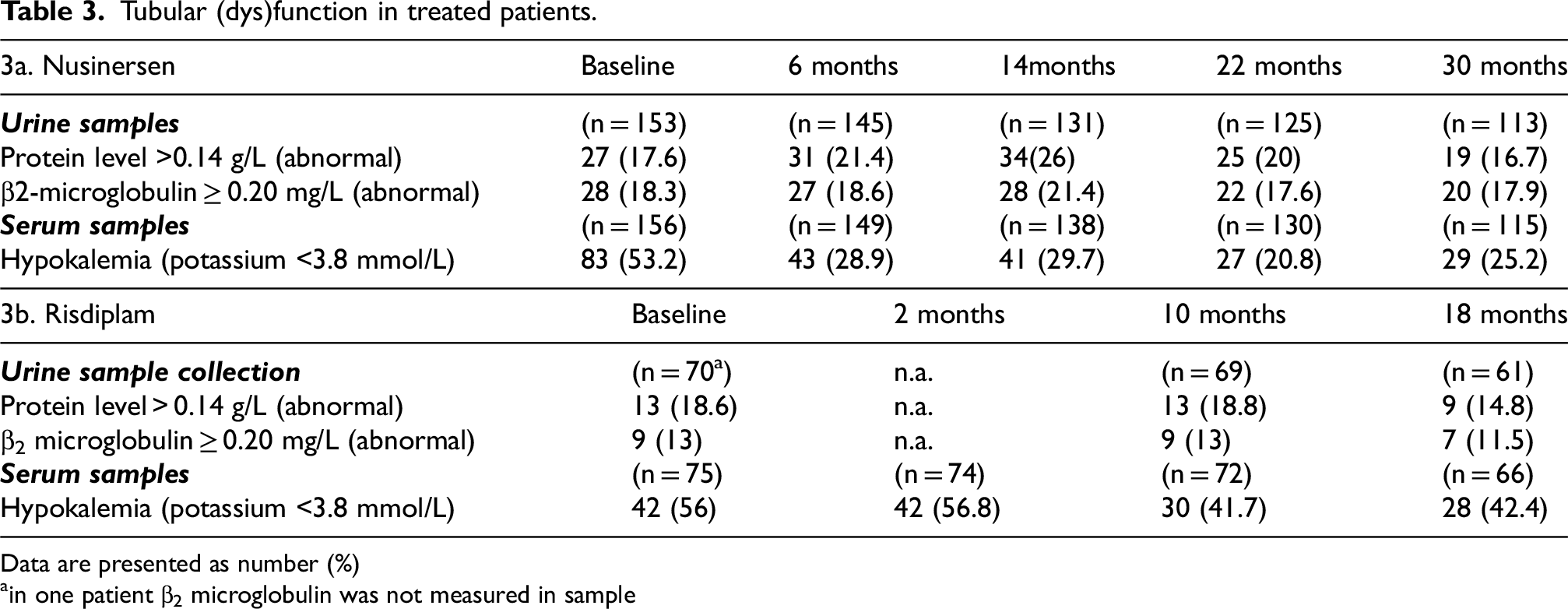
Data are presented as number (%)
in one patient β2 microglobulin was not measured in sample
Discussion
In this study, we assessed renal function in a large, single-center, population-based cohort of patients with SMA. We found that patients with SMA are at risk to develop a range of kidney-related pathologies, including decreased glomerular filtration rate, tubular dysfunction (i.e., hypokalemia and increased β2-microglobulin concentrations) and kidney stones or nephrocalcinosis. We found that decreased eGFR was underdiagnosed, due to routine but inappropriate use of serum creatinine concentrations and identified cystatin C as a useful alternative to calculate eGFR. Treatment with SMN2 splicing modifiers resulted in a partial reversal of tubular dysfunction, i.e., decrease of hypokalemia but not of urine protein levels and did not improve eGFR, which even markedly deteriorated during follow-up.
The kidney abnormalities found in mouse models and the equivalent levels of SMN protein expression and subcellular distribution in kidney compared to brain and spinal cord were reason to study renal function in patients with SMA in detail. 7 The most striking finding was that 9 patients with SMA had moderate to severe renal failure (eGFR < 60 ml/min/1.73m2), or even previously undiagnosed end-stage renal disease. This highlights the inappropriate routine monitoring of renal function by serum creatinine measurements in patients with SMA, especially in those with known risk factors for renal impairment such as diabetes and hypertension. Abnormally low muscle mass in SMA patients leads to creatinine levels that are below the detection limit in up to half of patients. Cystatin C, a low molecular weight protein that is produced constantly and independently of pathological conditions by all nucleated cells, is a widely available (although more expensive) alternative to adequately assess renal function. 15 Cystatin C measurements were previously found more suitable for monitoring renal function in patients with neuromuscular disorders and are increasingly used to asses eGFR in neuromuscular disorders with onset during childhood, which are often characterized by reduced muscle bulk. 16 However, we here show that even in neuromuscular diseases with adult onset such as ALS, creatinine measurements may not adequately reflect eGFR and that cystatin C levels represent a more reliable alternative.
Cystatin C-based eGFR indicate impaired renal clearance in patients with SMA at a relatively young age. Ageing is accompanied by a decrease in renal clearance of 1 ml/min/1.73m2 per year. 17 Our data suggests that this decline is sharper in patients with SMA, especially in patients with comorbidities as hypertension and diabetes and that this may ultimately increase the risk of renal failure at a relatively young age. 18 The mechanism underlying the decline in eGFR remains unknown. However, our study highlights the importance of prevention and follow-up in cardiovascular risk management for patients with SMA. It is possible that the abnormal development of vasculature that has been observed in SMA contributes to renal vulnerability by affecting glomerular function. 19 Our data also suggest that SMA severity does not determine renal vulnerability, since patients with SMA type 3 were among those with end stage renal disease. Moreover, the close-to-normal life expectancy of patients with SMA type 3 indicates that monitoring of renal function should not be confined to more severe phenotypes. 3
In addition to decreased abnormal clearance of the glomerulus, we observed proteinuria (with elevated β2-microglobulin) and hypokalemia compatible with abnormal tubular function. 22% of patients had proteinuria, a surprising finding given the relatively young age of our population and the virtual absence of relevant co-morbidity such as diabetes or cardiovascular disease. Elevated urine levels of β2-microglobulin, a protein with a lower molecular weight (12 kDa) compared to albumin (69 kDa), indicates impaired reabsorption in the proximal tubule. 12 This hypothesis is further supported by the high percentage (>50%) of patients with hypokalemia (<3.8 mmol/L). Decreased potassium levels are most often caused by renal potassium loss as insufficient potassium intake rarely causes significant hypokalemia. 20 Potassium intake is typically between 40 to 120 mmol/L per day, most of which is excreted via urine. When potassium plasma levels are low, the kidney lowers potassium excretion to a minimum of 5 to 25 mmol/L per day. Potassium secretion is mediated by the principal cells in the two segments that follow the distal tubule: the connecting segment and cortical collecting tubule. 20 Patients with hypokalemia had an average potassium excretion of 42 mmol/24 h, which is inappropriately high, supporting the concept of tubular dysfunction. Several tubulointerstitial diseases can lead to increased excretion of smaller proteins but are unlikely causes in patients with SMA. 12
Kidney stones are a common problem in general population, with a prevalence of around 5.5% in age groups between 20 to 39 years that increases to 10.6% and 19.7% percent respectively in females and males of 80 years and older, but the percentage of patients with SMA and kidney stones or nephrocalcinosis (16%) is higher than in the general population. 21 However, renal dysfunction is not a likely cause for nephrocalcinosis in SMA, since there were no biochemical abnormalities of the urine composition. Patients reported that, due to their impaired mobility, they lower daily intake of fluids. Low urine volume, in combination with the need for a wheelchair, scoliosis or other changes in physique and posture that may lower urine flow are the most likely causes of kidney stones in patients with SMA.
Our study reaffirms that SMA pathology is not limited to the CNS. Metabolic dysfunction in SMA patients and abnormal coagulation parameters have previously been described as extra-neural abnormalities in SMA.22,23 The high concentrations of SMN protein found in tubuli of the adult human kidney indicate that SMN protein may be required for normal tubular function. 24 In addition to the role of SMN protein in the translation of specific mRNA, its role in facilitating endocytosis and vesicle trafficking may be relevant since tubular function probably depends on discrete endocytic processes.7,25–27 Endocytosis in neurons and at the neuromuscular junction depends on sufficient SMN function and expression. 28 SMN has been found associated with the actin cytoskeleton, which is crucial required for endocytic function. 29 SMN may act as a regulator of cytoskeletal function and although this has not yet been investigated in kidneys, this may provide a molecular explanation for our observations. We analyzed effects on renal function of SMN2-splicing modifying therapies that augment SMN protein concentrations. SMN2 splicing modifiers (i.e., nusinersen or risdiplam) did not attenuate the decline in renal clearance. We found a clinically significant decrease in median cystatin C eGFR of 14 ml/min/1.73m² in patients treated with nusinersen for 30-months and 6 ml/min/1.73m² in 18 months in patients with risdiplam. The possible toxicity of antisense oligonucleotides on renal function was described before. In mice, oligonucleotide was thought to be present in the proximal tubules because the tubules contained small round basophilic granules. It is still uncertain whether renal toxicity is associated with the accumulation of basophilic granules. Other research indicates that vacuolation in the tubules occurs when antisense oligonucleotides are taken up by the endosomal/lysosomal system. 30 In contrast, no nephrotoxicity has been reported in association with risdiplam.
Because, at present, neither the literature nor our study provide certainty regarding the natural course of eGFR decline in SMA patients or the impact of current therapies, renal function in patients with SMA should be closely monitored through routine Cystatin C assessment.
In contrast to the possible aggravating effects on eGFR, treatment with SMN2 splicing modifiers did reduce the number of patients with hypokalemia, suggesting partial improvement of tubular function. We cannot exclude the possibility that reversal of proteinuria needs periods longer than the follow-up in this study.
In conclusion, our data suggest that renal function is impaired at different levels in patients with SMA, irrespective of disease severity. The kidney is a vulnerable organ when exposed to SMN deficiency for decades. Genetic SMA therapies only partially improve renal function. Renal function should be carefully monitored using serum cystatin c and/or urine analysis in all patients with SMA, to ensure timely interventions.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602251377240 - Supplemental material for Impaired renal function in patients with spinal muscular atrophy: A longitudinal cohort study
Supplemental material, sj-docx-1-jnd-10.1177_22143602251377240 for Impaired renal function in patients with spinal muscular atrophy: A longitudinal cohort study by Fay-Lynn Asselman, Sabine CA Meijvis, Renske I Wadman, Inge Cuppen, Robin WM Vernooij, Lina M Vermeer, Leonard H van den Berg, Ewout JN Groen and W Ludo van der Pol in Journal of Neuromuscular Diseases
Footnotes
Abbreviations
Acknowledgements
We thank our patients and their families for continuous participation in our cohort study.
Ethical considerations
The participants in this study take part in an ongoing observational cohort study on SMA in the Netherlands. The study was approved by the local Medical Ethics Committee (METC No. 09307/NL29692.041.09).
Consent to participate
All patients or their legal representatives gave written informed consent.
Consent for publication
Not applicable.
Funding
This work was supported by grants from stichting Spieren voor Spieren.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.