
Abstract
Patients suffering from cognitive decline such as mild cognitive impairment or neurodegenerative disorders including Alzheimer’s dementia, vascular dementia, frontotemporal dementia, and Lewy body dementia are often accompanied by symptoms like psychosis, depression, agitation, and apathy. Aging increases not only the prevalence of dementia but also the development of kidney disorders, which had emerged as possible risk factor of cognitive impairment and dementia. However, a contribution of renal dysfunction to psychosis associated with cognitive decline remains to be investigated. We addressed the question whether patients diagnosed with mild cognitive impairment or dementia and co-symptoms show alterations in serum parameters. Analyzing 309 patients in total, we detected a positive correlation between the occurrence of psychotic symptoms and increased retention parameters in serum, including creatinine and urea levels and the estimated glomerular filtration rates. This was in particular detected in female patients. In male patients, psychotic symptoms were associated with an increased number of leukocytes in blood. We propose that clinicians should be aware of psychotic symptoms in patients with reduced cognitive functions that could be associated with changes in the retention parameters.
Keywords
INTRODUCTION
With increasing age, the number of patients suffering from dementia is constantly rising [1]. Frequent neurodegenerative disorders include Alzheimer’s dementia (AD), vascular dementia (VaD), frontotemporal dementia (FTD), and Lewy body dementia (LBD). Mild cognitive impairment (MCI) is another common cause of memory loss in older people; about 10% of MCI patients progress to dementia each year [2]. Dementia includes a heterogeneous group of disorders that lead to cognitive decline [3]. Although cognitive decline is a core feature of dementia, these disorders may be associated with a variety of neuropsychiatric symptoms, which include affective and motivational symptoms, perceptual disturbances, delusions, disturbances of basic drives, and disinhibition and inappropriate behaviors. Investigations concerning the prevalence of these symptoms illustrated that within 5 years, 97% of patients experienced at least one symptom [4]. These neuropsychiatric symptoms fluctuate throughout the disease and could be distressing to the patient as well as the caregiver. Characteristics of psychotic symptoms in AD, the most frequent type of dementia, include delusions and hallucinations, agitation, and aggression. Psychosis is also a common feature that occurs with different prevalence in VaD, FTD, and LBD [5–8]. VaD is associated with a high frequency of psychosis, in particular delusions and depression [9, 10]. In LBD, visual hallucinations and delusions are common. Psychosis in FTD occurs with a prevalence of about 10% [11] and is especially characterized by verbal outbursts and inappropriate activities [12]. These symptoms may be a distinct clinical entity with poor outcome [13].
Cognitive decline alone cannot explain the occurrence of psychotic symptoms. Several biological factors have been identified which are associated with psychological symptoms in dementia including genetic factors, homocysteine levels, vascular changes, and psychosocial factors [14]. Hyperlipidemia, hypertension, and diabetes mellitus are risk factors for vascular changes, associated with moderate cognitive deficits and increase the risk of dementia in the elderly and might influence the development of psychosis [15–17]. The various contributing factors also include acute medical disorders. Previous studies suggested that demented patients suffer disproportionately more from undiagnosed medical illnesses than patients without cognitive impairment [18–20]. Infections of the urinary tract, pneumonia, dehydration, and anemia are frequent undiagnosed but treatable medical conditions that may contribute to abnormal behaviors and poor life quality [21].
Dehydration and malnutrition are common in demented patients and can result in hospitalizations [22]. It is important to note that dementia, admission to hospital with infection or dehydration, malnutrition, and renal impairment are common risk factors for delirium and urinary infections and electrolyte disturbance (dehydration, renal failure, hyponatremia, or hypernatremia) are precipitants for a delirium [23]. Delirium is the most frequent complication to hospital admission for older people and contributes substantially to increased mortality and morbidity. Features of a delirium include recent onset of fluctuating awareness, impairment of memory and attention, disorganized thinking, hallucinations, and disturbances in the sleep-wake cycle [24]. Given the strong inter-relationship between delirium and dementia, it might be difficult to distinguish both [25]. Dementia is associated with an increased risk of developing a delirium and vice versa.
The aim of our present study was to identify parameters obtained by routine blood analysis that may be associated with psychosis and patients with MCI, AD, VaD, FTD, and LBD.
METHODS
Study design and cohort
The study was performed in accordance with German laws, The Code of Ethics of the World Medical Association (Declaration of Helsinki), and the guidelines of the local institutional review board. All patients or, if necessary, their guardians have expressed their written informed consent for participation in this study.
The inclusion criterion for this study was the presence of one of the following diagnoses: MCI, AD, VaD, FTD, LBD, or mixed dementia (MD). Exclusion criteria were other types of dementia or other reasons for a loss of cognitive functioning, like alcohol-related dementia, normal pressure hydrocephalus, Parkinson’s disease dementia, Huntington’s disease, Creutzfeldt-Jakob disease, or depressive pseudodementia. In total, data from 309 geriatric psychiatry patients, suffering from MCI (n = 75) or dementia (n = 234), were involved in the present study. The dementia group consisted of 139 patients with MD, 40 AD patients, 38 VaD patients, 12 FTD patients, and 5 LBD patients. Mixed dementia was defined as a combination of two or more of the named dementia subtypes. The included patients were European Caucasians aged from 59 to 93 years and about 71.8% of the study participants were female. All these patients were treated at the geriatric psychiatry ward of the Department of Psychiatry at the University of Magdeburg, between 2010 and 2014. The most common reasons for treatment were, on the one hand, elective evaluations of cognitive deficits with influence of the daily living and, on the other hand, emergency referrals because of acute difficulties in their domestic environments. The correct diagnosis of MCI or a type of dementia according to ICD-10 criteria was made by skilled psychiatrists. For diagnosis, the medical history, the physical examination, magnetic resonance imaging (MRI) or computed tomography, neuropsychological assessments, if possible a lumbar puncture, and where appropriate an electroencephalography were used. The neuropsychological assessments were performed by trained psychologists or clinicians using Mini-Mental State Examination (MMSE) and Consortium to Establish a Registry for Alzheimer’s Disease-Neuropsychological Assessment Battery to evaluate the cognitive functions of the patients. Patients with MCI are able to function in everyday activities but have a slight but noticeable and measurable decline in cognitive abilities, including memory and thinking skills. The MMSE score usually ranges between a 25 and 28. The most common symptoms of AD patients are short-term memory loss and word-finding difficulties, but these patients are restricted in everyday activities. Diagnostic parameters include atrophy in the hippocampus, but also parts of the brain including temporal and parietal lobes (MRI) and characteristic changes in cerebrospinal fluid values (p tau >50 pg/ml, total tau >350 pg/ml, Aβ1 - 42 <485 pg/ml, Aβ ratio <0.8). VaD is caused by a disorder or injury that affects the blood supply to the brain. Typically, it involves a series of minor strokes. The symptoms of this dementia are dependent on the area in the brain where the strokes have occurred and the size of the vessels. Despite the typical alterations detected in MRI, no changes in Aβ or tau in cerebrospinal fluid are present. Patients with LBD primarily show visual hallucinations, fluctuations in alertness, slowness of movement, and features of Parkinson’s disease including tremor, rigid muscles, and a face without emotion. FTD is characterized by drastic personality changes and language difficulties; memory problems are not a main feature. MRI studies detected shrinking of the frontal and temporal lobes of the brain.
In the next step, the 309 subjects were classified into two groups according to the presence (n = 117) or absence (n = 192) of psychotic symptoms (Tables 1 and 2). Psychotic symptoms were considered if they were the primary cause for admission to our hospital or if they developed during the inpatient stay. For more differentiated analyses these two groups were further divided into sex-specific subgroups (Tables 1 and 3). All patients with psychotic symptoms received anti-psychotic medication immediately upon arrival at our university clinic (Table 4).
Demographic and biochemical characteristics of the study population diagnosed with mild cognitive impairment or dementia
*p < 0.05, **p < 0.01, Mann-Whitney U test. MMSE, Mini-Mental State Examination; CRP, C-reactive protein; WBC, white blood cell; eGFR, estimated glomerular filtration rate; ALT, alanine aminotransferase; AST, aspartate aminotransferase.
Demographic, biochemical, and clinical characteristics of the total sample diagnosed with mild cognitive impairment or dementia
*p < 0.05, Chi-square test with Yates correction, aFisher’s exact test. CRP, C-reactive protein; WBC, white blood cell; eGFR, estimated glomerular filtration rate.
Demographic, biochemical, and clinical characteristics of male and female patients diagnosed with mild cognitive impairment or dementia
**p < 0.01, Chi-square test with Yates correction. aFisher’s exact test. eGFR, estimated glomerular filtration rate; ALT, alanine aminotransferase; AST, aspartate aminotransferase.
Treatment of psychotic symptoms in patients with MCI or dementia
Given is the total number of psychotic patients, the number of treated patients and the drugs used to treat psychotic symptoms in patients with impaired cognitive function.
Psychopathological and clinical laboratory measurement
Psychopathology was assessed using the Association for Methodology and Documentation in Psychiatry scale [26]. Psychotic symptoms were defined as the occurrence of one or more of the following symptoms: hallucinations, delusions, and delusional misidentifications. As part of the routine diagnostic procedures, blood samples were obtained in clinical indication by peripheral venipuncture. The venous blood samples were collected before breakfast between 8:00 a.m. and 9:30 a.m. and as soon as possible after admission and were analyzed within one hour after collection. Out of about 55 gathered routine laboratory parameters, 7 parameters were examined closer in the present study (Table 1). Laboratory reference ranges were <5.0 mg/L for C-reactive protein (CRP), 4.0–10.0 Gpt/L for white blood cell count (WBC count), 59–104μmol/L for creatinine (men), 45–84μmol/L for creatinine (women), <11.9 mmol/L for urea, 0.17–0.83μmol/s.L for alanine aminotransferase (ALT) (men), 0.17–0.58μmol/s.L for ALT (women), 0.17–0.83μmol/s.L for aspartate aminotransferase (AST) (men), and 0.17–0.58μmol/s.L for AST (women). The estimated glomerular filtration rate (eGFR) was calculated with the CKD-EPI (hronic idney isease demiology collaboration) equation. An exact classification of renal function was obtained by grouping of female patients according to their eGFR: Group 1:90 mL/min/1.73 m2 or above (normal or high kidney function); group 2:60–89 mL/min/1.73 m2 (mildly decreased); group 3a: 45–59 mL/min/1.73 m2 (mildly to moderately decreased), group 3b: 30–44 mL/min/1.73 m2 (moderately to severely decreased), group 4:15–29 mL/min/1.73 m2 (severely decreased); and group 5: <15 mL/min/1.73 m2 (kidneyfailure).
Statistical analysis
The data were analyzed retrospectively and anonymously. All data analyses and statistical procedures were performed using the statistical software SPSS (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.). Demographic, clinical, and laboratory parameters were presented as medians with minimum and maximum values or as numbers and percentages. After testing for normal distribution with the Kolmogorov-Smirnov test, the non-parametric Mann-Whitney U test was used for analysis of continuous data. The Chi-square test with Yates correction and, if necessary, Fisher’s exact test was used to compare frequencies between the groups. To determine variables significantly associated with psychotic symptoms in MCI and dementias, a binary logistic regression model with backward elimination (using backward Wald) were employed (Supplementary Table 1). Statistical significance was considered when p < 0.05 and several significant results were presented in graphs.
RESULTS
Increased retention parameters in plasma of patients with psychotic symptoms
Our study cohort consisted of 309 individuals, 222 women (71.8%), and 87 men (28.2%); 117 patients showed psychotic symptoms, independent of gender (37.8% females, 37.9% males). The prevalence of psychosis ranged between 28.9% VaD and 100% in LBD patients (Supplementary Table 1). Retrospective analysis of serum laboratory parameters obtained revealed no differences in liver associated parameters AST and ALT as well as CRP level between psychotic and non-psychotic female and male patients. The WBC count in psychotic and non-psychotic females was also comparable, but in male patients a trend was detected concerning an enhanced WBC level (mean 7.3 Gpt/L) and the occurrence of psychotic symptoms compared to male persons without psychosis (mean 6.55 Gpt/L; p = 0.051; Table 1). Although we found no association between the occurrence of psychosis in female or male patients and the levels of sodium potassium and chloride (Supplementary Table 2), we detected an association between the presence of psychotic symptoms, and several renal associated parameters, creatinine and urea levels and eGFR. eGFR measures the level of kidney function. It is calculated from the results of the blood creatinine test, age, body size, and gender. Increased creatinine levels (86μmol/L) and urea levels 6.3 (mmol/L) were detected in psychotic patients compared to non-psychotic individuals (creatinine: 76μmol/L, p = 0.004; urea: 5.8 mmol/L, p = 0.022; Fig. 1). In psychotic patients, the eGFR was reduced to 60 mL/min/1.73 m2 compared to 69.9 mL/min/1.73 m2 in non-psychotic patients (p = 0.013), indicating a renal dysfunction in these patients. This effect was especially present in females: the creatinine levels (84μmol/L compared to 72μmol/L; p = 0.012) and the urea levels (6.2 mmol/L compared to 5.7 mmol/L; p = 0.046) were significantly increased in psychotic female patients compared to non-psychotic individuals. In psychotic female patients, the eGFR was decreased (57 mL/min/1.73 m2) compared to non-psychotic female (68.1 mL/min/1.73 m2). In male patients, we detected no significant differences in these plasma retention parameters. We found no significant association between the presence of psychosis and an imbalance of sodium, potassium, or chloride, neither below nor above the reference ranges (Supplementary Table 3). We also determined no correlation between these ions and eGFR, urea, or creatinine values (Supplementary Table 4). Neither hypertension nor hyperlipidemia or diabetes mellitus, known to contribute to neurocognitive disorders and maybe also psychosis, had a significant impact upon occurrence of psychosis (Table 2).
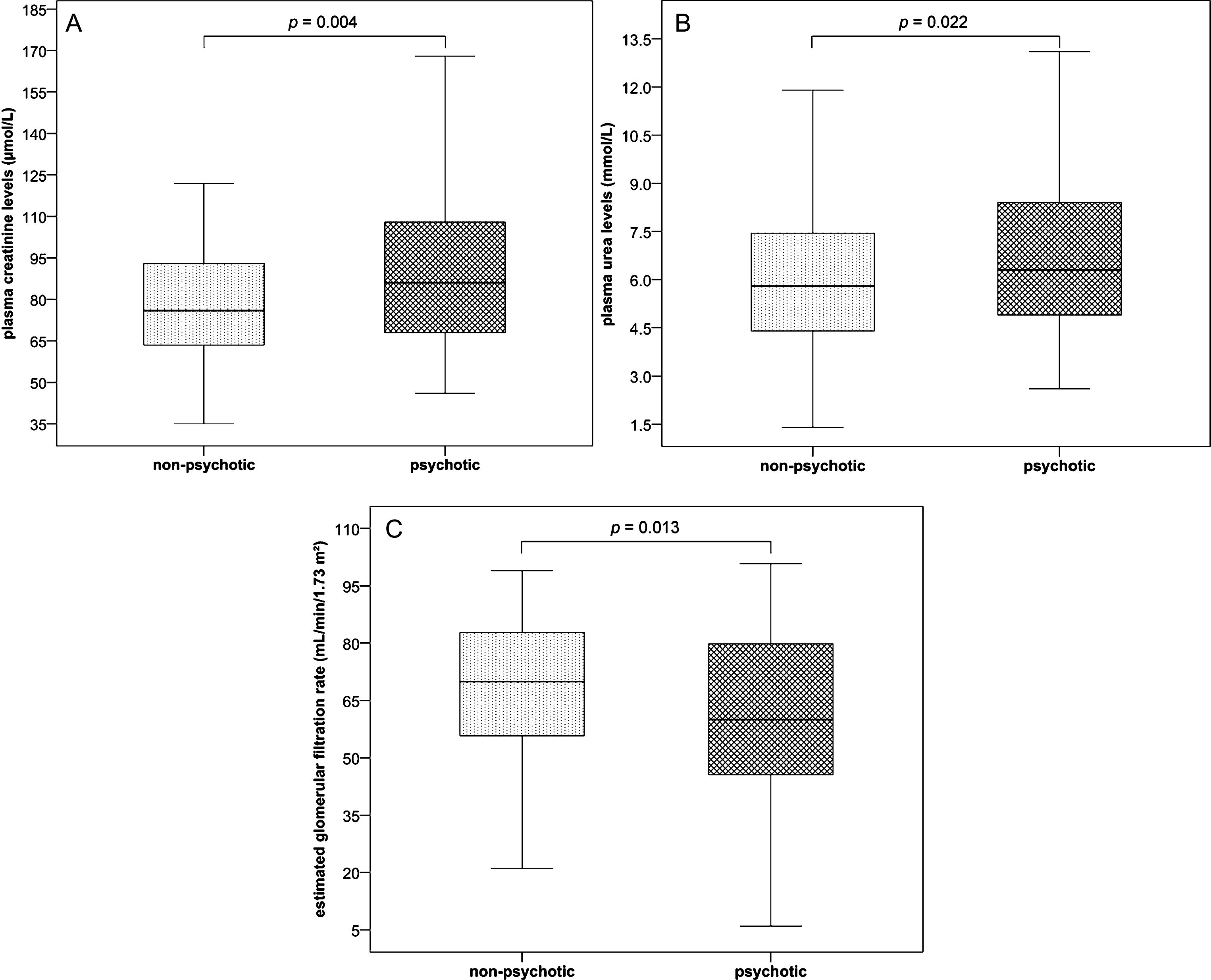
Box plots of plasma creatinine levels (A), plasma urea levels (B), and estimated glomerular filtration rates (C) of male and female patients with psychotic symptoms (psychotic, n = 117) and controls without psychotic symptoms (non-psychotic, n = 192) suffering from MCI or dementia.
Association of creatinine and eGFR and the occurrence of psychotic symptoms in females
Due to the fact that an association between parameters indicating a renal dysfunction and the occurrence of psychotic symptoms were mainly present in female patients, we further investigated creatinine and eGFR values in elderly women with or without psychotic symptoms. Given that creatinine levels >84μmol/L are regarded as pathologic, we found that only 25.4% of women without psychotic symptoms attained values above this level, but 48.8% of psychotic females presented pathological creatinine levels (p = 0.001; Fig. 2).
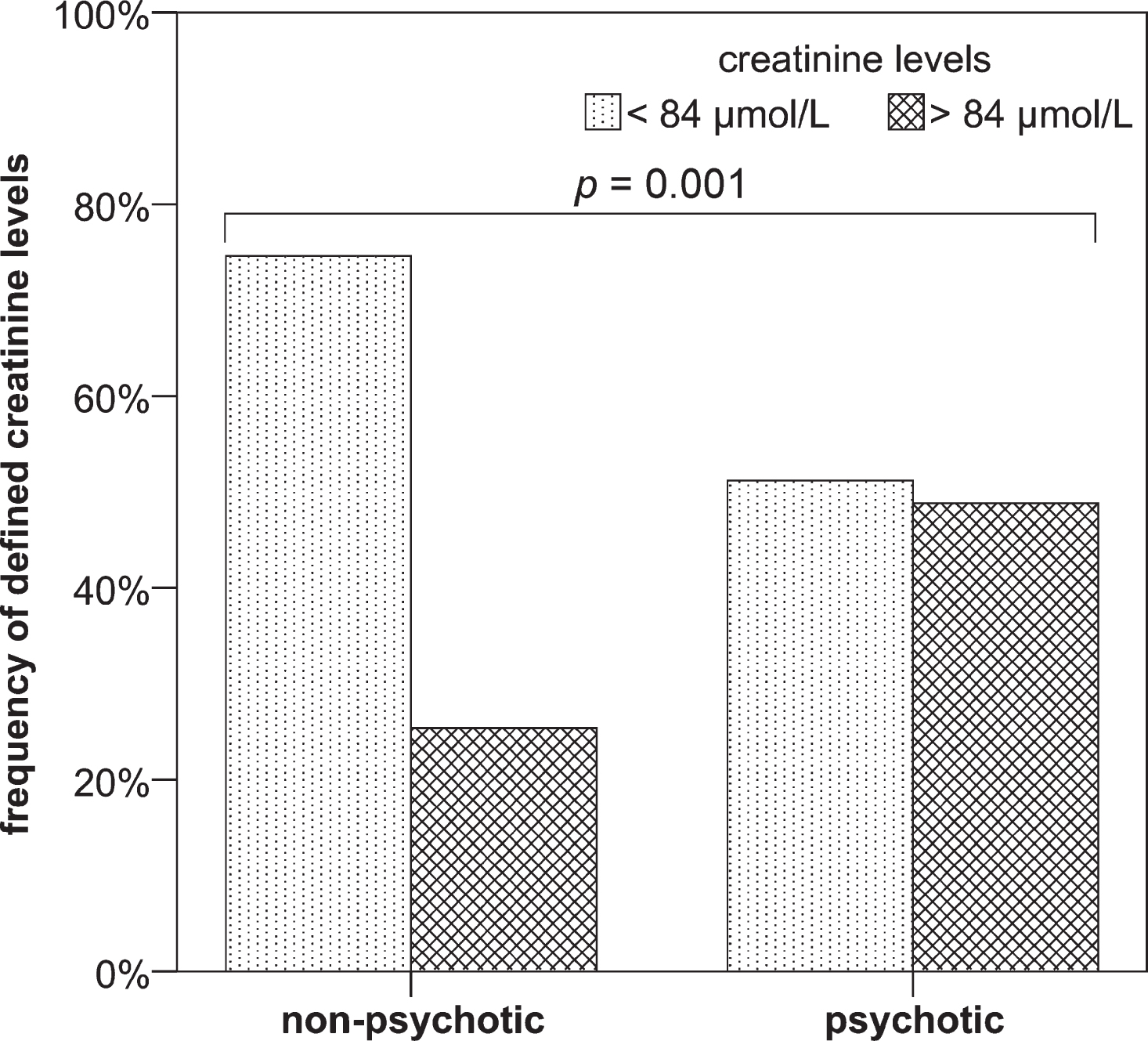
Frequencies of pathological increased (>84μmol/L) and normal (<84μmol/L) plasma creatinine levels in female patients with psychotic symptoms (psychotic, n = 84) and without psychotic symptoms (non-psychotic, n = 138) suffering from MCI or dementia.
Only a few patients (8.3% psychotic; 3.6% non-psychotic females) obtained values suitable for group 1 (normal kidney function). Women without psychotic symptoms were mainly (60.9%) integrated in group 2 and group 3 (31.2%), only a few (4.3%) showed a kidney failure to be classified into group 4 and none of them was put into group 5 (kidney failure; Fig. 3).
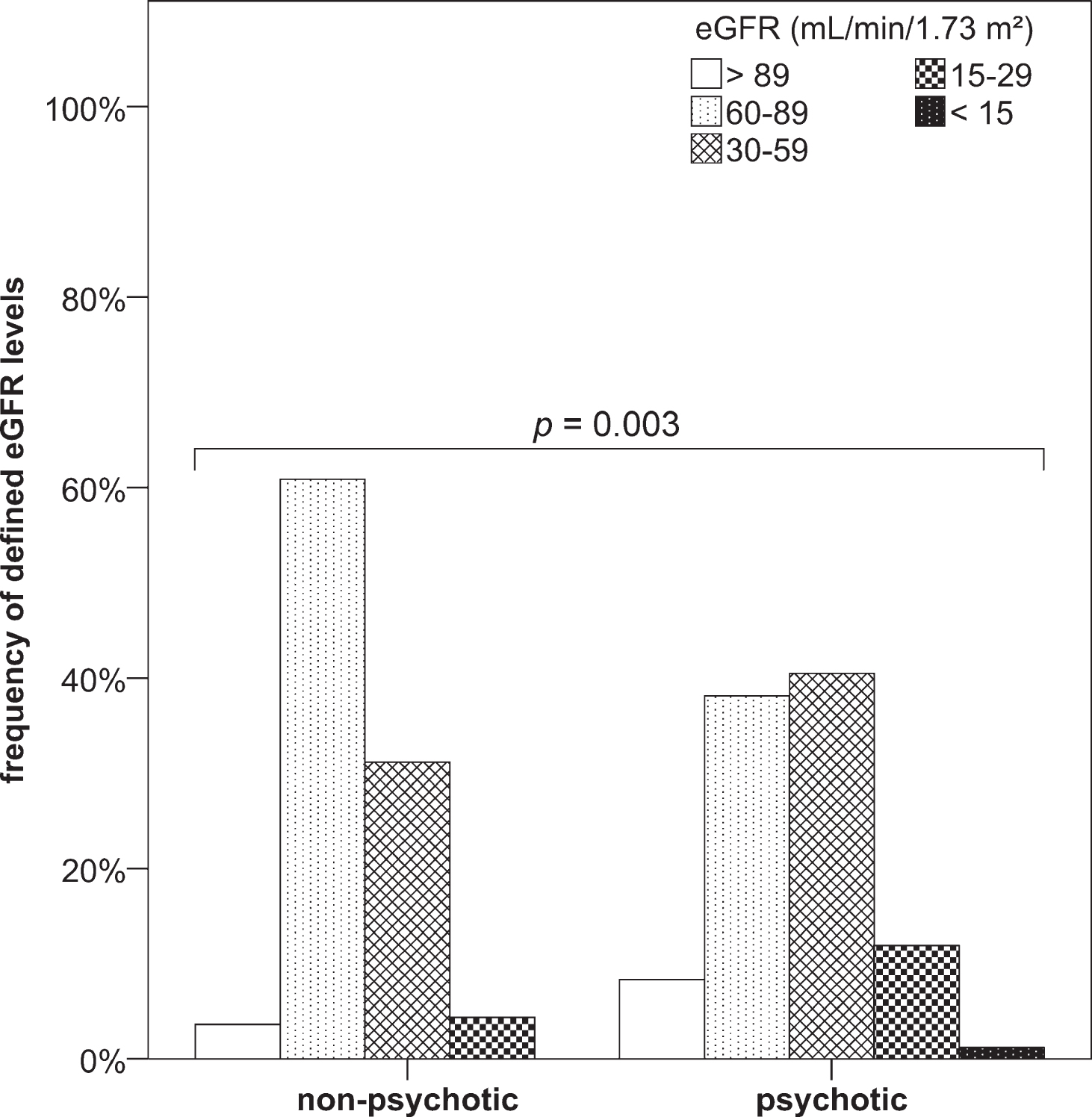
Frequency of defined eGFR levels (based on the CKD-EPI equation) in female patients with psychotic symptoms (psychotic, n = 84) and without psychotic symptoms (non-psychotic, n = 138) suffering from MCI or dementia.
Women with psychotic symptoms were comparably often classified into group 2 (38.1%) and group 3 (40.5%). In addition to the increased percentage classified into group 3, patients in group 4 (11.9%) were increased compared to the non-psychotic females, and even one patient (1.2%) was in group 5, indicating a kidney failure. Hypertension, hyperlipidemia, and diabetes mellitus did not influence the sex-specific presence of psychosis (Table 3).
Furthermore, male or female patients with an eGFR less than 60 mL/min/1.73 m2 had an approximately 2-fold increased risk of developing psychotic symptoms in our study (aOR 2.013; 95% CI 1.256–3.225; Supplementary Table 5).
Medication of psychotic patients
The majority of psychotic patients (95.7%) received immediately anti-psychotic medication (Table 4); the others refused the treatment. Data indicating that psychotic symptoms disappeared only using conventional therapies such as substitution of fluids and without drug treatment are therefore not available.
DISCUSSION
The aim of our present study was to evaluate blood parameters that could contribute to the occurrence of psychotic symptoms in patients with a decline in cognitive functions. Recently we found that the presence NMDA-R antibodies in serum of demented patients is one contributing factor [27–29]. Within our study cohort that consisted of patients with MCI or several types of dementia, we analyzed 55 parameters concerning their association with the presence of psychotic symptoms. We found that psychosis is associated with an increase in renal retention parameters and this holds true especially for female patients. However, the increased laboratory parameters are in the majority of patients not severely abnormal but more subclinical.
It is well known that hypertension, hyperlipidemia, and diabetes mellitus are risk factors for the development of neurocognitive disorders and chronic kidney disease [30, 31]. Ischemic cerebrovascular lesions, both symptomatic and subclinical, might explain the increased risk of patients with chronic kidney disorder risk of developing cognitive disorders and dementia [32]. It was also reported that patients with renal transplantation and chronic dialysis patients have an increased risk to develop hospitalized psychoses [33].
In general, we found no difference between the presence of psychosis in female and male patients with MCI or dementia. Our finding supports data showing that the occurrence of psychotic symptoms is associated with, for example, cognitive impairment but is gender-independent [34].
Gender differences were shown in several neuropsychiatric disorders: the prevalence of AD is higher in women compared to age-matched male individuals [35], which is also supported by our study. This might at least partially be affected by the decline of the female hormone estrogen after menopause since it has many effects in the brain such as neuroprotective, neurotrophic, neurodegenerative, anti-oxidative, and anti-inflammatory [36, 37]. Beside gender-related differences in kidney structure and functions, sex hormones are also important for the regulation of a variety of renal transport functions which result in differences in the development of various renal diseases [38, 39]. But also lifestyle differences such as dietary protein intake, salt, smoking, alcohol intake, and the prevalence and impact of metabolic syndrome might result in the higher incidence and prevalence of kidney disorders in men than in women [31]. However, the most important finding in our study was the association between enhanced renal retention parameters and psychosis, which was particular present in female patients. A huge problem in the treatment of demented patients is that despite higher rates of comorbid conditions, they tend to report fewer symptoms and complaints during visits with their primary care physicians. Consequently, the high prevalence of undiagnosed illness is not surprisingly [40]. It has to be considered that demented patients may display an increase in psychiatric symptoms before onset of acute illness such as dehydration or infection [41] and certain neuropsychiatric behaviors in demented patients may signal incipient acute illness [42]. For example, electrolyte disturbances associated with dehydration may result in challenging behaviors such as restlessness, delusions, or agitation [43], which is often misinterpreted as signaling a need for increased psychotropic medication [44]. Therefore, it is common that patients showing psychotic symptoms and a known history of dementia who were admitted to the hospital receive immediately antipsychotic medication.
Although the CRP level was unchanged between psychotic and non-psychotic patients, we detected in male psychotic patients an increase in leukocyte numbers indicating that an acute infection might be a reason for the symptoms in this subgroup. Concerning the prevalence of urinary tract infections, it is also important to note that patients with an undetected illness had lower functional ability and lower MMSE scores compared to those without illness. Therefore, the worsening of cognitive and functional status observed in patients with undiagnosed illness may be an indicator or potential risk factor for an underlying illness signaling the need for additional assessment [45]. On the other hand, 10% of elderly people without dementia suffer from psychotic symptoms. This is associated with a more rapid cognitive decline and an increased overall risk of later dementia [46]. In these patients, it is crucial to look at the laboratory parameters to exclude a delirium as cause for the symptoms.
Dementia, older age, infection, urinary catheterization, urea and electrolyte imbalance, and malnutrition are the most common factors associated with delirium [47]. Delirium is undiagnosed in over a half of patients with this condition, resulting in increased mortality. The most important reason for this is that the diagnosis of delirium rests solely on clinical skills; no diagnostic test exists to distinguish between dementia and delirium [23]. However, since we detected no significant associations between the level of the ions sodium, potassium, and chloride, which serve as indicators for dehydration and psychosis within female and male patients of any type of dementia, dehydration might play only a minor role in our study cohort.
In demented patients, it is not simple to differentiate a delirium from psychotic symptoms associated with dementia. The symptoms underlying the patients’ hospital admission should be treated fast to ensure a fast recovery, and the duration time in hospital should be kept short. This results in the rapid application of antipsychotic medications. Also in our study, we report that a large majority of patients were immediately treated with antipsychotic drugs and therefore we cannot differentiate between delirium and dementia. Whether simple application of fluid would be sufficient to improve the symptoms remains unknown. Therefore, we want to suggest that symptoms of patients presenting to hospitals are carefully considered, since many older adults may be quietly suffering from unrecognized disorders leading to under-treatment, wrong treatments, or unmet medical needs.
DISCLOSURE STATEMENT
Authors’ disclosures available online (http://j-alz.com/manuscript-disclosures/16-1306r1).